Embed Size (px)
Citation preview

Page | 1
Impact Assessment Study on Rasthtriya
Swasthya Bima Yojana (RSBY)
Study Report Submitted to Poorest Area Civil Society (PACS),
New Delhi
Study Team:
Sumit Mazumdar
Prashant Kumar Singh
Sudheer Kumar Shukla
Ashwani Kumar
POPULATION HEALTH & NUTRITION RESEARCH PROGRAMME (PHN-RP)
INSTITUTE FOR HUMAN DEVELOPMENT, NEW DELHI

Page | 2
Table of Contents Chapters Description Page no.
EXECUTIVE SUMMARY 3
Section I INTRODUCTION
Chapter 1 Introduction 10
1.1 Background
1.2 Aim and objectives
1.3 Review of literature
Chapter 2 Date and Methodology 20
2.1 Evaluation Research Design
2.1.1 Evaluation methodology
2.1.2 Sample selection
2.2 Study tools and techniques
Section II MAJOR FINDINGS
Chapter
3
Description of Study Population 29
3.1 Sample distribution
3.2 Health status and healthcare services utilization
3.2.1 Morbidity and healthcare utilization
3.2.2 Hospitalization
3.2.3 Out-of-pocket (OOP) expenditure
Chapter 4 RSBY: Awareness, Coverage and Utilization 38
4.1 PACS interventions in two selected states: A brief
4.2 RSBY in Jharkhand & West Bengal: An overview
4.3 Awareness
4.3.1 Overall awareness of RSBY scheme
4.3.2 Depth of awareness
4.3.3 Source of awareness
4.4 Enrolment
4.4.1 Coverage of RSBY scheme
4.4.2 Source of motivation
4.4.3 Help during enrolment process
4.4.4 Post enrolment visit for detailed information
4.5 Utilization
4.6 Effect of PACS interventions on awareness, enrolment and
utilization of RSBY scheme: Multivariate regression analysis

Page | 3
4.6.1 Effect on overall and specific awareness of RSBY
Scheme
4.6.2 Effect on utilization of RSBY scheme during
hospitalization
4.7 Finings from Qualitative Survey
4.7.1 Finding from Focus Group Discussions (FGDs)
4.7.2 Finding from In-Depth Interviews (IDIs)
Reference 66
Statistical Appendix 70
Technical Appendix: Sampling
Appendix: Household Questionnaire (Jharkhand)
Appendix: Household Questionnaire (West Bengal)
Appendix: Qualitative Guidelines and Domains

Page | 4
Executive Summary
In India, where around 28% of the total population lies below poverty line, it has been
observed that health care expenditure is one of the most important reasons for indebtedness. More
than 80% of the expenditure on health in India is through out of pocket which is one of the highest
in the world. To improve upon this scenario, Government has in the past launched a number of
health insurance schemes at both Central and State levels but most of these schemes have not
worked well in terms of reaching the desired objectives of reducing out of pocket expenditure and
improving access to health care. After taking into consideration, all the lessons learnt from these
insurance schemes and also after reviewing other successful models of health insurance across the
world in similar settings, Rashtriya Swasthya Bima Yojana was designed.
The Rashtriya Swasthya Bima Yojana (RSBY) attempts to insure poor people against shocks
from a low level of healthcare security. In the absence of any such security, the vulnerability of
people living at the margins or below the poverty line (BPL) increases and they get caught in a
“medical poverty trap”. It was to safeguard BPL/poor people from catastrophic out of pocket
(OOP) health spending that RSBY was launched in 2008 as a flagship scheme of the Government
of India. In the six years since, RSBY has been successful in enrolling a fair number of targeted
beneficiaries in the scheme yet the gap in its implementation need to be understood better.
Recognizing that performance of RSBY like many schemes in eastern Indian states, needs
to improve, PCAS with active support from the state and local government worked on raising the
overall awareness, enrolment and utilization of services in some of the poorest performing and
backward districts. Towards, this end PACS initiated number of activities and innovative ideas
with the involvement of local people to effectively communication hard-to-reach sections of
society. This study is an attempt to investigate the effectiveness of interventions led by PACS on
specific awareness, enrolment, and utilization of RSBY scheme in target districts across two states
– Jharkhand and West Bengal. Study selected two districts that had PACS actively involved and
two non-intervention districts where PACS had no intervention to compare outcomes including
awareness, enrolment and utilization of RSBY scheme.
Mixed methods approach was adopted with the inclusion of both quantitative and
qualitative research techniques. The evaluation methodology, in the absence of appropriate
baseline data in the intervention districts/communities, relies upon a treatment-control design. This
is done by separately sampling households from districts which are covered under the PACS
programmes (‘intervention’ group) and which are not (‘non-intervention’ group), in both the states.

Page | 5
Sample-level matching is followed to ensure that the study communities/villages selected from
both the groups are broadly similar in terms of socioeconomic characteristics.
The tools used were a household survey using semi-structured interview schedules, with
the data being subject to quantitative analyses, and qualitative interviews from other stakeholders.
While the quantitative approach has allowed assessing the impacts on a set of output indicators
such as levels of awareness about the programme and its benefits, enrolment in RSBY and/or
renewal of Smart Cards (program participation), The quantitative data measured the actual usage
of the during hospitalization events. The qualitative evidence was gathered to assess the process
dimensions of the interventions being conducted through in-depth interviews with district and field
level officials, representatives from insurance companies, third party administrators, smart card
providers, non-governmental organizations personnel, health service providers from empaneled
and non-empaneled hospitals and focus group discussions with community level functionaries
such as Anganwadi worker, Accredited Social Health Activists (ASHAs), male and female
beneficiaries.
This study was conducted in 8 selected districts – four each from PACS intervention and
non-intervention districts of Jharkhand and West Bengal. Districts were chosen to compare
‘target’ population proportion, even as the areas are not physically contagious. The selected
districts were West Singhbhum and Deogarh in Jharkhand, and Jalpaiguri and Murshidabad in
West Bengal that were selected as the PACS sample (‘treatment’) districts; while the control
districts were chosen as Khunti and Godda (Jharkhand), and Birbhum and Coochbehar (West
Bengal). The selection of blocks follow a slightly different logic: all blocks in the 8 districts
identified above were chosen on the basis of combined proportion of scheduled castes and tribes
as an indicator of vulnerable socioeconomic groups and female literacy rate, as per the latest
Census of India 2011 data based on the Primary Census Abstract. To select the blocks from the
PACS-sub sample, decisions were made based on discussions/feedback from respective state
teams and CSO partners. The identification of ‘treatment’ blocks defined target blocks to be of
similar socioeconomic standing in terms of the two indicators identified from the ‘control’ or non-
PACS sub-sample. Two Gram Panchayats within each of these blocks were then randomly chosen
through a random selection of sample of 1300 households. These households included 575 (500
beneficiaries or RSBY card-holders, 75 non-beneficiaries) from Jharkhand and 725 (625
beneficiaries, 100 non-beneficiaries) from West Bengal.
The preliminary sampling approach had envisaged a rapid houselisting exercise with a twin
objective of (a) identifying RSBY Smart-Card holders (beneficiaries) and non-beneficiaries, and
(b) stratifying the sample on the basis of key socioeconomic parameters, belonging to different
social/religious group affiliations and education levels. Subsequently higher costs both in financial
and time resources terms led to choosing an alternative. An updated list of beneficiary households
(‘RSBY rolls’), as available from the respective State Nodal Agencies and/or other agencies

Page | 6
(including the state PACS teams/CSO partners) was utilized as the sampling frame for selecting a
beneficiary sample of 1125 households. Thus purposive sampling was adopted to capture the
maximum households with RSBY card holders. This strategy allowed the assessment of the entire
process of the scheme, starting from awareness, motivation, enrolment processes, utilization of
scheme and its experience.
Finding shows substantial gap in overall awareness about the scheme in both selected states
and between intervention and non-intervention districts. In Jharkhand, about 80 percent of the
respondents from the non-intervention districts were aware about the scheme. However, in
intervention districts this awareness level is almost 95 percent. On the other hand poor RSBY
awareness i.e 24 percent was evident in West Bengal, particularly in intervention districts.
Awareness about specific components of RSBY scheme was recorded higher in
intervention districts of Jharkhand as the finding reveal that 50 percent respondents in non-
intervention districts were aware that Rs 30,000 is available under the RSBY scheme for a
year as compared to 75% in the intervention districts. The finding did not show variation
between intervention and non-intervention districts of West Bengal on six other specific
components of RSBY scheme.
The awareness about maximum amount available in each year under the RSBY scheme
among STs of intervention districts of Jharkhand was 85 percent – much higher than the
STs, living in non-intervention districts which was 49 percent. Thus, finding clearly
demonstrates, not only overall awareness about the RSBY scheme is higher in intervention
districts.
The major source of RSBY awareness in Jharkhand is the ASHA/AWW, followed by
RSBY Mitras. However, finding of the qualitative survey clearly shows prior to RSBY Mitra
appointment in their respective villages, none of the ASHA or AWW knew about the RSBY
scheme. Thus, one could very effectively conclude that although, majority of respondents
reported ASHA or AWW as the major source of RSBY scheme awareness, it is PACS
promoted RSBY Mitras who actually initiated the information and dissemination in the
community.
In case of West Bengal, about 55 percent respondents came to know about the RSBY
scheme by PACS community mobilizers, followed by friends and relatives (23 percent). This
clearly shows that across all four intervention districts of both states, PACS led initiatives is
playing very vital role in information and dissemination of RSBY scheme. This finding was
supported by qualitative results conducted across different stakeholders including users,
which categorically appraised the initiatives like RSBY Mitra in Jharkhand and Community
Moblizers in West Bengal. Results further shows higher reach of mass media campaigns

Page | 7
regarding RSBY scheme among marginalized sections population including STs and poor in
intervention districts as compare with non-intervention districts.
Based on both quantitative and qualitative results, this study identified critical gaps that
need to be addressed in future so that both overall and specific awareness of the scheme could
reach majority of population, particularly in West Bengal. For instance, in many cases lower
proportion of respondents from the intervention districts of West Bengal noticed awareness
activities including mike announcements, rallies, drama and wall writing. It is true that when
comparing these activities with the non-intervention districts, intervention districts performed well
in majority of actives but still more frequent activities is required to reach maximum households.
Result of this study shows higher enrolment rates across all intervention and non-
intervention districts in both states. Over 80 percent of the respondents covered in the sample from
both intervention and non-intervention districts enrolled in the scheme. The findings did not show
significant difference in overall enrolment by selected socioeconomic characteristics between
intervention and non-intervention districts. This pattern is expected since; the overall conversion
ratio (statistical appendix 1 and 2) of both states is over 50 percent, with majority of districts having
conversion ratios over 60-70 percent. However, this pattern could be explained based on
observations received during FGDs and IDIs. For instance, during FGDs in both states almost
every participant has been enrolling their family/household under RSBY scheme either since 2010
or 2011. Similarly, finding from IDIs from different stakeholders also supports the previous
arguments that villagers or community members have been enrolling under RSBY scheme over
last three to four years. However, it is very imperative to note that in spite of high enrolment under
the scheme none of them availed any benefits of the scheme due to lack of proper knowledge.
The utilization of RSBY scheme during hospitalization shows tremendous
improvement in intervention districts in comparison to the non-intervention districts, i.e in
Jharkhand. For instance, the logistic regression analysis after adjusting key socioeconomic
characteristics in the model revealed that the utilization of RSBY scheme is over four times
higher in the PACS intervention districts as compared with non-intervention districts of
Jharkhand. Moreover, utilization of RSBY scheme for hospitalization by marginalized
sections of society is considerably higher in intervention districts in comparison to the
nonintervention districts. For example, about 83 percent respondents from the ST
community in intervention districts utilized RSBY scheme for hospitalization which is
considerable higher than the STs of non-intervention districts (22 percent). Similarly, in
intervention districts of Jharkhand over 80 percent respondents from the poorest (MPCE)
household utilized RSBY scheme, whereas the corresponding figure in non-intervention
districts is less than 10 percent. This clearly suggest huge effect of PACS led intervention
programmes in Jharkhand and its subsequent outcomes in case of high use of RSBY scheme
across all sections of society.

Page | 8
However, in case of West Bengal study did not find significant variations in case of
utilization of scheme during hospitalization between intervention and non-intervention districts.
Moreover, in unadjusted cross tabulation, finding shows higher utilization rates in non-intervention
districts than to intervention districts. Although, regression analysis doses show higher odds of
RSBY use during hospitalization in intervention districts than to non-intervention districts but
depicts week statistical power to support this finding.
The higher utilization of RSBY scheme in intervention districts of Jharkhand and no
significant difference in case of West Bengal could be explained with the support of few
observations based on both quantitative and qualitative surveys. For instance, in intervention
districts of Jharkhand over 30 percent respondents said that during the enrollment process PACS
community mobilizes/ or RSBY Mitra helped them. Further, nearly 30 percent respondents in
intervention districts of Jharkhand said that RSBY Mitra visited their homes few days after the
enrolment and provide detailed information about the scheme. However, in case of West Bengal
comparatively lower proportion of respondents said about post enrolment visit by community
mobilize.
One could also link lower utilization of RSBY scheme in interventions areas of West
Bengal is the lack of timing and involvement of entire family members in tea gardens. As
mentioned above in the qualitative findings, many families who willing to either enroll or wanted
to use RSBY scheme during hospitalization could not do so due to non conducive work or
infrastrural issues such as not getting leave from work or not being able to organize transport to
reach the health facility. The lack of transportation remains of the big challenge in study areas. In
these circumstances, many families prefer to visit locally available traditional healers or health
providers for most illness. This has also been highlighted during in-depth interviews of community
mobilizes of one of the intervention districts in West Bengal. However, the effect of other
unobserved factors such availability and functional status of available health facilities and quality
dimensions could not be captured in this study.
To conclude, it has been observed from this study that there is a clear pattern of
increasing awareness, enrolment and most importantly utilization of RSBY scheme in
intervention districts as compared with the non-intervention districts. The pattern is much
apparent in Jharkhand than in case of West Bengal. Due to PACS led interventions programmes
in intervention districts, general and specific awareness about the RSBY scheme and its
benefits has increased in last few years. The most imperative change that PACS led initiative
programme is successful in bringing families to the health facility and subsequently use of
RSBY card for hospitalization. As people started utilizing RSBY scheme, the overall health
expenditure of households reduced. Now, people feel more secure during illness and
hospitalization after their being enrolled under the RSBY scheme. Hard-to-reach sections of the
society including SCs/STs and poor started utilizing this scheme to a greater extent.

Page | 9
Additionally, the PACS led interventions apart from targeting individuals or
households towards increasing the benefits of RSBY scheme, worked as a ‘catalyst
instrument’ that assisted in unlocking the community potentials, while involving different
stokeholds including PRI members, local leaders, and community workers that ultimately
leads towards more sustainable positioning of RSBY scheme in the community. Nevertheless,
in-spite of encouraging results much more work needs to be done to raise the utilization of RSBY
scheme. In case of West Bengal, special support and strategic analysis is needed to reach enhanced
the utilization of RSBY scheme, in particular.
Section – I:

Page | 10
Introduction
1.1 Background
Access to quality health care is still a distant reality for majority of population in India,
particularly for vulnerable groups like Scheduled Castes/Scheduled Tribes, and poor – in spite its
status as a rising economic power. As per WHO statistics in 2011, 26 % of total population in India
is living below poverty line which is about 300 million of total population. Burden of
communicable and non communicable diseases are increasing in India and this is
disproportionately affecting the vulnerable sections of the population. According to an estimate,
about 40% of the poor had to borrow money from lenders with high interest rates or have to sell
their assets in order to ensure quality medical care (Ahuja & Narang, 2005). In India, the central,

Page | 11
state and local governments together contribute only 20% of the total health expenditure while
71% of the total is contributed by individual households through out-of-pocket (OOP) expenditure
at the time of illness (Seshadri et al., 2011). This high level of OOP expenditure by individual
households is one of the highest amongst low and middle income countries, thus ranking India low
in terms of financial protection (Ellis et al., 2000).
The health care delivery system in India consists of private, public and mixed ownership
institutions. It has been estimated that the private sector accounts for more than 80% of the total
healthcare spending in India. In addition to private sector spending, the share of out of pocket
expenditure in the country runs high which ultimately creates a financial burden on the households,
pushing them increasingly towards poverty. According to Berman et al., (2010) more than ten
million households in India were pushed below the poverty line (BPL) due to spiraling healthcare
spending in 2004. The burden of costs incurred for accessing medical care has increased over the
last two decades. The latest data of the National Sample Survey (NSS) shows that on average,
households spent Rs 295 for outpatient care and Rs 7,116 for in-patient care. The National Sample
Survey 61st round, moreover, reports per capita expenditure in India to be Rs. 804 in the rural area
and Rs. 958 in the urban area (Gupta 2009). In India, health expenditure constitutes approximately
5% of the total household outlay (Gupta 2009). More ironically, the analysis of the NSS 60th round
suggests that around 6% of the total households (7% in the rural areas and 5% in the urban areas)
fell below the poverty line as a result of healthcare spending in 2004 (Berman et al 2010). It has
been estimated that about 2–3% of Indians are impoverished every year because of health care
expenditure. All these figures are aggregate, the picture is worse if one disaggregates along the
divides of socioeconomic strata including place of residence (urban/rural), gender, social groups
(upper/lower caste), household economic status, etc.
Financial constraints are the major barriers for access to healthcare in India, particularly
for marginalized sections of society where health care expenditure is a major cause of
impoverishment. Unequal distribution of health care facilities, socioeconomic conditions and
existing social and gender norms all play an important role in significantly reduced access to health
care especially by poor population. This scenario is exacerbated by reduction in governmental
health spending and high cost for health care services in private sector. The inequality in health
care services between public and private sector and economic constrains are found to affect health
of the poor sector of population which constitutes majority of India.
Over the past decades many low-and-middle income countries have found it increasingly
difficult to sustain sufficient financing for health care particularly for the poor and have been active
in recommending a range of suitable measures (Lagarde et al., 2009; Ekman 2004). In this
sequence, a focus on Social Health Insurance (SHI) schemes has been gaining strength in majority
of countries, including India (Gupta &Trivedi, 2006; Gupta &Trivedi, 2005). For instance, the
WHO in 2005 passed a resolution that it would support a strategy to mobilize more resources for

Page | 12
health, increase access to health care for the poor and deliver quality health care in all its member
states but especially in low income countries (WHO, 2005). In latter stage this strategy was also
supported by the World Bank (Hsiao, 2007).
The SHI schemes are generally understood as health insurance schemes provided by
governments to its citizens, especially to low and middle income populations.Most social health
insurance schemes combine different sources of funds, with government often contributing on
behalf of people who cannot afford to pay themselves (WHO, 2005). Social health insurance
differs from ‘tax based financing’ which typically entitles all citizens (and sometimes residents) to
services thereby giving universal coverage. However, social health insurance entitlement is linked
to a contribution made by, or on behalf of, specific individuals in the population (WHO, 2005).
Social health insurance pools both the health risks of its members, on the one hand, and the
contributions of enterprises, households and government, on the other, and is generally organized
by national governments (Carrin& James, 2004; WHO, 2005).
The government is committed to provide ‘Health for All’ set by the Alma Ata1 declaration
in 1978 and adequate financing is critical to ensure it. Universal Health Coverage (UHC) which
has subsequently replaced the “Health for All” agenda, defines “ensuring that all people can use
the promotive, preventive, curative and rehabilitative health services they need, of sufficient
quality to be effective, while also ensuring that the use of these services does not expose the user
to financial hardship2”.The government of India has decided to increase its health spending to
increase demand for healthcare and ensure equity in access to healthcare. To accomplish this in
the wake of high out of pocket health spending is a challenging task. This in turn requires
alternative security measures for those who cannot pay for healthcare. Coverage by other public
and private health insurance is limited in India. Hence, to provide universal health coverage in a
country like India, where most people are either unemployed, or employed informally in the
unorganized sector, is not only challenging but also expensive. These challenges are further
intensified due to the disparity in health systems across states and between rural and urban areas.
The RSBY Scheme
In order to achieve an equitable health system and move towards universal health coverage
in India, The Ministry of Labour and Employment launched the RashtriyaSwasthyaBimaYojana
(RSBY) for the poor (BPL) families of India. This National Health Insurance Scheme was
1Primary Health Care: Report of the International Conference on Primary Health Care. Alma-Ata, USSR, 6-12
September 1978. World Health Organization, Geneva, 1978
(http://whqlibdoc.who.int/publications/9241800011.pdf). 2WHO website. What is universal coverage?
(http://www.who.int/health_financing/universal_coverage_definition/en/index.html).

