Embed Size (px)
Citation preview

Implementing Single Session Family Consultation in a Youth Mental Health Service
Brendan O’Hanlon, Suzanne Fuzzard & Carol Harvey

Family Interventions as Recommended Practice• NICE Guidelines: Psychosis & Schizophrenia (2014)‘Offer family intervention to families of people with psychosis or schizophrenia who live with or are in close contact with the service user.’
• PORT Recommendations: Schizophrenia (2010)‘Persons with schizophrenia who have ongoing contact with their families, including relatives and significant others, should be offered a family intervention that lasts at least 6–9 months.’
• NICE Treatment Guidelines: Bipolar Disorder (2014)‘As early as possible negotiate with the person with bipolar disorder and their carers about how information about the person will be shared…………….. Foster a collaborative approach that supports both people with bipolar disorder and their carers, and respects their individual needs and interdependence.’

Policy Promoting Inclusion of Families in Mental Health
• The National Mental Health Plan, 2009-2014
• The National Mental Health Standards(2010)
• State Mental Health Acts e.g., Victorian Mental Health Act (2014)
• State government mental health policy
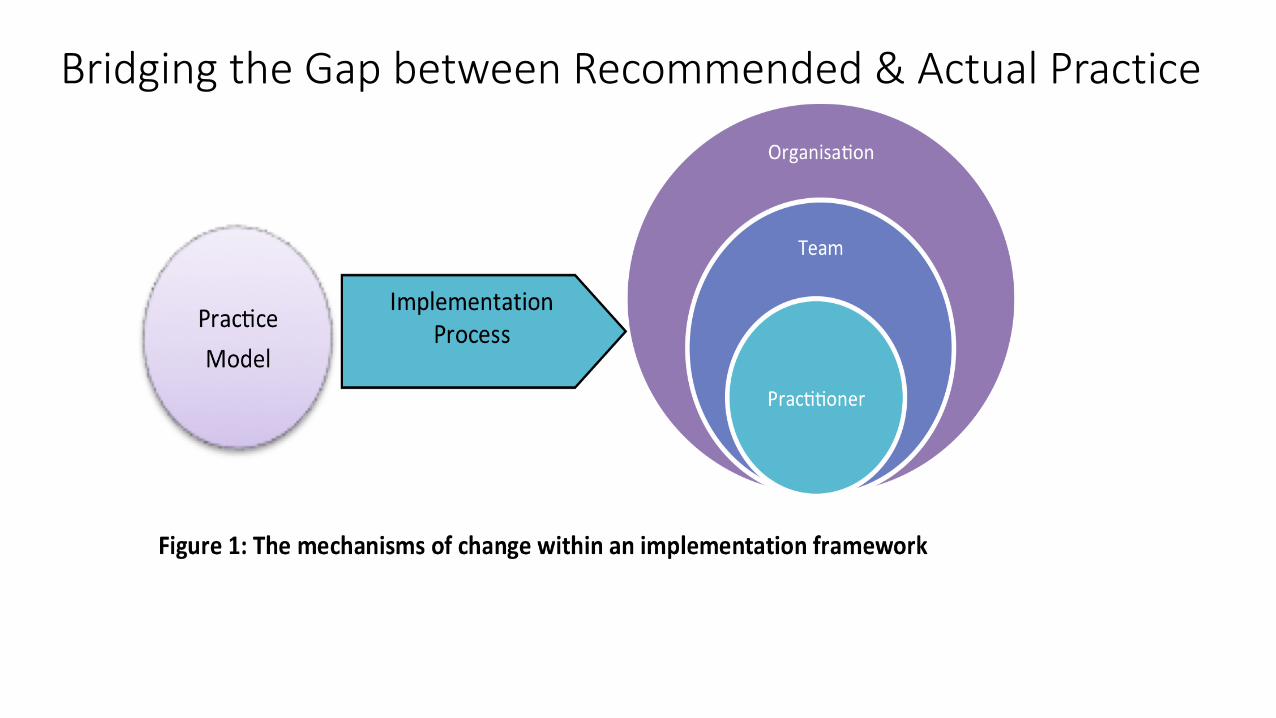
Bridging the Gap between Recommended & Actual Practice

• Growing interest in family inclusion within headspace but with history of limited success in achieving change
• Family Inclusion Project successful in competitive process for internal service development funds (Department of Health and Ageing)
• Limited data on family demographic and contact• Varied auspice and organisational arrangements• Sites selected on basis of interest and reflecting different settings
• Murraybridge• Port Augusta• Warrnambool • Frankston
The Context: Headspace Centres

The Practitioners
• Youth mental health practitioners and youth workers
• Practitioners from a range of disciplines
• Variable attitudes and levels of experience in relation to working with families
• Family Therapy trained practitioners at some centres

• Focus on all staff within headspace who see clients -have varied training and experience
• More staff comfortable seeing families then more families will be seen vs. specialist role of the Family Worker with limited reach
• Changing the work place culture in relation to family inclusion.
• A brief intervention focus
Why SSFC?

