Embed Size (px)
Citation preview

Research in Social and
Administrative Pharmacy 9 (2013) 531–541
Original Research
Impact of a health literacy assignment on studentpharmacist learning
Aleda M.H. Chen, Pharm.D., Ph.D.a,1,Marwa Noureldin, Pharm.D., M.S.b, Kimberly S. Plake, Ph.D.b,*
aCedarville University School of Pharmacy, Cedarville, Ohio, USAbPurdue University College of Pharmacy & Center on Aging and the Life Course, West Lafayette, Indiana, USA
Abstract
Background: The average American adult reads at the 8th grade level while most written healthinformation materials, including medication guides, are written at the 12th grade level. To assist studentswith health literacy-sensitive communication, pharmacy schools should incorporate educational activitiesaddressing health literacy competencies.
Objectives: The objectives of this study were to evaluate the impact of a health literacy assignment onstudent pharmacists’ perceptions of: 1) learning about health literacy; 2) ability to write health literacylevel-appropriate patient education material; and 3) the use of these skills in future pharmacy practice.
Methods: Third professional year student pharmacists were asked to rewrite a patient medicationinformation sheet at the 5th grade reading level, altering it from the 12th grade level. Following assignmentcompletion, students responded to a 4-item open-ended questionnaire on what they learned from the
activity, what information components were the most difficult to rewrite and reason for the difficulty, keystrategies to accomplish the assignment, and their perception of the impact this assignment had on theirfuture practice. Content analysis of the reflections was performed using QSR NVivo to identify themes
grounded in the students’ responses.Results: Reflections were completed in 2009 (n ¼ 159) and 2010 (n ¼ 144), for a total of 303 completedreflections. Predominant themes included greater understanding about the challenges, importance, andmethods of health literacy level-appropriate communication and greater awareness of the role of
pharmacists in presenting information clearly to patients.Conclusions: Students indicated the activity increased their understanding of the complexity of patientinformation, the educational needs of patients, and the importance of providing information that is
understandable. Student pharmacists learned methods of effective communication with patients and shouldbe better prepared to communicate in a health literacy-level appropriate manner.� 2013 Elsevier Inc. All rights reserved.
Keywords: Health literacy; Pharmacy students; Assessment
* Corresponding author. Purdue University, 575 Stadium Mall Dr., West Lafayette, IN 47907, USA. Tel.: þ1 765
494 5966; fax: þ1 765 494 0801.1 Portions of this project were completed while Aleda Chen was a graduate research assistant at Purdue University
College of Pharmacy, West Lafayette, Indiana.
E-mail address: [email protected] (K.S. Plake).
1551-7411/$ - see front matter � 2013 Elsevier Inc. All rights reserved.
http://dx.doi.org/10.1016/j.sapharm.2013.05.002

532 Chen et al. / Research in Social and Administrative Pharmacy 9 (2013) 531–541
Introduction
Health literacy is defined as “the degree towhichindividuals have the capacity to obtain, process,
and understand basic health information andservices needed to make appropriate health de-cisions.”1 According to the Agency for HealthcareResearch and Quality (AHRQ) National Health-
care Disparities Report, only 12% of adults havean adequate level of health literacy to manage theirhealthcare2 and health literacy has been identified
by Healthy People 2020 and the Institute of Medi-cine as a public health problem.3,4 The averageAmerican adult reads at the 8th grade level while
most written health information materials, includ-ingmedication guides, are written at the 12th gradelevel.5–7 This disparity is further magnified whenconsidering that approximately 25% of American
adults read at or below the 5th grade level.3,5 Adultswith low health literacy are more likely to misinter-pret prescription and over-the-counter label in-
structions, nutrition information on food labels,and discharge instructions.5,8–10 For example, onestudy reported that 42% of patients from a public
hospital were unable to interpret directions for tak-ing a medication on an empty stomach and 33%were unable to answer questions on how often
a medication should be taken during the day.11 Inaddition, low health literacy has been associatedwith adverse health outcomes includingmedicationnon-adherence, increased hospitalization, and
mortality.10–13
Adults with low health literacy often rely onverbal instruction from their healthcare pro-
viders.14 Although studies examining pharmacistability to provide health literacy level-appropriateinformation is limited, it has been reported that
physicians often do not communicate at an appro-priate level for these patients15 and many health-care practitioners overestimate the literacy levelsof patients.16–18 The U.S. Department of Health
and Human Services has developed a national ac-tion plan to address issues related to low patienthealth literacy and outlined seven goals. Strategies
for meeting these goals include encouraging healthprofessionals to participate in health literacy train-ing to improve clear communication, as well as in-
clude coursework on health literacy in all healthprofessions curricula.19 In addition, a variety ofgovernmental organizations, such as the Centers
Disease Control and Prevention (CDC)20 andAHRQ,21 have developed tools for practitionersand providers to use when working with patientsand improving their practice sites.
