Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Improved Detection of Hypervascular Liver LesionsWith CAIPIRINHA–Dixon–TWIST–Volume-Interpolated
Breath-Hold Examination
Philipp M. Kazmierczak, MD* Daniel Theisen, MD* Kolja M. Thierfelder, MD* Wieland H. Sommer, MD*Maximilian F. Reiser, MD* Mike Notohamiprodjo, MD*† and Konstantin Nikolaou, MD*†
Objectives: The aim of this study was to assess the diagnostic performance of adynamic, multiphasic contrast-enhanced volume-interpolated sequence with ad-vanced parallel imaging techniques, Dixon fat saturation, and view sharing with5 hepatic arterial subphases for the detection of focal liver lesions.Materials andMethods: Twenty-four consecutive patients (13 females, 11males;mean [SD] age, 58 [15] years) with focal liver lesions were included in this pro-spective study. The examination was performed at a 3-T magnetic resonance im-aging system (MAGNETOM Skyra; Siemens Healthcare, Erlangen, Germany).Five dynamic arterial subphases with a temporal resolution of 2.6 seconds,starting 17 seconds after injection of the hepatobiliary contrast agent gadolin-ium ethoxybenzyl diethylenetriaminepentaacetic acid (Eovist; Bayer HealthCare,Leverkusen, Germany), were acquired using an accelerated parallel imagingvolume-interpolated sequence with view sharing (multiarterial controlled aliasingin parallel imaging results in higher acceleration–Dixon–time-resolved angiogra-phy with interleaved stochastic trajectories–volumetric interpolated breath-holdexamination [MA-CDT-VIBE]). The fourth of the 5 arterial acquisition phases(ie, at 24.8 seconds after the start of contrast agent injection) was consideredthe equivalent of a standard hepatic arterial phase (equivalent standard arterialphase [ESAP]). The diagnostic value of all 5 dynamic arterial phases for the de-tection of focal liver lesions, as compared with the single ESAP, was judged in 2independent consensus readings. The 2 consensus reading groups were blindedto each others' results. The complete, comprehensive multisequence magneticresonance imaging examination, including T1-weighted, T2-weighted, and mul-tiphasic contrast-enhanced sequences, served as the standard of reference forlesion detection.Results: Forty-six percent of the patients (11/24) had hypervascular lesions. In79 % of all patients (19/24), the best arterial parenchymal contrast of one of theMA-CDT-VIBE acquisition phases was considered better than that of the ESAP.In one third of all cases (8/24 for the first and 6/24 for the second consensus read-ing), MA-CDT-VIBE showed an improved lesion detection rate compared withESAP, especially in hypervascular lesions (4/11, representing 36 % of all patientswith hypervascular lesions). There was a high degree of interrater agreement be-tween the 2 consensus reading groups (the Cohen κ, 0.71–1.00; P < 0.001).Conclusions: Compared with a standard hepatic arterial phase, MA-CDT-VIBEwith 5 hepatic arterial subphases demonstrated greater diagnostic accuracy forthe detection of hypervascular focal liver lesions and provided a robust and opti-mized hepatic arterial acquisition phase.
Key Words: multiarterial liver MRI, focal liver lesions, advanced parallelimaging, CAIPIRINHA-Dixon-TWIST-VIBE
(Invest Radiol 2015;50: 153–160)
Received for publication August 20, 2014; and accepted for publication, after revi-sion, October 9, 2014.
From the *Department of Clinical Radiology, University Hospitals Munich, Munich;and †Department of Diagnostic and Interventional Radiology, University HospitalTuebingen, Tuebingen, Germany.
Conflicts of interest and sources of funding: none declared.Reprints: PhilippM.Kazmierczak,MD, Department of Clinical Radiology, University
Hospitals Munich, Marchioninistrasse 15, 81377 Munich, Germany. E-mail:[email protected].
Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved.ISSN: 0020-9996/15/5003–0153
Investigative Radiology • Volume 50, Number 3, March 2015
Copyright © 2015 Wolters Kluwer H
D ynamic magnetic resonance imaging (MRI) of the liver usingcontrast-enhanced volumetric 3-dimensional T1-weighted fat-
saturated gradient-recalled echo (T1w-3D-fs-GRE) sequences is con-sidered the standard of reference for the diagnostic workup of focal liverlesions.1,2 Sequences of T1w-3D-fs-GRE (vendor-specific names: liveracquisition with volume acceleration [LAVA], GE; T1 high-resolutionisotropic volume excitation [THRIVE], Philips; volumetric interpolatedbreath-hold examination [VIBE], Siemens) offer the 3-dimensional ac-quisition of the entire liver during a single breath-hold, enabling dynamic,multiphasicMRI examinations at a high temporal and spatial resolution.3
Although several techniques for the determination of the optimalscan delay for hepatic arterial phase imaging are available, adequatetiming remains challenging. Using fixed delays, the optimal hepatic ar-terial phase may be missed and focal lesions with predominant arterialenhancement may be obscured. Administration of a test bolus and real-time bolus tracking are more advanced methods4–6; however, these re-quire the application of additional contrast agent, an additional scan,as well as additional training, and these are not yet readily availableat every site. Furthermore, administration of the hepatobiliary contrastagent gadolinium ethoxybenzyl diethylenetriaminepentaacetic acid (Gd-EOB-DTPA) (Eovist; Bayer HealthCare, Leverkusen, Germany) requiresadaptation of the acquisition protocol with regard to a shortened boluslength owing to lower injection volume and relatively higher relaxivity.7
Advanced parallel imaging technique controlled aliasing in par-allel imaging results in higher acceleration (CAIPIRINHA) allows fora considerably accelerated acquisition with maintained signal-to-noiseratio as compared with established parallel imaging techniques suchas generalized autocalibrating partially parallel acquisition.3 In an earlyfeasibility study in a mixed patient cohort, Michaely et al8 were able toshow that the combination of VIBE imaging with CAIPIRINHA, viewsharing (time-resolved angiography with interleaved stochastic trajecto-ries [TWIST]), and Dixon fat saturation allowed for the robust acquisi-tion of multiple hepatic arterial subphases within a single breath-hold(multiarterial CAIPIRINHA-Dixon-TWIST VIBE [MA-CDT-VIBE]).
