Embed Size (px)
Citation preview

Actualités néphrologiques Jean Hamburger Necker
Mai 2019
1
In-hospital management of urinary tract infections :
difficult situations

In-hospital management of urinary tract infections : difficult situations
2
• Infection is severe > ex. severe urinary tract infections
• Background is tricky > ex. urinary tract infections in pregnancy
• Bug is resistant > ex. new betalactams
• Localization is tricky > ex. infection of kidney cysts

Severe pyelonephritis Sepsis : qSOFA ≥ 2
Septic shock
Surgery requirement
To be distinguished from UTI at risk of complicationAny urinary tract anatomical / functional disorder
Pregnancy
Frail elderly patient
Creatinine clearance < 30 ml/min
Severe immunodeficiency
3
Q SOFARR ≥ 22/minSBP < 100mmHgAltered consciousness
Conférence de consensus SPILF 2014- 2017

Severe pyelonephritis
• Work-up within 24 hoursUrine culture, creatinin, blood culture, urinary tract CT scan
• Antibiotics: betalactam + amikacin
• How to select the appropriate betalactam: 2-3 questions > 3G-cephalosporin allergy ?
> Has ESBL-E carriage/infection been documented in the past 6 months ?
> In case of septic shock : is there a risk for ESBL-E carriage?
4
Conférence de consensus SPILF 2014- 2017

Severe pyelonephritis
5
No septic shock
Parenteral 3G-C + amikacin
Severe allergy to penicillinsor allergy to 3G-C > aztreonam + amikacin
Aztreonam CI in case of delayed hypersensitivity- DRESS syndrome- Lyell, Stevens-Johnson
ESBL-E carriage /infection < 6 months> Choice based on prior identification
Conférence de consensus SPILF 2014- 2017
CefotaximeCeftriaxone

Severe pyelonephritis
6
ESBL-E carriage /infection < 6 months
Risk of ESBL-E infection
Septic shock
Parenteral 3G-C + amikacin
Severe allergy to penicillinsor allergy to 3G-C > aztreonam + amikacin
Pas de choc septique
C3G parentérale + amikacine
Allergie grave pénicillines ou allergie C3G> aztréonam + amikacine
Colonisation /infection E-BLSE < 6 mois> Prendre en compte, selon antibiogramme
No septic shock
Parenteral 3G-C + amikacin
Severe allergy to penicillinsor allergy to 3G-C > aztreonam + amikacin
ESBL-E carriage /infection < 6 months> Choice based on prior identification