In response to this relative lack of healthliteracy-sensitive communication, several nationaland professional organizations such as the In-
stitute of Medicine (IOM),3 the American MedicalAssociation (AMA),22 and the American Pharma-cists Association (APhA),23 also have called forincorporation of health literacy education and
competencies in health professional curricula. Intheir 2011 Adopted Policy Statements, APhAhas encouraged “pharmacists and student phar-
macists to increase their awareness of healthliteracy..to assess patients’ health literacy andthen implement appropriate communications
and education and ..review of all patient infor-mation for health literacy appropriateness.”23
In addition, the Accreditation Council for Phar-macy Education (ACPE)Guideline 9.1 states, “The
college or school must ensure that the curriculumaddresses patient safety, cultural appreciation,health literacy, healthcare disparities, and compe-
tencies needed to work as a member of or on aninterprofessional team.”24 Published studies reportusing several strategies to incorporate health liter-
acy education in pharmacy curricula such as didac-tic lectures in required courses,25 implementation ofrequired26 or elective27,28 health literacy courses,
incorporation of health literacy concepts duringadvanced pharmacy practice experiences,29 orutilization of active learning exercises.25,26,29,30
Despite these recommendations, studies evaluating
the impact of health literacy education on studentpharmacists learning are limited.25,26
In addressing ACPE requirements, a health
literacy module was incorporated into the corecurriculum in the third professional year in a largeclassroom setting. Didactic lectures, as well as
active learning exercises, were utilized in deliveringthe content. In addition, students designedapatientmedication information sheet to apply skillslearned in the classroom. The objectives of this
studywere to evaluate the impact of a health literacycourse module and assignment on student pharma-cists’ perceptions of: 1) learning about health
literacy; 2) ability to write health literacy level-appropriate patient education material; and 3) theuse of these skills in future pharmacy practice.
Methods
Description of the health literacy course content
and assignment
Third professional year student pharmacistsattended a 3-h health literacy module as part of

533Chen et al. / Research in Social and Administrative Pharmacy 9 (2013) 531–541
a required pharmacy administration course. Themodule consisted of a formal class presentation,in-class activities, and health literacy videos.Learning objectives for student pharmacists in-
cluded being able to: 1) define health literacy; 2)compare and contrast literacy, health literacy, andfunctional literacy; 3) explain the importance of
health literacy with respect to patient healthoutcomes; 4) describe how to identify problemswith literacy or health literacy in patients; 5)
explain how literacy and health literacy is mea-sured; 6) identify patients with low health literacybased on measurement instruments; 7) evaluate
difficulty of written material; 8) describe strategiesto identify individuals who may need assistancedue to health literacy issues; 9) describe strategiesthat can be used to help people in understanding
health material; and 10) design an intervention toaddress issues with health literacy (Table 1).Learning objectives were developed to address
ACPE requirements, but also were based on theliterature, and feedback from clinical faculty,regarding communication skills necessary in
delivering patient care. Content included in themodule was selected to directly address each ofthe learning objectives and were derived from,
but not limited to, examples of health literacytraining in the literature, as well as AHRQ,AMA, and the Pfizer Clear Communication Ini-tiative (Table 1).3,11,18,25,26,31–38
Each of the learning objectives were addressedin the class presentation and supplemented within-class active learning exercises. Students learned
about methods to evaluate the reading level ofpatient information sheets and other writtenmaterials including the Fry readability formula39
and the Flesch-Kincaid readability tool40 pro-vided in Microsoft Word�. In-class group activi-ties involved brainstorming ways to simplifymedical jargon and using the Fry Readability for-
mula to assess the readability (by hand) of a para-graph taken from a medication information sheet.In addition, students were introduced to the Suit-
ability Assessment of Materials,32 a checklist toevaluate written material in the areas of content,literacy demand, graphics, layout and typogra-
phy, learning, stimulation and motivation, andcultural appropriateness.32 Students completedan in-class activity using this tool to evaluate pa-
tient education information regarding diet forSpanish-speaking patients. These tools were spe-cifically selected as they are accessible and citedfrequently in the literature. In addition, the
Flesch-Kincaid readability tool is available on
Microsoft Word�, of which most practitionersand students would have access at their practicesettings or home computers.
Similar to AHRQ’s Activity 5 in Advancing
Pharmacy Health Literacy Practices ThroughQuality Improvement Curricular Modules forFaculty,37 students then were asked to apply
knowledge learned about communicating ina health literacy level-sensitive manner by com-pleting an individual assignment that involved
rewriting and modifying an Ortho Evra� patientmedication information sheet to meet a fifth-grade reading level. This assignment specifically
addressed learning objectives 7–10. The originalpatient information sheet contained nine headingsincluding “ingredient name,” “drug manufac-turer,” “common uses,” “before using this medi-
cine/warnings,” “how to use this medicine,”“cautions,” “possible side effects,” “overdose,”and “additional information.” Based on the
Flesch-Kincaid readability tool provided in Mi-crosoft Word�, the original patient informationsheet had a twelfth grade reading level. Students
were instructed to use Microsoft Word� and theSuitability of Assessment Materials checklist indesigning their patient information sheet. The
purpose of the assignment was to incorporate anactive learning exercise into the pharmacy curric-ulum to address health literacy competencies andreinforce and apply concepts learned during the
didactic component.
Student assessment
Student assessment of the learning objectivesincluded completing an examination (Objectives1–6) and designing the patient medication in-
formation sheet (Objectives 7–10). Student sub-missions of the patient information sheets wereevaluated by a graduate level teaching assistant
with a grading rubric. Students also completeda qualitative 4-item questionnaire on the experi-ence, including what they learned from the activ-ity, what components were the most difficult to
rewrite and reason for difficulty, key strategies toaccomplish the assignment without compromisingaccuracy, and their perception of the impact this
assignment had on their future practice (seeTable 2). The results of this questionnaire arethe focus of this manuscript. The Institutional Re-
view Board (IRB) at Purdue University approvedthe analysis of the 4-item questionnaire as part ofthe course evaluation for research purposes.
