Embed Size (px)
Citation preview

UNIVERSIDADE FEDERAL DE SANTA MARIA CENTRO DE CIÊNCIAS DA SAÚDE PROGRAMA DE PÓS-GRADUAÇÃO
EM CIÊNCIAS ODONTOLÓGICAS
IMPACTO DOS FATORES SOCIOECONÔMICOS, PSICOSSOCIAIS E CLÍNICOS
NA QUALIDADE DE VIDA E NA UTILIZAÇÃO DOS SERVIÇOS ODONTOLÓGICOS EM ESCOLARES
DISSERTAÇÃO DE MESTRADO
Chaiana Piovesan
Santa Maria, RS, Brasil 2009
IMPACTO DOS FATORES SOCIOECONÔMICOS,
PSICOSSOCIAIS E CLÍNICOS NA QUALIDADE DE VIDA E
NA UTILIZAÇÃO DOS SERVIÇOS ODONTOLÓGICOS EM
ESCOLARES
por
Chaiana Piovesan
Dissertação apresentada ao Curso de Mestrado do Programa de Pós-Graduação em Ciências Odontológicas, Área de Concentração em
Odontopediatria, da Universidade Federal de Santa Maria (UFSM, RS), como requisito parcial para a obtenção do grau de Mestre em Ciências
Odontológicas
Orientador: Prof. Dr. Thiago Machado Ardenghi
Santa Maria, RS, Brasil 2009

Universidade Federal de Santa Maria Centro de Ciências da Saúde
Programa de Pós-Graduação em Ciências Odontológicas
A Comissão Examinadora, abaixo assinada, aprova a Dissertação de Mestrado
IMPACTO DOS FATORES SOCIOECONÔMICOS, PSICOSSOCIAIS E CLÍNICOS NA QUALIDADE DE VIDA E NA UTILIZAÇÃO DOS
SERVIÇOS ODONTOLÓGICOS EM ESCOLARES
elaborada por Chaiana Piovesan
como requisito parcial para a obtenção do grau de Mestre em Ciências Odontológicas
COMISSÃO EXAMINADORA:
Thiago Machado Ardenghi, Prof. Dr. (UFSM) (Presidente/Orientador)
Rachel de Oliveira Rocha, Profª Drª (UFSM) (Membro)
José Leopoldo Ferreira Antunes, Prof. Dr. (USP) (Membro)
Santa Maria, 18 de janeiro de 2010.

DEDICATÓRIA
Aos meus pais, por permitirem que este sonho se rea lizasse;
Mais do que simplesmente aqueles que me botaram no mundo, muito mais...
Os que me ensinaram MUITO de tudo o que sei e o que faço...
(Autor desconhecido)
A vocês, Pai e Mãe, muito obrigada por tudo que fizeram e fazem por mim. Obrigada
por me apoiarem sempre, muitas vezes abdicando dos seus sonhos para realizarem
os meus. Sem vocês nada disso aconteceria! Amo vocês!
Aos meus irmãos, Natiéli e Patrick , obrigada pelo companheirismo e pela paciência
que sempre tiveram comigo. Amo vocês!
Ser irmão é muito mais que simplesmente ter o mesmo sangue, ou algumas poucas
semelhanças físicas. É muito mais que qualquer coisa...
(Autor Desconhecido)

Ao Piero
Obrigada por todo amor e incentivo. Obrigada por me encorajar e me apoiar nos
momentos em que tive dúvidas. Obrigada por existir na minha vida!
Assim como o oceano
Só é belo com luar
Assim como a canção
Só tem razão se se cantar
Assim como uma nuvem
Só acontece se chover
Assim como o poeta
Só é grande se sofrer
Assim como viver
Sem ter amor não é viver
Não há você sem mim
Eu não existo sem você
Vinícius de Moraes

Agradecimentos
Primeiramente, a Deus , por me proteger, iluminar sempre o meu caminho e colocar
na minha vida pessoas certas, no lugar certo e no momento certo. Obrigada por
estar sempre ao meu lado.
“Porque aos seus anjos dará ordem a teu respeito, para te guardarem em todos os
teus caminhos”
Salmo 91:11.

Ao meu orientador, Thiago . Muito obrigada por tudo que você me ensinou até hoje.
Hoje acredito que existem pessoas inteligentes, sábias, generosas e humildes, e
você é a prova disso. Quando eu era apenas mais uma aluna da graduação, você
apareceu e me apresentou a fascinante Epidemiologia. Daí por diante, nem sei
como explicar. Simplesmente posso dizer que tive um orientador presente, que
sempre esteve disposto a me ajudar em tudo e me incentivou em todos os
momentos. Obrigada por sua dedicação e confiança. Sou uma pessoa abençoada
por ter você como meu orientador. Tenho você como um exemplo a ser seguido...
Um exemplo de pesquisador, de professor, de profissional e acima de tudo, um
exemplo de pessoa. Levarei seus ensinamentos por toda vida. Agradeço a Deus por
ter colocado você no meu caminho... Tenho certeza que esse é só o início de uma
caminhada que está muito longe de acabar! Obrigada por tudo!
Ser humilde com os superiores é uma obrigação, com os
colegas uma cortesia, com os inferiores é uma nobreza"
(Benjamin Frannklin)

Ao Prof. Dr. José Leopoldo Ferreira Antunes , da Universidade de São Paulo, por
toda ajuda nas análises deste trabalho. Muito obrigada!
Aos Professores da Clínica de Odontopediatria, Prof. Ma rta Dutra Machado
Oliveira, Prof. Leandro Osório, Prof. Juliana Praet zel , Prof. Ana Paula Mainardi
e Prof. Maurício Mezzomo , pelo acolhimento na clínica sempre que precisei.
Aos Funcionários da Clínica de Odontopediatria , por todos os momentos de
descontração.
À Coordenação e Professores e do Programa de Pós-Grad uação em Ciências
Odontológicas que me ajudaram em tudo que sempre precisei. Sou muito grata a
todos vocês.
À secretária do Programa de Pós-Graduação em Ciências Odontológicas ,
Jéssica , pela disponibilidade e “galhos quebrados” durante o curso.
Aos Colegas do Programa de Pós-Graduação em Ciências Od ontológicas , pelo
convívio nesta jornada.
Às minhas colegas e amigas Aline e Tathi . À Aline por todo convívio, conversas,
desabafos. Já éramos amigas antes, mas nunca imaginei que nossa amizade
pudesse crescer tanto em tão pouco tempo. À Tathi por me aguentar sempre, pela
parceria em nossas idas à São Paulo, por comemorar junto comigo nossas
conquistas, enfim, pela tua amizade. Isso tudo está só começando!
Aos Colegas do Grupo de Pesquisa “Determinantes epidemiológicos das doenças
bucais e impacto das condições de saúde bucal na qualidade de vida” pela ajuda
durante o levantamento epidemiológico.

À minha amiga e colega Renatinha que esteve comigo sempre. Obrigada pelo
companheirismo e principalmente pela tua amizade. Obrigada por toda a sua
disponibilidade em ajudar. Você vai estar sempre no meu coração.
Aos funcionários da Biblioteca do CCSH pela disponibilidade e boa vontade em
colaborar com meus estudos.
À Secretaria de Município da Educação de Santa Maria pelas informações e
autorização cedidas para o desenvolvimento deste estudo.
A todas as crianças e seus responsáveis, por toda colaboração. Nada disso
aconteceria sem o apoio de vocês.
À Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) pela
concessão de bolsa durante o curso.
A todos que de forma direta ou indireta, contribuíram para realização desse trabalho
e para minha formação.
O nosso caráter é o resultado da nossa conduta
(Aristóteles)

RESUMO
Dissertação de Mestrado Programa de Pós-Graduação em Ciências Odontológicas
Universidade Federal de Santa Maria
IMPACTO DOS FATORES SOCIOECONÔMICOS, PSICOSSOCIAIS E CLÍNICOS
NA QUALIDADE DE VIDA E NA UTILIZAÇÃO DOS SERVIÇOS
ODONTOLÓGICOS EM ESCOLARES
Justificativa: Medidas subjetivas de saúde têm sido frequentemente utilizadas para mensurar o impacto de condições de saúde bucal na autopercepção e qualidade de vida de crianças e adolescentes. Entretanto, nenhum estudo populacional demonstrou o impacto dos fatores clínicos, socioeconômicos e psicossociais na qualidade de vida relacionada à saúde bucal em crianças de 12 anos de idade utilizando o ”Child Perceptions Questionnaire” (CPQ11-14). Além disso, o efeito dos fatores psicossociais na utilização dos serviços odontológicos em escolares desta faixa etária tem sido raramente avaliado. Objetivo: O objetivo desta dissertação é apresentar dois artigos a respeito do impacto das condições de saúde oral, fatores socioeconômicos e psicossociais na COHRQoL e na utilização dos serviços odontológicos em escolares. Material e Métodos: Uma amostra de 792 escolares de 12 anos de idade foi selecionada em escolas públicas da cidade de Santa Maria-RS, Brasil. Dados a respeito da prevalência de overjet, cárie e trauma dental foram avaliados por examinadores calibrados. As crianças completaram a versão brasileira do CPQ11-14 e dados socioeconômicos foram coletados mediante emprego de um questionário semi-estruturado que foi enviado aos pais. Os dados foram analisados utilizando o Modelo de Regressão de Poisson para avaliar a associação das variáveis preditoras e os desfechos considerados (COHRQoL e uso de serviços odontológicos). Resultados: Houve um gradiente distinto nas médias dos escores do CPQ11-14 de acordo com variáveis socioeconômicas e clínicas. A presença de cárie dental e overjet acentuado foram associados com um alto impacto na COHRQoL. Crianças de família de baixa renda e cujas mães tinham menor nível educacional foram mais propensas a ter maiores médias nos scores do CPQ11-14. Quando se avaliou o efeito dos preditores considerados para o uso de serviços odontológicos, verificou-se que crianças que relataram sua saúde oral como “pobre” e de baixa condição social visitaram os serviços menos frequentemente e foram mais propensas a procurar os serviços públicos. As razões para a procura dos serviços foi relacionada com preditores clínicos e socioeconômicos. Crianças com cárie dental e cujas mães tinham baixo nível educacional utilizaram mais os serviços odontológicos por motivo curativo. Conclusão: Os dados demonstram que fatores clínicos, socioeconômicos e psicossociais causam impacto na qualidade de vida de crianças e influenciam o padrão de utilização dos serviços odontológicos em crianças.
Palavras-chave: crianças, saúde bucal; qualidade de vida, utilização dos serviços odontológicos

ABSTRACT
Master Dissertation Post Graduate Program in Dental Science
Universidade Federal de Santa Maria
IMPACT OF SOCIOECONOMIC, PSYCHOSOCIAL AND CLINICAL FACTORS ON
CHILD ORAL HEALTH-RELATED QUALITY OF LIFE AND ON TH E USE OF
DENTAL SERVICES IN SCHOOL CHILDREN
Background: The use of child oral health related quality of life measurements (COHRQoL) has been widely advocated. However, no population study demonstrated the impact of clinical, socioeconomic and psychosocial factors on COHRQoL in 12 years-old children using the Child Perceptions Questionnaire(CPQ11-14). Moreover, studies that evaluated the relation between perception of oral health and dental care utilization in school children are scarce. Aim: We assessed the impact clinical, socioeconomic and psychosocial factors on COHRQoL and on the use of dental service in school children. Methods: A multistage random sample of 792, 12 years-old Brazilians school children was examined for recoding overjet, dental caries and dental trauma. Children completed the Brazilian version of CPQ11-14
and data about socioeconomic variables were collected by means of a structured questionnaire. Poisson regression model were performed to assess the association between the predictor variables and the outcomes. Results: It showed a distinct gradient in mean CPQ 11-14 scores by socioeconomic indicators and clinical conditions. The presence of dental caries and overjet were associated with higher impacts on the COHRQoL. A socioeconomic gradient was found in COHRQoL. Children from lower household income and whose mothers had a low level of education were more likely to have higher means of CPQ11-14 scores than their counterparts. Children that rated their oral health as “poor” and from low socioeconomic backgrounds visited the services less frequently and were more likely to have gone to the public healthcare. The reasons for the dental visit were associated with clinical and socioeconomic indicators of the sample. Worse-off children with dental caries tend to visit a dentist only for treatment reasons. Conclusion: The data showed that clinical, socioeconomic and psychosocial factors were strong predictors for COHRQoL and influence the patterns of dental care utilization in school children.
Key words: children, oral health, quality of life, dental care utilization.

LISTA DE ANEXOS
ANEXO A Instrumentos usados para avaliar a percepção de saúde
bucal de crianças
ANEXO B Child Perceptions Questionnaire (CPQ11-14)
ANEXO C Carta do Comitê de Ética em Pesquisa da Universidade
Federal de Santa Maria (UFSM)
ANEXO D Índice para diagnóstico de trauma dentário
ANEXO E Índice para diagnóstico de cárie dentária

LISTA DE APÊNDICES
APÊNDICE A Termo de Consentimento Livre e Esclarecido (TCLE)
APÊNDICE B Questionário Socioeconômico
APÊNDICE C Ficha de coleta de dados

SUMÁRIO
1 INTRODUÇÃO GERAL ...................................................................................... 15
2 PROPOSIÇÃO......................................................................................................19
3 CAPÍTULOS…………………………………………………………………...... 20
ARTIGO I:
“Impact of socioeconomic and clinical factors on child oral health-related
Quality of life (COHRQoL).”
ARTIGO II:
“Influence of self-perceived oral health and socioeconomic predictors on
children’s dental care utilization.”
4 DISCUSSÃO GERAL E CONCLUSÃO ............................................................ 54
5 REFERÊNCIAS..................................................................................................... 56
6 ANEXOS E APÊNDICES ............................................................................ 62

1 INTRODUÇÃO GERAL
Conceitos contemporâneos de saúde sugerem que a saúde bucal seja definida
em termos de bem-estar físico, psicológico e social em relação ao status bucal
(GHERUNPONG; SHEIHAM; TSAKOS, 2006a). Tal conceito remete à avaliação de
saúde bucal através de métodos que incluam ambos os aspectos clínicos objetivos e
subjetivos em relação ao impacto das condições de saúde/doença nas atividades
físicas e psicossociais de um indivíduo (JIANG et al., 2005; WATT, 2007).
Estudos prévios têm demonstrado que diversas condições de saúde bucal ainda
são consideradas um problema de saúde pública na medida em que seus efeitos
extrapolam uma visão meramente bucal e causam impacto significativo na qualidade de
vida dos indivíduos afetados (DO; SPENCER, 2007a; LOCKER, 2007b; BARBOSA;
TURELI; GAVIAO, 2009). Neste contexto, tem sido frequente na literatura a utilização
de questionários autoaplicáveis denominados indicadores sócio-dentais (JOKOVIC et
al., 2004b; FOSTER PAGE et al., 2005) para verificar a severidade com que as
condições de saúde/doença interferem nas atividades diárias e na qualidade de vida de
grupos populacionais (SLADE, 1998a; FOSTER PAGE et al., 2005). Tais indicadores
têm sido desenvolvidos e epidemiologicamente testados em diferentes populações a
fim de se estruturar de maneira mais concreta as relações entre medidas subjetivas e
objetivas de saúde bucal, colaborando para uma estimativa mais clara das
necessidades de uma determinada população (LEÃO; LOCKER, 2006).
Diante disso, diversos instrumentos de mensuração têm sido desenvolvidos e
englobam aspectos psicológicos e sociais através da autopercepção e dos impactos
causados na qualidade de vida (SLADE; SPENCER, 1994b; ADULYANON;
VOURAPUKJARU; SHEIHAM, 1996; JOKOVIC et al., 2002a; TALEKAR; ROZIER;
SLADE, 2004). Entretanto, grande parte desses indicadores de saúde oral tem sido
desenvolvida para populações de adultos ou idosos e geralmente considerando um
único agravo. Poucos trabalhos têm sido conduzidos para verificar o impacto de
diferentes injúrias bucais na autopercepção e qualidade de vida de crianças e
adolescentes considerando sua inter-relação com estilo de vida e ambiente social
(LOCKER, 2007b).