Severe pyelonephritis
7
Risk factors for ESBL-E infection :- colonization /infection < 6 months- amox-clav/2-3G-C /FQ < 6 months- travel to an ESBL-E endemic area- hospitalization < 3 months- living in a long-term care facility
> Carbapenem + amikacin
ESBL-E carriage /infection < 6 months
Risk of ESBL infection
Septic shock
Parenteral 3G-C + amikacin
Severe allergy to penicillinsor allergy to 3G-C > aztreonam + amikacin
Severe pyelonephritis
Drainage of any obstruction
Clinical monitoring
Oral switch at 48 hrs > adapted to identification,
Treatment duration : 10 days (longer in abscesses)
Concomitant bacteremia does not require longer treatment duration
Initial severity does not require longer treatment duration
8
Conférence de consensus SPILF 2014- 2017
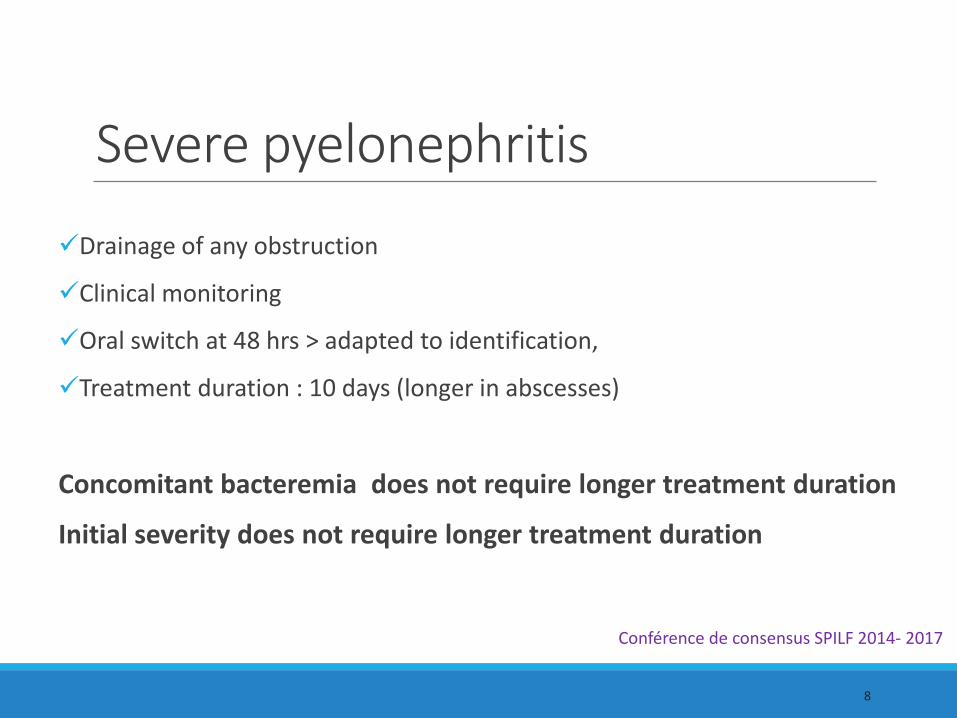
Pyelonephritis in pregnancy• Incidence 0.5%-1% of pregnancies
• Mechanical and hormonal risk factors
• Mostly T2/T3 : 80-90%
• Ecology is similar to non pregnant patients
9
Wing AJOG 2014
Duff Clin Obstet Gynecol 1984
Pathogen Frequency
E. coli 82%
Streptococcus B 21%
K. pneumoniae 7%
Proteus sp. 5%
Enterococcus sp. 5%
Wing AJOG 2014Hill Obstet Gynecol 2005
Pyelonephritis in pregnancy
• Bacteremia : 2-20% cas
• Pyelonephritis infections account for 55%
of E. coli bacteremia during pregnancy
