Embed Size (px)
Citation preview
IMPLEMENTING QSEN:
CHALLENGES & OPPORTUNITIES
Margaret Rowberg, DNP, APN
Jennifer Lillibridge, RN, PhD
California State University, Chico
School of Nursing
FOCUS OF PRESENTATION
Objectives Present results of faculty survey on
implementing QSEN
Discuss changes and barriers that were identified
Identify the strategies that have/can be used to train nursing faculty
SURVEY
n = 19 (35 full & part time faculty)
10 questions with fixed response or essay format
Online anonymous format using Survey Monkey
SURVEY RESULTS
Question 1 – knowledge of QSEN resources
68.4% = 13 were aware of QSEN
Question 2 – discuss resources used (only 15 answered the question)
2 faculty not aware of QSEN
staff work arounds
simulation strategies
safety & EBP materials,
reviewed KSAs
case studies

SURVEY CONTINUED
Courses where faculty are making plans for the future
Pathophysiology medical/surgical nursing course
Advanced practicum in MSN program
Simulation
Public health
Integrated theory/practicum
Leadership practicum
Fundamentals
CHALLENGES
TIME
Understanding best teaching strategies
Need more education about QSEN
Development of assignments
STRATEGIES
Picked theory & clinical leadership course as pilot
Reviewed current assignments to evaluate how and
where to incorporate QSEN competencies
Revised schedule & assignments so that each week
students would understand which competency was
the focus for that week

STRATEGIES
Include the IHI leadership modules as an assignment for the theory class
Class discussion examples – IHI forgotten team member, assignment on providing care through teamwork and collaboration (Pam Ironside), IHI human factors exercise
Incorporated a quality and safety assignment using staff workarounds (Lisa Day) as the topic into both the online theory course (paper assignment) and the on campus course (group poster assignment)
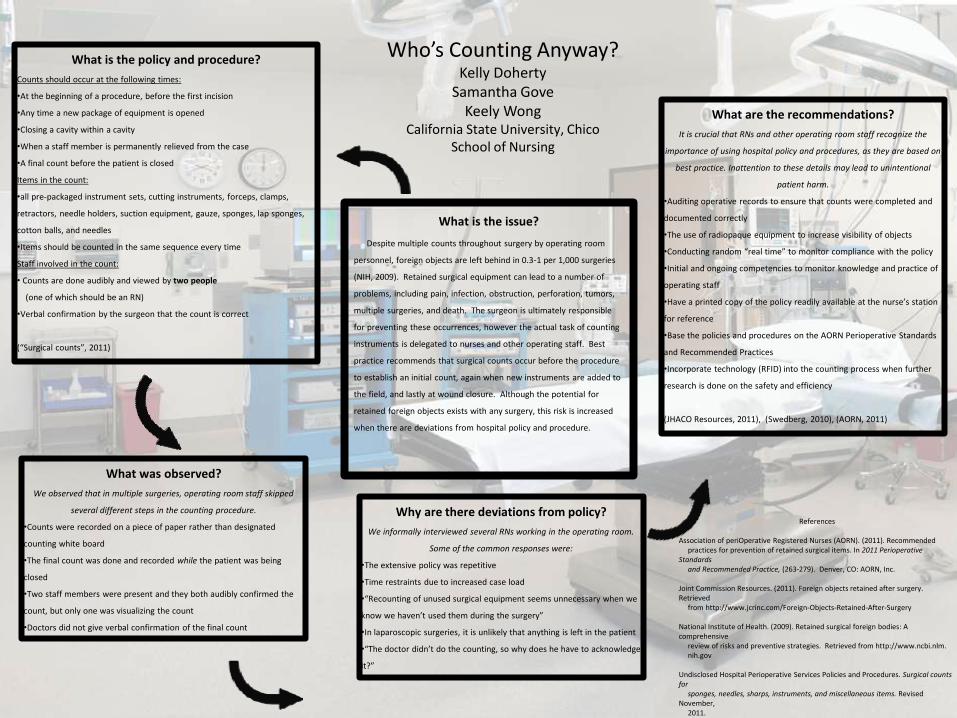
Who’s Counting Anyway? Kelly Doherty
Samantha Gove Keely Wong
California State University, Chico School of Nursing
What is the issue?
Despite multiple counts throughout surgery by operating room
personnel, foreign objects are left behind in 0.3-1 per 1,000 surgeries
(NIH, 2009). Retained surgical equipment can lead to a number of
problems, including pain, infection, obstruction, perforation, tumors,
multiple surgeries, and death. The surgeon is ultimately responsible
for preventing these occurrences, however the actual task of counting
instruments is delegated to nurses and other operating staff. Best
practice recommends that surgical counts occur before the procedure
to establish an initial count, again when new instruments are added to
the field, and lastly at wound closure. Although the potential for
retained foreign objects exists with any surgery, this risk is increased
when there are deviations from hospital policy and procedure.
What is the policy and procedure?