Page | 13
launched in April 2008 and the scheme is being functioning in all states. Around 37 million
households have been enrolled across the country and around 6.6 million people have benefitted
so far. More than 10,000 hospitals have been empanelled in the scheme and thirteen Insurance
Companies (both public and private sector) implement the scheme (Seshadri et al., 2011).
Main Objectives of RSBY
To provide financial protection against catastrophic health costs by reducing out of pocket expenditure
for hospitalization
To improve access to quality health care for below poverty line households and other vulnerable groups
in the unorganized sector
Provide beneficiaries the power to choose from a national network of providers
Provide a scheme which even the illiterate can use easily
Eligibility and Benifits
o Smart card based cashless and paperless social health insurance scheme
o Registered BPL families, MANREGA workers, registered daily wage labourer etc.
o Annual hospitalization coverage of up to Rs 30000/- for a family of five members through
health insurance companies
o Families pay a registration fee of Rs 30/- for accessing empanelled hospitals across the country
o Coverage is for inpatient treatment
o Transportation expenses of up to Rs 1000/- annually (with a limit of Rs 100 per hospitalization)
are provided in cash for travelling to the hospital (deducted from the benefit package of Rs
30000/-)
o All pre existing diseases are covered from day 1
o There is no age limit for enrollment into the scheme
o 75 percent of the premium is borne by the Central Government while 25 percent is the State’s
responsibility (90 percent in case of Jammu & Kashmir as well as North Eastern States)
o There is a provision for the State Governments to top up the coverage amount beyond Rs.
30000/-
Basic design of the scheme
Page | 14
Although other government-run public health insurance schemes existed in India, RSBY is a
pioneering scheme in many aspects. Some of its key design features are:
1. Public-Private Partnership (PPP): Public and private medical facilities, Third Party
Administrators (TPA) and insurers partner with the State Nodal Agencies (SNAs) that set the
guidelines, quality standards, and monitors programme implementation.
2. Central-State Government Collaborative Model: While the programme was designed by a
department of the central government, the implementation and management is undertaken in
collaboration with respective state governments. The premium subsidies are co-financed by
the centre and the states, thus ensuring mutual ownership and control.
3. Leveraging of Technology: Since the scheme targeted Below Poverty Line1 (BPL) families
with low literacy levels, paperwork was minimized by using biometric identification that
enabled instant enrolment, and control over fraud.
4. Demand-side Financing: The scheme financially empowers the patient through the provision
of a value-loaded smartcard that offers cashless access to medical facilities covering almost all
procedures. The smartcard can be used at any empanelled hospital in the national network,
allowing the convenience of flexibility to the considerable migratory population in the country.
5. Premium Subsidy: The premium is subsidised 100% from government funds, with only a
nominal enrolment cost paid by the beneficiary.
6. Collection, Storage and Maintenance of Data: Data collected from the administration of the
scheme is stored and maintained by the Government agency, thereby facilitating future
actuarial calculations and market development.
Different actors and their role in the RSBY
Beneficiaries: Initially the scheme targeted BPL population alone. Now it has started
expanding its coverage to include other occupational groups. Beneficiaries of the MGNREGA
scheme, domestic workers, auto-rickshaw drivers, etc. Beneficiaries are expected to enrol in the
scheme by paying Rs.30 (approx. US$ 0.5) per family (for five members) for a year, receive a
smart card, and then use the benefits when hospitalized in empanelled hospitals.
Non-governmental organisations (NGO): NGOs are expected to create awareness among
the community esp. the eligible groups about RSBY and mobilize them for enrolment.
Insurance Companies (both private and public sector companies): The companies
compete with each other for covering the eligible families in each State. The company with the
lowest bid gets the contract for implementing the scheme in that specific State. Once selected, the

Page | 15
company has to appoint smart card agencies, work closely with the State government’s Nodal
Agency to identify the eligible households, empanel hospitals and contract NGOs to create
awareness in the community.
Third Party administrators (TPA): These are private agencies that help the Insurance
Company in implementing the scheme in the field level.
Smart Card Providers: They provide the technology for this scheme.
Empanelled hospitals (both public and private): Once empanelled by the Insurance
Company, they provide the necessary services to the RSBY beneficiaries. Their services are
reimbursed by the Insurance Company via TPAs or directly.
State government Nodal Agency (SNA): It is an independent body formed by the
Government which acts as the focal point for governing the programme. In most States, it is led
by the Department of Labour while in some it is the Department of Health & Family Welfare. It
initiates the process of introducing the scheme in the State, negotiates with the insurance company
and monitors the enrolment and the utilization. The State contributes 25% of the premium through
this agency.
Central government: The Ministry of Labour and Employment launched the scheme and
its main responsibility is to develop technical and administrative guidelines and market the scheme
to the State governments. The Central government contributes 75% of the premium to the
Insurance Company through the Ministry.
1.2 Aims and Objectives
Poorest Area Civil Society Programme (PACS) intends to conduct an impact evaluation
study to assess the impact of various strategies it pursues along with the partner civil society
organizations (CSOs), aiming to improve access to health services and utilization of hospitalization
insurance facilities under the Rashtriya Swasthya Bima Yojana (RSBY), with an emphasis on
social and economically disadvantaged population groups. Institute of Human Development
(IHD), New Delhi has been entrusted with the assignment of conducting the impact assessment of
different strategies and interventions being pursued in certain districts in two states, Jharkhand and
West Bengal.
The main objective this assessment study is to:
Page | 16
i. Assess the effectiveness of various interventions and activities being undertaken by
PACS/CSO partners, in improving the awareness of communities regarding enrolment
and utilization processes under RSBY, such as access to and use of Smart Cards.
ii. Understand the impact on capacities of the partner CSOs towards building community
awareness and improved uptake of RSBY provisions, and also in sensitizing other
stakeholders such as community leaders, local self-government institutions, health
officials and local administrations to ensure smooth, better functioning of the scheme.
iii. Identify best practices in each of the study states and communities, that can help
benchmark PACS’ future initiatives and generate learning points for replication and
scaling-up.
1.3 Review of literature
Although, the RSBY scheme is now its sixth year of progress only a few studies have been
conducted across /different settings in India. The existing studies broadly covered awareness,
coverage, and enrolment aspects of the scheme. Some others have attempted to cover the effect of
scheme on health expenditure, hospitalization experiences and other aspects of service utilization.
Enrolment
As per the RSBY website, around 37.7 million BPL families are currently enrolled on the
RSBY scheme nationwide (www.rsby.gov.in). The scheme is being implemented in 512 districts
across 28 states and union territories. There are many evidences across different settings that have
highlighted substantial gaps in the scheme accessibility. For instance, Sun (2011) has studied
enrolment patterns at village, household and individual levels using administrative data. The
findings indicate that there are wide variations in enrolment rates across villages, districts, regions
and demographic groups. About 3% of the selected villages have witnessed that all BPL
households have been enrolled while none eligible families have enrolled in 10% of the villages.
This study also points out that variation in the performance of awareness raising is the main factor
causing the discrepancy of enrolment rates. Furthermore, Sun asserts that there may exist
“geographic discrimination based on the cost of enrolment” or the deliberate enrolment of
“healthier” villages in insurers’ behavior. Study further asserts that these variations may be linked
to various factors such as discrepancies in BPL data which has not taken into account factors of
birth; death; migration or marriage in the subsequent years after the BPL survey was conducted;
poor power back up in the villages; low awareness among the people about the scheme and
enrollment schedule in their respective villages etc. (Sun 2011).

Page | 17
Similarly, Rathi (2011) in his evaluation of RSBY in Amravati, Maharashtra, found that
the lack of information and late enrolment led to only 39% enrolment in the district. The tribal
blocks of the district which have the maximum number of poor householdswitnessed least
enrolment levels. The study further suggests that beneficiaries were concentrated in certain areas
and villages. Similarly, Narayana’s (2010) study shows huge enrolment variation within the states,
evidencing low enrolment in poorer districts.
It has been argued that any scheme which targets only BPL families risks leaving out a
large number of actual poor communities due to exclusion errors in the BPL list. In Chhattisgarh,
the government recognizes 74% of its population as poor and provides subsidized grain
accordingly (Wadhwa 2010). However, central government has fixed the percentage of BPL in the
State at 46%. Hence, there is a huge population of poor people who have not been even considered
eligible for the RSBY scheme, this being an entirely centrally – sponsored scheme.
Using a larger sample of 145 districts during the first year of RSBY, Swarup (2011) finds
district-wise imbalances in enrolment rates. The descriptive analysis by the author largely
attributes these variations in enrolment rates to ‘‘defective and outdated’’ BPL lists provided by
the state governments to insurance companies, and concludes that the errors in the lists also
produce a gender bias, since they include only the names of male heads of household. However,
this could also be attributed to skewed incentives for insurance companies because payment is
provided on enrolment per household instead of enrolment per individual (Das &Leino, 2011).
Dror and Vellakkal (2012) evaluate the financial burden of RSBY, and its implications for
enrolment. The authors argue that finance plays an important role in undertaking enrolment drives.
In order to scale up from the existing levels of enrolment, and to maintain the financial viability
of the scheme, the central budget allocation for RSBY should be increased and the scheme will
have to attract a large above-poverty-line enrolment (i.e., those who pay a non-subsidized
premium).
A recent study conducted in Maharashtra found that the ever-enrollment rate of RSBY
amongst BPL households (22%) was even lower than the proportion of households that reported
to be aware about the scheme. Further, the present found that only 12% of the eligible households
reported that they were currently enrolled under the RSBY programme, though a small proportion
of them were not having valid RSBY card during the period of data collection (Thakur &Ghosh,
2013).
Utilization of RSBY scheme
According to the study by Hou& Palacios (2011), utilization rates vary largely across
villages and districts. Their research reveals that districts served by three of the six insurance
companies have higher utilization rates than areas where two of the three are private insurers.

Page | 18
Study also found that the likelihood of RSBY scheme access depends on the number of people in
the same village who have already utilized the benefits and the number of hospitals empaneled
under the scheme in the area. The utilization rate is also found to be concentrated to a select few
empaneled hospitals in the district (Hou& Palacios 2011).
Narayana’s (2010) findings show that the average hospitalization rate per 1000 persons
over a scope of 365 days varies from 4 in Punjab to 25 in Gujarat. The study also reports the highest
hospitalization rate of 196.41 in the Dangs district of Gujarat and the lowest in 1 in the Jalandhar
district of Punjab. Study suggested that the low density of empaneled hospitals and the lower
empanelment of the private hospitals in total as the probable factor for variation in district
hospitalization rates.
In a study assessing existing health insurance schemes, Reddy et. al., (2011) find that the
nationwide hospitalization rate per 1000 persons for 2009-10 stands at 20, taking into
consideration those districts which have completed one year of the RSBY scheme. Assam, Goa,
Chandigarh report the lowest hospitalization rates of a mere 1while Gujarat reports the highest at
42. The hospitalization rate per 1000 beneficiaries in other state based insurance schemes is
reported to be five in the Rajiv Aarogyashri scheme; four in the Vajpayee Aarogyashri and
Kalaignar schemes and 22 in the Yesaswini scheme. This number is high (64) for private health
insurance. As per the study, the average nationwide hospital expenditure for RSBY is
approximately Rs. 4262. The lowest expenses are reported in Tamil Nadu (Rs. 886) and highest in
the state of Punjab (Rs.6554). The claims ratio in this study is found to be 7%, with Gujarat having
the highest claims ratio of 15% and Goa the lowest of 0.20% (Reddy et. al., 2011).
Kumar (2010) explores the implementation of RSBY in Puri district, Odisha state and finds
out that the reasons of low utilization of inpatient healthcare were due to the high proportion of
illiteracy and the poor performance of awareness raising, the BPL households lack enough
awareness of their RSBY benefits. Further, study suggest that the number of empaneled hospitals
in that area is far from enough along with few of them refuse or delay treatment to the BPL
households, which ultimately negatively associated with the scheme utilization. Similarly, a study
conducted in the Durg district of Chhattisgarh found that the in 99% of studied cases, the RSBY
brochure was not given when the BPL households are being enrolled. Consequently, the
respondents don’t have the list of empaneled hospitals at the time of enrolment (Nandi et al., 2012).
Based on a large scale survey of a randomly selected sample of 3,647 eligible households
and 39 interviews of empaneled hospitals, Rajasekhar et al. (2011) assessed the current
implementation of RSBY in India’s Karnataka state observed some serious problems that
significantly determine the utilization of the benefits, such as “delays of several months to issue
the smart cards; poor knowledge of how and where to utilise the scheme; hospitals not trained to

Page | 19
use card-reading technology; and month-long delays and arbitrary caps in the reimbursement of
treatment expenses to hospitals.”

Page | 20
Section – I1:
Data & Methodology
2.1 Evaluation Research Design
2.1.1 Evaluation Methodology
The evaluation methodology, in the absence of appropriate baseline data in the intervention
districts/communities, relies upon a treatment-control design, with a partially randomised
approach. This is done by separately sampling households from districts which are covered under
the PACS programmes (‘intervention’ group) and which are not (‘non-intervension’ group), in
both the states. Sample-level matching is followed to ensure that the study communities/villages
selected from both the groups are broadly similar in terms of socioeconomic characteristics.
The evaluation approach will follow a mixed-method design, involving a household survey
using semi-structured interview schedules, with the data being subject to quantitative analyses,
and qualitative interviews from other stakeholders. While the quantitative approach will allow
assessing the impacts on a set of output or outcome indicators such as levels of awareness about

Page | 21
the programme and its benefits, enrolment in RSBY and/or renewal of Smart Cards (program
participation), actual usage of the during hospitalization events, and ultimately the extent of
financial risk-protection (program benefits) thus availed, the qualitative evidence will be useful to
assess the process dimensions of the interventions being conducted on the one hand, and
functioning of the RSBY programme at large on the other.
For the quantitative analyses, the evaluation approach will primarily rely on standardized3
comparisons of the output/outcome indicators between the PACS (treatment) and non-PACS
(control) samples. Additionally, we also focus on examining the relative impacts on the specific
disadvantaged population, by incorporating appropriate socioeconomic profiling and stratums
during the sample design. In other words, this approach will allow both between-group (treatment-
control) as well as within-group (between disadvantaged vis-à-vis non-disadvantaged groups)
comparisons in terms of the output indicators.
The qualitative approach – evaluating the processes rather than specific outputs/outcomes
– will rely on the perspectives of the key stakeholders regarding specific interventions being in
place, or on the key aspects of RSBY such as the enrolment process, renewal of Smart Cards,
information on hospitals and use of cards etc. As elaborated in the next section, a few interviews
will be conducted in both the states, and the results helping to understand the important features
relating to the functioning of RSBY, covering the vulnerable groups, and the role of PACS/CSO
partners’ interventions and initiatives in impacting on the above.
2.1.2 Sample Selection
Details of the sample selection approach, for household survey, have been earlier described
in the Study Proposal. To briefly recapitulate, all districts in both the states were ranked according
to the proportion of BPL (or ‘target’) population, calculated on the basis of figures provided in the
RSBY website. From the list4, two districts from the PACS intervention districts were selected,
additionally keeping in view the geographical spread of the states. Districts of comparable ‘target’
population proportion, while at the same time, not being physically contagious is selected as the
3 Standardizing or statistical adjustments in the output/outcome indicators lie at the core of the analytical rigour of
the evaluation, and helps to prevent any biases or potentially faulty inferences. This will be primarily achieved in the
analysis through ‘need-standardizations’ i.e. controlling for need factors such as disease prevalence, and average
hospitalization rates, and standard demographic adjustments such as age-sex composition of the two sample-groups.
Such adjustments, based on observable characteristics, are rather straightforward but more tricky is to adequately
control for ‘unobserved’ effects such as similar interventions being in place in the ‘control’ communities, or risks of
spillover to these communities due to physical contagiousness to the ‘intervention’ communities. Entire elimination
of such unobserved effects is more data-demanding, but the evaluation design being adopted does this partly through
selecting geographically distant sampling units, and collecting data through screening questions on exposure to
similar interventions by the control sample as being given to the treatment sample. 4 See Annexure 1 of this Report

Page | 22
districts. Accordingly, West Singhbhum and Deogarh in Jharkhand, and Jalpaiguri and
Murshidabad in West Bengal were selected as the PACS sample (‘treatment’) districts; the
control districts respectively are Khunti and Godda (Jharkhand), and Birbhum and Coochbehar5
(West Bengal). The selection of blocks follow a slightly different logic: all blocks in the 8 districts
identified above are listed on the basis of two indicators: combined proportion of scheduled castes
and tribes (as an indicator of vulnerable socioeconomic groups) and female literacy rate, as per
the latest Census of India 2011 data (Primary Census Abstract). Detailed lists and tabulations are
included as Annexure 2. To select the blocks from the PACS-sub sample, decisions are made based
on discussions/feedback from respective state teams and CSO partners6. Once the ‘treatment’
blocks are identified, blocks of similar socioeconomic standing in terms of the two indicators
considered are identified from the ‘control’ or non-PACS sub-sample. Two Gram Panchayats, are
then randomly chosen from each of these blocks, followed by random selection of sample
households.
The target size of the sample households, as discussed at length in the proposal, have
been worked out to be 1300 households, including 575 (500 beneficiaries or RSBY card-
holders, 75 non-beneficiaries) from Jharkhand and 725 (625 beneficiaries, 100 non-
beneficiaries) from West Bengal (For the interested reader, the details of the sample size
determination methodology is included as Annexure 3).
The list of sampling units (finalized for Jharkhand, to be finalized based on state inputs for
West Bengal) is as follows:
Category State Districts Blocks Villages (PSU)
PACS-district
West Bengal
Jalpaiguri
1 Kumargram 1 Khurdanga 1
2 Khurdanga 2
2 Malbazar 3 Chengmari
4 Rangamati
Murshidabad
1 Jiaganj 1 Mukundabag
2 Prasadpur
2 Sagardighi 3 Barala
4 Gobardhandanga
Jharkhand West Singbhum
1 Chakradhapur 1 Asantaliya
2 Jamid
2 Majhgaon 3 Nayagaon
4 Ghodabandha
Devghar 1 Madhupur 1 Suggapahari
5Coochbehar although neighbouringJalpaiguri, is selected as a control, as all other districts (except Darjeeling) of
Northern West Bengal, a distinctive geographic and socioeconomic region of the state, are in the PACS intervention
sample. 6 At the time of submitting the Inception Report the blocks of the two Jharkhand districts could be decided based on
interaction meetings.