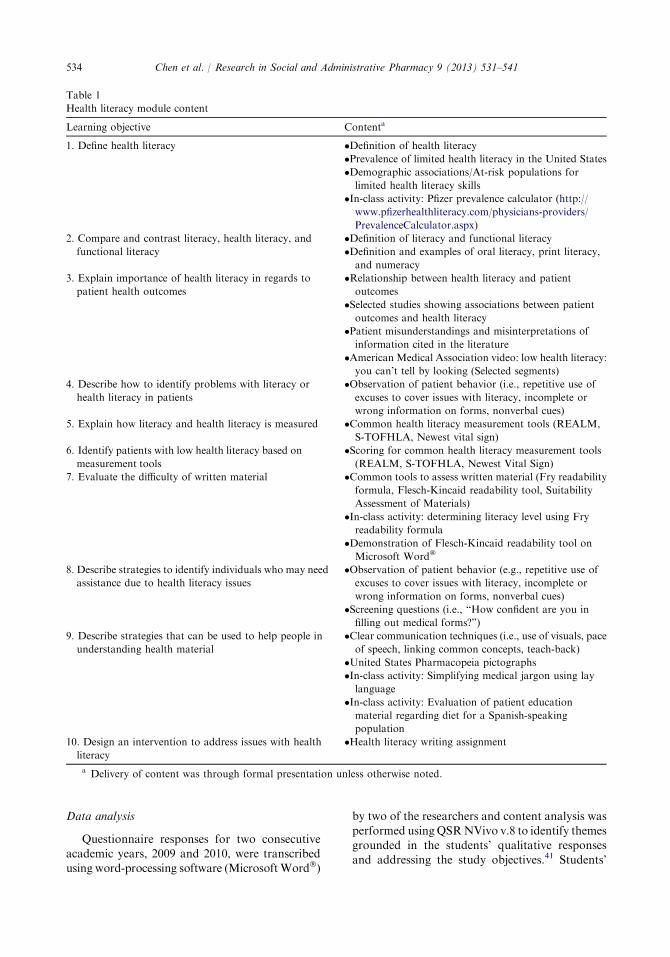
Table 1
Health literacy module content
Learning objective Contenta
1. Define health literacy �Definition of health literacy
�Prevalence of limited health literacy in the United States
�Demographic associations/At-risk populations for
limited health literacy skills
�In-class activity: Pfizer prevalence calculator (http://
www.pfizerhealthliteracy.com/physicians-providers/
PrevalenceCalculator.aspx)
2. Compare and contrast literacy, health literacy, and
functional literacy
�Definition of literacy and functional literacy
�Definition and examples of oral literacy, print literacy,
and numeracy
3. Explain importance of health literacy in regards to
patient health outcomes
�Relationship between health literacy and patient
outcomes
�Selected studies showing associations between patient
outcomes and health literacy
�Patient misunderstandings and misinterpretations of
information cited in the literature
�American Medical Association video: low health literacy:
you can’t tell by looking (Selected segments)
4. Describe how to identify problems with literacy or
health literacy in patients
�Observation of patient behavior (i.e., repetitive use of
excuses to cover issues with literacy, incomplete or
wrong information on forms, nonverbal cues)
5. Explain how literacy and health literacy is measured �Common health literacy measurement tools (REALM,
S-TOFHLA, Newest vital sign)
6. Identify patients with low health literacy based on
measurement tools
�Scoring for common health literacy measurement tools
(REALM, S-TOFHLA, Newest Vital Sign)
7. Evaluate the difficulty of written material �Common tools to assess written material (Fry readability
formula, Flesch-Kincaid readability tool, Suitability
Assessment of Materials)
�In-class activity: determining literacy level using Fry
readability formula
�Demonstration of Flesch-Kincaid readability tool on
Microsoft Word�
8. Describe strategies to identify individuals who may need
assistance due to health literacy issues
�Observation of patient behavior (e.g., repetitive use of
excuses to cover issues with literacy, incomplete or
wrong information on forms, nonverbal cues)
�Screening questions (i.e., “How confident are you in
filling out medical forms?”)
9. Describe strategies that can be used to help people in
understanding health material
�Clear communication techniques (i.e., use of visuals, pace
of speech, linking common concepts, teach-back)
�United States Pharmacopeia pictographs
�In-class activity: Simplifying medical jargon using lay
language
�In-class activity: Evaluation of patient education
material regarding diet for a Spanish-speaking
population
10. Design an intervention to address issues with health
literacy
�Health literacy writing assignment
a Delivery of content was through formal presentation unless otherwise noted.
534 Chen et al. / Research in Social and Administrative Pharmacy 9 (2013) 531–541
Data analysis
Questionnaire responses for two consecutiveacademic years, 2009 and 2010, were transcribedusing word-processing software (MicrosoftWord�)
by two of the researchers and content analysis wasperformed usingQSRNVivo v.8 to identify themesgrounded in the students’ qualitative responsesand addressing the study objectives.41 Students’

Table 2
Mapping of study objectives and reflection questions
Study objective Reflection question
To evaluate the impact of a health literacy course module on student pharmacists’ perceptions of:
1. Learning about health literacy 1. What did you learn from this activity?
2. What specific section of the information did you have most
trouble simplifying? Why?