The aim of the study was to evaluate an accelerated acquisitiontechnique (MA-CDT-VIBE) with regard to the robustness of the hepaticarterial phase and its diagnostic accuracy for the detection of focal liverlesions at 3 T. We hypothesized that the use of CDT-VIBE with 5 he-patic arterial subphases allowed for a robust and optimized timing ofthe hepatic arterial phase and an improved detection of hypervascular liverlesions, as compared with a standard single arterial phase acquisition.
MATERIALS AND METHODS
PatientsThis prospective single-center study obtained institutional re-
view board approval. From June to November 2013, patients withknown or suspected focal liver lesions were included consecutively. Pa-tients not able to consent to the examination and patients with commonMRI contraindications (eg, cardiac pacemakers, known adverse eventsrelated to gadolinium chelates, and terminal renal failure as indicated bya glomerular filtration rate < 30 mL/min) were excluded from the pro-tocol. Furthermore, data sets of patients with no evidence of disease,
www.investigativeradiology.com 153
ealth, Inc. All rights reserved.

Kazmierczak et al Investigative Radiology • Volume 50, Number 3, March 2015
defined as the absence of benign ormalignant liver lesions, were excludedfrom data analysis. In total, data sets of 24 patients (13 females, 11 males;mean [SD] age, 58 [15] years) were included for image evaluation.
Magnetic Resonance ImagingA dedicated liver examination protocol using an abdominal 18-
channel body array was performed on a 3-TMRI system (MAGNETOMSkyra; Siemens Healthcare, Erlangen, Germany). The comprehensive,multiphasic MRI protocol included a dynamic T1w-3D-fs-GRE se-quence with arterial, portovenous, late dynamic, and hepatobiliaryphases as well as a single-shot turbo-spin echo sequence (T2 half-Fourier acquisition single-shot turbo spin-echo [T2 HASTE]). Scanswere performed using the hepatobiliary contrast agent Gd-EOB-DTPA(Eovist; Bayer HealthCare, Leverkusen, Germany) administeredat weight-adapted doses according to the manufacturer's instructions.Table 1 displays individual sequence parameters. The arterial phase ofthe routine dynamic contrast-enhanced liver examination was performedwith 5 hepatic arterial subphases (MA-CDT-VIBE), whereas the othersequences including the portovenous, the late dynamic, and thehepatobiliary phases were acquired as single-phase CDT-VIBE. TheMA-CDT-VIBE allowed for the acquisition of 5 dynamic arterialsubphases with a temporal resolution of 2.6 seconds, starting 17 secondsafter manual contrast injection.
Image EvaluationTwo independent consensus readings were performed for image
evaluation. In each consensus reading session, 2 experienced radiolo-gists judged the diagnostic value of the 5 dynamic arterial phases forthe detection of focal liver lesions, comparing them with the standard
TABLE 1. Sequence Parameters of the Comprehensive MRI Protocol
ParameterMA-CDT-VIBE
CDT-VIBEPortovenous Phase
Subphases 5 1TR/TE1, milliseconds 3.83/1.23 3.83/1.23Flip angle, degrees 9 9FOV, mm 380 380FOV phase, % 81.3 81.3Base resolution, mm 288 288Phase resolution, % 75 75ST, mm 3 3Voxel size, mm3 1.3 � 1.3 � 3 1.3 � 1.3 � 3Slice number 72 72Temporal resolution, s 2.6 —PPA CAIPIRINHA 4 CAIPIRINHA 4TA, s 19 8.9Respiratory control Breath-hold Breath-holdFS Dixon DixonBandwidth, hertz per pixel 1160 1160Phase oversampling, % 0 0Slice oversampling, % 33.3 33.3Frames 5 1TWIST k-center, % 20 20TWIST k-periphery, % 25 25
CAIPIRINHA indicates controlled aliasing in parallel imaging results in higheautocalibrating partially parallel acquisition; CDT, CAIPIRINHA-Dixon-TWIST; HMRI, magnetic resonance imaging; PPA, partially parallel acquisition; ST, slice thicresolved angiography with stochastic trajectories; VIBE, volume-interpolated breath-
154 www.investigativeradiology.com
Copyright © 2015 Wolters Kluwer H
hepatic arterial phase. The comprehensive, multiparametric, multi-sequence MRI protocol served as the standard of reference for the pres-ence of any hepatic lesions. The 2 consensus reading groups wereblinded to each others' results. From the 4 Dixon data sets (ie, in-phase, opposed-phase, water-only, fat-only), only thewater-only imageswere evaluated. For comparison purposes with the standard examina-tion protocol, the fourth of the 5 hepatic arterial subphases (acquiredat 24.8 seconds after the start of contrast injection) was considered theequivalent standard arterial phase (ESAP), that is, the standard singlearterial hepatic phase. Single sequences were read with regard to thenumber of liver lesions detected and were compared with the T2HASTE as well as with the portovenous, late dynamic, and the hepa-tobiliary phases, which, in combination, served as the diagnostic crite-rion standard for the detection of any liver lesions. The readers notedwhether they were able to detect all (yes, 1) liver lesions in any or allof the 5 multiarterial phases or the ESAP, or not (no, 2). In addition, le-sions were judged as hypervascular if clear hyperintense lesion contrastenhancement in at least one of the MA-CDT-VIBE subphases was ob-served, and the number of hypervascular lesions per patient and for theentire cohort was noted. Furthermore, the MA-CDT-VIBE subphasewith the best visual parenchymal contrast was determined. If any le-sions were detected in at least one of the MA-CDT-VIBE subphasesbut not in the ESAP, MA-CDT-VIBE was considered to be of higherdiagnostic value as compared with the standard hepatic arterial phase.