• Brief model of family engagement (1-3 sessions)
• Strong focus on negotiating family involvement with the client
• A consultative meeting between a practitioner and family that aims to:
• Clarify the working relationship between the client, family & practitioner• Help families identify & address their needs
• Ideas from Single Session Therapy inform the process
Single Session Family Consultation (SSFC)

• Joint Bouverie and headspace management of the project• Pilot sites• Two day training in SSFC with follow up supervision & booster
sessions• Funded site leads(champions) in dedicated role• Support for site leads• Project newsletter• Development of support resources to aide sustainability
Process: Implementation strategy

• What was the extent of implementation of the SSFC model?
• What was the experience of young people, their families and practitioners concerning SSFC sessions?
• How effective was the chosen strategy for implementing SSFC from the perspectives of SSFC-trained workers and managers?
Evaluation Questions

• Impact of the project on levels of family-related activities
• Impact of training and implementation support on practitioners and the organisation including perceptions of family inclusive practice and organisational readiness to adopt SSFC
• The experiences of young people, their families and workers of SSFC family sessions
• Practitioners and managers experience of the implementation process including factors affecting uptake
Evaluation Domains

Practitioners and Managers

SSFC Sessions Conducted at Each Site
8
21
68
34
0
10
20
30
40
50
60
70
80
F P M W
SSFC conducted by site
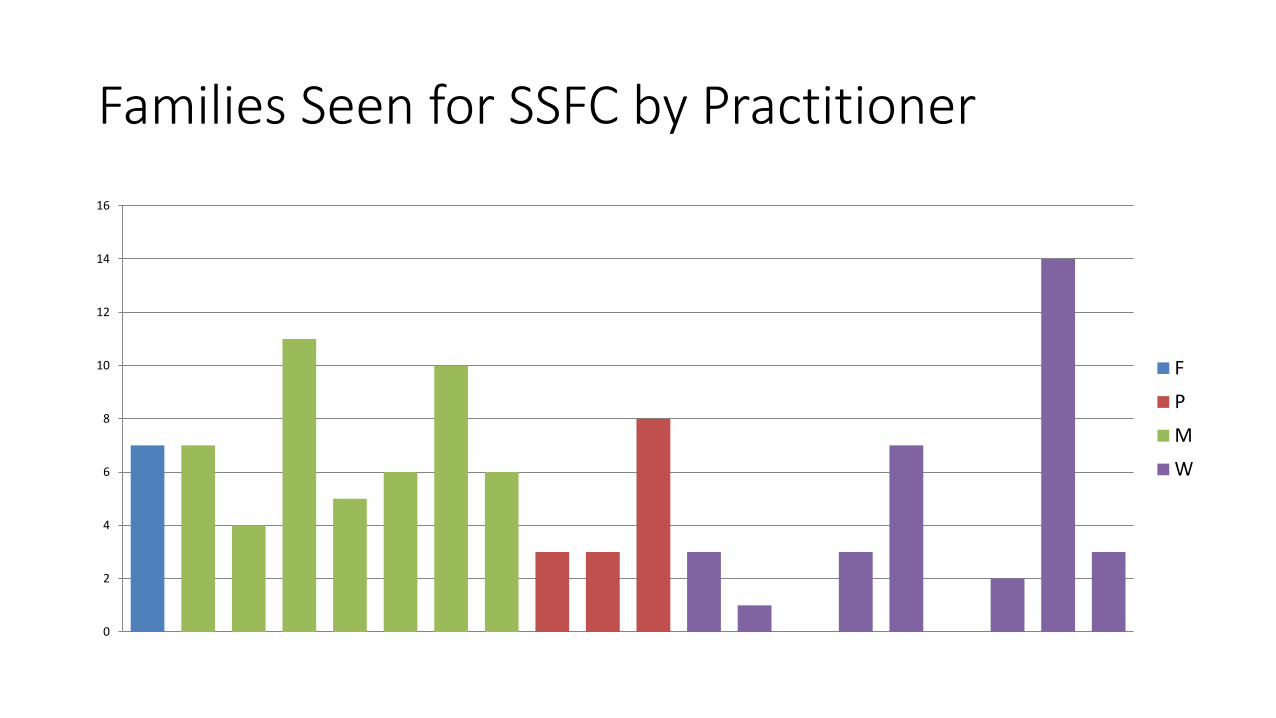
Families Seen for SSFC by Practitioner
0
2
4
6
8
10
12
14
16
F
P
M
W

Family Inclusive Practice Questionnaire Pre, Following Training and Six Months Post Training
• provision of supervision, • knowledge to conduct an interview with more than one person, • knowledge about how client’s difficulties impact on family, • knowledge to invite other people into client’s session, • workplace’s procedures on working with families, • practice to speak to each family member before having a family meeting, • skills to work with clients on their difficulties affecting their families, • confidence in working with families and • practice to work collaboratively with clients’ families.