2. Ability to write health literacy level-appropriate
patient education material
3. What were the key aspects of reducing the grade level from 12th
grade to the 5th grade? How did you accomplish this task?
3. The use of these skills in future practice 4. After comparing the information given to you and the one you
simplified, reflect on how this exercise will impact how you
practice in a community setting?
535Chen et al. / Research in Social and Administrative Pharmacy 9 (2013) 531–541
questionnaires were compared to determine thecommonalities among the students’ responses. Tworesearchers independently identified themes pres-
ent in responses and discussed themes until aconsensuswas reached on the predominant themes.For purposes of this project, a theme was consid-
ered predominant if 20% or more of students hadcomments related to the theme.
Results
All students (N ¼ 303) in their third profes-sional year of the pharmacy curriculum completedthe health literacy assignment in the fall of 2009
(N ¼ 159) and 2010 (N ¼ 144) and submitteda 4-item qualitative questionnaire to reflect onthe experience. Several predominant themes were
identified (Table 3) based on the student responsesto the guided reflection questions.
Theme 1: Students learned a great deal aboutthe challenges, importance, and methods of
communicating in a health literacylevel-appropriate manner with patients
Prompted by the question regarding what theylearned from this activity, students from bothyears indicated that it was challenging to simplify
health information (61.3%, N ¼ 186), often citingthat healthcare professionals and students takemedical terminology and knowledge for granted
(37.3%, N ¼ 113). A student in 2009 stated, “Ithink the largest issue I had to overcome when com-pleting this assignment was coming up with creative
ways to talk about the medical jargon that has be-come so commonplace in my vocabulary.” Anotherstudent in 2010 agreed: “First of all, I realized that
I have learned a lot of medical information and ter-minology since I started pharmacy school. After us-ing medical terminology on a regular basis, it is
sometimes hard to put the information in otherwords that are easier to understand.” After yearsof being encouraged to write with more complex-
ity, students found it hard to simplify and write inshort, concise sentences with simpler words andphrases.
Despite these challenges, students felt thatpatient information was written at too high ofa health literacy level (27.7%, N ¼ 84) and needed
to be simplified (30.4%, N ¼ 92). One student in2010 explained: “After completing this activity, Irealized how difficult it could be for some patients
to decipher and understand the leaflets that are con-tained in their prescription bags. The informationprovided in the example pamphlet would be verydifficult for a patient with a low literacy level.”
They often discussed how there was a great dealof medical terminology in the leaflet that wouldbe hard for a patient without healthcare training
to understand. Additionally, students mentionedthat the leaflets used long sentences with a greatdeal of information, which made reading the doc-
ument difficult.After completing this exercise, students be-
lieved that they better understood patients’ needsand perspectives regarding health information
(33.3%, N ¼ 101). There was a better understand-ing of how a patient may perceive health informa-tion and how the pharmacist can play a role in
meeting the needs of the patient. In 2009, onestudent stated: “I have a deeper compassion andunderstanding for patients who have difficulty fol-
lowing directions and understanding informationgiven to them about their medications. I alwaysthought patient leaflets were great resources, but
they can be overwhelming to patients and full of su-perfluous information. I learned that the pharmacistis essential in picking out what information is im-portant and communicating that information to
the patient.”

Table 3
Summary of predominant themes from student reflections (N ¼ 303)a
Theme Nb Percentagec (%)
Theme 1: Students learned from this activity:
1) How challenging it is to simplify health information. 186 61.3
2) Medical professionals often take their level of knowledge for granted. 113 37.3
3) Patient needs and perspective regarding health information. 101 33.3
4) The importance of simplifying patient information. 92 30.4
5) Patient information is written at too high of a health literacy level. 84 27.7
6) Methods of appropriate patient communication. 83 27.4
Theme 2: Students found it challenging to simplify:
1) Warnings and contraindications. 137 45.2
2) Side effects. 129 42.6
3) Directions for using the medication. 70 23.1
Theme 3: Students found it challenging to simplify the medication information sheet because:
1) Medical terminology and other complex words were difficult to replace. 210 69.3
2) Much of the information was important but quite complex. 68 22.4
Theme 4: Students were able to lower the health literacy level of medication information by:
1) Simplifying complex words and medical terminology. 234 77.2
2) Reducing the length of sentences and the information. 230 75.9
3) Using bullets points and lists. 169 55.8
4) Using pictures or graphs to assist in explaining information. 109 36.0
Theme 5: Students felt that this exercise had:
1) Improved their understanding of how to present information to patients. 176 58.1
2) Improved their understanding of patients’ experience in the healthcare system and needs. 115 38.0
3) Improved their ability to simplify medical terminology. 89 29.4
4) Taught them to be aware of health literacy. 77 25.4
5) Reinforced assessing patient understanding of health information. 71 23.8
6) Relayed the importance of communicating and counseling patients effectively. 62 23.4
7) Relayed the importance of emphasizing key information to patients. 66 21.8
a For a theme to be considered predominant, a minimum threshold of R20% of the students needed to comment on
the aspect.b N refers to the total number of students who expressed the theme out of 303 reflections assessed.c Percentage refers to the percent of students who expressed the theme out of 303 reflections assessed.