Statistical AnalysisStatistical analysis was performed using SPSS 22 (IBM Corp,
Armonk, NY). Interrater agreement between the 2 consensus readingswas calculated using the Cohen κ.
CDT-VIBELate Dynamic Phase
CDT-VIBEHepatobiliary Phase T2 HASTE
1 1 13.83/1.23 3.97/1.29 2000.00/91.00
9 9 160380 380 38081.3 81.3 78.1288 320 32075 85 803 3 5
1.3 � 1.3 � 3 1.2 � 1.2 � 3 1.2 � 1.2 � 572 72 36— — —
CAIPIRINHA 4 CAIPIRINHA 4 GRAPPA 28.9 20 180
Breath-hold Breath-hold TriggeredDixon Dixon —1160 1040 710
0 30 033.3 37.5 —
1 1 120 20 —25 25 —
r acceleration; FOV, field of view; FS, fat saturation; GRAPPA, generalizedASTE, half-Fourier acquisition single-shot turbo spin-echo; MA, multiarterial;kness; TA, acquisition time; TE, echo time; TR, repetition time; TWIST, time-hold examination.
© 2014 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

Investigative Radiology • Volume 50, Number 3, March 2015 Multiarterial MRI for Liver Lesion Detection
RESULTSIf not indicated otherwise, results refer to both consensus
readings.
Technical Success and Prevalence of Liver LesionsEvery examination was considered diagnostic, and all 24 pa-
tients showed liver lesions in imaging.Nine patients had primary liver lesions and 6 patients presented
withmalignant tumors (hepatocellular carcinoma [HCC], n = 3; cholangio-cellular carcinoma [CCC], n = 1; biliary cystadenocarcinoma, n = 1;mixed hepatocellular-CCC, n = 1). In total, 7 malignant lesions wereobserved in 5 patients, and 1 patient showed disseminated HCC (de-fined as >10 lesions). Eight benign lesions were detected in 3 patients(focal nodular hyperplasia [FNH], n = 2, with 1 hepatic adenoma foundsimultaneously; hemangioma, n = 1). Metastatic disease of the liver wasdetected in 15 patients, with 7 patients presenting with disseminatedmetastases (>10 liver metastases).
Forty-six percent (n = 11) of all lesions appeared hypervascular(HCC, FNH, metastases from neuroendocrine tumor and pancre-atic cancer, each n = 2; metastases from thyroid and breast canceras well as mixed hepatocellular-cholangiocellular carcinoma, eachn = 1). Table 2 presents detailed information on patient andlesion characteristics (Table 2).
Consensus Reading ResultsIn approximately one third of the cases, MA-CDT-VIBE allowed
for an improved lesion detection compared with ESAP. Detailed con-sensus reading results are provided in Table 3.
