Embed Size (px)
Citation preview
IMPORTANCE OF DATA EVIDENCE FOR PATIENT VALUE AND HEALTH
OUTCOMES BASED APPROACH
EM-11567
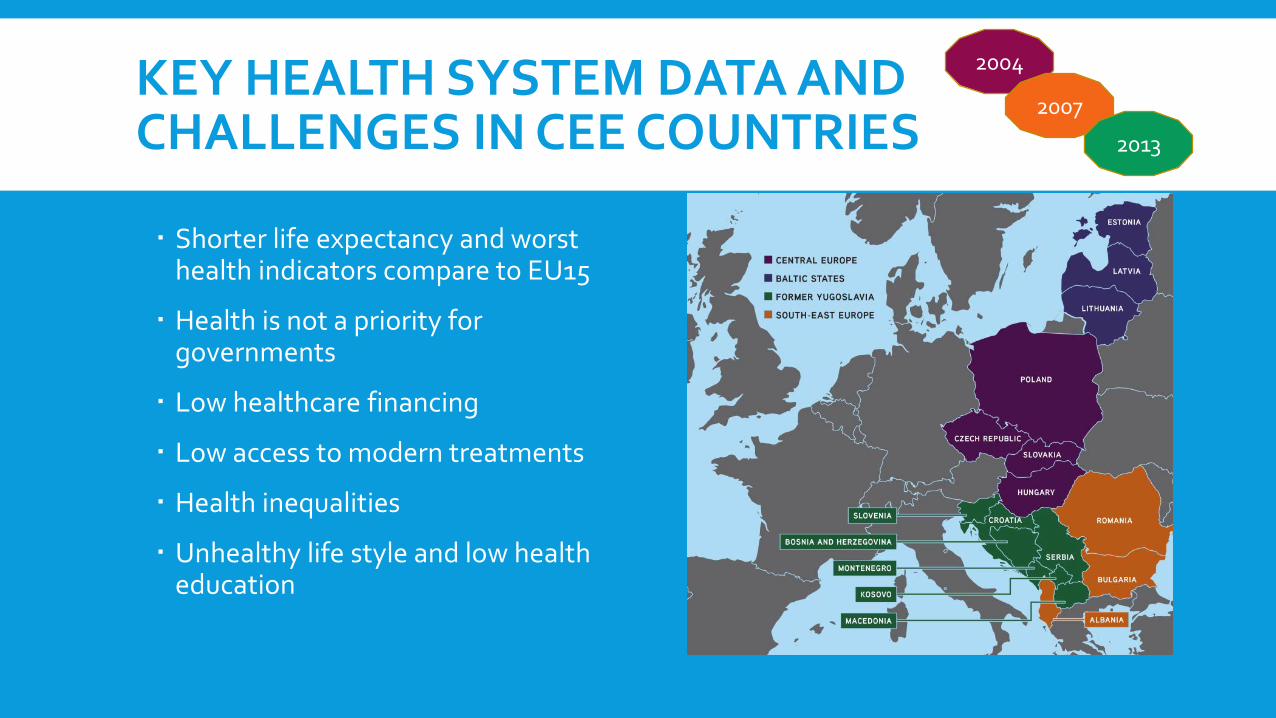
KEY HEALTH SYSTEM DATA AND CHALLENGES IN CEE COUNTRIES
Shorter life expectancy and worsthealth indicators compare to EU15
Health is not a priority for governments
Low healthcare financing
Low access to modern treatments
Health inequalities
Unhealthy life style and low healtheducation
2004
2007
2013
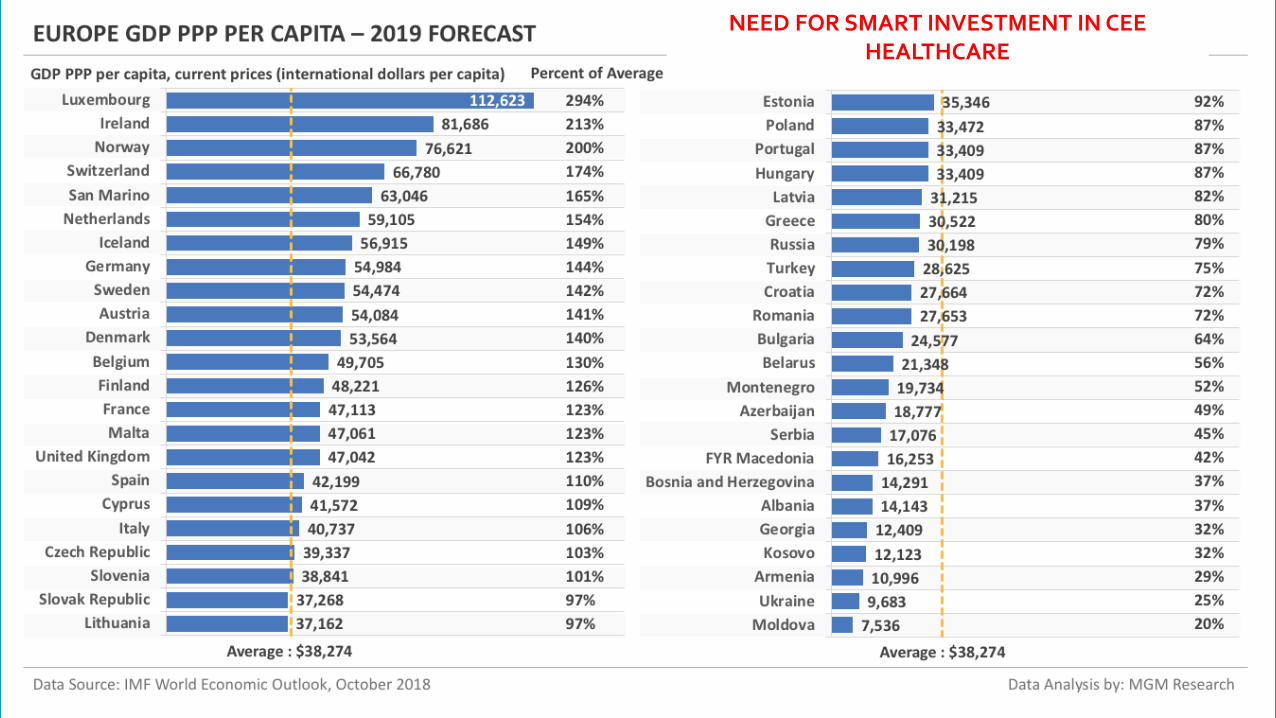
NEED FOR SMART INVESTMENT IN CEE HEALTHCARE
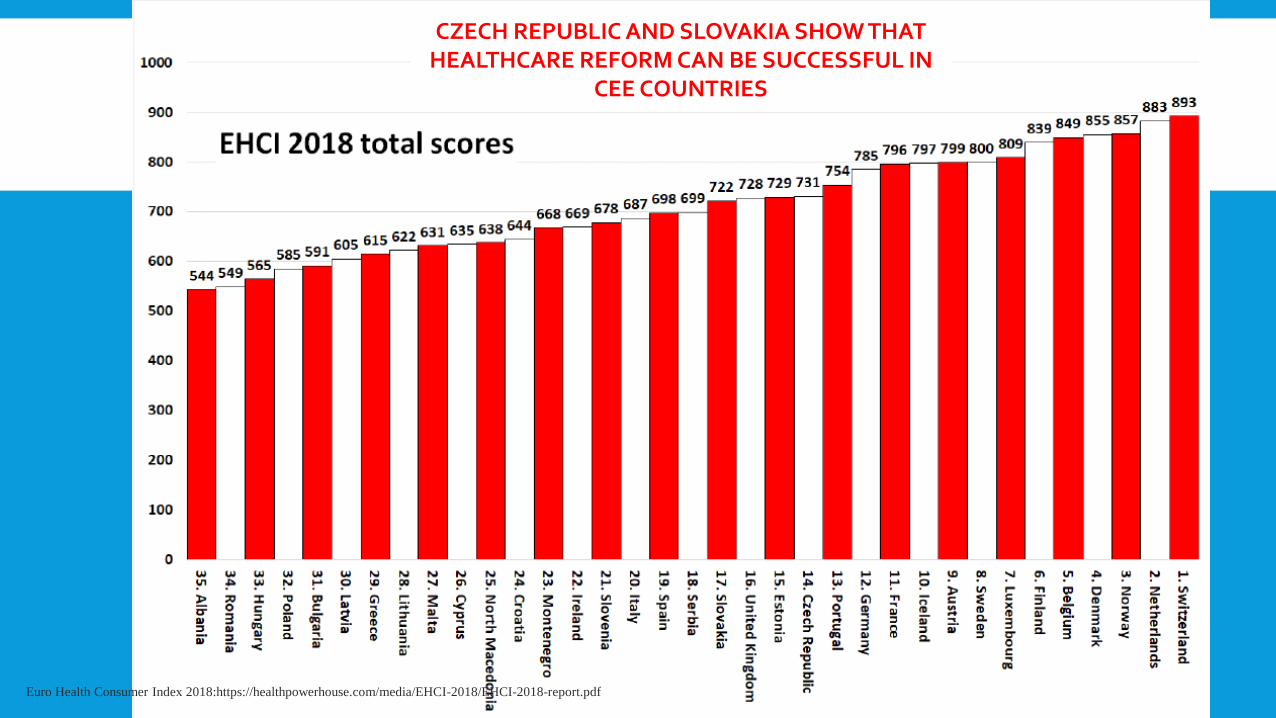
Euro Health Consumer Index 2018:https://healthpowerhouse.com/media/EHCI-2018/EHCI-2018-report.pdf
CZECH REPUBLIC AND SLOVAKIA SHOW THAT HEALTHCARE REFORM CAN BE SUCCESSFUL IN
CEE COUNTRIES
http://aipm.hu/data/upload/files/rendezvenyek/From%20innovation%20to%20outcomes,%20medicines%20cost%20in%20context.pdf.
http://aipm.hu/data/upload/files/rendezvenyek/From%20innovation%20to%20outcomes,%20medicines%20cost%20in%20context.pdf.