536 Chen et al. / Research in Social and Administrative Pharmacy 9 (2013) 531–541
Many students felt that they gained skills in
health literacy-level appropriate communication(27.4%, N ¼ 83). While methods of healthliteracy-level sensitive communication are often
mentioned in the classroom, the intent of this ac-tivity was to reinforce techniques, such as avoid-ing medical terminology, using simpler phrasingand sentences, and replacing text with pictures
and diagrams, to lower the health literacy levelof written communication. In their reflections,students commented specifically on the use of
these techniques in completing the assignment. Astudent in 2010 reflected: “After completing thisassignment, I gained insight as to how much health-
care providers should change the language that weuse when communicating with patients.. In orderto communicate effectively with patients who have
difficulty reading, we must condense words withmultiple syllables and use pictures to elaborate onpoints of importance.”
Themes 2 and 3: Students found it challenging to
simplify the warnings and side effects sections of theleaflet because they contained the most medicalterminology and complex directions
Sections of the leaflet that listed the warnings/
contraindications (before using this medicine/warnings) and the side effects (possible sideeffects) contained a great deal of medical termi-nology, and students found these two sections
particularly challenging (warnings/contraindica-tions: 45.2%, N ¼ 137; side effects: 42.6%, N ¼129). Medical terminology and other complex
words were difficult to replace (69.3%, N ¼210), as many students found that they were fa-miliar with these terms and had to define the
term rather than replace it with a single word.In 2009, one student noted: “The section that de-scribed if you have any of these conditions (i.e.,
blood circulation problems, history of heart disease

537Chen et al. / Research in Social and Administrative Pharmacy 9 (2013) 531–541
and stroke, diabetes, etc.) gave me the most trou-ble. Simplifying this section was hard because thereare no words to substitute for commonly acceptedmedical conditions like stroke or diabetes.” The
section of the leaflet which contained directionsfor use also was complicated to simplify (23.1%,N ¼ 70) because the directions for Ortho Evra�
were quite complex. Students themselves wereconfused by the directions and had difficulty figur-ing out how to explain the directions simply to
a patient, as one student related (2010): “Themost difficult section to simplify for me was the sec-tion telling the patient how to use the patch. I felt
that it was already somewhat confusing to beginwith, but to put it in concise terms that a patientcould easily follow was difficult.” Other reasonswhy the pamphlet was difficult to simplify (but
did not reach the minimum criteria for predomi-nance) included too much information provided(18.8%, N ¼ 57) and difficulty determining what
information was important (15.8%, N ¼ 48).
Theme 4: Students utilized various strategies to
lower the health literacy level of patient information
As part of the didactic component, methods oflowering the health literacy of patient informationwere outlined. Students incorporated these sug-
gestions and found that simplifying medical ter-minology and complex words (77.2%, N ¼ 234)and shortening sentence length (75.9%, N ¼230) were 2 key strategies to reduce the health lit-
eracy level of the pamphlet. A student in 2009stated: “The key aspects of reducing the gradelevel were shortening the sentences and using
smaller words. I broke up a lot of the longer sen-tences containing side effects to watch for or rea-son not to use the drug into lists to make it
easier on the eye and less intimidating for the pa-tient to read. I used shorter words that meant thesame thing as some of the larger words when I
could. When I came across a medical term thatwould be difficult for the patient to understand, Iexplained what it was in everyday terms in placeof the actual term.”
By further incorporating the use of bulletpoints or lists rather than using complete senten-ces (55.8%, N ¼ 169) and using pictures or graphs
to explain complex concepts (36%, N ¼ 109), suchas the directions for use, they could achieve a fifthgrade literacy level or lower. One student (2010)
explained how he found “using bullet points toorganize the document was an effective strategy toreduce the reading level. This helps present the
information in a more simplistic way that does notinitially discourage the patient from reading it.”Furthermore, another student in 2010 wrote thatusing pictures “especially for the regions where
the patch can be applied I believe are good waysto better explain the locations to the patient thanusing words. The pictures allowed the patient to
see visually where each patch can be applied insteadof the current patient information sheet, which hasthe instructions listed in paragraph format. The im-
age of the patient peeling off the patch also helps toexplain the application process better than wordscould.”
Theme 5: After completing this exercise, studentswere more aware of the problem of health literacyand their role in presenting information in a health
literacy level-sensitive manner
Prompted by the question asking students toreflect on how this exercise will impact theirpractice in the community setting, students in-
dicated that they believed this assignment hadimproved their understanding of how to appro-priately present information to patients (58.1%,
N ¼ 176), and they were much more aware ofhealth literacy (25.4%, N ¼ 77). For example, stu-dents stated (2009 and 2010, respectively): “This
exercise will impact how I practice in a communitysetting because I have learnt how to write and pres-ent patient information in such a manner that it canbe read and understood by everyone” and “In a com-
munity setting, I will be much more aware of healthliteracy issues.”
Students also felt they had gained a better
understanding of patients’ experiences in thehealthcare system with regard to health literacyand their needs from healthcare providers. Stu-
dents mentioned (2009): “This exercise will impacthow I practice in a community setting by openingmy eyes to the challenges faced by patients with
low health literacy (which is a considerable propor-tion of all patients)” and “This exercise opened upmy eyes to the difficulties that patients face with un-
derstanding patient information because I had as-
sumed that everyone knew what I was saying. Imust also be VERY understanding and patient..I must make sure that all my patients know the
most important information about the drugs thatthey might have been afraid to ask their doctorabout or did not understand the first time around.”
Emphasizing key information to patients(21.8%, N ¼ 66) was mentioned frequently as animportant component of patient communication.