TABLE 2. Patient Characteristics
Patient No. Sex Age, y Type of Liver L
1 F 62 Metastatic breas2 M 61 HCC3 M 70 Hemangiom4 F 53 FNH and ade5 M 65 Metastatic colorecta6 F 65 CCC7 M 70 Metastatic esophag8 F 66 Metastatic breas9 M 60 Metastatic pancrea10 F 50 Metastatic thyroi11 F 66 Metastatic N12 F 72 Metastatic breas13 F 48 Metastatic N14 M 50 HCC15 M 88 Metastatic colorecta16 M 63 Metastatic N17 F 30 Metastatic breas18 M 49 Metastatic pancrea19 F 76 Biliary cystadenoc20 M 35 Metastatic N21 M 58 HCC22 F 69 Metastatic pancrea23 F 31 Mixed hepatocellular/cholang24 F 25 FNH
*Defined as contrast enhancement on at least one of the MA-CDT-VIBE subphas
CCC indicates cholangiocellular carcinoma; F, female; FNH, focal nodular hyperp
© 2014 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2015 Wolters Kluwer H
Lesion Detection and Interrater AgreementThe multiparametric, multisequence MRI examination protocol
(T2 HASTE, T1-weighted contrast-enhanced portovenous/late dynamic/hepatobiliary phase) served as the standard of reference for lesion de-tection. Figures 1 to 4 provide examples of the dynamic, multiphasicacquisition using MA-CDT-VIBE. Evaluating the 5 MA-CDT-VIBEsubphases alone, the readers were able to detect all liver lesions in70% of the patients (first reading, 17/24) and 79% (second reading,19/24), respectively. Excluding patients with nonhypervascular lesions,the detection rate improved to 82% (n = 9/11) and 100% (n = 11/11), re-spectively. In 33% (8 patients) and 25% (second reading, n = 6), MA-CDT-VIBE had an improved lesion detection rate compared with ESAP.Of these patients, 50% (first reading, n = 4) and 75% (second reading,n = 6) had hypervascular liver lesions (FNH, HCC, metastatic neuroen-docrine tumor, and pancreatic cancer, each n = 1), representing 36% ofall patients with hypervascular liver lesions. There was a high degreeof interrater agreement regarding the diagnostic advantage of MA-CDT-VIBE (Cohen κ, 0.8; P < 0.001) and for the evaluation ofthe comprehensive, multiphasic imaging protocol (Cohen κ, 0.71–1.00; P < 0.001). Detailed consensus reading results are provided inTable 3. Figures 3 and 4 show the clinical cases in which MA-CDT-VIBE proved to be advantageous over ESAP.
Parenchymal ContrastTheMA-CDT-VIBE subphase 5/5 demonstrated the best arterial
lesion-to-parenchyma contrast in 79% (n = 19) of all cases, whereassubphase 4/5 (ESAP) showed the best arterial lesion-to-parenchymacontrast in 21% (n = 5) (Table 3).
esions Hypervascular* No. Liver Lesions
t cancer No >10Yes >10
a No 1noma Yes 6l carcinoma No >10
No 3eal cancer No 1t cancer No 1tic cancer No 5d cancer Yes >10ET No 3t cancer No >10ET Yes >10
Yes 1l carcinoma No 3ET Yes >10t cancer Yes 1tic cancer Yes 2arcinoma No 1ET No >10
No 1tic cancer Yes 4iocellular carcinoma Yes 1
Yes 1
es.
lasia; HCC, hepatocellular carcinoma; M, male; NET, neuroendocrine tumor.
www.investigativeradiology.com 155
ealth, Inc. All rights reserved.

TABLE
3.Con
sensus
Read
ingRe
sults
Patient
No.
T2HAST
EPV
LD
HB
ESA
P*
BestCon
trastMA-C
DT-V
IBESu
bpha
se(x/5)
BestCon
trastPha
seOverall
Hyp
ervascular
Advan
tage
MA-C
DT-V
IBE
11
22
12
2(5/5)
HB
No
No
1*1
22
12
2(5/5)
HB
No
No
21
21
12
2(4/5)
HB
Yes
No
2*2
22
12
2(4/5)
HB
Yes
No
31
22
12
1(5/5)
HB
No
Yes
3*1
22
12
1(5/5)
HB
No
Yes
41
11
22
1(5/5)
PVYes
Yes
4*1
11
22
1(5/5)
MA-CDT-VIBE
Yes
Yes
51
11
12
2(5/5)
HB
No
No
5*1
11
12
2(5/5)
HB
No
No
61
11
11
1(5/5)
PVNo
No
6*1
11
11
1(5/5)
PVNo
No
71
11
12
2(5/5)
PVNo
No
7*1
11
12
2(5/5)
PVNo
No
81
11
12
1(5/5)
HB
No
Yes
8*1
11
12
1(5/5)
HB
No
Yes
91
12
12
1(5/5)
HB
No
Yes
9*1
12
11
1(5/5)
HB
No
No
102
22
11
1(5/5)
MA-CDT-VIBE
Yes
No
10*
22
21
11(5/5)
MA-CDT-VIBE
Yes
No
111
11
12
2(5/5)
HB
No
No
11*
11
11
11(5/5)
HB
No
No
121
12
11
1(5/5)
HB
No
No
12*
11
11
11(5/5)
HB
No
No
131
11
11
1(4/5)
MA-CDT-VIBE
Yes
No
13*
11
11
11(4/5)
HB
Yes
No
142
11
12
1(5/5)
PVYes
Yes
14*
21
11
21(5/5)
HB
Yes
Yes
152
11
12
1(5/5)
HB
No
Yes
15*
21
11
11(5/5)
HB
No
No
161
11
12
1(5/5)
HB
Yes
Yes
16*
11
11
21(5/5)
T2HAST
EYes
Yes
172
11
11
1(4/5)
HB
Yes
No
17*
11
11
11(4/5)
HB
Yes
No
181
22
12
1(5/5)
HB
Yes
Yes
18*
12
21
21(5/5)
HB
Yes
Yes
191
11
11
1(5/5)
T2HAST
ENo
No
19*
11
11
11(5/5)
T2HAST
ENo
No
202
22
12
2(5/5)
HB
No
No
20*
22
21
22(5/5)
HB
No
No
211
11
11
1(5/5)
MA-CDT-VIBE
No
No
21*
11
11
11(5/5)
MA-CDT-VIBE
No
No
221
22
12
2(5/5)
HB
Yes
No
Kazmierczak et al Investigative Radiology • Volume 50, Number 3, March 2015
156 www.investigativeradiology.com © 2014 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.