• May lead to sepsis /septic shock 0.5- 2%
• May lead to premature delivery 10%
• May lead to recurrences up to 23%
10
Wing AJOG 2014Martin AJOG 2006
Surgers CMI 2014
Wing AJOG 2014
Archabald AJOG 2009
Gilstrap Obstet Gynecol 1981
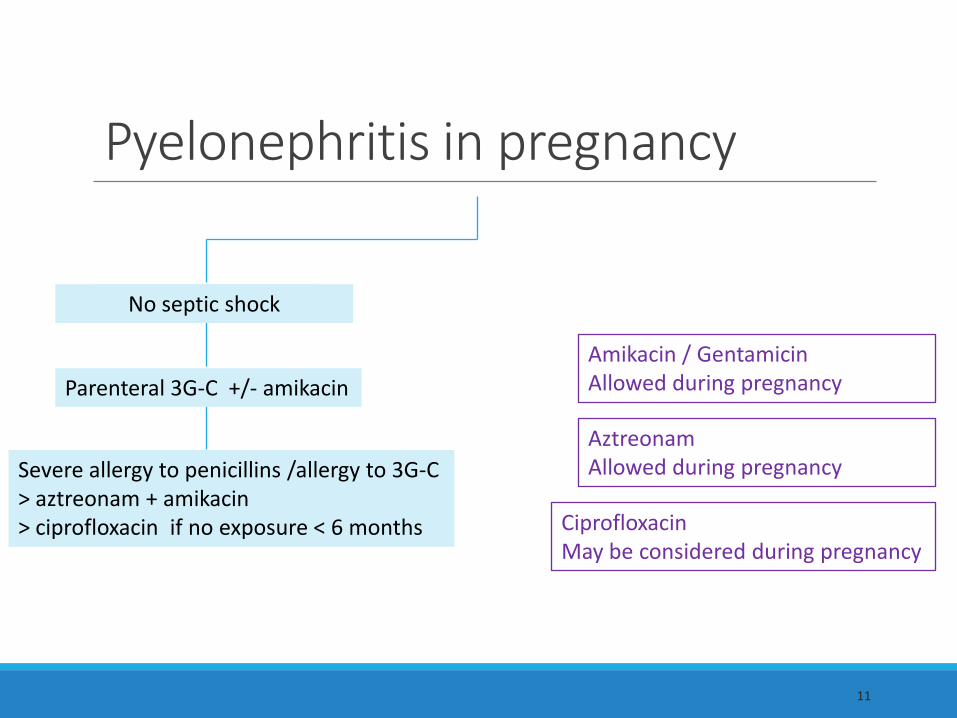
11
Pas de choc septique
CiprofloxacinMay be considered during pregnancy
AztreonamAllowed during pregnancy
Amikacin / GentamicinAllowed during pregnancy
No septic shock
Parenteral 3G-C +/- amikacin
Severe allergy to penicillins /allergy to 3G-C > aztreonam + amikacin> ciprofloxacin if no exposure < 6 months
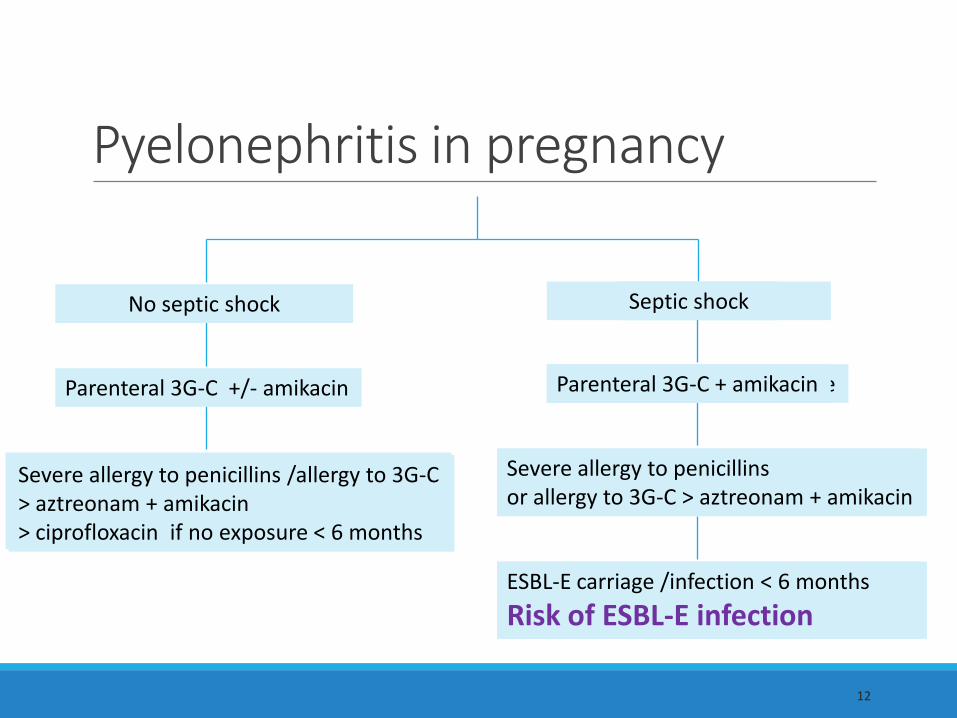
Pyelonephritis in pregnancy
12
Colonisation /infection E-BLSE < 6 mois
Risque d’infection à E-BLSE
Choc septique
C3G parentérale + amikacine
Allergie grave pénicillines ou allergie C3G> aztréonam+ amikacine
Allergie grave pénicillines ou allergie C3G> aztréonam +/- amikacine< 6 mois
No septic shock
Parenteral 3G-C +/- amikacin
Severe allergy to penicillins /allergy to 3G-C > aztreonam + amikacin> ciprofloxacin if no exposure < 6 months
ESBL-E carriage /infection < 6 months
Risk of ESBL-E infection
Septic shock
Parenteral 3G-C + amikacin
Severe allergy to penicillinsor allergy to 3G-C > aztreonam + amikacin
Pyelonephritis in pregnancy

