Upload
dabala-harish-reddy
View
62
Download
0
Tags:
Embed Size (px)
DESCRIPTION
ITS A GOOD MAGAZINE FOR DENTAL IMPLANTS LATEST TECHNIQUES
Citation preview
implants Vol. 3 Issue 1/2013
| user reportCamlog case studies
| case reportTapered implants and overdentures
| researchSingle molar restoration
12013the journal of oral implantology
1.5HoursCPDPoints
UPCOMING WEBINARS:
15/05/13
16/05/13
11/06/13
12/06/13
Photography is the most powerful part of practice
An Introduction to the uses of CEREC Technology for the GDP
Six Month Smiles: Leading the way in short term Ortho for GDPs
In Surgery Home Care for Implants
Over the last four years we have built a solid reputa-tion as the original and best dental webinar provider. The webinars are live and interactive to give a unique
learning experience. Interact with some of the industrys leading experts as they present the very latest in clinical practice.
smile-onhealthcarelearning
inspiring better care
Join the Dental Webinar club sign up for free:
www.dentalwebinars.co.uk
Sign up for free
I 03
Dear Reader,_Hello and welcome to the latest issue of Implants! I hope you find it both interesting
and informative.
This week Ive been catching up on the recently published Cochrane review on the impact of loading times on the success rates of implants (Esposito M, Grusovin MG, Maghaireh H, Worthington HV. Interventions for replacing missing teeth: different times for loading dental implants. Cochrane Database of Systematic Reviews 2013, Issue 3. Art. No.: CD003878. DOI: 10.1002/14651858.CD003878.pub5). The researchers looked at a number of Random Controlled Trials that looked at loading implants immediately, after six weeks (early) and at three months (conventionally).
According to the authors, Overall there was no convincing evidence of a clinically important difference in prosthesis failure, implant failure, or bone loss associated with different loading times of implants. This I find most interesting, as there are many who would lean very heavily on the evidence that you should always wait three months before loading and would be very reticent to change that view; or am I being unfair?
If you would like to read the full review, go to http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003878.pub5/full and let me know your thoughts.
Until next time
Lisa Townshend
Group Editor, Implants
implants 1_2013
Please contact your local BIOMET 3i Sales Representative or visit us online at
www.biomet3i.com to learn more.
Aforementioned have financial relationships with BIOMET 3i LLC resulting from speak-ing engagements, consulting engagements and other retained services.
The 3i T3 Implant* is designed to deliver
aesthetic results through tissue preservation.
Contemporary hybrid surface design with multi-level topography; media-blasted on the threaded region and dual-acid etched on the collar region
preservationBY DESIGN
Optimized aesthetics with as little as 0.37mm of bone recession1
Higher seal strength as compared to the competitive average2,3Seal integrity test was performed by BIOMET 3i on December 2011. Testing was done under testing standard ISO 14801. Five (5) BIOMET 3i PREVAIL Implant Systems and five (5) of three (3) competitors implant systems were tested. Bench test results are not necessarily indicative of clinical performance.
PREVAIL is a registered trademark of BIOMET 3i LLC. 3i T3, 3i T3 Implant design, Preservation By Design and Providing Solutions - One Patient At A Time are trademarks of BIOMET 3i LLC. 2012 BIOMET 3i LLC.
Seal IntegrIty2,3
Integrated Platform SwItchIng
multI-level Surface toPograPhy
Introducing the
1. stman PO, Wennerberg A, Albrektsson T. Immediate Occlusal Loading Of Nanotite Prevail Implants: A Prospective 1-Year Clinical And Radiographic Study. Clin Implant Dent Relat Res. 2010 Mar;12(1):39-47.
2. Lazzara R. Dental Implant System Design and the Potential Impact on Long-Term Aesthetics: A Review of the 3i T3 Tapered Implant. ART1193EU 3i T3 White Paper. BIOMET 3i, Palm Beach Gardens, Florida, USA.3. Suttin Z, Towse R, Cruz J. A Novel Method for Assessing Implant-Abutment Connection Seal Robustness.
BIOMET 3i, Palm Beach Gardens, Florida, USA. Poster Presentation, Academy of Osseointegration, 27th Annual Meeting; March 2012;Phoenix, AZ. http://biomet3i.com/Pdf/Posters/Poster_Seal%20Study_ZS_AO2012_no%20logo.pdf. Testing done by BIOMET 3i, Palm Beach Gardens, FL; n = 20.
*The 3i T3 Implant is not yet available for sale in the U.S.
T3 60x255.indd 1 14/01/13 16:07
04 I
I content _ implants
I editorial03 Dear Reader
_Lisa Townshend
I news
06 News
I events
07 Speaker announced for CIC 2013
I case report08 Immediate loading with a Straumann Bone Level
Implant after a horizontal tooth fracture in the aesthetic zone _Albert Barroso
I user report11 Implantology The Camlog way _Sunny Kaushal
I case report22 Immediate functional loading of the edentulous mandible _Suheil M Boutros
I research26 Single molar restoration wide implant versus two conventional _Amr Azim, Amani Zaki, Mohamed El-Anwar
32 Impression and registration for full-arch implant dentures _Gregory-George Zafiropoulos
I industry report38 Fixed full arch metal-free prosthesis on four SHORT implants _Mauro Marincola, Vincent Morgan, Angelo Pertuini, Stefano Lapucci
I product spotlight
43 Broaden your BioHorizons _Maurice Salama
manufacturer news44 Manufacturers news
I diary dates48 2013/International/UK
I about the publisher49 _ Guidelines for submission 50 _ Imprint
implants 1_2013
page 23
page 27 page 33 page 38
page 9 page 11
Sirona Dental Systems, Lakeside House, 1 Furzeground Way, Stockley Park, Heathrow, London UB11 1BD
sirona.com 0845 0715040 [email protected]
With the ORTHOPHOS XG family you can achieve
Highest level of Image quality for panoramic, cephalometric & 3D images
Crystal clear 2D images due to caesium iodide scinitilator material
Reduction of metal artifacts with innovative MARS software
HD 3D-sensor and smaller field of view for endodontics
Low noise and high contrast for a reliable diagnosis
Easy patient positioning
Guided surgery
Enjoy every day. With Sirona.
Brilliant imaging quality from Sirona.
With the ORTHOPHOS XG family you can achieve Highest level of image quality for panoramic, cephalometric & 3D images Crystal clear 2D images due to caesium iodide scinitilator material Reduction of metal artifacts with innovative MARS software HD 3D-sensor and smaller fi eld of view for endodontics Low noise and high contrast for a relaible diagnosis Easy patient positioning Guided surgeryEnjoy every day. With Sirona
06 I
I news_ implants
implants 1_2013
_The Association of Dental Implantology Dental Nurses Courses have been developed in response to the increased role played by dental nurses in supporting im-plant clinicians.
Attendees begin with the Original Dental Nurses Course, which aims to increase the understanding of den-tal implantology to dental nurses. This course provides dental nurses knowledge and confidence to support the operator with surgical implant placement and subsequent restorative appointments.
Delegates who move onto the Advanced Dental Nurses Course have the chance to learn complex surgical nurs-ing techniques involved in implant placement including, sinus lifts, bone grafting, socket preservation and soft tis-sue augmentation. The course has been designed to en-
courage confidence in their ability to assist throughout implant procedures, allowing the clinician to focus on the task in hand.
Dr Simon Wright, Director of Education at the ADI says, We feel it is crucial that dental nurses are highly trained to ensure that implant patients receive expert treatment. Clinicians are giving them more responsibility in many dental practices and the ADI Dental Nurses Courses are the ideal way to help them develop their skills.
Both courses are priced at a competitive 150. The Original course takes place on Saturday 28 September 2013. The Advanced course takes place on and Saturday 23 November 2013. Visit www.adi.org.uk/nurses_courses or call the Association on 020 8487 5555.
Dental nurses to benefit from ADI training
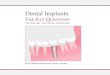
_Dental techniques to modify the alveolar ridge have been around for many years, often as a means of support for dentures. As dental implants have now become com-mon procedures, so has pre-implant preparation of the bone. The ridge-split procedure is one such method of wid-ening and augmenting the alveolar ridge that is finding re-newed interest.
The Journal of Oral Implantology presents a detailed de-scription of the alveolar ridge-split procedure, supplemented by photographs. The alveolar ridge is the bony ridge on both the upper and lower jaws that contains the sockets of the teeth. Establishing an alveolar ridge of proper dimensions has become essential with the advent of root-form endos-seous dental implants, the most common type of implants.
The ridge-split procedure described in this article is a form of ridge widening or augmentation. In cases of narrow alveolar ridges, it has proven to be consistently successful. Use of this minimally invasive technique has many advan-tages in the pre-prosthetic stage of dental implants. Low risk of inferior alveolar nerve injury, less pain and swelling, and no need for a second surgical site as donor are among
the benefits.
Because of differences in bone density, the ridge-split technique requires a single surgical stage in the maxilla, or upper jaw, and a two-stage approach in the mandible. The two stages of mandible surgery consist of corticotomy, a bone-cutting procedure, followed by splitting and grafting performed threefive weeks later. The staged approach of the ridge-split procedure has shown a higher implant suc-cess rate and better buccal cortical bone preservation.