Counts should occur at the following times:
•At the beginning of a procedure, before the first incision
•Any time a new package of equipment is opened
•Closing a cavity within a cavity
•When a staff member is permanently relieved from the case
•A final count before the patient is closed
Items in the count:
•all pre-packaged instrument sets, cutting instruments, forceps, clamps,
retractors, needle holders, suction equipment, gauze, sponges, lap sponges,
cotton balls, and needles
•Items should be counted in the same sequence every time
Staff involved in the count:
• Counts are done audibly and viewed by two people
(one of which should be an RN)
•Verbal confirmation by the surgeon that the count is correct
(“Surgical counts”, 2011)
What was observed?
We observed that in multiple surgeries, operating room staff skipped
several different steps in the counting procedure.
•Counts were recorded on a piece of paper rather than designated
counting white board
•The final count was done and recorded while the patient was being
closed
•Two staff members were present and they both audibly confirmed the
count, but only one was visualizing the count
•Doctors did not give verbal confirmation of the final count
Why are there deviations from policy?
We informally interviewed several RNs working in the operating room.
Some of the common responses were:
•The extensive policy was repetitive
•Time restraints due to increased case load
•“Recounting of unused surgical equipment seems unnecessary when we
know we haven’t used them during the surgery”
•In laparoscopic surgeries, it is unlikely that anything is left in the patient
•“The doctor didn’t do the counting, so why does he have to acknowledge
it?”
What are the recommendations?
It is crucial that RNs and other operating room staff recognize the
importance of using hospital policy and procedures, as they are based on
best practice. Inattention to these details may lead to unintentional
patient harm.
•Auditing operative records to ensure that counts were completed and
documented correctly
•The use of radiopaque equipment to increase visibility of objects
•Conducting random “real time” to monitor compliance with the policy
•Initial and ongoing competencies to monitor knowledge and practice of
operating staff
•Have a printed copy of the policy readily available at the nurse’s station
for reference
•Base the policies and procedures on the AORN Perioperative Standards
and Recommended Practices
•Incorporate technology (RFID) into the counting process when further
research is done on the safety and efficiency
(JHACO Resources, 2011), (Swedberg, 2010), (AORN, 2011)
References
Association of periOperative Registered Nurses (AORN). (2011). Recommended practices for prevention of retained surgical items. In 2011 Perioperative Standards and Recommended Practice, (263-279). Denver, CO: AORN, Inc. Joint Commission Resources. (2011). Foreign objects retained after surgery. Retrieved from http://www.jcrinc.com/Foreign-Objects-Retained-After-Surgery National Institute of Health. (2009). Retained surgical foreign bodies: A comprehensive review of risks and preventive strategies. Retrieved from http://www.ncbi.nlm. nih.gov Undisclosed Hospital Perioperative Services Policies and Procedures. Surgical counts for sponges, needles, sharps, instruments, and miscellaneous items. Revised November, 2011. Swedberg, Claire. (2010). ORLocate RFID-Enabled system for surgical sponges and instruments gets FDA clearance. RFID Journal. Retrieved from http://www.rfid journal.com/article/view/
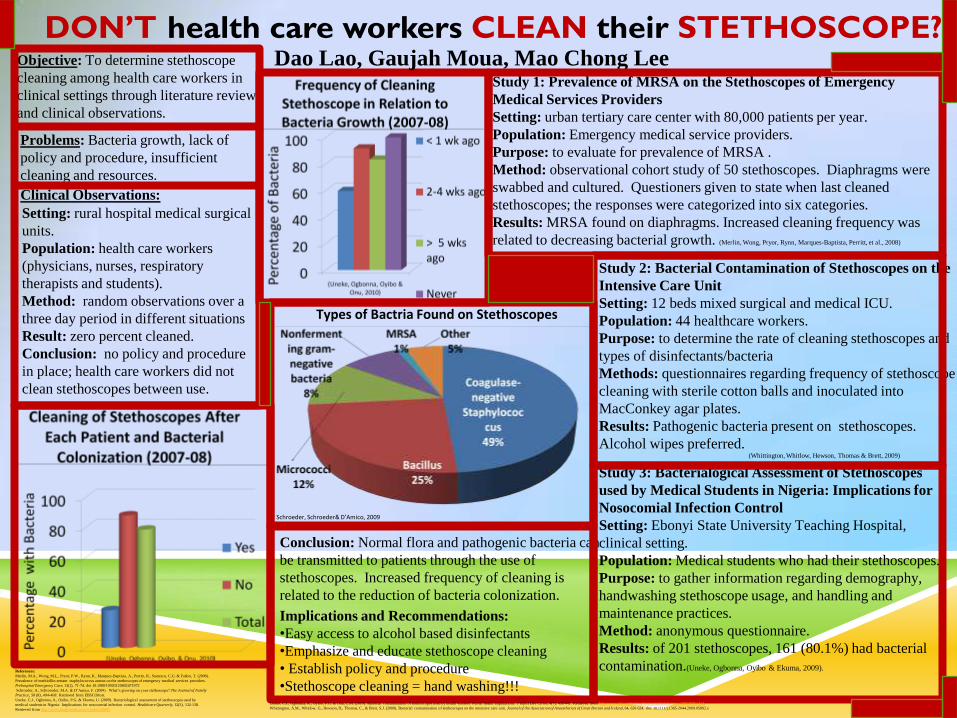
DON’T health care workers CLEAN their STETHOSCOPE?