• Work-up
Urine culture, creatinin, blood culture if severe/ dg uncertainties
Echography if hyperalgic /sepsis
Obstetrical evaluation
• Oral switch with compatible antibiotics
• Treatment duration 10-14days
• Urine culture 10d after antibiotic completion then /month until delivery
13
Pyelonephritis in pregnancy

Antibiotics and pregnancy
Yes Yes if… No
Betalactams ClavulanateAvoid at term
Cyclins
Macrolides Synergistins
CotrimoxazoleTeratogenic < 10SAAvoid at term
Kanamycin, Streptomycin
Furane Fosfomycin
CiprofloxacinIf no alternative
Other quinolon
INH, RMPPZA, ETB
AmikacinGentamicinX1/d , > 3 days
Colimycin
14
Czeizel Reprod Toxicol 2001Hernandez-Diaz NEJM 2000
Briggs 9th Ed. 2012
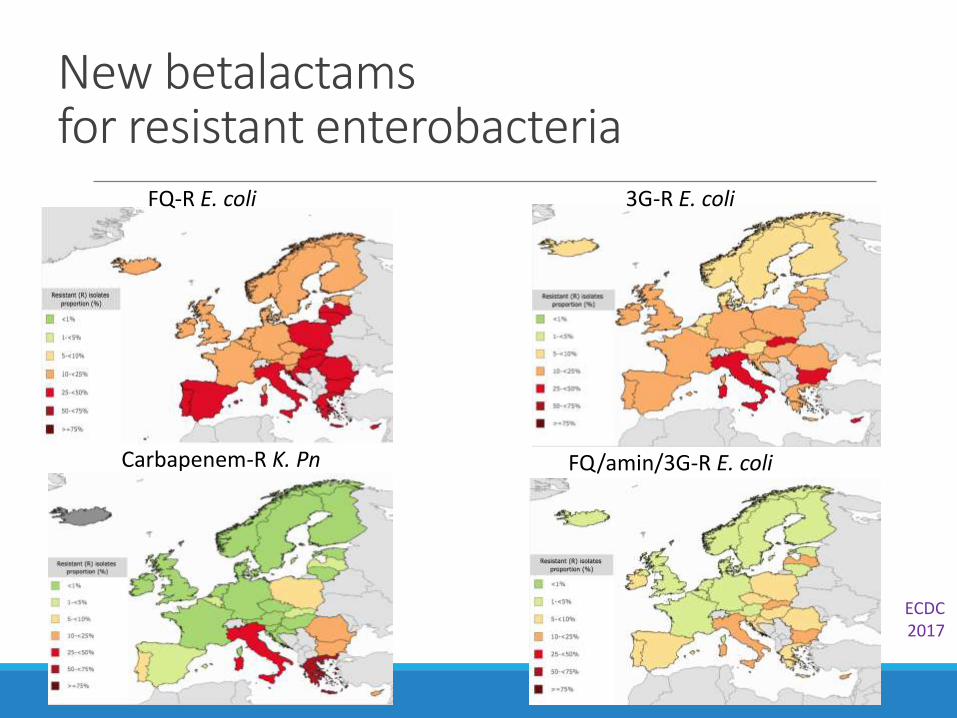
New betalactamsfor resistant enterobacteria
15
FQ/amin/3G-R E. coli
FQ-R E. coli 3G-R E. coli
Carbapenem-R K. Pn
ECDC2017

Aztreonam if no add. resistance
CarbapenemPeni+ inhib +/-TemocillinCefoxitin
Ruppé Ann Intensive Care 2015
C4GCarbapénèmes
CAZAZMCEPC3GMight work if no add. resistance