22*
11
11
21(5/5)
HB
Yes
No
231
11
11
1(5/5)
MA-CDT-VIBE
Yes
No
23*
11
11
11(5/5)
MA-CDT-VIBE
Yes
No
241
11
11
1(4/5)
MA-CDT-VIBE
Yes
No
24*
11
11
11(4/5)
MA-CDT-VIBE
Yes
No
κ†0.75
0.90
0.71
1.00
0.75
0.90
(0.90)
0.71
1.00
0.80
Twoindependentconsensus
readings
judged
whetheralllesions
couldbe
detected
(1denotesyes;2,no)inT2HAST
E,the
portovenous/latedynamic/hepatobiliaryphase,theequivalentstandard
arterialphase(ESA
P,MA-
CDT-VIBEsubphase
considered
equivalent
tothestandard
hepatic
arterialphase),ortheMA-CDT-VIBEsubphase
with
thebestlesion-to-parenchymacontrast(subphasex/5indicatedin
brackets).Interrater
agreem
entw
ascalculated
usingtheCohen
κ.
*Secondconsensusreading.
†P<0.001.
CDTindicatesCAIPIRIN
HA-D
ixon-TWIST;E
SAP,equivalentstandardarterialphase;HASTE,half-Fourieracquisitio
nsingle-shotturbo
spin-echo;HB,hepatobiliaryphase;LD,latedynamicphase;MA,m
ultiarterial;PV
,portovenousphase;TWIST,
time-resolved
angiographywith
stochastictrajectories;V
IBE,volum
e-interpolated
breath-holdexam
ination.
Investigative Radiology • Volume 50, Number 3, March 2015 Multiarterial MRI for Liver Lesion Detection
© 2014 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2015 Wolters Kluwer H
DISCUSSIONThe CDT-VIBE is a novel, contrast-enhanced T1w-3D-fs-GRE
sequence that allows for the acquisition of multiple hepatic arterialsubphases during a single breath-hold (MA-CDT-VIBE).8,9 The MA-CDT-VIBE facilitated the timing of the arterial phase and generatedadditional dynamic information on the vascular status of focal liver le-sions. In the present study, MA-CDT-VIBE showed an improved lesiondetection rate as compared with the single, standard hepatic arterialphase, especially in patients with hypervascular liver lesions.
Optimized Contrast Timing and HepaticArterial Enhancement
An optimal hepatic arterial dominant phase in at least one of theMA-CDT-VIBE subphases could be obtained in all cases. Therefore,our results suggest that the use of MA-CDT-VIBE allows for an opti-mized timing of the hepatic arterial phase, even in a fixed-delay imagingapproach.
This is consistent with the most recent retrospective data demon-strating the potential of a CAIPIRINHA-Dixon-VIBE without TWISTview sharing for the reduction of motion-induced artifacts acquiring 3hepatic arterial subphases, although at a relatively low temporal reso-lution of 7.5 seconds, as compared with 2.6 seconds in the presentstudy.10 Mori et al11 conducted another trial to evaluate MRI with sev-eral hepatic arterial subphases. The authors examined 31 patients withHCC on a 1.5-T magnetic resonance scanner, using a T1-weighted se-quence with parallel imaging (sensitivity encoding [SENSE], accelera-tion factor R = 2), acquiring 3 hepatic arterial subphases at a temporalresolution of 8.4 seconds. From these 3 subphases, they identified themiddle subphase, acquired at 8.4 seconds after peak aortic enhance-ment, as optimal for HCC detection. However, the acquisition was per-formed with a slice thickness of 8 to 9 mm, potentially obscuring smalllesions owing to partial-volume effects. On the contrary, MA-CDT-VIBE allows for a slice thickness as thin as 3 mm.
Currently, several technical approaches for an optimal timing ofthe hepatic arterial phase are available, for example, scanning at fixedtime points or individually tailored solutions including a prescan testbolus or real-time bolus tracking.6 For the latter, however, no consensuson what vascular reference point to use has been reached. For instance,breath-hold command and data acquisition can be started as soon as thecontrast bolus reaches the aortic arch, the descending aorta, or the ab-dominal aorta.5,6,12 In addition, real-time bolus tracking requires specialtraining of the radiology technicians and is yet not readily available atevery site. Therefore, fixed scan delay techniques can be consideredmore user-friendly and potentially more robust.
In general, it is assumed that the proximal abdominal aorta en-hances at 17 seconds and the common hepatic artery at approximately20 seconds after cubital intravenous contrast agent injection.13,14 How-ever, several studies reported a significant variability of hepatic arterialenhancement in individual patients.6,15 Sharma et al6 performed fluoro-scopic T1-weighted scans in 100 consecutive patients, observing en-hancement of the abdominal aorta at the level of the celiac trunk at18.2 ± 4.1 seconds, with a range of 12 to 31 seconds. These resultsare in accordance with a study by Van Beers et al,15 who investigateda population of 47 patients with hypervascular liver tumors (FNH,HCC, adenoma) and found a maximum lesion contrast-to-noise ratioat 26.5 seconds after contrast injection.
