Embed Size (px)
Citation preview


The PDF version of the Atlas of Genetics and Cytogenetics in Oncology and Haematology is a reissue of the original articles published in collaboration with the Institute for Scientific and Technical Information (INstitut de l’Information Scientifique et Technique - INIST) of the French National Center for Scientific Research (CNRS) on its electronic publishing platform I-Revues. Online and PDF versions of the Atlas of Genetics and Cytogenetics in Oncology and Haematology are hosted by INIST-CNRS.
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Scope
The Atlas of Genetics and Cytogenetics in Oncology and Haematology is a peer reviewed on-line journal in open access, devoted to genes, cytogenetics, and clinical entities in cancer, and cancer-prone diseases. It presents structured review articles (“cards”) on genes, leukaemias, solid tumours, cancer-prone diseases, and also more traditional review articles (“deep insights”) on the above subjects and on surrounding topics. It also present case reports in hematology and educational items in the various related topics for students in Medicine and in Sciences.
Editorial correspondance
Jean-Loup Huret Genetics, Department of Medical Information, University Hospital F-86021 Poitiers, France tel +33 5 49 44 45 46 or +33 5 49 45 47 67 [email protected] or [email protected]
The Atlas of Genetics and Cytogenetics in Oncology and Haematology is published 4 times a year by ARMGHM, a non profit organisation. Philippe Dessen is the Database Director, and Alain Bernheim the Chairman of the on-line version (Gustave Roussy Institute – Villejuif – France).
http://AtlasGeneticsOncology.org
© ATLAS - ISSN 1768-3262

Atlas Genet Cytogenet Oncol Haematol. 1998;2(2)
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Editor
Jean-Loup Huret (Poitiers, France)
Volume 2, Number 2, April-June 1998
Table of contents
Gene Section
FGFR1 (fibroblast growth factor receptor 1) 35 Jean-Loup Huret
LCP1 (lymphocyte cytosolic protein1) 36 Sylvie Galiègue-Zouitina
MTCP1 (mature T cell proliferation 1) 37 Marc-Henri Stern
NF2 (neurofibromin 2) 39 Jean-Loup Huret
MYCN (myc myelocytomatosis viral related oncogene, neuroblastoma derived) 41 Jean-Loup Huret
POU2AF1 (POU domain, class 2, associating factor 1) 43 Sylvie Galiègue-Zouitina
ABCB1 (ATP-binding cassette, sub-family B (MDR/TAP), member 1) 45 Franck Viguié
TAL1 (T-cell acute leukemia 1) 47 Jean-Loup Huret, Marie-Claude Labastie
TCL1 (T cell leukemia/lymphoma 1) 49 Marc-Henri Stern
TCTA (T-cell leukemia translocation-associated gene) 51 Jean-Loup Huret
ZNF198 (zinc finger protein 198) 52 Jean-Loup Huret, Dominique Leroux
Leukaemia Section
t(9;12)(p24;p13) 54 Jean-Loup Huret
del(9q) solely 55 Franck Viguié

Atlas Genet Cytogenet Oncol Haematol. 1998;2(2)
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Essential thrombocythemia 57 Jean-Loup Huret
Acute basophilic leukemia; t(X;6)(p11;q23) 58 Nicole Dastugue
t(5;14)(q33;q32) PDGFRB/TRIP11 59 Jean-Loup Huret
t(11;16)(q23;p13) 60 Jean-Loup Huret
t(16;21)(p11;q22) 62 Christine Pérot
Solid Tumour Section
Nervous system: Peripheral neuroblastic tumours (Neuroblastoma, Ganglioneuroblastoma, Ganglioneuroma) 63 Jérôme Couturier, Daniel Satgé
Cancer Prone Disease Section
Bloom syndrome 65 Jean-Loup Huret
Dubowitz syndrome 67 Jean-Loup Huret, Claude Léonard
Fanconi anaemia 68 Jean-Loup Huret

Atlas Genet Cytogenet Oncol Haematol. 1998;2(2)
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS

Gene Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 35
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
FGFR1 (fibroblast growth factor receptor 1) Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France
Published in Atlas Database: March 1998
Online updated version: http://AtlasGeneticsOncology.org/Genes/FGFR1113.html DOI: 10.4267/2042/37403
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: BFGFR (basic fibroblast growth factor receptor); FLT2 (FMS-like tyrosine kinase 2); FLG (FMS-like gene); CEK; FGFBR; N-SAM Location: 8p11 Local order: more telomeric than MOZ.
DNA/RNA Transcription 2.7 mRNA.
Protein Description 822 amino acids; 100-135 kDa glycoprotein from a 90-115 kDa protein core; tyrosine kinase receptor; contains three major domains: an extracellular domain with 3 Ig-like loops, a transmembrane domain and an intracellular domain with tyrosine kinase activity.
Localisation Plasma membrane.
Function FGF receptor with tyrosine kinase activity; binding of ligand (FGF) induces receptor dimerization, autophosphorylation and signal transduction.
Homology With other FGFR (FGFR2, FGFR3, and FGFR4).
Implicated in t(8;13)(p12;q12)/ANLL-NHL → ZNF198/FGFR1 Disease Combined myeloid malignancy and T-cell NHL. Prognosis Very poor (median survival: 12 mths).
Cytogenetics Additional anomalies: +8, +der(13), +21. Hybrid/Mutated Gene 5' ZNF198 - 3' FGFR1. Abnormal Protein N-term zinc fingers from ZNF198 fused to the Tyrosine kinase domain of FGFR1 in C-term. Oncogenesis Constitutive activation of FGFR1.
Pfeiffer syndrome (inborn disease) Disease One form of Pfeiffer syndrome, an autosomal dominant craniosynostosis syndrome with broad thumbs and usually no mental deficiency, is due to a mutation in amino acid 252 of FGFR1.
References Lee PL, Johnson DE, Cousens LS, Fried VA, Williams LT. Purification and complementary DNA cloning of a receptor for basic fibroblast growth factor. Science 1989;245:57-60.
Itoh N, Terachi T, Ohta M, Seo MK. The complete amino acid sequence of the shorter form of human basic fibroblast growth factor receptor deduced from its cDNA. Biochem Biophys Res Commun 1990;169:680-685.
Johnson DE, Lu J, Chen H, Werner S, Williams LT. The human fibroblast growth factor receptor genes: a common structural arrangement underlies the mechanisms for generating receptor forms that differ in their third immunoglobulin domain. Mol Cell Biol 1991;11:4627-4634.
Wennstrom S, Sandstrom C, Claesson-Welsh L. cDNA cloning and expression of a human FGF receptor which binds acidic and basic FGF. Growth Factors 1991;4:197-208.
Webster MK, Donoghue DJ. FGFR activation in skeletal disorders: too much of a good thing. Trends Genet 1997;13:178-182. (Review).
This article should be referenced as such:
Huret JL. FGFR1 (fibroblast growth factor receptor 1). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):35.

Gene Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 36
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
LCP1 (lymphocyte cytosolic protein1) Sylvie Galiègue-Zouitina
U.124 INSERM, I.R.C.L., Place de Verdun, 59045 Lille Cedex, France
Published in Atlas Database: March 1998
Online updated version: http://AtlasGeneticsOncology.org/Genes/LCP1ID95.html DOI: 10.4267/2042/37404
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: L-Plastine Location: 13q14
DNA/RNA Description Spans on a 90 kb genomic fragment; 16 exons, large first intron (20 kb).
Transcription 3.7 kb mRNA; coding sequence from exon 2 to exon 16: 3500 bp.
Protein Description 570 amino acids.
Expression Restricted to the hematopoietic cells (leukocytes); expression induced in all tumor cells of all tissues.
Localisation Membrane.
Homology Belongs to an actin-binding protein family (T-Plastin, Fimbrin, I-Plastin).
Implicated in
t(3;13)(q27;q14)/NHL → LCP1/ BCL6 Disease Non Hodgkin follicular as well as Burkitt lymphomas.
Cytogenetics t(3;13) is observed as a secondary anomaly. Hybrid/Mutated Gene Both 5' L-Plastin- 3' BCL6 and 5' BCL6 - 3' L-Plastin, leading to two fusion transcripts. Abnormal Protein No fusion protein, but promoter exchange between both partner genes.
References Lin CS, Aebersold RH, Kent SB, Varma M, Leavitt J. Molecular cloning and characterization of plastin, a human leukocyte protein expressed in transformed human fibroblasts. Mol Cell Biol 1988 Nov;8(11):4659-4668.
Lin CS, Park T, Chen ZP, Leavitt J. Human plastin genes. Comparative gene structure, chromosome location, and differential expression in normal and neoplastic cells. J Biol Chem 1993 Feb 5;268(4):2781-2792.
Park T, Chen ZP, Leavitt J. Activation of the leukocyte plastin gene occurs in most human cancer cells. Cancer Res 1994 Apr 1;54(7):1775-1781.
Prassler J, Stocker S, Marriott G, Heidecker M, Kellermann J, Gerisch G. Interaction of a Dictyostelium member of the plastin/fimbrin family with actin filaments and actin-myosin complexes. Mol Biol Cell 1997 Jan;8(1):83-95.
Lai JL, Michaux L, Dastugue N, Vasseur F, Daudignon A, Facon T, Bauters F, Zandecki M. Cytogenetics in multiple myeloma: a multicenter study of 24 patients with t(11;14)(q13;q32) or its variant. Cancer Genet Cytogenet 1998 Jul 15;104(2):133-8.
This article should be referenced as such:
Galiègue-Zouitina S. LCP1 (lymphocyte cytosolic protein1). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):36.
Gene Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 37
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
MTCP1 (mature T cell proliferation 1) Marc-Henri Stern
Unité INSERM U462, Centre Hayem, Hopital Saint Louis, 75475 Paris Cedex 10, France
Published in Atlas Database: March 1998
Online updated version: http://AtlasGeneticsOncology.org/Genes/MTCP1ID89.html DOI: 10.4267/2042/37405
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: C6.1B Location: Xq28 Local order: Centromere- Factor VIII - c6.1A - MTCP1 - telomere.
MTCP1 (Xq28) - Courtesy Mariano Rocchi, Resources for Molecular Cytogenetics. Laboratories willing to validate the probes are welcome: contact [email protected].
DNA/RNA
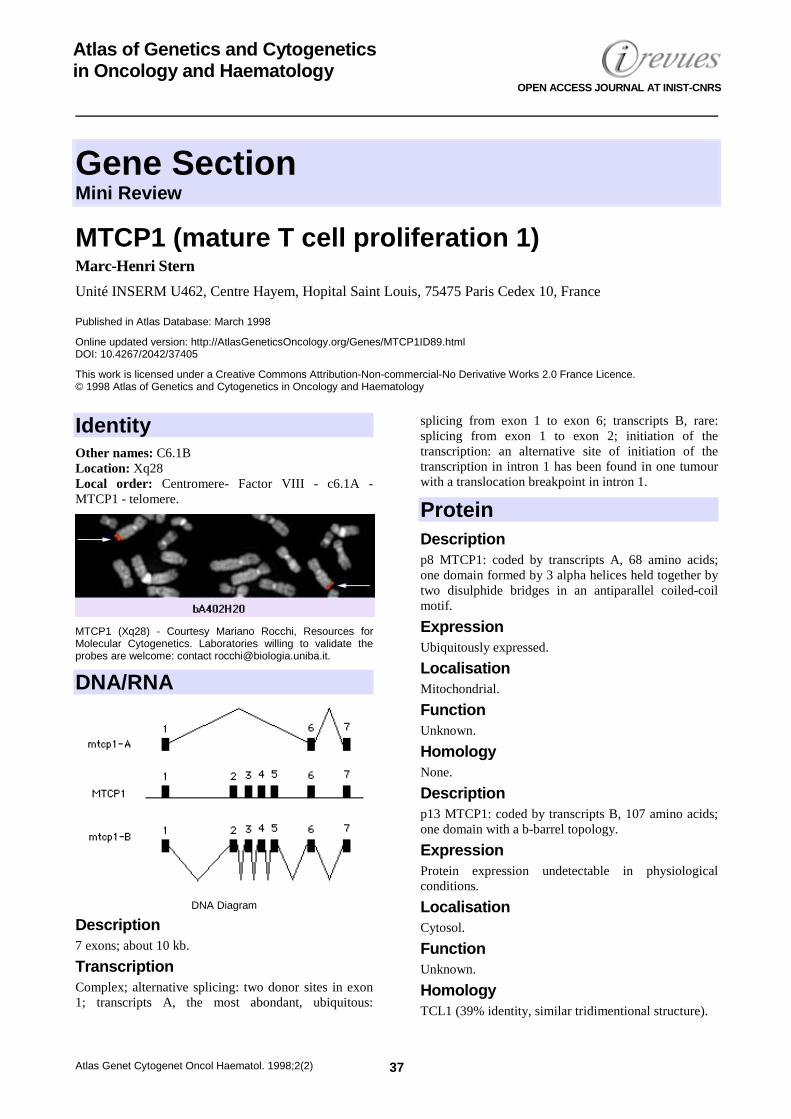
DNA Diagram
Description 7 exons; about 10 kb.
Transcription Complex; alternative splicing: two donor sites in exon 1; transcripts A, the most abondant, ubiquitous:
splicing from exon 1 to exon 6; transcripts B, rare: splicing from exon 1 to exon 2; initiation of the transcription: an alternative site of initiation of the transcription in intron 1 has been found in one tumour with a translocation breakpoint in intron 1.
Protein Description p8 MTCP1: coded by transcripts A, 68 amino acids; one domain formed by 3 alpha helices held together by two disulphide bridges in an antiparallel coiled-coil motif.
Expression Ubiquitously expressed.
Localisation Mitochondrial.
Function Unknown.
Homology None.
Description p13 MTCP1: coded by transcripts B, 107 amino acids; one domain with a b-barrel topology.
Expression Protein expression undetectable in physiological conditions.
Localisation Cytosol.
Function Unknown.
Homology TCL1 (39% identity, similar tridimentional structure).

