Embed Size (px)
Citation preview

Improving the Spiritual Dimension of Palliative Care: Advanced Interprofessional Spiritual
Care
Betty Ferrell, PhD, RNGeorge Handzo, BCC, MDivShirley Otis-Green, MSW,
Christina Puchalski, MD, MS
AAHPM, 2012

What is Whole Person Care?
• Transcends control of a disease process and the relief of symptoms
• Aims at full health, understood as the recovery of an integrated and authentic self
• Maintains focus on the patient as a whole person, regardless of how intractactable, difficult, time consuiming, expensive or challenging the patient’s problems are
© cpuchalski

Biopsychosocialspiritual
© cpuchalski

Spiritual/Religious/Cultural Beliefs, Practices, and Rituals
• May be dynamic in patient’s understanding of illness
• Religious convictions/beliefs may affect healthcare decision-making
• May be a patient need
• May be important in patient coping, quality of life, and healthcare outcomes
• Integral to whole-patient care© cpuchalski

5
Guidelines for Interprofessional
Spiritual Care: Improving the Quality of
Spiritual Care as a Dimension of
Palliative Care:A Consensus Conference Convened February 2009
Supported by the Archstone Foundation, Long Beach, CA. as a part of their End-of-Life Initiative.
© cpuchalski

6
The NCP 8 domains of care
• Structure and Processes; • Physical Aspects; • Psychological and Psychiatric Aspects; • Social Aspects; • Spiritual, Religious, and Existential Aspects; • Cultural Aspects; • Imminent Death; and • Ethical and Legal Aspects.
© cpuchalski

7
Consensus Definition was Developed
• “Spirituality is the aspect of humanity that refers to the way individuals seek and express meaning and purpose and the way they experience their
connectedness to the moment, to self, to others, to nature, and to the significant or sacred.”
© cpuchalski

8
Final Conference Report
• Puchalski, C., Ferrell, B., Virani, R., Otis-Green, S., Baird, P., Bull, J., et al. (2009). Improving the quality of spiritual care as a dimension of palliative care: The report of the consensus conference. Journal of Palliative Medicine, 12(10), 885-904. DOI:10.1089=jpm.2009.0142
• Puchalski,C. & Ferrell, B. (2010). Making Healthcare Whole: Integrating Spirituality into Patient Care. West Conshohocken, PA: Templeton Press.
© cpuchalski

9
Conference Recommendations•Recommendations for improving spiritual care
are divided into seven keys areas:
I.Spiritual Care ModelsII.Spiritual AssessmentIII.Spiritual Treatment/Care PlansIV.Interprofessional TeamV.Training/CertificationVI.Personal and Professional DevelopmentVII.Quality Improvement
© cpuchalski

Recommendations
• Integral to any patient-centered health care system
• Based on honoring dignity
• Spiritual distress treated the same as any other medical problem
• Spirituality should be considered a “vital sign”
• Interdisciplinary
© C.Puchalski
I. Spiritual Care Models

Spirituality and HealthFetzer Health Advisory Council , 2011
• Love/compassion• Dignity• Forgiveness • Wholeness, full-self• Other-regarding• Relationship-centered• Healing as transformational in context of
relationship• Humanity of providers and patients
© C.Puchalski

National Consensus Conference
Spiritual care models should be interdisciplinary and clinical settings should have a clinical pastoral education trained board-certified chaplain as part of the inter-professional team.
Puchalski, C., Ferrell, B., Virani, R., Otis-Green, S., Baird, P., Bull, J., et al. (2009). Improving the quality of spiritual care as a dimension of palliative care: The report of the consensus conference. Journal of Palliative Medicine, 12(10), 885-904. DOI:10.1089=jpm.2009.0142.© cpuchalski

13
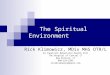
Inpatient spiritual care implementation
model
© cpuchalski

Role on the Team
• Spiritual Care Generalist
• Vs.
• Spiritual Care Specialist
• Handzo, G. F. & Koenig, H. G. (2004). Spiritual Care: Whose Job is it Anyway? Southern Medical Journal, 97(12), 1242-1244.
• © cpuchalski

15
II. Spiritual Assessment of Patients and
Families• Recommendations• Spiritual screening, history• Assessment tools• All staff members should be trained to recognize
spiritual distress• HCP’s should incorporate spiritual screening and
history as a part of routine history/evaluation• Formal assessment by Board Certified Chaplain• Documentation• Follow-up• Chaplain Response within 24 hours
© cpuchalski

Impaired ability to experience and integrate meaning and purpose in life through connectedness with self, others, art, music, literature, nature, and/or a power greater than oneself.
NANDA, 2007
Terms: Spiritual Distress
© C.Puchalski