17
•Ceftolozane- Tazobactam> Zerbaxa
Caftazidime – Avibactam> Zavicefta
Inhibitor Is a betalactaminTargets class A enzymes
Is not a betalactaminTargets class A, C, D enzymes
Betalactam Cephalosporin derived from ceftazidime X 2 affinity for PBP Increased resistance to AmpC Much less AmpC induction
Cephalosporin
Streptococci (not Enterococcus sp.)Aerobic Gram negative bacteriaPseudomonas aeruginosaNo : Staphylococci, Stenotrophomonas sp., Acinetobacter sp. Limited anti anaerobic effect
New betalactamsfor MDR- enterobacteria
COMAI APHP 2018Van Duyn , Bonomo CID 2016
20% E. coli BLSE are resistant Farrell AAC 201350% KP BLSE are resistant Sader JAC 2014

CFT/TAZ
CAZ/AVI
18

19
•
Ceftolozane- Tazobactam> Zerbaxa
Caftazidime- Avibactam> Zavicefta
PK/PD IV only, 1g/500mg x 3/dKidney elimination , dialysedDouble dose in VAPAdapt if Cl < 50 ml/min
IV only, 2g/0,5g x 3/dKidney elimination , dialysed
Adapt if Cl < 50 ml/min
Indic. Complicated intra-abdominal infectionsComplicated UTI
Complicated intraabdominal infectionsComplicated UTINosocomial Pneumonias/VAP ++
In documented infections only Zerbaxa ++ Pseudomonas aeruginosa cefta-R Zavicefta ++ in some ESBL-E and OXA-48 documented infections Impact on the gut flora : no comparative study Cost ++
New betalactams for MDR- enterobacteria
COMAI APHP 2018Van Duyn , Bonomo CID 2016

20
COMAI APHP
Cyst infections in polycystic kidney disease• Cyst infections requiring hospitalization reported in 9% ADPKD
• Cyst infections are associated with morbi-moratlity• Up to 7% mortality
• Enhanced renal impairment
• Sources of infection• Ascendant/hematogenous/nosocomial
• A diagnostic and therapeutic challenge
• Few available data
21
Sallée Clin J Am Soc Nephrol 2009
Fick Clin J Am Soc Nephrol 1995Cornec-Le Gall J Am Soc Nephrol 2016
Sallée Clin J Am Soc Nephrol 2009
Sallée Clin J Am Soc Nephrol 2009Suwabe EJCMID 2015
Lantinga NDT 2015Sklar AJKD 1985
ADPKD, KDIGO Guidelines, Kidney Int 2015

• Clinical presentation is not specific
> 2 main differential diagnoses = pyelonephritis, cyst hemorrhage
> Pyelonephritis and cyst infection may coexist in the same ADPKD patient
> Hemorrhages may superinfect
> Kidney transplanted ADPKD : higher risk of native kidney infections
Non-functional end-stage polycystic kidneys may also be infected
22
Cyst infection in ADPKDA diagnosis challenge
Ziebell Clin Nephrol 2002

•Microbiological presentation
> Same ecology as other UTI
> Both urine and blood cultures may be negative in 25%
> Gold standard : cyst punction
• Diagnosis criteria
23
Cyst infection in ADPKDA diagnosis challenge
Oh Plos ONE 2018Sallée Clin J Am Soc Nephrol 2009
Suwabe EJCMID 2015
Fever > 38°5C > 3 daysAbdominal PainCRP > 50 mg/LNo recent bleeding on CT scanNo alternate cause of fever
Lantinga NDT 2015

• Radiological presentation non specific and not sensitive
• Echography• Hyperechoic
• Heterogeneous
• Internal septation
• CT scan• Irregular
• High attenuation
• Peripherical C+ enhancement
• Pericystic infiltration
•MR imaging > similar
24
Cyst infection in ADPKDA diagnosis challenge
Oh PLOSONE 2018
• Sensibility is poor
CT and MRI show contributive images in 18 and 40% of cyst infection cases
CT and MRI yield negative results in >50% cases confimed by cyst punction
• Specificity is low
Intraluminal heterogeneity may be seen in uninfected cysts (cellular debris)
Contrast enhancement lining cyst walls can be caused by inflammation
• Administration of contrast agents may be contra-indicated
25
Cyst infection in ADPKDA diagnosis challenge
Jouret NDT 2012
Sallée Clin J Am Soc Nephrol 2009