Page | 23
2 Gadiya
2 Mohanpur 3 Bichgarha
4 Jamuniya
Non-PACS-district
West Bengal
Coochbehar
1 Tufanganj-II 1 Salbari I
2 Mahishkuchi I
2 Mekhliganj 3 Niztarof
4 Changrabandha
Birbhum
1 Rajnagar 1 Lauberia/Aligarh
2 Balarampur/Chandrapur
2 Sainthia 3 Derpur/Hatora
4 Paharpur/Ikra
Jharkhand
Godda
1 Basantray 1 Jamnikola
2 Bodra
2 Meherma 3 Gajhanda
4 Dhodra
Khunti
1 Khunti 1 Siladon
2 Dadiguttu/Gutjora
2 Erki (Tamar II) 3 Erki/Arki
4 Sindri
In the preliminary sampling approach specified in the Project Proposal, it was envisaged
to conduct a rapid houselisting exercise from the twin objective of (a) identifying RSBY Smart-
Card holders (beneficiaries) and non-beneficiaries, and (b) stratifying the sample on the basis of
key socioeconomic parameters, namely social/religious group affiliations and education levels.
However, during subsequent interactions it was felt that such screening exercise would lead to
higher costs both in financial and time resources terms, given the project’s timeframes. As an
alternative, it was proposed that updated lists of beneficiary households (‘RSBY rolls’), as
available from the respective State Nodal Agencies and/or other agencies (including the state
PACS teams/CSO partners) be used as the sampling frame for selecting the beneficiary sample
(1125 households). In this approach, stratification will be left random, i.e. without any separate
screening, but using other a-priori information sources (e.g. social mapping, feedback from local
key informants), and non-beneficiary households will be selected randomly from neighbouring
households (not possessing RSBY cards) of the beneficiaries. However, during the household
selection it will be ensured to have a balanced mix of all socioeconomic stratums, and particularly
adequate representation of the vulnerable or priority groups. A systematic circular sampling
allowing common intervals will be followed to identify beneficiary households to be interviewed
from the ‘RSBY rolls’; it was also agreed that the state PACS teams and CSO partners will
facilitate procuring the RSBY rolls/cardholder’s lists for the selected GPs and making these
available to the evaluation team, for both PACS as well as non-PACS areas under the study.
As stated earlier, the household survey will be supplemented by qualitative data collected
through alternative techniques such as in-depth and key-informant interviews, focus group
discussions and interactions with key programme personnel, from both the providers (government)
and the community organizations. While the exact numbers of each tools/techniques and targeted
interviewees will be finalized at the time of data collection, a broad indication is provided by the
two schemas below:

Page | 24
2.2 Study Tools and Techniques
The tools and techniques that will be applied in this study is divided into two segments:
Quantitative research tools:
Section 1: This section includes questions related to the household member’s
demographics and socioeconomics characteristics, which will be used for stratification, and group-
based analysis (2 pages)
Section 2: Information related to the household living condition, household assets, income
and livelihoods, and social networks will be asked. This section will help in distinguishing between
treatment-seeking behaviour, and allow observing financial risk-protection impacts, based on a
household’s economic ability to pay, arising out of insurance coverage (2 pages, including poverty
profile and consumption expenditure module).
Section 3: This is the core health module. In this section, detailed information related to
health including short-term and chronic morbidities and health care utilization will be asked.
Further information on hospitalization will also be covered with special focus on type of
hospitalization, number of days spend, cost of hospitalization etc. A separate block will collect
information on health care financing, or health expenditure patterns, sources of financing the
expenses, coping mechanism adopted in response to the financial implications arising out of the
health shocks, and any adverse welfare consequences (3-4 pages).
Section 4: This section deals with the RSBY users’ experience that essentially includes
flow of information, their perception & satisfaction. More specifically, we will ask about the
source of information, experience of the enrolment process, utilization of smart card, whether they
have explained about the process/how to use your RSBY card, information of nearest hospitals to
seek treatment and be able to use the Card etc. In addition, questions will also cover the reasons
for not utilizing the health card and their suggestions to improve the overall efficiency of RSBY
programme. Developing this section which can help in assessing the relative outreach, coverage,
impacts and people’s perception on the different interventions and initiatives being supported by
PACS/CSO partners’ activities in the intervention communities, is of much importance for the
evaluation’s approach, and currently interactions between the research and programme teams are
being held to fine-tune the dimensions to be included in the interview schedules, and make them
suitable for precise, objective assessments. This section is expected to be about 5 pages including
all the domains stated above. A draft matrix, which is being updated and fine-tuned during the
state-level briefings, is appended (Annexe 4).

Page | 25
Qualitative research tools:
The study has applied following qualitative techniques to understand the different
dimensions related to RSBY from different stakeholders. Detailed descriptions of the number of
qualitative surveys are graphically presented below.
FGDs: The study has conducted six FGDs from individual users and different stakeholders
as illustrated in the table earlier, to understand the flow of information related to RSBY scheme,
enrolment process etc. The domain included covered problems or constrains related to enrolment
in RSBY scheme, time taken to complete the entire process and staff behaviour. The FGD also
covered processes and steps adopted by different stakeholders for mobilizing people for enrolling
in this scheme with special emphasis on socially excluded groups in the community. We also tried
to examine the challenges in encouraging people for enrolling in the RSBY scheme. The FGDs
was based on stratified groups or stakeholders, which was finalized in consultation with PACS and
its other partners.
IDIs: This study has also performed about 20 IDIs, across all eight selected districts. The
IDIs included those individuals who were directly associated with the RSBY scheme at state,
district, block and local/community level along with beneficiaries. For instance, detailed in depth
interviews was conducted to the district programme managers (DPM) in charge of RSBY
programme unit. The issues that were covered in IDIs strategies related to the management
information system (MIS), smart card distribution and key steps towards expanding the
beneficiaries under RSBY. Further at village level members of Panchayat interviewed to
understand the village or community specific knowledge and perceptions of RSBY, constraints
that restricts the coverage of the scheme. What are the steps so far taken to encourage the scheme
among socially deprived groups at village or community level and their progresses? Further,
detailed interview related to nearest hospital travel arrangements; overall facility and experiences
was also examined by RSBY beneficiaries. Study also captured suggestions, recommendations
and key issues that need to be focused towards universal coverage of RSBY scheme among
marginalised sections of the society. One of the key drivers of any scheme at community level is
the NGOs and CSOs. The study also covered their views on RSBY scheme and what they have
the strategies to strengthen the overall impact of scheme, particularly among poorer sections of the
society.
Qualitative approach of the study
FGDs (6)
(8)
IDIs (20)
(25)
Case study (2)
(4)
West Bengal
(3)
PACS(2)
Non-PACS(1)
Jharkhand
West Bengal
(10)
PACS(5)
Non-PACS(5)
Jharkhand
West Bengal
(1)

Page | 26

Page | 27
Part III

Page | 28
Major Findings
3. Description of the study population
3.1 Primary survey: Sample distribution
This section presents the description of the study population in intervention and non-
intervention districts in two states. It briefly covered demographic, socioeconomic and some
household level sample characteristics.
The age wise distribution of the sample population shows that the majority of the sample
(over 50 percent) belonged to the age group 15-49 in both intervention and non-intervention
districts in two selected states. Population aged 6-14 years contributes nearly one in five across all
eight selected districts. The sex wise sample distribution shows higher proportion of males across
all eight districts. However, in Jharkhand, the proportion of female population in non-intervention
district is higher (46 percent) than to intervention district (48 percent).

Page | 29
The distribution of sample size by social group (caste) shows that the majority of
population belonged to the General/OBC categories in all eight selected districts, followed by
Scheduled Tribes (STs) except in non-intervention district of West Bengal. The sample distribution
in West Bengal shows higher proportion of ST population in intervention district (26 percent), as
compare with non-intervention district (5 percent). As far as the religious composition is concern,
majority were Hindus (71 percent). A considerable proportion of the sample was belonged to the
Muslim community (29 percent).
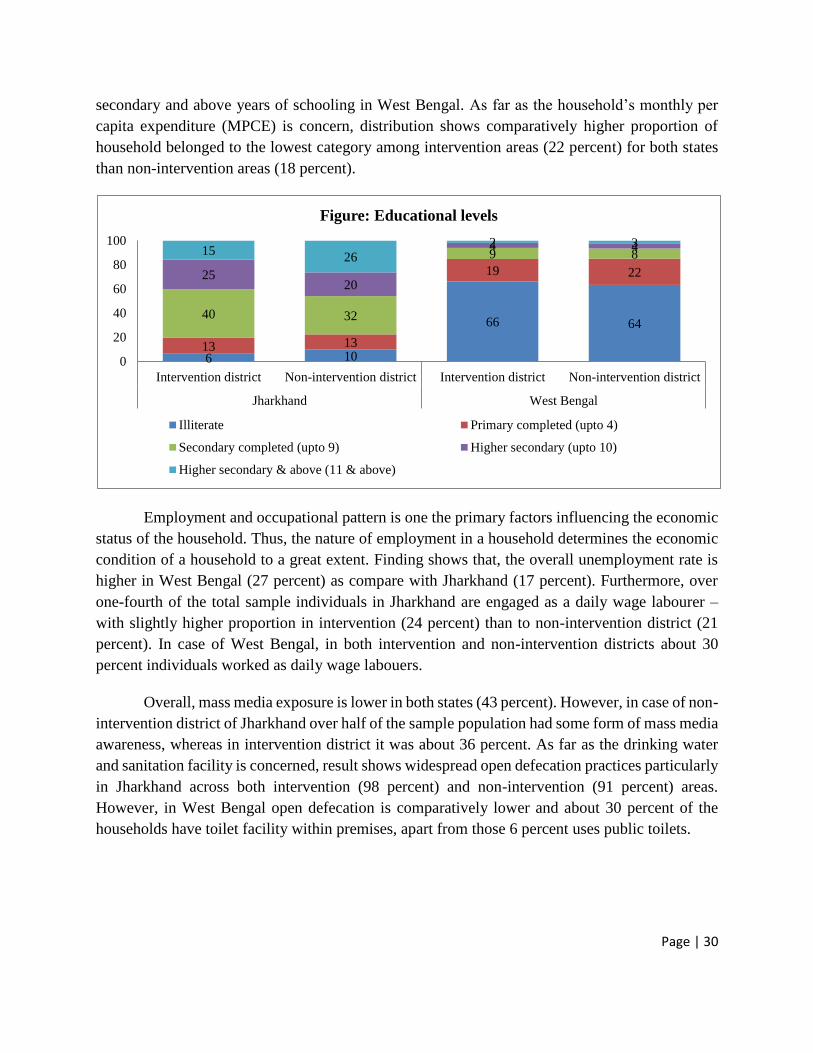
The distribution of sample population by education categories shows contrast picture
across two study states. For instance, in both intervention and non-intervention areas over three in
every five did not have any formal level of education. However, the corresponding figure in
Jharkhand is less than 10 percent. Moreover, about 15 percent in intervention and 26 percent in
non-intervention areas of Jharkhand had completed higher secondary and above years of
schooling. On the other side, less than 5 percent of the sample individuals had completed higher
58 53 6244
17 21 12 52
25 26 265
0
20
40
60
80
100
Intervention district Non-intervention district Intervention district Non-intervention district
Jharkhand West Bengal
Figure: Caste wise population distributaion
General/OBC Scheduled Castes Scheduled Tribes
7284
30
83
79
58
17217 12
0
0
20
40
60
80
100
Intervention district Non-intervention district Intervention district Non-intervention district
Jharkhand West Bengal
Figure: Religions composition
Hindu Muslims Sarna/Christians/Others
Page | 30
secondary and above years of schooling in West Bengal. As far as the household’s monthly per
capita expenditure (MPCE) is concern, distribution shows comparatively higher proportion of
household belonged to the lowest category among intervention areas (22 percent) for both states
than non-intervention areas (18 percent).
Employment and occupational pattern is one the primary factors influencing the economic
status of the household. Thus, the nature of employment in a household determines the economic
condition of a household to a great extent. Finding shows that, the overall unemployment rate is
higher in West Bengal (27 percent) as compare with Jharkhand (17 percent). Furthermore, over
one-fourth of the total sample individuals in Jharkhand are engaged as a daily wage labourer –
with slightly higher proportion in intervention (24 percent) than to non-intervention district (21
percent). In case of West Bengal, in both intervention and non-intervention districts about 30
percent individuals worked as daily wage labouers.
Overall, mass media exposure is lower in both states (43 percent). However, in case of non-
intervention district of Jharkhand over half of the sample population had some form of mass media
awareness, whereas in intervention district it was about 36 percent. As far as the drinking water
and sanitation facility is concerned, result shows widespread open defecation practices particularly
in Jharkhand across both intervention (98 percent) and non-intervention (91 percent) areas.
However, in West Bengal open defecation is comparatively lower and about 30 percent of the
households have toilet facility within premises, apart from those 6 percent uses public toilets.
6 10
66 64
13 13
19 22
40 32
9 8
2520
4 41526
2 3
0
20
40
60
80
100
Intervention district Non-intervention district Intervention district Non-intervention district
Jharkhand West Bengal
Figure: Educational levels
Illiterate Primary completed (upto 4)
Secondary completed (upto 9) Higher secondary (upto 10)
Higher secondary & above (11 & above)

Page | 31
3.2 Health status and healthcare services utilization
3.2.1 Morbidity and healthcare utilization
This section presents the morbidity prevalence, hospitalization and utilization of health
facility across intervention and non-intervention districts in two states. The survey asked number
of questions related with the different morbidities, illness, injuries, accidents etc. Survey further
asked type of healthcare use for each morbidity/illness. To understand the health needs of the
population including health insurance coverage, a glimpse of morbidity and hospitalization is
useful.
64
4955 59
36
5145 41
0
20
40
60
80
100
Intervention district Non-intervention district Intervention district Non-intervention district
Jharkhand West Bengal
Figure: Mass media exposure
No exposure Any exposure
16
9
12 11
Intervention district Non-intervention district Intervention district Non-intervention district
Jharkhand West Bengal
Figure: Overall Morbidity Prevalence (in%)

Page | 32
Results suggest higher morbidity prevalence (minor aliment during last 30 days) in
intervention areas of both states –Jharkhand (16 percent) and West Bengal (12 percent). This
clearly suggests that the healthcare needs and coverage of health insurance is comparatively higher
in intervention districts than to non-intervention. Further, finding shows considerable variations
by key socioeconomic characteristics in both intervention and non-intervention areas. For instance,
among all five educational categories, morbidity prevalence is considerably higher in intervention
area of Jharkhand, than to non-intervention. Respondents belong to the SC group has reported
higher morbidity rates in intervention areas (Jharkhand 24 percent; West Bengal 15 percent) as
compare with non-intervention areas (Jharkhand 9 percent; West Bengal 10 percent).
Except Muslims of the intervention area in West Bengal, morbidity prevalence is higher
across all religious categories in intervention areas of Jharkhand and West Bengal as compare with
intervention areas. Similarly, when comparing the household’s monthly per capita expenditure
(MPCE), finding shows higher morbidity prevalence in intervention districts than to non-
intervention, particularly in case of Jharkhand.
Table. Morbidity prevalence: Differentials across socioeconomic characteristics
Jharkhand West Bengal
Socioeconomic characteristics Intervention
District
Non-
Intervention
District
Intervention
District
Non-
Intervention
District
Sex Male 19.9 12.2 6.1 4.0
Female 12.0 5.6 4.6 3.3
Highest Education Level Illiterate 29.8 13.5 11.6 11.5
Primary completed (upto 4) 10.4 4.8 11.7 8.0
Secondary completed (upto 9) 11.0 9.9 9.4 18.6
Higher secondary (upto 10) 12.7 8.1 20.6 11.4
Higher secondary & above (11 & above) 3.2 7.6 3.9 4.0
Caste
General/OBC 16.7 10.1 9.2 12.7
Scheduled Castes 23.5 9.3 15.4 10.1

Page | 33
Scheduled Tribes 9.8 7.0 15.4 7.3
Religion Hindu 18.2 9.2 15.8 11.1
Muslims 16.3 11.5 8.5 11.4
Sarna/Christians/Others 9.2 4.5 15.7 0.0
MPCE
MPCE quintile 1 (Lowest) 7.9 3.6 8.7 6.5
MPCE quintile 2 12.3 7.0 8.8 8.1
MPCE quintile 3 16.1 8.0 11.6 11.1
MPCE quintile 4 22.4 9.4 15.1 15.4
MPCE quintile 5 (Higher) 24.2 18.1 14.6 17.0
As far as the type of healthcare visits for morbidity is concern, about half of the individuals
gone to informal providers (51 percent) in intervention area, followed by private facility (38
percent) in Jharkhand. However, in case of West Bengal over two-third had visited private
healthcare providers in intervention areas. It is important to note that considerably lower
proportion utilized public health facility across both intervention and non-intervention areas of
Jharkhand and West Bengal. This pattern further strengthens the evidence of heavily reliance of
majority of population in these areas on private and informal healthcare providers. In such
circumstances, household expenditure on healthcare could be higher.
3.2.2 Hospitalization
The hospitalization rate in the sample population is another key indicator that essentially
provides overall impression about the health insurance requirements. Survey asked in every
household whether any of the members hospitalized in last 365 (one year) days due to any illness
or accident. Results indicate that overall hospitalization rate is higher in Jharkhand (5.8 percent)
than West Bengal (4.4 percent). However, result did not fine considerable variations across
intervention and non-intervention areas in Jharkhand. But in West Bengal, hospitalization is
comparatively higher in intervention (5.3 percent) than non-intervention area (3.6 percent).

Page | 34
According to the different background characteristics, results show higher hospitalization
among STs in intervention districts across both states (Jharkhand 8 percent and West Bengal 5
percent). Similarly, in both study states and across all education categories, higher hospitalization
is reported among intervention than non-intervention districts. As expected, considerable
variations in hospitalization is evident by individuals age group. For instance, in case of Jharkhand
about 28 percent sample in intervention district aged 50-64 years were admitted in the hospital in
last one year, much higher than the non-intervention district (21 percent). Overall, irrespective of
the type of districts hospitalization is higher among male than female in both states.
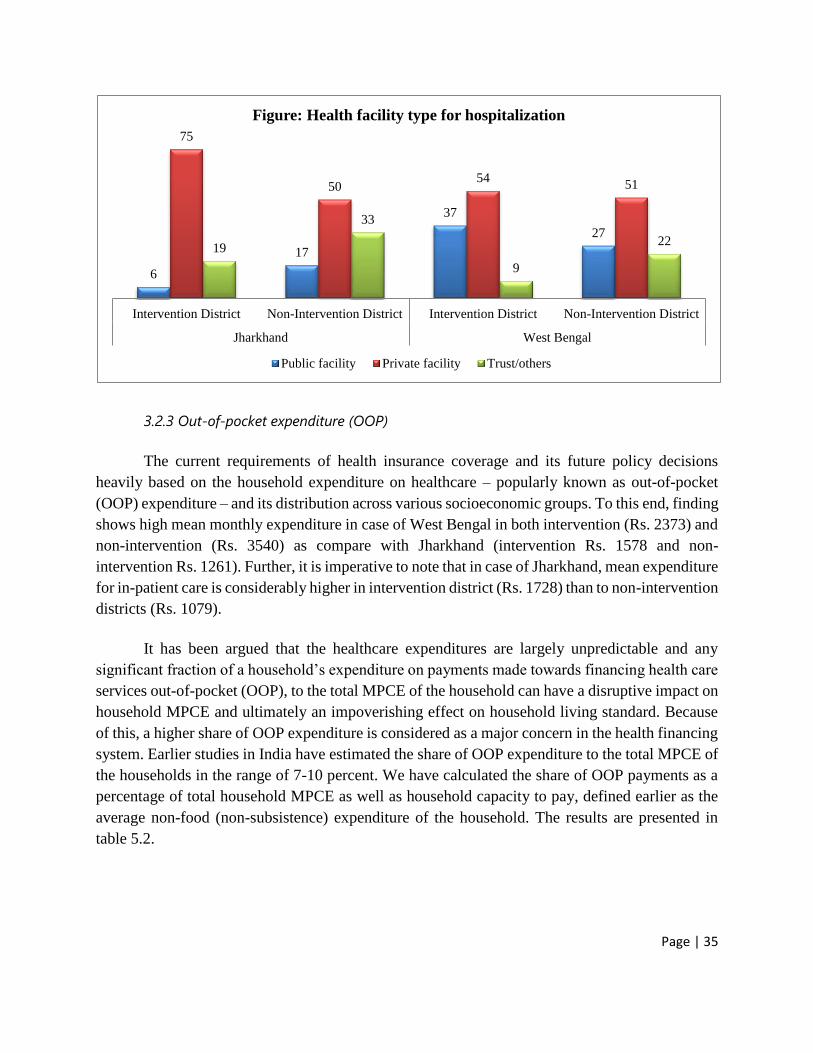
Finding suggests that in Jharkhand about three-fifth of the hospitalization utilized private
health facility, followed by trust/others (19 percent) in intervention district. Whereas, in case of
non-intervention district about half of the hospitalization cased utilized private health facility,
followed by trust/others providers (33 percent). Similarly, in case of West Bengal across both
intervention and non-intervention districts over half of the total hospitalization cases utilized
private health, followed by government health facility. Thus, the pattern empirically confirms
much lower use of public health facility for hospitalization in both states and elevated use of private
health facility. Furthermore, type of health facility use for the hospitalization by selected
socioeconomic characteristics does not show much variation. Like, in Jharkhand about 72 percent
lowest MPCE household gone for private health facility for hospitalization as compared with 85
percent among highest MPCE household in intervention area. Similarly, in the intervention area
of West Bengal, about half of the households belonged to the both top and bottom MPCE
categories opted private health facility for hospitalization.
5.56.0
5.3
3.6
Intervention district Non-intervention district Intervention district Non-intervention district
Jharkhand West Bengal
Figure: Hospitalization (in %)
Page | 35
3.2.3 Out-of-pocket expenditure (OOP)
The current requirements of health insurance coverage and its future policy decisions
heavily based on the household expenditure on healthcare – popularly known as out-of-pocket
(OOP) expenditure – and its distribution across various socioeconomic groups. To this end, finding
shows high mean monthly expenditure in case of West Bengal in both intervention (Rs. 2373) and
non-intervention (Rs. 3540) as compare with Jharkhand (intervention Rs. 1578 and non-
intervention Rs. 1261). Further, it is imperative to note that in case of Jharkhand, mean expenditure
for in-patient care is considerably higher in intervention district (Rs. 1728) than to non-intervention
districts (Rs. 1079).
It has been argued that the healthcare expenditures are largely unpredictable and any
significant fraction of a household’s expenditure on payments made towards financing health care
services out-of-pocket (OOP), to the total MPCE of the household can have a disruptive impact on
household MPCE and ultimately an impoverishing effect on household living standard. Because
of this, a higher share of OOP expenditure is considered as a major concern in the health financing
system. Earlier studies in India have estimated the share of OOP expenditure to the total MPCE of
the households in the range of 7-10 percent. We have calculated the share of OOP payments as a
percentage of total household MPCE as well as household capacity to pay, defined earlier as the
average non-food (non-subsistence) expenditure of the household. The results are presented in
table 5.2.
6
17
37
27
75
5054
51
19
33
9
22
Intervention District Non-Intervention District Intervention District Non-Intervention District
Jharkhand West Bengal
Figure: Health facility type for hospitalization
Public facility Private facility Trust/others