16
Além disso, a percepção de crianças e adultos a respeito do impacto dos
problemas bucais na qualidade de vida é diferente (TESCH; OLIVEIRA; LEAO, 2007a).
As crianças têm autopercepção peculiar, em virtude de apresentarem uma visão própria
de si mesmas que depende do seu desenvolvimento cognitivo, emocional e social
(JOKOVIC et al., 2002a).
Por esse aspecto, inúmeros instrumentos foram desenvolvidos para mensurar a
saúde bucal e o seu impacto na qualidade de vida da população infantil, utilizando tanto
os pais - como respondentes secundários (proxy)- quanto a autorresposta da criança
(ANEXO A). As medidas de autopercepção incluem o Child-OIDP (Oral Impacts on
Daily Performances) (GHERUNPONG; TSAKOS; SHEIHAM, 2004b), o ECOHIS (Early
Childhood Oral Health Impact Scale) (PAHEL; ROZIER; SLADE, 2007), o COHQOL
(Child Oral Health Quality of Life) (JOKOVIC et al., 2002a), o CPQ (Child Perceptions
Questionnaire) (JOKOVIC et al., 2002a) e o COHIP (Child Oral Health Impact Profile)
(BRODER; MCGRATH; CISNEROS, 2007). Embora originalmente desenvolvidos em
língua inglesa, esses instrumentos têm sido adaptados e validados para serem
utilizados em diferentes populações. Até o presente momento, os questionários Child-
OIDP (CASTRO et al., 2008), ECOHIS (TESCH; OLIVEIRA; LEAO, 2008b) e os CPQ8-
10 (BARBOSA; TURELI; GAVIAO, 2009) e o CPQ11-14 (GOURSAND et al., 2008;
BARBOSA; TURELI; GAVIAO, 2009) originais e em sua forma reduzida (TORRES et
al., 2009), foram adaptados transculturalmente e validados para crianças brasileiras. A
escolha de um deles deve estar baseada no propósito do estudo, na faixa etária e na
população-alvo.
Dentre os instrumentos propostos para crianças com 12 anos de idade, o CPQ11-
14 (ANEXO B) demonstrou ser um instrumento válido para ser aplicado em crianças
brasileiras da referida faixa etária (GOURSAND et al., 2008; BARBOSA; TURELI;
GAVIAO, 2009). O CPQ11-14 foi desenvolvido na Canadá (JOKOVIC et al., 2002a),
porém estudos do Reino Unido (MARSHMAN et al., 2005; O'BRIEN et al., 2006), Nova
Zelândia (FOSTER PAGE et al., 2005), Arábia Saudita (BROWN; AL-KHAYAL, 2006),
China (MCGRATH et al., 2008b), Austrália (DO; SPENCER, 2008b) e Dinamarca
(WOGELIUS et al., 2009) já testaram e confirmaram sua validade e confiabilidade,
sendo, portanto, atualmente válido para ser utilizado na população desses países. O

17
CPQ11-14 é estruturalmente composto por 37 questões dividas em quatro domínios:
sintomas orais (6 questões), limitação funcional (10 questões), bem-estar emocional (9
questões) e bem-estar social (12 questões). A escala “5-point Likert” é usada com as
seguintes opções de resposta: “nunca”= 0, “uma ou duas vezes”= 1, “algumas vezes”=
2, “frequentemente”= 3 e “todos dias/quase todos dias”= 4. A pontuação do CPQ11-14 é
computada através da soma de todos os itens. A pontuação de cada domínio também
pode ser feita separadamente. O resultado total do questionário pode variar de 0 até
148 pontos, sendo que quanto maior a pontuação, maior é o impacto das condições de
saúde oral na qualidade de vida da criança.
No Brasil, apesar de alguns estudos já terem utilizado o CPQ11-14 para avaliar o
efeito de preditores na qualidade de vida relacionada à saúde bucal em crianças
(GOURSAND et al., 2008; BARBOSA; TURELI; GAVIAO, 2009), nenhum estudo
avaliou COHRQoL associada com fatores socioeconômicos em uma amostra
representativa até o momento. Além disso, alguns trabalhos brasileiros avaliaram o
impacto da autopercepção de saúde oral, de fatores clínicos e socioeconômicos na
utilização dos serviços odontológicos (MATOS et al., 2001b; MATOS ;LIMA-COSTA,
2006a; PINHEIRO; TORRES, 2006; PATTUSSI et al., 2007; ANTUNES et al., 2008;
FREDDO et al., 2008; KRAMER et al., 2008; NORO et al., 2008). Entretanto, quando é
considerada a população de escolares de 12 anos de idade, os trabalhos são escassos
(FREDDO et al., 2008).
O próprio conceito de acesso aos serviços de saúde é complexo e está
relacionado à percepção das necessidades de saúde, da conversão destas
necessidades em demanda e destas em uso (SANDERS; SLADE, 2006a; SOMKOTRA;
DETSOMBOONRAT, 2009). No entanto, os resultados de estudos anteriores a respeito
do tema são conflitantes. Enquanto alguns trabalhos encontraram uma associação
entre autopercepção de saúde oral e utilização dos serviços odontológicos em crianças
(JIANG et al., 2005; PERERA; EKANAYAKE, 2008), esta relação não foi demonstrada
como significativa em outro estudo (PATTUSSI et al., 2007).
O entendimento dos fatores socioeconômicos, sociodemográficos, psicossociais
e clínicos associados com COHRQoL e com a utilização dos serviços odontológicos em
crianças poderiam ser úteis para o planejamento de políticas públicas de saúde como a

18
priorização de atendimentos e avaliação dos resultados das iniciativas e estratégias de
tratamentos (MCGRATH; BRODER; WILSON-GENDERSON, 2004a). Além disso, a
realização de estudos dessa natureza é importante, pois o acesso às informações
providas por estes instrumentos permite que a percepção do paciente seja avaliada,
incrementando, assim, a comunicação entre profissionais e pacientes e promovendo
melhor entendimento das consequências e do impacto das condições de saúde bucal
na qualidade de vida de um indivíduo (MCGRATH; BRODER; WILSON-GENDERSON,
2004a).

2 PROPOSIÇÃO
O objetivo desta dissertação é apresentar dois artigos a respeito do
impacto das condições de saúde oral, fatores socioeconômicos e psicossociais
na qualidade de vida e na utilização dos serviços odontológicos em crianças de
12 anos de idade, da cidade de Santa Maria, RS, Brasil.

3 CAPÍTULOS
Esta dissertação está baseada nas normativas da Universidade Federal da
Santa Maria. Por se tratar de pesquisa envolvendo seres humanos, o projeto de
pesquisa deste trabalho foi submetido à apreciação do Comitê de Ética em Pesquisa
da Universidade Federal de Santa Maria, tendo sido aprovado (ANEXO C). Sendo
assim, esta dissertação é composta de dois artigos que serão enviados para
publicação nas revistas “International Journal of Paediatric Dentistry” (Capítulo 1) e
“Cadernos de Saúde Pública” (Capítulo 2).
Capítulo 1
“Impact of socioeconomic and clinical factors on child oral health-related quality of life
(COHRQoL)” .
Piovesan C, Antunes JLF, Guedes RS, Ardenghi TM.
Capítulo 2
“Influence of self-perceived oral health and socioeconomic predictors on children’s
dental care utilization”.
Piovesan C, Antunes JLF, Guedes RS, Ardenghi TM.

1
Capítulo 1
Impact of socioeconomic and clinical factors on chi ld oral-health-related quality of
life (COHRQoL)
CHAIANA PIOVESAN1, JOSÉ LEOPOLDO FERREIRA ANTUNES2, RENATA SARAIVA
GUEDES3, THIAGO MACHADO ARDENGHI4
1DDS, MSc Students, Universidade Federal de Santa Maria (UFSM), Rio Grande do
Sul, Brazil.
2MSc, PhD, Professor, Escola de Artes, Ciências e Humanidades, Universidade de São
Paulo, São Paulo, Brazil.
3DDS, MSc Students, Universidade Federal de Santa Maria (UFSM), Rio Grande do
Sul, Brazil.
4DDS, MSc, PhD, Adjunct Professor, Department of Stomatology, Universidade Federal
de Santa Maria (UFSM), Rio Grande do Sul, Brazil.
Word Count : 3832.
Send all correspondence to:
Chaiana Piovesan (e-mail: [email protected])
Rua Acamapamento 239/01, Santa Maria - RS, Brazil.
Zip-code: 97.050-000
Phone number: +55(55) 99 69 94 02

2
Summary
Background : While the use of child oral health-related quality of life measures
(COHRQoL) has been increasing in oral health surveys, few studies have assessed the
influence of socioeconomic status on COHRQoL in developing countries. Objectives :
This study assessed the relationship among socioeconomic backgrounds, clinical factors
and COHRQoL. Methods: A cross-sectional study in a multistage random sample of
792, 12-years-old Brazilians school children was conducted in Santa Maria, Brazil. We
recorded dental caries experience, dental trauma and occlusal pattern. Children
completed the Brazilian version of Child Perceptions Questionnaire (CPQ11-14) and
parents provided information about several socioeconomic indicators by means of a
semi-structured questionnaire. Data were analyzed using Poisson regression model.
Results : The presence of dental caries and overjet were associated with higher impacts
on the COHRQoL. A socioeconomic gradient was found in COHRQoL, being those from
lower household income and which the mothers had a low level of education more likely
to have higher means of CPQ11-14 scores than other children. Conclusion:
Socioeconomic disadvantage and clinical disorder have a negative impact on
COHRQoL indicated the need for policies targeting more disadvantage groups for the
reduction of inequities in oral health status.

3
Introduction
Oral health problems have been increasingly recognized as important cause of
negative impact on daily performance and quality of life of individuals and society 1-5.
Over the last 30 years, the use of measurements of self-perceived oral health related
quality of life (OHRQoL) has been widely advocated, because normative indicators of
oral disease, when used alone, do not document the full impact of oral disorders 6.
These indices are most commonly used for adults or elderly populations 6, 7 . There are
few instruments specifically designed to assess the Oral Health-Related Quality of Life
in children (COHRQoL) 3, 8, 9. The Children Perception Questionnaire (CPQ11-14) is one of
these 3.
The CPQ11-14 assesses children’s perceptions of the impact of oral disorders on
physical and psychosocial functioning. It was developed in Canada 3 but studies have
confirmed the validity and reliability in other countries, such as the United Kingdom 10, 11,
New Zealand 1, Saudi Arabia 12, China 13, Australia 14, Denmark 15 and Brazil 2, 5.
Although several studies had confirmed that problems of oral health cause
negative impact on quality of life of individuals1, 3, 5, 14, it has been suggested that the
relationship between oral disease and health-related quality of life outcomes is mediated
by personal and environmental variables 4. In Brazil, besides previous studies
demonstrated that CPQ 11-14 is available for Brazilian children 2, 5, no study had
previously performed to assess the association between COHRQoL and
socioeconomics variables in a representative sample.
The understanding of the socioeconomic and clinical factors associated with
COHRQoL could be useful as an important information to planning public health as
prioritization of care and evaluating outcomes from treatments strategies and initiatives.

4
Therefore, we performed a cross-sectional study with a representative sample of
Brazilian schoolchildren to assess the influence of socioeconomics and clinical factors
on their quality of life. It was hypothesized that children with great caries experience and
from a lower socioeconomic background would have higher overall and domain CPQ 11-
14 scores than their counterparts.
Material and Methods
Sample
A survey was performed to assess the oral health status of 12 years-old children
living in Santa Maria-RS, Brazil. Santa Maria is a medium-size city located in the south
of Brazil. The city has an estimated population of 263,403. According to the Bureau of
Education, there were 3180 children with 12 years-old regularly attending in public
schools in 2008. A multistage sampling procedure was performed. The first unit included
all primary public schools of Santa Maria. The second unit included all students enrolled
in the select schools. Twenty from 39 schools were randomly selected. A random
sample was obtained using a list with all students enrolled in the select schools. Only
subjects who were intellectually and physically capable of responding to the
questionnaire were included in the study.
For the sample calculation, a standard error of 5%, a confidence interval level of
95% and a prevalence of 50% of children with dental caries and dental trauma were
adopted. The decision to use a prevalence of 50% was due to lack of information of the
actual prevalence of the outcomes. In addition, a design effect of 1.5 and adding 10% to
losses or refuses were applied. The final sample size was large than the minimum size
to satisfy the requirements (n=634) because the survey included other outcomes that

5
required large samples. With this sample size, the study had a power of 80% to detect a
significant mean difference (Rate Ratio- RR) of at least 1.4 in the scores of CPQ 11-14
between children with and without dental caries.
Data collection
Data were collected through clinical oral examinations and structured interviews.
Six examiners and six interviewers participated in the study. They were previously
trained and calibrated for data collection before the survey. Calibration process lasted
for 36 h.
Children were examined visually in a room with natural light using CPI probe and
plane dental mirror (WHO, 1997). Clinical examination for recording dental caries
(DMFT- WHO, 1997), overjet (WHO, 1997) and dental trauma 16 were performed.
Socioeconomic characteristics of the sample were collected through questionnaire which
was completed by the parents. The questionnaire provided information about the age,
gender, ethnics, parents’ schooling, parents’ occupation and household income. The
feasibility of the questionnaire was assessed previously in a sample of 20 parents during
the calibration process.
All children completed the Brazilian version of the CPQ11–14 questionnaire 2 in the
room at the school in face-to-face interviews conducted by a trained research assistant.
The interview was individual to preserve the individuality of the child. The CPQ11-14 is
structurally composed of 37 items distributed among 4 domains: oral symptoms (6
questions), functional limitation (10 questions), emotional well-being (9 questions) and
social well-being (12 questions). A 5-point Likert scale is used with the following options:
'Never' = 0; 'Once/twice' = 1; 'Sometimes' = 2; 'Often' = 3; and ‘Every’ day/almost every

6
day' = 4. The CPQ 11–14 scores are computed by summing all of the item scores. Scores
for each of the four domains can also be computed. The total score can vary from 0 to
148, which a higher score denotes a greater impact of oral conditions on children’s
quality of life.
Analyses
Data analyses were performed using STATA software 9.0. Descriptive and
bivariate analyses were conducted to provide summary statistics and preliminary
assessment of the association of predictor variables and the outcome. Poisson
regression model were performed to assess the association between the independents
variables and means CPQ11-14 scores and domain scores. In the analyses, the outcomes
were considered as a count variable and rate ratio (RR;95%C.I) were calculated for the
predictive variables. A backward stepwise procedure was used to include or exclude
explanatory variables in the fitting of models. Explanatory variables presenting a P value
≤ 0.20 in the assessment of correlation with each outcome (bivariate analyses) were
included in the fitting of the model. Explanatory variables were retained in the final
models only if they had a P value ≤ 0.05 after adjustment.
Ethics
The study was approved by the Human Research Ethics Committee of the Federal
University of Santa Maria and parents’ consent was obtained prior to the study.