A practitioners experience is an important component of this technique. This form of surgery modifies the con-figuration of the bone and is usually performed in a closed fashion and uses a tactile sense. The authors emphasise the need for careful manipulation of the thin ridge, knowledge of precise surgical principles, and specialised training.
Full text of the article, Horizontal Augmentation Through the Ridge-Split Procedure: A Predictable Surgical Modality in Implant Reconstruction, Journal of Oral Implantology, Vol. 39, No.1, 2013, is available at www.joionline.org/doi/full/10.1563/AAID-JOI-D-12-00112.
Established ridge-split procedure offers new application in dental implant surgery
events_ CIC 2013 I
I 07implants 1_2013
_On 17th and 18th May 2013, Healthcare Learn-ing; Smile-on will be presenting the 10th Clinical In-novations Confer-ence, in conjunc-
tion with The Dental Directory and the AOG. The widely anticipated event will be held in the Millennium Gloucester Hotel in Kensington, London, attracting hundreds of dental professionals in their quest to remain abreast of the very latest developments in the industry.
A selection of world-class speakers has been confirmed to attend this years event, taking delegates to the very cut-ting-edge of the profession.
One of these is Dr Shakeel Shahdad (pictured). Dr Shahdad is a registered spe-cialist in Restorative Dentistry, Periodon-tics, Prosthodontics and Endodontics, as well as a consultant and Honorary Clini-cal Senior Lecturer in Restorative Den-tistry at The Royal London Dental Hos-pital and Queen Mary University, Barts and The London School of Medicine and Dentistry. In addition, Dr Shahdad is a Fellow of the International Team for Im-plantology (ITI) and a Diplomat of the Brit-ish Society of Oral Implantology, all the while running a multi-specialist referral practice in the West End of London.
Dr Shahdad will be speaking on behalf of Straumann at the event, discussing Beauty or the Beast? Tissue-level im-plants in aesthetic zone.
Osseo-integration of implants has become a well established technique, and the focus is now on achieving ideal aesthetics, explains Dr Shahdad. Long-term maintenance of soft tissue aesthet-ics around implants is a challenge, and we are only now coming to understand it better. Factors that influence peri-implant bone remodelling and timing of implant placement have a profound af-fect on labial bone maintenance.
My presentation at CIC 2013 will be based on current research findings, and will aim to demonstrate and highlight the important surgical and restorative dimensions for predictably achieving and maintaining aesthetically optimised implant restorations. Emphasis will be placed on integration of biological prin-ciples into planning and decision-mak-ing in aesthetic implant dentistry. I will also present the arguments for Tissue or Bone level, Immediate or Delayed place-ment._
Speaker Announced for Clinical Innovations Conference 2013
17th and 18th May 2013, Millennium Gloucester Hotel, London
implants
For more information about Clinical Innovations Conference 2013 and to book your place call 020 7400 8989, email [email protected] or go to www.clinicalinnovations.co.uk
_contact
I case report_ aesthetic placement
08 I implants 1_2013
_Patient history
A 38 year-old non-smoking woman, in good general health and with high aes-thetic demands, presented at our dental office with mobility of tooth #12 (Fig 1). After clinical and radiological examina-tion a horizontal fracture near CEJ (ce-ment enamel junction) was detected (Figs 1-4). Clinical examination showed class III mobility of the crown of #12. Aesthetic parameters were not altered. The buccal bone plate was not affected (Fig 2). The patients plaque control was adequate and no periodontal disease or periapical infection was detected (Fig 4).
_Treatment planning
It was not possible to prepare the tooth for restoration with a single crown due to the absence of ferrule. The short length of the root would lead to an un-satisfactory crown-root ratio in case of orthodontic extrusion, and crown lengthening was not indicated in this case because of aesthetic concerns. For
these reasons tooth #12 was consid-ered hopeless. According to the options proposed by the ITI group in terms of implant placement timing after tooth extraction, the present situation would correspond to the Type I classification. Though the lip line is high, a medium-thick biotype, the lack of infection and a width of 1mm or more of the buccal bone wall (as revealed by computerised tomography) permits placing the implant immediately after tooth extraction.
_Surgical procedure
A very accurate root extraction was performed to keep the buccal plate in-tact (Fig 5). After verifying the integri-ty of the socket walls, the implant bed was prepared without flap elevation (Fig 6). We know that this approach - leaving the periostium attached to the bone - minimises the remodelling of the alveolar ridge. A Straumann Bone Level Implant with SLActive sur-face (Fig 7) was palatally positioned. The filling of the vestibular gap was
Immediate loading with a Straumann Bone Level Implant after a horizontal tooth fracture in the aesthetic zoneAuthor_Albert Barroso
Fig. 1 Fig. 2 Fig. 3 Fig. 4
case report_ aesthetic placement I
I 09implants 1_2013
done with Straumann BoneCeramic which helps to preserve the horizontal dimension of the ridge and, to some degree, the vertical dimension (Fig 8).
_Immediate temporary restoration
An immediate provisionalisation was done by an adhesive-fixed provisional with the crown of the recently extracted tooth #12 used as a Maryland bridge. Seven days after the extraction and immediate implant placement the tis-sues around the zone look completely healthy (Fig 9). This not only permitted providing the patient with an immedi-ate aesthetic fixed provisional but also to maintain the adequate gingival ar-chitecture during the osseointegration period.
_Final restoration
After a healing period of six to seven weeks an adequate gingival architec-
ture was already achieved by the adhe-sive immediate provisionalisation (Figs 10&11). At this time a Straumann NC Cementable Abutment with a mini-mally invasive approach is connected and screwed in at 20Ncm torque (Figs 12&13). By applying this protocol the abutment will not be disconnected, al-lowing the soft tissue to accommodate to the ideal apico-coronal position and minimising its possible future recession.
With a periapical radiograph we checked the adequate fit of the abut-ment to the implant connection and confirmed maintaining of the mesial and distal bone around the implant (Fig 14). The preparation of the definitive abutment was done intraorally (Fig.15) and after this the definitive impres-sion was taken. A new provisional was cemented to the definitive abutment to maintain adequate soft tissue aes-thetics (Figs 16&17). A metal-ceramic crown was prepared by the laboratory
Fig. 5 Fig. 6 Fig. 7 Fig. 8
Fig. 9 Fig. 10 Fig. 11
Fig. 12 Fig. 13 Fig. 14 Fig. 15 Fig. 16
10 I
I case report_ aesthetic placement
implants 1_2013
(Figs 18&19) and adapted to the mouth. Immediately after cementation, the in-terproximal areas were not fully filled by soft tissue (Fig 20).
After some weeks, the integration of the implant restoration to the neigh-bouring teeth and the soft tissue was optimal (Fig 21). Aesthetic parameters were achieved for medium and pro-nounced smiling of the patient (Figs 22&23). The CBCT taken two years after rehabilitation shows the maintenance of an adequate buccal bone width which will ensure the correct position of the soft tissues over time (Fig 24).
_Conclusion
Patients nowadays demand less inva-sive surgery, the shortest healing time possible and optimal aesthetic results. Clinicians, on the other hand, are not only looking to satisfy their patients expectations, but also to obtain predict-able long-term results. Both needs can only be satisfied by performing accurate planning followed by an adequate exe-cution and by using implant designs and biomaterials that minimise the remodel-ling of the surrounding tissues._
implants_author infoDr. Albert BarrosoDegree in dentistry and Master in Implantology from the Universitat In-ternacional de Catalunya/Spain. Private practice in Girona, specialised in Implant Dentistry and Oral Surgery. Lecturer at the
International Master Course in Oral Implantology at the Universitat Internacional de Catalunya. ITI Member.
www.clinicabarroso.com
Fig. 17 Fig. 18 Fig. 19
Fig. 20 Fig. 21 Fig. 22
Fig. 23
Fig. 24
I 11
user report_ Camlog I
implants 1_2013
_With well over a thousand implant systems currently on the market there is a lot of choice when it comes to pick-ing the right one to put in your practice. After extensive experience with a vari-ety of systems dating back to the mid 1990s, I recently began placing Camlog dental implants, developed by Dr. Axel Kirsch. This was after seeing the system being extensively used in Germany by some of my colleagues. I could clearly see the merits of the system along with the final results being produced.
_Surgical
The system is well thought out and has all of the features that most of the widely used systems have. The surgical kit is incredibly easy to use with a logical colour coded drilling sequence. An at-tractive design feature is the incorpora-tion of removable depth stops for all the burs. These stops slide on and off easily,
making maintenance simple while fit-ting well to the bur shank. The profiling drills are not end-cutting, so they will follow the pilot hole closely.
The combination of these two features acts as a failsafe, which is especially neat for the inexperienced. I found from my mentees, that this was a big plus in their minds.
_Benefits at a glance
One surgical set for both implant types
Colour-coded instruments arranged in the surgery set in logical order of use
Depth stops and laser markings for safe and individual implant bed prepa-ration
Special design of multiple-use drills for atraumatic, efficient and accurate
Implantology The Camlog Way Author_Sunny Kaushal
Fig. 1 Fig. 2 Fig. 3
I user report_ Camlog
12 I implants 1_2013
preparation
Implant packaging includes cover screw for submerged healing
There are two implant types in the Camlog system:
CAMLOG Implants: The heart of the CAMLOG Implant Systems is the inno-vative implant-to-abutment connection, known as the Tube-in-Tube. The posi-tive press fit of the highest precision and anti-rotation stability allows the simple and durable prosthetic rehabilitation of single crowns and bridges as well as a secure and lasting screw connection.
