Embed Size (px)
Citation preview

1
Improving Palliative Care in Rhode Island ICUs
Margaret Cornell Vigorito, MS, RN, CPHQ
Senior Program Administrator
Healthcentric Advisors
Lynn McNicoll, MD
Clinical Consultant, Healthcentric Advisors
Associate Professor, Warren Alpert School of Medicine, Brown University
RI ICU Collaborative Background
• Launched in the fall, 2005
• Partnership between three state quality organizations: The RI Quality Institute, Hospital Association of RI, Healthcentric Advisors
• Funded by Blue Cross Blue Shield of Rhode Island (70%) and UnitedHealthcare of New England (30%) for three 2-year phases
• 100% of RI adult ICUs enrolled (23 ICUs from 11 hospitals)

2
ICU Collaborative Goal
• Goal: To improve patient safety and
clinical outcomes for adult ICU patients
through the development of a unit
based safety program and
implementation of evidence-based
practices.
Program Improvement Components
– Comprehensive Unit-Based Safety Program (CUSP) including SAQ – fall, 2005
– Central-Line Associated Blood Stream Infection Bundle (CLA-BSI) – winter, 2006
– Ventilator Associated Pneumonia Bundle (VAP) –winter, 2006
– Sepsis – spring, 2008
– Palliative Care, Spring, 2010

3
ICU Palliative Care ProgramWhy? Demographics and Cost
• Demographics
– 20% of deaths occur in an ICU
– 30% of acute care costs
– Continued growth of population over the age of 65 placing greater demands on ICU services
ICU Palliative Care ProgramWhy? – Communications• Family members of pts dying in the ICU
– Higher concerns with physician communication
– More likely to have care decisions without enough family input and not consistent with patient wishes
» Ward NS, Levy MM, Teno JM AJRCCM 2004
• Family meetings
– Average duration 10 min
– 54% did not understand prognosis or tx» Azoulay E et al; 2000 CCM;28(8):3044-49

4
ICU Palliative Care ProgramWhy? - Anxiety and depression• 43 family interviews in France (hospital
anxiety and depression scale)
– Anxiety - 69%
– Depression – 35.4%
• Factors
– Absence of regular MD mtgs
– Lack of space
– Contradictory information» Pochard et al CCM 2001;29:1893-1897
Our Palliative Care Journey
Journey:
process of development:
a gradual passing from one
state to another regarded as
more advanced

5
Palliative Care -Prelaunch Activity
PC Sub-Committee: May-June 2009
• recommendations on bundle selection,
quality indicators, and academic faculty
– Literature review and environmental scan
– Customized bundle and quality measures
– Developed exclusion criteria (“opt out” vsopt in” approach)
Palliative Care -Prelaunch Activity
PC Sub-Committee: May-June 2009
• Gap analysis
• Pre-launch survey
• Unit participation

6
Palliative Care -Prelaunch Activity PC Steering Committee: Sept 2009-Apr 2010
• Program structure design
• Goals and metrics
• Data Abstraction specifications
• Data collection and submission process
• Learning Session Launch planning
• PC “logo”
Palliative Care -Prelaunch Activity
Project Management
• Data base development
• Team work plan
• Comprehensive toolkit
• On-site visits
7
Key Pre-Launch Resources
�Center to Advance palliative Care (CAPC) www.capc.org
�Center to Advance Palliative Care (CAPC) –IPAL-ICU www.capc.org/ipal-icu
�End of Life Palliative Care Education Resource Center (EPERC) www.mcw.edu/eperc
�Institute for Healthcare Improvement (IHI) www.ihi.org
Key Pre-Launch References�Crosswalk of JCAHO Standards and Palliative Care – with PC
Policies, Procedures and Assessment Tools. Center to Advance
Palliative Care Sutton Group. February 18, 2004
�Lynn J, Chaudhry E, Simon LN, Schuster JL, Wilkinson AM. The
Common Sense Guide to Improving Palliative Care. New York:
Oxford University Press; 2007.
�Lynn J, Schuster J, Kabcenell A. Improving Care for the End-
of-Life, New York: Oxford University Press; 2000.
�Nelson J.E., Mulkerin C.M, Adams L.L, Pronovost P.J. Improving
Comfort and Communication in the ICU: a Practical new Tool
for Palliative Care Performance Measurement and feedback.
Quality and Safety in Health Care. 2006; 15:264-271
�Clarke E, Curtis JR, Luce J, Levy M, Danis M, Nelson J, Solomon
M for the Robert Wood Johnson Foundation Critical Care End-of-
Life Peer Workgroup Members. Quality Indicators for End-of-Life
Care in the Intensive Care Unit. Critical Care Medicine. 2003.