MTCP1 (mature T cell proliferation 1) Stern MH
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 38
Implicated in t(X;14)(q28;q12)/prolymphocytic leukaemia → TCRA-D/MTCP1 Disease T-cell prolymphocytic leukaemia. Cytogenetics Associated with i(8q). Hybrid/Mutated Gene Unconstant TCRA-c6.1A transcripts have been described. Abnormal Protein None. Oncogenesis Overexpression of p13 MTCP1 is considered as critical in the oncogenetic mechanism.
t(X;7)(q28;q35)/prolymphocytic leukaemia → TCRB/MTCP1 Disease T-cell prolymphocytic leukaemia. Oncogenesis Overexpression of p13 MTCP1.
References Fisch P, Forster A, Sherrington PD, Dyer MJ, Rabbitts TH. The chromosomal translocation t(X;14)(q28;q11) in T-cell pro-lymphocytic leukaemia breaks within one gene and activates another. Oncogene 1993 Dec;8(12):3271-6.
Soulier J, Madani A, Cacheux V, Rosenzwajg M, Sigaux F, Stern MH. The MTCP-1/c6.1B gene encodes for a cytoplasmic 8 kD protein overexpressed in T cell leukemia bearing a t(X;14) translocation. Oncogene 1994 Dec;9(12):3565-70.
Thick J, Mak YF, Metcalfe J, Beatty D, Taylor AM. A gene on chromosome Xq28 associated with T-cell prolymphocytic leukemia in two patients with ataxia telangiectasia. Leukemia 1994 Apr;8(4):564-73.
Madani A, Choukroun V, Soulier J, Cacheux V, Claisse JF, Valensi F, Daliphard S, Cazin B, Levy V, Leblond V, Daniel MT, Sigaux F, Stern MH. Expression of p13MTCP1 is restricted to mature T-cell proliferations with t(X;14) translocations. Blood 1996 Mar 1;87(5):1923-7.
Thick J, Metcalfe JA, Mak YF, Beatty D, Minegishi M, Dyer MJ, Lucas G, Taylor AM. Expression of either the TCL1 oncogene, or transcripts from its homologue MTCP1/c6.1B, in leukaemic and non-leukaemic T cells from ataxia telangiectasia patients. Oncogene 1996 Jan 18;12(2):379-86.
Barthe P, Yang YS, Chiche L, Hoh F, Strub MP, Guignard L, Soulier J, Stern MH, van Tilbeurgh H, Lhoste JM, Roumestand C. Solution structure of human p8MTCP1, a cysteine-rich protein encoded by the MTCP1 oncogene, reveals a new alpha-helical assembly motif. J Mol Biol 1997 Dec 19;274(5):801-15.
Gritti C, Choukroun V, Soulier J, Madani A, Dastot H, Leblond V, Radford-Weiss I, Valensi F, Varet B, Sigaux F, Stern MH. Alternative origin of p13MTCP1-encoding transcripts in mature T-cell proliferations with t(X;14) translocations. Oncogene 1997 Sep;15(11):1329-35.
Yang YS, Guignard L, Padilla A, Hoh F, Strub MP, Stern MH, Lhoste JM, Roumestand C. Solution structure of the recombinant human oncoprotein p13MTCP1. J Biomol NMR 1998 Apr;11(3):337-54.
This article should be referenced as such:
Stern MH. MTCP1 (mature T cell proliferation 1). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):37-38.

Gene Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 39
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
NF2 (neurofibromin 2) Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France
Published in Atlas Database: March 1998
Online updated version: http://AtlasGeneticsOncology.org/Genes/NF2117.html DOI: 10.4267/2042/37406
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: SCH (schwannoma) Location: 22q12.1-12.2 junction, incidentally not far from EWS.
DNA/RNA Description 16 exons; spans 120 kb; open reading frame: 1.8 kb.
Transcription Alternate splicings, in particular after exon 15.
Protein Description Called merlin, schwannomin, or SCH; 590 or 595 amino acids; 66 kDa; NH2 -- membrane binding -- large a helix domain binding to actin of the cytoskeleton -- COOH
Expression Wide: in lung, kidney, ovary, breast, placenta, neuroblasts; high in fetal brain.
Localisation Membrane associated.
Function Membrane-cytoskeleton anchor (as APC also appears to be); role in the development of extraembryonic structures before gastrulation; has characteristics of a tumour suppressor, as has been found in sporadic as well as neurofibromatosis type 2 induced schwannomas and meningiomas.
Homology Ezrin, talin, radixin, moesin, members of the erythrocytes band 4.1 family, especially in the N-term.
Mutations Germinal Inborn condition of neurofibromatosis type 2 patients: protein truncations due to various frameshift deletions or insertions or nonsense mutations; splice-site or missense mutations are also found; phenotype-genotype correlations are observed (i.e. those severe phenotypes are found in cases with protein truncations rather than those with amino acid substitution).
Somatic Mutation and allele loss events in tumours in neurofibromatosis type 2 and in sporadic schwannomas and meningiomas are in accordance with the two-hit model for neoplasia, as is found in retinoblastoma.
Implicated in Neurofibromatosis type 2 Disease Autosomal dominant cancer prone disease; neurofibromatosis type 2 (NF2: the same symbol is used for the disease neurofibromatosis type 2 and the gene neurofibromin 2) is a hamartoneoplastic syndrome. Prognosis Hamartomas have a potential towards neoplasia; those, in NF2, are schwannomas and meningiomas.
Sporadic meningioma Sporadic schwannoma Other tumours Ependymoma; mesothelioma.
References Rouleau GA, Merel P, Lutchman M, Sanson M, Zucman J, Marineau C, Hoang-Xuan K, Demczuk S, Desmaze C,

NF2 (neurofibromatosis type 2) Huret JL
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 40
Plougastel B, et al. Alteration in a new gene encoding a putative membrane-organizing protein causes neuro-fibromatosis type 2. Nature 1993 Jun 10;363(6429):515-21.
Parry DM, Eldridge R, Kaiser-Kupfer MI, Bouzas EA, Pikus A, Patronas N. Neurofibromatosis 2 (NF2): clinical characteristics of 63 affected individuals and clinical evidence for heterogeneity. Am J Med Genet 1994 Oct 1;52(4):450-61.
Marineau C, Mérel P, Rouleau GA, Thomas G. Le gène de la neurofibromatose de type 2. Médecine/sciences 1995;11(1):35-42. (Review). French.
Parry DM, MacCollin MM, Kaiser-Kupfer MI, Pulaski K, Nicholson HS, Bolesta M, Eldridge R, Gusella JF. Germ-line mutations in the neurofibromatosis 2 gene: correlations with disease severity and retinal abnormalities. Am J Hum Genet 1996 Sep;59(3):529-39.
Ruttledge MH, Andermann AA, Phelan CM, Claudio JO, Han FY, Chretien N, Rangaratnam S, MacCollin M, Short P, Parry D, Michels V, Riccardi VM, Weksberg R, Kitamura K, Bradburn
JM, Hall BD, Propping P, Rouleau GA. Type of mutation in the neurofibromatosis type 2 gene (NF2) frequently determines severity of disease. Am J Hum Genet 1996 Aug;59(2):331-42.
McClatchey AI, Saotome I, Ramesh V, Gusella JF, Jacks T. The Nf2 tumor suppressor gene product is essential for extraembryonic development immediately prior to gastrulation. Genes Dev 1997 May 15;11(10):1253-65.
Deguen B, Merel P, Goutebroze L, Giovannini M, Reggio H, Arpin M, Thomas G. Impaired interaction of naturally occurring mutant NF2 protein with actin-based cytoskeleton and membrane. Hum Mol Genet 1998 Feb;7(2):217-26.
This article should be referenced as such:
Huret JL. NF2 (neurofibromin 2). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):39-40.

Gene Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 41
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
MYCN (myc myelocytomatosis viral related oncogene, neuroblastoma derived) Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France
Published in Atlas Database: March 1998
Online updated version: http://AtlasGeneticsOncology.org/Genes/NMYC112.html DOI: 10.4267/2042/37407
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity
MYCN (2p24) - Courtesy Mariano Rocchi, Resources for Molecular Cytogenetics. Laboratories willing to validate the probes are welcome: contact [email protected].
Location: 2p24.1 Local order: centromeric to DDX1
DNA/RNA Description 3 exons.
Protein Description 464 amino acids; contains a phosphorylation site, an acidic domain, an HLH motif, and a leucine zipper in
C-term; forms heterodimers with MAX and recognize the core concensus sequence CACCTG. Expression During fetal development.
Localisation Nuclear.
Function Probable transcription factor; possible role during tissue differentiation.
Homology With members of the myc family of helix-loop-helix transcription factors.

MYCN (myc myelocytomatosis viral related oncogene, neuroblastoma derived) Huret JL
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 42
Mutations Somatic Amplification, either in extrachromosomal double minutes or in homogeneously staining regions within chromosomes (there is amplification when, for exemple, 10 to 1000 copies of a gene are present in a cell); found amplified in a variety of human tumours, in particular in and also in retinoblastoma, small cell lung carcinoma, astrocytoma; level of amplification related to the tumour progression; transgenic mice that overexpress MYCN in neuroectodermal cells develop neuroblastoma.
Implicated in Neuroblastoma Oncogenesis MYCN amplification is found in 15% of neuroblastoma, is an adverse prognostic feature per se, and is often associated with other adverse features (older age, abdominal tumour, advanced disease, and
high lactate dehydrogenase, ferritin, and neuron-specific enolase serum levels).
References Kohl NE, Kanda N, Schreck RR, Bruns G, Latt SA, Gilbert F, Alt FW. Transposition and amplification of oncogene-related sequences in human neuroblastomas. Cell 1983 Dec;35(2 Pt 1):359-67.
Tonini GP, Boni L, Pession A, Rogers D, Iolascon A, Basso G, Cordero di Montezemolo L, Casale F, Pession A, Perri P, Mazzocco K, Scaruffi P, Lo Cunsolo C, Marchese N, Milanaccio C, Conte M, Bruzzi P, De Bernardi B. MYCN oncogene amplification in neuroblastoma is associated with worse prognosis, except in stage 4s: the Italian experience with 295 children. J Clin Oncol 1997 Jan;15(1):85-93.
Weiss WA, Aldape K, Mohapatra G, Feuerstein BG, Bishop JM. Targeted expression of MYCN causes neuroblastoma in transgenic mice. EMBO J 1997 Jun 2;16(11):2985-95.
This article should be referenced as such:
Huret JL. MYCN (myc myelocytomatosis viral related oncogene, neuroblastoma derived). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):41-42.