7
Results
A total of 792 children, 44.3% boys and 55.7% girls, were enrolled in the study.
The response rate was 98% of all children invited. Reasons for non-participation were
mainly due to the illiteracy of parents. Interexaminer and intraexaminer agreement for
dental caries ranged from 0.68 to 0.71 and from 0.60 to 0.88, respectively. For dental
trauma, the values ranged from 0.71 to 0.83 and from 0.85 to 1.0 respectively for inter
and intraexaminer agreement.
Table 1 summarizes the demographic characteristics of the sample. Children were
predominately white with low caregivers’ level of education. More than half of the
parents were employed and half of them had a household income equal or great than 2
Brazilian minimum wage (BMW). Prevalence of overjet (≥ 3mm), dental caries and
dental trauma were 17%, 39.3% and 9.7%, respectively.
Scores on the CPQ11-14 ranged from 0 to 99 with a mean of 20.9 (SD = ±14.8). It
was observed a high variation in the domain scores, being the emotional well-being
domain having the highest variation (0 – 36) (Table 2). Bivariate regression analyses
demonstrate that mean CPQ11-14 scores were associated with gender, household
income, mother’s and father’s levels of education , father’s occupation , and dental
caries (Table 3).
After the multiple regression analysis (Table 4), the variables gender, household
income, mother’s level of education, overjet and cavity of caries remained associated
with the mean CPQ11-14 score. In general, children from low socioeconomic status were
more likely to have higher means of CPQ 11-14. When considering the effect of clinical
conditions on the COHRQoL, we observed that the dental caries and overjet had a
negative impact on the CPQ 11-14 scores. Children with cavity of caries were more likely

8
to report higher means of CPQ11-14 total scores and domains after the adjustment for
socioeconomic status and other clinical conditions. In the final models, gender difference
was also observed in relation to COHRQoL, whereas girls tend to report more impacts
on the CPQ11-14 scores than boys. This difference could be observed for almost all
domains of CPQ11-14, excepted for the Oral symptom.
Discussion
This study shows that COHRQoL is influenced by socioeconomics and clinical
variables. In accordance with previous authors 1, 3, 5, 14, 17 we found that children with oral
health problems have more severe impacts of oral conditions on their quality of life.
Results from recent study also suggest that socioeconomic variables may influence the
oral health related quality of life outcomes but in older people 18. However, when
considered the association between socioeconomic variables and COHRQoL within a
representative sample, studies are scarce. In Brazil, this is the first study that report
associated factors with COHRQoL in a representative sample using CPQ11-14.
In general, ours results demonstrated a socioeconomic gradient in the COHRQoL
(Tables 3 and 4). When we applied the multivariate regression analyses, a clear
association between socioeconomic conditions and mean scores for CPQ 11-14 could
be seen (Table 4). Children from low socioeconomic status, whose mothers have lower
level of education were more likely to have higher means of CPQ11-14 and domains
scores than their counterparts.
It is well established that people from low socioeconomic backgrounds are more
likely to be exposed to a various risk factors that affect their oral health 4. Moreover, oral
health status contributes significantly to the quality of life of people and affects them not

9
only physically, but also psychologically and socially 2, 4, 18. At the time, only one study 4
related the effect of socioeconomic status in the mean CPQ11-14 scores. In that study,
the highest mean CPQ11-14 scores were observed among low income children with the
more severe levels of oral disease. This is similar to the findings found in our study.
Social inequality in oral health is a universal phenomenon 19, 20. Higher levels of disease
are found in more deprived areas and a poor oral health may have a profound effect on
general health. The experience of pain, problems with eating, chewing, smiling and
communication due to missing, discolored or damaged teeth have a major impact on
people’s daily lives and well-being. Furthermore, oral diseases restrict activities at
school, at work and at home causing millions of school and work hours to be lost each
year throughout the world 20.
There is no shortage of opinion on explain relationship between socioeconomic
status and health. Existing theories vary in their focus from the effects of material
deprivation to individual lifestyle decisions 19. One of these theories – Cultural/
behavioral explanation – suggest that people from low socioeconomic backgrounds are
more likely to engage in behaviors that are damaging to their health than people from
higher socioeconomic backgrounds 21 and consequently this leads to higher levels of
disease causing more severe impacts of oral health and reduced quality of life 20.
In this study, when we considered the mother’s level of education as a proxy for
socioeconomic status, an independent negative impact on COHRQoL could be
observed (Table 4). Previous studies have shown deprivation gradients in oral health
problems in children and adults while fewer studies have shown the association of
education gradients for broad subjective oral health measures 18, 22. Results from recent

10
study 18 demonstrated that low educational level has an independent negative impact on
OHRQoL in older people.
Lower educational leads to worse employment prospective and lower
socioeconomic status that could influences health behaviors and self-rated oral health
23. Nevertheless, precious authors have been suggested that oral health outcomes in
children may be correlated with mother’s level of education 24, 25 and the environment in
which these children are inserted may have a direct influence their healthy style and the
way in which they rate their oral health 4.
We also demonstrated that clinical variables may influence the COHRQoL.
Children with overjet and cavity of dental caries were more likely to have higher means
of total CPQ 11-14. The self-image dissatisfaction could explain the association between
increased overjet and mean CPQ11-14 scores (mainly in social well-being domain). The
questions included in this domain address issues related with social relations as to avoid
showing your teeth, laugh and talk with children at school or with people at home.
Therefore, any deviation from the ‘norm’ as simple as dental anomaly will make a person
less acceptable socially 26. There appears to be some evidence to suggest that
individuals who have unaesthetic occlusal traits attract unfavorable social responses in
becoming targets for nicknames and teasing from other school children 26, 27. Our
findings are in agreement with previous authors which demonstrated that having an
increased overjet cause a negative impact on individual’s OHRQoL 26, 27 . Therefore, this
study confirms that dentofacial aesthetics plays an important role in social interactions
and psychosocial wellbeing.
Considering the presence of dental caries, there were distinct differences in both
the overall and the domain scores between those who had cavity of dental caries.

11
Previous studies have detected significant difference in the CPQ11-14 scores only among
groups with higher levels of caries 1. Therefore, we created the variable cavity of dental
caries because it includes only children with dental decay. These children are more
likely to have experienced oral pain, had difficulties in chewing, to have worried or been
upset about their mouths which can cause more severe impacts of oral health on their
quality of life 1.
Our findings confirmed that girls have higher impacts of oral health conditions on
their quality of life than boys (Table 4) 1, 4, 5. We suggest that this significant association
between gender and mean CPQ11-14 scores and domain scores could be explained by
the fact that girls have higher concerns about their health and tend to report higher
impact of oral health on their quality of life. Findings from other studies with adults
demonstrated that men are less likely to report health problems than women 28. Such
different between women and men may be related to the perception and values of oral
health in addition to specific conditions like hormonal changes 29.
Some methodological shortcoming need to be discussed when considering the
results reported here. The findings are limited by the cross-sectional nature of the data.
Therefore, it is not possible to establish a temporal relationship between the outcomes
and predictors variables. However, cross-sectional designs are useful to identify risk
indicators that can be confirm in further longitudinal designs. We found a high variation
for the scores of the CPQ11-14 (from 0 to 99- Table 2). Previous studies have
demonstrated different variation in CPQ11-14 scores 1-3, 5, 12-15. The domain scores also
showed substantial variability in our study and the emotional well-being domain was the
only which had floor and ceiling effects. In this study, the outcomes were considered as
a count variable. Alternatively, studies have computed the prevalence of people

12
reporting one or more item as ‘fairly often’ or ‘very often’, and the results can then be
present as the proportions of people who have better (or worse) OHRQoL 7. In fact,
when use binary outcomes for the assessment of correlations of oral health-related
questionnaire, it probably make the results more meaningful for clinicians, but it also
results in loss of information and loss of statistical power 30.
Besides of its limitations, this study brings new information for a public health
perspective. We used a representative sample of Brazilian school children with a
random selection process in different sample schools. This random process avoided
bias which might occurs if the sample is collected in a clinical setting, for example, and
the high response rate and the acceptable level of inter/intra-rate agreement, increase
the intern validity of the study. Moreover, this the first study that used a representative
sample for assess the association between socioeconomic and clinical variables and
mean CPQ11-14 scores in Latin America context.
This study demonstrated the role of socioeconomic inequalities and some dental
conditions as strong predictors for COHRQoL in a representative sample of 11-14-years-
old Brazilian children. The presence of a gradient in COHQoL throughout socioeconomic
status indicates the need for policies that taken into account the social, psychosocial
and oral factors for reducing the inequalities in oral health among groups of populations.

13
Bullet Points
What this paper adds
• This paper is the first to assess the associations between socioeconomic
gradients and COHRQoL in a representative sample using the CPQ11-14.
Why this paper is important to paediatric dentists
• This paper is important because to understand of the socioeconomic and clinical
factors associated with COHRQoL could be useful as important information to
planning public health as prioritization of care and evaluating outcomes from
treatments strategies and initiatives.
Acknowledgment
The authors would like to thank for all the children for their cooperation and the
Education Authorities in Santa Maria for all information and authorization. The authors
stated that there are no Potential conflicts of interest.

14
References
1 Foster Page LA, Thomson WM, Jokovic A, Locker D. Validation of the Child Perceptions Questionnaire (CPQ 11-14). J Dent Res. 2005; 84: 649-52.
2 Goursand D, Paiva SM, Zarzar PM et al. Cross-cultural adaptation of the Child Perceptions Questionnaire 11-14 (CPQ11-14) for the Brazilian Portuguese language. Health Qual Life Outcomes. 2008; 6: 2.
3 Jokovic A, Locker D, Stephens M, Kenny D, Tompson B, Guyatt G. Validity and reliability of a questionnaire for measuring child oral-health-related quality of life. J Dent Res. 2002; 81: 459-63.
4 Locker D. Disparities in oral health-related quality of life in a population of Canadian children. Community Dent Oral Epidemiol. 2007; 35: 348-56.
5 Barbosa TS, Tureli MC, Gaviao MB. Validity and reliability of the Child Perceptions Questionnaires applied in Brazilian children. BMC Oral Health. 2009; 9: 13.
6 Slade GD. Assessing change in quality of life using the Oral Health Impact Profile. Community Dent Oral Epidemiol. 1998; 26: 52-61.
7 Locker D, Jokovic A, Stephens M, Kenny D, Tompson B, Guyatt G. Family impact of child oral and oro-facial conditions. Community Dent Oral Epidemiol. 2002; 30: 438-48.
8 Filstrup SL, Briskie D, da Fonseca M, Lawrence L, Wandera A, Inglehart MR. Early childhood caries and quality of life: child and parent perspectives. Pediatr Dent. 2003; 25: 431-40.
9 Broder HL, McGrath C, Cisneros GJ. Questionnaire development: face validity and item impact testing of the Child Oral Health Impact Profile. Community Dent Oral Epidemiol. 2007; 35 Suppl 1 : 8-19.
10 Marshman Z, Rodd H, Stern M et al. An evaluation of the Child Perceptions Questionnaire in the UK. Community Dent Health. 2005; 22: 151-5.
11 O'Brien K, Wright JL, Conboy F, Macfarlane T, Mandall N. The child perception questionnaire is valid for malocclusions in the United Kingdom. Am J Orthod Dentofacial Orthop. 2006; 129: 536-40.
12 Brown A, Al-Khayal Z. Validity and reliability of the Arabic translation of the child oral-health-related quality of life questionnaire (CPQ11-14) in Saudi Arabia. Int J Paediatr Dent. 2006; 16: 405-11.

15
13 McGrath C, Pang HN, Lo EC, King NM, Hagg U, Samman N. Translation and evaluation of a Chinese version of the Child Oral Health-related Quality of Life measure. Int J Paediatr Dent. 2008; 18: 267-74.
14 Do LG, Spencer AJ. Evaluation of oral health-related quality of life questionnaires in a general child population. Community Dent Health. 2008; 25: 205-10.
15 Wogelius P, Gjorup H, Haubek D, Lopez R, Poulsen S. Development of Danish version of child oral-health-related quality of life questionnaires (CPQ8-10 and CPQ11-14). BMC Oral Health. 2009; 9: 11.
16 O' Brien M. Children’s dental health in the United Kingdom 1993 IN: Report of dental survey, Office of Population Censuses and Surveys. LONDON: Her Majesty’s Stationery Office. 1994.
17 Locker D, Allen F. What do measures of 'oral health-related quality of life' measure? Community Dent Oral Epidemiol. 2007; 35: 401-11.
18 Tsakos G, Sheiham A, Iliffe S et al. The impact of educational level on oral health-related quality of life in older people in London. Eur J Oral Sci. 2009; 117: 286-92.
19 Sisson KL. Theoretical explanations for social inequalities in oral health. Community Dent Oral Epidemiol. 2007; 35: 81-8.
20 Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005; 83: 661-9.
21 Davey-Smith G, Blane D, Bartley M. Explanations for socioeconomic differentials in mortality: evidence from Britain and elsewhere. Eur J Public Health. 1994; 4: 131-44.
22 Sabbah W, Tsakos G, Sheiham A, Watt RG. The effects of income and education on ethnic differences in oral health: a study in US adults. J Epidemiol Community Health. 2009; 63: 516-20.
23 Sanders AE, Spencer AJ. Childhood circumstances, psychosocial factors and the social impact of adult oral health. Community Dent Oral Epidemiol. 2005; 33: 370-7.
24 Pine CM, Adair PM, Nicoll AD et al. International comparisons of health inequalities in childhood dental caries. Community Dent Health. 2004; 21: 121-30.
25 Traebert J, Guimaraes Ldo A, Durante EZ, Serratine AC. Low maternal schooling and severity of dental caries in Brazilian preschool children. Oral Health Prev Dent. 2009; 7: 39-45.
26 Johal A, Cheung MY, Marcene W. The impact of two different malocclusion traits on quality of life. Br Dent J. 2007; 202: E2.

16
27 Bernabe E, de Oliveira CM, Sheiham A. Condition-specific sociodental impacts attributed to different anterior occlusal traits in Brazilian adolescents. Eur J Oral Sci. 2007; 115: 473-8.
28 Macintyre S, Ford G, Hunt K. Do women 'over-report' morbidity? Men's and women's responses to structured prompting on a standard question on long standing illness. Soc Sci Med. 1999; 48: 89-98.
29 McGrath C, Bedi R. Measuring the impact of oral health on quality of life in Britain using OHQoL-UK(W). J Public Health Dent. 2003; 63: 73-7.
30 Guyatt G, Schunemann H. How can quality of life researchers make their work more useful to health workers and their patients? Qual Life Res. 2007; 16: 1097-105.