538 Chen et al. / Research in Social and Administrative Pharmacy 9 (2013) 531–541
Students also mentioned they were more likely toutilize simpler terminology as a result of this as-signment, stating (2009): “I have already imple-
mented this exercise while working. This pastweekend when I was counseling patients, I recog-nized that I needed to use terms that were as simpleas possible..and to provide the most important in-
formation” and “This exercise has been an eye-opening assignment..This assignment put me ina patient’s shoes. When I practice in a community
setting, I will try my best to translate medical jar-gon to the customers/patients.”
This assignment also reinforced the importance
of patient counseling (23.4%, N ¼ 62) in the com-munity setting and of assessing patient under-standing (e.g., using “teach back” method) (23.8%,N ¼ 71). As one student stated (2010): “Our job as
healthcare professionals is to educate, counsel, andpromote the overall health of our community, andthe main way we do all three of these things is
through developing outstanding communicationskills. This has given me a new understanding ofmy purpose in this profession..” Another student
relayed the importance of making counseling ef-fective (2010), “By making use of the teach-backmethod, it will help me evaluate how well I relayed
the information to the patient.”
Discussion
Bridging the health literacy gap between pa-
tients and the healthcare system creates a challengein the education of future healthcare professionals.Healthcare providers are expected to communicate
in a manner that all patients can understand.However, some healthcare providers may havedifficulties communicating with patients with low
health literacy, as they routinely use medicalterminology. Therefore, a need exists to improvestudent understanding of patient literacy and the
readability level of healthcare information. Fur-thermore, the current ACPE standards for phar-macy education deem health literacy level-sensitivecommunication an important aspect to address
within curricular efforts.24 Activities and experien-tial learning should be incorporated in the phar-macy curriculum to address this challenge.
Based on the results of the analysis, incorpo-ration of the health literacy assignment devel-oped and enhanced students’ understanding of
health literacy and its place in pharmacy practice.Prior studies have focused on quantitative ap-proaches to self-assessment, whereas this study
focused on students’ reflections and written self-assessments of learning that resulted from thisactivity. This approach allows students to in-
dicate specific areas of perceived growth beyondwhat is typically seen in quantitative question-naires. Results are similar to previous researchdescribing or examining the impact of health
literacy activities. In these prior studies, studentsalso indicated enhancement of their knowledgeor understanding of health literacy,25,26,42–45 and
the development of their perceived ability tocommunicate in a more health literacy level-sensitive manner.25,28,42,43,45 Furthermore, stu-
dents in this study were similar to other studentpharmacists who had underestimated the prob-lem of health literacy25 and found it challengingto lower the literacy level of health informa-
tion.30 Creating additional opportunities for stu-dents to practice their skills may increase theirproficiency in delivering health information and
lessen the challenges students expressed.Healthcare students and professionals who
work in the community setting tend to over-
estimate the health literacy of their patients,16–18
as did the student pharmacists who completedthis activity. Even though didactic portions of
the curriculum introduced students to the problemof health literacy, activities such as this assign-ment appeared to reinforce concepts learned andenhance student evaluation of their own ability
to communicate clearly. In 2009, one studentwrote: “This activity made me really contemplatehow I present information to a patient. Being so
heavily submersed in a highly educated environmentmakes it easy to develop high expectations ofothers’ education level and forget what is actually
the “norm.” When reading the original patient in-formation handout, I could see why lay peoplemight get discouraged and not bother with it.. Ilearned the importance of really approaching edu-
cation from the patient’s standpoint.” Incorporat-ing active learning exercises, such as this activity,throughout the curriculum may aid in student
learning about the experiences of adults with lim-ited health literacy and dispel any preconceivedideas about health literacy.
The activity was incorporated into the thirdprofessional year pharmacy administration courseto advance student understanding of health liter-
acy and ability to communicate with patients ofany health literacy level. Most students indicatedprogress in meeting the learning objectives, spe-cifically commenting on the development of their
skills in using health literacy techniques. In

539Chen et al. / Research in Social and Administrative Pharmacy 9 (2013) 531–541
addition, students expressed a willingness to altertheir future practices in favor of health literacylevel-sensitive communication practices, such asavoiding the use of medical terminology, assessing
patient understanding, and counseling patients onimportant information. These practices are im-portant, as adults with low health literacy typi-
cally utilize verbal instruction from healthcareproviders to gain information.14
However, health literacy level-appropriate
communication practices should be reinforcedand assessed throughout the curriculum to givestudents the opportunity to practice their com-
munication skills, both in oral and written for-mats. Students were introduced to the problemof health literacy within this course and givenan opportunity to gain skills in appropriate
written communication practices. Future researchshould incorporate and assess health literacylevel-sensitive communication in each patient
counseling activity, thereby improving patient-provider communication. In the future, healthliteracy content will be introduced during the first
professional year with plans to reinforce andassess skills throughout the didactic curriculumusing the pharmacy practice laboratories. In
addition, plans include expanding this activityand providing opportunities for students to prac-tice their skills in communicating about diseasestates in addition to medications.
Limitations
The depth and breadth of student responsesmay have been limited, since guided reflections
were utilized. Students may have learned aboutother aspects of health literacy and appropriatepatient communication, which were unrelated to
the questions asked. The questions were generatedto measure the learning outcomes for the activity,but the use of open-ended or free-form reflections
may have revealed other items that studentslearned. Students also may have felt the need torespond favorably to the questions, introducingsocial desirability bias. Attempts were made to
minimize social desirability bias by limiting theassignment grade to the assessment of the patientinformation sheet and not the reflection responses.