As a result of this positive press fit and the specially designed cams of the Tube-in-Tube connection, all forces
acting on the connection are distributed in an ideal manner. The abutment screws are minimally loaded and only have a holding function. Therefore, screw loos-ening or screw fractures are practically eliminated. Clinical results confirm these outstanding properties. (Fig 1)
Tube-in-Tube connection Ben-efits at a glance
Precise, anti-rotational positive lock-ing allows simple and durable pros-thetic connections
Three grooves (implant) and three cams (abutment) enable clear, secure and fast positioning of abutments
Comparative studies with other well-known implant systems have dem-onstrated that the CAMLOG connec-tion yields excellent results for fit and accuracy
CONELOG Implants - The CONELOG implant is equipped with a conical (7.5) connection combined with a three groove index system. This gives all the benefits of the tried and tested conical connection and is my personal preference.
The CONELOG abutments are conical apically and have three cams which slot effortlessly in to the implant to form a
Fig. 4 Fig. 5
Fig. 6
Best ever value cone beam CTVeraviewepocs 3D R100 & F40
Up to three times the image detail of other 3D X-ray systems Revolutionary R100 Reuleaux triangle full arch fi eld of view
Compact, versatile and affordable
Extra clarity for implantology, endodontics and oral surgery
Focus on the anatomy you need to see
Up to six fi elds of view from 40mm to R100 Reuleaux arch
Confi dence of high defi nition, distortion-free radiographs
High speed, high quality, low dose imageEasy and accurate automatic scout positioningMulti-layer panoramic images
Up to three times the image
The Dental Imaging Experts Comprehensive service and support plans Independent specialists in digital X-ray systems
Telephone: 0845 602 4944Email: [email protected]
FREE demonstration call 0845 388 3380
or email [email protected]
See what youre missing
www.thedentalimagingcompany.co.uk
NEW
updated Conebeam A4 advert 9280.indd 1 17/10/2012 10:46
14 I
I user report_ Camlog
implants 1_2013
Fig 9_Post-operative radiograph at
the time of cementation
positive connection. The abutment does not cover the implant shoulder, thereby, offering integrated platform switching.
Conical Connection - Benefits at a glance
Precise, self-locking anti-rotational conical implant/abutment connection
Integrated platform switching
Proven CAMLOG indexing makes abut-ment positioning simple, fast and accu-rate
Accurate and tight microbial seal
Implant Surface - Benefits at a glance
Sand-blasted, acid etched Promote surface for fast osseointegration
Six weeks healing time in good bone
quality
Scientifically documented, clinically proven
The following case studies demon-strate the surgical and prosthetic flex-ibility of the Camlog system from cli-nicians who understand the need for a reliable and user friendly system.
_Case Study 1
Dr Marcus Gambroudes BDS (U. Birm) (Fig 2) is a principal dentist at Cape Road Dental Practice & Implant Centre in War-wick and director of The Warwickshire Oral Surgery Clinic, where he receives re-ferrals for both simple and complex im-plant cases.
Marcus is a Committee Member of the Association of Dental Implantology (ADI) and an active member of the Interna-tional Team for Implantology (ITI)
His main area of interest is in guided surgery and immediate load. He also works alongside Consultant Oral and Maxillofacial Surgeon Mr Sat Parmar of-fering treatment under general anaes-thetic.
This 67-year-old lady was referred to me with a view to replacing her failing upper incisors with dental implants. This was to include replacement of her up-per right canine that was lost some time ago and being replaced with a badly de-
Fig. 7
Fig. 8 Fig. 9 Fig. 10
I 15
user report_ Camlog I
implants 1_2013
signed cantilever bridge.
Her medical history was clear and she had a heavily restored dentition that was otherwise well maintained. Her oral hygiene was excellent. (Fig 3)
Following a full clinical and radio-graphic examination I opted to extract all four incisors with immediate implant placement. In this case, I chose to re-place each tooth with a dental implant. Not something I would routinely do, however, I was concerned about the long-term prognosis of some of her up-per posterior teeth and this would give me the option of creating a reduced dental arch, with minimal future inter-vention should the need arise.
The sockets were thoroughly debrided and implant osteotomies were prepared to engage the palatal shelf and ensure good primary stability (Fig 4). All four sites were prepared to receive 3.8mm x 11mm Conelog Implants. The implants were placed and covered with the clo-sure screw provided. Any local defects were augmented with Bio-Oss particles and a Bio-Guide membrane was used to stabilise the graft material. (Fig 5)
The healing was uneventful and the implants were uncovered after approxi-mately 12 weeks. Large wide body heal-ing caps were inserted to commense site development. This was followed by open-tray pick-up impressions two weeks later. (Figs 6&7)
The laboratory produced four cast abutments. These were milled parallel and a five-unit fixed porcelain fused to metal bridge was constructed as the de-finitive restoration. This was cemented in place to achieve an excellent final re-sult. (Figs 8-10)
I have been placing and restoring CAMLOG implants for several years with great success, due to its precision and simplicity in both the surgical and re-storative aspects. The system also offers complete versatility with terrific afford-ability, without compromise. CAMLOG has well over 10 years history of use and clinical studies to back it up. For my pa-tients, I want to provide the best treat-ment and materials I can.
_Case Study 2
Andrew Chandrapal BDS MFGDP(UK) DPDS(Bris) MClinDent(Pros) qualified from Birmingham University and rapidly progressed to achieve further qualifica-tions and training which form the basis of his special interests, dental cosmetics, bonding rehabilitation and management of wear. Andrew works with eminent col-leagues in various disciplines of den-tistry to create smiles that not only look naturally outstanding but also function efficiently and comprehensively.
Fig. 11 Fig. 12
Fig. 13
16 I
I user report_ Camlog
implants 1_2013
Andrew has gained knowledge in all aspects of restorative disciplines and continues to update his knowledge with international studies on a regular basis. His interests and skills have led to a focus on prosthodontic interfaces and com-posite bonding.
He is Chair of communications on the Board of Directors for the British Acad-emy of Cosmetic Dentistry and a long-standing member of the AACD, the In-ternational Team for Implantology, the Association of Dental Implantology and the British Society of Occlusal Studies. He is also an educator to other dentists and key opinion leader to the industry within the disciplines of aesthetic den-tistry, treatment planning and compos-
ite resin artistry. (Fig 11)
All lab work for Andy Chandrapal is credited to Allport and Vincent Dental Laboratory. Monument Business Park, Warpsgrove Lane, Chalgrove, Oxford. OX44 7RW
This lady was presented with ad-vanced periodontal disease affecting all her remaining teeth and was looking for a fixed solution. The first stage in the treatment process was to remove all the remaining teeth and provide convention-al upper and lower full dentures. (Fig 12)
Following a healing period of approxi-mately three months the patients exist-ing dentures were relined and duplicat-ed to form radiographic stents. This was done using a mixture of 10-15 per cent Barium Sulphate in the base acrylic and radiopaque teeth (SR Vivo TAC and SR Ortho TAC by Ivoclar Vivadent). The pa-tient was then referred to have CT scans of both jaws. (Fig 13)
The digital data obtained from the scans was then used to plan the posi-tions of the Camlog implants and sent to a specialist laboratory for surgical drilling guides (Camlog Guide) to be produced. There was sufficient bone for
Fig. 14 Fig. 15 Fig. 16
Fig. 17
2012
2010 Preferred Products
Often times, compromises have to be made when develo-ping impression materials. Because normally the rheological properties of stability and good flow characteristics would stand in each others way. DMGs Honigum overcomes these contradictions. Thanks to its unique rheological active
matrix, Honigum yields highest ratings in both disciplines. We are very pleased to see that even the noted test institute The Dental Advisor values that fact: Among 50 VPS Honigum received the best clinical ratings* www.dmg-dental.com
honigum.Overcoming opposites.
* The Dental Advisor, Vol. 23, No. 3, p 2-5
AZM_Honigum_DeEnItFr_1203.indd 1 02.04.12 09:47
18 I implants 1_2013
I user report_ Camlog
six implants in the upper jaw and four interforaminal implants in the lower (Camlog Guide Screw Line Implants, Promote Plus). The laboratory also pro-vided the provisional acrylic bridges to immediately load the implants after placement.
With the planning complete the pa-tient returned for surgery. This was car-ried out under local anaesthetic, and in-volved securing the surgical guide with small pre-determined screws followed by preparation of the implant beds with the corresponding guided drills. (Fig 14) The upper jaw was completed first, followed by the lower. The provisional acrylic bridges were then secured to the implants.
The provisional bridges were left in
situ for approximately six months before being removed and impressions taken for the definitive bridgework. Duralay verification jigs were used to ensure the accuracy of the impressions. (Fig 15)
The definitive, screw retained, bridg-es were constructed from a milled bar overlayed with acrylic. The patient was delighted with the result. (Figs 16-18)
The CAMOG system was introduced to me around three-four years ago when I found more and more indications for finding a more economical solution to restoring edentulous arches. After looking into CAMLOG implants and their restorative versatility together with the simple system of placement I trained up on CT guided implant placement and found the guided CAMLOG implants to be of perfect application to my needs.