Table 1- Clinical and demographic characteristics o f the sample.
Variable n* (%)
Gender 792
Male 351 44.3
Female 441 55.7
Ethnics 783
White 609 77.8
Non-White 174 22.2
Household Income 667
≥ 2BMW 341 51.1
< 2BMW 326 48.9
Mother’s schooling(years) 764
≥ 8 330 43.1
< 8 434 56.8
Father’s schooling (years) 738
≥ 8 273 40.0
< 8 465 63.0
Mother’s occupation 782
Employed 497 63.5
Unemployed 285 36.4
Father’s occupation 746
Employed 651 87.3
Unemployed 95 12.7
Overjet 792
< 3mm 657 82.9
≥ 3mm 135 17.0
Dental trauma 792
Without 715 90.3
With 77 9.7
Cavity of caries 792
Without 590 74.5
With 202 25.5
* values lower than 792 due missing data BMW= Brazilian Minimum Wage;

18
Table 2 - Descriptive distribution o f total CPQ 11-14 and domain scores.
Number of
Items
Mean CPQ11-14 Scores
(±SD)
Possible
range
Range
CPQ (overall scale) 37 20.9 (±14.8) 0 – 148 0 - 99
Domains
Oral Symptoms 6 6.8 (±3.6) 0 – 24 0 - 18
Functional Limitation 10 6.0 (±3.9) 0 – 40 2 - 27
Emotional Well-being 9 5.9 (±6.8) 0 – 36 0 - 36
Social Well-being 12 3.0 (±4.1) 0 – 48 0 - 26
CPQ 11-14 – Child Perception Questionnaire

Table 3 – Association between socioeconomics and cl inical variables and mean CPQ 11-14 scores and domains – univariate analysis.
Variables CPQ11-14
RR (95%CI) OS
RR (95%CI) FL
RR (95%CI) EWB
RR (95%CI) SWB
RR (95%CI)
Gender p < 0.01 p = 0.70 p < 0.01 p < 0.01 p = 0.02
Male 1.00 1.00 1.00 1.00 1.00
Female 1.19 (1.08 - 1.31) 1.01 (0.94 - 1.09) 1.17 (1.07 - 1.28) 1.43 (1.21 - 1.69) 1.25 (1.03 - 1.51)
Ethnics p = 0.05 p = 0.18 p = 0.20 p < 0.01 p = 0.45
White 1.00 1.00 1.00 1.00 1.00
Non-White 1.12 (1.00 - 1.26) 1.06 (0.97 - 1.15) 1.07 (0.96 - 1.19) 1.31 (1.10-1.57) 1.09 (0.86 - 1.38)
Household Income p < 0.01 p < 0.01 p = 0.01 p < 0.01 p < 0.01
≥ 2 BMW 1.00 1.00 1.00 1.00 1.00
< 2 BMW 1.28 (1.15 - 1.42) 1.17 (1.08 - 1.26) 1.13 (1.03 - 1.25) 1.49 (1.25 - 1.77) 1.39 (1.13 - 1.70)
Mother’s schooling p < 0.01 p < 0.01 p < 0.01 p < 0.01 p < 0.01
≥ 8 years 1.00 1.00 1.00 1.00 1.00
< 8 years 1.34 (1.21 - 1.48) 1.13 (1.05 - 1.22) 1.23 (1.12 - 1.35) 1.56 (1.32 - 1.85) 1.61 (1.33 - 1.95)
Father’s schooling p < 0.01 p < 0.01 p < 0.01 p < 0.01 p < 0.01
≥ 8 years 1.00 1.00 1.00 1.00 1.00
< 8 years 1.23 (1.11 - 1.37) 1.14 (1.05 - 1.23) 1.14 (1.04 - 1.26) 1.37 (1.16-1.64) 1.35 (1.11 - 1.65)
Mother’s occupation p = 0.70 p = 0.85 p = 0.83 p = 0.80 p = 0.20
Employed 1.00 1.00 1.00 1.00 1.00
Unemployed 1.02 (0.91 - 1.13) 0.99 (0.91 - 1.07) 0.98 (0.89 – 1.08) 1.02 (0.86 - 1.20) 1.13 (0.93 - 0.38)
Father’s occupation p = 0.03 p = 0.46 p = 0.11 p < 0.01 p = 0.47
Employed 1.00 1.00 1.00 1.00 1.00
Unemployed 1.17 (1.01 - 1.35) 1.04 (0.93 – 1.16) 1.11 (0.97 - 1.27) 1.36 (1.09-1.70) 1.10 (0.84 - 1.44)
Overjet p = 0.05 p = 0.32 p = 0.13 p = 0.24 p < 0.01
< 3mm 1.00 1.00 1.00 1.00 1.00
≥ 3mm 1.15 (0.99 - 1.33) 1.05 (0.95 - 1.16) 1.10 (0.96 - 1.25) 1.13 (0.91 - 1.40) 1.49 (1.17 - 1.90)
Dental Trauma p = 0.91 p = 0.93 p = 0.71 p = 0.94 p = 0.70
Without 1.00 1.00 1.00 1.00 1.00
With 1.00 (0.86 - 1.18) 0.99 (0.89 – 1.10) 1.02 (0.88 - 1.20) 0.98 (0.75-1.29) 1.06 (0.79 - 1.41)
Cavity of caries p < 0.01 p < 0.01 p = 0.03 p < 0.01 p < 0.01
Without 1.00 1.00 1.00 1.00 1.00
With 1.29 (1.16 - 1.43) 1.15 (1.07 - 1.25) 1.12 (1.01 - 1.24) 1.41 (1.20-1.67) 1.50 (1.22 - 1.83)
RR= Rate ratio; CPQ11-14 = Child Perceptions Questionnaire; OS = Oral Symptoms; FL = Functional Limitation; EWB = Emotional well-being; SWB = Social well-being

20
Table 4 – Association between socioeconomics and cl inical variables and mean CPQ 11-14 scores and domains – multivariate analysis
Variables CPQ11-14
RR (95%CI) OS
RR (95%CI) FL
RR (95%CI) EWB
RR (95%CI) SWB
RR (95%CI)
Gender p < 0.01 p < 0.01 p < 0.01 p = 0.01
Male 1.00 1.00 1.00 1.00
Female 1.27 (1.15 - 1.41) 1.18 (1.08 - 1.29) 1.68 (1.40 - 2.00) 1.26 (1.03 - 1.53)
Ethnics ** ** ** ** **
White Non-White Household Income 0.01 ** ** p = 0.01 **
≥ 2 BMW 1.00 1.00
< 2 BMW 1.13 (1.02 - 1.26) 1.24 (1.04 - 1.49) Mother’s schooling p < 0.01 p < 0.01 p < 0.01 p = 0.01 p < 0.01
≥ 8 years 1.00 1.00 1.00 1.00 1.00 < 8 years 1.30 (1.17 - 1.44) 1.12 (1.04 - 1.21) 1.23 (1.12 - 1.34) 1.49 (1.24 -1.80) 1.55 (1.28 - 1.88) Father’s schooling ** ** ** ** **
≥ 8 years < 8 years Mother’s occupation **
Employed Unemployed Father’s occupation ** ** **
Employed
Unemployed Overjet p = 0.02 p < 0.01
< 3mm 1.00 1.00 ≥ 3mm 1.19 (1.02 - 1.40) 1.51 (1.18-1.93) Dental Trauma
Without With Cavity of caries p < 0.01 p < 0.01 ** p = 0.01 p < 0.01
Without 1.00 1.00 1.00 1.00 With 1.20 (1.07 - 1.35) 1.13 (1.04 - 1.23) 1.34 (1.12 - 1.60) 1.39 (1.13 - 1.71)
RR= Rate ratio; CPQ11-14 = Child Perceptions Questionnaire; OS = Oral Symptoms, FL = Functional Limitation, EWB = Emotional well-being, SWB = Social well-being; ** Variables not included in the final multiple model after the adjustment.

1
Capítulo 2
Influence of self-perceived oral health and socioec onomic predictors on
children’s dental care utilization.
CHAIANA PIOVESAN1, JOSÉ LEOPOLDO FERREIRA ANTUNES2, RENATA SARAIVA
GUEDES3, THIAGO MACHADO ARDENGHI4
1 DDS, MSc Students, Universidade Federal de Santa Maria (UFSM), Rio Grande do
Sul, Brazil.
2 MSc, PhD, Professor, Escola de Artes, Ciências e Humanidades, Universidade de São
Paulo, São Paulo, Brazil.
3 DDS, MSc Students, Universidade Federal de Santa Maria (UFSM), Rio Grande do
Sul, Brazil.
4 DDS, MSc, PhD, Adjunct Professor, Department of Stomatology, Universidade Federal
de Santa Maria (UFSM), Rio Grande do Sul, Brazil.
Send all correspondence to:
Thiago Machado Ardenghi (e-mail: [email protected])
Rua Cel.Niederauer 917/208, Santa Maria - RS, Brazil.
Zip-code: 97.015-121
Phone number: +55(55) 99 98 96 94

2
Abstract
This cross-sectional study assessed the influence of socioeconomic factors and self-
rated oral health on dental care utilization by 792, 12-years-old Brazilians school
children. Clinical examination for recording dental caries was performed. Data about the
uses of dental service, socioeconomic status and self-perceived oral health were
collected by means of a structured questionnaire. Poisson regression model showed
that children from low socioeconomic backgrounds and that rated their oral health as
“poor” visited the services less frequently and were more likely to have gone to the
public healthcare. Reasons for dental visit were associated with clinical and
socioeconomic indicators. Worse-off children with dental caries tend to visit a dentist
only for treatment reasons. Clinical, socioeconomic and psychosocial factors are strong
predictors for the patterns of dental care utilization indicating the need for health polices
that facilitate dental access to school children.
Key words: dental health services, dental care, chi ldren
Resumo
O objetivo deste estudo foi avaliar a influência de fatores socioeconômicos e
psicossociais na procura por atendimento odontológico em escolares Brasileiros de 12
anos de idade. Examinadores calibrados avaliaram a prevalência de cárie dentária.
Dados socioeconômicos da criança, questões relativas à autopercepção de saúde oral
e ao uso dos serviços odontológicos foram coletados através de um questionário. Os
dados foram analisados utilizando regressão de Poisson. Crianças de baixa condição
social e que relataram sua saúde oral como “pobre” visitaram os serviços menos
frequentemente e foram mais propensas a procurar os serviços públicos. As razões
para a procura dos serviços foi relacionada com preditores clínicos e socioeconômicos.
Crianças com cárie dental e cujas mães tinham baixo nível educacional utilizaram mais
os serviços odontológicos por motivo curativo. Os dados demonstram que fatores
clínicos, socioeconômicos e psicossociais são fortes preditores para o padrão de
utilização dos serviços odontológicos indicando a necessidade de políticas públicas de
saúde para facilitar o acesso aos serviços odontológicos por escolares.
Palavras-chave: Serviços de saúde bucal, assistênci a odontológica, crianças

3
Introduction
Disparities in oral healthcare utilization have been observed in several countries
mainly between disadvantages groups 1-4. However, in most developing countries, data
about the child use of dental services are scarce 1, 2, 5-7.
In Brazilian context, data from official publications demonstrated that 18.4% of
population between 10 and 14 years old had never gone to the dentist 8. In the same
study, regional inequality could be seen in the healthcare utilization according to the
socioeconomic development of the region, namely the most developed Brazilian regions
having the lower percentage of people whom never gone to the dentist when comparing
to the last developed one.
It has been suggested that dental care utilization could be influenced by
socioeconomic and psychosocial factors 1, 9-11. However, data about the interaction of
different predictors for dental care utilization in representative sample are rarely
assessed in Brazilian school children. Results from one recent study 12 demonstrated
that the most important determinants of dental services use in 10-19-year-old Brazilian
were high socioeconomic status and schooling. In the same study, adolescents that
rated their oral health as “good” showed higher prevalence dental services utilization
when compared with those who rated their oral health as “poor”.
Perception of oral health could influences the oral health decisions and patterns
of healthcare utilization. It has been suggested that these perceptions could be
associated with clinic and socioeconomic conditions 13-15. A population-based study in
15-year-old adolescents found that poor perceived oral health was significantly
associated with low household income, not using dental services and presence of oral
diseases 16. Nevertheless, the relation between dental care utilization and perception of
oral health in school children is inconclusive 14, 16.
The understanding of the impact of socioeconomic and psychosocial predictors
for oral healthcare utilization could be useful as important information to planning public
health polices leading to a better resource allocated 2. Therefore, we performed a cross-
sectional study with a representative sample of 12 years-old Brazilian children to assess
the influence of socioeconomics factors and self-rated oral health on school children

4
dental health utilization. We hypothesized that there are socioeconomic and
psychosocial gradients in the pattern of oral healthcare utilization, which in general is
characterized for a pro-rich inequality in the use of dental service and reasons for.
Methods
Sample
A cross-sectional study was conducted on a representative sample of 12 years old
schoolchildren living in Santa Maria, Brazil. Santa Maria is a medium-size city located in
the south of Brazil. The city has an estimated population of 263,403 8. According by
Bureau of Education, there were 3,180 12-years-old-children regularly attending in
public schools in 2008.
For the sample calculation to assess the prevalence of regular use of dental
service, we adopted a standard error of 5%, a confidence interval level of 95% and an
expected prevalence of 47% 6. In addition, a design effect of 1.4 and adding 10% to non-
response were applied. The minimum sample size to satisfy the requirements was
estimated in 590 children. To explore the association between use of regular service
and independent variables, we adopted the following parameters: 5% of standard error,
80% of power, 95% of confidence interval, design effect of 1.4, 10% to non-response,
ratio unexposed to exposed 2:1 and a prevalence ratio to be detected of at least 1.7.
A multistage sampling procedure was performed. The first unit included all primary
public schools of Santa Maria 17. The second unit included all students enrolled in the
select schools. Twenty schools were randomly selected from a total of 39 schools in the
city 17. A random sample was obtained using a list with all students enrolled in the select
schools.
Data collection
The data were collected by means of structured questionnaires send to parents,
one questionnaire to the children and clinical oral examinations. Six examiners
participated in the study. They were previously trained and calibrated for data collection
before the survey. Theoretical, clinical and calibration process for data collection lasted
for 36 hours.