8
ICU Palliative Care
Goals
• improve palliative care in the ICU which includes easing pain and suffering for patients and families
• strengthen staff communication skills for addressing palliative care and end-of-life issues
• improve ICU infrastructure to support a strong palliative care program
Launched April 8, 2010…

9
The ICU Communication Bundle• Who is eligible?
– All ICU patients except:
• LOS <24 hours
• Expected ICU stay (i.e. post-op CABG)
• Boarding in ICU
• Psych or suicidal dx
• 10 evidenced-based quality metrics
– 6-Day 1 measures, 4-Day 3 measures
• Secondary outcome measures
– ICU mortality, ICU LOS, time to DNR
Communication BundleDay 1 measures1. Proxy decision-maker identified AND documented in medical record within 24 hours
2. Presence or absence of advance directive identified AND documented in medical record within 24 hours
3. CPR status addressed AND documented in
medical record within 24 hours

10
Communication BundleDay 1 measures – cont’d4. Pain assessment completed AND documented in medical record within 24 hours
5. Dyspnea assessment completed AND documented in medical record within 24 hours
6. ICU informational brochure provided to family AND documented in medical record within 24 hours
Communication BundleDay 3 measures7. Family meeting scheduled, occurred, and documented within 3 days
8. Patient prognosis discussed at the family meeting and documented
9. Patient goals discussed at the family meeting and documented
10. Need for spiritual care was evaluated, provided and documented within 3 days

11
Communication Bundle Aims
Aims:
- Achieve an overall compliance of 90% or > in the 6 Day 1 quality indicators
- Achieve an overall compliance of 90% or > in the 4 Day 3 quality indicators
Team Education and Collaborative Shared Learning
• Full day Learning Sessions q 6 mos
• Bi-monthly Coaching calls
• Bi-monthly Team Lead Forums
• Bi-monthly newsletters
• List serve

12
How have we progressed on our journey??
ResultsTotal charts reviewed –
April 2010 to Sept 2011
14,645
Patients analyzed (met criteria) 7,758 (53%)
patients excluded 6887 (47%)
Reason for exclusion 97% of exclusionswere for routine expected stay or <24 hour stay

13
Results
Hospital Size
<200 bed 18.1%
200-500 beds 31.5%
>500 bed 50.4%
Teaching status
Teaching status 77.6%
Non-teaching 22.4%
ICU Type
Medical 45.0%
Surgical 12.1%
Med-Surg 42.7%
Exclusion Types
Q3 2011 data preliminary