I now use CAMLOG implants for most of my surgical and restorative cases. My laboratory technician based in California is also very comfortable with the system resulting in superior technical results as well as the simplicity and versatil-ity of placement. It appears to be a well researched and documented system to which I have found the product support to also be very good.
_Case Study 3
Marc Northover (Fig 19) is consid-ered to be one of the UKs leading Clini-cal Dental Technicians, where for the last decade he has worked as an opin-ion leader on behalf of an international dental organisation, offering master classes and one-to-one mentoring to up and coming Clinical Dental Technicians. Marc regularly teaches on courses for dental professions in the UK and abroad on his chosen topic of complete dentures and continues to work very closely with
Fig. 18
Fig. 19 Fig. 20
I 19
user report_ Camlog I
implants 1_2013
the UKs leading Dentists, Dental Techni-cians and Clinical Dental Technicians as part of the network of Changing Faces Denture Clinics.
Marc graduated from the Royal Col-lege of Surgeons, England in 2007 with a Diploma in Clinical Dental Technol-ogy and was a founding advisory board member of British Association of Clinical Dental Technology and remains an ac-tive member today. Marcs profession-alism, patient care and expertise were recognised at the annual Dental Awards 2009 and 2010 where he was awarded Clinical Dental Technician of the year for two consecutive years.
He practices as a CDT at Changing Faces Denture Clinic, Birmingham, where working with Dental Practices that share his vision, he offers the high-est standards of care possible as part of a multi-disciplinary team. Marc is a regular delegate at international confer-ences and has a particular interest in the role of dental implants to assist denture stabilisation.
This delightful 56-year-old lady pre-sented to me complaining that she wasnt happy with the appearance of her teeth and she couldnt tolerate wearing dentures. She had had some teeth ex-tracted a short time before and was giv-en a set of immediate partial dentures that were poorly fitting and causing a lot of discomfort. (Fig 20)
The patient had obvious on-going is-sues with her remaining teeth and was referred to a colleague for a full exami-nation. It was clear that all the remain-ing teeth needed to be extracted. This was duly carried out and the patient was constructed a set of transitional full upper and lower dentures whilst her mouth healed. This was a very positive step forward for the patient however she was still experiencing some diffi-culty retaining her new teeth, especially the lower set.
After a lengthy discussion about her options, she opted to proceed with im-plant supported over dentures. This tra-ditionally constitutes a minimum of four implants in the maxilla and two in the mandible. This option would also allow me to uncover the patients palate and increase her taste and temperature per-
Fig. 21 Fig. 22
Fig. 23
20 I
I user report_ Camlog
implants 1_2013
ception.
Four Conelog Implants were placed in the maxilla and two in the mandible. Even distribution of the maxillary im-plants is essential to ensure adequate retention and the distribution of occlu-sal forces.(Fig 21)
After a healing period of three months the implants were uncovered and Loca-
tor Attachments (Zest Anchors) were torqued on. (Fig 22)
This was followed by construction of a new set of implant retained overden-tures. (Figs 23&24)
I have found working with the Camlog company extremely refreshing as have my colleagues. They are a fast moving and forward thinking set up who have embraced the modern way of communi-cation, back up and teaching. I find their on-line blog service Camlog Connect extremely useful. The platform demon-strates case studies from international clinicians via videos, pictures and we-binars. There is also an excellent iPad/iPhone App which makes all the infor-mation required at your fingertips._
Fig. 24
_About the author
Sunny Kaushal BDS (U. Birm) Dip Imp Dent RCS (Eng) MSc (U. Lond) is the principal dentist at Chic Teeth in Birmingham and has more than 16 years experience in dental implant surgery and restoration. He is also an implant surgeon at the Harley Street Oral Reconstruction Cen-tre. He was an elected Committee Member of the Association of Dental Implantology (ADI) and member of the British Academy of Cosmetic Dentists. He is a graduate of the Royal College of Surgeons and gained a Diploma in Implant Dentistry with an advanced certificate followed by an MSc (ImpDent) with distinction from the University of London. Sunny has a special interest in implant-retained overdentures and is a lead implant surgeon for changing faces denture clinics. He also has a passion for teaching and is an ADI mentor as well as a tutor for the highly respected Royal College of Surgeons of England. To compliment this, he actively encourages referring dentists to get involved in the restorative process and provides one to one training in all aspects of restoring implants.
implants
Celebrating 10 years of innovation
smile-onhealthcarelearning
inspiring better care
Friday 17th and Saturday 18th May 2013Millennium Gloucester Hotel, London Kensington
BOOK NOW for early booking discount
[email protected] 7400 8989
3
Speakers include:Nasser BarghiIrfan AhmadLouis MacKenzieAsh ParmarIan Buckle
22 I
I case report _ Immediate loading
implants 1_2013
_Abstract
The aim of this case report is to demon-strate the concept of immediate functional loading in the mandible using unsplinted implants to support a locator attachment-supported overdenture.
The patient was treated by placing four tapered implants in the anterior mandible. The implants were immediately loaded us-ing individual unsplinted locators to sup-port a removable overdenture. The patient was followed for 24 months. To date, none of the implants has lost osseointegration. The radiographic bone levels remain sta-ble. The patient has been able to maintain healthy soft tissue around all individual implants and indicated that she is com-fortable and is able to function well with
her overdenture. This preliminary report presents a case in which individual imme-diately functionally loaded unsplinted im-plants maintained osseointegration when used to retain a removable locator over-denture.
_Introduction
Patients with an edentulous mandible may not be able to consume a normally textured diet. As they continue to lose alveolar bone height, the dislodgement pressure by the perioral musculature on the prosthesis becomes greater than its re-tentive aspects. This can cause discomfort, sores and trauma to the mental nerve. The placement of endosseous implants into the anterior mandible is an excellent therapy for reconstruction. It helps to restore eden-
Immediate functional loading of the edentulous mandible Tapered implants & overdentures Author_Dr Suheil M. Boutros
Fig 1_Mandible at the time of
implant placement with moderate
bone resorption
Fig 2_Pre-op panoramic radiograph
Fig 3_Guiding pins at the time of
implant placement
Fig 4_Four tapered implants at
placement
Fig 5_Flap was sutured around the
locators using 4-0 vicryl suture
Fig 6_Panoramic radiograph
immediately after implant
placement
Fig 7_Occlusal view of the
processing rings
Fig 8_The processing rings were
picked up directly in the mouth
Fig. 1 Fig. 2 Fig. 3 Fig. 4
Fig. 5 Fig. 6 Fig. 7 Fig. 8
I 23
case report _ Immediate loading I
implants 1_2013
tulous patients to a normally textured diet, normal nutritional intake, better health and improved self-confidence.13
A locator-supported overdenture is a well-documented modality of treatment. The conventional method of treatment is to place the implants in a submerged two-stage approach. After allowing the implants to osseointegrate for three months, the im-plants are uncovered and the locators are delivered to support the overdenture. The concept of immediate functional loading has been documented in the mandible and the maxilla: implants are connected rigidly and immediately after placement to avoid micro-motions, which can have a negative impact on the osseointegration process.48
A higher failure rate has been reported in only very few reports in the literature about immediate functional loading of individual implants to support a mandibu-lar overdenture.9 This case report demon-strates the use of tapered implants in the mandible to immediately load and support four separate implants by means of a lo-cator-supported mandibular overdenture.
_Patient presentation
A 55-year-old female patient without any medical contra-indication for implant therapy presented with an ill-fitting, lower
complete denture that she had been wear-ing for four years. The clinical and radio-graphic findings revealed slight to moder-ate mandibular ridge resorption with an ill-fitting lower denture (Figs 1 & 2). The patient was given the option of placing four implants to support her existing lower denture. The treatment plan was accepted and included an immediate functional loading by using a locator attachment-supported mandibular overdenture.
_Surgical treatment
At the surgical appointment, following the administration of local anaesthetic, a mid-crestal incision was performed and a full-thickness flap was reflected. In addi-tion, osteotomies were prepared in type II bone. Bone taps were used to countersink the sites, after which four OSSEOTITE Ta-pered Certain implants (BIOMET 3i; 4 mm in diameter, 13 mm in length) were placed with the handpiece and hand ratchet. The implants were torqued to 35 N (Figs 3 & 4).