5
Children were examined visually in a room with natural light using CPI probe and
plane dental mirror 17. Clinical examinations for recording dental caries were performed.
Use of dental service by school children as well socioeconomic status of the target
population were collected by means of a structured questionnaire which was sent to
parents. The questionnaire presented a series of questions regarding socioeconomic
and demographic characteristics such as age, sex, mother’s level of education, race and
family income. The questionnaire was also used to collect our dependents variables: if
the child has visited any dental service in the previous 6 months; the reasons for the
dental visit (preventive or other reasons) and type of healthcare used (private or public).
The feasibility of the questionnaire was assessed previously in a sample of 20 parents
during the calibration process.
Data about self-perceived of oral health were obtained asking “Would you say that
you oral health is: 1- excellent; 2- good; 3- fair and 5- poor”. This variable was
dichotomised in “excellent / good” and “fair/poor” oral health.
Analyses
Data analyses were performed using STATA software 9.0. Descriptive and
bivariate analyses were conducted to provide summary statistics and preliminary
assessment of the association of predictor variables and the outcomes. Three
outcomes were considered in the analyses: prevalence of children whom have sought
the services in the last 6 months, reasons for the dental visit (preventive/other than
preventive) and type of healthcare used (public/ private).
Poisson regression model (Prevalence ratio: PR;95% C.I.) was performed to
assess the association between the predictor variables and the outcomes. A backward
stepwise procedure was used to include or exclude explanatory variables in the fitting of
models. Explanatory variables presenting a P value ≤ 0.20 in the assessment of
correlation with each outcome (bivariate analyses) were included in the fitting of the
model. Explanatory variables were selected for the final models only if they had a P
value ≤ 0.05 after adjustment.
Ethics

6
The study was approved by the Human Research Ethics Committee of the Federal
University of Santa Maria and parents’ consent was obtained prior to the study. A letter
was sent to all parents explaining the aims of the study and asking them for consent for
their children to participate in the study.
.
Results
A total of 792 children, 44.3% boys and 55.7% girls, participated in the study. The
response rate was 90% of all children invited. Reasons for non-participation were mainly
due to the illiteracy of parents and not return of the questionnaire.
Table 1 summarizes the demographic characteristics of the sample. Children were
predominately white with a low level of parents’ education. Half of parents had a
household income equal or greater than 2 Brazilian Minimum Wages (BMW).
Prevalence of dental caries was 39.3%.
Prevalence of children that visited the services in the previous 6 months and
associated factors is shown in table 2. The results demonstrated that prevalence of
children that visited the services within the previous 6 months was associated with
mother’s level of education, father’s level of education, self-rated oral health and dental
caries. In the multiple regression analyses mother’s level of education, self-rated oral
health and dental caries remained associated with the outcome after the adjustment.
Children that rated their oral health as “fair / poor” and whose mothers had lower level of
education were less likely to have visited the services in the previous 6 months. In
addition, children with dental caries visited more the services than their counterparts.
Table 3 expresses the reasons for the child’s dental visit and associated factors.
Bivariate analyses demonstrate that the prevalence of children that had gone to the
dentist for preventive reasons was associated with household income, mother’s level of
education and dental caries. Multivariate analyses demonstrate that the variables
mother’s level of education and dental caries were associated with the prevalence of
children that had gone to the dentist for preventive reasons. Children with dental caries
and whose mothers had a low level of education were less likely to have gone to the
dentist for preventive reasons.

7
There is an association between the type of healthcare (private/public) and
socioeconomic factors (Table 4). The majority of the sample sought for public service
(61.2%). Bivariate analyses demonstrate that the variables race, household income,
mother’s and father’s level of education, self-rated oral health and dental caries were
associated with the prevalence of children that sought for public service. Household
income, mother’s education and self-rated oral health remained associated with the
outcome after the adjustment. Children that rated their oral health as “fair / poor, from
low household income and whose mothers had a low level of education were more likely
to have visited the public service than other children.
Discussion
This paper provides the analyses on the complex association between the different
determinants of dental visits by Brazilian school children. In this study, 47.8% of school
children had a dental visit within previous 6 months. Such result is in accordance with
other study that documented a prevalence of dental care utilization within previous 6
months of 46.8 % among Brazilian children with similar age 6. Studies in other
developing countries have reported a prevalence of 27.7% among children in Mexico 2
and 1.7% in suburban African school 18. In develop countries, such as Spain and United
States, it has been reported a prevalence of child dental visit of 40% 10 and over 50%
respectively 19 . However, in both develop and developing countries, social gradients
even exists in children’s dental care utilization 1, 2, 10, 11, 19 .
We found that the use of dental service was strongly associated with
socioeconomic, psychosocial and clinical factors. In general, children at lower
socioeconomic status, with dental caries and with poor perception of oral health were
less likely to have gone to the dentist (Table 2).
It is widely recognized the underlying impact of socioeconomic conditions on
different health outcomes 20. Socioeconomic inequalities could affect oral health
operating at both individual and population level, and by psychosocial or material
deprivation causal pathways 20. In our study, increasing socioeconomic disadvantage
was related to decreased utilization of services. After the multiple regression analyses, it
could be demonstrated that children whose mothers have lower level of education
8
visited less frequently. This confirms previous reports regarding to the important
determinants of children’s dental visit, such as caregiver’s educational level 1, 11, 19. It has
been shown that level of education may reflect a range of non-economic conditions such
as the accumulation of knowledge which can influence the adoption of healthy habits or
improve social conditions 20. Results from previous study demonstrated that the parents
who have had no further education presented lower levels of dental knowledge and
positive dental attitudes 21. A general improved level of education may mean that
parents are more able to access appropriate sources of information and understand that
information more fully 21. Considering that these factors may be related to health’s
behaviors, it may help to explain why level of education is associated with dental
healthcare utilization 1, 5, 11. Nevertheless, inadequate resources, such as income or
knowledge, limit people’s opportunities for choice and the potential to gain control over
decision-making. The perceptions and interpretations of being constrained in deprived
social and material conditions are likely to evoke a chronic level of stress and further
erode the sense of life satisfaction in general. The low sense of control may impact
health indirectly through behaviors pathways such as to maintain an adequate utilization
of dental services.22.
The prevalence of children’s dental visit was associated with self-perception of oral
health and oral health status (Table 2). In general, children who rated their oral health
more favorably and with dental caries were more likely to have visited a dentist when
comparing to their counterparts.
Studies that related dental care utilization and self-rated oral health in school
children are scarce. Results from one study with 14-15-year-olds Brazilian adolescents
failed to find a relation between use of dental services and perception of oral health 14.
Other studies showed that the perception of oral health is directly affected by
socioeconomic factors 14, 16, 23. It is well established that people from low socioeconomic
backgrounds are more easily to be exposed to a various risk factors that affect their self-
perception of oral health and well-being 12, 24. Evidence suggested that individuals with
more oral diseases and at lower socioeconomic position do not generally visit the dentist
for routine checkups 2, 24 and they are more likely to rate their oral health as poor
compared to their counterparts 16, 23. Therefore, socioeconomic inequalities may be

9
associated with different health outcomes and such iniquities could affect the dental care
utilization by the underlying influence of the psychosocial, environmental and material
deprivation.
The results of table 3 showed that the prevalence of children who had gone to
the dentist for “other reasons than preventive” were associated with clinical and
socioeconomic conditions. Children with dental caries and whose mothers had a low
level of education were less likely to have gone to the dentist for preventive reasons.
Previous studies have demonstrated the impact of dental diseases in the
reasons for healthcare utilization 1, 3, 24, 25. A recent study found that oral health needs,
determined by the examiner in terms of caries burden, were positively associated with
the use of oral healthcare service for curative reasons 2. In addition, it has been
demonstrated that dental caries could cause toothache and previous research cited oral
pain as primary motivator for seeking dental attention 26. Therefore, the utilization of oral
health services is associated with greater oral health problems and such utilization
would be geared toward curative services than preventive.
Other studies showed the influence of socioeconomic status on the reasons for
healthcare utilization, which is characterized by a pro-rich inequity in the use of dental
service for check-ups or preventive reasons 4, 24, 27, 28. This is in agreement with our
results (Table 3). Children from low socioeconomic group and with high level of dental
diseases tend to receive episodic or emergency dental care, which may be the reason
for their highest prevalence of visiting a dentist just for restorative treatments or
underwent extractions.
The distribution of utilization at the types of oral healthcare (public or private)
varied across socioeconomic groups (Table 4). The majority of the sample visited the
public service (61.2%). Children whose mothers have lower level of education and from
low household income were more likely to have visited the public service than other
children.
Our results reveal a pro-poor utilization at the public healthcare, according to the
patterns of utilization. Data from official Brazilian publications showed that only 24.6% of
population has private health insurance 29. Moreover, the private dental service in Brazil
is expensive and, generally, only part of population can pay for care. Results from

10
Brazilian study with representative sample of children demonstrated that 85.4% had
used public dental services at least once in their lives 1. Thus, our findings are in
agreement with one recent study that reported that the poor are more likely to utilize
services at subsidized public and that an investment of care or allocation of resource to
city-areas may facilitate the access for worse-off people 27.
This study has several limitations. First, we used a cross-sectional design and,
therefore, we cannot determine causality and direction. Further studies using a
longitudinal design could increase the knowledge on determinants of dental healthcare
utilization. Second, the outcomes were collected through a self-administered
questionnaire sent to parents. It is possible that responsible did not clearly remember
information or responded incorrectly regarding children’s previous dental visits.
A single question asking people to rate their oral health would be one limitation.
However, this is one of the most frequently used measures of self-rated oral health
status. Moreover, a single item rating of perceived oral health is particularly appropriate
to obtain information from children and adolescents 16. Assessing perception of oral
health status is relatively simple and it may be an easier and complementary method to
collect dental information 14.
Besides of its limitations, this study is one of few to investigate the relation
between socioeconomic and psychosocial factors and dental healthcare utilization in
representative sample of Brazilian school children. This study showed that
socioeconomic gradients and psychosocial factors are important predictors for use of
dental services. Inequalities in dental services utilization were observed. Therefore, the
development of socially appropriate polices of oral health promotion is important for to
reduce these inequalities.

11
References
1. Noro LR, Roncalli AG, Mendes Junior FI, Lima KC. Use of dental care by children
and associated factors in Sobral, Ceara State, Brazil. Cad Saude Publica. 2008; 24:
1509-16.
2. Medina-Solis CE, Maupome G, del Socorro HM, Perez-Nunez R, Avila-Burgos L,
Lamadrid-Figueroa H. Dental health services utilization and associated factors in
children 6 to 12 years old in a low-income country. J Public Health Dent. 2008; 68: 39-
45.
3. Muirhead VE, Quinonez C, Figueiredo R, Locker D. Predictors of dental care
utilization among working poor Canadians. Community Dent Oral Epidemiol. 2009; 37:
199-208.
4. Pizarro V, Ferrer M, Domingo-Salvany A, Benach J, Borrell C, Pont A et al. The
utilization of dental care services according to health insurance coverage in Catalonia
(Spain). Community Dent Oral Epidemiol. 2009; 37: 78-84.
5. Medina-Solis CE, Maupome G, Avila-Burgos L, Hijar-Medina M, Segovia-
Villanueva A, Perez-Nunez R. Factors influencing the use of dental health services by
preschool children in Mexico. Pediatr Dent. 2006; 28: 285-92.
6. Freddo SL, Aerts DR, Abegg C, Davoglio R, Vieira PC, Monteiro L. Oral hygiene
habits and use of dental services among teenage students in a city in southern Brazil.
Cad Saude Publica. 2008; 24: 1991-2000.
7. Kramer PF, Ardenghi TM, Ferreira S, Fischer Lde A, Cardoso L, Feldens CA. Use
of dental services by preschool children in Canela, Rio Grande do Sul State, Brazil. Cad
Saude Publica. 2008; 24: 150-6.
8. IBGE. Instituto Brasileiro de Geografia e Estatística. [acessado em 29 novembro
2009]. Disponível em: URL: http://www.ibge.gov.br
9. Jiang H, Petersen PE, Peng B, Tai B, Bian Z. Self-assessed dental health, oral
health practices, and general health behaviors in Chinese urban adolescents. Acta
Odontol Scand. 2005; 63: 343-52.

12
10. Jimenez R, Tapias-Ledesma MA, Gallardo-Pino C, Carrasco P, de Miguel AG.
Influence of sociodemographic variables on use of dental services, oral health and oral
hygiene among Spanish children. Int Dent J. 2004; 54: 187-92.
11. Sohn W, Ismail A, Amaya A, Lepkowski J. Determinants of dental care visits
among low-income African-American children. J Am Dent Assoc. 2007; 138: 309-18;
quiz 95-96, 98.
12. Araujo CS, Lima RC, Peres MA, Barros AJ. Use of dental services and
associated factors: a population-based study in southern Brazil. Cad Saude Publica.
2009; 25: 1063-72.
13. Tassinari Wde S, de Leon AP, Werneck GL, Faerstein E, Lopes CS, Chor D et al.
[Socioeconomic context and perceived oral health in an adult population in Rio de
Janeiro, Brazil: A multilevel analysis. Cad Saude Publica. 2007; 23: 127-36.
14. Pattussi MP, Olinto MT, Hardy R, Sheiham A. Clinical, social and psychosocial
factors associated with self-rated oral health in Brazilian adolescents. Community Dent
Oral Epidemiol. 2007; 35: 377-86.
15. Sanders AE, Slade GD. Deficits in perceptions of oral health relative to general
health in populations. J Public Health Dent. 2006; 66: 255-62.
16. Perera I, Ekanayake L. Factors influencing perception of oral health among
adolescents in Sri Lanka. Int Dent J. 2008; 58: 349-55.
17. WHO. Oral health surveys basic methods 4ed. GENEVA: World Health
Organization 1997.
18. Adekoya-Sofowora CA, Nasir WO, Oginni AO, Taiwo M. Dental caries in 12-year-
old suburban Nigerian school children. Afr Health Sci. 2006; 6: 145-50.
19. Vargas CM, Ronzio CR. Relationship between children's dental needs and dental
care utilization: United States, 1988-1994. Am J Public Health. 2002; 92: 1816-21.
20. Braveman PA, Cubbin C, Egerter S, Chideya S, Marchi KS, Metzler M et al.
Socioeconomic status in health research: one size does not fit all. Jama. 2005; 294:
2879-88.
21. Williams NJ, Whittle JG, Gatrell AC. The relationship between socio-demographic
characteristics and dental health knowledge and attitudes of parents with young
children. Br Dent J. 2002; 193: 651-4; discussion 42.

13
22. Sanders AE, Spencer AJ. Why do poor adults rate their oral health poorly? Aust
Dent J. 2005; 50: 161-7.
23. Matos DL, Lima-Costa MF. Self-rated oral health among Brazilian adults and
older adults in Southeast Brazil: results from the SB-Brasil Project, 2003. Cad Saude
Publica. 2006; 22: 1699-707.
24. Afonso-Souza G, Nadanovsky P, Chor D, Faerstein E, Werneck GL, Lopes CS.
Association between routine visits for dental checkup and self-perceived oral health in
an adult population in Rio de Janeiro: the Pro-Saude Study. Community Dent Oral
Epidemiol. 2007; 35: 393-400.
25. Brennan DS, Luzzi L, Roberts-Thomson KF. Dental service patterns among
private and public adult patients in Australia. BMC Health Serv Res. 2008; 8: 1.
26. Duncan RP, Gilbert GH, Peek CW, Heft MW. The dynamics of toothache pain
and dental services utilization: 24-month incidence. J Public Health Dent. 2003; 63: 227-
34.
27. Somkotra T, Detsomboonrat P. Is there equity in oral healthcare utilization:
experience after achieving Universal Coverage. Community Dent Oral Epidemiol. 2009;
37: 85-96.
28. Bhatti T, Rana Z, Grootendorst P. Dental insurance, income and the use of dental
care in Canada. J Can Dent Assoc. 2007; 73: 57.
29. Pinheiro R, Torres T. Uso de serviços odontológicos entre os Estados do Brasil. .
Ciênc Saúde Coletiva. 2006; 11: 999-1010.