Page | 36
The socioeconomic disparity in household OOP is also evident. For instance, in Jharkhand
mean monthly OOP expenditure on health is equal among General/OBCs and household belonged
to the SCs categories. However, it is well known fact that the income gap between these two social
groups has been enormous, particularly in northern and eastern states of India, including
Jharkhand.
The extent of the absolute financial burden on the households on account of the out-of-
pocket expenses on healthcare can be examined by studying the proportional share of these
expenses to the total MPCE expenditure of the households. For the study population as a whole,
we find that on average about 25 percent of the total MPCE expenditure, is spent for
healthcare services in intervention districts across both the states. The figures indicate a
considerable share almost one-fourth of the total non-food expenditure of households is committed
towards the treatment of ailing members, exerting substantial financial burden on the households.
Moreover, the impact is not uniform; it rather differs according to the socioeconomic status of the
households. There are striking differences in the percentage share, when the population is viewed
in terms of socioeconomic status.
As seen from the table below, households belonged to the ST social group in intervention
district of Jharkhand spent 34 percent, in terms of the percentage share of mean out-of-pocket
expenditure to household MPCE expenditure. Further, in both intervention and non-intervention
districts of Jharkhand and West Bengal, he percentage share of mean out-of-pocket expenditure to
household MPCE expenditure is substantially higher among illiterate as compare with those who
had completed higher level of schooling.
Table: : Mean Out of Pocket Expenditure (OOPE) and percentage share of OOPE of total Household
expenditure, according to selected Household Attributes
1512 1453
2642
4120
1728
1079
19072317
15781261
2373
3540
Intervention District Non-Intervention District Intervention District Non-Intervention District
Jharkhand West Bengal
Figure: Mean monthly health expenditure (in Rs.)
Out-patient In-patient Total

Page | 37
Jharkhand West Bengal
Socioeconomic characteristics Intervention
District
Non-
Intervention
District
Intervention
District
Non-
Intervention
District
Highest Education Level
Illiterate 26.4 28.1 29.0 31.7
Primary completed (upto 4) 29.0 16.6 25.2 22.1
Secondary completed (upto 9) 27.1 21.3 27.3 16.5
Higher secondary (upto 10) 20.9 21.4 18.1 30.7
Higher secondary & above (11 & above) 22.4 21.4 23.0 28.1
Caste
General/OBC 23.2 22.9 25.3 26.3
Scheduled Castes 33.8 16.8 23.1 23.2
Scheduled Tribes 21.5 21.9 26.9 26.4
Religion
Hindu 26.3 22.1 24.1 23.2
Muslims 25.9 22.8 25.8 34.0
Sarna/Christians/Others 18.5 12.0 28.4
MPCE
MPCE quintile 1 (Lowest) 23.8 14.8 18.9 24.3
MPCE quintile 2 21.0 20.2 22.4 22.2
MPCE quintile 3 19.2 23.0 26.3 23.5
MPCE quintile 4 28.5 19.7 25.6 26.4
MPCE quintile 5 (Higher) 31.1 25.8 31.8 26.8
Total 24.9 21.5 25.6 24.9
4. RSBY: Awareness, Coverage and Utilization
4.1 PACS interventions in two selected states: A brief

Page | 38
Prior to study results, it would be important to briefly describe the key strategies or
interventions conducted by PACS in two selected states for this study – Jharkhand and West
Bengal. It has been acknowledge by many experts that boosting awareness, increasing enrolment
and encouraging people to use schemes like RSBY require multi-sectoral approach. Moreover,
ensuring proper coordination and synergies across different actors both government and non-
government involved directly or indirectly is indispensable towards achieving the desirable goals
for any programmes. A detailed description of the intervention types along with its description and
target population is mentioned below. It is worth to note the few interventions could be conducted
in both states.
Intervention Types Description of interventions Target group/audience
JHARKHAND
Stakeholder
sensitization
To create a buy in among community level
stakeholders for RSBY and activate
community level channels of communication
1. Panchayat members and urban
functionaries
2. Hospital authorities
3. Representatives from insurance
companies, district administration and
civil society organisation
Exposure visits More than 1900 members from community
based organisations (CBOs) are taken for
exposure visit to RSBY empanelled hospitals
which are conducted across Jharkhand
Community Based Organisations
(CBOs)
Jharkhand Mahila
Samakhya Society
The objective to expand the outreach of the
scheme to more women from socially
excluded groups
Monthly meetings of JMSS
District
Consultations
District level meetings with insurance
companies are being conducted for getting
information on enrollment and extending
support during enrollment
Insurance companies
IEC activities 1. Rallies, street plays, wall writings,
community radio shows, home visits, health
camps and mass level religious ceremonies;
2. Jingles are being used to raise the
awareness
Community
Special RSBY
enrolment stations
CSO have supported enrollment teams during
enrollment in naxal affected areas
Naxal affected areas
District Review
Committees (DRC)
It has been mandated that these committees
would monitor the RSBY progress in terms
of enrolment, hospital empanelment and IEC
through regular weekly meetings
PACS, insurance companies and
empanelled hospitals in presence of
DKM

Page | 39
RSBY Impact
Assessment study
Teams during enrollment in naxal affected
areas
PACS & Partner organisations
RSBY Mitra
initiative
A community cadre on RSBY has been
initiated.
Community
WEST BENGAL
Capacity building District level capacity building programme
for community mobilisers were organised in
West Bengal in which 100 community
mobilisers were given training on RSBY.
Awareness
meetings
Making communities aware about scheme
through them and inculcating positive health
seeking behaviour
School teachers and students
RSBY Enrolment
stations
Advocacy for setting up of enrolment stations
at places which can be accessed easily by
communities
Village level
IEC activities 1. Local folk shows, tableau, wall writing and
awareness camps during religious ceremonies
to raise the motivation of communities;
2. Four booklets on FAQs on RSBY
3. Poster depicting steps of hospitalisation;
4. Leaflet and poster on RSBY enrolment;
5. Home visits and community level radio
shows;
6. Mass level religious ceremonies;
7. Distribution of pamphlets and leaflets
Community facilitators and CBO
members
District
Consultations
Key issues related to RSBY implementation
at field level have been shared with district
administration by CBO and CSO members
CBO's and CSO's
RSBY Impact
Assessment study
The aim to assess the initiatives of PACS and
its partbers on RSBY in better uptake of
services and in creating space for civil society
in RSBY scheme
PACS & Partner organisations
RSBY Technical
assistance manual
and Policy Brief
Technical assistance manual on RSBY which
would provide road map to state government
as well as CSO's to implement RSBY in
partnership mode
State level and CSO's
Hospital
Sensitization
meetings
Conducted with hospital staff and authorities
to sensitize them on providing discrimination
free access to health facilities to socially
excluded communities
Hospital staff and authorizes
4.2 RSBY in Jharkhand & West Bengal: An overview

Page | 40
This section provides key features of RSBY scheme in two study states, that main includes
district wise enrolment under scheme, hospitalization and overall expenditure. The performance
of the scheme is being considered from the perspective of the government as an implementing
authority, and the BPL households as beneficiaries. Enrolment and conversion ratios7 are used to
analyse the performance of RSBY from the point of view of the government, and the conversion
ratio is the ratio of targeted to enrolled beneficiaries. This measures how effectively RSBY scheme
was able to identify and enroll targeted beneficiaries. Below mentioned estimates and figures are
not based on the present study, rather obtained from the RSBY MIS data collected from respective
states health society websites (Statistical Appendix 1 & 2).
In case of Jharkhand, the overall conversion ratio of the state is 51%. However, district
wise pattern suggests considerable disparity – from lowest in Deoghar (29%) to highest in Giridih
(68%). Out of 24 districts, about 8 districts had a conversion ratio below 50%. On the other hand
nearly 8 districts in Jharkhand observed conversion ratio above 60%. The conversion ratio for
West Bengal is 55%, with Bankura toppled (85%) across all 19 districts. The lowest conversion
ratio was observed in Darjiling (24%), followed by Howrah (36%).
The hospitalization ratio8 is used to measures the percentage of policy holders who claim
benefits under RSBY. It reveals the actual use of the scheme. It is important to note that while
considering hospitalization cases, multiple claims are not included. Estimates from Jharkhand
shows overall hospitalization ratio at 0.6%, much lower than the West Bengal (5.5%). Further, out
of 24 districts of Jharkhand, only four districts namely Dhanbad (3.8%), Lohardaga (2.7%),
Bokaro (1.4%) and Deoghar (1.1%) have a hospitalization ratio above 1%. Moreover, in nearly 13
districts in Jharkhand have a hospitalization ratio below 0.5%. The district wise pattern in
hospitalization ratio across 19 districts of West Bengal suggests vast disparity. For instance,
hospitalization ratio in Jalpaigudi and Birbhum is over 10%, whereas the ratio is as low at 0.1%
and 0.6% in Dakshin Dinajpur and Kolkata respectively.
4.3 Awareness
4.3.1 Overall awareness of RSBY scheme
7 𝐶𝑜𝑛𝑣𝑒𝑟𝑠𝑖𝑜𝑛 𝑅𝑎𝑡𝑖𝑜 =Enrolled
Targetedx100
8 𝐻𝑜𝑠𝑝𝑖𝑡𝑎𝑙𝑖𝑧𝑎𝑡𝑖𝑜𝑛 𝑅𝑎𝑡𝑖𝑜 =
Hospitalized cases
Enrolledx100

Page | 41
Awareness about a scheme is vital for its effectiveness. RSBY incorporates in its
procedural definition the spreading of information with the purpose of increasing awareness and
knowledge about the same. Awareness about RSBY includes information about one’s eligibility,
process of enrolment, and benefits of the scheme. The survey asked range of questions related to
RSBY awareness including whether respondent heard about the scheme, specific information
related with benefits available under the RSBY scheme, source of awareness etc.
Finding of this study reveals huge inter-state variations in overall awareness of the RSBY
scheme. For instance, in West Bengal less between 24-27 percent were aware about the RSBY
scheme in both intervention and non-interventions areas. On the other hand, over 90 percent
respondents in intervention districts of Jharkhand had said that they knew about the scheme.
However, the proportion in case of non-intervention district is low at 82 percent, but still it is one
and half times higher to the West Bengal.
Awareness about RSBY scheme does not vary uniformly across key socioeconomic
characteristics of the population within districts and across intervention and non-intervention
areas. In both states, finding shows higher level of awareness about RSBY scheme in intervention
districts as compare with the non-intervention. For example, in case of West Bengal about 40
percent of illiterate respondents in intervention district told that they were aware of the RSBY
scheme. However the corresponding figure among illiterate in non-intervention district of West
Bengal is less than 25 percent. The different in RSBY awareness does not restrict to the illiterate.
Moreover, in non-intervention area of West Bengal, about 26 percent of the higher educated
respondents aware of RSBY scheme – much below than the intervention areas, where about half
of the respondents completed higher education were aware about the scheme.
94
82
24 27
Intervention district Non-intervention district Intervention district Non-intervention district
Jharkhand West Bengal
Figure: Overall awareness of RSBY scheme (in%)
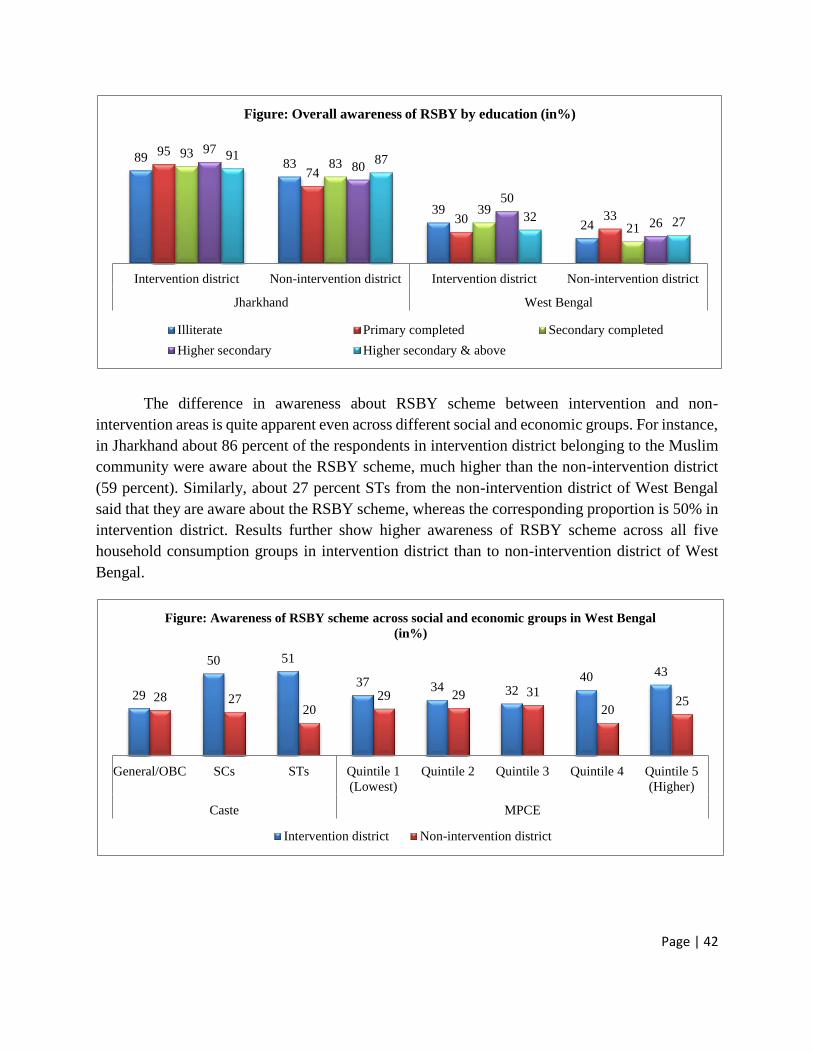
Page | 42
The difference in awareness about RSBY scheme between intervention and non-
intervention areas is quite apparent even across different social and economic groups. For instance,
in Jharkhand about 86 percent of the respondents in intervention district belonging to the Muslim
community were aware about the RSBY scheme, much higher than the non-intervention district
(59 percent). Similarly, about 27 percent STs from the non-intervention district of West Bengal
said that they are aware about the RSBY scheme, whereas the corresponding proportion is 50% in
intervention district. Results further show higher awareness of RSBY scheme across all five
household consumption groups in intervention district than to non-intervention district of West
Bengal.
8983
39
24
95
74
30 33
9383
39
21
97
80
50
26
91 87
32 27
Intervention district Non-intervention district Intervention district Non-intervention district
Jharkhand West Bengal
Figure: Overall awareness of RSBY by education (in%)
Illiterate Primary completed Secondary completed
Higher secondary Higher secondary & above
29
50 51
37 34 3240 43
28 2720
29 29 31
2025
General/OBC SCs STs Quintile 1
(Lowest)
Quintile 2 Quintile 3 Quintile 4 Quintile 5
(Higher)
Caste MPCE
Figure: Awareness of RSBY scheme across social and economic groups in West Bengal
(in%)
Intervention district Non-intervention district

Page | 43
4.3.2 Depth of awareness
It is important to note that for the schemes like RSBY, its awareness could not be judged
alone based on the basic awareness or if anyone just heard about the name. Since, the entire
enrolment process and its proper utilization require in-depth knowledge including eligibility, date
and venue of enrolment, knowledge about empanelled health facility and type of care covered
under the scheme. Thus, considering this aspect, the survey asked range of questions related with
the specifics of schemes.
Overall, finding of this study shows higher awareness regarding different specific
components of RSBY in intervention district as compare with non-intervention district,
particularly in case of Jharkhand. For instance, about 88 percent respondents are aware about the
eligibility criteria of RSBY scheme, while the corresponding figure is 76 percent in case of non-
intervention district. Results further shows nearly 55 percent respondents in non-intervention
district knew that Rs. 30,000/- could be spend in a year for hospitalization. On the other hand about
73 percent respondents from intervention district had the knowledge of maximum amount that can
be spend on hospitalization per year. In case of West Bengal, finding does not show any promising
difference in awareness about specific components of RSBY scheme between intervention and
non-intervention districts.
Difference in awareness about the specific components of the RSBY scheme by key
socioeconomic groups across intervention and non-intervention districts is quite apparent in
Jharkhand. Results shows across castes and religious groups, awareness of the maximum amount
one can spend per year on hospitalization is higher in intervention district as compare with non-
intervention. For example, in non-intervention district about 57 percent respondents belonged to
70 6585
72
43
87
56 58 49 57
30
59
Gen
eral
/OB
C
SC
s
ST
s
Hin
du
Mu
slim
s
Sar
na/
Chri
stia
ns/
Oth
ers
Caste Religion
Figure: Awareness of maxmium amount per year paid under RSBY scheme in
Jharkhand (in%)
Intervention district Non-intervention district