Objective: To determine stethoscope
cleaning among health care workers in
clinical settings through literature reviews
and clinical observations.
Problems: Bacteria growth, lack of
policy and procedure, insufficient
cleaning and resources.
Setting: rural hospital medical surgical
units.
Population: health care workers
(physicians, nurses, respiratory
therapists and students).
Method: random observations over a
three day period in different situations
Result: zero percent cleaned.
Conclusion: no policy and procedure
in place; health care workers did not
clean stethoscopes between use.
Clinical Observations:
Study 1: Prevalence of MRSA on the Stethoscopes of Emergency
Medical Services Providers
Setting: urban tertiary care center with 80,000 patients per year.
Population: Emergency medical service providers.
Purpose: to evaluate for prevalence of MRSA .
Method: observational cohort study of 50 stethoscopes. Diaphragms were
swabbed and cultured. Questioners given to state when last cleaned
stethoscopes; the responses were categorized into six categories.
Results: MRSA found on diaphragms. Increased cleaning frequency was
related to decreasing bacterial growth. (Merlin, Wong, Pryor, Rynn, Marques-Baptista, Perritt, et al., 2008)
Conclusion: Normal flora and pathogenic bacteria can
be transmitted to patients through the use of
stethoscopes. Increased frequency of cleaning is
related to the reduction of bacteria colonization.
Implications and Recommendations:
•Easy access to alcohol based disinfectants
•Emphasize and educate stethoscope cleaning
• Establish policy and procedure
•Stethoscope cleaning = hand washing!!!
Dao Lao, Gaujah Moua, Mao Chong Lee
Types of Bactria Found on Stethoscopes
Study 3: Bacterialogical Assessment of Stethoscopes
used by Medical Students in Nigeria: Implications for
Nosocomial Infection Control
Setting: Ebonyi State University Teaching Hospital,
clinical setting.
Population: Medical students who had their stethoscopes.
Purpose: to gather information regarding demography,
handwashing stethoscope usage, and handling and
maintenance practices.
Method: anonymous questionnaire.
Results: of 201 stethoscopes, 161 (80.1%) had bacterial
contamination.(Uneke, Ogbonna, Oyibo & Ekuma, 2009).
Study 2: Bacterial Contamination of Stethoscopes on the
Intensive Care Unit
Setting: 12 beds mixed surgical and medical ICU.
Population: 44 healthcare workers.
Purpose: to determine the rate of cleaning stethoscopes and
types of disinfectants/bacteria
Methods: questionnaires regarding frequency of stethoscope
cleaning with sterile cotton balls and inoculated into
MacConkey agar plates.
Results: Pathogenic bacteria present on stethoscopes.
Alcohol wipes preferred.
Schroeder, Schroeder& D’Amico, 2009
(Whittington, Whitlow, Hewson, Thomas & Brett, 2009)
References:
Merlin, M.A., Wong, M.L., Pryor, P.W., Rynn, K., Marques-Baptista, A., Perritt, R., Stanescu, C.G. & Fallon, T. (2008).
Prevalence of methicillin-restant staphylococcus aureus on the stethoscopes of emergency medical services providers.
Prehospital Emergency Care, 13(1), 71-74. doi 10.1080/10903120802471972
Schroeder, A., Schroceder, M.A. & D’Amico, F. (2009). What’s growing on your stethoscope? The Journal of Family
Practice, 58 (8), 404-408. Retrieved from EBSCOhost.
Uneke, C.J., Ogbonna, A., Oyibo, P.G. & Ekuma, U. (2009). Bacteriological assessment of stethoscopes used by
medical students in Nigeria: Implications for nosocomial infection control. Healthcare Quarterly, 12(3), 132-138.
Retrieved from http://www.longwoods.com/content/20887.
Uneke, C.J., Ogbonna, A., Oyibo, P.G. & Onu, C.M. (2010). Bacterial contamination of stethoscopes used by health workers: Public health implications. J Infect Dev Ctries, 4(7), 436-441. Retrieved from http://www.jidc.org/index.php/journal/article/view/20818091/414.
Whittington, A.M., Whitlow, G., Hewson, D., Thomas, C., & Brett, S.J. (2009). Bacterial contamination of stethoscopes on the intensive care unit. Journal of the Association of Anaesthetists of Great Britain and Ireland, 64, 620-624. doi: 10.1111/j.1365-2044.2009.05892.x
FACULTY TRAINING STRATEGIES
Raised awareness of the need for incorporation of the QSEN Competencies – ie showed Lewis Blackman & Chasing Zero videos
Buy in from faculty regarding Student Learning Outcomes representing QSEN/IOM competencies.
Lewis Blackman video has been incorporated into the curriculum for student viewing
Faculty discussions about existing exercises that could be incorporated into current classes
Adopted the philosophy of a culture of safety and root cause analysis for student error
SO NOW WHAT?
New Student Learning Outcomes based on IOM Competencies
Semester meetings during summer to plan assignments
One Day workshop for part time faculty
Dedicated planning time at each faculty meeting





