Gene Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 43
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
POU2AF1 (POU domain, class 2, associating factor 1) Sylvie Galiègue-Zouitina
U.124 INSERM, I.R.C.L., Place de Verdun, 59045 Lille Cedex, France
Published in Atlas Database: March 1998
Online updated version: http://AtlasGeneticsOncology.org/Genes/OBF94.html DOI: 10.4267/2042/37408
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: BOB1; OCA-B; POU2AF1 (POU domain, class2, associating factor 1) Location: 11q23.1 Local order: telomeric to ATM.
POU2AF1 (11q23) - Courtesy Mariano Rocchi, Resources for Molecular Cytogenetics. Laboratories willing to validate the probes are welcome.
DNA/RNA
DNA Diagram
Description Spans on a 30 kb genomic fragment; five exons; large fifth exon, with many 3'-UTR repetitive elements, two pyrimidine rich regions (a duplicated CT-rich region and a [CCTT]n tetranucleotide tandem repeat) and a 282 nucleotides long Alu element.
Transcription 3.4 kb mRNA; coding sequence: 770 bp, spanning from the end of exon 1 to the beginning of exon 5.
Protein Description 256 amino acids; 27.4 kDa; proline rich protein with no recognizable domain or motifs.
Expression Constitutively expressed in B-cells and inducible in T-cells.
Localisation Nuclear.
Function B-cell specific transcriptional coactivator: involved in the transcription of immunoglobulin genes through recruitment to the highly conserved octamer site of immunoglobulin promoters, mediated by either Oct-1 or Oct-2 transcription factor; forms a ternary complex on DNA together with either Oct-1 or Oct-2 transcription factor; is essential for the response of B-cells to antigens and is required for the formation of germinal centres.
Homology No homology to known proteins.
Implicated in t(3;11)(q27;q23.1)/NHL → BCL6/OBF1 Disease NHL.

POU2AF1 (POU domain, class 2, associating factor 1) Galiègue-Zouitina S
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 44
Cytogenetics Found in complex karyotypes. Hybrid/Mutated Gene 5' BOB1 - 3' BCL6 and 5' BCL6 - 3' BOB1, leading to two fusion transcripts. Abnormal Protein No fusion protein, but promoter exchange between both partner genes.
References Gstaiger M, Knoepfel L, Georgiev O, Schaffner W, Hovens CM. A B-cell coactivator of octamer-binding transcription factors. Nature 1995 Jan 26;373(6512):360-2.
Luo Y, Roeder RG. Cloning, functional characterization, and mechanism of action of the B-cell-specific transcriptional coactivator OCA-B. Mol Cell Biol 1995 Aug;15(8):4115-24.
Strubin M, Newell JW, Matthias P. OBF-1, a novel B cell-specific coactivator that stimulates immunoglobulin promoter
activity through association with octamer-binding proteins. Cell 1995 Feb 10;80(3):497-506.
Galiègue Zouitina S, Quief S, Hildebrand MP, Denis C, Lecocq G, Collyn-d'Hooghe M, Bastard C, Yuille M, Dyer MJ, Kerckaert JP. The B cell transcriptional coactivator BOB1/OBF1 gene fuses to the LAZ3/BCL6 gene by t(3;11)(q27;q23.1) chromosomal translocation in a B cell leukemia line (Karpas 231). Leukemia 1996 Apr;10(4):579-87.
Schubart DB, Rolink A, Kosco-Vilbois MH, Botteri F, Matthias P. B-cell-specific coactivator OBF-1/OCA-B/Bob1 required for immune response and germinal centre formation. Nature 1996 Oct 10;383(6600):538-42.
Zwilling S, Dieckmann A, Pfisterer P, Angel P, Wirth T. Inducible expression and phosphorylation of coactivator BOB.1/OBF.1 in T cells. Science 1997 Jul 11;277(5323):221-5.
This article should be referenced as such:
Gali. POU2AF1 (POU domain, class 2, associating factor 1)
Atlas Genet Cytogenet Oncol Haematol.1998;2(2):43-44.

Gene Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 45
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
ABCB1 (ATP-binding cassette, sub-family B (MDR/TAP), member 1) Franck Viguié
Laboratoire de Cytogénétique - Service d'Hématologie Biologique, Hôpital Hôtel-Dieu, 75181 Paris Cedex 04, France
Published in Atlas Database: March 1998
Online updated version: http://AtlasGeneticsOncology.org/Genes/PGY1ID105.html DOI: 10.4267/2042/37409
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: MDR1 (multidrug resistance 1) Location: 7q21.2
DNA/RNA Description Spans on a 120 kb genomic fragment; separated from MDR3 gene (which is transcribed in the same direction) by only 34 kb of intergenic DNA.
Transcription 5 kb mRNA.
Protein Description The protein is called P-glycoprotein; 170 kDa transmembrane glycoprotein which includes 10-15 kDa of N-term glycosylation; the N-term half of the molecule contains 6 transmembrane domains, followed by a large cytoplasmic domain with an ATP binding site, and then a second section with 6 transmembrane domains and an ATP binding site which shows over 65% of amino acid similarity with the first half of the polypeptide.
Expression Normally expressed at secretory surface of a number of tissues, including biliary canaliculi, proximal tubules of the kidney, intestinal and colonic epithelium; hematopoietic stem cells express high levels of P-glycoprotein; overexpressed in many multidrug resistant cell lines and in tumour cells resistant to chemotherapy.
Localisation Mainly at the cell membrane, with a secondary localisation at the Golgi apparatus.
Function The P-glycoprotein is an energy-dependent efflux pump involved in extrusion of many types of lypophilic coumpounds; it may acts in normal tissues as a protective mechanism against noxious xenobiotics and as a transporter of endogenous substrates; in tumour cells, the drug efflux pump results in a decrease in intracellular drug concentration.
Homology Closely related gene to MDR3 (also called PGY3), located at the same chromosomal site but not implicated in multidrug resistance; there are 3 murine homolog genes (mdr1, mdr2, mdr3) out of which only 2 (mdr1 and mdr3) are involved in multidrug resistance; member of a large superfamily of transmembrane transporter proteins named ATP Binding Cassette (ABC) transporters or Traffic ATPases; structural homology with other ABC transporter proteins (CFTR, MRP).
Implicated in Tumour cells resistance Disease Tumour cells resistance to a wide variety of antineoplasic agents: doxorubicin, daunorubicin, vinblastine, vincristine, colchicine, actinomycine D, etoposide, tenoposide, mitoxantrone, homoharringtonine; this phenomenon is named 'multidrug resistance' (MDR); P-glycoprotein is the main protein responsible for the MDR phenotype;

ABCB1 (ATP-binding cassette, sub-family B (MDR/TAP), member 1) Viguié F
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 46
however, other agents may be involved in MDR, independently or in association with P-glycoprotein: "multidrug resistant associated protein" (MRP), "lung resistance protein" (LRP), 'anthracycline associated resistance protein" (ARX).
Leukemias Disease In leukemia, MDR1 overexpression is observed in patients with a lower complete remission rate and with a shortening of overall survival; frequently associated with intermediate and poor prognosis karyotype; in ANLL, approximately 50% of patients are MDR positive at diagnosis (range 22-70%) and the MDR phenotype is more frequently observed in CD34+ leukemias; in ALL, the average number of MDR-positive cases is 22% at diagnosis.
Tumour cell lines Note In numerous continuous tumour cell lines which acquired experimentally a MDR phenotype when cultured with progressively increasing drug concentration, the acquisition of MDR was associated with hyperexpression of P-glycoprotein; for the higher levels of expression, southern blots revealed an increase in the number of copies of the MDR1 gene per cell. Cytogenetics The genomic amplification of MDR1 appears as extrachromosomic 'double-minute chromosomes' (DM) or intrachromosomic 'homogeneous staining regions' (HSR). Oncogenesis Amplification.
References Ruiz JC, Choi KH, von Hoff DD, Robinson IB, Wahl GM. Autonomously replicating episomes contain mdr1 genes in a multidrug-resistant human cell line. Mol Cell Biol 1989 Jan;9(1):109-15.
Baer MR, Bloomfield CD. Multidrug resistance in acute myeloid leukemia. J Natl Cancer Inst 1991 May 15;83(10):663-5.
Trent JM, Callen DE. Molecular and Cellular Biology of Multidrug Resistance in Tumor Cells (IM Roninson Ed.), Plenum Publishing Corporation 1991; pp169.
Schoenlein PV, Shen DW, Barrett JT, Pastan I, Gottesman MM. Double minute chromosomes carrying the human multidrug resistance 1 and 2 genes are generated from the dimerization of submicroscopic circular DNAs in colchicine-
selected KB carcinoma cells. Mol Biol Cell 1992 May;3(5):507-20.
Simon SM, Schindler M. Cell biological mechanisms of multidrug resistance in tumors. Proc Natl Acad Sci USA 1994 Apr 26;91(9):3497-504.
Torigoe K, Sato S, Kusaba H, Kohno K, Kuwano M, Okumura K, Green ED, Tsui LC, Scherer SW, Schlessinger D, et al. A YAC-based contig of 1.5 Mb spanning the human multidrug resistance gene region and delineating the amplification unit in three human multidrug-resistant cell lines. Genome Res 1995 Oct;5(3):233-44.
Bosch I, Croop J. P-glycoprotein multidrug resistance and cancer. Biochim Biophys Acta 1996 Oct 9;1288(2):F37-54.
Gottesman MM, Pastan I, Ambudkar SV. P-glycoprotein and multidrug resistance. Curr Opin Genet Dev 1996 Oct;6(5):610-7.
Hegewisch-Becker S, Hossfeld DK. The MDR phenotype in hematologic malignancies: prognostic relevance and future perspectives. Ann Hematol 1996 Mar;72(3):105-17.
Srivastava RK, Srivastava AR, Cho-Chung YS. Multidrug resistance in cancer. Int J Oncol 1996:9:879-84. (Review)
Zhou DC, Ramond S, Viguie F, Faussat AM, Zittoun R, Marie JP. Sequential emergence of MRP- and MDR1-gene over-expression as well as MDR1-gene translocation in homoharringtonine-selected K562 human leukemia cell lines. Int J Cancer 1996 Jan 26;65(3):365-71.
Hunault M, Zhou D, Delmer A, Ramond S, Viguié F, Cadiou M, Perrot JY, Levy V, Rio B, Cymbalista F, Zittoun R, Marie JP. Multidrug resistance gene expression in acute myeloid leukemia: major prognosis significance for in vivo drug resistance to induction treatment. Ann Hematol 1997 Feb;74(2):65-71.
Martínez A, San Miguel JF, Valverde B, Bárez A, Moro MJ, García-Marcos MA, Pérez-Simón JA, Vidriales B, Orfao A. Functional expression of MDR-1 in acute myeloid leukemia: correlation with the clinical-biological, immunophenotypical, and prognostic disease characteristics. Ann Hematol 1997 Sep;75(3):81-6.
van den Heuvel-Eibrink MM, van der Holt B, te Boekhorst PA, Pieters R, Schoester M, Löwenberg B, Sonneveld P. MDR 1 expression is an independent prognostic factor for response and survival in de novo acute myeloid leukaemia. Br J Haematol 1997 Oct;99(1):76-83.
Willman CL. The prognostic significance of the expression and function of multidrug resistance transporter proteins in acute myeloid leukemia: studies of the Southwest Oncology Group Leukemia Research Program. Semin Hematol 1997 Oct;34(4 Suppl 5):25-33.
This article should be referenced as such:
Viguié F. ABCB1 (ATP-binding cassette, sub-family B (MDR/TAP), member 1) Atlas Genet Cytogenet Oncol Haematol.1998;2(2):45-46.