RELIABLE DATA
OECD http://www.oecd.org/health/
EUROSTAT: https://ec.europa.eu/eurostat/statistics-explained/index.php/Health_in_the_European_Union_%E2%80%93_facts_and_figures
WHO Europe http://www.euro.who.int/en/home

RELIABLE DATA http://www.oecd.org/els/health-systems/health-data.htm
917
1 05
6
1 33
7
3 85
6
5 87
6
6 22
8
8 29
4
8 84
7
12 1
61
13 6
90
14 0
24
15 4
03
17 9
57
20 4
04
22 4
05
26 4
89
26 8
62
27 2
37
29 6
69
32 7
72
44 3
21
51 0
75 10
0 67
6
107
083
162
045
164
411
169
835
226
662
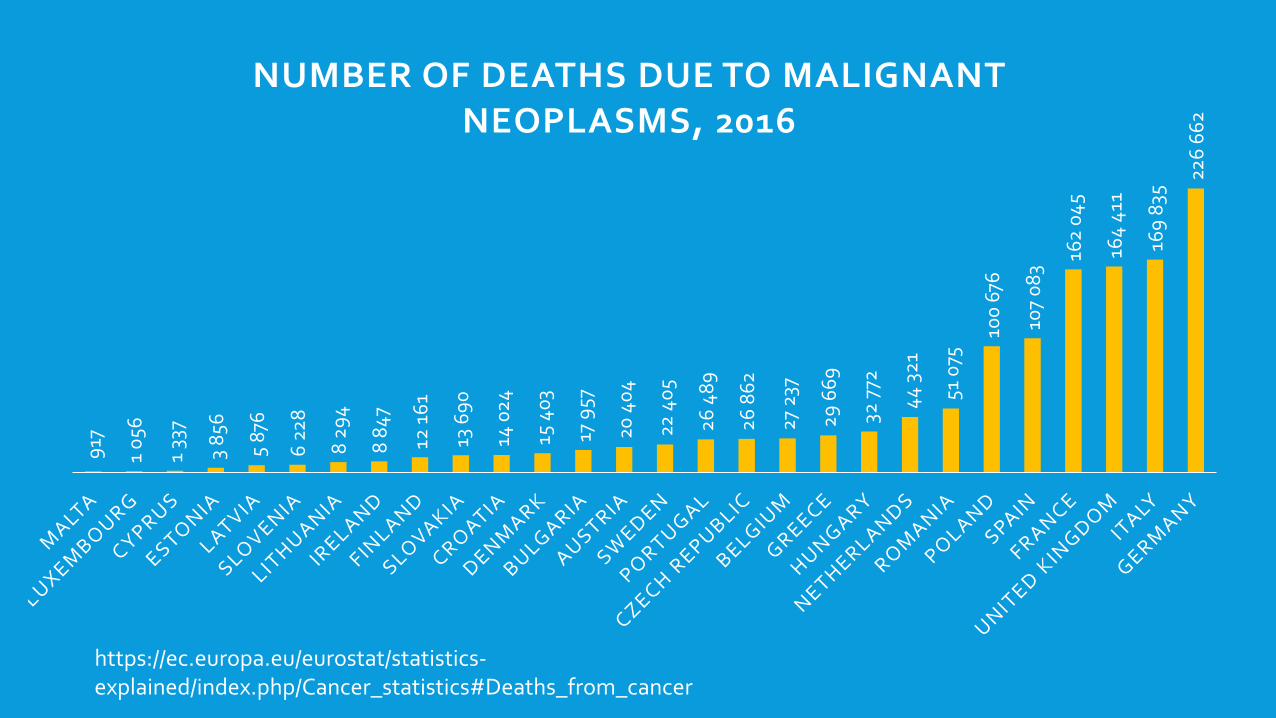