26
Cyst infection in ADPKDA diagnosis challenge
• Pet 18FDG
18FDG not nephrotoxic
Localization
Follow-up : negativation within 9 weeks
False negative results described
Timing?
Specificity ? > Hemorrhages/pericystic pyelonephritis/tumoral lesion
Cost and availability?
Jouret Clin J Am Soc Nephrol 2011Neuville PLoSONE 2016
Bobot CMI 2016
ADPKD, KDIGO Guidelines, Kidney Int 2015

Cyst infections in ADPKDA therapeutic challenge
No therapeutic trial
Intracyst diffusion of antibiotics• Glomerular filtration
• Transepithelial diffusion
• Proximal vs distal cyst
• Lipophilic/phobic
Quinolons
Cotrimoxazole
Clindamycin
Metronidazole
27
Moleculs Cyst/plasma ratio Reference
Ciprofloxacin 2-4.4 Elzinga AAC 1987; Telenti Mayo Clin Proc 1990
Levofloxacin 0.96 Hiyama AJKD 2006
Trimethoprim 3.9-8/ 1-23 Elzinga kidn Int 1987; Schwab AJKD 1986
Sulfamethox. 0.43 Elzinga kidn Int 1987
Gentamicin 0.18-0.34 Muther Kidney Int 1981; Schwab AJKD1083
Amikacine 0 Bennett AJKD 1985
Ticarcilline 0.12 Muther Kidney Int 1981
Meropenem 0.04-0.13 Hamanoue BMCN 2018
Cefotaxime 0 after 1 dose Bennett AJKD 1985
Amoxicillin 0-4.6 after 1-8 d Bennett AJKD 1985
Metronidazole 0.8-1 Bennett AJKD 1985
Vancomycin 0.06-0.61 Bennett AJKD 1985
Clindamycin 0.52-069/2.4-8.7 Bennett AJKD 1985; Schwab 1983
ADPKD, KDIGO Guidelines, Kidney Int 2015Adapted from Sallée CJASN 2009

Cyst infections in ADPKDA therapeutic challenge
Diffusion, although low, might be above the MIC
Diffusion might be enhanced in infected cysts
> amikacin cyst/plasma ratio 0 in uninfected cyst 0.5 in infected cyst
Slow delayed diffusion > prefer longer treatments
28
Ohkawa Nephron 1991
Bennett AJKD 1985

Cyst infections in ADPKDA therapeutic challenge
Treatment failure requiring drainage reported in up to 30% of cases
Parameters associated with failure • Cyst size > 5cm
• Non E. coli bacteria
29
Julien DANGOngoing study
Retrospective monocentric cohort140 episodes : 91 patients 56 episodes in Tx patients 2000-2018Confirmed : by punctionProbable : clin + RxPossible : clin
Survival without recurrentUTI
0 100 300 400
0
50
100Cotrimoxazole (n=6)
Fluoroquinolone (n=32)
Beta-Lactam (n=24)
log-rank p=0.052
200
Days
Julien DANG Thèse de Médecine en cours

Cyst infections in ADPKDA therapeutic challenge
Treatment failure requiring drainage reported in up to 30% of cases
Parameters associated with failure • Cyst size > 5cm
• Non E. coli bacteria
30
Julien DANGOngoing study
Retrospective monocentric cohort140 episodes : 91 patients 56 episodes in Tx patients 2000-2018Confirmed : by punctionProbable : clin + RxPossible : clin
Survival without recurrentUTI
0 100 300 400
0
50
100ATB > 28 days (n=47)
ATB 22-28 days (n=28)
ATB 15-21 days (n=48)
ATB < 15 days (n=12)
log-rank p<0.001
200
Days
Julien DANG Thèse de Médecine en cours

Cyst infections in ADPKDA therapeutic challenge
• Prefer antibiotics with good cyst diffusion
• Prefer long treatment duration > 21 days
• Timing of cyst punction ?
• Use of Pet 18FDG to monitor treatment ?
31
Julien DANG Thèse de Médecine en cours

Thank you for your attention
32