_Prosthetic treatment
Immediately after implant surgery, the mandibular denture was seated in the patients mouth and adjusted to provide clearance in the area of the locator(s). Four locators (4 mm in length) were torqued to 30 N (Figs 5 & 6). Following the suture
Fig. 9 Fig. 10 Fig. 11 Fig. 12
Fig. 13 Fig. 14 Fig. 15 Fig. 16
Fig 9_Occlusal view of the locators
two weeks post-implant placement
Fig 10_Buccal view of the locators
two weeks post-implant placement
Fig 11_The processing rings
were removed ten weeks post-
placement
Fig 12_The blue retention rings
were placed as the final rings
Fig 13_Occlusal view of the
overdenture in place at ten weeks
post-placement
Fig. 14_Buccal view of the
overdenture in place
Fig 15_Occlusal view of the locators
six months post-placement
Fig 16_Buccal view of the locators
six months post-placement
24 I
I case report _ Immediate loading
implants 1_2013
implants
Dr Suheil M. Boutros
Periodontal Specialists of Grand Blanc8185 Holly Road, Suite 19Grand Blanc, MI 48439, USA
_contact
of the flap with 4-0 vicryl, the process-ing rings were placed over the locators and were picked up directly in the mouth using hard self-curing acrylic (Rebase II, Tokuyama; Figs 7&8). The patient was giv-en post-operative instructions, including the use of 0.12 per cent chlorhexidine glu-conate (Peridex, Procter & Gamble) three times a day. She was furthermore pre-scribed 500mg of amoxicillin (to be taken every six hours for seven days). The patient was then informed that the implant-sup-ported overdenture was to be left in place for 48 hours. Two days later, she was seen for a follow-up visit and the healing pro-cess was uneventful. The black process-ing rings were switched to blue rings ten weeks after the placement (Figs 914).
_Follow-up and maintenance
After six months, the patient returned for another follow-up visit and all four lo-cators were torqued to 30 N (Figs 1521). It was determined that all four implants had
achieved full integration. Currently, the pa-tient is on a six-month recall to ensure the proper maintenance of the implants and the prosthesis. The last maintenance visit was 24 months post-placement and all im-plants have maintained healthy soft tissue and a stable bone level.
_Clinical relevance
With a higher demand by patients for immediate implant placement and load-ing, the use of tapered implants can help achieve quick, economic and predictable results without having to use a rigid (bar) attachment, since they a provide high de-gree of primary stability._
Editorial note: A complete list of refer-ences is available from the publisher.
Fig. 17 Fig. 18 Fig. 19
Fig. 20 Fig. 21
Figs 17-20_Retorquing the locators
to 30 N six months post-placement
Fig 21_Final panoramic radiograph
six months post-placement
THE NEW POWERHOUSE IN IMPLANT DENTISTRY
Trusted implant systems
Prosthetic digital innovation
Practice growth support
Clinical skills development
Why not join us? www.dentsplyimplants.co.uk 0845 450 0586 [email protected]
Helping you succeedRLAX
A4 Dentsply ad Implants mar13 runner.indd 1 07/02/2013 15:20
26 I
I research_ Single molar restoration
implants 1_2013
_The single-tooth restoration has be-come one of the most widely used procedures in implant dentistry.1 In the posterior region of the oral cavity, bone volume and density are often compromised. Occlusal forces are greater in this region and, with or without parafunctional habits, can easily compromise the stability of the restorations (Fig 1). 2, 3
The single-molar implant-supported res-toration has historically presented a chal-lenge in terms of form and function. The me-siodistal dimensions of a molar exceed that of most standard implants (3.75 to 4.0 mm), creating the possibility of functional overload resulting in the failure of the retaining com-ponents or the failure of the implant (Figs 2 & 3).4 Wider-diameter implants have a genuine use in smaller molar spaces (8.0 to 11.0 mm) with a crestal width greater than or equal to 8mm (Fig 4 a).5 Clinical parameters gov-erning the proposed restoration should be carefully assessed in light of the availability of implants and components that provide a
myriad of options in diameter, platform con-figurations and prosthetic connections. Many of the newer systems for these restorations are showing promising results in recent clini-cal trials.6-8 It has further been suggested by Davarpanah and others,9 Balshi and others,2 English and others10 and Bahat and Handels-man11 that the use of multiple implants may be the ideal solution for single-molar implant restorations (Figs 4 b & c).
Most standard implants and their associ-ated prosthetic components, when used to support a double implant molar restoration, will not fit in the space occupied by a molar unless the space has been enlarged (12 mm or larger).4 Moscovitch suggests that the con-cept of using two implants requires the avail-ability of a strong and stable implant having a minimum diameter of 3.5 mm. Additionally, the associated prosthetic components should ideally not exceed this dimension.2
Finite element analysis (FEA) is an engi-
Single molar restoration-Wide implant versus two conventional Author_Amr Abdel Azim, Dr Amani M. Zaki & Dr Mohamed I. El-Anwar, Egypt
Fig. 1 Fig. 2 Fig. 3
Fig. 1_Load distribution during
mastication shows marked
increase in the molar and premolar
area23
Fig. 2_Occlusal view showing a
missing first molar. The mesio
distal width is very wide and
restoration couldnt compensate it
leaving a space distally
Fig. 3_Proximal cantilever shown
radiographic view of maxillary right
first molar on standard Brnemark
implant with standard abutment
(Nobel Biocare)1
I 27
research_ Single molar restoration I
implants 1_2013
neering method that allows investigators to assess stresses and strains within a solid body.10-13 FEA provides calculation of stress-es and deformations of each element alone and the net of all elements. A finite element model is constructed by breaking a solid ob-ject into a number of discrete elements that are connected at common nodal points. Each element is assigned appropriate material properties that correspond to the properties of the structure to be modelled. Boundary conditions are applied to the model to stimu-late interactions with the environment.14 This model allows simulated force application to specific points in the system, and it provides the resultant forces in the surrounding struc-tures. FEA is particularly useful in the evalu-ation of dental prostheses supported by im-plants.13-16 Two models were subjected to FEA study to compare between a wide implant restoration versus the two implant restora-tion of lower first molar.
_Material and Methods
Three different parts were modelled to simulate the studied cases; the jaw bones, implant/abutment assembly, and crown. Two of these parts (jaw bone and implant/abut-ment) were drawn in three dimensions by commercial general purpose CAD/CAM soft-ware AutoDesk Inventor version 8.0. These parts are regular, symmetric, and its dimen-
sions can be simply measured with their full details.
On the other hand, crown is too compli-cated in its geometry therefore it was not possible to draw it in three dimensions with sufficient accuracy. Crown was modelled by using three-dimensional scanner, Roland MDX-15, to produce cloud of points or trian-gulations to be trimmed before using in any other application.
The second phase of difficulty might ap-pear for solving the engineering problem, is importing and manipulating three parts one scanned and two modelled or drawn parts on a commercial FE package. Most of CAD/CAM and graphics packages deal with parts as shells (outer surface only). On the other hand the stress analysis required in this study is based on volume of different materials.3 Therefore set of operations like cutting vol-
Fig. 4a Fig. 4b Fig. 4c
Fig. 5
Fig. 6a Fig. 6b
Fig. 4a_Radiographic view of wide
implants used to restore missing
lower first molars.1, 24
Fig. 4b_Buccal view of 2 standard
20-degree abutments on 3.5 mm
Astra Tech implants for restoration
of
mandibular right first molar.1, 24
Fig. 4c_Radiographic view of the
restoration.1, 24
Fig. 5_Crown, implants and bone
assembled in a model (FEA
software).
Figs. 6a & b_Von Mises stress on
crown (a) wide implant;
(b) two implants.
Tab. 1_Material Properties.
28 I
I research_ Single molar restoration
implants 1_2013
umes by the imported set of surfaces in addi-tion to adding and subtracting volumes can ensure obtaining three volumes representing the jaw bone, implant/abutment assembly, and crown.2 Bone was simulated as cylin-der that consists of two parts. The inner part represents the spongy bone (diameter 14mm and height 22mm) that filling the internal space of the other part (shell of 1 mm thick-ness) that represents cortical bone (diam-eter 16mm and height 24mm). Two implants were modelled one of 3.7mm diameter and the other of 6.0mm. The implants/abutment design and geometry were taken from Zim-mer dental catalogue (Fig 5).
Linear static analysis was performed. The solid modelling and finite element analy-sis were performed on a personal computer Intel Pentium IV, processor 2.8 GHz, 1.0 GB RAM. The meshing software was ANSYS ver-sion 9.0 and the used element in meshing all three dimensional model is eight nodes Brick element (SOLID45), which has three degrees of freedom (translations in the global direc-
tions). Listing of the used materials in this analysis is found in Table 1. The two models were subjected to 120 N vertical load equally distributed (20 N on six points simulate the occlusion; one on each cusp and one in the central fossa). On the other hand, the base of the cortical bone cylinder was fixed in all di-rections as a boundary condition.17-21
_Results and Discussion
Results of FEA showed a lot of details about stresses and deformations in all parts of the two models under the scope of this study. Figures 6a & b showed a graphical comparison between the crowns of the two models which are safe under this range of stresses (porcelain coating, gold crown, and implants showed the same ranges of safety). No critical difference can be noticed on these parts of the system. All differences might be found are due to differences in supporting points and each part volume to absorb load energy (equation 2).**
Generally a crown placed on two implants is weaker than the same crown placed on one implant. This fact is directly reflected on porcelain coating and the two implants that have more deflections. Comparing wide im-plant model with the two implants from the geometrical point of view it is simply noted that cross sectional area was reduced by 43.3 per cent while the side area increased by 6.5 per cent. Using one implant results as a refer-ence in a detailed comparison between the two models by using equation (1) resulted in Table 2 for porcelain coating, gold crown, implant(s), spongy and cortical bones respec-
Fig. 7bFig. 7a Fig. 8a
Fig. 7a & b_Spongy bone deflection
in vertical direction (a) wide
implant;
(b) two implants.