NUMBER OF DEATHS DUE TO MALIGNANTNEOPLASMS, 2016
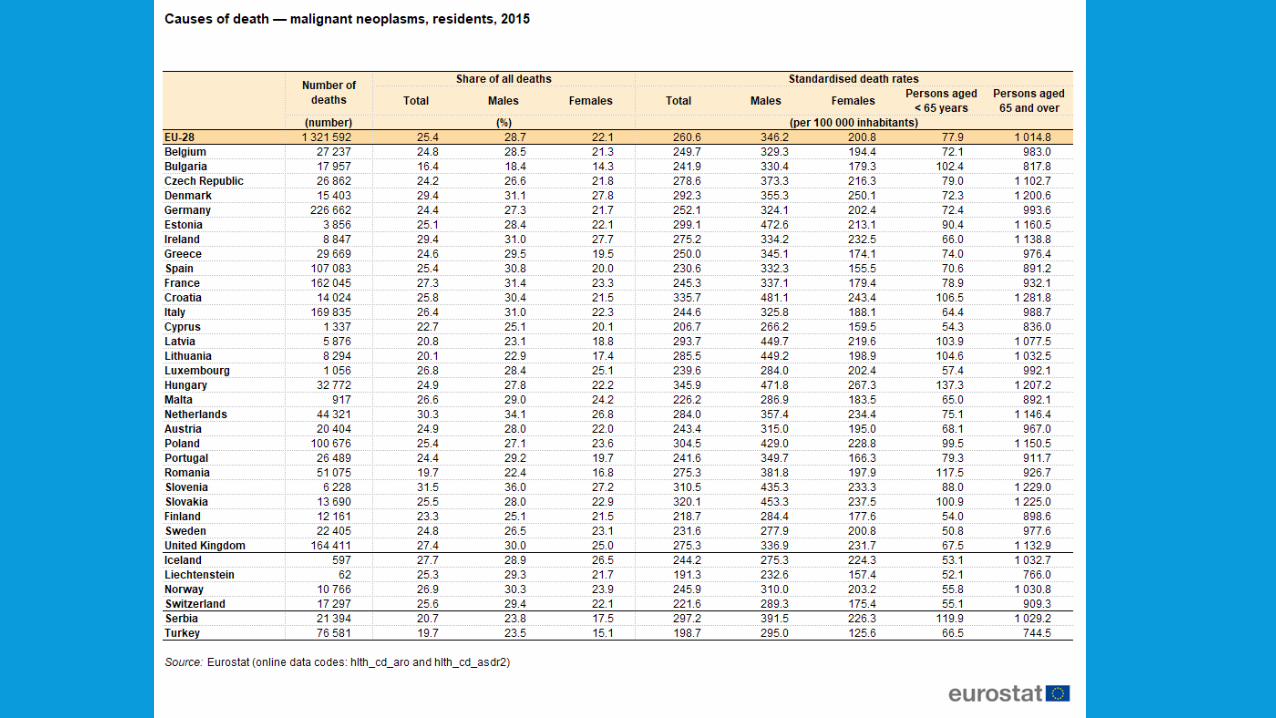
https://ec.europa.eu/eurostat/statistics-explained/index.php/Cancer_statistics#Deaths_from_cancer
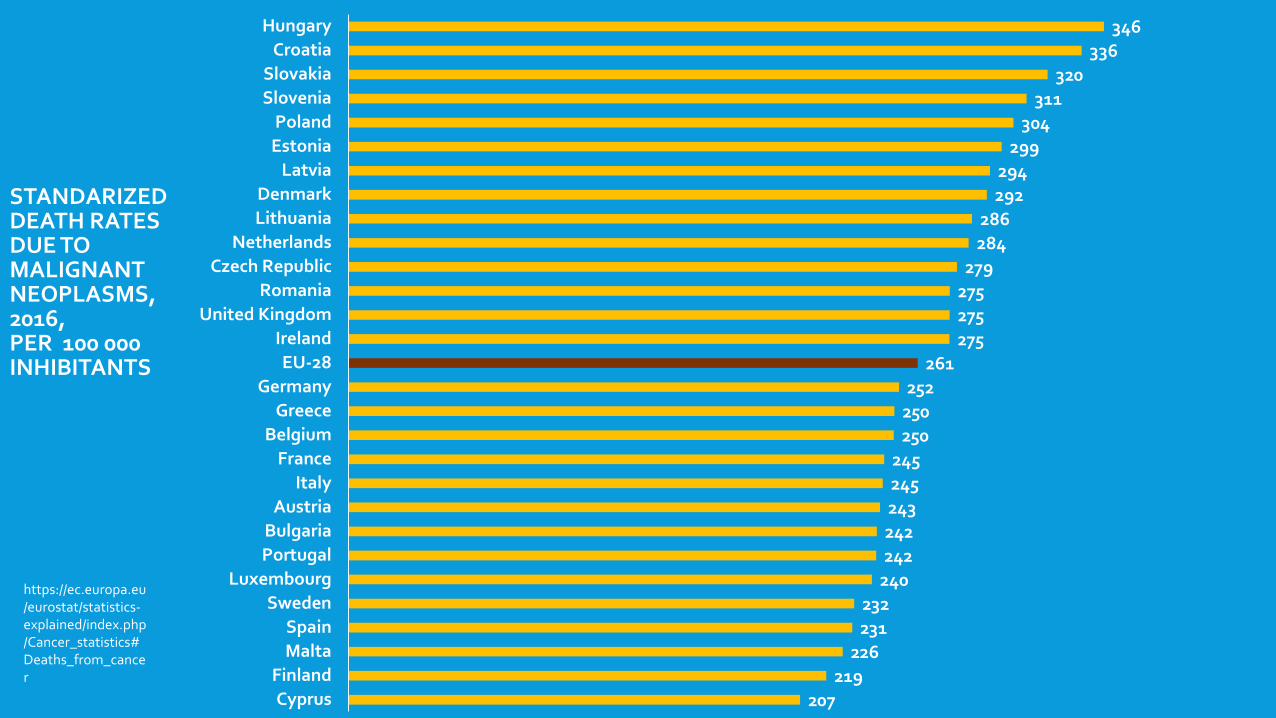
STANDARIZEDDEATH RATESDUE TO MALIGNANT NEOPLASMS, 2016, PER 100 000 INHIBITANTS
https://ec.europa.eu/eurostat/statistics-explained/index.php/Cancer_statistics#Deaths_from_cancer
207219
226231232
240242242243245245
250250252
261275275275279
284286
292294
299304
311320
336346
CyprusFinland
MaltaSpain
SwedenLuxembourg
PortugalBulgaria