• Questioning the credibility of one’s belief system.• Demonstrating discouragement or despair.• Inability to practice usual religious rituals.• Ambivalent feelings (doubts) about beliefs.• Expressing that he/she has no reason for living.• Feeling a sense of spiritual emptiness.• Showing emotional detachment from self and others.• Expressing concern, anger, resentment, fear - over
the meaning of life, suffering, death.• Requesting spiritual assistance for a disturbance in
belief system.RN Central Online, 2007
Clinical Presentationsof Spiritual Distress
© C.Puchalski

Spiritual DiagnosisDiagnoses (Primary) Key feature from history Example Statements
ExistentialLack of meaning / questions meaning about one’s own existence / Concern about afterlife / Questions the meaning of suffering / Seeks spiritual assistance
“My life is meaningless”“I feel useless”
Abandonment God or otherslack of love, loneliness / Not being remembered / No Sense of Relatedness
“God has abandoned me”“No one comes by anymore”
Anger at God or othersDisplaces anger toward religious representatives / Inability to Forgive
“Why would God take my child…its not fair”
Concerns about relationship with deity
Closeness to God, deepening relationship “I want to have a deeper relationship with God”
Conflicted or challenged belief systems
Verbalizes inner conflicts or questions about beliefs or faith Conflicts between religious beliefs and recommended treatments / Questions moral or ethical implications of therapeutic regimen / Express concern with life/death and/or belief system
“I am not sure if God is with me anymore”
Despair / Hopelessness Hopelessness about future health, lifeDespair as absolute hopelessness, no hope for value in life
“Life is being cut short”“There is nothing left for me to live for”
Grief/loss Grief is the feeling and process associated with a loss of person, health, etc
“I miss my loved one so much”“I wish I could run again”
Guilt/shameGuilt is feeling that the person has done something wrong or evil; shame is a feeling that the person is bad or evil
“I do not deserve to die pain-free”
Reconciliation Need for forgiveness and/or reconciliation of self or othersI need to be forgiven for what I didI would like my wife to forgive me
Isolation From religious community or other“Since moving to the assisted living I am not able to
go to my church anymore”
Religious specificRitual needs / Unable to practice in usual religious practices
“I just can’t pray anymore”
Religious / Spiritual StruggleLoss of faith and/or meaning / Religious or spiritual beliefs and/or community not helping with coping
“What if all that I believe is not true”© cpuchalski

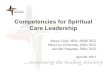
Spiritual Diagnosis Decision Pathways
© cpuchalski

Patients’ Spiritual Needs
• Love and belonging
• Meaning and purpose
• Appreciation of nature and beauty
• Spiritual/religious practices and guidance
• Positivity, gratitude and peace
• Resolution of issues involving life and death
• (National survey of US hospitals HCC)Flannelly, K.J., et al Hospital Topics, 2005
© C.Puchalski

• Occurs through a dynamic and interactive growth process that leads to a realization of the ultimate purpose and meaning of life. (Hungelmann et al., 1996)
• Ability to experience and integrate meaning and purpose in life through connectedness with self, others, art, music, literature, nature, and/or a power greater than oneself that can be strengthened. (Johnson, 2006)
• Spiritual well-being is the affirmation of life in a relationship with God, self, community and environment that nurtures and celebrates wholeness. (NICA, 1975)
Terms: Spiritual Well-Being
© C.Puchalski

Spiritual Resources of Strength
• Beliefs, values, practices that are supportive to patient
• Spiritual, religious support groups• Hope• Resiliency, good coping skills• Finding meaning, purpose
© C.Puchalski

Can be spirituality be reduced to a diagnosis?
© C.Puchalski

Reductionsim: Language of medicine, nursing
Sharing stories: Language of chaplains, social workers
The Challenge: How to blend the two….
Language: Talking to Colleagues

Recommendations
• Screen & Access
• All HCPs should do spiritual screening
• Clinicians who refer should do spiritualhistories and develop appropriate treatment plans working with Board Certified Chaplain if possible
• Diagnostic labels/codes
• Treatment plans
• Support/encourage in expression of needs and beliefs
© C.Puchalski
III. Formulation of a Spiritual Treatment Care Plan

• Spiritual care referral (BCC, pastoral counselor, spiritual director, clergy as appropriate)
• Documentation of spiritual support resources
• Follow up evaluations
• Treatment algorithms
• Discharge plans of care
• Bereavement care
• Establish procedure
© C.Puchalski
III. Formulation of a Spiritual Treatment Plan (cont’d)


Ms. Harper is a 75 yo s/ cva with hemiparesis and mild cognitive impairment
Physical Ongoing physical therapy, rehab
Emotional Grief rxn over loss of previous state of functioningSupportive counseling, presence.
Social Engage activist community in her care as much as possibleNeeds home health aidFinancial issues about long term care
Spiritual Meaninglessness, consider referral to pastoral counselor or chaplain,Explore ways to find meaning in current situation, meaning oriented therapy
Case example: Biopsychosocial-Spiritual
Model Assessment and Plan