14
Table 1. Clinical and demographic characteristics of the sample.
Variable n* (%)
Gender
Male 351 44.3
Female 441 55.7
Ethnics
White 609 77.8
Non-White 174 22.2
Household Income
≥ 2BMW 341 51.1
< 2BMW 326 48.9
Mother’s schooling
≥ 8 years 330 43.1
< 8 years 434 56.8
Father’s schooling
≥ 8 years 273 40.0
< 8 years 465 63.0
Dental caries
DMF =0 481 60.7
DMF >0 311 39.3
Self-rated oral health
Good-excellent 389 49.1
Fair-poor 403 50.9
BMW= Brazilian Minimum Wage

15
Table 2- Predictors of dental service utilization within previous 6 months (Prevalence ratio:
95%IC).
Visited the service Variables N
n (%) PR (95%IC) PR adj.(95%IC)
Gender 751 359 (47.8) p = 0.64
Male 333 156 (43.4) 1
Female 418 203 (56.5) 1.03 (0.89 – 1.20)
Ethnics 743 352 (47.4) p = 0.06 **
White 581 286 (49.3) 1
Non-White 162 66 (40.7) 0.82 (0.67 – 1.01)
Household Income 639 297 (46.5) p = 0.07 **
≥ 2BMW 331 165 (49.8) 1
< 2BMW 308 132 (42.8) 0.85 (0.72 – 1.01)
Mother’s level of education 727 346 (47.6) p = 0.02 p = 0.02
≥ 8 years 319 167 (52.3) 1 1
< 8 years 408 179 (43.9) 0.83 (0.72 – 0.97) 0.83 (0.71 – 0.96)
Father’s level of education 703 336 (47.8) p = 0.01 **
≥ 8 years 266 142 (53.4) 1
< 8 years 437 194 (44.4) 0.83 (0.71 – 0.96)
Dental caries 751 359 (47.8) p = 0.03 p = 0.02
DMF=0 452 202 (44.7) 1 1
DMF>0 299 157 (52.5) 1.17 (1.01 – 1.36) 1.20 ( 1.03 – 1.40)
Self-rated oral health 751 359 (47.8) p = 0.03 p = 0.01
Good-excellent 373 193 (51.7) 1 1
Fair-poor 378 166 (43.9) 0.84 (0.73 – 0.98) 0.82 ( 0.71 – 0.96)
* values lower than 792 due missing data
**= Variables not included in the final multiple model after the adjustment.

16
Table 3. Reason for the dental visit (preventive/other) and associated factors (Prevalence
ratio:95%IC).
Reason for the visit (preventive)Variables N
n (%) PR (95%IC) PR adj.(95%IC)
Gender 748 367 (49.1) p = 0.36
Male 332 169 (50.9) 1
Female 416 198 (47.6) 0.93 (0.80 – 1.08)
Ethnics 740 363 (49.0) p = 0.07 **
White 582 296 (50.9) 1
Non-White 158 67 (42.4) 0.83 (0.68 – 1.01)
Household Income 636 304 (47.8) p = 0.03 **
≥ 2BMW 303 171 (51.8) 1
< 2BMW 306 133 (43.5) 0.83 (0.71 – 0.98)
Mother’s level of education 723 353 (48.8) p < 0.01 p = 0.04
≥ 8 years 318 173 (54.4) 1 1
< 8 years 405 180 (44.4) 0.81 (0.70 – 0.94) 0.85 (0.74 – 0.99)
Father’s level of education 699 339 (48.5) p = 0.13 **
≥ 8 years 267 139 (52.1) 1
< 8 years 432 200 (46.3) 0.88 (0.76 – 1.03)
Dental caries 748 367 (49.1) p < 0.01 p < 0.01
DMF=0 450 256 (56.9) 1 1
DMF>0 298 111 (37.2) 0.65 (0.55 – 0.77) 0.67 (0.57 – 0.80)
Self-rated oral health 748 367 (49.1) p = 0.42
Good-excellent 374 189 (50.5) 1
Fair-poor 374 178 (47.6) 0.94 (0.81 – 1.09)
* values lower than 792 due missing data
**= Variables not included in the final multiple model after the adjustment.

17
Table 4. Type of healthcare used (private/public) and associated factors (Prevalence ratio:95%IC).
Type of Healthcare (PR for public)Variables N
n (%) PR (95%IC) PR adj.(95%IC)
Gender 745 456 (61.2) p = 0.10 **
Male 328 190 (57.9) 1
Female 417 266 (63.8) 1.10 (0.97 – 1.23)
Ethnics 738 452 (61.2) p < 0.01 **
White 577 336 (58.2) 1
Non-White 161 116 (72.0) 1.23 (1.09 – 1.39)
Household Income 633 399 (63.0) p < 0.01 p < 0.01
≥ 2BMW 330 154 (46.7) 1 1
< 2BMW 303 245 (80.9) 1.73 (1.52 – 1.96) 1.51 (1.33 – 1.72)
Mother’s level of education 722 441 (61.1) p < 0.01 p < 0.01
≥ 8 years 317 137 (43.2) 1 1
< 8 years 415 304 (75.1) 1.73 (1.51 – 1.99) 1.50 (1.30 – 1.72)
Father’s level of education 699 420 (60.1) p < 0.01 **
≥ 8 years 263 115 (43.7) 1
< 8 years
Dental caries 436 305 (69.9) 1.59 (1.37 – 1.85)
DMF=0 450 259 (57.6) 1
DMF>0 295 197 (66.8) 1.16 (1.03 – 1.29)
Self-rated oral-health 745 456 (61.2) p < 0.01 p < 0.01
Good-excellent 371 206 (55.5) 1 1
Fair-poor 374 250 (66.8) 1.20 (1.07 – 1.35) 1.16 (1.04 – 1.30)
* values lower than 792 due missing data
**= Variables not included in the final multiple model after the adjustment.

4 DISCUSSÃO GERAL E CONCLUSÃO
Esta dissertação avaliou o efeito dos fatores socioeconômicos, clínicos e
psicossociais na qualidade de vida relacionada à saúde bucal (COHRQoL) e na
utilização dos serviços odontológicos em escolares de 12 anos de idade de Santa Maria
– RS. Apesar de estudos prévios já terem demonstrado o impacto dos fatores
socioeconômicos e psicossociais na COHRQoL (LOCKER, 2007b) e na utilização dos
serviços odontológicos em crianças (SOHN et al., 2007; MEDINA-SOLIS et al., 2008b;
NORO et al., 2008), este é o primeiro estudo que avaliou a associação destes
preditores com COHRQoL em uma amostra representativa de crianças de 12 anos de
idade utilizando o CPQ11-14. Além disso, estudos que abordaram o efeito da
autopercepção de saúde oral na utilização dos serviços odontológicos em crianças são
escassos.
Pelo atual estudo, o que se pode constatar de maneira significativa foi a
influência dos preditores socioeconômicos nos desfechos considerados.
Variáveis socioeconômicas, como renda, etnia, nível educacional e classe social
podem influenciar negativamente a qualidade de vida relacionada à saúde bucal e a
utilização dos serviços odontológicos (SANDERS et al., 2006b; PATTUSSI et al., 2007;
PERERA; EKANAYAKE, 2008; SABBAH et al., 2009b). Estudos anteriores sugerem
que indivíduos de menor nível socioeconômico tendem a concentrar maiores níveis de
doenças orais, e, esta condição, poderia causar maior impacto na sua qualidade de
vida ocasionando uma autopercepção negativa da sua saúde oral e,
consequentemente, influenciando o padrão de utilização dos serviços odontológicos e
os comportamentos relacionados à saúde (AFONSO-SOUZA et al., 2007; PATTUSSI et
al., 2007; PERERA ; EKANAYAKE, 2008).
É sugerido que esta complexa relação existente entre status socioeconômico e
saúde é decorrente das diferenças culturais e comportamentais dos indivíduos, ou seja,
indivíduos de baixo nível socioeconômico tendem a apresentar restrito acesso a
serviços básicos de saúde, capital social reduzido e exposição a fatores de risco
(MELCHIOR et al., 2007; SISSON, 2007; PERES et al., 2009). Além disso, estudos
demonstraram que o nível de escolaridade materna, usado como “proxy” para status

54
socioeconômico, é um importante determinante para a visita odontológica da criança
(VARGAS; RONZIO, 2002; SOHN et al., 2007; NORO et al., 2008).
Poucos estudos têm demonstrado a associação de gradientes educacionais com
medidas subjetivas de saúde oral (BORRELL et al., 2004; SANDERS et al., 2006b;
SABBAH et al., 2007a) e nenhum estudo avaliou o impacto do nível educacional
materno nos scores do CPQ11-14. Porém, tem sido sugerido que a saúde oral da criança
pode ser correlacionada com o nível de escolaridade da mãe (PINE et al., 2004;
FERREIRA et al., 2007; TRAEBERT et al., 2009) e o ambiente no qual a criança está
inserida pode influenciar seus comportamentos relacionados a saúde e o modo como
ela percebe sua saúde oral (LOCKER, 2007b).
Este estudo também demonstrou que variáveis clínicas estiveram associadas
negativamente à autopercepção dos escolares e a utilização dos serviços
odontológicos. Sabe-se que o status de saúde oral dos indivíduos contribui
significativamente para a sua qualidade de vida e pode afetá-los tanto fisicamente
quanto psicologicamente e socialmente (LOCKER, 1988a; LOCKER, 2007b; TSAKOS
et al., 2009). Os efeitos reportados por crianças com experiência severa de cárie
dentária incluem dor, desconforto, dificuldade de mastigação, diminuição do rendimento
escolar e alteração no comportamento (FEITOSA; COLARES; PINKHAM, 2005;
FOSTER PAGE et al., 2005) e, estudos anteriores, citaram a dor dental como primeiro
motivador para a procura por atendimento odontológico (DUNCAN et al., 2003).
Portanto, condições desfavoráveis de saúde bucal são importantes coadjuvantes
negativos que podem interferir na qualidade de vida dos indivíduos e no padrão de
utilização dos serviços odontológicos, por causarem dor, sofrimento, problemas
psicológicos, privação social e prejuízos em nível individual e coletivo (JOKOVIC et al.,
2002a; BROWN; AL-KHAYAL, 2006; MEDINA-SOLIS et al., 2006a; DO; SPENCER,
2007a; GOMES; ABEGG, 2007; ANTUNES et al., 2008; GOURSAND et al., 2008;
MEDINA-SOLIS et al., 2008b; BARBOSA; TURELI ;GAVIAO, 2009).
Neste estudo, devido à utilização do delineamento transversal, os resultados
devem ser interpretados com cautela. Mesmo que se tenha realizado um estudo com
uma amostra representativa, vieses poderiam ocorrer principalmente no que se refere
ao tipo de estudo utilizado. Este tipo de delineamento não nos permite estabelecer o

55
nexo temporal entre preditores e desfecho, ou seja, uma relação causa-efeito não pode
ser verdadeiramente obtida. No entanto, esse tipo de investigação é conveniente para
obtermos o primeiro retrato das condições de saúde bucal de uma população. Sugere-
se a realização de estudos longitudinais, que permitam o acompanhamento dos
indivíduos para confirmar os nossos resultados.
Considerando as limitações de cada estudo apresentado e discutidas
previamente, nós acreditamos que estes estudos trazem informações relevantes para a
prática clínica e de saúde pública. Até o presente momento, não há estudos na
literatura que utilizaram o CPQ11-14 em uma amostra representativa de crianças de 12
anos de idade para verificar o impacto das condições de saúde bucal e fatores
socioeconômicos na qualidade de vida. Além disso, os resultados dos estudos que
avaliaram a associação entre autopercepção de saúde oral de crianças desta faixa
etária e a utilização dos serviços odontológicos são escassos e conflitantes. A utilização
desses dados em conjunto com indicadores normativos serviria como base para a
tomada de decisões públicas de acordo com as reais necessidades da população e
para um redirecionamento dos recursos alocados em saúde.
Em resumo, os dados demonstram que fatores clínicos, socioeconômicos e
psicossociais causam impacto na qualidade de vida de crianças e influenciam o padrão
de utilização dos serviços odontológicos em crianças de 12 anos de idade de Santa
Maria - RS.

56
5 REFERÊNCIAS *
1. ADULYANON, S., VOURAPUKJARU, J., SHEIHAM, A. Oral impacts affecting daily performance in a low dental disease Thai population. Community Dent Oral Epidemiol , v.24, n.6, p.385-9, 1996.
2. AFONSO-SOUZA, G. et al. Association between routine visits for dental checkup and self-perceived oral health in an adult population in Rio de Janeiro: the Pro-Saude Study. Community Dent Oral Epidemiol , v.35, n.5, p.393-400, 2007.
3. ANTUNES, J.L. et al. Gingival health of adolescents and the utilization of dental services, state of Sao Paulo, Brazil. Rev Saude Publica , v.42, n.2, p.191-9, 2008.
4. BARBOSA, T.S., TURELI, M.C., GAVIAO, M.B. Validity and reliability of the Child Perceptions Questionnaires applied in Brazilian children. BMC Oral Health , v.9, p.13, 2009.
5. BORRELL, L.N. et al. Perception of general and oral health in White and African American adults: assessing the effect of neighborhood socioeconomic conditions. Community Dent Oral Epidemiol , v.32, n.5, p.363-73, 2004.
6. BRAVEMAN, P.A. et al. Socioeconomic status in health research: one size does not fit all. Jama , v.294, n.22, p.2879-88, 2005.
7. BRODER, H.L., MCGRATH, C., CISNEROS, G.J. Questionnaire development: face validity and item impact testing of the Child Oral Health Impact Profile. Community Dent Oral Epidemiol , v.35 Suppl 1, p.8-19, 2007.
8. BROWN, A., AL-KHAYAL, Z. Validity and reliability of the Arabic translation of the child oral-health-related quality of life questionnaire (CPQ11-14) in Saudi Arabia. Int J Paediatr Dent , v.16, n.6, p.405-11, 2006.
9. CASTRO, R.A. et al. Child-OIDP index in Brazil: cross-cultural adaptation and validation. Health Qual Life Outcomes , v.6, p.68, 2008.
10. DO, L.G., SPENCER, A.J. Oral health-related quality of life of children by dental caries and fluorosis experience. J Public Health Dent , v.67, n.3, p.132-9, 2007a.