AustriaItaly
FranceBelgium
GreeceGermany
EU-28Ireland
United KingdomRomania
Czech RepublicNetherlands
LithuaniaDenmark
LatviaEstoniaPoland
SloveniaSlovakia
CroatiaHungary
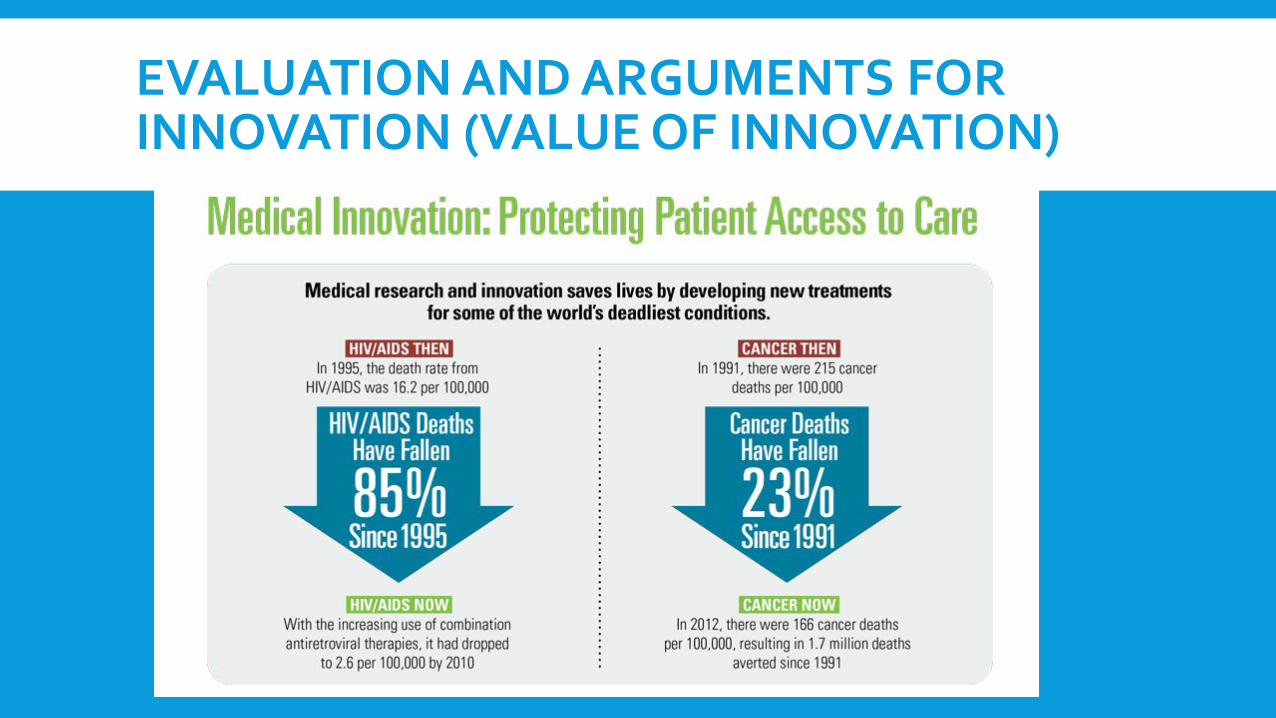
EVALUATION AND ARGUMENTS FOR INNOVATION (VALUE OF INNOVATION)
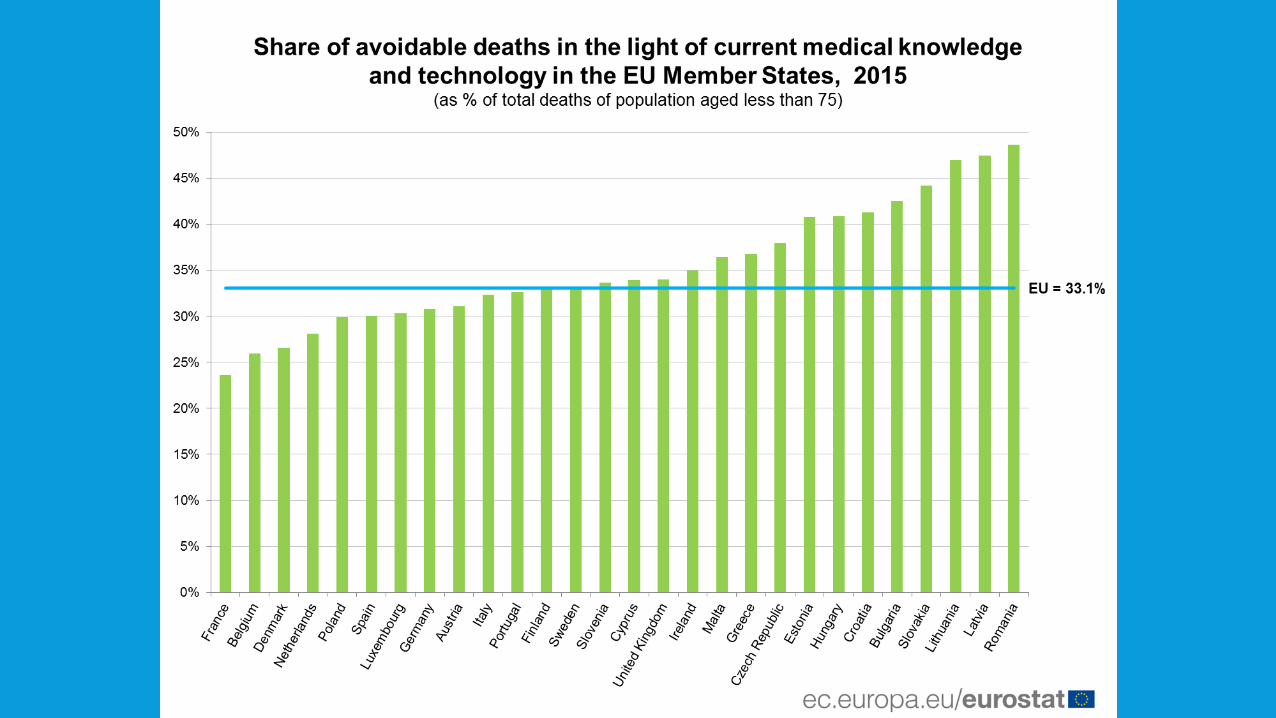
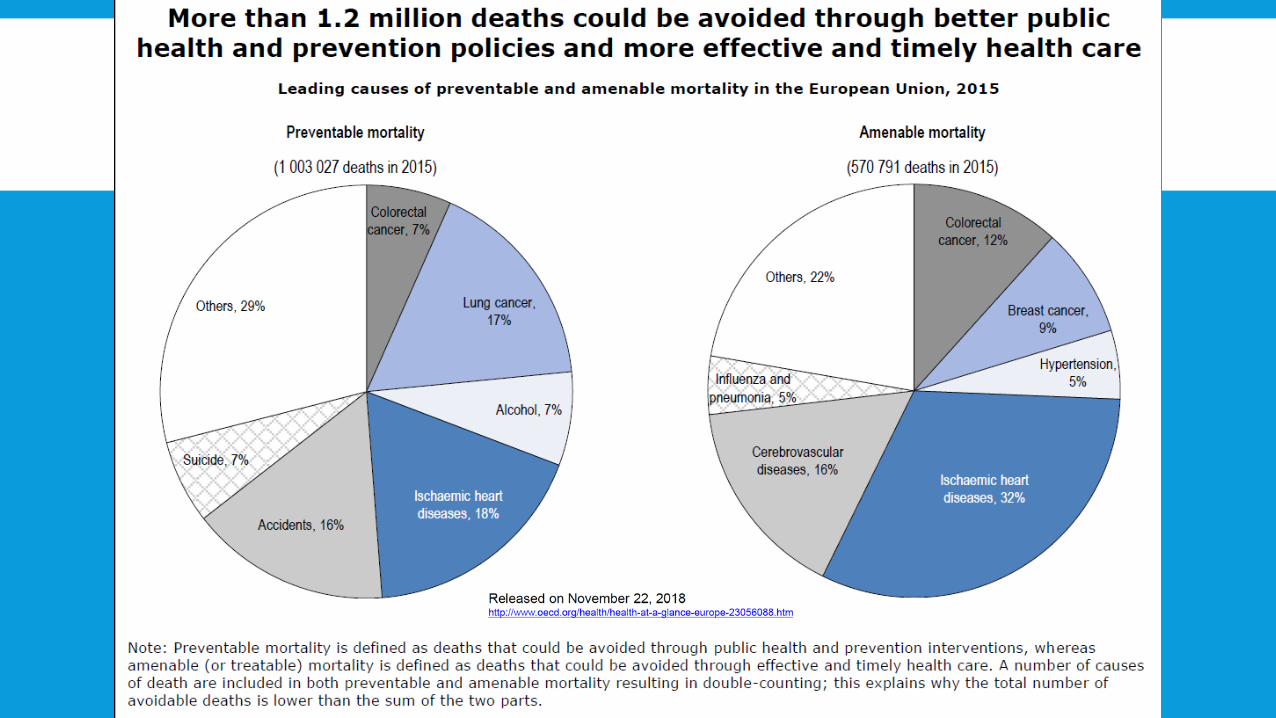
AVOIDABLE DEATHS
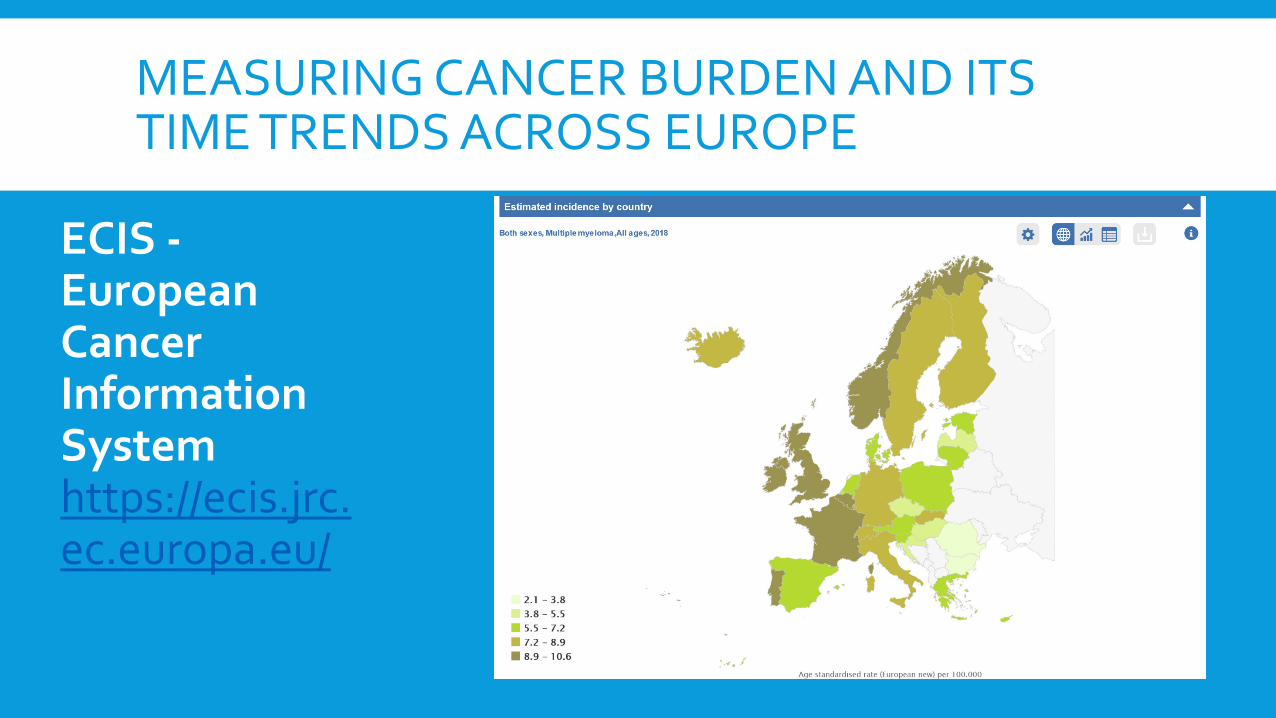
MEASURING CANCER BURDEN AND ITS TIME TRENDS ACROSS EUROPE
ECIS -European Cancer Information Systemhttps://ecis.jrc.ec.europa.eu/