14
Day 1 and 3 Composite
* Q3 2011 data preliminary
Individual Process Measures
0
20
40
60
80
100
Q2 '10 Q3 '10 Q4 '10 Q1 '11 Q2 '11 Q3 '11
Proxy
Adv. Dir.
CPRStatus
Pain
Dyspnea
Brochure
FamilyMtg.
Prognosis
Goals
SpiritualCare
Improvement range = -1.8- 249%!
*Q3 2011 data preliminary
15
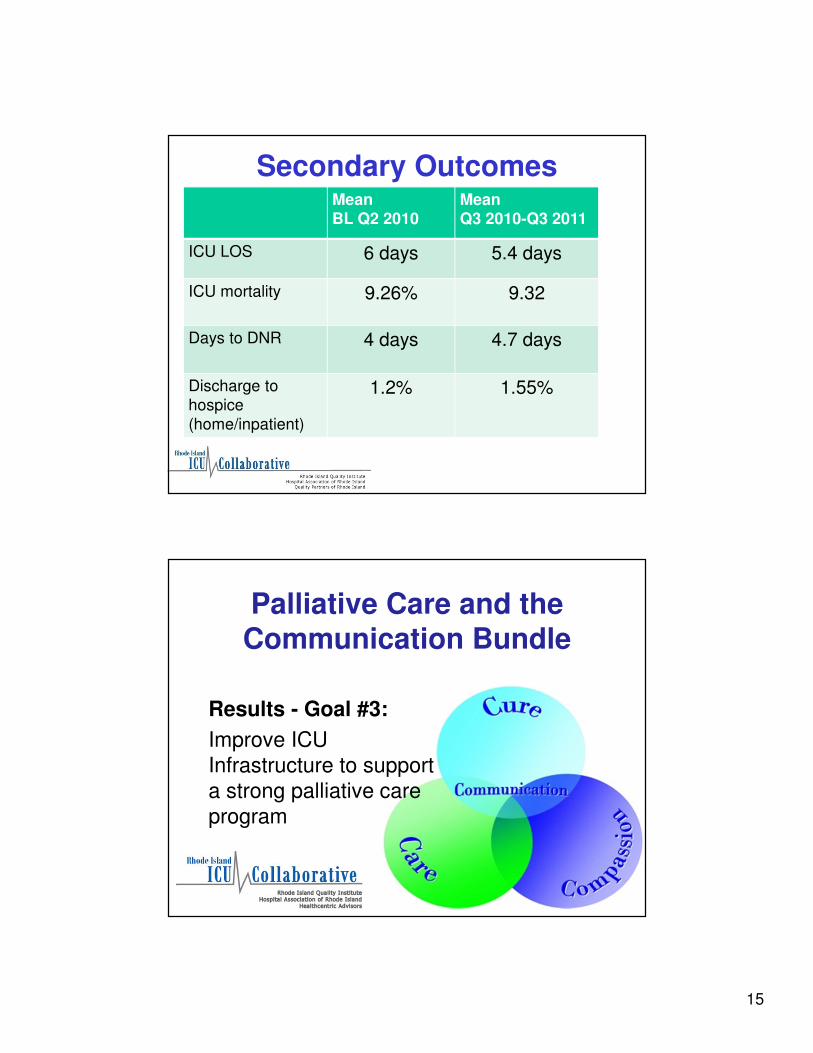
Secondary OutcomesMeanBL Q2 2010
MeanQ3 2010-Q3 2011
ICU LOS 6 days 5.4 days
ICU mortality 9.26% 9.32
Days to DNR 4 days 4.7 days
Discharge to
hospice
(home/inpatient)
1.2% 1.55%
Palliative Care and the Communication Bundle
Results - Goal #3:
Improve ICU
Infrastructure to support
a strong palliative care
program

16
ICU Pre and Post Launch Assessment
Measure % Pre % Post
Family Room 45 70
Format for family meeting 0 30
Protocol for scheduling meeting 12 30
ICU Brochure 75 100
Open visiting hours 70 77
Palliative care order sets 0 0
Palliative care team 35 62

17
Journey Challenges
Project Management Challenges• Physician engagement (surgeons)
• Sustaining staff engagement and energy
– Quality improvement burnout
• Timely unit data submission
• Competing demands on units
• Executive understanding and buy-in
• Misperceptions about palliative care
– Perception that this does not apply to those who are not
imminently dying

18
Staff Perceived Challenges
• Operational
– Lack of fmly mtg space
– 2 disciplines present (attending and resident does not qualify as is the opinion of some)
– w/e admissions with day 3 on Monday
– Staffing changes with residents
– Some ICUs with low “inclusion” numbers
– Physician buy-in – primarily surgeons
Staff Perceived Challenges
• Family meetings
– Spontaneous meetings with no planning
– Family lack of availability r/t work schedule
– Time constraints (i.e. nurses torn between caring for a sick patient or attending mtg)
– Meeting at bedside not perceived as family mtg by some

19
Staff Perceived Challenges• Documentation
– EMR-difficult to find previous fmly mtg notes
– Checklists helpful, but often lacks detail
– Drs struggle with documentation
– EMR implementation - additional time burden
– Disciplines present often missing in notes
– Confusion on “who” should document on family meeting
The Journey Continues!16 month transition period for the
RI ICU Collaborative
September, 2011 to December, 2012

20
Kudos to the RI Teams…Taking time Celebrate!
Summary• Using a multifaceted intervention for behavior
change, we were able to improve compliance with the bundled elements targeting improving communication with patients and families in a broad ICU population.
• This change in compliance was associated with unchanged overall mortality, length of stay, and time to DNR order.
• Work to sustain and improve the gains to date are on-going.

21
“To cure sometimes, to relieve often, to comfort always —
this is our work.”
Anonymous
QUESTIONS????
22
Thank You to Our Funders!!!
• Blue Cross Blue Shield of Rhode Island
• UnitedHealthcare of New England
• Neighborhood Health Plan of Rhode
Island





