Figs. 8a & b_Cortical bone
deflection
in vertical direction (a) wide
implant;
(b) two implants.
Tab. 2_Results
I 29
research_ Single molar restoration I
implants 1_2013
tively.
Difference % = {One implant ResultTwo implants Result}*100 / One implant Result(1)
Spongy bone deformation and stresses (Table 2) seems to be the same in the two cases. Simple and fast conclusion can be tak-en that using one wide implant is equivalent to using two conventional implants. On the other hand a very important conclusion can be exerted that, under axial loading, about 10 per cent increase in implant side area can overcome reduction of implant cross section area by 50 per cent. In other words, effective-ness of increasing implant side area might be five times higher than the increasing of implant cross section area on spongy bone stress level under axial loading. Starting from Figure 7 a & b, slight differences can be no-ticed on spongy bone between the two mod-els results. The stresses on the spongy bone are less by about five per cent in the two implants model than the one wide diameter implant. The exceptions are the relatively in-crease in maximum compressive stresses and deformations of order 12 per cent and 0.3 per cent respectively.
The bone is known to respond the best to compressive and the least to shear stresses22, so considering the difference in compressive stresses less significant, the two implants were found to have a better effect on spongy bone. Contrarily, Figures 8a & b, showed bet-ter performance with cortical bone in case of using one wide implant over using two im-plants, that, deformations in cortical bone are less by 20 per cent while the stresses are less by about 40 per cent. The stresses and dis-placements were significantly higher in the two implant model due to having two close holes, which results in weak area in-between.
_Conclusions
This study showed various results between
cortical and spongy bone. It was expected that the maximum stresses in the cortical bone was placed in the weak area between the two implants. In addition to be higher than the case of using one wide implant. Al-though the middle part of spongy bone was stressed to the same level in the two cases, using two implants resulted in more volume of the spongy bone absorbed the load en-ergy** which led to reduction of stress con-centration and rate of stress deterioration by moving away from implants. That is consid-ered better distribution of stresses from the mechanics point of view, which may result in longer lifetime. Porcelain coating showed less stress in case of two implants, longer life for the brittle coating material is expected.
Contrarily more stresses were found on the gold crown placed on two implants due to its volume reduction (less material under the same load). This is clearly seen in in-creasing stresses on the two implants, that more load effect was transferred through the weak crown to the two implants. That showed maximum stresses in the area under the crown, while the wide implant showed maximum stresses at its tip. Looking to en-ergy** absorption and stress concentration on whole system starting from coating to cortical and spongy bone, although the stress levels found was too low and far from crack-ing danger, the following conclusions can be pointed out; the total results favour the two implants in spongy bone and the wide implant in the cortical layer, but the alveolar bone consists of spongy bone surrounded by a layer of cortical bone. Its also well known that according to the degree of bone density
Fig. 9_Strain energy = area under
stress strain curve.
Fig. 8b
Fig. 9
30 I
I research_ Single molar restoration
implants 1_2013
SPMP12245 REV C OCT 2012
make the switch
The Tapered Plus implant system offers all the great benefits of BioHorizons highly successful Tapered Internal system PLUS it features a Laser-Lok treated beveled-collar for bone and soft tissue attachment and platform switching designed for increased soft tissue volume.
For more information, contact BioHorizonsCustomer Care: +44 (0)1344 752560 or visit us online at www.biohorizons.com
increased soft tissue volume.
Laser-Lok zonecreates a connective tissue seal and maintains crestal bone
platform switchingdesigned to increase soft tissue volume around the implant connection
optimized threadformbuttress thread engineered for superior stability over microthreaded implants
restorative easeconical internal hex connection is color-coded for quick identification and component matching
the alveolar bone is classified to D1,2,3,4 23 in a descending order.
So, provided that the edentulous space after the molar extraction permits, its rec-ommended in the harder bone quality (D1,2) to use one wide diameter implant and in the softer bone (D3,4) quality two average sized implants. Therefore more detailed study to compromise between the two implants size/design and intermediate space can put this stress values in safe, acceptable, and control-lable region under higher levels of loading.
** The area under the __-__ curve up to a given value of strain is the total mechanical energy per unit volume consumed by the ma-terial in straining it to that value (Fig. 9). This is easily shown as follows in equation 2:
_Summary
Restoration of single molar using implants encounters many problems; mesio-distal cantilever due to very wide occlusal table is the most prominent. An increased occlusal force posteriorly worsens the problem and increases failures. To overcome the overload, the use of wide diameter implants or two regular sized implants were suggested. The
aim of this study was to verify the best solu-tion that has the best effect on alveolar bone under distributed vertical loading. Therefore, a virtual experiment using Finite Element Analysis was done using ANSYS version 9. A simplified simulation of spongy and cortical bones of the jaw as two co-axial cylinders was utilised. Full detailed with high accuracy simulation for implant, crown, and coating was implemented. The comparison included different types of stresses and deformations of both wide implant and two regular im-plants under the same boundary conditions and load application.
The three main stresses compressive, ten-sile, shear and the equivalent stresses in ad-dition to the vertical deformity and the total deformities were considered in the compari-son between the two models. The results were obtained as percentages using the wide im-plant as a reference. The spongy bone showed about five per cent less stresses in the two implants model than the one wide diameter implant. The exceptions are the relatively in-crease in maximum compressive stresses and deformations of order 12 per cent and 0.3 per cent respectively.
The stresses and displacements on the cortical bone are higher in the two implant model due to having two close holes, which results in weak area in-between. The spongy bone response to the two implants was found to be better considering the stress distribu-tion (energy absorbed by spongy bone**). Therefore, it was concluded that, using the wide diameter implant or two average ones as a solution depends on the case primarily. Provided that the available bone width is suf-ficient mesio distally and bucco-lingual, the choice will depend on the type of bone. The harder D1,2 types having harder bone qual-ity and thicker cortical plates are more con-venient to the wide implant choice. The D3,4 types consist of more spongy and less cortical bone, are more suitable to the two implant solution._
Editorial note: A complete list of references is available from the author.
Fig. 10
Fig. 10_Equation 2 (stress energy).
implants
Prof. Amr Abdel Azim
Professor, Faculty of Dentistry, Cairo [email protected]
Dr Amani M. Zaki
GBOI. 2009, [email protected]
Dr Mohamed I. El-Anwar
Researcher, Mechanical Engineering Department,National Research Center, [email protected]
_contact
SPMP12245 REV C OCT 2012
make the switch
The Tapered Plus implant system offers all the great benefits of BioHorizons highly successful Tapered Internal system PLUS it features a Laser-Lok treated beveled-collar for bone and soft tissue attachment and platform switching designed for increased soft tissue volume.
For more information, contact BioHorizonsCustomer Care: +44 (0)1344 752560 or visit us online at www.biohorizons.com
increased soft tissue volume.
Laser-Lok zonecreates a connective tissue seal and maintains crestal bone
platform switchingdesigned to increase soft tissue volume around the implant connection
optimized threadformbuttress thread engineered for superior stability over microthreaded implants
restorative easeconical internal hex connection is color-coded for quick identification and component matching
32 I
I research_ Impression and registration
implants 1_2013
Fig. 1a_Full denture in situ
Fig. 1b_Duplicate (DentDu)
of the interim denture
Fig. 1c_Trial of the DentDu
Fig. 2a_Placement of the DentDu
in the articulator
Fig. 2b_Pick-up impression system
On the left: titanium impression post
(placed on the implant)
On the right: plastic impression
sleeve (will be left in the impression)
_Usually, a full denture is delivered fol-lowing tooth extraction or implant insertion of a fully edentulous arch. A denture is usu-ally used until the final restoration is per-formed. A well-designed full denture should fulfill the following criteria: 1) correct verti-cal height and maxilla-mandibular relation-ship; 2) accurate occlusion; 3) appropriate choice of teeth with regard to shape, length, width and position; 4) adequate lip sup-port, and 5) proper function and aesthetics to meet the patients expectations. The final restoration should fulfill or surpass these requirements. Obtaining a correct impres-sion and accurately evaluating the interoc-clusal relationship (e.g., interocclusal dis-tance, occlusal recording and determination of the exact position of the placed implants)
are often challenging and time-consuming tasks.1
The aim of the current report is to present an impression and registration technique that allows the transfer of the interocclu-sal relationship, occlusal recording and aes-thetics that were initially applied to produce a full denture as a template for the recon-struction of the final full-arch implant.
_Materials and Methods
Following multiple extraction of a non-salvageable rest dentition and the place-ment of six dental implants in positions #4, #5, #6, #11, #12, #13, a full denture was fabricated. After the extraction sites had healed and denture sores were eliminated, the function and aesthetics of the denture was optimised. If necessary, angulations, shape and colour of the denture teeth and the shape of the denture base were cor-
Impression and registra-tion for full-arch implant dentures Author_Prof. Gregory-George Zafiropoulos
Fig.1a Fig.1b
Fig.1c Fig.2a Fig.2b
33
research_ Impression and registration I
implants 1_2013
rected (Fig 1a). The resulting denture was used by the patient until the final restora-tion was delivered. For the final restoration of the maxilla, an implant-retained denture with telescopic crowns as attachments was planned.