Gene Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 47
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
TAL1 (T-cell acute leukemia 1) Jean-Loup Huret, Marie-Claude Labastie
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France (JLH); Institut d'Embryologie Cellulaire et Moléculaire-CNRS UPR 9064, Nogent-sur-Marne, France (MCL)
Published in Atlas Database: March 1998
Online updated version: http://AtlasGeneticsOncology.org/Genes/TAL1.html DOI: 10.4267/2042/37410
This article is an update of: Huret JL, Labastie MC. TAL1 (T-cell acute leukemia 1). Atlas Genet Cytogenet Oncol Haematol.1997;1(1):3. This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: SCL (stem cell leukaemia), TCL5 (T cell leukaemia 5) Location: 1p32
DNA/RNA
DNA diagram
Description 8 exons; 16 kb; SIL (a different gene) sits 90 kb further in 5'.
Transcription (Complex) alternate splicing of: 1A with 2A, or 3 vs 1B, 2B, 3... or directly 4, 5, 6.
Protein Description 331 amino acids for the major form of 48 kDa; a truncated form of 26 kDa only in some T-ALL; domains: prolin rich in N-term; poly Gly; basic Helix-Loop-Helix from the exon 6.
Expression In hematopoietic stem cells, erythroid and megakaryocytic lineages of the adult and in the embryonic brain; indispensable for the genesis of the hematopoietic system.
Function Transcription factor; exhibits sequence-specific DNA binding activity when in dimers with another bHLH
protein such as E2A (DNA specific sequences are: CANNTG, especially: CAGATG); direct interactions of the bHLH with the LIM domain of RBTN2 or RBTN1.
Homology TAL2 in 9q32; LYL1 in 19p13; more distantly: MYC and other members of the MYC family of Helix-Loop-Helix transcription factors.
Implicated in t(1;7)(p32;q34) or t(1;14)(p32;q11)/T-ALL → TAL1/TCRB or TAL1/TCRD Disease T-cell ALL. Prognosis Is not too poor, compared to other T-ALL. T-ALL with normal karyotype, but with submicroscopic deletions of part of TAL1 in the 5' region → SIL/TAL1
Disease Found in 10 to 30% of T-ALL with a normal karyotype. Hybrid/Mutated Gene Deletions which place SIL (SCL interrupting sequence) in close 5' of TAL1; hybrid gene with exon 1 from SIL. Abnormal Protein TAL1 is under the promoter sequences controle of SIL, a gene active during T cell development.
t(1;3)(p32;p21)/T-ALL → TAL1/TCTA Disease T-cell ALL.

TAL1 (T-cell acute leukemia 1) Huret JL, Labastie MC
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 48
Breakpoints Note: mainly in 5' in a 1 kb region; but also dispersed in rare cases.
References Bash RO, Crist WM, Shuster JJ, Link MP, Amylon M, Pullen J, Carroll AJ, Buchanan GR, Smith RG, Baer R. Clinical features and outcome of T-cell acute lymphoblastic leukemia in childhood with respect to alterations at the TAL1 locus: a Pediatric Oncology Group study. Blood 1993 Apr 15;81(8):2110-7.
Wadman I, Li J, Bash RO, Forster A, Osada H, Rabbitts TH, Baer R. Specific in vivo association between the bHLH and LIM proteins implicated in human T cell leukemia. EMBO J 1994 Oct 17;13(20):4831-9.
Osada H, Grutz G, Axelson H, Forster A, Rabbitts TH. Association of erythroid transcription factors: complexes
involving the LIM protein RBTN2 and the zinc-finger protein GATA1. Proc Natl Acad Sci USA 1995 Oct 10;92(21):9585-9.
Hofmann TJ, Cole MD. The TAL1/Scl basic helix-loop-helix protein blocks myogenic differentiation and E-box dependent transactivation. Oncogene 1996 Aug 1;13(3):617-24.
Porcher C, Swat W, Rockwell K, Fujiwara Y, Alt FW, Orkin SH. The T cell leukemia oncoprotein SCL/tal-1 is essential for development of all hematopoietic lineages. Cell 1996 Jul 12;86(1):47-57.
Ono Y, Fukuhara N, Yoshie O. Transcriptional activity of TAL1 in T cell acute lymphoblastic leukemia (T-ALL) requires RBTN1 or -2 and induces TALLA1, a highly specific tumor marker of T-ALL. J Biol Chem 1997 Feb 14;272(7):4576-81.
This article should be referenced as such:
Huret JL, Labastie MC, TAL1 (T-cell acute leukemia 1). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):47-48.

Gene Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 49
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
TCL1 (T cell leukemia/lymphoma 1) Marc-Henri Stern
Unité INSERM U462, Centre Hayem, Hopital Saint Louis, 75475 Paris Cedex 10, France
Published in Atlas Database: March 1998
Online updated version: http://AtlasGeneticsOncology.org/Genes/TCL1ID66.html DOI: 10.4267/2042/37411
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Location: 14q32.1
DNA/RNA Description 4 exons; telomere - exon 1 to 4 - centromere orientation.
Transcription 1.3 kb transcripts.
Protein Description 114 amino acids; one domain with a b-barrel topology.
Expression Immature T and B lymphoid cells.
Localisation Cytoplasm.
Function Unknown.
Homology MTCP1 (38 % identity, similar tridimentional structure).
Implicated in t(14;14)(q12;q32.1) or inv(14)(q12q32.1)/T-cell malignancies → TCRA/D/TCL1 Disease Mainly T-cell prolymphocytic leukemia (T-PLL); T- cell NHL; T-cell ALL.
Cytogenetics Associated with i(8q) in T-PLL. Hybrid/Mutated Gene None. Abnormal Protein None. Oncogenesis Over expression of TCL1 is considered as critical in the oncogenetic mechanism.
t(7;14)(q35;q32.1)/T-cell malignancies → TCRB/TCL1 Disease Mainly T-cell prolymphocytic leukemia. Cytogenetics Associated with i(8q). Hybrid/Mutated Gene None. Abnormal Protein None. Oncogenesis Over expression of TCL1.
References Virgilio L, Isobe M, Narducci MG, Carotenuto P, Camerini B, Kurosawa N, Abbas-ar-Rushdi, Croce CM, Russo G. Chromosome walking on the TCL1 locus involved in T-cell neoplasia. Proc Natl Acad Sci USA 1993 Oct 15;90(20):9275-9.
Fu TB, Virgilio L, Narducci MG, Facchiano A, Russo G, Croce CM. Characterization and localization of the TCL-1 oncogene product. Cancer Res 1994 Dec 15;54(24):6297-301.
Virgilio L, Narducci MG, Isobe M, Billips LG, Cooper MD, Croce CM, Russo G. Identification of the TCL1 gene involved in T-cell malignancies. Proc Natl Acad Sci USA 1994 Dec 20;91(26):12530-4.
Narducci MG, Virgilio L, Isobe M, Stoppacciaro A, Elli R, Fiorilli M, Carbonari M, Antonelli A, Chessa L, Croce CM, et al. TCL1

TCL1 (T-cell leukemia/lymphoma 1) Stern MH
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 50
oncogene activation in preleukemic T cells from a case of ataxia-telangiectasia. Blood 1995 Sep 15;86(6):2358-64.
Thick J, Metcalfe JA, Mak YF, Beatty D, Minegishi M, Dyer MJ, Lucas G, Taylor AM. Expression of either the TCL1 oncogene, or transcripts from its homologue MTCP1/c6.1B, in leukaemic and non-leukaemic T cells from ataxia telangiectasia patients. Oncogene 1996 Jan 18;12(2):379-86.
Narducci MG, Stoppacciaro A, Imada K, Uchiyama T, Virgilio L, Lazzeri C, Croce CM, Russo G. TCL1 is overexpressed in patients affected by adult T-cell leukemias. Cancer Res 1997 Dec 15;57(24):5452-6.
Narducci MG, Virgilio L, Engiles JB, Buchberg AM, Billips L, Facchiano A, Croce CM, Russo G, Rothstein JL. The murine
Tcl1 oncogene: embryonic and lymphoid cell expression. Oncogene 1997 Aug 18;15(8):919-26.
Hoh F, Yang YS, Guignard L, Padilla A, Stern MH, Lhoste JM, van Tilbeurgh H. Crystal structure of p14TCL1, an oncogene product involved in T-cell prolymphocytic leukemia, reveals a novel beta-barrel topology. Structure 1998 Feb 15;6(2):147-55.
This article should be referenced as such:
Stern MH. TCL1 (T-cell leukemia/lymphoma 1). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):49-50.

Gene Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 51
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
TCTA (T-cell leukemia translocation-associated gene) Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France
Published in Atlas Database: March 1998
Online updated version: http://AtlasGeneticsOncology.org/Genes/TCTA.html DOI: 10.4267/2042/37412
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Location: 3p21
DNA/RNA
DNA diagram
Transcription 2.1 kb mRNA.
Protein Description 103 amino acids; 11 kDa; rich in hydrophobic amino acids (residues 41-61).
Expression Wide, especially in kidneys.
Localisation May be a membrane associated protein, as there is a hydrophobic domain.
Function Unknown.
Homology None is known.
Implicated in
t(1;3)(p32;p21)/T-cell ALL → TAL1/TCTA Disease T-cell ALL. Hybrid/Mutated Gene Head to head orientation of TAL1 and TCTA. Abnormal Protein No fusion protein, but possibly promoter exchange and gene disregulation.
To be noted Note: on day 04 Feb 1998, nothing new has appeared since the above coted paper.
References Aplan PD, Johnson BE, Russell E, Chervinsky DS, Kirsch IR. Cloning and characterization of TCTA, a gene located at the site of a t(1;3) translocation. Cancer Res 1995 May 1;55(9):1917-21.
This article should be referenced as such:
Huret JL. TCTA (T-cell leukemia translocation-associated gene). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):51.

Gene Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 52
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
ZNF198 (zinc finger protein 198) Jean-Loup Huret, Dominique Leroux
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France (JLH); Lymphoma Research Group - Groupe de Recherche sur les Lymphomes, Institut Albert Bonniot, La Tronche 38706, France (DL)
Published in Atlas Database: March 1998
Online updated version: http://AtlasGeneticsOncology.org/Genes/ZNF198ID114.html DOI: 10.4267/2042/37413
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: FIM (fused in myeloproliferative disorders) Location: 13q12 Local order: proximal from FLT1 and FLT3.
FIM (13q12) - Courtesy Mariano Rocchi, Resources for Molecular Cytogenetics. Laboratories willing to validate the probes are welcome: contact [email protected].
DNA/RNA Description 5.0 kb cDNA; coding sequence: 4.1 (formely 2.7 kb).
Transcription Main transcripts: 5.0 and 7.5 kb.
Protein Description 1379 amino acids; 4 zinc fingers in N-term, a highly hydrophobic proline repeat, and a C-term acidic domain.
Expression Wide.
Homology With DXS6673E, a gene which may be related with mental retardation.
4 zn f ingers NLSProlineZNF198
Proline: proline richNLS: Nuclear localisation signal
Implicated in
t(8;13)(p12;q12)/ANLL-NHL → 5' ZNF198 - 3' FGFR1
ZNF198/FGFR1 Ty r kinase4 zn f ingers Disease Combined myeloid malignancy and T-cell NHL. Prognosis Very poor (median survival: 12 mths). Cytogenetics Additional anomalies: +8, +der(13), +21. Hybrid/Mutated Gene 5' ZNF198 - 3' FGFR1.