Page | 44
the STs knew about the maximum amount that can be utilized for hospitalization in a year under
RSBY scheme, whereas the corresponding proportion is 72 percent in intervention district.
Similarly, respondents from the Muslim and others religion have much higher level of awareness
of the maximum amount per year available under RSBY scheme in intervention area than to
respondents from the non-intervention district.
4.3.3 Sources of awareness
In terms of main sources of awareness, finding shows that in intervention districts of both
selected states, substantial proportion of respondents got to know about the RSBY scheme from
the PACS initiated activities. For instance, about 38 percent of the respondents reported RSBY
Mitra as the main source in Jharkhand. Apart from RSBY Mitra, respondents from intervention
districts also got to know about the RSBY scheme either through local teachers/ASHA or
Anganwadi workers. Fewer respondents also reported that they came to know about the RSBY
scheme from friends (19 percent) or through TV/radios (6 percent). On the other hand, in non-
intervention district over half of the respondents reported local teachers/ASHA/Anganwadi
workers (64 percent) and family/friends (31 percent) as the main sources from whom they got to
know about the RSBY scheme.
Results further suggest high reach of RSBY Mitras among marginalized sections of society
including STs and poor. For example, in Jharkhand over 60 percent of respondents belonging to
the STs and poorest MPCE quintile in intervention district reported RSBY Mitra as the main
source of information related to the RSBY scheme.
19
52
38
6
36
64
8 5
24 26
55
917
42
4 7
Friends/
Relatives/
Neighbours
Teacher/
Panchayat/
ANM/ AWW
PACS Mitra/
Mobilizer
TV/ Radio/
Others
Friends/
Relatives/
Neighbours
Teacher/
Panchayat/
ANM/ AWW
SHG/ NGO TV/ Radio/
Others
Intervention district Non-intervention district
Figure: Sources of awareness about RSBY scheme (in %)
Jharkhand West Bengal

Page | 45
In West Bengal, the most sited source of RSBY awareness is from the different means of
campaigns conducted by PACS, in case of intervention. However, the main point the need to
highlight in case of West Bengal is higher reach of PACS supported mass-media campaign in
intervention district (55 percent) than the mass-media campaign conducted by other organizations
in non-intervention district
(43 percent). Further, it is also interesting to note that the mass-media campaign led by PACS in
intervention district have a higher reach across all social and economic groups as compare with
mass-media campaign conducted by other organizations in non-intervention district.
4.4 Enrolment
4.4.1 Coverage of RSBY scheme
Enrolment is the first step towards the utilization of the scheme. It is at this stage that the
beneficiary enters the periphery of RSBY scheme. We have found earlier considerable inter-state
and intra-state disparity in overall awareness of the RSBY scheme along with disparity in specific
components of the scheme. However, in case of enrolment results do not show many variations in
enrolment of the RSBY scheme across all eight selected districts in both states. For instance, in
both states across intervention and non-intervention districts over 80 percent of the households
enrolled in RSBY scheme. The high coverage of RSBY scheme in all eight selected districts could
be explained in terms of overall study design of the entire study. Since, this study design heavily
depends up on households enrolled under RSBY scheme to examine the entire process of RSBY
scheme including experiences during enrolment, utilization etc. In addition, for both states the
conversion ratio (mentioned earlier) of the RSBY scheme is over 50 percent, with many districts
48 52
77
59 5766
44
64
4045
52 5243 43
39 40
General/OBC SCs STs Quintile 1
(Lowest)
Quintile 2 Quintile 3 Quintile 4 Quintile 5
(Higher)
Caste MPCE
Figure: Reach of mass media compagin in West Bengal (in%)
Intervention district Non-intervention district

Page | 46
lies between 60-80 percent. Thus, it is not surprising to have enrolment rates in eight selected
districts is considerably higher.
Table: Enrolment of households under RSBY scheme by selected socioeconomic characteristics
Jharkhand West Bengal
Background Characteristics Intervention
District
Non-Intervention
District
Intervention
District
Non-Intervention
District
Highest education level in HH
Illiterate 84.2 86.2 80.7 90.7
Primary completed 87.2 86.8 89.1 84.7
Secondary completed 83.3 87.2 81.9 85.2
Higher secondary 89.0 79.7 83.3 84.5
Higher secondary & above 84.8 83.3 70.0 84.4
Caste (HH)
General/OBC 83.2 86.8 82.3 82.1
Scheduled Castes 87.8 87.1 77.8 89.7
Scheduled Tribes 89.3 77.9 87.7 85.7
Religion (HH)
Hindu 86.0 85.5 84.9 87.9
Muslims 76.2 81.5 82.2 78.9
Sarna/Christians/Others 87.1 77.3 83.3 75.6
MPCE
MPCE quintile 1 (Lowest) 90.9 84.9 79.4 90.5
MPCE quintile 2 91.5 83.3 85.7 88.4
MPCE quintile 3 82.5 89.3 82.0 82.4
MPCE quintile 4 80.0 84.1 86.4 87.1
MPCE quintile 5 (Higher) 81.4 81.7 82.8 82.8
Total 85.5 84.6 83.2 86.2
4.4.2 Source of motivation
Present study also attempted to assess the possible sources that encourage enrolment under
the RSBY scheme. Finding suggests higher motivation from the local teachers/ASHA or panchayat
members towards enrolment of the scheme across both intervention and non-intervention districts
in both states. In case of non-intervention districts, followed by local teachers/ASHA or panchayat,
friends and relatives played key role towards enrolment. However, in case of intervention districts,
PACS interventions such as RSBY Mitra in Jharkhand and other PACS supported community
mobilizes in West Bengal encouraged households to enroll under this scheme. Here, once again as
reflected in case of awareness, substantial higher percentage (66) of STs in intervention district of
Jharkhand reported RSBY Mitra as the main source of motivation behind enrolment under RSBY
scheme.

Page | 47
4.4.3 Help during enrolment processes
The entire enrolment process of RSBY scheme is very complicated and requires all
documents ready for the enrolment day. Since, in majority of cases the entire enrolment process
for a village or group of villages takes place in single day, prior information including venue of
enrolment, require documents, presence of desire number of family members along with head of
the households quite vital. In many cases, the refusal rates are very high due to lack of proper
guidance prior and during enrolment process. Thus, in that case appropriate and timely guidance
is one of the key dimensions of entire RSBY scheme to ensure high enrolment rates.
Finding shows that in non-intervention districts majority of respondents said nobody
helped them during the enrolment process – Jharkhand (92 percent) and West Bengal (59 percent).
However, in case of intervention districts about 63 percent of the respondents in Jharkhand and 38
percent in West Bengal informed that nobody extended any kind of support during the enrolment
process. It is important to note that in case of West Bengal across both intervention and non-
intervention districts, local political leaders or workers quite often extended their support in these
kind of schemes design for marginalized sections of society. However, such kind of political
awareness or initiatives lacking in other eastern Indian states, including Jharkhand. Moreover,
results clearly revealed that in intervention districts, about 31 percent respondents in Jharkhand
and 23 percent in West Bengal reported PACS initiatives interventions such as Mitra (in
Jharkhand) and other community mobilizers (particularly in West Bengal) helped they during
RSBY enrolment process. It is also important to note that across all eight intervention and non-
intervention districts, respondents unanimously said they did not get any help during the enrolment
process from the smart card providers.
7
34
51
37
2 412
4757
7 3 228 9 8 4 4 2 5
16
211
1
Sel
f
Fri
end
s/ r
elat
ives
Tea
cher
/ A
SH
A/
Pan
chay
at
RS
BY
-Mit
ra/
Mo
bil
izer
s
Po
liti
cal
lead
er
Oth
ers
Sel
f
Fri
end
s/ r
elat
ives
Tea
cher
/ A
SH
A/
Pan
chay
at
NG
Os/
SH
Gs
Po
liti
cal
lead
er
Oth
ers
Intervention District Non-Intervention District
Figure: Source of motivation (in%)
Jharkhand West Bengal

Page | 48
The comparison between interventions districts in both states in terms of help
provided during the enrolment process by selected socioeconomic characteristics of sample
population, suggest considerable variations. Overall, PACS led initiatives have higher reach in
Jharkhand than to West Bengal by major background characteristics. However, across religious
groups, finding identified one exception in Jharkhand where none of the Muslim respondent
reported PACS led initiatives helped them during the entire enrolment process. Nevertheless, in
many cases Jharkhand figure shows much promising results than in West Bengal. For example,
only 6 percent illiterate respondents said they received help from PACS led community mobilizers
during enrolment process in West Bengal, as against 38 percent reported support from PACS led
initiatives (mainly RSBY Mitra) in Jharkhand.
Finding further shows respondents belonged to the STs group in Jharkhand reported
considerably higher support received from the PACS supported initiatives during enrolment
process (59 percent), than to West Bengal (33 percent). It appears from the results that the PACS
led initiatives have a higher reach among poor during enrolment process in Jharkhand than to West
Bengal. For example, about 40 percent respondents from the poorest MPCE quintile said that they
received some kind of support from the PACS led initiatives during the enrolment process.
However, the corresponding figure in case of West Bengal is about 30 percent among poorest
MPCE quintile who reported support extended from the PACS led interventions during enrolment.
1
31
63
5 0 1
92
75
23
3844
5 2
59
35
Smart card
provider
PACS
Interventions
Nobody Others Smart card
provider
NGOs/SHGs Nobody Others
Intervention District Non-Intervention District
Figure: Helped during enrolment process (in%)
Jharkhand West Bengal

Page | 49
Table: Helped during RSBY enrolment process in intervention districts according to key background
characteristics
Jharkhand West Bengal
Background Characteristics PACS
Interventions
Nobody Others PACS
Interventions
Nobody Others
Highest education level in HH
Illiterate 37.5 56.3 6.3 5.6 44.4 55.6
Primary completed 31.4 65.7 2.9 24.0 40.0 40.0
Secondary completed 21.0 73.3 4.8 25.0 37.5 50.0
Higher secondary 42.4 54.6 0.0 50.0 25.0 25.0
Higher secondary & above 36.6 51.2 12.2 33.3 33.3 33.3
Caste
General/OBC 21.7 73.7 4.0 13.2 42.1 50.0
Scheduled Castes 20.9 79.1 0.0 40.0 40.0 40.0
Scheduled Tribes 58.8 29.4 8.8 33.3 33.3 36.7
Religion
Hindu 22.4 71.9 5.2 40.0 30.0 43.3
Muslims 0.0 100.0 0.0 11.4 45.7 42.9
Others 70.9 21.8 3.6 12.5 37.5 50.0
MPCE
MPCE quintile 1 (Lowest) 39.3 44.3 11.5 0.0 30.0 55.0
MPCE quintile 2 45.5 50.9 3.6 7.7 53.9 30.8
MPCE quintile 3 29.1 69.1 1.8 21.4 35.7 42.9
MPCE quintile 4 14.6 82.9 2.4 30.0 25.0 40.0
MPCE quintile 5 (Higher) 21.6 76.5 2.0 43.8 43.8 43.8
4.4.4 Post enrolment visit for detailed information
Apart from the detailed information prior to and during enrolment process, in-depth and
accurate information is needed to every household about the benefits of the scheme including,
amount available per year for hospitalization, name and location of the empanelled hospitals,
process at health facility and other benefits like transportation allowances etc. In many cases it has
been observed that households enroll in the schemes but inadequately informed about the benefits
of the scheme which ultimately led to the underutilization of schemes. Thus, the present study
asked household whether anyone visited your home after the RSBY enrolment completed to
inform you about the benefits of the scheme.
Finding of this survey clearly suggest absence of any kind of post enrolment household
visits in all four non-intervention districts in both states. For instance, nearly all sample household
(98 percent) in two non-intervention districts of Jharkhand reported no visit by anyone after the
enrolment procedure of RSBY scheme. However, in case of West Bengal about 35 percent of the

Page | 50
household visited by someone after the enrolment process, most possibly either by some panchayat
member or by ASHA worker in non-intervention areas. On the other hand, across all four
intervention districts in both states, nearly 30 percent of the household were visited by PACS
related community mobilizes in Jharkhand, compared to 23 percent in case of West Bengal.
Further, results suggest higher percentage of households belonging to STs were visited by
PACS led community mobilizes in Jharkhand (63 percent). Even, 46 percent of the respondents
who are illiterate in intervention districts of Jharkhand said that PACS supported community
mobilizes visited their household after the enrolment to inform about the different benefits that
one could receive from the RSBY scheme. However, the overall pattern suggest that PACS led
community mobilizes have a higher reach to the households in Jharkhand than to West Bengal,
particularly among marginalized sections including STs, illiterate and poor.
4.5 Utilization
One of the most essential indicators of assessing real coverage of any scheme, apart from
knowledge and enrolment is the utilization. Thus, in case of RSBY scheme, utilization of benefits
during hospitalization remains vital to gauge the real progress of the scheme, particularly among
marginalized sections of the population including STs, SCs, minorities and the poor. It is important
to mention here that the utilization rates of RSBY scheme is based on those household reported
hospitalization cases in last one year.
The use of RSBY scheme during hospitalization significantly varies across both the states.
Moreover, considerable variations are evident between intervention and non-intervention districts
in Jharkhand but not in West Bengal. To illustrate, in case of West Bengal higher use of RSBY
67
30
3
98
2 0
58
2328
61
5
35
Nobody PACS initiatives Others Nobody NGOs/SHGs Others
Intervention District Non-Intervention District
Figure: Post enrolment household visit (in%)
Jharkhand West Bengal

Page | 51
scheme is observed in non-intervention districts (26 percent) than the intervention districts (20
percent). However, on the other hand in Jharkhand over half of the households reporting
hospitalization in the sample has utilized RSBY scheme benefits in intervention areas, whereas the
use of RSBY scheme during hospitalization is 21 percent in non-intervention districts.
Finding suggests progressive utilization of RSBY benefits among
vulnerable/marginalized communities in Jharkhand. As far as the socioeconomic disparity
between intervention and non-intervention districts in uptake of RSBY scheme is concern,
finding suggests comparatively higher utilization in intervention districts of Jharkhand than
to non-intervention districts. For example, the use of RSBY scheme during hospitalization
among illiterates in intervention districts of Jharkhand is about 67 percent, whereas the
corresponding figure in non-intervention districts is 33 percent. Similarly just one in five
respondents from the ST group utilized scheme in non-intervention districts, much lower
than the STs of intervention districts (83 percent). The highest gap between intervention and
non-intervention districts in terms of use of RSBY scheme observed in case household
MPCE. For instance, just 6 percent households from the lowest MPCE category in non-
intervention areas utilized RSBY scheme during hospitalization, which is considerably lower
as compare with the intervention districts of 81 percent.
Results however, do not show similar promising comparative utilization pattern between
intervention and non-intervention districts of West Bengal. Except few, the RSBY utilization
pattern remains equal in majority of socioeconomic categories across intervention and non-
intervention districts. Like, in case of ST groups, the utilization of RSBY scheme during
hospitalization is higher in intervention districts (38 percent) than to non intervention districts (20
percent).
52.3%
20.9% 20.0%
25.6%
Intervention district Non-intervention district Intervention district Non-intervention district
Jharkhand West Bengal
Figure: Utilization of RSBY for hospitalization (in%)

Page | 52
Table: Utilization of RSBY scheme during hospitalization by selected socioeconomic characteristics
Jharkhand West Bengal
Background Characteristics Intervention
district
Non-
intervention
district
Intervention
district
Non-
intervention
district
Highest education level in HH
Illiterate 66.7 33.3 22.2 21.4
Primary completed 46.2 44.4 13.6 24.1
Secondary completed 44.0 20.8 23.8 18.8
Higher secondary 40.0 15.8 11.1 46.7
Higher secondary & above 80.0 14.3 30.0 12.5
Caste
General/OBC 45.2 16.7 15.1 27.0
Scheduled Castes 13.3 33.3 30.0 25.0
Scheduled Tribes 82.8 21.7 38.1 20.0
Religion
Hindu 44.3 17.1 30.8 23.9
Muslims 20.0 57.1 14.6 36.4
Sarna/Christians/Others 85.0 22.2 16.7 21.0
MPCE
MPCE quintile 1 (Lowest) 81.0 6.3 25.0 40.0
MPCE quintile 2 78.6 26.7 30.8 40.0
MPCE quintile 3 37.5 10.5 25.0 18.2
MPCE quintile 4 31.6 30.4 11.5 17.6
MPCE quintile 5 (Higher) 31.3 30.8 17.6 22.2
4.6 Effect of PACS interventions on awareness, enrolment and utilization of RSBY scheme:
Multivariate regression analysis

Page | 53
The net effect of PACS led interventions programmers in selected districts of Jharkhand
and West Bengal with aim of enhancing overall and specific awareness about the RSBY scheme,
along with increasing the utilization rates of the scheme during hospitalization requires application
to multivariate logistic regression analysis. The main purpose of logistic regression analysis
applied here to examine the net effect of awareness, and utilization in intervention districts, after
adjusting the effect of other key independent variables in the model.
4.6.1 Effect on overall and specific awareness of RSBY Scheme
In case of overall awareness about RSBY scheme is concern, result clearly shows higher
odds of awareness in intervention districts than to non-intervention districts in both the states.
However, the strength of association across two states differs but the direction remains positive.
To illustrate, in Jharkhand the likelihood of overall awareness about the RSBY scheme in
intervention districts is over three and half times higher as compare with non-intervention districts,
with statistical significant at 1%. On the other hand, in case of West Bengal, although the odds of
overall awareness of RSBY scheme is little more than twice higher in intervention districts
compare with non-intervention districts, this association statistically significant at 10%.
Table. Estimated odds ratio to examine the effect of PACS interventions on overall awareness of RSBY
scheme in Jharkhand and West Bengal
Independent variables Jharkhand West Bengal
Odds Ratio p-value Odds Ratio p-value
Education
Illiterate (ref.) 1.00 1.00
Primary completed 0.75 0.609 0.95 0.209
Secondary completed 0.91 0.847 0.83 0.204
Higher secondary 0.89 0.841 1.11 0.311
Higher secondary & above 0.87 0.802 0.76 0.257
Castes
General/OBC (ref.) 1.00 1.00
Scheduled Castes 1.03 0.940 0.87 0.204
Scheduled Tribes 0.74 0.409 1.19 0.379
Religion
Hindu (ref.) 1.00 1.00
Muslims 0.31** 0.002 0.45 0.126
Christians/Others 1.37 0.570 0.56 0.230
MPCE
MPCE quintile 1 (ref.) 1.00 1.00
MPCE quintile 2 1.37 0.484 0.99 0.252

Page | 54
MPCE quintile 3 1.15 0.753 0.88 0.225
MPCE quintile 4 0.83 0.650 0.79 0.206
MPCE quintile 5 (Higher) 1.04 0.931 0.92 0.235
Mass media exposure
No exposure (ref.) 1.00 1.00
Any exposure 1.62 0.113 1.46 0.249
District
Non-Intervention (ref.) 1.00 1.00
Intervention 3.40*** 0.000 2.16* 0.071
Ref.: Reference Category; Level of significance: * p<0.10, ** p<0.05, *** p<0.001
As far as the awareness of specific components of RSBY scheme is concern, out of six
different dimensions, regression results shows higher awareness of four components in
intervention districts than to non-intervention districts of Jharkhand. For instance, regression
analysis after adjusting other independent variables in the model shows over two time higher level
of awareness about amount available for one year under RSBY scheme for hospitalization in
intervention districts as compare with non-intervention districts of Jharkhand. Similarly, the odds
of awareness about the transportation allowance provided under RSBY scheme is nearly twice
higher in intervention districts than to non-intervention districts.
In case of West Bengal, none of the models show any statistical significant difference
between level of specific components of RSBY scheme between intervention and non-intervention
districts. Although, the direction of odds rations in case of all six specific domains remains positive
in case of intervention districts, but difficult to conclude due to lack of statistical power.
There are other independent variables which are significantly associated with the specific
knowledge about different domains. In particular, many specific awareness indicators significantly
influences by level of education and consumption expenditure of the household.