57
11. DO, L.G., SPENCER, A.J. Evaluation of oral health-related quality of life questionnaires in a general child population. Community Dent Health , v.25, n.4, p.205-10, 2008b.
12. DUNCAN, R.P. et al. The dynamics of toothache pain and dental services utilization: 24-month incidence. J Public Health Dent , v.63, n.4, p.227-34, 2003.
13. FEITOSA, S.,COLARES, V., PINKHAM, J. The psychosocial effects of severe caries in 4-year-old children in Recife, Pernambuco, Brazil. Cad Saude Publica , v.21, n.5, p.1550-6, 2005.
14. FERREIRA, S.H. et al. Dental caries in 0- to 5-year-old Brazilian children: prevalence, severity, and associated factors. Int J Paediatr Dent , v.17, n.4, p.289-96, 2007.
15. FOSTER PAGE, L.A. et al. Validation of the Child Perceptions Questionnaire (CPQ 11-14). J Dent Res , v.84, n.7, p.649-52, 2005.
16. FREDDO, S.L. et al. Oral hygiene habits and use of dental services among teenage students in a city in southern Brazil. Cad Saude Publica , v.24, n.9, p.1991-2000, 2008.
17. GHERUNPONG, S., SHEIHAM, A., TSAKOS, G. A sociodental approach to assessing children's oral health needs: integrating an oral health-related quality of life (OHRQoL) measure into oral health service planning. Bull World Health Organ , v.84, n.1, p.36-42, 2006a.
18. GHERUNPONG, S., TSAKOS, G., SHEIHAM, A. Developing and evaluating an oral health-related quality of life index for children; the CHILD-OIDP. Community Dent Health , v.21, n.2, p.161-9, 2004b.
19. GOMES, A.S., ABEGG, C. The impact of oral health on daily performance of municipal waste disposal workers in Porto Alegre, Rio Grande do Sul State, Brazil. Cad Saude Publica , v.23, n.7, p.1707-14, 2007.
20. GOURSAND, D. et al. Cross-cultural adaptation of the Child Perceptions Questionnaire 11-14 (CPQ11-14) for the Brazilian Portuguese language. Health Qual Life Outcomes , v.6, p.2, 2008.
58
21. JIANG, H. et al. Self-assessed dental health, oral health practices, and general health behaviors in Chinese urban adolescents. Acta Odontol Scand , v.63, n.6, p.343-52, 2005.
22. JOKOVIC, A. et al. Validity and reliability of a questionnaire for measuring child oral-health-related quality of life. J Dent Res , v.81, n.7, p.459-63, 2002a.
23. JOKOVIC, A. et al. Questionnaire for measuring oral health-related quality of life in eight- to ten-year-old children. Pediatr Dent , v.26, n.6, p.512-8, 2004b.
24. KRAMER, P.F. et al. Use of dental services by preschool children in Canela, Rio Grande do Sul State, Brazil. Cad Saude Publica , v.24, n.1, p.150-6, 2008.
25. LEÃO, A.T., LOCKER, D. Impacto das condições de saúde bucal na qualidade de vida . In: Antunes, J.L.F.; Peres, M.A. Epidemiologia da saúde bucal. Rio de Janeiro: Guanabara Koogan; 2006. cap. 3, parte 2, p. 260-8.
26. LOCKER, D. Measuring oral health: a conceptual framework. Community Dent Health , v.5, n.1, p.3-18, 1988a.
27. LOCKER, D. Disparities in oral health-related quality of life in a population of Canadian children. Community Dent Oral Epidemiol , v.35, n.5, p.348-56, 2007b.
28. MARSHMAN, Z. et al. An evaluation of the Child Perceptions Questionnaire in the UK. Community Dent Health , v.22, n.3, p.151-5, 2005.
29. MATOS, D.L., LIMA-COSTA, M.F. Self-rated oral health among Brazilian adults and older adults in Southeast Brazil: results from the SB-Brasil Project, 2003. Cad Saude Publica , v.22, n.8, p.1699-707, 2006a.
30. MATOS, D.L. et al. The Bambui Project: a population-based study of factors associated with regular utilization of dental services in adults. Cad Saude Publica , v.17, n.3, p.661-8, 2001b.
31. MCGRATH, C.,BRODER, H., WILSON-GENDERSON, M. Assessing the impact of oral health on the life quality of children: implications for research and practice. Community Dent Oral Epidemiol , v.32, n.2, p.81-5, 2004a.

59
32. MCGRATH, C. et al. Translation and evaluation of a Chinese version of the Child Oral Health-related Quality of Life measure. Int J Paediatr Dent , v.18, n.4, p.267-74, 2008b.
33. MEDINA-SOLIS, C.E. et al. Factors influencing the use of dental health services by preschool children in Mexico. Pediatr Dent , v.28, n.3, p.285-92, 2006a.
34. MEDINA-SOLIS, C.E. et al. Dental health services utilization and associated factors in children 6 to 12 years old in a low-income country. J Public Health Dent , v.68, n.1, p.39-45, 2008b.
35. MELCHIOR, M. et al. Why do children from socioeconomically disadvantaged families suffer from poor health when they reach adulthood? A life-course study. Am J Epidemiol , v.166, n.8, p.966-74, 2007.
36. NORO, L.R. et al. Use of dental care by children and associated factors in Sobral, Ceara State, Brazil. Cad Saude Publica , v.24, n.7, p.1509-16, 2008.
37. O'BRIEN, K. et al. The child perception questionnaire is valid for malocclusions in the United Kingdom. Am J Orthod Dentofacial Orthop , v.129, n.4, p.536-40, 2006.
38. PAHEL, B.T., ROZIER, R.G., Slade, G.D. Parental perceptions of children's oral health: the Early Childhood Oral Health Impact Scale (ECOHIS). Health Qual Life Outcomes , v.5, p.6, 2007.
39. PATTUSSI, M.P. et al. Clinical, social and psychosocial factors associated with self-rated oral health in Brazilian adolescents. Community Dent Oral Epidemiol , v.35, n.5, p.377-86, 2007.
40. PERERA, I., EKANAYAKE, L. Factors influencing perception of oral health among adolescents in Sri Lanka. Int Dent J , v.58, n.6, p.349-55, 2008.
41. PERES, M.A. et al. Life course dental caries determinants and predictors in children aged 12 years: a population-based birth cohort. Community Dent Oral Epidemiol , v.37, n.2, p.123-33, 2009.
42. PINE, C.M. et al. International comparisons of health inequalities in childhood dental caries. Community Dent Health , v.21, n.1 Suppl, p.121-30, 2004.

60
43. PINHEIRO, R., TORRES, T. Uso de serviços odontológicos entre os Estados do Brasil. . Ciênc Saúde Coletiva , v.11, p.999-1010, 2006.
44. SABBAH, W. et al. Social gradients in oral and general health. J Dent Res , v.86, n.10, p.992-6, 2007a.
45. SABBAH, W. et al. The effects of income and education on ethnic differences in oral health: a study in US adults. J Epidemiol Community Health , v.63, n.7, p.516-20, 2009b.
46. SANDERS, A.E., SLADE, G.D. Deficits in perceptions of oral health relative to general health in populations. J Public Health Dent , v.66, n.4, p.255-62, 2006a.
47. SANDERS, A.E. et al. The shape of the socioeconomic-oral health gradient: implications for theoretical explanations. Community Dent Oral Epidemiol , v.34, n.4, p.310-9, 2006b.
48. SISSON, K.L. Theoretical explanations for social inequalities in oral health. Community Dent Oral Epidemiol , v.35, n.2, p.81-8, 2007.
49. SLADE, G.D. Assessing change in quality of life using the Oral Health Impact Profile. Community Dent Oral Epidemiol , v.26, n.1, p.52-61, 1998a.
50. SLADE, G.D., SPENCER, A.J. Development and evaluation of the Oral Health Impact Profile. Community Dent Health , v.11, n.1, p.3-11, 1994b.
51. SOHN, W. et al. Determinants of dental care visits among low-income African-American children. J Am Dent Assoc , v.138, n.3, p.309-18; quiz 95-96, 98, 2007.
52. SOMKOTRA, T., DETSOMBOONRAT, P. Is there equity in oral healthcare utilization: experience after achieving Universal Coverage. Community Dent Oral Epidemiol , v.37, n.1, p.85-96, 2009.
53. TALEKAR, B.S., ROZIER, R.G., SLADE, G.D. Development of an OHRQoL instrument for preschool children. . J Dent Res , v.83, p.686, 2004.

61
54. TESCH, F.C., OLIVEIRA, B.H., LEAO, A. Measuring the impact of oral health problems on children's quality of life: conceptual and methodological issues. Cad Saude Publica , v.23, n.11, p.2555-64, 2007a.
55. TESCH, F.C.,OLIVEIRA, B.H., LEAO, A. Semantic equivalence of the Brazilian version of the Early Childhood Oral Health Impact Scale. Cad Saude Publica , v.24, n.8, p.1897-909, 2008b.
56. TORRES, C.S. et al. Psychometric properties of the Brazilian version of the Child Perceptions Questionnaire (CPQ11-14) - short forms. Health Qual Life Outcomes , v.7, p.43, 2009.
57. TRAEBERT, J. et al. Low maternal schooling and severity of dental caries in Brazilian preschool children. Oral Health Prev Dent , v.7, n.1, p.39-45, 2009.
58. TSAKOS, G. et al. The impact of educational level on oral health-related quality of life in older people in London. Eur J Oral Sci , v.117, n.3, p.286-92, 2009.
59. VARGAS, C.M., RONZIO, C.R. Relationship between children's dental needs and dental care utilization: United States, 1988-1994. Am J Public Health , v.92, n.11, p.1816-21, 2002.
60. WATT, R.G. From victim blaming to upstream action: tackling the social determinants of oral health inequalities. Community Dent Oral Epidemiol , v.35, n.1, p.1-11, 2007.
61. WOGELIUS, P. et al. Development of Danish version of child oral-health-related quality of life questionnaires (CPQ8-10 and CPQ11-14). BMC Oral Health , v.9, p.11, 2009.
*
* Estrutura e apresentação de monografias, dissertações e teses: MDT / UFSM

� ��
APÊNDICE A - TERMO DE CONSENTIMENTO LIVRE E ESCLARE CIDO
Universidade Federal de Santa Maria
Centro de Ciências Da Saúde
Curso de Odontologia
Departamento de Estomatologia
Pesquisador responsável : Thiago Machado Ardenghi Endereço: Cel. Niederauer 917, apto:208, Santa Maria-RS. Contato: 3220 9266
Nome do adolescente: .............................. ............................................
Este termo tem como objetivo informar, esclarecer e pedir a sua
autorização para a participação de seu/sua filho (a) na pesquisa intitulada:
“IMPACTO DOS FATORES SOCIOECONOMICOS, PSICOSSOCIAIS E CLÍNICOS
NA QUALIDADE DE VIDA E NA UTILIZAÇÃO DOS SERVIÇOS ODONTOLÓGICOS
EM ESCOLARES” com orientação do Prof. Dr. Thiago Machado Ardenghi. Esta
pesquisa tem como objetivo avaliar como a cárie e os traumas dentais podem afetar
o desempenho escolar e a qualidade de vida de crianças. Sabendo isto, ficará mais
fácil de verificar as necessidade de cuidados com a saúde bucal de seu/sua filho (a).
A pesquisa será desenvolvida na própria escola do seu filho, durante um
intervalo de aula. Dentistas da Universidade Federal de Santa Maria irão realizar um
exame na boca de seu/sua filho (a), para verificar se ele (a) tem cárie, se ele bateu
algum dente ou tem desgaste. Após o exame O seu (sua) filho (a) também
responderá a uma entrevista realizada pelas dentistas onde ele (a) irá responder
como é sua mastigação, fala, alimentação, sua satisfação com o sorriso, entre
outros. Seu/sua filho (a) não terá nenhum gasto financeiro ou danos participando
desta pesquisa. Como esta pesquisa se trata apenas de um exame odontológico e
preenchimento de um questionário, os riscos que poderão ocorrer na participação
do Sr (a) e seu/sua filho (a) nesta pesquisa são pequenos como, por exemplo,
cansaço durante o exame ou preenchimento do questionário, e/ou desconforto na
hora de ver a boca, sendo que como benefício, o Sr. (Sra.) será informado e
orientado a procurar assistência odontológica caso seja observado algum problema
durante o exame do (a) seu/sua filho (a). Cabe repetir que o (a) Sr (a) será
orientado a procurar um atendimento, não sendo de responsabilidade desta

� ��
pesquisa dar garantia de que este atendimento seja realizado caso seja encontrado
algum problema no seu filho. Também será pedido que o (a) Sr (a) responda um
questionário a respeito das suas condições socioeconômicas, sendo que o (a) Sr (a)
não é obrigado a responder este questionário, mesmo que o Sr (a) permita que
seu/sua filho (a) participe da pesquisa.
Todos os dados de identificação de seu/sua filho (a) serão mantidos em
sigilo. O seu/sua filho (a) poderá se recusar participar da pesquisa, bem como
interromper o exame a qualquer momento sem que aja qualquer problema para ele
na escola ou quando ele for procurar atendimento odontológico. Para esclarecer
qualquer dúvida, o (a) senhor (a) poderá falar com o pesquisador pelo telefone ou
endereço de contato que estão escritos no início deste documento. Este documento
foi redigido em duas vias (uma do pesquisador e outra que lhe está sendo entregue)
Eu_____________________________, R.G._____________, declaro que fui
devidamente esclarecido (a), e estou de acordo com os termos acima expostos,
autorizando a participação de meu/minha filho (a) ________________________
nesta pesquisa.________________________-
_____________________ ______________________
Assinatura do responsável Thiago Machado Ardenghi
Qualquer esclarecimento entre em contato com:
Comitê de Ética em Pesquisa da UFSM:
Comitê de Ética em Pesquisa - UFSM - Av. Roraima, 1000 – Prédio da Reitoria - 7º
andar - Campus Universitário. 97105-900 – Santa Maria – RS. Tel:0xx55-3220-
9362– email: [email protected]
Prof.Thiago Machado Ardenghi (pesquisador responsáv el)
Rua Cel. Niederauer, 917, ap.: 208, Santa Maria-RS
email: [email protected]

64
APÊNDICE B - QUESTIONÁRIO SOCIOECONÔMICO
Nome do adolescente:_________________________________________________
Endereço:___________________________________________________________
Data de Nascimento:___/___/___ Sexo: F ( ) M ( )
Você considera seu filho da raça: ( ) branca ( ) negra ( ) mulato ( )outro
(oriental, índio)
Seu filho mora com: pai e mãe ( ); só com a mãe ( ); só com o pai ( );
outros ( )
Quantos cômodos tem a casa? _________
Renda familiar: _________ reais Quantos irmãos o adolescentes tem?
________
O pai do adolescente trabalha? Sim ( ) Não ( )
A mãe do adolescente trabalha? Sim ( ) Não ( )
A mãe estudou até: não estudou( ); até 1 grau ( ); até 2 grau ( ); terminou
faculdade ( )
O pai estudou até: não estudou( ); até 1 grau ( ); até 2 grau ( ); terminou
faculdade ( )
Procurou dentista nos últimos 6 meses? S ( ) N ( )
Tempo decorrido desde a última visita: ( ) até 3 meses
( ) 3 a 6 meses ( ) 6 meses a 1 ano ( ) mais que 1 ano;
Motivo da última consulta: ( )dor de dente; ( ) dor na boca ( ) batidas e quedas
( )exame e rotina
( ) outros:_______________________
Tipo de serviço que você levou seu filho na última consulta: ( )dentista particular (
) dentista público (posto de saúde, faculdade, escola)