Family Intervention SchedulePre, Following Training and Six Months Post Training• availability of appropriate families to work with, • non-applicability of existing approaches in working with families, • having to work outside working hours, • lack of familiarity with approaches, • keeping family discussions on track, • clash of working with families with other needs of clients, • confidence working with families, • concern on conflicts in family meetings and • anticipation that families will be hostile to worker or service • travel to family session

Organisational Readiness Tool• supervision and mentoring to provide SSFC, • encouragement to try a new and different technique, • clear policies and procedures to support family work, • overwhelmed by amount of work, • support from co-workers to provide SSFC, • clear vision and commitment from management to SSFC, • frequent turnover, • feeling of “bogged down” by the system, • help from staff, • agreed upon process for recording family work, • strong commitment from workers to include families in working with clients and• expectation of management to implement SSFC.

Themes from Practitioner and Manager InterviewsSix months post training
• The model was well implemented in the four sites showing feasibility and acceptability of SSFC in headspace.
• Training and ongoing supervision were recognised as important elements in the model.
• Managerial support in family inclusive practice was important to encourage staff to provide SSFC.
• Teamwork was considered helpful in the implementation and uptake of SSFC.

Themes from Practitioner and Manager InterviewsSix months post training• Availability of experienced family-therapy trained workers as
supervisors and motivators in the organisations was an advantage.
• Provision of SSFC was limited by the shortage of suitable consultation rooms and by caseloads.
• SSFC had to be modified so that it was suitable for the intake process.
• Difficulties with reimbursement to private practitioners for them to attend training and provide family sessions as they were reimbursed by Medicare for standard patient consultations only.

Young People and Their Families

Invitations to Participate in SSFC
72%
28%
Offers of SSFC
SSFC declined
N=200
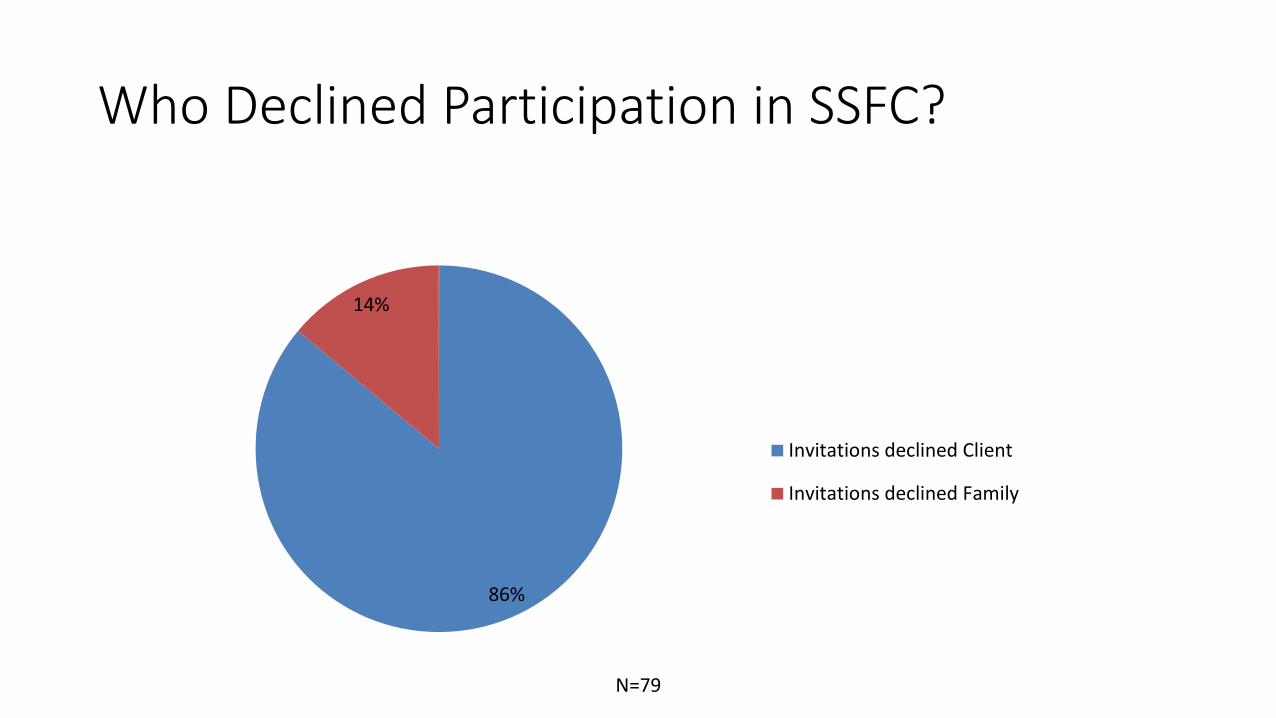
Who Declined Participation in SSFC?
86%
14%
Invitations declined Client
Invitations declined Family
N=79