Page | 55
Table. Estimated odds ratio to examine the effect of PACS interventions on specific awareness of different components about RSBY scheme in Jharkhand
and West Bengal
Independent variables Awareness about
eligibility
No. of enrollment
member
Awareness
about
enrollment
expenses
How much
amount,
RSBY/year
Type of
treatment
provided under
RSBY
Awareness about
transportation
allowance
JH WB JH WB JH WB JH WB JH WB JH WB
Education
Illiterate (ref.) 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00
Primary completed 1.27*** 1.05*** 2.63** 0.83* 3.08* 0.47*** 1.00 0.58** 1.44 0.78*** 1.57 0.73***
Secondary completed 1.22 1.29 2.83** 0.84 2.17 1.04 1.16 0.72 1.89* 1.14 1.11 0.86
Higher secondary 2.41** 1.29 3.06** 0.87 1.77 1.82 2.43** 0.99 2.71** 0.88 1.39 1.15
Higher secondary & above 2.35** 1.15 3.64** 0.84 2.31 0.25** 2.65** 0.56 3.34** 0.40** 1.99 0.55
Castes
General/OBC (ref.) 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00
Scheduled Castes 1.03 1.41 1.49 0.84 0.55 2.07 1.04 0.90 1.05 0.97 0.69 0.70
Scheduled Tribes 0.65 0.62 0.54** 0.53** 0.67 0.73 0.69 0.67 0.72 1.04 1.02 1.42
Religion
Hindu (ref.) 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00
Muslims 2.04** 1.81** 1.20 1.17 0.59 1.17 0.39** 1.64 0.57* 1.16 0.64 0.68
Christians/Others 0.71 1.31 1.04 1.45 0.78 2.52 1.96* 1.04 1.77 0.60 2.10** 0.28
MPCE
MPCE quintile 1 (ref.) 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00
MPCE quintile 2 0.58 1.06 0.95 0.74 0.42* 0.13** 0.71 0.68 0.62 1.22 0.64 1.27
MPCE quintile 3 0.29*** 0.97 0.57 0.80 0.29* 0.11** 0.52 0.76 0.51** 1.19 0.46** 0.66
MPCE quintile 4 0.39** 1.15 0.64 0.94 0.22** 0.15* 0.46 0.92 0.46** 1.27 0.44** 0.20*
MPCE quintile 5 0.39** 1.37 0.47** 0.76 0.34* 0.08** 0.33 0.81 0.48** 0.85 0.39** 0.63
Mass media exposure
No exposure (ref.) 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00
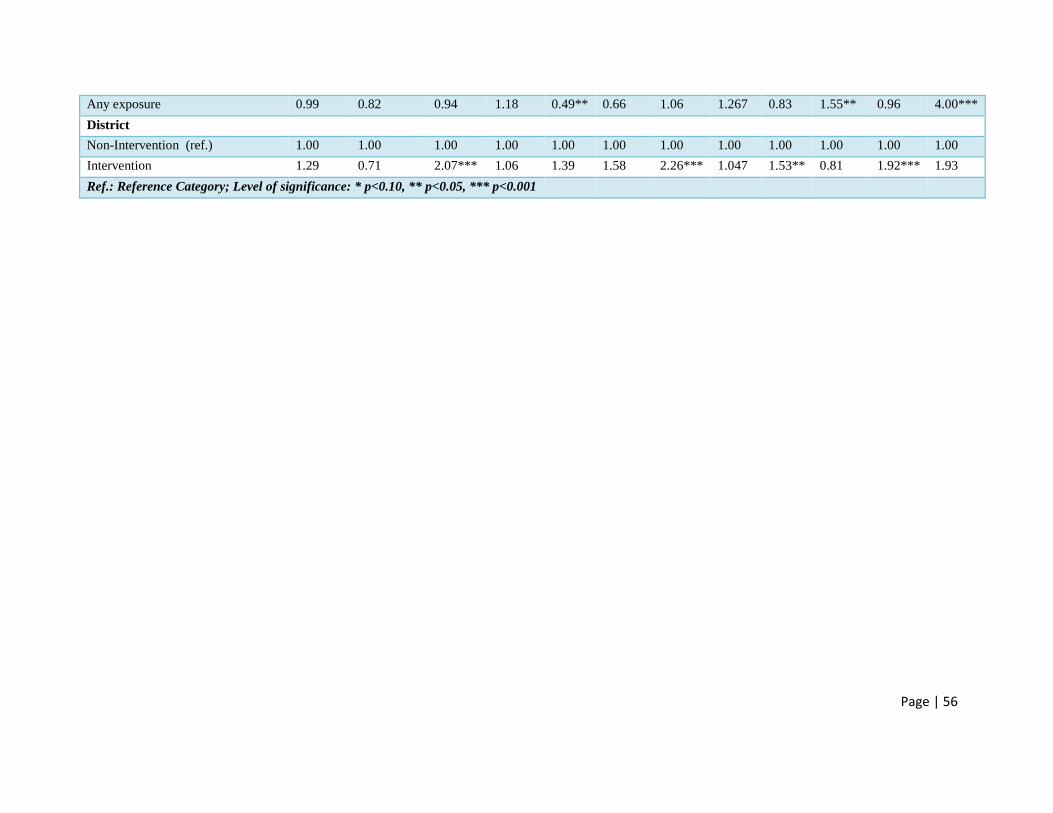
Page | 56
Any exposure 0.99 0.82 0.94 1.18 0.49** 0.66 1.06 1.267 0.83 1.55** 0.96 4.00***
District
Non-Intervention (ref.) 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00
Intervention 1.29 0.71 2.07*** 1.06 1.39 1.58 2.26*** 1.047 1.53** 0.81 1.92*** 1.93
Ref.: Reference Category; Level of significance: * p<0.10, ** p<0.05, *** p<0.001

Page | 57
4.6.2 Effect on utilization of RSBY scheme during hospitalization
As mention previously, utilization of scheme remains one of the key indicators that show
actual performance in any area or population. Thus, to examine whether districts covered under
PACS intervention programmes have higher utilization rates than the non-intervention districts,
we performed multivariate regression analysis by including other independent variables in the
model.
In Jharkhand, finding shows that the likelihood of RSBY scheme utilization for
hospitalization is nearly five times higher in intervention districts as compare with non-
intervention districts, with high statistical power at 1%. This pattern is quite expected since in
previous results including basic cross tabulation pattern with regard to awareness, enrolment, and
utilization has been fairly encouraging across intervention districts in Jharkhand.
However, in case of West Bengal the likelihood of RSBY scheme in intervention district
is lower than the non-intervention districts, but the association is very week. This association is in
continuation what the entire pattern suggested in previous sections about low level of performance
in various dimensions that the study covered, particularly in intervention districts of West Bengal.
Table. Estimated odds ratio to examine the effect of PACS interventions on utilization of RSBY scheme in
Jharkhand and West Bengal
Independent variables Jharkhand West Bengal
Odds Ratio p-value Odds Ratio p-value
Education
Illiterate (ref.) 1.00 1.00
Primary completed 0.90 0.913 0.63 0.475
Secondary completed 0.52 0.461 0.99 0.983
Higher secondary 0.51 0.471 1.27 0.749
Higher secondary & above 1.30 0.779 1.18 0.840
Castes
General/OBC (ref.) 1.00 1.00
Scheduled Castes 0.74 0.589 0.83 0.750
Scheduled Tribes 2.30 0.124 4.75* 0.062
Religion
Hindu (ref.) 1.00 1.00
Muslims 2.56 0.192 1.30 0.699
Christians/Others 1.40 0.584 0.40 0.466
MPCE
MPCE quintile 1 (ref.) 1.00 1.00
MPCE quintile 2 1.11 0.861 1.03 0.961

Page | 58
MPCE quintile 3 0.29* 0.044 0.43 0.216
MPCE quintile 4 0.56 0.282 0.27* 0.065
MPCE quintile 5 (Higher) 0.49 0.247 0.44 0.237
Mass media exposure
No exposure (ref.) 1.00 1.00
Any exposure 0.79 0.573 3.26** 0.009
District
Non-Intervention (ref.) 1.00 1.00
Intervention 4.73*** 0.000 0.32* 0.074
Ref.: Reference Category; Level of significance: * p<0.10, ** p<0.05, *** p<0.001

Page | 59
4.7 Findings from Qualitative Methods
The statistical analysis performed in previous sections may help us to understand the
current pattern, socioeconomic differences across districts in terms of overall awareness about
RSBY scheme, enrolment, and utilization for hospitalization care. Moreover, it also helps to
examine the net effect of difference in RSBY awareness, enrolment and utilization between
intervention and non-intervention districts in both states. However, when it comes to in-depth
understanding about the different process involved, functional constrains and dimensions that
difficult to capture in quantitative surveys, qualitative approach is needed. Thus, this study has
performed some focus group discussion along with in-depth interviews in intervention districts
across both states.
4.7.1 Finding from Focus Group Discussions (FGDs)
Key domains Jharkhand West Bengal
Effect of
PACS
interventions
on
Awareness
Overall awareness about the RSBY
scheme has increased over last few
months. Participants were anonymously
agreed that after RSBY Mitra infinitives
awareness about RSBY scheme has gone
up manifold. One participant from ST
community told that prior to the RSBY
Mitra, he did not know about the actual
benefit of the RSBY scheme.
In general participants told continuous
visit of RSBY Mitra in the village and
always try to search whether anyone in
case suffer for any illness in the
household must visit health facility along
with card.
It was also observed during the discussion
that majority of villagers did not know
previously about the empanelled hospitals
and transportation allowance covered
under the RSBY scheme.
Majority of respondents came to know
about the RSBY scheme during mother’s
day meeting held in Sahayata Kendra.
After the mother’s day meeting local
PACS community mobilizes took a
session on RSBY scheme.
During the meeting respondents were told
about the details benefits of the RSBY
scheme, along with the enrolment process.
Effect of
PACS
interventions
on
enrolment
During FGDs, the team member felt that
the enrolment under RSBY schemes
remain higher, since majority of
participants enrolled under the scheme
either in 2010 or 2011.
The overall enrolment rate is moderate, as
mentioned by majority of participants.
Although, in many cases participants
enrolled in the scheme in 2011, but never
used for any hospitalization.

Page | 60
and
enrolment
processes
It was also noticed that one of the main
huddle towards enrolment under the
RSBY scheme is older BPL list.
However, few two of the participants
from the ST community elaborated that
although her family name is not included
in the BPL lists but RSBY Mitra told
them to use their MNREGA job card for
the enrolment under the RSBY scheme.
Many respondents told that during last
enrolment in the village RSBY Mitra
contacted majority of family in the village
and told about the entire process including
essential documents needed, number of
family members that needs to be present,
enrolment timing and venue.
A major constraint towards enrolment in
the RSBY scheme that was highlighted
during FGDs is timing. As majority of
family works as a tea garden worker in
villages where normal timing is from
morning 8AM to evening 4-5 PM, they do
not find enough time to enroll.
Being asked, they replied that they were
denied leave grants for the day of
enrolment, even after the PACS local
community mobilizes discussed issue with
the employers regarding importance of the
scheme.
One of the participant recalled that the
enrolment process last time lasted up to 9
PM in the night, but due to huge rush she
could not enrolled.
Effect of
PACS
interventions
on
Utilization
One of the key observations that the study
team noticed during the FGDs is the high
level of RSBY scheme use during
hospitalization in recent months in the
community. Although, there are many
issues that remain significant for
restricting total utilization of scheme
which we will discussed in subsequent
sections.
Participants were unanimous about the
fact that in spite of high enrolment rates
for over three to four years they did not
see anyone from the community who used
this scheme during hospitalization.
Earlier they used to enroll in the scheme
as they were enrolling in other schemes
but nobody informed about its benefits.
However, two of the participants who
used this scheme recently for
hospitalization praise the help and kind of
support extended by RSBY Mitra in
obtaining this benefit.
They shared with us that since they never
visited any hospital facility, it was
impossible if RSBY Mitra did not
It was felt that the actual use of RSBY
scheme for hospitalization visits started
very recently in the village. Earlier people
used to visit health facility provided by tea
gardens to their employees. However,
limited health facility is available and
hospitalization facility in many cases not
available in these health facilities.
However, after the launch of RSBY
Sahaya Kendra majority of participants
came to know about the lists of
empanelled hospitals.
Moreover, one of the participants who
knew about the scheme earlier was
refused by the empanelled hospital. But
once he came to know through the
Sahayata Kendara that the same hospital
cannot refuse, since it is one of the
empanelled hospitals he went again and
utilized RSBY scheme for in-patient care.

Page | 61
accompany them to the health facility. It
was due to the RSBY Mitras continues
visits to the family and motivations that
helped them to use hospital facility.
Overall
Impact
Overall, participants who themselves
utilized RSBY scheme for in-patient care
and those who interacted with their
friends and neighborhood benefited from
the scheme categorically registered many
benefits that are mentioned below:
- Better health facility in hospitals
- No economic burden on family
- Early cure due to proper check-ups
and continuous monitoring during
hospitalization
- Many used to sell their animals and
land for high cost of hospitalization
which stopped completely
- High level of Malaria presence each
year cause heavy burden in terms of
financial loss of household, which
has reduced substantially this year.
The participants were not very firm to
comment on the impact of RSBY scheme.
This could be due to the fact that very
little hospitalization rate observed in
villages. One respondent that used RSBY
scheme for eye operation however told
that in absence of RSBY scheme it was
impossible for him to undergone this
operation due to low income.
Constraints There are many issues that was raised
during the discussion ranging from need
of up gradation of BPL lists, distance to
nearest empanelled hospital, loss of
income for additional member who
accompany to the patient, poor quality of
food served in hospitals etc.
One major issue that was raised during
the discussion is the unavailability of
costly medicine in the hospitals for which
people bound to buy from outside.
One of the main constrains that was
highlighted during the discussion was lack
of timing and non-cooperation from the
tea garden authorities during enrolment.
The other main issue was the old BPL
lists that do not include many households.
Poor quality of food in hospitals remains
of the key problems from the users point
of view

Page | 62
4.7.2 Finding from In-Depth Interviews (IDIs)
Present study, apart from FDGs had also conducted few IDIs from different
stokeholds/actors that are directly and indirectly associated with the RSBY scheme in terms of
awareness, enrolment, utilization and monitoring related issues.
Type Jharkhand West Bengal
Gram
Pradhan
Earlier people did not know about the
RSBY scheme
Although, few people in the village
earlier enrolled in the scheme but nobody
know how to use it.
Moreover, she told that even she herself
did not aware about the scheme till very
recently.
Since PACS led prorammes (through
SHARE) launched in the village, people
came to know about the RSBY scheme
and its benefits
She told that RSBY Mitra visits each
family in the village prior to the
enrolment day and inform about the
detailed information related with
enrolment process and documents that are
required.
Many families in the village used benefits
under this scheme recently with the help
of RSBY Mitra.
She further told that villagers are poor
and illiterate and have extensive believe
in traditional healers. But due to the
awareness about the benefits under
RSBY scheme, number of families
utilizing hospital care increased in recent
months.
In many cases, vehicles pooling by three
to four families for hospital visits is
common to reduce the expenses on travel,
idea initiated by RSBY Mitra.
Prior to CINI, no PRI member of this
village were aware about the RSBY
scheme.
Earlier people including many PRI
members believe that RSBY card is one
additional card like BPL
A three days meeting in Kolkata was
conducted by CINI and along with other
participants many PRI members were
invited to attend.
It was very intense meeting on RSBY
scheme and due to this meeting only
many PRI members came to know about
the benefit of the scheme.
While returning from the meeting, all
PRI members passed a resolution to
restrict agents from different private
hospitals who used to visit villages quite
often.
We extent every support to the RSBY
Sahayata Kendra established by PACS-
CINI in the village to support RSBY
related work.
PRI members always in active contact
with the Sahayata Kendra and prior to
every decision with related to RSBY
scheme we discussed with the local CINI
community mobilizes
Moreover, PRI members provide
information related to RSBY in almost
every meeting held in the village

Page | 63
However, she said that till now she never
invited by RSBY Mitra to attend any
community meeting
She further told that she will provide
every help in case she approached to raise
the awareness and utilization of RSBY
scheme in the village. She would be
happy to be part of any such programme
that is related with the RSBY scheme.
After the launch of Sahayata Kendra
many people able to utilize the benefits
provided by the scheme.
Overall hospitalization rates have
increased in recent years since people
aware that the cost will be covered by
this RSBY card.
He agreed that if proper awareness were
spread earlier, many deaths in the village
could easily be prevented due to lack of
financial support.
ASHA/
AWW
She first came to aware about the RSBY
scheme in 2011 through SHARE self
helped group meeting.
She was then aware about the eligibility
of the households in obtaining RSBY
scheme including BPL, MGNERA.
Earlier few people used to enroll in the
scheme, but the card only delivered to
those who used to pay Rs.15 per card
extra.
In many cases cards were delivered near
expiry date and none was able to use
them.
Till 2013, many families in the village
enrolled in the scheme but none of them
able to use since they did not know the
benefits.
However, after 2014 many people started
utilizing scheme for hospitalization.
But still majority of villages do not want
to go hospitals since they never gone out
of the village in their lifetime and they
feel very scare.
In this situation, people still prefer to take
care from traditional healers, whom they
feel more confident in interacting at the
doorsteps, and they charge less
However, few families started visiting
hospitals as they are now aware about the
benefits and hospitals that they know are
empanelled under RSBY scheme.
Prior to 2012, she did not know about
the RSBY scheme at all. Neither any
PRI members ever asked her about the
progress related to the scheme.
She first came to know about the scheme
in 2012 through CINI and realized how
important the scheme is for villagers.
Prior to interaction with CINI members,
she did not at all involve in the scheme.
However, after knowing the benefits she
attends every meeting conducted by
CINI to support the awareness and
enrolment.
In monthly meeting along with PRI
members and other local workers,
doctors are also invited and discuss
about the RSBY scheme and its
progress.
Previously villagers fears to go hospitals
due to high costs of treatment, but now
since they know about the scheme along
with details of empanelled hospitals,
they starts going hospitals frequently.

Page | 64
She further complained that the RSBY
Mitra does not visit households
frequently and at many occasions when
people are in need of her, no one could
find her.
Community
mobilizes
She joined as a RSBY Mitra in 2013 and
went for four days rigorous training in
Ranchi.
Prior to this training she did not know
about the RSBY scheme and the benefits
provider under the scheme.
When asked she told that she was
selected as a RSBY Mitra due to her
higher educational qualifications and well
known face in entire village.
Till 2012, very few families enrolled
under the RSBY scheme and none of
them ever used benefits for
hospitalization.
However, after completion of her training
in 2013 she started working and
contacted many families and provided
them knowledge about the scheme.
She recalled, in 2014 with her
commitment and motivation about 97
families in the village enrolled under
RSBY scheme.
In 2013 about 13 families utilized
benefits of RSBY scheme for
hospitalization care, which increased to
37 in 2014.
She told that in every weekly meeting,
she assess household where any of the
family member suffers from illness. She
than visit those household and provide
necessary counseling and if needed she
encourage family to visit empanelled
hospital for proper care.
In many cases she said family fears to
visit hospitals since nobody from the
family visited any hospital previously. In
that situation she accompanies family
The local community mobilize said that
his hobby is social work and due to this
he got interested to work closer in RSBY
scheme.
He joined as a PACS community
mobilize in 2013 and manage 9 villages.
His education qualification is
graduation.
Prior to joining as communities
mobilize, he did not aware about the
RSBY scheme at all.
When I joined this position in 2013, the
biggest challenge was lower coverage of
RSBY card, in many villages no RSBY
enrolment camps ever been conducted.
Of those who have RSBY scheme hardly
anybody knows its proper utilization.
There were several hospitals agents who
frequently visited villages and cheat
people in the name of health camps and
withdrawn entire money from their
cards.
In many cases I have seen, hospitals
scratch smart cards without any
hospitalization.
However, after joining this position, I
first make PRI members aware about the
wrongdoing that was going on in many
villages.
A resolution than passed by PRI
members and complete ban was imposed
on those private agents.
According to him, the biggest challenge
during enrolment of RSBY scheme is
bringing five family members to the
enrolment venue. Since majority of them
working on tea gardens on daily wages,

Page | 65
members to the hospitals and extent
every possible support in terms of
contacting RSBY help desk at hospitals,
talk to the doctors etc.
She further recalls that in many instances,
once she helped any family for
hospitalization from next time onwards
the family go alone, which she think is
the most important.
She further said that if any family in the
village benefited from the hospitalization,
it helps others to motivate and encourage
them to use the scheme.
However, she said that in spite of all
affords many families still prefer to
contact traditional healers for healthcare.
The most common problem is that if any
family which she encouraged to visit
hospitals does not get hospitalized, in that
condition family need to spend on
medical and transportation, that goes
negative to the family and others
neighborhoods.
it becomes very challenging to
convenience them.
At many occasions I personally, talked
to the tea garden administration to grant
leave from the jobs at least for half day
to enable families to enroll under the
SRBY scheme. But very few actually
follow what they promised to me.
I conducted many hospital exposure
visits to enable villagers to learn them
about the experience of hospitalization
which ultimately increases their
confidence.
Due to the lack of timing, families still
prefer to reach traditional healers who
are locally available.