DEFINITIONS FOR EBM
Evidence-based medicine (EBM) can be defined as the formal practice of making decisions regarding the best treatment of patients based on the systematic and detailed approach of current best research evidence.
EBM is of paramount importance in the provision of the best health care policy.
Sacket DJ, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS, Evidence based medicine: what it is and what it isn't. Br Med J 1996;312:71.

Systematic Reviews, http://libguides.mq.edu.au/content.php?pid=371659&sid=3291432

DOMAINS OF QUALITY: CAPTURING PATIENTS’ PERSPECTIVES ON THE EFFECTS OF CANCER AND ITS TREATMENT
The two main domains advocated for capturing patients’ perspectives on the effects of cancer and its treatment are:
1) Patient-Reported Outcome Measures (PROMs), which measure the impact of an illness and the effects of interventions on symptomatology and well-being (e.g. physical function, emotional distress, health-related quality of life, health status)
2) Patient-Reported Experience Measures (PREMs), which capture patients’ views of what happened during the health encounter (care processes)
Tremblay D et al. Determinants of patient-reported experience of cancer services responsiveness. BMC Health Serv Res. 2015; 15: 425.
PROM & PREM AS EVOLUATION OF QUALITY FROM PATIENT’S PERSPECTIVE
PROM
• Effectiveness of care –Does it reduce symptoms, improve function, improve quality of life?
• Safety – Does it cause harm eg mortality, complications?
https://www.kingsfund.org.uk/sites/default/files/media/andrew-hutchings-prems-affect-proms-dec13.pdf
PREM
• Experience of care -What do patients think of the process of care egdignity, information, trust in staff, cleanliness, timeliness?
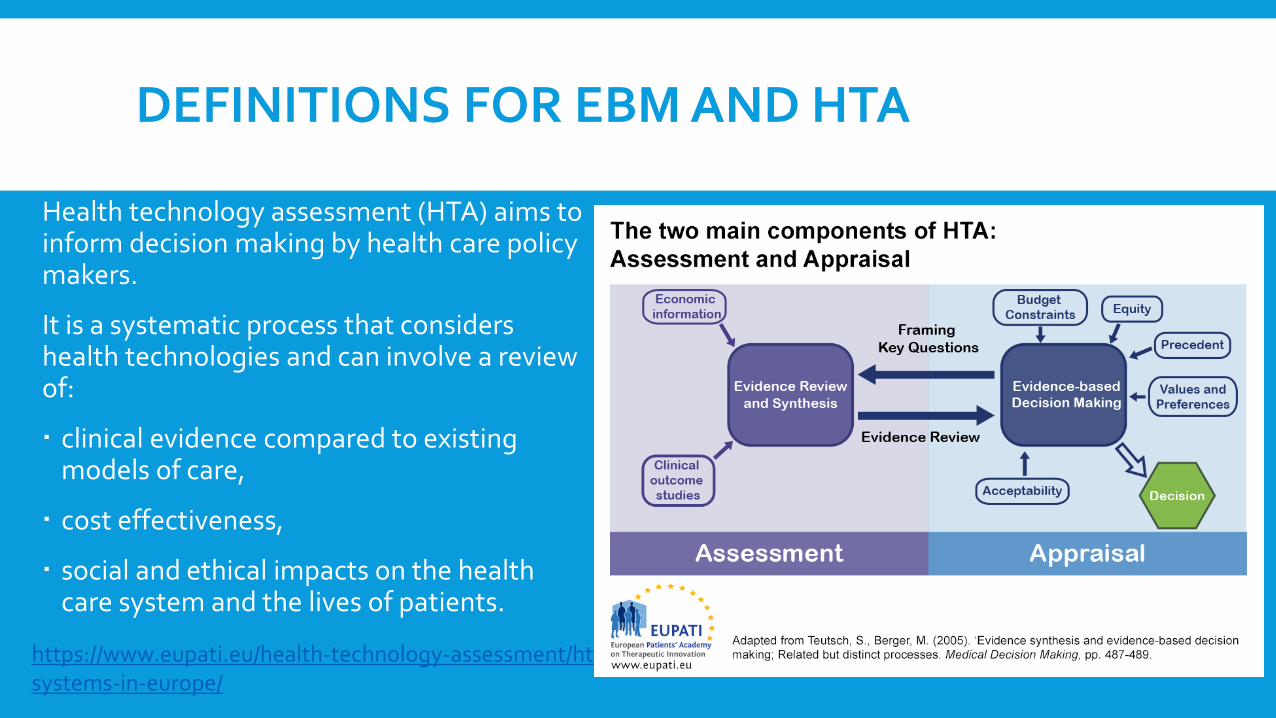
DEFINITIONS FOR EBM AND HTA
Health technology assessment (HTA) aims to inform decision making by health care policy makers.
It is a systematic process that considers health technologies and can involve a review of:
clinical evidence compared to existing models of care,
cost effectiveness,
social and ethical impacts on the health care system and the lives of patients.
https://www.eupati.eu/health-technology-assessment/hta-systems-in-europe/

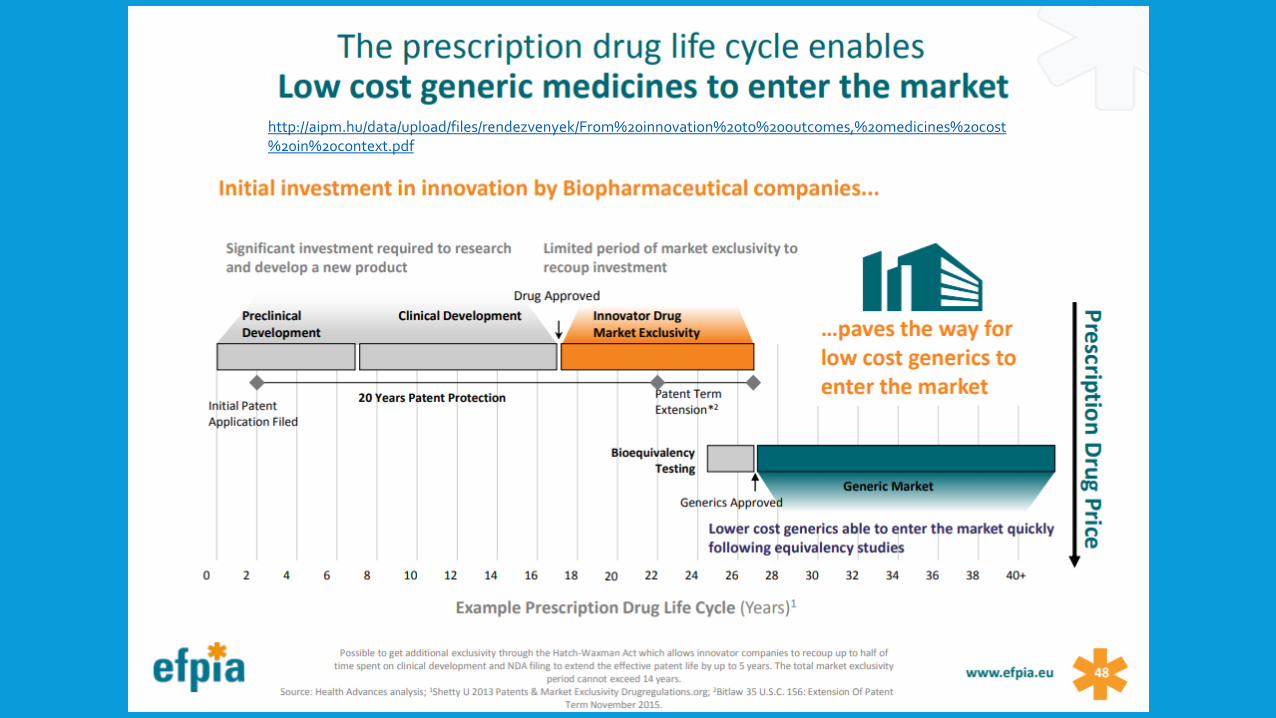
HEALTH INNOVATION
According to WHO “Health innovation identifies new or improved health policies, systems, products and technologies, and services and delivery methods that improve people’s health and wellbeing.
Health innovation responds to unmet public health needs by creating new ways of thinking and working with a focus on the needs of vulnerable populations.
It aims to add value in the form of improved efficiency, effectiveness, quality, sustainability, safety and/or affordability. Health innovation can be preventive, promotive, curative and rehabilitative and/or assistive care.
WHO engages in health innovation to achieve universal health coverage within the context of the Sustainable Development Goals.”
https://www.who.int/topics/innovation/en/
http://aipm.hu/data/upload/files/rendezvenyek/From%20innovation%20to%20outcomes,%20medicines%20cost%20in%20context.pdf.
http://aipm.hu/data/upload/files/rendezvenyek/From%20innovation%20to%20outcomes,%20medicines%20cost%20in%20context.pdf.