ZNF198 (zinc finger protein 198) Huret JL, Leroux D
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 53
Abnormal Protein N-term zinc fingers from ZNF198 fused to the Tyrosine kinase domain of FGFR1in C-term. Oncogenesis Constitutive activation of FGFR1.
References Popovici C, Adélaïde J, Ollendorff V, Chaffanet M, Guasch G, Jacrot M, Leroux D, Birnbaum D, Pébusque MJ. Fibroblast growth factor receptor 1 is fused to FIM in stem-cell
myeloproliferative disorder with t(8;13). Proc Natl Acad Sci USA 1998 May 12;95(10):5712-7.
Xiao S, Nalabolu SR, Aster JC, Ma J, Abruzzo L, Jaffe ES, Stone R, Weissman SM, Hudson TJ, Fletcher JA. FGFR1 is fused with a novel zinc-finger gene, ZNF198, in the t(8;13) leukaemia/lymphoma syndrome. Nat Genet 1998 Jan;18(1):84-7.
This article should be referenced as such:
Huret JL, Leroux D. ZNF198 (zinc finger protein 198). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):52-53.

Leukaemia Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 54
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
t(9;12)(p24;p13) Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France
Published in Atlas Database: February 1998
Online updated version: http://AtlasGeneticsOncology.org/Anomalies/1122t0912.html DOI: 10.4267/2042/37414
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics and pathology Disease Acute leukaemias; poorly known: only 3 available cases, and with different phenotypes: a T-cell ALL, a CD10+-ALL, and a 'CML-like' disease in transformation; all 3 were male patients.
Genes involved and Proteins JAK2 Location: 9p24 DNA / RNA 24 exons. Protein Tyrosine kinase; possibly membrane associated; signal transduction.
ETV6 Location: 12p13 DNA / RNA 9 exons; alternate splicing. Protein Contains a Helix-Loop-Helix and ETS DNA binding domains; wide expression; nuclear localisation; ETS-related transcription factor.
Results of the chromosomal anomaly Hybrid gene Description 5' ETV6 - 3' JAK2.
Fusion protein Description N-term- HLH oligomerization domain from ETV6 fused to the tyrosine kinase C-term domains of JAK2 (or even starting with the JH2); the reciprocal JAK2-ETV6 may not be expressed. Oncogenesis It may be speculated that the HLH domain of ETV6 induces oligomerization, resulting in constitutive activation of the kinase domain of JAK2.
References Lacronique V, Boureux A, Valle VD, Poirel H, Quang CT, Mauchauffé M, Berthou C, Lessard M, Berger R, Ghysdael J, Bernard OA. A TEL-JAK2 fusion protein with constitutive kinase activity in human leukemia. Science 1997 Nov 14;278(5341):1309-12.
Peeters P, Raynaud SD, Cools J, Wlodarska I, Grosgeorge J, Philip P, Monpoux F, Van Rompaey L, Baens M, Van den Berghe H, Marynen P. Fusion of TEL, the ETS-variant gene 6 (ETV6), to the receptor-associated kinase JAK2 as a result of t(9;12) in a lymphoid and t(9;15;12) in a myeloid leukemia. Blood 1997 Oct 1;90(7):2535-40.
This article should be referenced as such:
Huret JL. t(9;12)(p24;p13). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):54

Leukaemia Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 55
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
del(9q) solely Franck Viguié
Laboratoire de Cytogénétique - Service d'Hématologie Biologique, Hôpital Hôtel-Dieu, 75181 Paris Cedex 04, France
Published in Atlas Database: February 1998
Online updated version: http://AtlasGeneticsOncology.org/Anomalies/del9q.html DOI: 10.4267/2042/37415
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity
del(9q) G-banding - Courtesy Diane H. Norback, Eric B. Johnson, Sara Morrison-Delap Cytogenetics at theWaisman Center (left and middle) and Jean-Luc Lai (right).
Note: del(9q) as the sole abnormality must be distinguished from syndromes where it is associated with other chromosome rearrangements; in particular, there is frequent association with LAM2 expressing t(8;21)(q22;q22), and, also, with t(15;17)(q24;q21); we herein describe del(9q) as the sole anomaly, when not otherwise specified.
Clinics and pathology Disease ANLL mainly; rarely observed in myelodysplastic syndroms (MDS) or myeloproliferative disorders; biphenotypic T-lymphoid / myeloid leukemias cases have also been described. Phenotype / cell stem origin ANLL: M1, M2, M4, M6 FAB subtypes; pluripotent stem cell probably involved; there is a trilineage myelodysplasia; six patients (4 M1, 1 M2 and 1 T- ALL) from two reports have been described with
del(9q) and CD34+, CD7+, T lymphoid / myeloid biphenotypic leukemia. Epidemiology 0 to 3% of ANLL cases, depending on series; both sexes equally represented; adults and children may be affected. Cytology Frequent sideroblasts; leukemic blasts are agranular, with large vacuoles on Giemsa staining and localized positivity for myeloperoxydase (MPO); giant MPO positive granules are described, corresponding to =AB pseudo-Chediak-Higashi =BB granules; most blast cells are CD34 positive. Prognosis When del(9q) is the unique chromosome abnormality the prognosis, depending on AML subtype, is variable; (del(9q) as a secondary anomaly in t(8;21) has no prognostic consequence for some workers and is a factor of worse prognosis for others).

del(9q) solely Viguié F
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 56
Cytogenetics Cytogenetics, morphological Interstitial deletion of chromosome 9 long arm, called del(9q) or 9q-, involving a variable chromosome segment; the region 9q21-22 seems constantly involved.
Cytogenetics, molecular This constantly deleted region has not yet been more precisely defined and it is not known whether deletion of one or more critical gene(s) are involved. Thus there are presently no 9q molecular probes availaible to assess 9q deletion.
Probes Whole chromosome 9 painting, to exclude 9q translocations.
Additional anomalies On 31 reviewed cases of ANLL with del(9q) as a primary change, none had additional anomalies del(9q) as a secondary anomaly: - Association with t(8;21) represents the majority of cases; t(8;21) occurs in 5 to 10 % of patients with ANLL, and its association with del(9q) is the second more frequent, after the association with loss of one sex chromosome; it represents approximatly 10-15 % of cases. - Association with t(15;17), in promyelocytic leukaemia, has also seldom (1%) been observed. - In these two syndromes, del(9q) is usually not present at diagnosis but appears as an additional change at relapse. - del(9q) has never been described in association with other recurrent primary changes. Variants Unbalanced translocations involving 9q may, in a way, be considered as del(9q) variants.
Genes involved and Proteins Note: genes involved are unknown; there is probable deletion of one or several tumor suppressor gene(s) involved in the progression of the disease.
References Hossfeld DK, Higi M, Köhler S, Miller A, Zschaber R. A subtype of the prototypic karyotype in acute myeloid leukemia t (8; 21)(q22; q22), del 9 (q13; q23). Blut 1980 Jan;40(1):27-32.
Mecucci C, Vermaelen K, Kulling G, Michaux JL, Noens L, Van Hove W, Tricot G, Louwagie A, Van den Berghe H. Interstitial 9q- deletions in hematologic malignancies. Cancer Genet Cytogenet 1984 Aug;12(4):309-19.
Kao YS, Sartin BW, Van Brunt J, Hew AY Jr. Interstitial 9q deletion (q12q22) in two cases of acute myeloblastic leukemia. Cancer Genet Cytogenet 1986 Jan 15;19(3-4):365-6.
Hoyle C, Sherrington PD, Hayhoe FG. Cytological features of 9q- deletions in AML. Br J Haematol 1987 Jun;66(2):277-8.
Kerndrup G, Pedersen B, Bendix-Hansen K. Specific minor chromosome deletions in myelodysplastic syndromes: clinical and morphologic correlations. Cancer Genet Cytogenet 1987 Jun;26(2):227-34.
Smadja N, Krulik M, de Gramont A, Gonzalez G, Debray CJ. A new case of de novo AML with 9q interstitial deletion as the sole chromosomal abnormality. Br J Haematol 1987 Dec;67(4):494-5.
Minamihisamatsu M, Gregorio JS, Onozawa Y, Ishihara T. Acute nonlymphocytic leukemia following lung cancer in a patient with a constitutional supernumerary chromosome. Cancer Genet Cytogenet 1988 Oct 15;35(2):263-8.
Ringressi A, Mecucci C, Grossi A, Bernabei PA, Ferrini PR, Van den Berghe H. 6p+ and 9q- in two chromosomally distinct clones occurring in a case of myelodysplastic syndrome evolving to acute nonlymphocytic leukemia. Cancer Genet Cytogenet 1988 Oct 15;35(2):213-21. (Review).
Sreekantaiah C, Baer MR, Preisler HD, Sandberg AA. Involvement of bands 9q21-q22 in five cases of acute nonlymphocytic leukemia. Cancer Genet Cytogenet 1989 May;39(1):55-64.
Akashi K, Shibuya T, Harada M, Oogami A, Teshima T, Takamatsu Y, Kikuchi M, Niho Y. Interstitial 9q deletion in T-lymphoid/myeloid biphenotypic leukaemia. Br J Haematol 1992 Feb;80(2):172-7.
Kwong YL, Chan TK, Chan LC. Interstitial deletion of the long arm of chromosome 9 as the sole anomaly in acute myeloid leukaemia is associated with dyserythropoiesis. Leukemia 1992 Jan;6(1):64-5.
Kwong YL, Ha SY, Liang RH, Wan TS, Chan LC. Interstitial deletion of 9q in a case of acute myeloid leukemia. Cancer Genet Cytogenet 1993 Mar;66(1):79-80.
Johansson B, Mertens F, Mitelman F. Secondary chromosomal abnormalities in acute leukemias. Leukemia 1994 Jun;8(6):953-62.
Lunde JH, Allen EF. Interstitial 9q- deletion in a case of acute myeloid leukemia-M2 arising from a granulocytic sarcoma. Cancer Genet Cytogenet 1994 Dec;78(2):239-41.
Kwong YL. Interstitial 9q- and dyserythropoiesis in acute myeloid leukemia. Am J Hematol 1995 Jan;48(1):63-4.
Ferrara F, Scognamiglio M, Di Noto R, Schiavone EM, Poggi V, Fiorillo A, Libertini R, Vicari L, Del Vecchio L, Sebastio L. Interstitial 9q deletion is associated with CD7+ acute leukemia of myeloid and T lymphoid lineage. Leukemia 1996 Dec;10(12):1990-2.
Schoch C, Haase D, Haferlach T, Gudat H, Buchner T, Freund M, Link H, Lengfelder E, Wandt H, Sauerland MC, Löffler H, Fonatsch C. Fifty-one patients with acute myeloid leukemia and translocation t(8;21)(q22;q22): an additional deletion in 9q is an adverse prognostic factor. Leukemia 1996 Aug;10(8):1288-95.
This article should be referenced as such:
Viguié F. del(9q) solely. Atlas Genet Cytogenet Oncol Haematol.1998;2(2):55-56.

Leukaemia Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 57
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Essential thrombocythemia Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France
Published in Atlas Database: February 1998
Online updated version: http://AtlasGeneticsOncology.org/Anomalies/ET.html DOI: 10.4267/2042/37416
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics and pathology Disease Chronic myeloproliferative syndrome. Phenotype / cell stem origin Pluripotent stem cell is involved. Epidemiology Annual incidence is less than 1/106; sex ratio 1M/; median age 50-60 years. Clinics Often revealed by haemorrhages or thrombosis; splenomegaly is found in 50% of cases; blood data: the disease is defined by a thrombocytosis > 600 X 109L; the platelet count is actually often > 1000 X 109L. Prognosis Evolution: chronic disease; can evolve towards polycytemia vera or myelofibrosis, seldom towards ANLL; prognosis: often fair, is variable according to age and depends on haemorrhages, thromboses, and embolisms, which are the major causes of death in this disease.
Cytogenetics Cytogenetics, morphological A normal karyotype is found in 95% of cases; +9 is the only anomaly having been described in as far as 4 cases!
Genes involved and Proteins Note: genes involved are unkown.
References [No authors listed]. Report on essential thrombocythemia. Cancer Genet Cytogenet 1981 Oct;4(2):138-42.
Cournoyer D, Noël P, Schmidt MA, Dewald GW. Trisomy 9 in hematologic disorders: possible association with primary thrombocytosis. Cancer Genet Cytogenet 1987 Jul;27(1):73-8.
Mertens F, Johansson B, Heim S, Kristoffersson U, Mitelman F. Karyotypic patterns in chronic myeloproliferative disorders: report on 74 cases and review of the literature. Leukemia 1991 Mar;5(3):214-20. (Review).
This article should be referenced as such:
Huret JL Essential thrombocythemia. Atlas Genet Cytogenet Oncol Haematol.1998;2(2):57.