Page | 66
References
Ahuja R and NarangA (2005) Emerging Trends in Health Insurance for Low-Income Groups. Economic
and Political Weekly, 40(38): 4151-4157.
Berki SE (1986) A Look at Catastrophic Medical Expenses and the Poor.Health Affairs5: 138 145.
Berman P, Ahuja R, and Bhandari L (2010) The Impoverishing Effect of Healthcare Payments in India:
New Methodology and Findings. Economic and Political Weekly, 45(16): 65-71.
Berman P, Ahuja R, Bhandari L (2010) The impoverishing effect of healthcare payments in India: new
methodology and findings. Economic & Political Weekly, 45:65-71
Carrin G and James C (2004). Reaching universal coverage via social health insurance: key design
features in the transition period. Health Financing Policy Issue Paper, WHO, Geneva. Available at:
http://www.who.int/health_financing/issues/en/reaching_universal_dp_04_2.pdf
Das J &Leino J (2011) Evaluating the RSBY: lessons from an experimental information campaign.
Economic & Political Weekly, 46(32): 85-93.
Dror DM &Vellakkal S (2012) Is RSBY India’s platform to implementing universal hospital insurance?
Indian Journal of Medical Research, 135, 56–63.
Ellis RP, Alam M and Gupta I (2000) Health Insurance in India: Prognosis and Prospectus. Economic and
Political Weekly, 35(4): 207-217
Eman B (2004) Community based health insurance in low-income countries: a systematic review of the
evidence. Helath Policy and Planning, 19(5): 249-70
Filmer D, and Pritchett L (1999) The Effect of Household Wealth on Educational Attainment: Evidence
from 35 Countries. Population and Development Review, 25: 85-120.
Garg C & Karan A (2005) Out-of-pocket Expenditure and Impoverishment: Policy Implications for
Targetted Populations in India.Paper presented at Forum 9, Mumbai, India, 12-16 September,
2005.
Grover, S & Palacios R (2011) The first two years of RSBY in Delhi. In Palacios, Robert, Das, Jishnu and
Sun. Changqing (eds) “India's Health Insurance Scheme for the Poor: Evidence from the Early
Experience of the RashtriyaSwasthyaBimaYojana” Centre for Policy Research, New Delhi

Page | 67
Gupta I (2009) Out-of-pocket Expenditures and Poverty: Estimates from NSS 61st Round, Institute of
Economic Growth, Delhi, 2009. Available at:
http://planningcommission.nic.in/reports/genrep/indrani.pdf
Gupta I and Trivedi M (2005) Social Health Insurance Redefined: Health for All through Coverage for
All. Economic and Political Weekly, 40(38): 4132-4140
Gupta I and Trivedi M (2006) Health Insurance: Beyond a Piecemeal Approach. Economic and Political
Weekly, 41(25): 2525-2528
Hou, X & Palacios R (2011) Hospitalization patterns in RSBY: preliminary evidence from the MIS. In
Palacios, Robert, Das, Jishnu and Sun. Changqing (eds) “India's Health Insurance Scheme for the
Poor: Evidence from the Early Experience of the RashtriyaSwasthyaBimaYojana” Centre for
Policy Research, New Delhi
Hsiao W and Shaw RP (2007) Social Health Insurance for Developing Nations. The World Bank
Washington, D.C.
Kumer S (2010) Awareness, Accessibility and barriers in utilization of RashtriyaSwathyaBimaYojana
among BPL households in Puri district, Ordisha. Available:
http://www.slideshare.net/SudheirYadav/awareness-accessibility-and-barriers-in-utilization-of-
rastriya-swasthya-bima-yozna-services-among-bpl-families-in-puri-district-odisha
Lagarde M, Haines A, Palmer N (2009) The impact of conditional cash transfers on health outcomes and
use of health services in low and middle income countries. Cochrane Database System
Review,7(4):CD008137.
Mazumdar S. &Mazumdar P.G. (2013). Health and Healthcare.Delhi Human Development Report- 2013.
Academic Foundation & Institute for Human Development, New Delhi
Montgomery M, Gragnolati M, Burke KA, Paredes E (2000) Measuring Living Standards with Proxy
Varables.Demography, 37(2): 155-74.
Nandi S, Nundy M, Prasad V, Kanungo K, Khan H, Haripriya S, Mishra T &Garg S (2012) The
Implementation of RSBY in Chhattisgarh, India: A study of the Durg district. Health, Culture and
Society, 2(1):
Narayana D (2010) Review of the RashtriyaSwasthyaBimaYojana.Economic and Political Weekly
45(29): 13-18.
Pannarunothai S & Mills A (1997) The Poor Pay More: Health-related Inequality in Thailand. Social
Science and Medicine, 44(12): 1781-1790.
Rajasekhar D, Berg E, Ghatak M & Roy S (2010) Implementing Health Insurance: The Rollout of
RashtriyaSwasthyaBimaYojana in Karnataka. Economic and Political Weekly, 46(20): 56-63.
Rathi P (2011) Evaluation of ´RashtriyaSwasthyaBimaYojana, a Health Insurance Scheme for below
poverty line people in Amravati. IIM Bangalore, India, 2011.

Page | 68
Reddy KS &Selvaraj S (2011) A Critical Assessment of the Existing Health Insurance Models in India.
Public Health Foundation of India, New Delhi. Available:
http://planningcommission.nic.in/reports/sereport/ser/ser_heal1305.pdf
Seshadri T, Trivedi M, Saxena D, Nair R, Soors W, Criel B, Devadasan N (2011) Study of
RashtriyaSwasthyaBimaYojana Health Insurance in India. WHO Reference no. 2011/126289-0.
Available: http://www.iphindia.org/v2/wp-content/uploads/2013/01/RSBY-
report_2013_Jan_02.pdf
Su TT, Kouyate B &Flessa S (2006) Catastrophic Household expenditure for Health Care in a Low-
income Society: A Study from Nouna District, Burkina Faso”, Bulletin of the WorldHealth
Organization, 84(1): 21-27.
Sun C (2011) An analysis of RSBY enrolment patterns: Preliminary evidence and lessons from the early
experience. In Palacios, Robert, Das, Jishnu and Sun. Changqing (eds) “India's Health Insurance
Scheme for the Poor: Evidence from the Early Experience of the RashtriyaSwasthyaBimaYojana”,
Centre for Policy Research, New Delhi.
Swarup A (2011) RashtriyaSwasthyaBimaYojana (RSBY) … some initial trends. RSBY Working Paper,
New Delhi.
Thakur H &Ghosh S (2013) Social Exclusion and (RSBY) RashtriyaSwasthyaBimaYojana in
Maharashtra.Tata Institute of Social Sciences, Mumbai. Available:
http://www.healthinc.eu/PDF/TISS_Maharashtra_RSBY_Case_Study_report.pdf
Thuan NBT, Lofgren C, Chuc NKT, Janlert U &Lindholm L (2006) Household Out-of-pocket Payments
for Illness: Evidence from Vietnam. Public Health, 6: 283
Wadhwa JDP (2010) Central Vigilance Committee on Public Distribution System Report on the State Of
Chhattisgarh. New Delhi: Justice Wadhwa Committee.
WHO. Sustainable Health Financing, Universal Coverage, and Social Health Insurance. In: 58th World
Health Assembly. Agenda Item 13.16 Edition. Geneva, 2005.
World Bank, 2000. “Measuring Living Standards: Household Consumption and Wealth Indices”,
Quantitative Techniques for Health Equity Analysis—Technical Note #4, The World Bank: Poverty
and Health, health, Nutrition and Population Division, Washington D.C. Available at
http://siteresources.worldbank.org/INTPAH/Resources/Publications/Quantitative-
Techniques/health_eq_tn04.pdf.
World Health Organisation (2005) Sustainable Health Financing, Universal Coverage, and Social Health
Insurance. In: 58th World Health Assembly. Agenda Item 13.16 Edition. Geneva.
Xu K (2005) Distribution of Health Payments and Catastrophic Expenditures: Methodology”, WHO
Discussion Paper, Number 2-2005, Geneva: WHO.
Xu K, Evans DB, Kawabata K, Zeramdini R, Klavus J & Murray CJL (2003a) Household Catastrophic
Health Expenditure: A Multicountry Analysis. Lancet, 362:111-117.
Xu K, Klavus J, Kawabata K, Evans DB, Hanvoravongchai P, Ortiz JP, Zeramdini R & Murray CJL
(2003b) Household Health System Contributions and Capacity to Pay: Definitional, Empirical and

Page | 69
Technical Challenges, in C.J.L. Murray & D.B. Evans (eds.), Health SystemPerformance
Assessment: Debates, Methods and Empiricism, Geneva: WHO, pp. 533-542.

Page | 70
Statistical Appendix

Page | 71

Page | 72
Appendix 1: RSBY in Jharkhand: A situational analysis
S.No. District Year of
Policy
Premium
(With
Service
tax)
Total Target Families Hospitals
Empanelled
Hospitalization
Total Enrolled
Conversion
ratio Private Public
Hospitalization
cases
Hospitalization
value (Rs)
Hospitalization-
ratio*
1 Bokaro 3 279 104886 55588 53.0 14 13 761 5,267,350 1.4
2 Chatra 3 279 133289 74867 56.2 8 6 49 145375 0.1
3 Deoghar 4 450 141175 41517 29.4 6 8 454 3358425 1.1
4 Dhanbad 4 450 157825 84546 53.6 24 9 3196 20912925 3.8
5 Dumka 3 376 125287 62276 49.7 4 10 208 712000 0.3
6 Garhwa 4 450 274843 86203 31.4 7 6 176 1408000 0.2
7 Giridih 3 376 188230 126996 67.5 11 12 1203 7957825 0.9
8 Godda 3 279 131196 68837 52.5 4 8 57 594,500 0.1
9 Gumla 3 376 87545 55410 63.3 3 11 244 825375 0.4
10 Hazaribag 2 279 167290 110102 65.8 15 12 623 2702000 0.6
11 Jamtara 3 450 109850 52024 47.4 3 6 149 808375 0.3
12 Khunti 4 450 62763 40332 64.3 4 6 65 180250 0.2
13 Kodarma 2 279 51638 32210 62.4 8 7 149 982750 0.5
14 Latehar 3 279 111744 67800 60.7 7 13 0 0 0.0
15 Lohardaga 3 376 45555 23646 51.9 5 7 645 1192500 2.7
16 Pakaur 3 279 129854 74095 57.1 7 6 132 799,250 0.2
17 Palamu 3 376 258719 93778 36.2 13 11 593 4667825 0.6
18
Pashchimi
Singhbhum 4 450 174506 79992 45.8 4 14 107 483283 0.1
19 Purbi Singhbhum 3 376 148810 79654 53.5 10 11 571 1821100 0.7
20 Ramgarh 2 279 95430 53385 55.9 15 4 42 230,250 0.1
21 Ranchi 4 450 226006 103400 45.8 34 16 1332 7450975 1.3
22 Sahibganj 3 279 137517 80018 58.2 2 7 0 0 0.0
23 Saraikela 3 450 184868 111153 60.1 7 10 38 180875 0.0
24 Simdega 3 376 71629 30267 42.3 2 7 103 248750 0.3
Total 3320455 1688096 50.8 217 220 10897 62,929,958 0.6
Source: RSBY website accessed on February 15, 2015 (http://jhr.nic.in/templates/rsbyproject/index.html)

Page | 73
Appendix 2: RSBY in West Bengal: A situational analysis
S. No District Year
of
Policy
Premium
(With
Service
tax)
Total Target Families
Hospitals
Empanelled Hospitalization
Total Enrolled
Conversion
ratio Private Public
Hospitalization
cases
Hospitalization
value (Rs)
Hospitalization
ratio*
1 Bankura 3 460 418430 354436 84.7 30 2 23355 149954442 6.6
2 Birbhum 3 460 424717 335541 79.0 24 2 34718 264494407 10.3
3 Burdwan 5 232 972156 673953 69.3 70 5 44763 292761858 6.6
4 Coochbehar 3 460 472396 179391 38.0 3 5 9811 60441932 5.5
5 Dakshin Dinajpur 2 460 234732 137000 58.4 3 4 142 716450 0.1
6 Darjiling 2 460 144484 33987 23.5 8 3 633 3214357 1.9
7 Hoogly 3 460 547375 347485 63.5 32 3 14917 87089447 4.3
8 Howrah 3 460 238342 85626 35.9 29 1 5559 35551919 6.5
9 Jalpaiguri 3 460 619180 228123 36.8 10 3 24096 121580338 10.6
10 Kolkata 1 432 217846 112912 51.8 35 9 733 4962910 0.6
11 Maldah 5 185 654264 366123 56.0 15 2 13265 85698223 3.6
12 Murshidabad 4 205 1021376 558776 54.7 44 1 47037 342073927 8.4
13 Nadia 4 262 690852 370858 53.7 52 1 29048 215522881 7.8
14 North 24 Parganas 4 380 874840 444780 50.8 43 10 14303 94703415 3.2
15 Paschim Medinipur 4 212 813626 449362 55.2 26 2 14154 91804037 3.1
16 Purba Midnapore 4 380 461806 277280 60.0 63 1 10123 76494191 3.7
17 Purulia 3 460 394035 197619 50.2 8 2 4265 21894603 2.2
18 South 24 Parganas 2 460 706669 343831 48.7 45 5 17754 121191692 5.2
19 Uttar Dinajpur 3 460 293416 146000 49.8 4 1 40 274250 0.0
Total 10200542 5643083 55.3 544 62 308716 2070425279 5.5
Source: RSBY website accessed on February 15-*, 2015 (http://www.rsbywb.gov.in/home#)

Page | 74
Appendix 3. Profile of the sample population by background characteristics
Jharkhand West Bengal
Background characteristics Intervention
District
Non-
intervention
district
Total Intervention
District
Non-
intervention
district
Total
Age group
0-5 11.3 9.7 10.5 7.2 7.9 7.6
6-14 21.5 22.8 22.1 17.3 16.4 16.8
15-49 50.7 51.4 51.0 59.4 59.2 59.3
50-64 12.7 12.0 12.3 12.3 12.3 12.3
65+ 3.9 4.1 4.0 3.8 4.2 4.1
Sex
Male 51.8 53.9 52.8 50.2 51.1 50.7
Female 48.2 46.1 47.2 49.8 48.9 49.3
Highest education level in HH
Illiterate 6.4 9.7 8.1 66.3 63.5 64.7
Primary completed 13.1 12.8 12.9 18.7 21.6 20.3
Secondary completed 40.4 31.5 36.0 9.2 8.5 8.8
Higher secondary 24.6 19.8 22.2 4.2 3.9 4.0
Higher secondary & above 15.5 26.2 20.8 1.7 2.5 2.2
Occupation
Daily wage labourer 24.4 21.6 23.1 29.7 30.4 30.1
Self employed/Salaried 16.0 16.7 16.3 7.1 5.5 6.2
Unemployed/Non-salary 17.1 16.4 16.7 26.9 27.7 27.4
Student 27.6 29.5 28.5 26.4 24.4 25.2
Elderly/Handicap/children 15.0 15.8 15.4 9.9 12.0 11.1
Caste
General/OBC 58.3 53.4 55.8 62.1 43.5 51.1
Scheduled Castes 16.5 20.8 18.7 11.7 51.8 35.4
Scheduled Tribes 25.3 25.8 25.6 26.2 4.7 13.5
Religion
Hindu 72.1 83.6 77.8 30.1 82.8 61.3
Muslims 7.1 9.1 8.1 58.3 17.0 33.8
Sarna/Christians/Others 20.9 7.4 14.1 11.7 0.2 4.9
MPCE
MPCE quintile 1 (Lowest) 22.2 17.8 20.0 22.0 18.8 20.1
MPCE quintile 2 19.9 20.1 20.0 18.1 21.2 20.0
MPCE quintile 3 21.2 18.8 20.0 19.7 20.3 20.1
MPCE quintile 4 16.8 23.2 20.0 21.4 19.0 20.0
MPCE quintile 5 (Higher) 19.9 20.1 20.0 18.8 20.8 20.0
Toilet facility
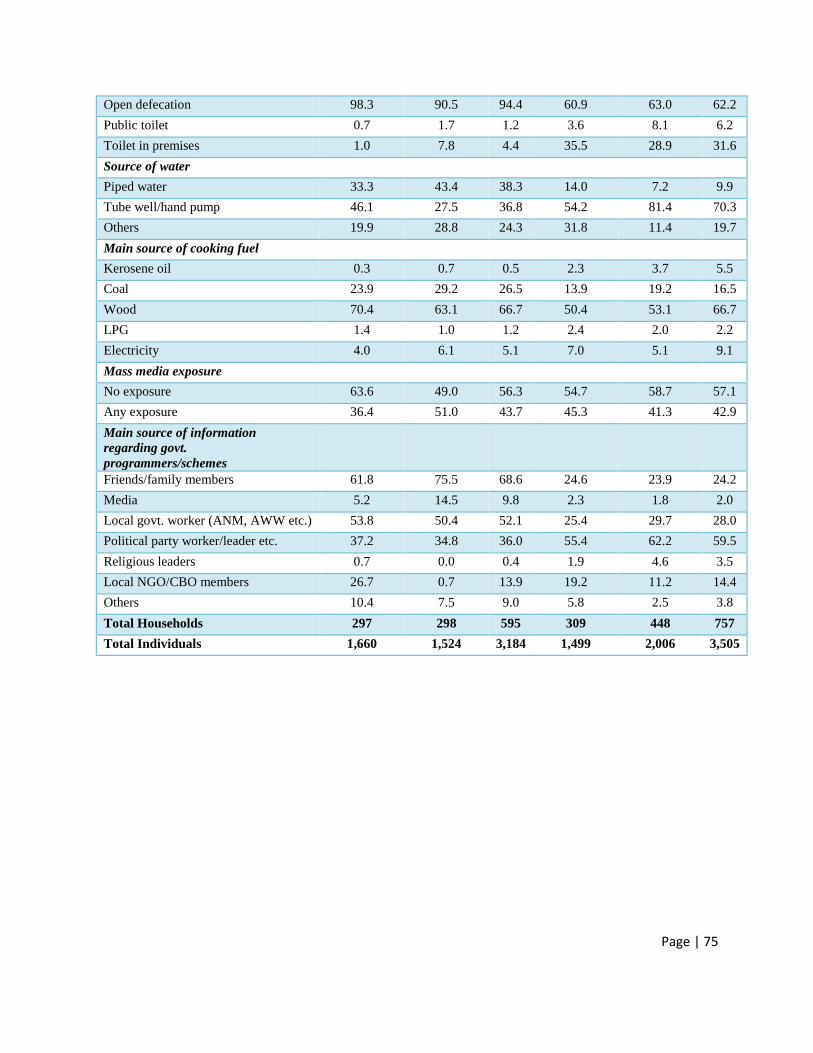
Page | 75
Open defecation 98.3 90.5 94.4 60.9 63.0 62.2
Public toilet 0.7 1.7 1.2 3.6 8.1 6.2
Toilet in premises 1.0 7.8 4.4 35.5 28.9 31.6
Source of water
Piped water 33.3 43.4 38.3 14.0 7.2 9.9
Tube well/hand pump 46.1 27.5 36.8 54.2 81.4 70.3
Others 19.9 28.8 24.3 31.8 11.4 19.7
Main source of cooking fuel
Kerosene oil 0.3 0.7 0.5 2.3 3.7 5.5
Coal 23.9 29.2 26.5 13.9 19.2 16.5
Wood 70.4 63.1 66.7 50.4 53.1 66.7
LPG 1.4 1.0 1.2 2.4 2.0 2.2
Electricity 4.0 6.1 5.1 7.0 5.1 9.1
Mass media exposure
No exposure 63.6 49.0 56.3 54.7 58.7 57.1
Any exposure 36.4 51.0 43.7 45.3 41.3 42.9
Main source of information
regarding govt.
programmers/schemes
Friends/family members 61.8 75.5 68.6 24.6 23.9 24.2
Media 5.2 14.5 9.8 2.3 1.8 2.0
Local govt. worker (ANM, AWW etc.) 53.8 50.4 52.1 25.4 29.7 28.0
Political party worker/leader etc. 37.2 34.8 36.0 55.4 62.2 59.5
Religious leaders 0.7 0.0 0.4 1.9 4.6 3.5
Local NGO/CBO members 26.7 0.7 13.9 19.2 11.2 14.4
Others 10.4 7.5 9.0 5.8 2.5 3.8
Total Households 297 298 595 309 448 757
Total Individuals 1,660 1,524 3,184 1,499 2,006 3,505