https://transparencyreport.janssen.com/us/us-pharmaceutical-transparency-report
https://blogs.lse.ac.uk/healthandsocialcare/2017/01/05/value-in-cancer-drug-spending-assessing-the-clinical-risks-and-benefits-from-a-decades-worth-of-innovation/
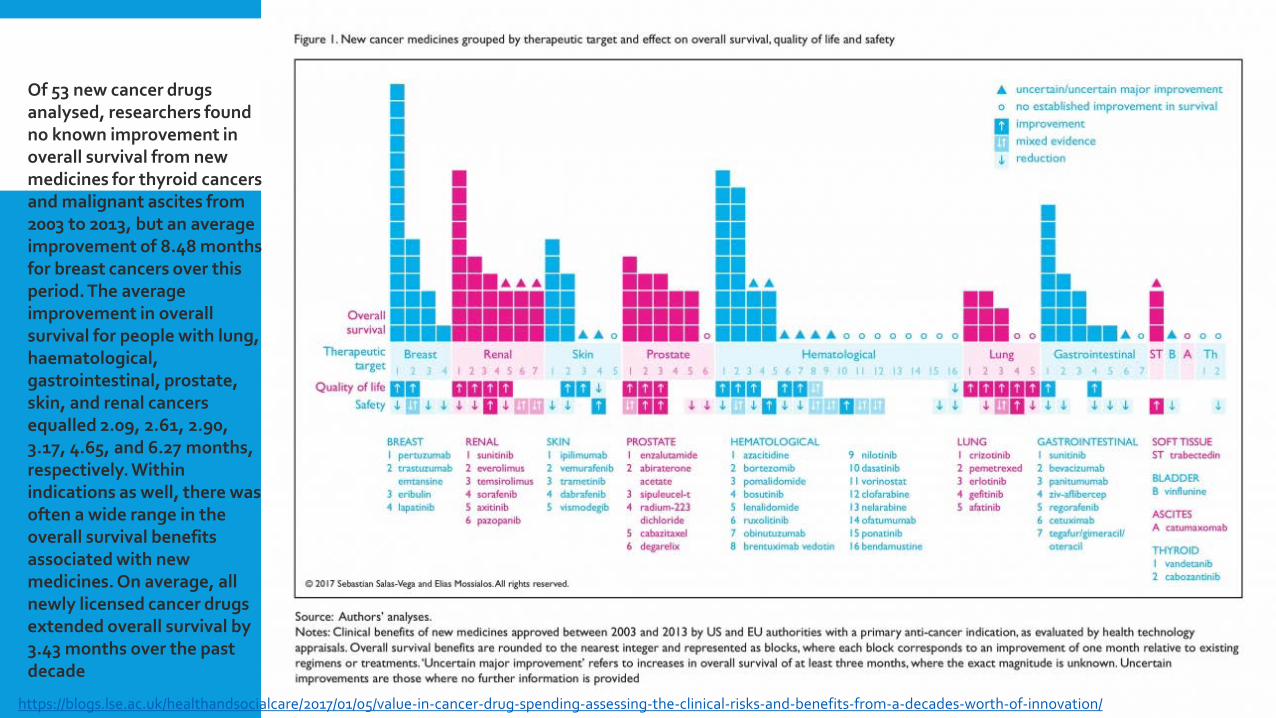
Of 53 new cancer drugs analysed, researchers found no known improvement in overall survival from new medicines for thyroid cancers and malignant ascites from 2003 to 2013, but an average improvement of 8.48 months for breast cancers over this period. The average improvement in overall survival for people with lung, haematological, gastrointestinal, prostate, skin, and renal cancers equalled 2.09, 2.61, 2.90, 3.17, 4.65, and 6.27 months, respectively. Within indications as well, there was often a wide range in the overall survival benefits associated with new medicines. On average, all newly licensed cancer drugs extended overall survival by 3.43 months over the past decade
http://aipm.hu/data/upload/files/rendezvenyek/From%20innovation%20to%20outcomes,%20medicines%20cost%20in%20context.pdf.
http://aipm.hu/data/upload/files/rendezvenyek/From%20innovation%20to%20outcomes,%20medicines%20cost%20in%20context.pdf.
http://aipm.hu/data/upload/files/rendezvenyek/From%20innovation%20to%20outcomes,%20medicines%20cost%20in%20context.pdf.
HEALTH INDICATORS IN HAEMATOLOGY
OS (overall survival) - The length of time from either the date of diagnosis or the start of treatment for a disease, such as cancer, that patients diagnosed with the disease are still alive. In a clinical trial, measuring the overall survival is one way to see how well a new treatment works.
PFS (progression-free survival) - The length of time during and after the treatment of a disease, such as cancer, that a patient lives with the disease but it does not get worse. In a clinical trial, measuring the PFS is one way to see how well a new treatment works.
QoL (quality of life) - Many clinical trials assess the effects of cancer and its treatment on the quality of life. These studies measure aspects of an individual’s sense of well-being and ability to carry out activities of daily living.
https://www.cancer.gov/publications/dictionaries/cancer-terms/def/overall-survival

RWD/RWE: medical and payer registries, big data

REAL-WORLD DATA ANALYSIS
To improve health outcomes for patients by accelerating research and real-world data generation and analysis, increase transparency and information sharing, and enhance the understanding and utilization of real world data.
The collaboration has focused on the follow-up and effects of disease and treatment, using routine data from health care ("Real World Data"), and how they relate to effects in clinical trials, all while social and economic factors are evaluated.
https://www.janssen.com/partnerships/collaborating-karolinska-institutet-advanced-real-world-data-analysis

RWD/RWE AS A SOLID BASIS FOR REIMBURSEMENT DECISIONS

REAL-WORLD DATA ANALYSIS
• The need to generate evidence in the real world, based on data derived in the clinical
setting outside of the randomized clinical trial, is growing rapidly.
• Through extensive external collaborations, Janssen develops infrastructure and
incorporate diverse capabilities and skillsets to interact with and analyze real world data
(RWD) to generate real world evidence (RWE).
• The introduction of RWD/EHR (Electronic Health Records) platforms could facilitate
optimization of clinical research and stimulate strategic collaborations to advance medical
science overall.
https://www.janssen.com/partnerships/collaborating-karolinska-institutet-advanced-real-world-data-analysis

REGISTRIES
European Platform on Rare Disease Registration(EU RD Platform) https://eu-rd-platform.jrc.ec.europa.eu/
Myeloma Sweden http://www.haematologica.org/content/103/3/506 Denmark http://www.danishhealthdata.com/find-health-
data/Dansk-Myelomatose-Database Austria https://www.oncotyrol.at/amr/ Czech Rep. https://www.myeloma.cz/index-en.php?pg=rmg-
registry-of-monoclonal-gammopathies