Leukaemia Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 58
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Acute basophilic leukemia t(X;6)(p11;q23) Nicole Dastugue
Génétique des Hémopathies, Laboratoire d'Hématologie, Hôpital Purpan, 31000, Toulouse Cedex, France
Published in Atlas Database: February 1998
Online updated version: http://AtlasGeneticsOncology.org/Anomalies/LAbaso1124.html DOI: 10.4267/2042/37417
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics and pathology Disease Rare type of acute myeloid leukemia. Phenotype / cell stem origin Basophilic precursor. Epidemiology Very rare but might be prominent in infants. Clinics Hyperhistaminemia syndrome has been reported in some of the cases. Cytology Major component of undifferentiated blasts + minor component of basophilic blasts (blasts containing large granules reacting positively to toluidine blue staining). Treatment ANLL protocols. Prognosis Good response to standard therapy for chilhood ANLL.
Cytogenetics Cytogenetics, morphological t(X;6)(p11;q23)
Cytogenetics, molecular Not done.
Genes involved and Proteins Note: are unknown.
References Dastugue N, Duchayne E, Kuhlein E, Rubie H, Demur C, Aurich J, Robert A, Sie P. Acute basophilic leukaemia and translocation t(X;6)(p11;q23). Br J Haematol 1997 Jul;98(1):170-6.
This article should be referenced as such:
Dastugue N. Acute basophilic leukemia. t(X;6)(p11;q23). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):58.

Leukaemia Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 59
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
t(5;14)(q33;q32) PDGFRB/TRIP11 Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France
Published in Atlas Database: February 1998
Online updated version: http://AtlasGeneticsOncology.org/Anomalies/t0514ANL.html DOI: 10.4267/2042/37418
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics and pathology Disease Yet poorly known: 1 case of ANLL. Clinics Found at relapse with eosinophilia of a M2 ANLL with t(7;11).
Cytogenetics Cytogenetics, morphological So far found as an additional anomaly in a clone bearing a t(7;11)(p15;p15).
Genes involved and Proteins PDGFRB Location: 5q33 Protein PDGFRB is the receptor for PDGFB (platelet-derived growth factor-b); membrane protein; belongs to the immunoglobulin superfamily.
CEV14 Location: 14q32 Protein Contains a N-term leucine zipper and a C-term putative thyroid hormone receptor interacting domain.
Results of the chromosomal anomaly Hybrid gene Description 5' CEV14 - 3' PDGFRb
Transcript 10 kb fusion transcript (major) and other (minor) transcripts.
Fusion protein Description N-term leucine zipper from CEV14 fused to the transmembrane domain and the Tyr kinase domain of PDGFRb in C-term; the reciprocal transcript is not expressed; breakpoints at amino acids 1936 of PDGFRb and 567 of CEV14. Oncogenesis Ectopic constitutive tyrosine kinase activation of PDGFRb may occur.
To be noted The above t(5;14)(q33;q32) with PDGFRb and CEV14 rearrangements must not be confused with the t(5;14)(q31;q32) with IL3 and IgH involvements found in ALL.
References Abe A, Tanimoto M, Towatari M, Matsuoka A, Kitaori K, Kato H, Toyozumi H, Takeo T, Adachi K, Emi N, et al. Acute myeloblastic leukemia (M2) with translocation (7;11) followed by marked eosinophilia and additional abnormalities of chromosome 5. Cancer Genet Cytogenet 1995 Aug;83(1):37-41.
Abe A, Emi N, Tanimoto M, Terasaki H, Marunouchi T, Saito H. Fusion of the platelet-derived growth factor receptor beta toa novel gene CEV14 in acute myelogenous leukemia after clonal evolution. Blood 1997 Dec 1;90(11):4271-7.
This article should be referenced as such:
Huret JL. t(5;14)(q33;q32) PDGFRB/TRIP11. Atlas Genet Cytogenet Oncol Haematol.1998;2(2):59.

Leukaemia Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 60
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
t(11;16)(q23;p13) Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France
Published in Atlas Database: February 1998
Online updated version: http://AtlasGeneticsOncology.org/Anomalies/t1116q23p13ID1120.html DOI: 10.4267/2042/37419
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics and pathology Disease ANLL/MDS: only treatment related leukaemias cases so far (in other 11q23 translocations, most cases occur in de novo acute leukaemia). Phenotype / cell stem origin M4, M2 ANLL; CMML and RAEBT, although MDS is otherwise rarely seen in 11q23 translocations; the fusion gene is found in all the mature monocytes, in some of the granulocytes and erythroblasts, not in the lymphocytes. Epidemiology 13 available cases; most cases are children cases: median age is 10-14 yrs, range is 2-74 yrs; sex ratio is balanced. Clinics Secondary to antitopoisomerase II drugs (etoposide or teniposide, but also doxorubicin); this secondary malignancy occurs within 6-60 mths (median 20 mths); the primary malignancy was a t(8;21)(q22;q22)/M2-ANLL in 2 cases. Prognosis Yet unknown.
Cytogenetics Additional anomalies Are found in 8 of 11 cases; variable, except the unexpectected recurrence of 1p36.1 involvement.
Genes involved and Proteins MLL Location: 11q23
DNA / RNA 21 exons, spanning over 100 kb; 13-15 kb mRNA. Protein 431 kDa; contains two DNA binding motifs (a AT hook, and Zinc fingers), a DNA methyl transferase motif, a bromodomain; transcriptional regulatory factor; nuclear localisation.
CBP Location: 16p13 Protein Nuclear localisation; transcriptional adaptor/coactivator: binds CREB; has histone acetyltransferase activity.
Results of the chromosomal anomaly Hybrid gene Description 5' MLL - 3' CBP
Fusion protein Description N-term AT hook and DNA methyltransferase from MLL fused to most of CBP starting with the bromodomain of CBP -or even more in N-term with the CREB binding domain- and also comprising the cystein/histidine rich and the glutamine rich domains of CBP in C-term around 1400 amino acids from MLL; the reciprocal CBP-MLL may or may not be expressed. Oncogenesis May promote histone acetylation of genomic regions targeted by the MLL AT-hooks; may loose CBP cell cycle inhibition capability.

t(11;16)(q23;p13) Huret JL
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 61
References Satake N, Ishida Y, Otoh Y, Hinohara S, Kobayashi H, Sakashita A, Maseki N, Kaneko Y. Novel MLL-CBP fusion transcript in therapy-related chronic myelomonocytic leukemia with a t(11;16)(q23;p13) chromosome translocation. Genes Chromosomes Cancer 1997 Sep;20(1):60-3.
Taki T, Sako M, Tsuchida M, Hayashi Y. The t(11;16)(q23;p13) The t(11;16)(q23;p13) translocation in myelodysplastic syndrome fuses the MLL gene to the CBP gene.. Blood 1997 Jun 1;89(11):3945-50.
Rowley JD, Reshmi S, Sobulo O, Musvee T, Anastasi J, Raimondi S, Schneider NR, Barredo JC, Cantu ES, Schlegelberger B, Behm F, Doggett NA, Borrow J, Zeleznik-Le N. All patients with the T(11;16)(q23;p13.3) that involves MLL
and CBP have treatment-related hematologic disorders. Blood 1997 Jul 15;90(2):535-41.
Sobulo OM, Borrow J, Tomek R, Reshmi S, Harden A, Schlegelberger B, Housman D, Doggett NA, Rowley JD, Zeleznik-Le NJ. MLL is fused to CBP, a histone acetyltransferase, in therapy-related acute myeloid leukemia with a t(11;16)(q23;p13.3). Proc Natl Acad Sci USA 1997 Aug 5;94(16):8732-7.
This article should be referenced as such:
Huret JL. t(11;16)(q23;p13). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):60-61.

Leukaemia Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 62
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
t(16;21)(p11;q22) Christine Pérot
Laboratoire de Cytogenetique, Hopital Saint-Antoine, Paris, France
Published in Atlas Database: February 1998
Online updated version: http://AtlasGeneticsOncology.org/Anomalies/t1621.html DOI: 10.4267/2042/37420
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Clinics and pathology Disease De novo ANLL; (one case of blast crisis CML). Phenotype / cell stem origin Mainly M2 or M4, but also M1, M5a, M5b, or M7 ANLL; may be preceded by MDS. Epidemiology About 30 reported cases, mainly found in young adults; children cases are described; median age is about 30 yrs; balanced sex ratio. Clinics Blood data: anemia, thrombocytopenia, mild hyperleucocytosis; with high monocytic cell count at times. Cytology Myelocytic and monocytoid features are often present; eosinophils in the bone marrow are sometimes abnormal and/or elevated; erythrophagocytosis may be found. Prognosis Seems poor: complete remission may not be achieved; there is high incidence of relapse within a year and a median of survival is about 22 months (cases herein reviewed).
Cytogenetics Additional anomalies Rarely found solely; most often associated with various numerical or structural abnormalities; trisomy 10 was found in 4 of 17 cases.
Genes involved and Proteins FUS Location: 16p11
ERG Location: 21q22
Results of the chromosomal anomaly Hybrid gene Description 5' FUS - 3' ERG
Fusion protein Description N-term FUS RNA binding domain fused to the C-term DNA binding ETS domain of ERG. Oncogenesis Seems to act as a transcriptional activator.
References Mecucci C, Bosly A, Michaux JL, Broeckaert-Van Orshoven A, Van den Berghe H. Acute nonlymphoblastic leukemia with bone marrow eosinophilia and structural anomaly of chromosome 16. Cancer Genet Cytogenet 1985;17:359-63.
Morgan R, Riske CB, Meloni A, Ries CA, Johnson CH, Lemons RS, Sandberg AA. t(16;21)(p11.2;q22): a recurrent primary rearrangement in ANLL. Cancer Genet Cytogenet 1991;53:83-90.
Hiyoshi M, Koh KR, Yamane T, Tatsumi N. Acute non-lymphoblastic leukaemia with t(16;21): case report with a review of the literature. Clin Lab Haematol 1995;17:243-6.
Kong XT, Ida K, Ichikawa H, Shimizu K, Ohki M, Maseki N, Kaneko Y, Sako M, Kobayashi Y, Tojou A, Miura I, Kakuda H, Funabiki T, Horibe K, Hamaguchi H, Akiyama Y, Bessho F, Yanagisawa M, Hayashi Y. Consistent detection of TLS/FUS-ERG chimeric transcripts in acute myeloid leukemia with t(16;21)(p11;q22) and identification of a novel transcript. Blood 1997;90:1192-9.
This article should be referenced as such:
Pérot C. t(16;21)(p11;q22). Atlas Genet Cytogenet Oncol Haematol.1998;2(2):62.