After the implant was uncovered, the den-ture was modified to allow sufficient space for the healing abutments. A duplicate of the denture (DentDu) was made out of clear resin (Paladur, Heraeus, Hanau, Germany, Fig 1b). A trial of the DentDu was performed and minor occlusal discrepancies were cor-rected (Fig. 1c). Bite records were taken in centric occlusion with modelling resin (pat-tern resin, GC, Alsip, IL; Fig. 1c), using the casts of the original denture. Afterwards, the DentDu was placed in an articulator and a controlling of the occlusion was made (Fig 2a) with the bite records. A pickup transfer system consisting of a titanium impression post and a plastic impression sleeve was employed (Dentegris, Duisburg, Germany, Fig 2b). The DentDu was carefully modified by creating internal clearance in the area of the implants so that it could be applied as an individualised custom tray. This permit-ted it to be fully seated when the impression posts were in place. Impressions were gen-erated by a polyether material (Impregum, 3M ESPE, St. Paul, MI). During this process, the DentDu was kept in centric occlusion using the bite records (Fig 3a).
The titanium impression posts were con-nected with the implant analogues and with the plastic impression sleeves (Dentegris), which were embedded in the impression
material (Fig 3b). A master cast was then fabricated and articulated with the help of the bite records (Fig 3c, Figs 4a & 4b).
Customisable abutments (Dentegris) were taken to fabricate the implant abut-ments. Parallelism, angulation, position and shape of the implant abutments were determined using a silicon key fabricated from a matrix of C-silicone (Zeta - labor, Zhermack SpA, Badia Polesine, Italy, Fig 5).
The dentist and the dental technician relied on two alternatives for customised abutments selection: 1) UCLA customis-able abutments (UCLA, Dentegris) for cast-ing with a gold alloy (for example, Portadur P4, Au 68.50 per cent, Wieland, Pforzheim, Germany, Fig 6a) or 2) platinum - iridium custoiable abutments (PTIR, Dentegris) for-
Fig.3a Fig.3b Fig.3c
Fig. 4a Fig. 4b
Fig. 5 Fig. 6a Fig. 6b
Fig. 3a_Taking the impression with
the DentDu. The bite records were
used to determine the exact position.
Fig. 3b_Fabrication
of the master cast
Fig. 3c_Placement of the cast
into the articulator using
the bite registrations
Fig. 4a_Master cast
Fig. 4b_The master cast is placed
into the articulator
Fig. 5_The customized implant
abutments are fabricated using
a matrix of C-silicone
Fig. 6a_Gold customized abutments
Fig. 6b_Chromium cobalt (CrCo)
customized abutments
34 I
I research_ Impression and registration
implants 1_2013
casting with a chromium cobalt (CrCo) alloy (for example, Ankatit, Anka Guss, Waldas-chaff, Germany, Fig. 6b).
After casting, the customised implant abutments were grinded, polished and served as the basis for the fabrication of electroformed puregold copings with a thickness of 0.25 mm (AGC Galvanogold, Au > 99.9 per cent, Wieland, Fig. 6c).2-4 The framework was then constructed via CAD/CAM.
To ensure proper functioning of the framework, a plastic mock-up and a tempo-rary fixed denture (TFD) were milled (ZENO-PMMA, Wieland). The customised implant abutments, the electroformed copings, the mock-up and the TFD were delivered by the dental laboratory for the next clinical ses-sion.
The abutments were transferred, posi-tioned on the implants and torqued to 35 Nm using a resin transfer key (pattern resin, GC; Figs 7a & b). From this point on, the cus-tomised abutments remained fixed in order to avoid any possible inaccuracies. The elec-troformed copings were placed on the im-plant abutments (Fig. 7c). The mock-up was
placed over the electroformed copings and the occlusion was checked with the bite re-cords (Figs. 8a & b). A final impression with a polyether impression material (Impregum, 3M ESPE) was taken with electroformed copings. The mock-up was further set up and used for the fabrication of a new (final) master cast. After the impression was taken, the TFD was fixed on the implant abutments using temporary cement (TempBond, Kerr, Orange, CA).
It was then left in place until the delivery of the final restoration (Fig 8c).
The new master cast was articulated with the help of the gold copings and the mock-up. The metal framework was milled (here: Titanium Zenotec TI, Wieland, Fig. 9a). The veneering of the superstructure was made using a light-cured indirect ceramic poly-mer (Ceramage, SHOFU, Menlo Park, CA, Figs. 9ad). The electroformed gold copings were fixed in the metal framework using a self-curing compomer cement (AGC Cem, Wieland, Fig 10).
The above-described procedures can be also performed in cases in which a fixed denture was planned for the rehabilitation of the full-arch (Figs 11a&b, Figs 12ac) and
Fig. 6c Fig. 7a Fig. 7b
Fig. 7c
Fig. 8a Fig. 8b Fig. 8c
Fig. 6c_Electroformed gold copings.
Figs. 7a & b_The customized
abutments are mounted on the
implants using a transfer key.
Fig. 7c_Electroformed gold
copings in situ.
Figs. 8a & b_Brial of the mock-up.
Fig. 8c_Temporary fixed
denture in situ
I 35implants 1_2013
research_ Impression and registration I
in cases where part of the natural dentition is periodontally stable and can be applied as abutments. In these cases, the immedi-ate full denture can be designed as a cover denture. From this cover denture, a DentDu could be fabricated and further used as de-scribed above (Figs 13ac).
Porcelain is a possible material for ve-neering of fixed-denture frameworks. If the angulation of the implants does not allow for taking impressions in the above-described way and an open-tray impression is preferable, fenestrations can be fabricated into the DentDu (Fig 14).
_Discussion
The reconstruction of the fully edentu-lous arch with implant-retained dentures necessitates thorough planning and a pre-cise and passive fit of the suprastructure. A previous study demonstrated that a passive fit between the implant superstructure and the underlying abutments is essential for the long-term success of the implant pros-
thesis.5 To achieve a passive fit, an accurate positioning of the implant replicas in the master cast must be assured. The impression technique and the splinting of the implant copings are factors which may contribute to errors in the final positioning of the im-plant analogues, thus leading to inaccura-cies in the fit of the final superstructure.5-10 Furthermore, the angulation or proximity of the implants may inhibit proper seating of the impression copings and/or caps, which may also have a detrimental effect on the registration of the implant position.11
The precise recording of the maxillo-mandibular, eg interocclusal, relationship is a prerequisite for achieving proper occlu-sion and a successful treatment outcome.1,10 The initially delivered denture allowed for the correction of the interocclusal relation-ship, tooth shape and colour and angula-tions during the entire healing period. In this way, the patient was able to acclimatise to the function and aesthetics of the denture. In the method described in this report, an accurate impression and recording of the
Fig. 9a Fig. 9b
Fig. 9c
Fig. 9d
Fig. 10
Fig. 11a Fig. 11b
Figs. 9ad_Final telescopic crown
retained implant denture, palatal;
(a), anterior teeth (b), right side (c),
left side (d).
Fig. 10_Placement of the
electroformed copings
into the frame.
Figs. 11a & b_A case of fixed
implant retained denture for the
maxilla full-arch rehabilitation: trial
of the mock-up (a) and the milled
temporary fixed denture is placed on
the abutments (b).
36 I
I research_ Impression and registration
implants 1_2013
full denture was achieved by using a du-plicate as a custom tray for the impression. Therefore, it was not necessary to repeat all the steps usually needed for recording the interocclusal relationship, eg wax-up, etc., at the time of the fabrication of the final restoration.
If an open-tray impression is preferred, only minor changes to the procedure are necessary. This method is based on a pre-vious publication.12 In cases such as this, it is advisable to fabricate two DentDus. The
impression can be taken by the first DentDu; the second DentDu is used for the remain-ing steps. Customised abutments are ap-plied instead of a bar, galvano copings allow a precise transfer coping, and secondary telescopes as well as different technologies are employed for the transfer of implant positions and for the construction of the superstructure.
Customised implant abutments allows for better angulations and shape, for im-proved occlusal force transmission from the crown to the implant and the bone, and also for facilitating the fabrication of an aesthet-ically pleasing implant-supported denture. Ways in which abutment design contributes to improved aesthetics include changes in the location of the crown and changes in the dimension and/or form of the restor-ative platform.
Additionally, features of the abutment design contribute to the health and dimen-sional stability of the soft tissue. Current attempts to objectively define implant-restoration aesthetics have focused on pe-riimplant mucosal parameters.13,14 The in-troduction of the UCLA abutment provided a custom solution for implant restorations. This direct-to-implant restoration con-
Fig. 12a Fig. 12b Fig. 12c
Fig. 13a Fig. 13b Fig. 13c
Fig. 14
Figs 12ac_A case of fixed-implant
retained denture for the maxilla
full-arch rehabilitation, right site (a),
anterior area (b), left site (c).
Figs. 13ac_Impression of a case
with natural dentition (teeth #11 and
#12) and implants. Master cast
in the articulator with a duplicate
of the over-denture in place (b).
Gold copings fixed on the remaining
teeth #11 and #12 and customised
implant abutments mounted on the
implants (both of them served as
primary telescopes (c).
Fig. 14_DentDu modified for open-
tray impression technique.