• Spiritual Screening• Spiritual History• Comprehensive Spiritual Assessment• What underlies this is compassion…
Talking About Spiritual Issues
© C.Puchalski

Spiritual/Religious Screening
A quick determination of whether a person is experiencing a serious spiritual/religious crisis and therefore needs an immediate referral to a professional chaplain. Good models of spiritual/religious screening employ a few, simple questions, which can be asked by any health care professional in the course of an overall screening.
Fitchett, G., & Canada, A. L. (2010). The Role of Religion/Spirituality in Coping with Cancer: Evidence, Assessment, and Intervention. In J. C. Holland (Ed.). Psycho-oncology, 2nd Edition. New
York: Oxford University Press.
© C.Puchalski

Spiritual Screening
• Do you have any spiritual beliefs that might affect your stay here at the hospital?
• Are there any spiritual beliefs that you want to have discussed in your care with us here?
• How important is spirituality in your coping? and “How well are those spiritual resources working for you at this time?”
© C.Puchalski

Spiritual History Taking
The process of interviewing patients, asking them questions about their lives in order to come to a better understanding of their needs and resources. The history questions are usually asked in the context of a comprehensive examination by the clinician who is primarily responsible for providing direct care or referrals to specialists, such as professional chaplains.
Fitchett, G., & Canada, A. L. (2010). The Role of Religion/Spirituality in Coping with Cancer: Evidence, Assessment, and Intervention. In J. C. Holland (Ed.). Psycho-oncology, 2nd Edition. New York: Oxford University Press.
© C.Puchalski

Spiritual Assessment
A more extensive [in-depth, on-going] process of active listening to a patient's story as it unfolds in a relationship with a professional chaplain and summarizing the needs and resources that emerge in that process. The summary includes a spiritual care plan with expected outcomes which should be communicated to the rest of the treatment team.
Fitchett, G., & Canada, A. L. (2010). The Role of Religion/Spirituality in Coping with Cancer: Evidence, Assessment, and Intervention. In J. C. Holland (Ed.). Psycho-oncology, 2nd Edition. New York: Oxford University Press.
© C.Puchalski

Spiritual History
• Comprehensive• Done in context of intake exam or during a
particular visit such as breaking bad news, end of life issues, crisis
• Done by the clinician who is primarily responsible for providing direct care or referrals to specialists such as professional chaplains.
© C.Puchalski

Spiritual History
• FICA (Puchalski, 1996, 2000, 2006)• Spirit (Maugins, 1996 )• Hope (Anandarajah, 2001)
© C.Puchalski

FICA
Developed with a focus group of primary care physicians
Used in the social history section of H & PTool used to invite patients to share about their
beliefs and valuesHelps identify spiritual distress, conflict,
meaning of illness, inner resources of strengthHelps identify referrals (chaplain, meditation,
journaling, music, spiritual direction, pastoral counseling, other spiritual resources)
© C.Puchalski

Social History
• Important relationships; sexual history• Occupational history• Avocation interests• Wellness/prevention: exercise, nutrition, spiritual
beliefs, smoking, alcohol/drugs, seat belts, domestic violence, mood
© C.Puchalski

Spiritual History
F - Do you have a spiritual belief? Faith? Do you have spiritual beliefs that help you cope with stress/what you are going through/ in hard times? What gives your life meaning?
I - Are these beliefs important to you? How do they influence you in how you care for yourself?
C - Are you part of a spiritual or religious community?
A - How would you like your healthcare provider to address these issues with you?
© C.Puchalski

52-year-old female with breast mass. Has a strong family history of breast cancer. Her mother died of breast cancer when the patient was 18 years old. Her two sisters have breast cancer.
Ms. Smith
© C.Puchalski

F - MD: Do you have any spiritual beliefs that help you in your life?
PT: I find meaning in Nature.
I - MD: How does that help you?
PT: I feel at one with nature. Each morning I sit on my patio looking out over the trees in the woods and feel “centered and with purpose”
MD: Do your beliefs affect your healthcare decisions?
PT: If I am dying I would want to be in a hospice that has nature around it.
C - MD: Is there a community that supports you in this.
PT: Close friends who share her values
A - After the discussion about belief, she sill try to meditate, focusing on nature, on a daily basis to increase her peacefulness and her ability to cope with whatever the biopsy shows.
Ms. Smith
© C.Puchalski

Share your course materials, lectures, tutorials, etc.
© cpuchalski

Resources• www.gwish.org
• Education resources (SOERCE, National Competencies etc)
• Retreats in for Healthcare Professionals (Assisi, US)• FICA Assessment tool--- online DVD• Summer Institute in spirituality and health at GWU.
June 2011
• www.coh.org
• www.healthcarechaplaincy.org
© cpuchalski