Solid Tumour Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 63
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Nervous system: Peripheral neuroblastic tumours (Neuroblastoma, Ganglioneuroblastoma, Ganglioneuroma) Jérôme Couturier, Daniel Satgé
Department of Pathology, Institut Curie, Paris, France
Published in Atlas Database: February 1998
Online updated version is available from: http://AtlasGeneticsOncology.org/Tumors/neurob5002.html DOI: 10.4267/2042/37421
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Note: belongs to the group of 'small blue round cell' tumours of the children, and differential diagnosis with primitive neurectodermal tumours (PNET), lymphoma, Ewing's tumour, and rhabdomyosarcoma may be difficult.
Clinics and pathology Disease Tumour of the sympathetic nervous system: medulloadrenal gland (50%), abdominal (25%), thoracic (15%), cervical or pelvic paraspinal ganglia; metastatic at diagnosis in 60% of cases (lymph nodes, bones and bone marrow, liver, skin). Embryonic origin Neural crest cells. Etiology Unknown; possible excess in neurofibromatosis type I, Wiedemann-Beckwith syndrome, and maternal exposure to phenyl hydantoin; exceptional familial cases. Epidemiology Incidence is 5-10 per million children per yr; 10% of cancers in childhood; half cases by the age of 2 yrs, 90% before 6 yrs. Clinics Presenting signs are according to the localization of the tumoural mass; high catecholamin excretion. Pathology Tumours may exhibit various degrees of differentiation:
1- Neuroblastoma: undifferentiated cells that may be arranged in rosettes surrounding a fibrillar centre; 2- Ganglioneuroblastoma: presenting with more fibrillar material and a mixture of the above described with >50% of more mature cells; 3- Ganglioneuroma composed of well differentiated ganglion cells and Schwann cells; a given tumour may contain more and less mature cell areas. Staging (Evans): Stage I: confined to the organ or structure of origin, Stage II: extending beyond the organ, but not crossing the midline (e.g. homolateral lymph nodes may be involved), Stage III: extending and crossing the midline, Stage IV: distant metastases, Stage IVs: stage I or II otherwise in children aged < 1 yr, with metastases in: liver, skin, bone marrow, but not in the bones. Treatment Surgery and/or radiation therapy, and/or chemotherapy. Evolution Spontaneous (and treatment induced) regression or differenciation into benign cells (ganglioneuroma) occurs rarely in tumours (mainly in infant cases). Prognosis Prognosis is very poor in most cases (median survival 1 yr); good outcome (90%) only for patients with lymph nodes negative for tumour (POG stage A); younger patients have better outcome than older patients; cytogenetic and genetic anomalies are of important prognostic value (see below).

Nervous system: Peripheral neuroblastic tumours (Neuroblastoma, Ganglioneuroblastoma, Ganglioneuroma) Couturier J, Satgé D
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 64
Genetics Note: heterogenous disease from the genetic viewpoint; 90% cases exhibit genetic abnormalities.
Cytogenetics Morphological cytogenetics Two types can be delineated according to ploidy: - Aneuploid tumours (near triploid, pentaploid or hexaploid), with whole chromosome anomalies, often with relative gains of chromosomes 17, 7, 6, relative losses of chromosomes 11, 14, X (molecular cytogenetics: detection with comparative genomic hybridization (CGH)); these are low grade tumours, with good prognosis. - Diploid and/or tetraploid tumours, with del(1p) -minimal critical region being 1p36- in 40% cases, del(11q), partial trisomy for 17q21-qter (in 90% of high grade tumours), DM or HSR (N-myc amplification); these anomalies are often associated, found in high grade tumours, and bear a grave prognosis.
Genes involved and Proteins MYCN Location: 2p24 Protein Nuclear protein; contains a helix-loop-helix and a leucine zipper; transcription factor.
Result of the chromosomal anomaly Fusion protein Oncogenesis Amplification of NMYC is found in various tumours, in particular neuroblastoma; the level of amplification increases with tumour progression.
To be noted Screening programs in several countries could not induce a fall in mortality
References Evans AE, D'Angio GJ, Randolph J. A proposed staging for children with neuroblastoma. Children's cancer study group A. Cancer 1971 Feb;27(2):374-8.
Shimada H, Chatten J, Newton WA Jr, Sachs N, Hamoudi AB, Chiba T, Marsden HB, Misugi K. Histopathologic prognostic factors in neuroblastic tumors: definition of subtypes of ganglioneuroblastoma and an age-linked classification of neuroblastomas. J Natl Cancer Inst 1984 Aug;73(2):405-16.
Triche TJ. Neuroblastoma and other childhood neural tumors: a review. Pediatr Pathol 1990;10(1-2):175-93. (Review).
Look AT, Hayes FA, Shuster JJ, Douglass EC, Castleberry RP, Bowman LC, Smith EI, Brodeur GM. Clinical relevance of tumor cell ploidy and N-myc gene amplification i childhood neuroblastoma: a Pediatric Oncology Group study. J Clin Oncol 1991 Apr;9(4):581-91.
Brodeur GM, Nakagawara A. Molecular basis of clinical heterogeneity in neuroblastoma. Am J Pediatr Hematol Oncol 1992 May;14(2):111-6. (Review).
Carlsen NL. Neuroblastoma: epidemiology and pattern of regression. Problems in interpreting results of mass screening. Am J Pediatr Hematol Oncol 1992 May;14(2):103-10. (Review).
Caron H, van Sluis P, van Hoeve M, de Kraker J, Bras J, Slater R, Mannens M, Voûte PA, Westerveld A, Versteeg R. Allelic loss of chromosome 1p36 in neuroblastoma is of preferential maternal origin and correlates with N-myc amplification. Nat Genet 1993 Jun;4(2):187-90.
Craft AW, Parker L. Screening for neuroblastoma: 20 years and still no answer. Eur J Cancer 1996 Aug;32A(9):1540-3. (Review).
Meddeb M, Danglot G, Chudoba I, Venuat AM, Benard J, Avet-Loiseau H, Vasseur B, Le Paslier D, Terrier-Lacombe MJ, Hartmann O, Bernheim A. Additional copies of a 25 Mb chromosomal region originating from 17q23.1-17qter are present in 90% of high-grade neuroblastomas. Genes Chromosomes Cancer 1996 Nov;17(3):156-65.
Plantaz D, Mohapatra G, Matthay KK, Pellarin M, Seeger RC, Feuerstein BG. Gain of chromosome 17 is the most frequent abnormality detected in neuroblastoma by comparative genomic hybridization. Am J Pathol 1997 Jan;150(1):81-9.
This article should be referenced as such:
Couturier J, Satgé DNervous system: Peripheral neuroblastic tumours (Neuroblastoma, Ganglioneuroblastoma, Ganglioneuroma) Atlas Genet Cytogenet Oncol Haematol.1998;2(2):63-64.

Cancer Prone Disease Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 65
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Bloom syndrome Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France
Published in Atlas Database: February 1998
Online updated version is available from: http://AtlasGeneticsOncology.org/Kprones/BLO10002.html DOI: 10.4267/2042/37422
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Inheritance: autosomal recessive; frequency is about 2/105 newborns in Ashkenazi Jews and in the Japanese (founder effect: affected persons descent from a common ancestor); much rarer otherwise.
Clinics Note: 168 cases have been registered in the Bloom's syndrome Registry by James German; BS patients are predisposed to all types of cancer observed in the general population; thus, BS is a model of initiation and promotion of cancer, and highligths internal causes/processes of cancers.
Phenotype and clinics - Phenotypic spectrum variable. - Growth: dwarfism: intrauterine growth retardation; birth weight: below 2.3 kg; mean length: 44 cm; adult length < 145 cm; - Skin: hyperpigmented (café au lait) spots; hypopigmented areas; sun sensitive telangiectatic erythema; in butterfly configuration across the face: resembles lupus erythematosus; - Head: microcephaly; dolichocephaly; narrow face; prominent nose and/or ears; characteristic high-pitched voice; - Normal intelligence; - Immune deficiency → frequent infections (may be life-threatening); - Other: myocardopathy; hypogonadism in male patients; hypertriglyceridemia.
Neoplastic risk Nearly half of patients have had at least one cancer (10% of whom having had more than one primary cancer, which is quite characteristic of Bloom's); mean age at first cancer onset: 25 yrs (range: 2-49 yrs).
- Acute leukaemias (ALL and ANLL) in 15 % of cases; lymphomas in 15 % as well; these occur mainly before the thirties. - Carcinomas (of a wide variety) occur in 30 % of cases, mainly after the age of 20 yrs. - Benign tumours (10%).
Evolution Major medical complications apart from cancers are: chronic lung disease, and diabetes mellitus (in 10 %).
Prognosis 1/3 of patients are dead at mean age 24 yrs (oldest died at 49 yrs, youngest died before 1 yr) and the mean age of the 2/3 remaining alive patients is 22 yrs (range: 4-46 yrs).
Cytogenetics Inborn condition - Chromatid/chromosome breaks; triradial and quadriradial figures, in particular symetrical quadriradial configuration involving homologous chromosomes (Class I qr), which are pathognomonic and which may be due to a mitotic crossing-over; found in 3-4% of metaphases (normal: 1/105). - Diagnosis is on the (pathognomonic) highly elevated spontaneous sister chromatid exchange rate (90 SCE per cell; more than 10 times what is normally found, which is about 8-10 SCE per cell with BrDU; spontaneous SCE rate (without DNA damaging agent) in the normal population being about 1 per cell); in some persons a minor population of low SCE cells exists, suggesting a recombination event between maternal and paternal alleles (with different mutations), giving rise to a wild type functional gene (called somatic reversion); this allowed to localize the gene in a very elegant strategy. - Heterozygotes are not detectable by cytogenetic studies.

Bloom syndrome Huret JL
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 66
Other findings Note: slowing of the cell cycle (lenthening of the G1 and S phases); DNA ligase I deficiency (delayed junction of Okazaki fragments).
Genes involved and Proteins BLM Location: 15q26.1 Protein Description: ATP binding, DEAH box, and two putative nuclear localization signals. Localisation: nuclear. Function: DNA helicase; probable role in DNA replication and repair. Homology with the RecQ helicases. Mutations Germinal: the mutated BLM protein is retained in the cytoplasm or both in the cytoplasm and the nucleus, while the normal protein is nuclear.
Somatic: random somatic mutations in random DNA segments appear to randomly cause tumour initiation and/or progression: every cancer type is over-represented in this syndrome, and at a much earlier age than normal.
References German J. Bloom's syndrome. I. Genetical and clinical observations in the first twenty seven patients. Am J Hum Genet 1969;2:196-227.
Gorlin RJ, Cohen MM, Levin LS. Syndromes of the head and neck. Oxford Monogr Med Genet 1990;19:297-300.
Ellis NA and German J. Molecular genetics of Bloom's syndrome. Hum Mol Genet 1996;5 Spec No:1457-63. (Review).
German J. Bloom's syndrome. XX. The first 100 cancers. Cancer Genet Cytogenet 1997;93:100-6. (Review).
This article should be referenced as such:
Huret JL. Bloom syndrome. Atlas Genet Cytogenet Oncol Haematol.1998;2(2):65-66.

Cancer Prone Disease Section Short Communication
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 67
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Dubowitz syndrome Jean-Loup Huret, Claude Léonard
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France (JLH); Cytogénétique Laboratoire d'Anatomo Pathologie, CHU Bicêtre, 78 r Leclerc, F94270 Le Kremlin-Bicêtre, France (CL)
Published in Atlas Database: February 1998
Online updated version is available from: http://AtlasGeneticsOncology.org/Kprones/DUB10016.html DOI: 10.4267/2042/37423
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Note: Dubowitz syndrome may be confused with Bloom syndrome; another differential diagnosis is fetal alcohol syndrome. Inheritance: autosomal recessive; heterogeneity cannot be excluded; less than 150 cases described.
Clinics Phenotype and clinics - Phenotypic spectrum variable. - Growth: from normal to severe retardation; intrauterine growth retardation is frequent; birth weight: 2.3 kg; length: 45 cm; cranial perimeter: 30 cm; delayed bone age. - Head: microcephaly; high forehead; sparse hair; broad nose; epicanthus; hypertelorism; blepharophimosis; microretrognathia. - Skin: eczema, a classical sign, may be absent. - Congenital heart defects in 10%; other malformations: ocular, dental, skeletal, urogenital in male patients; frequent infections. - Mental retardation in 30-70 % of cases (from normal in 30% to severe retardation in 10%); siezures in 10%
high-pitched voice; behaviour problems in 40%; most patients are 'hyperactive, shy, like music'.
Neoplastic risk Haematological malignancies and pancytopenia in 10%, childhood myelodysplasia in particular; lymphomas.
Cytogenetics Inborn condition Appears to be normal or near to normal in most cases, although an increased rate of chromosomal breakage has also been described.
References Gorlin RJ, Cohen MM, Levin LS. Syndromes of the head and neck. Oxford Monogr Med Genet 1990;19:304-6.
Tsukahara M, Opitz JM. Dubowitz syndrome: review of 141 cases including 36 previously unreported patients. Am J Med Genet 1996 May 3;63(1):277-89.
This article should be referenced as such:
Huret JL, Léonard C. Dubowitz syndrome. Atlas Genet Cytogenet Oncol Haematol.1998;2(2):67.

