Embed Size (px)
Citation preview
Pierre Barker MD
Senior Vice President IHI
Improving Quality: Theories of Change

“Every system is perfectly
designed to achieve the
result it gets” Paul Batalden

Every System……

Basic
science
Proof of
concept
Large
scale
efficacy
Study
What are we trying to solve?
The “What”
Reliable
“real-life”
implement-
ation
Scale-up to
populations
The “How”
Guidelines, Training & Resources,
Adaptive Designs that are context
sensitive
Designs that can be scaled-
up with the resources at
hand

Quality Improvement: Bringing Together
Two Types of Knowledge – (Deming)
Implementation
Knowledge Motivation/Leadership
Efficient Systems
Accurate Reflective Data
Context-sensitive
learning
Evidence
Based Subject
Matter
Knowledge Protocols/Guidelines,
Physical resources,
Clinical Training
the “what”
the “how”

Implementation
Knowledge
Evidence-based Subject
Matter Knowledge
Improvement
Improvement: Bringing Together Two
Types of Knowledge

Dr. Joseph M. Juran’s “Trilogy” 7
QUALITY PLANNING
QUALITY IMPROVEMENT
QUALITY CONTROL

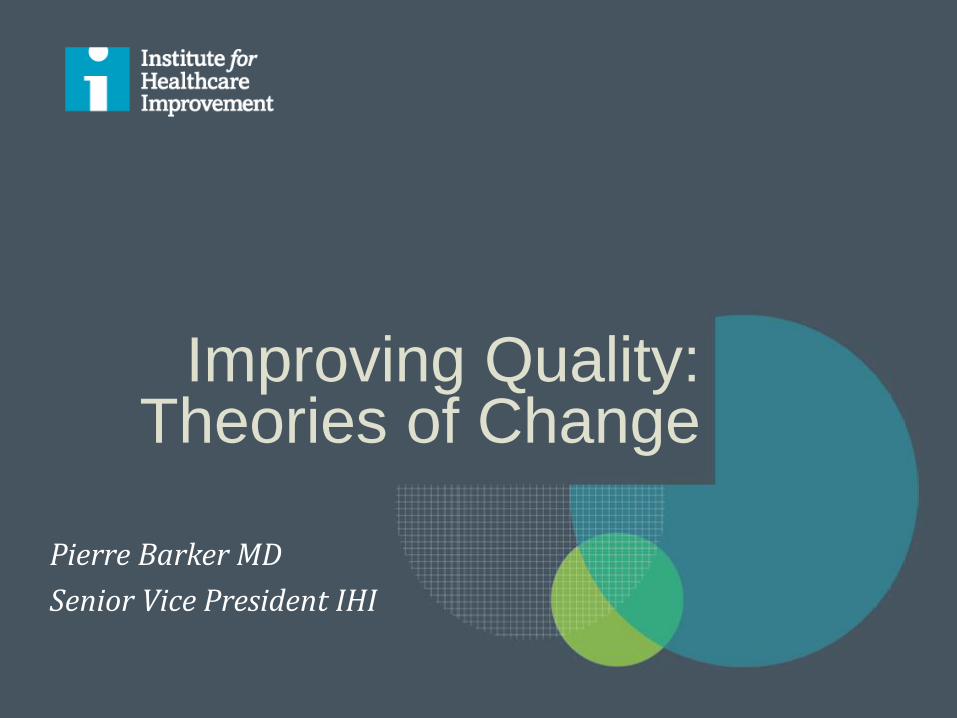
Juran Trilogy: All three elements are
needed
8
PERFORMANCE SHIFT
Chronic waste (opportunity for improvement)
Sporadic spike
Source: Juran J, Godfrey AB, eds. Juran’s Quality
Handbook: Fifth Edition. New York: McGraw-Hill, 1999.

Juran Trilogy: All three elements are
needed
9
PERFORMANCE SHIFT
Chronic waste (opportunity for improvement)
Sporadic spike
Source: Juran J, Godfrey AB, eds. Juran’s Quality
Handbook: Fifth Edition. New York: McGraw-Hill, 1999.
Juran Trilogy: All three elements are
needed
10
PERFORMANCE SHIFT
Chronic waste (opportunity for improvement)
Sporadic spike
Source: Juran J, Godfrey AB, eds. Juran’s Quality
Handbook: Fifth Edition. New York: McGraw-Hill, 1999.

Policy, resources, coordination, accountability, mandates, etc.
Quality Planning
Components of quality: structure,
quality control and quality improvement
11
Quality
Improvement Motivation/Leadership
Efficient Systems
Reflective Data
Context-sensitive
learning
Standards/ Guidelines/
protocols
Professional oversight
Accreditation
Checklists
Inspection &
reward/censure
Quality Control
IMPROVED
OUTCOMES