To conclude, these data underline the need for and the potentialbenefit of an optimally timed hepatic arterial phase achieved by amultiarterial acquisition at a high temporal resolution.
Diagnostic Accuracy and Lesion DetectionMichaely et al8 evaluated the clinical robustness and value of
CDT-VIBE with gadolinium tetra-azacyclododecane tetraacetic acid in47 patientswith various intra-abdominalmalignancies, including hepatic,
www.investigativeradiology.com 157
ealth, Inc. All rights reserved.

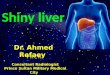
FIGURE 2. Hepatic arterial contrast dynamics of histologically confirmed mixed hepatocellular-cholangiocellular carcinoma. The MA-CDT-VIBEsubphases at 17.0 seconds (A), 19.6 seconds (B), 22.2 seconds (C), 24.8 seconds (D, ESAP), and 27.4 seconds (E) after intravenous administration ofGd-EOB-DTPA. Note the dynamic arterial contrast enhancement of the right liver lobe tumor (arrow).
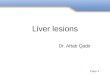
FIGURE 1. Hepatic arterial contrast dynamics of liver metastases from primary thyroid carcinoma. The MA-CDT-VIBE subphases at 17.0 seconds (A),19.6 seconds (B), 22.2 seconds (C), 24.8 seconds (D, ESAP), and 27.4 seconds (E) after intravenous administration of Gd-EOB-DTPA. Note the earlyhepatic arterial enhancement of the lesions in segments VII/VIII (black pointed arrow) and IVa (white pointed arrow), beginning 19.6 seconds aftercontrast injection (B).
FIGURE 3. Diagnostic advantage of MA-CDT-VIBE in a female patient. TheMA-CDT-VIBE subphases at 17.0 seconds (A), 19.6 seconds (B), 22.2 seconds(C), 24.8 seconds (D, ESAP), and 27.4 seconds (E) after intravenous administration of Gd-EOB-DTPA. Note the small lesion in segment II/IVa (E, whitepointed arrow),which is only detected in the fifth of the 5MA-CDT-VIBE subphases at 27.4 seconds after contrast injection andwould havebeenmissed inthe ESAP (D). This finding is consistent with data in the literature, which state that peak enhancement of hypervascular lesions such as FNH is at 26.5seconds after intravenous contrast agent injection.15 Histolopathological analysis confirmed the diagnosis of multifocal FNH.
Kazmierczak et al Investigative Radiology • Volume 50, Number 3, March 2015
pancreatic, and renal lesions. Thirteen of these 47 patients had le-sions within the liver, and hypervascular lesions were not specificallyassessed. In the present study, we focused on the detection of focal liverlesions using the hepatocyte-specific contrast agent Gd-EOB-DTPA.Adding a steady-state, hepatobiliary phase to the comprehensive liverimaging protocol, Gd-EOB-DTPA has been shown to improve detec-tion of focal solid hepatic lesions.16 However, the timing of thehepatic-arterial phase in Gd-EOB-DTPA–enhanced examinations withfixed delay is challenging because only half of the contrast volumeand dose is used compared with Gd-DTPA.4 Accordingly, Zech et al7
investigated different injection and dose regimens of Gd-EOB-DTPAin an animal model and concluded that bolus stretching by a lower in-jection rate compensated for the lower injection volume, maintaininga robust hepatic arterial phase. TheMA-CDT-VIBEwas predominantlyadvantageous for the detection of hypervascular lesions, such as HCC,
158 www.investigativeradiology.com
Copyright © 2015 Wolters Kluwer H
FNH, and hypervascular metastases, and thus may potentially detectadditional hypervascular lesions that could be missed in a single, stan-dard hepatic arterial phase.
Potential Clinical Applications of MA-CDT-VIBEMost eminently in the setting of presurgical planning and
pretransplant evaluation, it is essential not to miss any HCC nodules be-cause correct patient assignment according to the Milan Criteria is piv-otal for therapy decision.17,18 Likewise, the use of MA-CDT-VIBEmayhelp to detect liver metastases that demonstrate only discrete enhance-ment, again influencing and guiding the various therapeutic decisionsand options.19 Obviously, complete detection of all malignant lesionsis of headmost importance for the correct staging of patients with can-cer using established clinical tumor response criteria such as the mod-ified Response Evaluation Criteria in Solid Tumors (mRECIST) and
© 2014 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

FIGURE 4. Diagnostic advantage of MA-CDT-VIBE in a hypovascular type of lesion (pancreatic cancer metastasis). The MA-CDT-VIBE subphases at 17.0seconds (A), 19.6 seconds (B), 22.2 seconds (C), 24.8 seconds (D, ESAP), and 27.4 seconds (E) after intravenous administration of Gd-EOB-DTPA. Notethe small hypovascular lesion in segment V (E, black pointed arrow) showing subtle rim enhancement in the fifth of the 5MA-CDT-VIBE subphases at 27.4seconds after contrast injection, which would have been missed in the ESAP (D). In addition, note the subtle respiratory motion artifacts occurring in thelater arterial phases (D, E), which do not impair the diagnostic quality of the scan.