Cancer Prone Disease Section Mini Review
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 68
Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Fanconi anaemia Jean-Loup Huret
Genetics, Dept Medical Information, University of Poitiers, CHU Poitiers Hospital, F-86021 Poitiers, France
Published in Atlas Database: February 1998
Online updated version is available from: http://AtlasGeneticsOncology.org/Kprones/FA10001.html DOI: 10.4267/2042/37424
This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 1998 Atlas of Genetics and Cytogenetics in Oncology and Haematology
Identity Other names: Fanconi pancytopenia Inheritance: autosomal recessive; frequency is about 2.5/105 newborns.
Clinics Note: Fanconi anaemia is a chromosome instability syndrome with progressive bone marrow failure and an increased risk of cancers.
Phenotype and clinics - Growth retardation (70% of cases). - Skin abnormalities: hyperpigmentation and/or café au lait spots in 80%. - Squeletal malformations (60%), particularly radius axis defects (absent or hypoplastic thumb or radius...). - No immune deficiency (in contrast with most other chromosome instability syndromes). - Progressive bone marrow failure; mean age of onset of anemia: 8 yrs; diagnosis made before onset of haematologic manifestations in only 30%. - Other: renal anomalies, hypogonadism, mental impairment, heart defects, and perhaps diabetes mellitus, also occur in 10 to 30% of cases.
Neoplastic risk - Myelodysplasia (MDS) and acute non lyphocytic leukaemia (ANLL): 10% of cases; i.e. a 15000 fold increased risk of MDS and ANLL has been evaluated in FA, and it has been assumed that 'it is reasonable to regard the Fanconi anemia genotype as 'preleukaemia''; mean age at diagnosis: 15 yrs. - Hepatocarcinoma (androgen-therapy induced) in 10%; mean age at diagnosis: 16 yrs. - Other cancers in 2-5%: in particular squamous cell carcinoma.
Treatment Androgens and steroids to improve haematopoietic functions; bone marrow transplantation prevents from terminal pancytopenia, and from ANLL as well.
Prognosis Mean age at death: 16 years; most patients die from marrow aplasia (haemorrhage, sepsis), and others from malignancies; MDS and ANLL in FA bear a very poor prognosis (median survival of about 6 mths); survival is also poor in the case of a squamous cell carcinoma.
Cytogenetics Inborn condition - Spontaneous chromatid/chromosome breaks, triradials, quadriradials. - Hypersensitivity to the clastogenic effect of DNA cross-linking agents (increased rate of breaks and radial figures); diepoxybutane, mitomycin C, or mechlorethamine hydrochlorid are used for diagnosis.
Cancer cytogenetics - Various clonal anomalies are found in MDS or ANLL in Fanconi anaemia patients, such as the classical -5/del(5q), and -7/del(7q), found in 10 % of cases; telomeres appear to be non randomly involved in FA's clonal anomalies.
Other findings Note: - Slowing of the cell cycle (G2/M transition, with accumulating of cells in G2). - Impaired oxygen metabolism. - Defective P53 induction.

Fanconi anaemia Huret JL
Atlas Genet Cytogenet Oncol Haematol. 1998;2(2) 69
Genes involved and Proteins Complementation groups: 4 well known complementation groups: group A (gene FA1 in 16q24, perhaps another gene 20q13), group B, group C (gene FACC in 9q22), group D (gene FAD in 3p24 has sometimes been located in 11q23); a fifth group, group E, may, per se, be heterogenous; however, the different complementation groups display similar phenotypes, and genes may therefore be functionally related (recently was found that FA1 and FACC form heterodimers).
FA1 Location: 16q24 Protein Expression: wide. Localisation: mostly cytoplasmic. Function: binds to the protein encoded by FACC (see below), the dimer being found in the cytoplasm and the nucleus. Homology: no known homology. Mutations Germinal: various nucleotide substitutions, deletions, or insertions.
FACC Location: in 9q22 Protein Expression: wide. Localisation: cytoplasmic when unbound. Function: peak expression during the G2/M transition; binds to cdc2 (mitotic cyclin-dependent kinase); probably involved in basic aspect(s) of the cell protection against DNA damages: role in the cell cycle regulation and/or in DNA repair and/or in the prevention of cellular apoptosis; binds to FAA, the protein encoded by FA1 (see above), the dimer being found in the cytoplasm and the nucleus. Homology: no known homology. Mutations Germinal: nucleotide substitutions.
FAD Location: 3p24
To be noted Clinical diagnosis may, in certain cases, be very difficult; cytogenetic ascertainment is then particularly useful; however, cytogenetic diagnosis may also, at times, be very uncertain; this is a great problem when bone marrow engraftment has been decided in a
pancytopenic patient: if this patient has FA, bone marrow conditioning must be very mild, as FA cells are very clastogen sensitive. FA patients (i.e. patients with defective alleles) may have, in a percentage of cells, a somatic reversion (by revert mutation towards wild-type gene); such a phenomenon is also known in Bloom syndrome, another chromosome instability syndrome.
References Glanz A, Fraser FC. Spectrum of anomalies in Fanconi anaemia. J Med Genet 1982;19(6):412-6.
Alter BP, Potter NU. Chromosome Mutation and neoplasia. J German Ed. AR Liss 1983; pp 43.
Huret JL, Tanzer J, Guilhot F, Frocrain-Herchkovitch C, Savage JR. Karyotype evolution in the bone marrow of a patient with Fanconi anemia: breakpoints in clonal anomalies of this disease. Cytogenet Cell Genet 1988;48(4):224-7.
TM Schroeder-Kurth, AD Auerbach, G Obe. Fanconi anemia. Clinical, cytogenetic and experimental aspects. Eds. Springer-Verlag 1989.
Auerbach AD, Allen RG. Leukemia and preleukemia in Fanconi anemia patients. A review of the literature and repAuerbach AD, Allen RGort of the International Fanconi Anemia Registry. Cancer Genet Cytogenet 1991;51(1):1-12.
Strathdee CA, Duncan AM, Buchwald M. Evidence for at least four Fanconi anaemia genes including FACC on chromosome 9. Nat Genet 1992;1(3):196-8.
Strathdee CA, Gavish H, Shannon WR, Buchwald M. Cloning of cDNAs for Fanconi's anaemia by functional complementation. Nature 1992;356(6372):763-767.
Butturini A, Gale RP, Verlander PC, Adler-Brecher B, Gillio AP, Auerbach AD. Hematologic abnormalities in Fanconi anemia: an International Fanconi Anemia Registry study. Blood 1994;84(5):1650-5.
Diatloff-Zito C, Duchaud E, Viegas-Pequignot E, Fraser D, Moustacchi E. Identification and chromosomal localization of a DNA fragment implicated in the partial correction of the Fanconi anemia group D cellular defect. Mutat Res 1994;307(1):33-42.
Lo Ten Foe JR, Rooimans MA, Bosnoyan-Collins L, Alon N, Wijker M, Parker L, Lightfoot J, Carreau M, Callen DF, Savoia A, Cheng NC, van Berkel CG, Strunk MH, Gille JJ, Pals G, Kruyt FA, Pronk JC, Arwert F, Buchwald M, Joenje H. Expression cloning of a cDNA for the major Fanconi anaemia gene, FAA. Nat Genet 1996;14(3):320-3.
[No authors listed]. Positional cloning of the Fanconi anaemia group A gene. The Fanconi anaemia/breast cancer consortium. Nat Genet 1996;14(3):324-8.
D'Andrea AD, Grompe M. Molecular biology of Fanconi anemia: implications for diagnosis and therapy. Blood 1997;90(5):1725-36.
This article should be referenced as such:
Huret JL. Fanconi anaemia. Atlas Genet Cytogenet Oncol Haematol.1998;2(2):68-69.

Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS
Instructions to Authors Manuscripts submitted to the Atlas must be submitted solely to the Atlas. Iconography is most welcome: there is no space restriction. The Atlas publishes "cards", "deep insights", "case reports", and "educational items". Cards are structured review articles. Detailed instructions for these structured reviews can be found at: http://AtlasGeneticsOncology.org/Forms/Gene_Form.html for reviews on genes, http://AtlasGeneticsOncology.org/Forms/Leukaemia_Form.html for reviews on leukaemias, http://AtlasGeneticsOncology.org/Forms/SolidTumour_Form.html for reviews on solid tumours, http://AtlasGeneticsOncology.org/Forms/CancerProne_Form.html for reviews on cancer-prone diseases. According to the length of the paper, cards are divided, into "reviews" (texts exceeding 2000 words), "mini reviews" (between), and "short communications" (texts below 400 words). The latter category may not be accepted for indexing by bibliographic databases. Deep Insights are written as traditional papers, made of paragraphs with headings, at the author's convenience. No length restriction. Case Reports in haematological malignancies are dedicated to recurrent -but rare- chromosomes abnormalities in leukaemias/lymphomas. Cases of interest shall be: 1- recurrent (i.e. the chromosome anomaly has already been described in at least 1 case), 2- rare (previously described in less than 20 cases), 3- with well documented clinics and laboratory findings, and 4- with iconography of chromosomes. It is mandatory to use the specific "Submission form for Case reports": see http://AtlasGeneticsOncology.org http://atlasgeneticsoncology.org/Reports/Case_Report_Submission.html. Educational Items must be didactic, give full information and be accompanied with iconography. Translations into French, German, Italian, and Spanish are welcome.
Subscription: The Atlas is FREE!
Corporate patronage, sponsorship and advertising Enquiries should be addressed to [email protected].
Rules, Copyright Notice and Disclaimer Conflicts of Interest: Authors must state explicitly whether potential conflicts do or do not exist. Reviewers must disclose to editors any conflicts of interest that could bias their opinions of the manuscript. The editor and the editorial board members must disclose any potential conflict. Privacy and Confidentiality – Iconography: Patients have a right to privacy. Identifying details should be omitted. If complete anonymity is difficult to achieve, informed consent should be obtained. Property: As "cards" are to evolve with further improvements and updates from various contributors, the property of the cards belongs to the editor, and modifications will be made without authorization from the previous contributor (who may, nonetheless, be asked for refereeing); contributors are listed in an edit history manner. Authors keep the rights to use further the content of their papers published in the Atlas, provided that the source is cited. Copyright: The information in the Atlas of Genetics and Cytogenetics in Oncology and Haematology is issued for general distribution. All rights are reserved. The information presented is protected under international conventions and under national laws on copyright and neighbouring rights. Commercial use is totally forbidden. Information extracted from the Atlas may be reviewed, reproduced or translated for research or private study but not for sale or for use in conjunction with commercial purposes. Any use of information from the Atlas should be accompanied by an acknowledgment of the Atlas as the source, citing the uniform resource locator (URL) of the article and/or the article reference, according to the Vancouver convention. Reference to any specific commercial products, process, or service by trade name, trademark, manufacturer, or otherwise, does not necessarily constitute or imply its endorsement, recommendation, or favouring. The views and opinions of contributors and authors expressed herein do not necessarily state or reflect those of the Atlas editorial staff or of the web site holder, and shall not be used for advertising or product endorsement purposes. The Atlas does not make any warranty, express or implied, including the warranties of merchantability and fitness for a particular purpose, or assumes any legal liability or responsibility for the accuracy, completeness, or usefulness of any information, and shall not be liable whatsoever for any damages incurred as a result of its use. In particular, information presented in the Atlas is only for research purpose, and shall not be used for diagnosis or treatment purposes. No responsibility is assumed for any injury and/or damage to persons or property for any use or operation of any methods products, instructions or ideas contained in the material herein. See also: "Uniform Requirements for Manuscripts Submitted to Biomedical Journals: Writing and Editing for Biomedical Publication - Updated October 2004": http://www.icmje.org.
http://AtlasGeneticsOncology.org
© ATLAS - ISSN 1768-3262

Atlas of Genetics and Cytogenetics in Oncology and Haematology
OPEN ACCESS JOURNAL AT INIST-CNRS