12
Aims
Measures
Changes
Model for
Improvement
The “Engine” of Improvement: the
Model for Improvement
1. What are we trying to accomplish?
2. How will we know that a change is an improvement?
3. What change can we make that will result in an improvement?
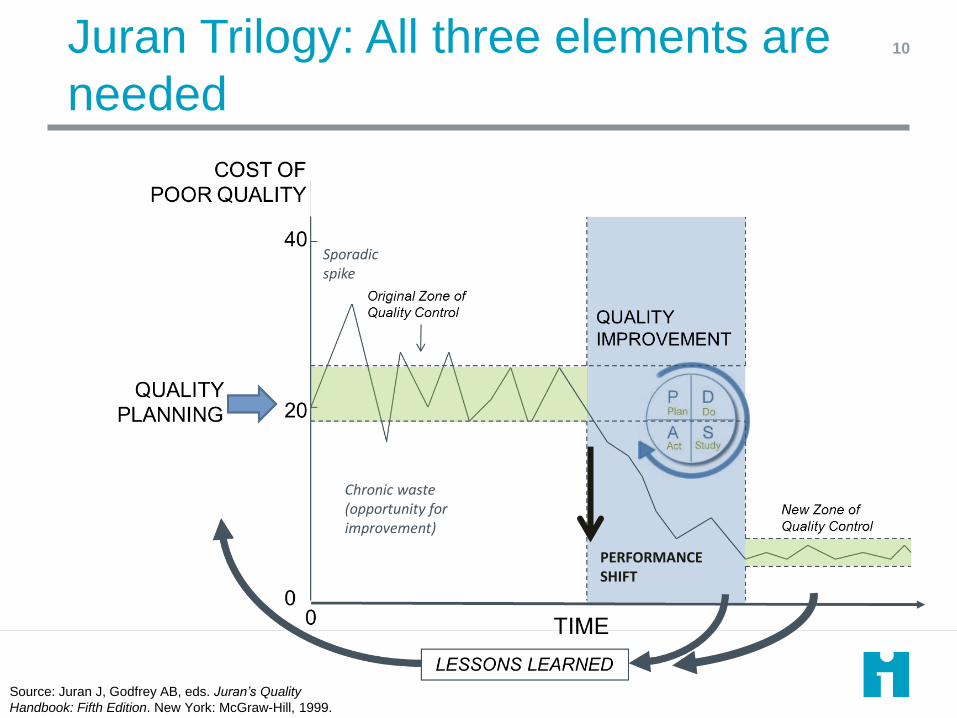
Quality Planning
13
Quality
Improvement Aims
Measures
Changes
Quality Control
IMPROVED
OUTCOMES
QA and “QI” confusion: both use Model
for Improvement and long/short PDSAs
Aims
Measures
Changes

QA and QI: Differences in approach QA QI
Performance goal
Perform to standards (controls) across multiple parts of the system
Aspire to a best performance goal for a focused improvement area
Measurement Periodic inspection of past events (large set of measures of inputs and/or processes)
Continuous tracking of current activity (few key processes linked to outcome)
Data Tracking Before and after change Continuous (e.g. run charts)
Data System External: e.g. inspection tools Internal: e.g. registers and tally sheets
Changes Standards driven. Normative. Can be linked to frontline system analysis
Theory driven. Adaptive. Always linked to frontline system analysis
Motivation for change
Management led, compliance, incentives, competition
Shared governance, internal motivation, “all teach all learn”
PDSA Management planning with single “slow” (months) intervention cycle. Can use frontline rapid cycle to respond to defects
Frontline planning Rapid cycle (days/weeks) is core activity

Putting it together on the QA/QI Spectrum
QA QI Accreditation
COPE
SBM-R
Training and Supportive Supervision

QA Approach
IMPLEMENT
PROBLEM
SOLUTION
Review (Succeed/Fail)
SYSTEM BARRIERS

QI Approach
GREAT IDEAS
SYSTEM ANALYSIS
DO
STUDY
ACT IMPLEMENT
SUCCEED/ FAIL
PROBLEM
PLAN


Theory of Change: Drivers of Maternal
and Newborn Survival
Decrease Maternal and
newborn mortality by
50%
Motivation for change
Knowledgeable health workers ready to use their
skills
Immediate access to essential commodities
Data systems in real time
A Learning System Cross-professional teams meet regularly, review data, test changes, report progress
Progress celebrated, challenges supported
Informed/activated patients & communities
Drills, mentoring
Decision support, checklists
Key suppliers part of QI team
Data for improvement vs data for reporting
Data “owned” at every level
Multi-level leaders promote change
Supportive Supervision

% eligible women received at least one
dose of corticosteroids
2
1

% eligible women received at least one
dose of corticosteroids
Zone of control QI Status Quo

Sustainability
Hospital 1
Hospital 2
Nkhoma
1 1
2
1
1 1
2
1 1
2
2
1 1
3
1 1
3
1 1 1

Sustainability
February 2014
June 2014
December 2014

Role of QI, QA in Scale-up 24

P25
Set-up (Status Quo)
Scalable Model for Improvement
(innovation)
Test Scale- Up (Context adaptations)
Go to Full-Scale (Spread)
Phases of Scale-up
QA QI QA
Role of QI, QA in Scale-up
Questions
Are some methods intrinsically more suitable for different
aspects/phases of implementation?
Should we ensure that large system improvement
designs include all elements of Juran trilogy (QP, QC,
QI)
How do we ensure that our improvement efforts are
sustained into the future?