Investigative Radiology • Volume 50, Number 3, March 2015 Multiarterial MRI for Liver Lesion Detection
therefore bears direct impact on clinical decision making.20 FormRECIST in HCC, the longest diameter of any viable HCC lesion isassessed, with viability being defined as contrast enhancement duringthe arterial phase. Hence, a precise timing of the hepatic-arterial phaseis even more important for an adequate response evaluation accordingto mRECIST.21
In addition, the use of MA-CDT-VIBE may involve a semiquan-titative or quantitative evaluation of lesion enhancement (ie, lesion per-fusion) over time, using dedicated methods for signal-to-noise ratiocalculations.22 Quantitative assessment, if needed in combination withmethods for breath correction, could potentially play a role in thefollow-up of hypervascular lesions, for example, HCC after selective in-ternal radiation therapy.
Respiratory Motion ArtifactsIn the present cohort, marginal respiratory motion artifacts were
observed in 4 patients, particularly during the later phases of themultiarterial acquisition (subphases 4/5 and 5/5). However, the diagnos-tic quality of the scans was not affected because the artifacts were onlymarginal and at least 1 arterial subphase in each of these cases prove tobe artifact-free. Figure 4 shows marginal respiratory motion artifacts insubphases 4/5 and 5/5.
Despite featuring a lower temporal and spatial resolution,CAIPRINHA-Dixon-VIBEwithout TWIST view sharing may be supe-rior to CDT-VIBE with regard to respiratory motion artifacts.10 As forall keyhole techniques, a complete k-space readout is only performedduring the first acquisition of the TWIST sequence.23 If breath-inducedmotion occurs during the initial readout, the following acquisitions willbe impaired, resulting in reduced image quality. Therefore, applicabilityof keyhole view-sharing techniques may be limited in uncooperativepatients. However, we did not observe any severe respiratory motionartifacts in the present study.
Because particularly the late MA-CDT-VIBE subphases dem-onstrated to be advantageous for lesion detection, it can be argued thatthe acquisition of additional subphases would increase the diagnosticperformance. Appending additional hepatic arterial subphases is techni-cally feasible, as shownbyMichaely et al,8 who acquired 14 3-dimensionaldata sets with a temporal resolution of 2.1 seconds. However, prolongedbreath-hold intervals bear the risk for respiratory motion artifacts in thelate arterial phase and the following portovenous and late dynamicphases, thus potentially decreasing the diagnostic performance of thecomprehensive, multisequence imaging protocol. From our experience,most patients with liver disease discover difficulty in maintaining abreath-hold for half a minute. In the present study, a breath-hold intervalof 19 seconds was considered a reasonable compromise with regard tothe diagnostic quality of the complete examination protocol as well asto the number and temporal resolution of the hepatic arterial phases.
Finally, a sound compromise has to be found between the neces-sary number of hepatic arterial phases and the number of images acquired,
© 2014 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2015 Wolters Kluwer H
concerning data handling and data storing. This refers to reporting andreading of several additional data sets as well as the option for a quan-titative evaluation of time-resolved MA-CDT-VIBE data sets. Theseissues pose some challenges for any picture archiving and communi-cation systems and may require additional dedicated postprocessingsoftware.
LimitationsThere are several limitations to our study. First of all, the fourth
of 5 arterial subphases was considered the equivalent of a single, stan-dard hepatic arterial phase. Therefore, the diagnostic value of MA-CDT-VIBE was assessed through internal validation. However, com-parison with an additional arterial standard VIBE sequence would ne-cessitate a second MRI examination with an additional administrationof contrast media. Second, the reproducibility and intraindividual vari-ability were not assessed in this study. It remains to be elucidated howlesions appear in repeated scans and how intraindividual variabilitycompares with the standard imaging protocol. Third, lesions of differenthistologic origin were evaluated in this study. Focusing on a single typeof liver lesion, for example, HCC, may lead to a better understanding ofthe diagnostic performance of MA-CDT-VIBE. Particularly, the detec-tion of small hypervascular type of lesions, for example, small HCCnodules or pre-HCC lesions less than 1 cm, may benefit from multi-arterial acquisition.
ConclusionsIn conclusion, MA-CDT-VIBE allowed for high temporal and
spatial resolution of dynamic acquisition of the liver, with 5 hepatic ar-terial subphases being acquired during a single breath-hold. The use ofMA-CDT-VIBE with 5 hepatic arterial subphases allowed for an op-timized and robust timing of the hepatic arterial phase and improvedthe detection and differential diagnosis of hypervascular focal liverlesions.
ACKNOWLEDGMENTSThe authors thank Wilhelm Horger and Dominik Nickel from
Siemens Healthcare for providing the CDT-VIBE sequence and for theirtechnical support and the joint optimization of this new application.
REFERENCES
1. Fowler KJ, Brown JJ, Narra VR. Magnetic resonance imaging of focal liver le-sions: approach to imaging diagnosis. Hepatology. 2011;54:2227–2237.
2. Elsayes KM, Narra VR, Yin Y, et al. Focal hepatic lesions: diagnostic value of en-hancement pattern approach with contrast-enhanced 3D gradient-echo MR imag-ing. Radiographics. 2005;25:1299–1320.