Feedback from Clients and Families
0
1
2
3
4
5
6
Relationship (0-6) Goals and topics (0-6) Approach or method (0-6) Helpfulness (0-6) Overall (0-6)
Clients (n=129)
Family members (n=191)

Client-Young Person Feedback-1
SSFC sessions enhanced communicationMost of young people expressed that SSFC helped them to share their feelings and stories with their families. They were able to find out the thoughts and feelings of another family member and SSFC helped to clear misunderstandings among them. • “We could all sit there and talk about family stuff together and tell someone
else that could help us.” [YP1]SSFC helped them to obtain advice and find solutionsThe majority of the young people reported that they were able to resolve problems and set goals through SSFC sessions. • “I liked that we got to talk about things that would make me feel better in
the future.” [YP4]

Client-Young Person Feedback-2Young people felt supported in SSFC sessionsYoung people felt supported and were comfortable to share their stories in the sessions. They said that the sessions were conducted in a warm, casual and non-judgmental manner.• “That I could be open and honest and that I was listened to and that I felt
comfortable.” [YP6]
Sessions might be too long and confronting for some, while most preferred more sessions• Some young people felt that the sessions were too long and confronting. The
uneasiness was due to some feeling uncomfortable discussing things in front of a particular family member, while some felt that others did not understand them. On the positive side, most young people preferred more frequent sessions.
• “I guess the part where everyone was really focused on me; I was just thinking well I am not the only one in the room.” [YP 9]
Family Member Feedback-1SSFC sessions enhanced communication• The most common comment was SSFC sessions enabled communication to be open, honest
and non-judgmental. SSFC provided opportunities for them to listen to the young person and for them to communicate their stories.
• “The openness of it all. Being able to express my opinion as well as listening to my child’s opinion, and the feedback we got.” [Family 1]
SSFC helped them to obtain advice and find solutions• The families reported many benefits such as getting advice and information on services and
learning coping strategies. They also appreciated that issues were resolved and goals for the future were made.
• “Made me feel like I’m normal. Have some good ideas what to do. There is some hope and help available.” [Family 6]
Workers were helpful• Many families expressed their appreciation of the workers. They felt that the workers were
warm, caring and non-judgmental and facilitated the discussions well. They felt that the atmosphere was comfortable and safe. They also appreciated the bonding between the young people and the workers.
• “Felt that she was encouraging, supportive. Felt comfortable to open up and share.” [Family 7]

Family Member Feedback-2Sessions might be too stressful and serious for some young people and their families• Some family members said that the sessions might be too stressful for the young
person for reasons such as asking them too many questions and also that some of the questions were too long and serious. Some family members reported they felt emotional when they heard about the circumstances that the young person was facing.
• “Seeing my child feeling helpless and hurt by her life situations.” [Family 11]More frequent sessions • Most of the families preferred more frequent sessions. They also suggested that
future sessions could be longer, conducted in a bigger family consultation room and incorporate more strategies and coping methods.
• “Probably if I had a chance to say more, ask more questions with my daughter.” [Family 14]

Projects Resources

Training DVD

Practice Manual

Implementation Guide
http://thebouveriecentreheadspace01.iformat.com.au

Conclusions• Relatively high levels of uptake of SSFC with evidence of consolidation
of the practice for most practitioners• Only three of 20 trained did not use the model • Practitioner measures point to a growth in confidence in use of the model
• Two centres where a larger number of staff conducted SSFC achieved the higher rates of uptake-supports SSFC as a generalist rather than specialist model
• SSFC an acceptable model for young people and their families• Evidence of workplace changes that supported practice of SSFC• External training & supervision; management authorising &
encouraging uptake of SSFC; teamwork and the availability of experienced family therapy practitioners/site leads were important to outcome





