I 37implants 1_2013
research_ Impression and registration I
cept provided adaptability. Through waxing and casting, the height, diameter and an-gulations can be addressed in order to pro-vide a wide range of clinical solutions for problems associated with limited interoc-clusal distance, interproximal distance, im-plant angulations and related soft tissue responses.15
The customised implant abutments served as primary telescopes, and the electroformed copings served as second-ary telescopes in cases where a removable denture with telescopic crowns was used as the attachment. Electroformed gold copings are associated with several advantages, in conjunction with both removable and fixed restorations. The galvano-forming and elec-troforming process yielded a precisely-fitted secondary coping for the implant abutment with a gap of only 1230m. The gold elec-troformed coping saves space and is made of high-quality material.2-4 Using gold cop-ings for the impression allows for the ex-act transfer of the form, angulations and position of the inserted customised implant abutments.
With the help of the milled mock-up, the future fit of the CAD/CAM fabricated framework can be evaluated and neces-sary changes in the shape of the restoration and occlusion can be made. Making these changes on the mock-up was easier and less time consuming than making them on the metal framework itself, and it was then possible to transfer them directly to the fi-nal framework. Furthermore, the mock-up almost splinted the electroformed gold copings during the impression, allowing for the exact transfer of the abutment position. At the same time, the vertical height and interocclusal relationship were recorded. The delivery of a milled temporary restora-tion permitted a slow and non-progressive loading of the implants, which then leads to bone remodeling.16 Abutments were left in place after mounting. Combined with the
fabrication of a new cast, this further de-creased the risk of inaccuracies during the transfer process.
_Conclusion
The method described here can be used for fullarch restorations with both fixed and removable implant supported dentures. Ac-curate impressions can be accomplished and occlusion, vertical dimensions, as well as implant positions can be transferred while facilitating the full-arch restoration process. In addition, this technique resulted in a reduction of the required chair time.
Disadvantages of this technique lie in the fact that the quality of laboratory techni-cians work meets higher demands than usual, and that the clinician also needs to acquire some additional skills. Further dis-advantages of this method include the need for a highly qualified technical lab and higher technical costs relative to those as-sociated with prefabricated titan implant abutments.
To date, this method has not been applied in conjunction with immediate implant loading. However, dentists and patients have come to expect this level of rehabilita-tive accuracy, precision, long-term success and aesthetics._
Editorial note: A complete list of referenc-es is available from the publisher.
implants
Prof. Gregory-George Zafiropoulos
Blaues HausSternstr. 6140479 Dsseldorf, [email protected]
www.prof-zafiropoulos.de
_contact
38 I
I industry report _ Full arch rehabilitation
implants 1_2013
_The concept of having only four SHORT implants for the support of a fixed full arch non-metallic prosthesis (Trinia), a CAD/CAM fiber reinforced resin, was first
executed in 2010. The clinically based results performed in three different implant den-tistry centres are showing clinical success because of Trinias inherent mechanical and clinical properties. Another factor were the 360 degrees of universal abutment position-ing provided by the Implants Locking Taper connection (Bicon), which gives the oppor-tunity to use the Trinia prosthesis to orient and seat the abutments in the well of the im-plants. The Trinia framework may be covered with either customised poly-ceramic indirect composite material or by conventional den-ture teeth and resin.
We want to show how short implants have been successfully used to restore se-verely atrophic mandibles without the use of difficult bone augmentation procedures and complicated prosthetic suprastructures in the past decade.
_Material and methods
Bicon Dental implants (Bicon LLC, Boston, MA, USA) were used for the reconstruction of the case, combined with a CAD/CAM fi-ber reinforced resin framework (Trinia) and conventional denture teeth and resin pros-thesis. Bicon implants can be characterised by their special macro-structure, including a root-shaped design with wide fins called plateaus, by a sloping shoulder and by a well which holds the abutment post by means of a Locking Taper connection.1
The plateaus are of particular importance for the biomechanical performance, allowing SHORT implants with a wide diameter to be used in any position in the oral cavity. Their insertion into the osteotomy, which has been prepared using atraumatic drills rotating at 50rpm, is executed by using mechanical pressure. The countless micro-retentions cre-ated on the surface of the fine edges with the walls of the osteotomy ensure primary stabil-ity of the implant in the implant site. Further-more, the wide spaces between the plateaus avoid vertical compression on the bone walls and rapidly collect the clotted blood, allow-ing rapid bone formation without the clas-
Fixed full arch metal-free prosthesis on four SHORT implants Author_Prof. Mauro Marincola, Dr Vincent J. Morgan, Angelo Perpetuini & Stefano Lapucci
Fig 1
Fig 2 Fig 3 Fig 4 Fig 5
I 39implants 1_2013
industry report _ Full arch rehabilitation I
sic macrophagic and osteoclastic processes of bone resorption taking place. Thus well- defined bone is formed, with haversian ca-nals and blood vessels which enable continu-ous bone remodelling around the implant/bone contact surface. This ensures stability of the implant in any situation involving biome-chanical stimulus.2
The sloping shoulder is vitally important for the preservation of crestal bone after implant osseo - integration and for implant function. The Bicon implant design offers platform switching with a neck which con-verges from the widest diameter of the first plateau, to 2 or 3mm towards the crestal zone (converting crest module). In our pa-tient, we used implants 5mm in diameter, but the space taken up at crestal level is only three mm. This ensures bone augmentation above the neck, also because the implant is seated at least one mm below the crest dur-ing the first surgical stage. This allows the above structures, such as the crestal bone, periosteum and epithelium, to grow around the hemispherical base of the abutment and to give sufficient space for maintenance and the growth of the papillae.
Another important factor for obtaining long term crestal bone stability is the bacte-rial seal within the connection between im-plant and abutment. If crestal bone mainte-nance and the formation of papillae can only be achieved when the implant is placed in a subcrestal position and by platform switching at the level of the implant neck, it is also true that this situation can only be accomplished if the connection is hermetically sealed from bacterial infiltration. Without this feature, the placement of a sub-crestal implant without a bacterial seal would result in the rapid spread
of pathogens around vital structures, crestal bone, periosteum and epithelium. The result would be bone resorption well below the original crestal bone level.
Bicons locking taper is a design feature ensuring crestal bone level maintenance around an implant with a convergent slop-ing shoulder placed subcrestally.3 The Lock-ing Taper is a precise connection formed by cold welding out of two surfaces of the same material which are brought into close con-tact with pressure. In this way, the oxidation layers formed both on the abutment post and on the surface of the implant well are detached.4, 5 The prosthetic components (one-piece titanium abutments made from the same surgical grade titanium alloy as the implants) ensure maximum mechanical re-sistance and optimum biocompatibility. The subgingival hemispheric base geometry is ide-al for the stability of periimplant connective tissues.
The abutments are connected to the im-plant well by means of a post, which is 2mm, 2.5mm or 3mm in diameter. Implants which are 3.0mm and 3.5mm in diameter are suit-able for 2mm posts, while implants of a di-ameter of 4.5mm, 5mm or 6mm match with abutments with a 3mm post. All of the abut-ment posts have diameters or emergence profiles of 3.5, 4.0, 5.0 or 6.5mm, suitable for allowing a natural anatomical shape of
Fig 6 Fig 7 Fig 8 Fig 9
Fig 10 Fig 11
40 I
I industry report _ Full arch rehabilitation
implants 1_2012
For further information and details of upcoming UK courses please contact
the soft tissues. Abutment diameters are therefore independent of implant diameters, which means that any implant may host the four different abutment emergence profiles. The different emergence profiles start from the 2mm, 2.5mm or 3mm posts, placed at crestal bone level. The geometry of the abut-ments provides for platform switching even at a prosthetic level, which is of vital impor-tance in the organisation of the connecting tissue and the epithelial layer.
The supraperiosteal space involved in the shift from the connecting post diameter (23mm) to the diameter of the abutment hemisphere (36.5mm), allows a thicker and denser connecting tissue to form, resulting in the optimal preservation of the papilla. In the following case, all the selected abutments have a 3mm post, as they must connect to the 3mm wells of the 5.0 x 6.0mm implants. Abutment post heights, inclinations and di-ameters are selected in the laboratory in ac-cordance with the position of the implants relative to the anatomy of the alveolar ridge.
Trinia is a CAD/CAM multidirectional fibre reinforced resin material, which despite its light weight is capable of withstanding oc-clusal forces.
_Case report
A 52-year-old male patient, presenting a severely compromised mandibular bone, was treated with the placement of four short implants. Two SHORT implants (4.5 x 8mm) were placed bilaterally at the canine region and two ULTRA SHORT implants (4 x 5mm) were bilaterally located at the first molar re-gion (Fig 1). The implants were placed in a two-stage surgery and they were uncovered after a healing period of three months (Figs 2&3).
Clinically, the prosthetic treatment be-gan with an implant level transfer impres-sion by inserting with only finger pressure a green impression post with its corresponding acrylic sleeve into the 3.0mm implant well,
prior to recording their position by mak-ing an implant level impression with any conventional impression material (Fig 4). Upon the removal of the full arch impres-sion, green impression posts were removed from the implant wells and inserted into an implant analogue of the same colour be-fore inserting them into their correspond-ing acrylic sleeves within the impression.
Prior to the pouring of a stone model, a resilient acrylic was applied around the im-pression posts to simulate a soft tissue con-tour in the stone m