The generalizability of the findings is limited as themodule and assignment took place at one in-stitution. However, this educational approach to
teaching and assessing health literacy skills couldbe easily incorporated into other schools of phar-macy, as the health literacy content was presented
in relatively few hours. The major limitation to itsincorporation at other institutions is the timerequired for grading the patient medication in-formation sheets.
It is unknown whether students’ understandingof health literacy and willingness to communicatein a health literacy level-sensitive manner persisted
over time. Students felt that their understandingand willingness improved, but the goal of incorpo-rating these types of activities into the curriculum is
to impact student knowledge of a particular issue(in this case, health literacy) and have this knowl-edge reinforced by practice experiences (activities/
assignments, IPPEs/APPEs) throughout the cur-riculum. There is potential for this activity to havelasting impact, but future research should examinewhether there is a long-term effect of this assign-
ment and other experiences on student understand-ing and willingness to communicate in a healthliteracy level-sensitive manner.
Conclusion
A health literacy active learning assignment wasincorporated into the professional pharmacy cur-riculum to address the ACPE standards regarding
health literacy competencies. After completing theassignment, student pharmacists reflected on whatthey had learned, the challenges to and solutions forlowering the health literacy of medical information,
and changes they plan on making in their futurepractice. Through their questionnaire responses,students felt they achieved the learning outcomes
for the assignment. Students indicated they gainedan understanding of the literacy level of patientinformation, the patient experience with health
information, and strategies to lower the literacylevel of patient information. Furthermore, studentsplanned to incorporate health literacy level-sensitive
communication in their practice, based on thisexperience.
Acknowledgments
Support for Aleda Chen while a graduatestudent was provided by the National Institute
on Aging (T32AG025671) and the Purdue Uni-versity Center on Aging and the Life Course aswell as from the American Foundation for Phar-
maceutical Excellence. Thank you to BrittanyMelton, Pharm.D., for reviewing this manuscriptand to Stephanie Cailor, pre-pharmacy student at

540 Chen et al. / Research in Social and Administrative Pharmacy 9 (2013) 531–541
Cedarville University, for her assistance in review-ing and preparing this manuscript.
References
1. U.S. Department of Health and Human Services.
Healthy People 2010. 2nd ed. Washington D.C.:
U.S. Government Printing Office; 2000.
2. Kutner M, Greenberg E, Jin Y, Paulsen C. The
Health Literacy of America’s Adults: Results From
the 2003 National Assessment of Adult Literacy
(NCES 2006–483). U.S.Department of Education.
Washington, DC: National Center for Education
Statistics; 2006.
3. Institute ofMedicine.Health Literacy: A Prescription
to End Confusion. National Academy of Sciences;
2004.
4. U.S. Department of Health and Human Services.
Healthy People 2020: Health Communication and
Health Information Technology Objectives, 2010.
Available at: http://www.healthypeople.gov/2020/
topicsobjectives2020/objectiveslist.aspx?topicid¼18.
Accessed 11.06.12.
5. Ngoh LN. Health literacy: a barrier to pharmacist-
patient communication and medication adherence.
J Am Pharm Assoc 2009;49:e132–e149.
6. Wolf MS, Davis TC, Shrank WH, Neuberger M,
Parker RM. A critical review of FDA-approved
medication guides. Patient Educ Couns 2006;62(3):
316–322.
7. Davis TC, Crouch MA, Wills G, Miller S,
Abdehou DM. The gap between patient reading
comprehension and the readability of patient educa-
tion materials. J Fam Pract 1990;31:533–538.
8. Wolf MS, Davis TC, Tilson HH, Bass PF III,
Parker RM. Misunderstanding of prescription drug
warning labels among patients with low literacy.
Am J Health Syst Pharm 2006;63:1048–1055.
9. Rothman RL, HousamR,Weiss H, et al. Patient un-
derstanding of food labels: the role of literacy and
numeracy. Am J Prev Med 2006;31:391–398.
10. Williams MV, Parker RM, Baker DW, et al. Inade-
quate functional health literacy among patients at
two public hospitals. JAMA 1995;274:1677–1682.
11. Youmans SL, Schillinger D. Functional health liter-
acy and medication use: the pharmacist’s role. Ann
Pharmacother 2003;37:1726–1729.
12. Berkman ND, Sheridan SL, Donahue KE, et al.
Health Literacy Interventions and Outcomes: An
Updated Systematic Review. Evidence Report/Tech-
nology Assesment No. 199. Prepared by RTI Interna-
tional–University of North Carolina Evidence-based
Practice Center under contract No. 290-2007-10056-
I. AHRQ Publication Number 11-E006. Rockville,
MD: Agency for Healthcare Research and Quality;
March 2011.
13. Baker DW, Wolf MS, Feinglass J, Thompson JA,
Gazmararian JA, Huang J. Health literacy and
mortality among elderly persons. Arch Intern Med
2007;167:1503–1509.
14. Schwartzberg JG, Cowett A, VanGeest J, Wolf MS.
Communication techniques for patients with low
health literacy: a survey of physicians, nurses, and
pharmacists. Am J Health Behav 2007;31(Suppl 1):
S96–S104.
15. Wolf MS, Gazmararian JA, Baker DW. Health liter-
acy and functional health status among older adults.
Arch Intern Med 2005;165:1946–1952.
16. Kelly PA, Haidet P. Physician overestimation of
patient literacy: a potential source of health care dis-
parities. Patient Educ Couns 2007;66:119–122.