INTRODUCTION TO VALUE BASED HEALTH CARE
Porter’s definition and methodology
https://www.isc.hbs.edu/health-care/vbhcd/Pages/default.aspx
INTRODUCTION TO VALUE BASED HEALTH CARE
VALUE BASED HEALTH CARE - VBHC
Patient should be in the center of system with access to qualitycare, monitoredin terms of improved healthoutcomes and optimal costs
https://crcaustralia.com/media-releases/from-evidence-based-medicine-to-value-based-healthcare-is-australia-ready/figure2/
INTRODUCTION TO VALUE BASED HEALTH CARE
Measure Outcomes & Costs for Every PatientMeasuring CostsSystems Integration
https://www.isc.hbs.edu/health-care/vbhcd/Pages/default.aspx
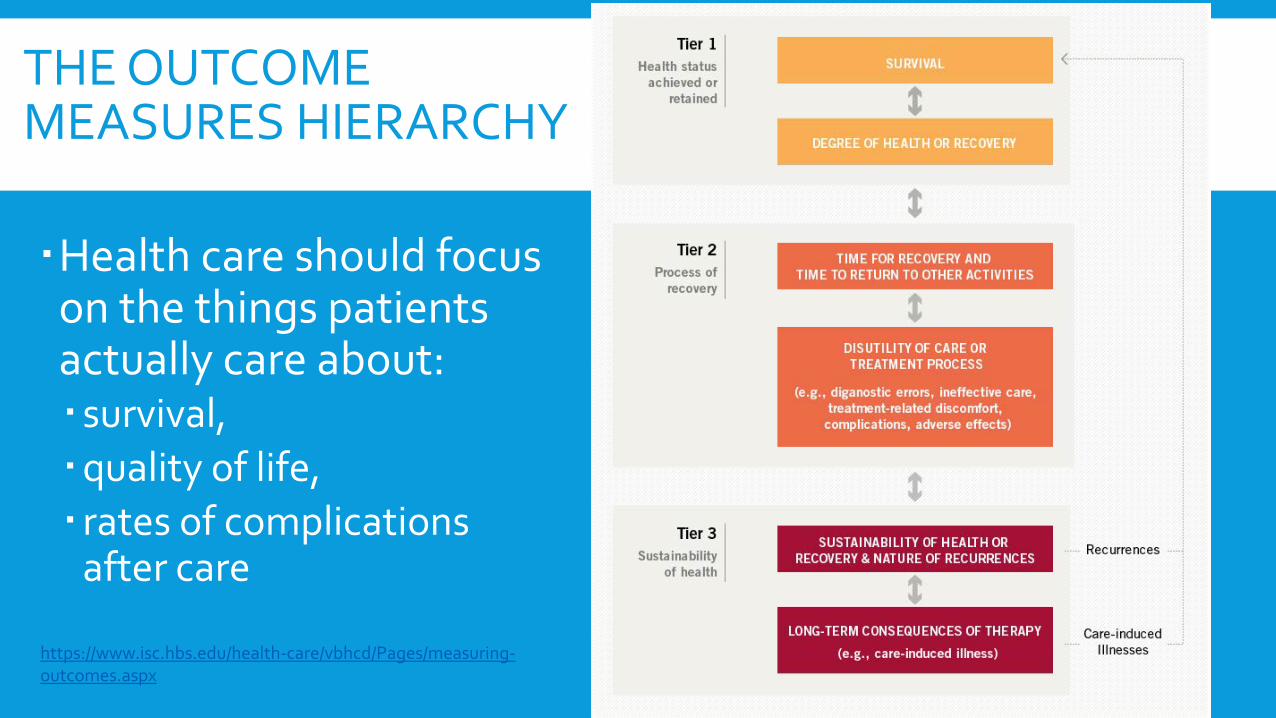
THE OUTCOMEMEASURES HIERARCHY
Health care should focuson the things patients actually care about: survival, quality of life, rates of complications
after care
https://www.isc.hbs.edu/health-care/vbhcd/Pages/measuring-outcomes.aspx
THE OUTCOME MEASURES HIERARCHY
What is the value-based approach to outcome measurement?
Outcomes are the ultimate measure of quality. In health care, measurement of value should focus on how well the care delivered meets individual patients' needs.
Measuring success, or the results of treatment, requires following the patient through the process of care, and looking at medical conditions and patients holistically.
For example, for patients with cancer, their medical condition includes co-existing fatigue, immunodifficency, and mal nutrition. Success in treating cancerincorporates the combined effect of caring for all of these needs.
https://www.isc.hbs.edu/health-care/vbhcd/Pages/measuring-outcomes.aspx
PRINCIPLES OF MEASURING THE COST OF CARE
Cost is the actual expense of patient care, not the charges billed or collected
Cost should be measured around the patient
Cost should be aggregated over the full cycle of care for the patient’s medical condition, not for departments, services, or line items
Cost depends on the actual use of resources involved in a patient’s care process (personnel, facilities, supplies):• The time devoted to each patient by these resources• The capacity cost of each resource• The support costs required for each patient-facing resource
https://www.isc.hbs.edu/health-care/vbhcd/Pages/measuring-outcomes.aspx

SYSTEMS INTEGRATION
Value-based health care delivery organizes care around patient needs
Steps for Creating an Integrated Care Delivery System
Choose an overall scope of services where the provider system can achieve excellence in value
Rationalize service lines / IPUs across facilities to improve volume, better utilize resources, and deepen teams
Offer specific services at the appropriate facility based on medical condition, acuity level, resource intensity, cost level, need for convenience
Clinically integrate care across units and facilities using an IPU structure:• Integrate services across the care cycle• Integrate preventive/primary care units with specialty Integrated Patient Units (IPUs)
https://www.isc.hbs.edu/health-care/vbhcd/Pages/measuring-outcomes.aspx