AP
ÊN
DIC
E C
– F
ICH
A C
LÍN
ICA
– O
DO
NT
OG
RA
MA
Nom
e: _
____
____
____
____
____
____
__
id
ade:
___
____
____
5
5
54
53
52
51
61
6
2
63
6
4
65
85
8
4
8
3
82
81
7
1
72
7
3
74
75
TR
AU
MA
TIS
MO
:
11:
12:
21:
22
SE
LAM
EN
TO
LA
BIA
L: (
)
adeq
uado
(
) n
ão a
dequ
ado
OV
ER
JET
: (
) n
orm
al
(
) a
cent
uado
____
_mm
65
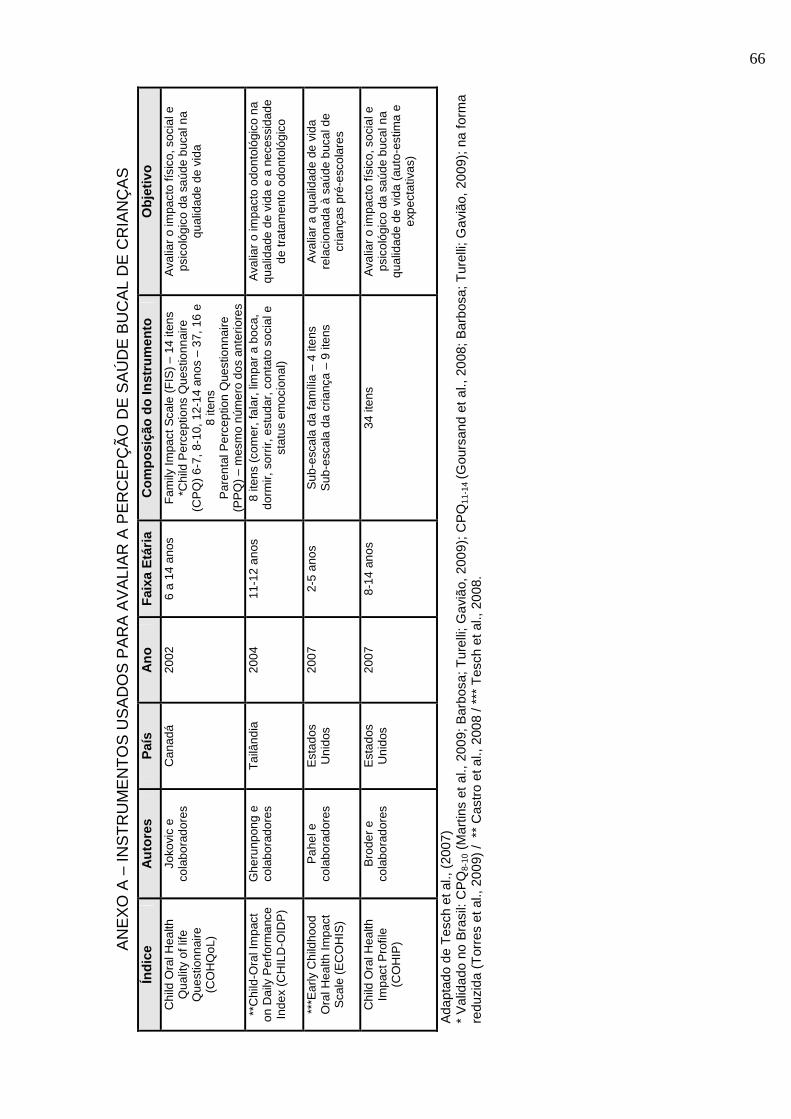
AN
EX
O A
– IN
ST
RU
ME
NT
OS
US
AD
OS
PA
RA
AV
ALI
AR
A P
ER
CE
PÇ
ÃO
DE
SA
ÚD
E B
UC
AL
DE
CR
IAN
ÇA
S
Ada
ptad
o de
Tes
ch e
t al.,
(20
07)
* V
alid
ado
no B
rasi
l: C
PQ
8-10
(M
artin
s et
al.,
200
9; B
arbo
sa; T
urel
li; G
aviã
o, 2
009)
; CP
Q11
-14
(Gou
rsan
d et
al.,
200
8; B
arbo
sa; T
urel
li; G
aviã
o, 2
009)
; na
form
a re
duzi
da (
Tor
res
et a
l., 2
009)
/ *
* C
astr
o et
al.,
200
8 / *
** T
esch
et a
l., 2
008.
Índi
ce
Aut
ores
P
aís
Ano
F
aixa
Etá
ria
Com
posi
ção
do In
stru
men
to
Obj
etiv
o
Chi
ld O
ral H
ealth
Q
ualit
y of
life
Q
uest
ionn
aire
(C
OH
QoL
)
Joko
vic
e co
labo
rado
res
Can
adá
2002
6
a 14
ano
s F
amily
Impa
ct S
cale
(F
IS)
– 14
iten
s *C
hild
Per
cept
ions
Que
stio
nnai
re
(CP
Q)
6-7,
8-1
0, 1
2-14
ano
s –
37, 1
6 e
8 ite
ns
Par
enta
l Per
cept
ion
Que
stio
nnai
re
(PP
Q)
– m
esm
o nú
mer
o do
s an
terio
res
Ava
liar
o im
pact
o fís
ico,
soc
ial e
ps
icol
ógic
o da
saú
de b
ucal
na
qual
idad
e de
vid
a
**C
hild
-Ora
l Im
pact
on
Dai
ly P
erfo
rman
ce
Inde
x (C
HIL
D-O
IDP
)
Ghe
runp
ong
e co
labo
rado
res
Tai
lând
ia
2004
11
-12
anos
8
itens
(co
mer
, fal
ar, l
impa
r a
boca
, do
rmir,
sor
rir, e
stud
ar, c
onta
to s
ocia
l e
stat
us e
moc
iona
l)
Ava
liar
o im
pact
o od
onto
lógi
co n
a qu
alid
ade
de v
ida
e a
nece
ssid
ade
de tr
atam
ento
odo
ntol
ógic
o
***E
arly
Chi
ldho
od
Ora
l Hea
lth Im
pact
S
cale
(E
CO
HIS
)
Pah
el e
co
labo
rado
res
Est
ados
U
nido
s 20
07
2-5
anos
S
ub-e
scal
a da
fam
ília
– 4
itens
S
ub-e
scal
a da
cria
nça
– 9
itens
A
valia
r a
qual
idad
e de
vid
a re
laci
onad
a à
saúd
e bu
cal d
e cr
ianç
as p
ré-e
scol
ares
Chi
ld O
ral H
ealth
Im
pact
Pro
file
(CO
HIP
)
Bro
der
e co
labo
rado
res
Est
ados
U
nido
s 20
07
8-14
ano
s 34
iten
s A
valia
r o
impa
cto
físic
o, s
ocia
l e
psic
ológ
ico
da s
aúde
buc
al n
a qu
alid
ade
de v
ida
(aut
o-es
tima
e ex
pect
ativ
as)
66

67
ANEXO B
CPQ 11-14
1. Nome: turma 2. Sexo: ( ) M ( ) F Data de nascimento: ________/________/________ 3. Você diria que a saúde de seus dentes, lábios, maxilares e boca é: ( ) Excelente ( ) Boa ( ) Regular ( ) Ruim 4. Até que ponto a condição dos seus dentes, lábios, maxilares e boca afetam sua vida em geral? ( ) De jeito nenhum ( ) Bem pouco ( ) Muito
PERGUNTAS SOBRE PROBLEMAS ORAIS
Nos últimos 3 meses, com que freqüência você teve?
nunc
a
1 ou
2 v
ezes
algu
mas
ve
zes
freq
uent
emen
te
todo
s os
dia
s ou
qua
se
todo
s
5. Dor nos lábios, boca, ou maxilares
6. Gengivas sangrantes?
7. Feridas na boca
8. Mau hálito?
9. Restos de alimentos presos dentre ou entre os seus dentes?
10. Restos de alimentos no céu da sua boca?
Isso aconteceu por causa de seus dentes, lábios, ma xilares e boca? Nos últimos 3 meses, com que freqüência você:
nunc
a
1 ou
2 v
ezes
algu
mas
ve
zes
freq
uent
emen
te
todo
s os
dia
s ou
qua
se
todo
s
11. Respirou pela boca?
12. Demorou mais que os outros para terminar sua refeição?
13. Teve problemas para dormir?
Nos últimos 3 meses, por causa dos seus dentes, láb ios, boca e maxilares com que freqüência você teve?

68
nunc
a
1 ou
2 v
ezes
algu
mas
ve
zes
freq
uent
emen
te
todo
s os
dia
s ou
qua
se
todo
s
14. Dificuldade para morder ou mastigar alimentos como maçãs, espiga de milho ou carne?
15. Dificuldade de abrir bastante sua boca?
16. Dificuldade para dizer algumas palavras?
17. Dificuldades para comer alimentos que você gostaria de comer?
18. Dificuldade de beber com canudo?
19. Dificuldades para beber ou comer alimentos quentes ou frios?
20. Dificuldade de tocar um instrumento musical como flauta, clarinete, corneta ou trompete?
PERGUNTAS SOBRE SENTIMENTOS E/OU SENSAÇÕES
Você já experimentou esse sentimento por causa de s eus dentes, lábios, maxilares ou boca? Se você se sentiu desta maneira por outro motivo, r esponda “nunca”.
nunc
a
1 ou
2 v
ezes
algu
mas
ve
zes
freq
uent
emen
te
todo
s os
dia
s ou
qua
se
todo
s 21. Ficou irritado (a) ou frustrado (a)?
22. Ficou inseguro consigo mesmo (achou que não era capaz de realizar alguma coisa)?
23. Ficou tímido (a), constrangido (a) ou com vergonha?
Nos últimos 3 meses, por causa dos seus dentes, láb ios, boca ou maxilares, com que freqüência você:
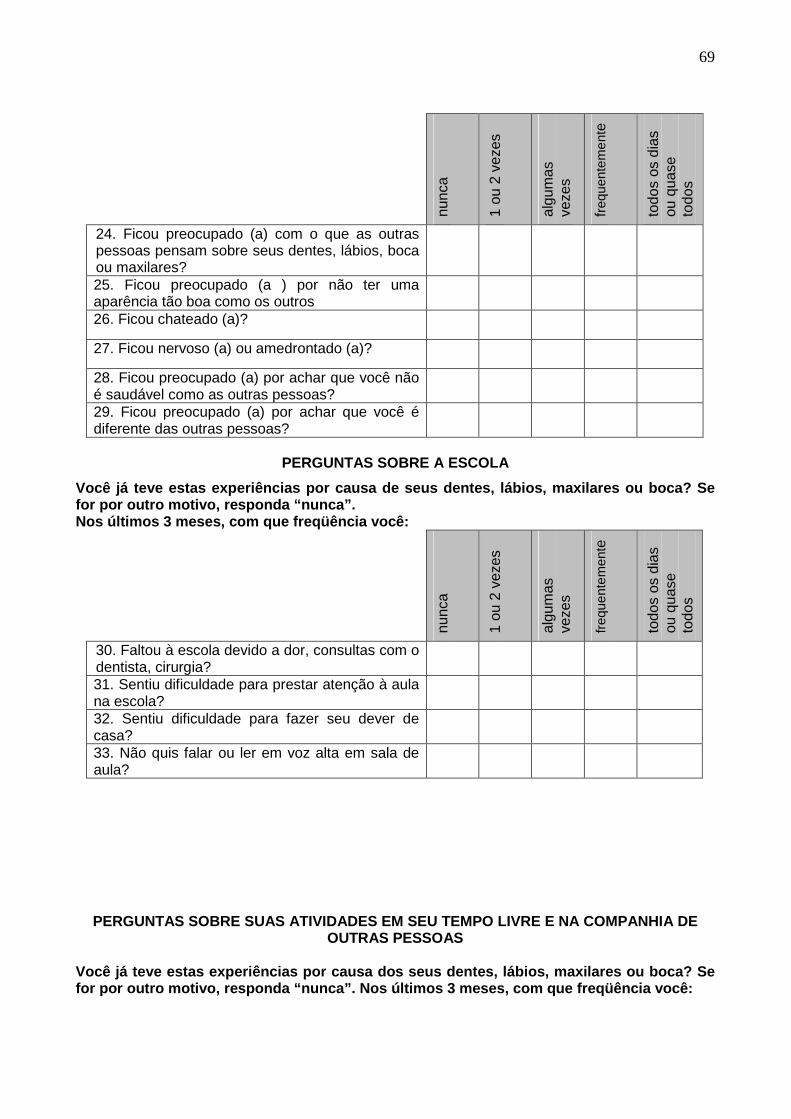
69
nunc
a
1 ou
2 v
ezes
algu
mas
ve
zes
freq
uent
emen
te
todo
s os
dia
s ou
qua
se
todo
s
24. Ficou preocupado (a) com o que as outras pessoas pensam sobre seus dentes, lábios, boca ou maxilares?
25. Ficou preocupado (a ) por não ter uma aparência tão boa como os outros
26. Ficou chateado (a)?
27. Ficou nervoso (a) ou amedrontado (a)?
28. Ficou preocupado (a) por achar que você não é saudável como as outras pessoas?
29. Ficou preocupado (a) por achar que você é diferente das outras pessoas?
PERGUNTAS SOBRE A ESCOLA
Você já teve estas experiências por causa de seus d entes, lábios, maxilares ou boca? Se for por outro motivo, responda “nunca”. Nos últimos 3 meses, com que freqüência você:
nunc
a
1 ou
2 v
ezes
algu
mas
ve
zes
freq
uent
emen
te
todo
s os
dia
s ou
qua
se
todo
s
30. Faltou à escola devido a dor, consultas com o dentista, cirurgia?
31. Sentiu dificuldade para prestar atenção à aula na escola?
32. Sentiu dificuldade para fazer seu dever de casa?
33. Não quis falar ou ler em voz alta em sala de aula?
PERGUNTAS SOBRE SUAS ATIVIDADES EM SEU TEMPO LIVRE E NA COMPANHIA DE OUTRAS PESSOAS
Você já teve estas experiências por causa dos seus dentes, lábios, maxilares ou boca? Se for por outro motivo, responda “nunca”. Nos últimos 3 meses, com que freqüência você:

70
nunc
a
1 ou
2 v
ezes
algu
mas
ve
zes
freq
uent
emen
te
todo
s os
dia
s ou
qua
se
todo
s
34. Evitou participar de atividades como esporte, clubes, teatro, música, passeios escolares?
35. Não quis conversar com outras crianças?
36. Evitou sorrir ou dar risadas quando está com outras crianças?
37. Não quis brincar com outras crianças?
38. Discutiu com outras crianças ou pessoas de sua família?
39. Outras crianças lhe aborreceram ou lhe chamaram por apelidos?
40. Outras crianças deixaram você excluído?
41. outras crianças fizeram perguntas sobre seus dentes,lábios ou maxilares e boca

71
ANEXO C – AUTORIZAÇÃO DO COMITÊ DE ÉTICA EM PESQUIS A (UFSM)

72
ANEXO D - CLASSIFICAÇÃO DE TRAUMATISMO DENTÁRIO UTI LIZADA NO UNITED
KINGDOM CHILDREN’S DENTAL HEALTH SURVEY (1993) – ADAPTADA
Código Descrição
0 Sem traumatismo
1 Fratura de esmalte somente
2 Fratura do esmalte e dentina
3 Quaisquer fratura e sinais ou sintomas de envolvimento pulpar
4 Sem fratura, mas com sinais ou sintomas de envolvimento pulpar
5 Dente perdido devido ao traumatismo
6 Outro dano: outros tipos de traumatismo - especificar
9 Não-avaliado: os sinais do traumatismo não podem ser avaliados à presença de prótese,
bandas, entre outros, que impeçam a observação; ausência de todos os incisivos

73
ANEXO E - CÓDIGOS E CRITÉRIOS PRECONIZADOS PELA ORG ANIZAÇÃO
MUNDIAL DE SAÚDE PARA O DIAGNÓSTICO E REGISTRO DE C ÁRIE DA
COROA DENTÁRIA (WHO, 1997)
Código Critérios
Coroa
0 Hígido
1 Cariado
2 Restaurado e com cárie
3 Restaurado e sem cárie
4 Perdido devido à cárie
5 Perdido por outras razões
6 Apresenta selante
7 Apoio de ponte ou coroa
8 Não erupcionado
T Trauma (fratura)
9 Dente Excluído