3. Riffel P, Attenberger UI, Kannengiesser S, et al. Highly accelerated T1-weightedabdominal imaging using 2-dimensional controlled aliasing in parallel imagingresults in higher acceleration: a comparison with generalized autocalibrating par-tially parallel acquisitions parallel imaging. Invest Radiol. 2013;48:554–561.
www.investigativeradiology.com 159
ealth, Inc. All rights reserved.

Kazmierczak et al Investigative Radiology • Volume 50, Number 3, March 2015
4. Nakamura S, Nakaura T, Kidoh M, et al. Timing of the hepatic arterial phase atGd-EOB-DTPA-enhanced hepatic dynamic MRI: comparison of the test-injectionand the fixed-time delay method. J Magn Reson Imaging. 2013;38:548–554.
5. Sharma P, KalbB, KitajimaHD, et al. Optimization of single injection liver arterialphase gadolinium enhanced MRI using bolus track real-time imaging. J MagnReson Imaging. 2011;33:110–118.
6. Sharma P, Kitajima HD, Kalb B, et al. Gadolinium-enhanced imaging of livertumors and manifestations of hepatitis: pharmacodynamic and technical consider-ations. Top Magn Reson Imaging. 2009;20:71–78.
7. ZechCJ, Vos B, Nordell A, et al. Vascular enhancement in early dynamic liverMRimaging in an animal model: comparison of two injection regimen and two differ-ent doses Gd-EOB-DTPA (gadoxetic acid) with standard Gd-DTPA. InvestRadiol. 2009;44:305–310.
8. Michaely HJ, Morelli JN, Budjan J, et al. CAIPIRINHA-Dixon-TWIST (CDT)-volume-interpolated breath-hold examination (VIBE): a new technique for fasttime-resolved dynamic 3-dimensional imaging of the abdomen with high spatialresolution. Invest Radiol. 2013;48:590–597.
9. Budjan J, Ong M, Riffel P, et al. CAIPIRINHA-Dixon-TWIST (CDT)-volume-interpolated breath-hold examination (VIBE) for dynamic liver imaging: Compar-ison of gadoterate meglumine, gadobutrol and gadoxetic acid. Eur J Radiol. 2014;83:2007–2012.
10. Pietryga JA, Burke LM, Marin D, et al. Respiratory motion artifact affecting he-patic arterial phase imaging with gadoxetate disodium: examination recovery witha multiple arterial phase acquisition. Radiology. 2014;271:426–434.
11. Mori K, Yoshioka H, Takahashi N, et al. Triple arterial phase dynamic MRI withsensitivity encoding for hypervascular hepatocellular carcinoma: comparison ofthe diagnostic accuracy among the early, middle, late, and whole triple arterialphase imaging. AJR Am J Roentgenol. 2005;184:63–69.
12. Park YS, Hee Lee C, Kim IS, et al. Usefulness of controlled aliasing in parallel im-aging results in higher acceleration in gadoxetic acid-enhanced liver magnetic reso-nance imaging to clarify the hepatic arterial phase. Invest Radiol. 2014;49:183–188.
160 www.investigativeradiology.com
Copyright © 2015 Wolters Kluwer H
13. Ohtomo K, Itai Y, Yoshikawa K, et al. Hepatic tumors: dynamic MR imaging.Radiology. 1987;163:27–31.
14. Earls JP, Rofsky NM, DeCorato DR, et al. Hepatic arterial-phase dynamicgadolinium-enhanced MR imaging: optimization with a test examination and apower injector. Radiology. 1997;202:268–273.
15. Van Beers BE, Materne R, Lacrosse M, et al. MR imaging of hypervascular livertumors: timing optimization during the arterial phase. J Magn Reson Imaging.1999;9:562–567.
16. HaimerlM,WachtlerM, Platzek I, et al. Added value ofGd-EOB-DTPA- enhancedhepatobiliary phase MR imaging in evaluation of focal solid hepatic lesions.BMC Med Imaging. 2013;13:41.
17. Wong RJ, Devaki P, Nguyen L, et al. Increased long-term survival among patientswith hepatocellular carcinoma after implementation of model for end-stage liverdisease score. Clin Gastroenterol Hepatol. 2014;12:1534–1540.
18. Raza A, Sood GK. Hepatocellular carcinoma review: current treatment, andevidence-based medicine. World J Gastroenterol. 2014;20:4115–4127.
19. Namasivayam S, Martin DR, Saini S. Imaging of liver metastases: MRI. CancerImaging. 2007;7:2–9.
20. Fournier L, Ammari S, Thiam R, et al. Imaging criteria for assessing tumour re-sponse: RECIST, mRECIST, Cheson. Diagn Interv Imaging. 2014;95:689–703.
21. Kim DJ, Clark PJ, Heimbach J, et al. Recurrence of hepatocellular carcinoma: im-portance of mRECIST response to chemoembolization and tumor size. Am JTransplant. 2014;14:1383–1390.
22. Wiens CN, Kisch SJ,Willig-Onwuachi JD, et al. Computationally rapid method ofestimating signal-to-noise ratio for phased array image reconstructions. MagnReson Med. 2011;66:1192–1197.
23. Song T, Laine AF, Chen Q, et al. Optimal k-space sampling for dynamic contrast-enhanced MRI with an application to MR renography. Magn Reson Med. 2009;61:1242–1248.
© 2014 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.