A VBHC APPROACH OF MULTIPLE MYELOMA - A HIGH COMPLEX MEDICAL CONDITION THAT REQUIRES A FOCUS ON TRUE OUTCOMES
In order to provide the best, most valuable care possible, Máxima Oncology Center developed a set of outcome measures that really matter to patients with MultipleMyeloma.
Patients became part of the expert teams responsible for the integrated pathways of care
The most important learning of the identification of outcome measures that really matter to patients with Multiple Myeloma is that all employees, working in Máxima Oncology Center, think about adding value for the patients every day. Every treatment, intervention and development always takes place in collaboration with the patient.
Another learning of the development of outcome measures is to involve a multidisciplinary team with different perspectives. This team should include patient representatives from official patient organizations, registry experts and leading physicians. Use universal health outcomes to facilitate international collaboration.
https://www.vbhc.nl/wp-content/uploads/VBHC-Thinkers-Magazine-VBHC-Prize-2018-edition_v2.pdf
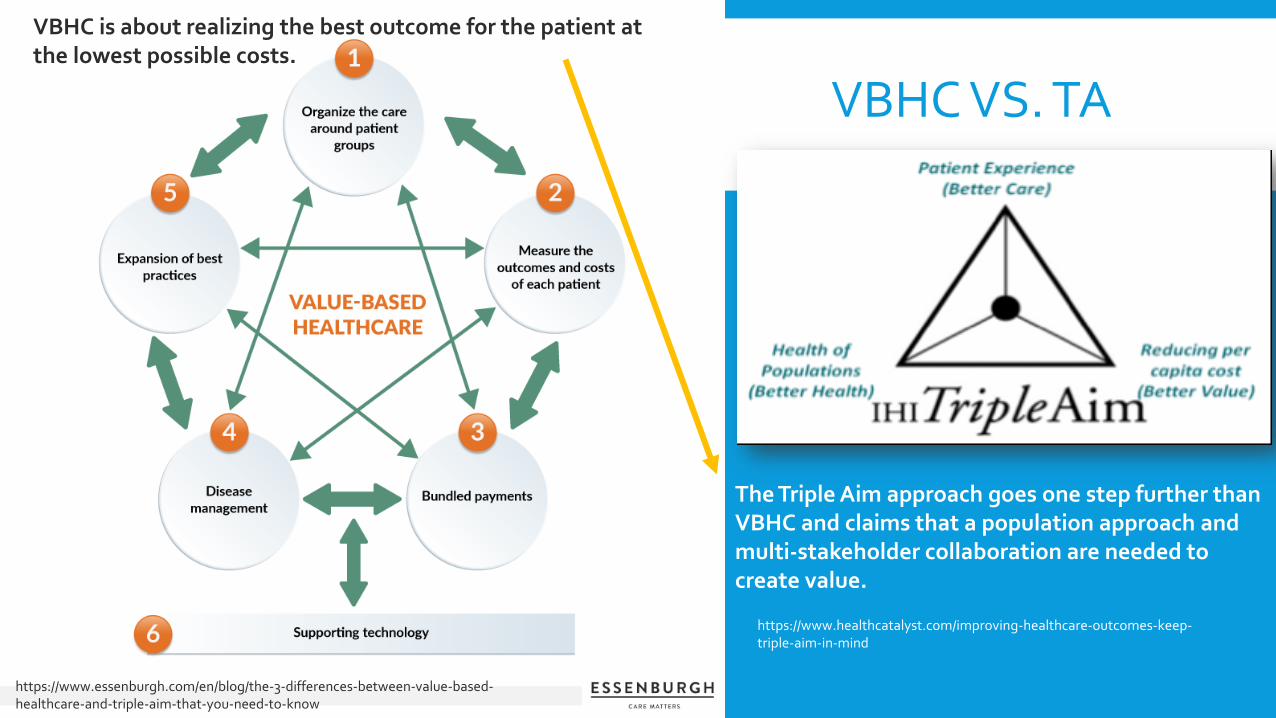
VBHC VS. TA
https://www.essenburgh.com/en/blog/the-3-differences-between-value-based-healthcare-and-triple-aim-that-you-need-to-know
https://www.healthcatalyst.com/improving-healthcare-outcomes-keep-triple-aim-in-mind
The Triple Aim approach goes one step further than VBHC and claims that a population approach and multi-stakeholder collaboration are needed to create value.
VBHC is about realizing the best outcome for the patient at the lowest possible costs.
HOW TO CONVINCE THE PAYERS WITH EVIDENCE
Data evidence for Value based approachPatient’s centric approachManaged entry agreements and key data - how
to use themHow to benchmark best examples from other
CEE countriesNetworking in Data and Value evidence
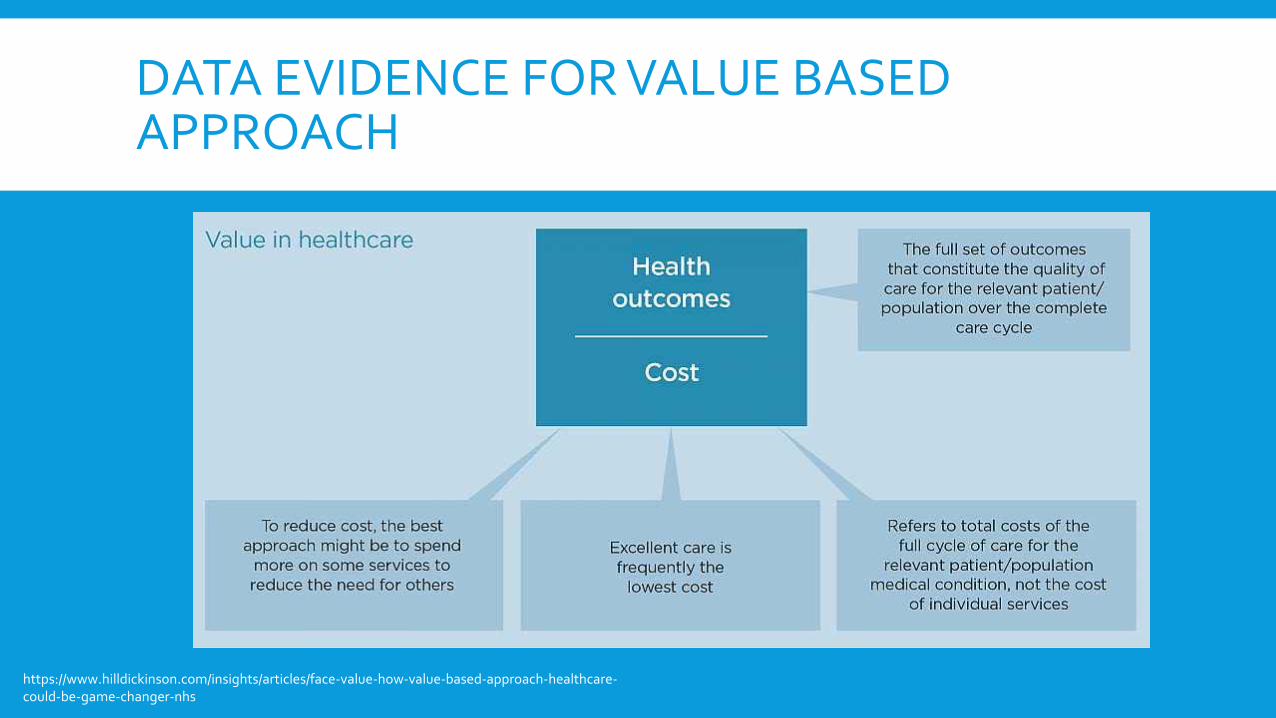
DATA EVIDENCE FOR VALUE BASED APPROACH
https://www.hilldickinson.com/insights/articles/face-value-how-value-based-approach-healthcare-could-be-game-changer-nhs
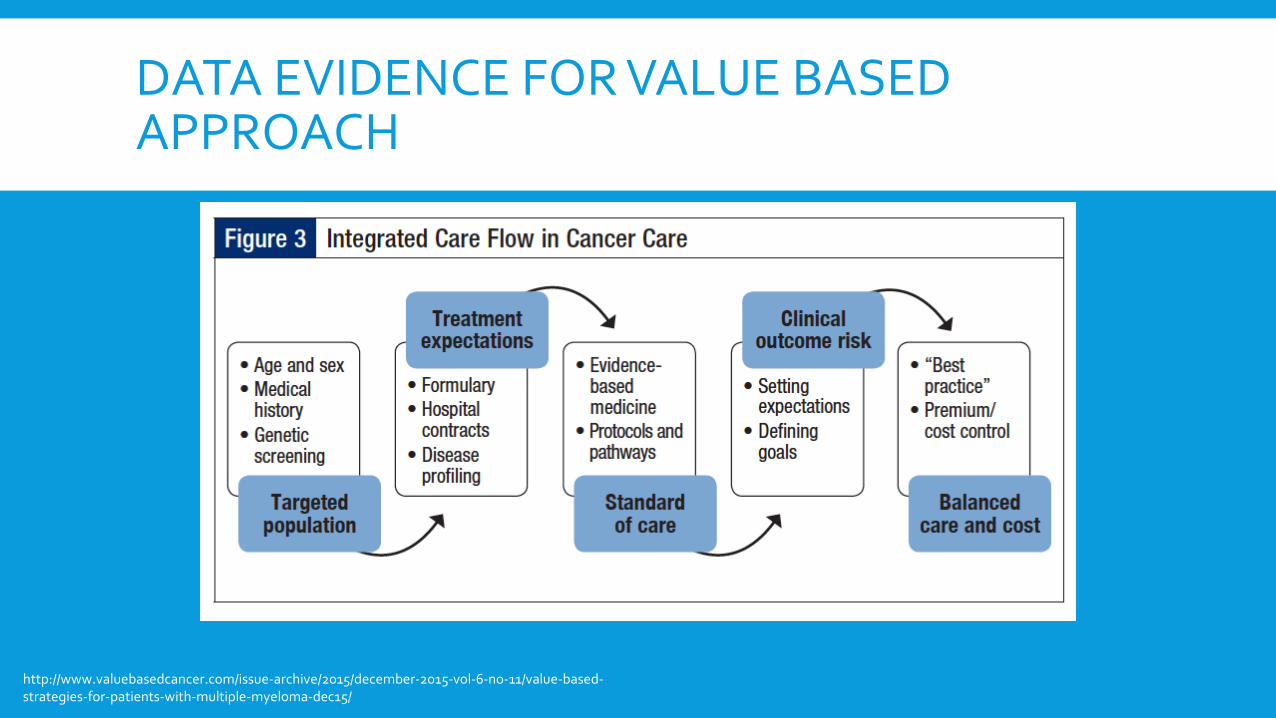
DATA EVIDENCE FOR VALUE BASED APPROACH
http://www.valuebasedcancer.com/issue-archive/2015/december-2015-vol-6-no-11/value-based-strategies-for-patients-with-multiple-myeloma-dec15/
SELECTED PRINCIPLES OF VALUE-BASED COMPETITION
Refocus on the value for patients rather than lowering costs consistently at all levels within the healthcare institution
Competition is driven by results, i.e., favor processes which demonstrate improved value of the care delivered
Reduce cost of high-quality care
Competition should expand from local areas to regional and national settings
Provide transparency and accessibility of value-based results from all participants in value-based care
Reward and endorse innovations that better the value of care provided for a medical condition
Johansen N. Value-Based Care in the Worldwide Battle Against Cancer, Cureus. 2017 Feb; 9(2): e1039 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5356991/

PATIENT’S CENTRIC APPROACH
https://www.ttec.com/articles/customer-focused-injection-patient-experience
PATIENTINVOLVEMENT
http://aipm.hu/data/upload/files/rendezvenyek/From%20innovation%20to%20outcomes,%20medicines%20cost%20in%20context.pdf.





