17. Safeer RS, Keenan J. Health literacy: the gap be-
tween physicians and patients. Am Fam Physician
2005;72:463–468.
18. Kripalani S, Weiss BD. Teaching about health liter-
acy and clear communication. J Gen Intern Med
2006;21:888–890.
19. US Dept of Health and Human Services, Office of
Disease Prevention and Health Promotion. National
Action Plan to Improve Health Literacy; 2010. Wash-
ington, DC.
20. Center for Disease Control. Health Literacy: Accu-
rate, Accessible, and Actionable Health Information
for All, 2011. Available at: http://www.cdc.gov/
healthliteracy/index.html. Accessed 26.06.12.
21. Agency for Healthcare Research and Quality.Health
Literacy and Cultural Competency, 2011. Available
at: http://www.ahrq.gov/browse/hlitix.htm. Accessed
26.06.12.
22. AdHoc Committee onHealth Literacy for the Coun-
cil on Scientific Affairs for the AmericanMedical As-
sociation. Health literacy report of the Council on
Scientific Affairs. JAMA 1999;281:552–557.
23. American Pharmacists Association. Current Adopted
APhA Policy Statements 1963–2011. Washington,
D.C: American Pharmacists Association; 2011.
24. Accreditation Council for Pharmacy Education. Ac-
creditation Standards and Guidelines for the Profes-
sional Program in Pharmacy Leading to the Doctor
of Pharmacy Degree. Guidelines Version 2.0, 2011.
Available at: http://www.acpe-accredit.org/pdf/
S2007Guidelines2.0_ChangesIdentifiedInRed.pdf.
Accessed 01.06.12.
25. Sicat BL, Hill LH. Enhancing student knowledge
about the prevalence and consequences of low health
literacy. Am J Pharm Educ 2005;69(4):Article 62.
26. Devraj R, Butler LM, Gupchup GV, Poirier TI. Ac-
tive-learning strategies to develop health literacy
knowledge and skills. Am J Pharm Educ 2010;74(8):
Article 137.
27. Lahoz MR. Connecting the dots in a health literacy
course [abstract]. Am J Pharm Educ 2007;71(3):Arti-
cle 60.
28. Capehart KD. Development and implementation
of a health literacy elective in a pharmacy curricu-
lum [abstract]. Am J Pharm Educ 2008;72(3):Article
72.

541Chen et al. / Research in Social and Administrative Pharmacy 9 (2013) 531–541
29. Patterson BY. An advanced pharmacy practice expe-
rience in public health. Am J Pharm Educ 2008;72(5):
Article 125.
30. Bastianelli K, Conway J. Pharmaceutical care
lab activity promotes literacy awareness in phar-
macy students. Am J Pharm Educ 2008;72(3):Ar-
ticle 72.
31. Andrus MR, Roth MT. Health literacy: a review.
Pharmacotherapy 2002;22(3):282–302.
32. Doak CC, Doak LG, Root JH. Teaching Patients
with Low Literacy Skills. 2nd ed. Philadelphia, Pa:
JB Lippincott Company; 1996.
33. Kirksey O, Harper K, Thompson S, Pringle M. As-
sessment of selected patient educational materials
of various chain pharmacies. J Health Commun
2004;9(2):91–93.
34. Pfizer, Inc. Clear Health Communication, 2012.
Available at: http://www.pfizerhealthliteracy.com/.
Accessed 26.06.12.
35. National Patient Safety Foundation. Ask Me 3.
Available at: http://www.npsf.org/for-healthcare-
professionals/programs/ask-me-3/. Accessed 26.06.12.
36. U.S. National Library of Medicine, National Insti-
tutes of Health. MedlinePlus, 2012. Available at:
http://www.nlm.nih.gov/medlineplus/. Accessed 26.
06.12.
37. Agency for Healthcare Research and Quality.
AHRQ Pharmacy Health Literacy Center. Available
at: http://www.ahrq.gov/pharmhealthlit/. Accessed
26.06.12.
38. Weiss BD. Health literacy and patient safety: Help
patients understand. A Man Clinicians. Available
at: http://www.ama-assn.org/resources/doc/ama-
foundation/healthlitclinicians.pdf. Accessed 18.01.13.
39. Fry E. Fry’s readability graph: clarifications, valid-
ity, and extensions to level 17. J Reading 1997;
21(3):242–252.
40. Flesch RF. A new readability yardstick. J Appl Phys
1948;32:221–223.
41. Elo S, Kyngas H. The qualitative content analysis
process. J Adv Nurs 2008;62(1):107–115.
42. Hess J, Whelan JS. Making health literacy real: adult
literacy andmedical students teach each other. JMed
Libr Assoc 2009;97:221–224.
43. Mackert M, Ball J, Lopez N. Health literacy aware-
ness training for healthcare workers: improving
knowledge and intentions to use clear communica-
tion techniques. Patient Educ Couns 2011;85:e225–
e228.
44. Torres BA, Gonzalez-Diaz L, Martinez MD, et al.
Advanced ambulatory practice experiences that ad-
dress health disparities [abstract]. Am J Pharm Educ
2008;72(3):Article 72.
45. Harper W, Cook S, Makoul G. Teaching medical
students about health literacy: 2 Chicago initiatives.
Am J Health Behav 2007;37(Suppl1):S111–S114.

