Page | 76
Appendix 4. Prevalence of short-term morbidity by background characteristics
Jharkhand West Bengal
Background characteristics Intervention
District
Non-
intervention
district
Total Intervention
District
Non-
intervention
district
Total
Age group
0-5 0.0 0.7 0.3 2.8 3.8 3.4
6-14 1.1 0.0 0.6 3.5 2.4 2.9
15-49 15.7 9.7 12.8 12.8 12.4 12.5
50-64 47.6 25.7 37.4 20.9 16.3 18.2
65+ 47.7 24.2 36.2 15.5 26.4 22.1
Sex
Male 19.9 12.2 16.1 11.8 13.0 12.5
Female 12.0 5.6 9.0 11.4 9.3 10.2
Highest Education Level
Illiterate 29.8 13.5 21.9 11.6 11.5 11.5
Primary completed 10.4 4.8 7.9 11.7 8.0 9.4
Secondary completed 11.0 9.9 10.5 9.4 18.6 14.6
Higher secondary 12.7 8.1 10.3 20.6 11.4 15.5
Higher secondary & above 3.2 7.6 6.0 3.9 4.0 4.0
Occupation
Daily wage labourer 24.2 16.4 20.7 16.0 15.8 15.9
Self employed/Salaried 32.5 18.5 25.6 12.2 12.4 12.3
Unemployed/Non-salary 14.5 6.8 10.9 11.9 12.6 12.3
Student 1.8 0.4 1.1 5.6 4.3 4.9
Elderly/Handicap/children 13.7 7.9 10.8 12.7 9.5 10.7
Caste
General/OBC 16.7 10.06 13.6 9.2 12.7 10.9
Scheduled Castes 23.5 9.3 15.9 15.4 10.1 10.9
Scheduled Tribes 9.8 7.0 8.5 15.4 7.3 14.1
Religion
Hindu 18.2 9.2 13.6 15.8 11.1 12.1
Muslims 16.3 11.5 13.7 8.5 11.4 9.3
Sarna/Christians/Others 9.2 4.5 8.1 15.7 0.0 15.4
MPCE
MPCE quintile 1 (Lowest) 7.9 3.6 5.9 8.7 6.5 7.5
MPCE quintile 2 12.3 7.0 9.7 8.8 8.1 8.3
MPCE quintile 3 16.1 8.0 12.6 11.6 11.1 11.3
MPCE quintile 4 22.4 9.4 15.5 15.1 15.4 15.3
MPCE quintile 5 (Higher) 24.2 18.1 21.1 14.6 17.0 16.0
Toilet facility

Page | 77
Open defecation 15.8 8.6 12.5 11.3 11.1 11.2
Public toilet 33.3 15.0 21.9 13.7 14.2 14.1
Toilet in premises 35.3 14.1 16.6 11.7 10.6 11.1
Source of water
Piped water 30.0 66.7 38.5 11.6 20.4 15.3
Tube well/hand pump 19.5 8.1 15.7 8.9 10.2 9.8
Others 13.0 8.4 11.9 16.2 12.0 14.9
Mass media exposure
No exposure 16.9 8.7 13.5 12.3 11.7 11.9
Any exposure 14.7 9.5 11.9 10.8 10.5 10.6
Total 16.1 9.1 12.8 11.6 11.2 11.4

Page | 78
Appendix 5. Hospitalization rates by selected background characteristics
Jharkhand West Bengal
Background characteristics Intervention
District
Non-
intervention
district
Total Intervention
District
Non-
intervention
district
Total
Age group
0-5 0.0 0.0 0.0 1.9 0.0 0.8
6-14 0.0 0.0 0.0 1.2 1.5 1.4
15-49 4.4 6.4 5.4 5.3 3.0 3.9
50-64 17.6 15.3 16.5 9.7 8.9 9.3
65+ 27.7 21.0 24.4 17.5 12.9 14.8
Sex
Male 7.3 7.8 7.6 6.1 4.0 4.9
Female 3.6 3.8 3.7 4.6 3.3 3.8
Highest Education Level
Illiterate 7.7 9.0 8.3 5.3 3.9 4.5
Primary completed 5.1 3.5 4.3 3.9 3.2 3.5
Secondary completed 3.9 7.2 5.4 8.8 2.4 5.2
Higher secondary 8.2 4.7 6.4 3.2 5.1 4.3
Higher secondary & above 6.4 2.5 3.9 3.9 2.0 2.6
Occupation
Daily wage laborer 7.7 10.9 9.1 8.3 4.9 6.3
Self employed/Salaried 15.1 12.6 13.9 4.7 4.5 4.6
Unemployed/Non-salary 2.5 2.8 2.6 4.5 3.8 4.1
Student 0.0 0.2 0.1 1.0 1.2 1.1
Elderly/Handicap/children 5.6 6.2 5.9 10.1 4.6 6.7
Caste
General/OBC 4.4 6.3 5.3 6.0 3.6 4.8
Scheduled Castes 5.3 5.7 5.5 2.9 3.9 3.8
Scheduled Tribes 8.2 5.4 6.9 4.8 1.2 4.2
Religion
Hindu 5.3 6.0 5.6 5.6 3.9 4.3
Muslims 4.7 3.9 4.2 5.9 2.5 4.9
Sarna/Christians/Others 6.7 8.9 7.2 2.0 0.0 2.0
MPCE
MPCE quintile 1 (Lowest) 5.1 5.6 5.3 2.7 2.2 2.4
MPCE quintile 2 5.4 4.2 4.8 5.1 3.0 3.8
MPCE quintile 3 5.0 6.0 5.5 3.3 4.8 4.2
MPCE quintile 4 6.8 8.4 7.7 8.6 4.2 6.3
MPCE quintile 5 (Higher) 5.8 5.6 5.7 7.9 4.4 5.9

Page | 79
Toilet facility
Open defecation 5.6 6.1 5.8 5.0 4.0 4.4
Public toilet 0.0 0.0 0.0 4.0 4.5 4.4
Toilet in premises 5.9 5.5 5.5 6.0 2.7 4.3
Source of water
Piped water 8.9 19.7 11.1 7.8 4.7 6.5
Tube well/hand pump 4.6 6.4 5.2 5.5 3.6 4.2
Others 3.0 5.2 3.2 3.9 3.0 3.6
Mass media exposure
No exposure 4.2 4.9 4.5 4.4 3.8 4.1
Any exposure 7.7 7.0 7.3 6.3 3.4 4.7
Total 5.5 6.0 5.8 5.3 3.6 4.4

Page | 80
Appendix 6. Type of health facility use for hospitalization by selected socioeconomic characteristics in Jharkhand
Intervention District Non-Intervention District Total
Background
Characteristic
Public
facility
Private
facility
Informal
providers
Public
facility
Private
facility
Informal
providers
Public
facility
Private
facility
Informal
providers
Age group
15-49 4.6 59.1 36.4 8.0 52.0 40.0 6.4 55.3 38.3
50-64 4.4 91.3 4.4 33.3 33.3 33.3 15.8 68.4 15.8
65+ 12.5 75.0 12.5 12.5 75.0 12.5 12.5 75.0 12.5
Sex
Male 5.3 73.7 21.1 17.7 47.1 35.3 11.1 61.1 27.8
Female 6.7 80.0 13.3 14.3 57.1 28.6 10.3 69.0 20.7
Highest education level
Illiterate 4.2 75.0 20.8 19.2 53.9 26.9 12.0 64.0 24.0
Primary completed 13.3 66.7 20.0 16.7 66.7 16.7 14.3 66.7 19.1
Secondary completed 0.0 83.3 16.7 8.3 33.3 58.3 5.6 50.0 44.4
Higher secondary 0.0 80.0 20.0 33.3 66.7 0.0 12.5 75.0 12.5
Higher secondary & above 0.0 100.0 0.0 0.0 0.0 100.0 0.0 75.0 25.0
Occupation
Daily wage laborer 0.0 85.0 15.0 26.3 47.4 26.3 12.8 66.7 20.5
Self employed/Salaried 8.7 60.9 30.4 17.7 41.2 41.2 12.5 52.5 35.0
Unemployed/Non-salary 0.0 100.0 0.0 0.0 75.0 25.0 0.0 85.7 14.3
Student 14.3 85.7 0.0 0.0 62.5 37.5 6.7 73.3 20.0
Caste
General/OBC 7.1 71.4 21.4 0.0 59.3 40.7 3.6 65.5 30.9
Scheduled Castes 12.5 75.0 12.5 66.7 22.2 11.1 41.2 47.1 11.8
Scheduled Tribes 0.0 82.4 17.7 16.7 50.0 33.3 6.9 69.0 24.1
Religion
Hindu 8.8 73.5 17.7 11.9 57.1 31.0 10.5 64.5 25.0
Muslims 0.0 80.0 20.0 0.0 0.0 100.0 0.0 66.7 33.3
Sarna/Christians/Others 0.0 78.6 21.4 60.0 0.0 40.0 15.8 57.9 26.3
MPCE
MPCE quintile 1 (Lowest) 9.1 72.7 18.2 9.1 54.6 36.4 9.1 63.6 27.3
MPCE quintile 2 0.0 66.7 33.3 28.6 28.6 42.9 12.5 50.0 37.5
MPCE quintile 3 10.0 80.0 10.0 16.7 58.3 25.0 13.6 68.2 18.2
MPCE quintile 4 0.0 70.0 30.0 14.3 57.1 28.6 8.3 62.5 29.2
MPCE quintile 5 (Higher) 7.7 84.6 7.7 25.0 25.0 50.0 11.8 70.6 17.7
Mass media exposure
No exposure 0.0 76.0 24.0 18.2 40.9 40.9 8.5 59.6 31.9
Any exposure 10.7 75.0 14.3 15.4 57.7 26.9 13.0 66.7 20.4
Total 5.7 75.5 18.9 16.7 50.0 33.3 10.9 63.4 25.7

Page | 81
Appendix 7. Type of health facility use for hospitalization by selected socioeconomic characteristics in West Bengal
Intervention District Non-Intervention District Total
Background
characteristic
Public
facility
Private
facility
Informal
providers
Public
facility
Private
facility
Informal
providers
Public
facility
Private
facility
Informal
providers
Age group
0-5 50.0 50.0 0.0 na na na 50.0 50.0 0.0
6-14 33.3 66.7 0.0 50.0 25.0 25.0 42.9 42.9 14.3
15-49 25.8 58.1 16.1 24.0 60.0 16.0 25.0 58.9 16.1
50-64 61.5 38.5 0.0 15.4 38.5 46.2 38.5 38.5 23.1
65+ 37.5 62.5 0.0 42.9 57.1 0.0 40.0 60.0 0.0
Sex
Male 35.3 64.7 0.0 29.6 48.2 22.2 32.8 57.4 9.8
Female 39.1 39.1 21.7 22.7 54.6 22.7 31.1 46.7 22.2
Highest education level
Illiterate 45.0 45.0 10.0 33.3 43.3 23.3 40.0 44.3 15.7
Primary completed 11.1 88.9 0.0 16.7 75.0 8.3 14.3 81.0 4.8
Secondary completed 16.7 66.7 16.7 25.0 25.0 50.0 20.0 50.0 30.0
Higher secondary 0.0 100.0 na 0.0 50.0 50.0 0.0 66.7 33.3
Higher secondary & above na na 0.0 0.0 100.0 0.0 0.0 100.0 0.0
Occupation
Daily wage labourer 44.0 48.0 8.0 26.3 47.4 26.3 36.4 47.7 15.9
Self employed/Salaried 25.0 75.0 0.0 75.0 0.0 25.0 50.0 37.5 12.5
Unemployed/Non-salaried 21.4 64.3 14.3 7.1 78.6 14.3 14.3 71.4 14.3
Student 33.3 66.7 0.0 20.0 40.0 40.0 25.0 50.0 25.0
Elderly/Handicap/children 40.0 50.0 10.0 42.9 42.9 14.3 41.2 47.1 11.8
Caste
General/OBC 37.2 51.2 11.6 13.6 63.6 22.7 29.2 55.4 15.4
Scheduled Castes 0.0 100.0 0.0 37.0 40.7 22.2 32.3 48.4 19.4
Scheduled Tribes 50.0 50.0 0.0 na na na 50.0 50.0 0.0
Religion
Hindu 42.9 57.1 0.0 29.6 47.7 22.7 32.8 50.0 17.2
Muslims 35.7 52.4 11.9 0.0 80.0 20.0 31.9 55.3 12.8
Christians/Others 0.0 100.0 0.0 na na na 0.0 100.0 0.0
MPCE
MPCE quintile 1 (Lowest) 33.3 50.0 16.7 25.0 50.0 25.0 30.0 50.0 20.0
MPCE quintile 2 66.7 33.3 0.0 12.5 75.0 12.5 41.2 52.9 5.9
MPCE quintile 3 11.1 88.9 0.0 33.3 33.3 33.3 23.8 57.1 19.1
MPCE quintile 4 33.3 55.6 11.1 23.1 61.5 15.4 29.0 58.1 12.9
MPCE quintile 5 (Higher) 40.0 46.7 13.3 33.3 41.7 25.0 37.0 44.4 18.5
Mass media exposure
No exposure 48.2 37.0 14.8 18.5 51.9 29.6 33.3 44.4 22.2

Page | 82
Any exposure 26.7 70.0 3.3 36.4 50.0 13.6 30.8 61.5 7.7
Total 36.8 54.4 8.8 26.5 51.0 22.5 32.1 52.8 15.1

Page | 83
Appendix 8. Mean monthly healthcare expenditure by background characteristics (in Rs.)
Jharkhand West Bengal
Background Characteristic Out-patient In-patient Total Out-patient In-patient Total
Highest education level in HH
Illiterate 2026 665 1591 2453 2592 2495
Primary completed 1475 1296 1335 2540 1955 2351
Secondary completed 1527 1829 1618 3265 1203 2521
Higher secondary 1015 1246 1097 2041 1995 2027
Higher secondary & above 1677 1282 1463 15415 3309 9557
Caste
General/OBC 1604 1582 1577 4356 2340 3687
Scheduled Castes 1473 1737 1575 2586 2131 2389
Scheduled Tribes 1110 828 940 1997 1204 1777
Religion
Hindu 1511 1520 1503 3205 1841 2716
Muslims 1928 1986 1949 4189 2545 3619
Christians/Others 866 448 628 2286 2137 2255
MPCE
MPCE quintile 1 (Lowest) 889 955 899 2177 556 1672
MPCE quintile 2 871 1276 1029 4281 957 3173
MPCE quintile 3 918 1110 994 1842 2493 2070
MPCE quintile 4 1311 1563 1435 3101 1876 2633
MPCE quintile 5 (Higher) 2639 2056 2417 5469 3776 4915
Mass media exposure
No exposure 1584 1471 1525 2878 2825 2862
Any exposure 1344 1333 1325 4445 1310 3188
District Type
Intervention 1512 1728 1578 2642 1907 2373
Non-intervention 1453 1079 1261 4120 2317 3540
Total 1488 1396 1433 3469 2105 2,997

Page | 84
Appendix 9. Mean Out of Pocket Expenditure (OOPE) and percentage share of OOPE of total household expenditure according to selected
household attributes in Jharkhand (in %)
Background Characteristics Intervention District Non-Intervention District Total
Out-patient In-patient Total Out-patient In-patient Total Out-patient In-patient Total
Highest education level in HH
Illiterate 17.6 52.9 26.4 39.8 10.6 28.1 30.9 21.2 27.5
Primary completed (upto 4) 26.6 35.1 29.0 15.1 18.1 16.6 20.5 27.1 23.1
Secondary completed (upto 9) 27.8 25.1 27.1 20.0 23.5 21.3 25.2 24.3 24.9
Higher secondary (upto 10) 18.0 24.8 20.9 19.8 25.0 21.4 18.7 24.9 21.1
Higher secondary & above (11 & above) 22.8 22.0 22.4 15.8 25.7 21.4 18.9 24.2 21.8
Caste
General/OBC 21.6 27.3 23.2 24.2 21.9 22.9 22.6 24.3 23.0
Scheduled Castes 32.8 35.6 33.8 16.1 17.7 16.8 25.6 26.7 26.0
Scheduled Tribes 24.7 19.5 21.5 14.8 28.9 21.9 20.0 23.9 21.7
Religion
Hindu 25.2 28.8 26.3 19.7 25.3 22.1 22.8 26.9 24.3
Muslims 21.1 36.5 25.9 28.2 15.0 22.8 24.5 24.0 24.3
Christians/Others 21.9 15.3 18.5 15.2 12.0 12.0 21.0 14.2 16.8
MPCE
MPCE quintile 1 (Lowest) 18.3 32.1 23.8 9.8 18.2 14.8 15.2 25.4 20.2
MPCE quintile 2 19.0 24.5 21.0 19.3 22.7 20.2 19.1 23.5 20.6
MPCE quintile 3 17.6 23.1 19.2 15.2 29.1 23.0 17.0 26.4 20.7
MPCE quintile 4 28.3 28.7 28.5 15.4 23.1 19.7 22.5 25.6 24.0
MPCE quintile 5 (Higher) 36.0 23.3 31.1 29.3 19.2 25.8 32.6 21.5 28.5
Mass media exposure
No exposure 26.2 24.0 25.1 23.5 27.9 25.3 25.2 25.8 25.2
Any exposure 21.0 28.9 24.5 17.3 19.9 18.3 19.1 23.7 21.2
Total 24.4 26.4 24.9 20.5 23.0 21.5 22.8 24.6 23.3

Page | 85
Appendix 10. Mean Out of Pocket Expenditure (OOPE) and percentage share of OOPE of total household expenditure according to selected
household attributes in West Bengal (in %)
Background Characteristics Intervention District Non-Intervention District All District
Out-patient In-patient Total Out-patient In-patient Total Out-patient In-patient Total
Highest education level in HH
Illiterate 28.8 29.4 29.0 34.1 24.2 31.7 31.7 27.4 30.3
Primary completed (upto 4) 26.0 22.5 25.2 22.8 20.5 22.1 24.3 21.6 23.6
Secondary completed (upto 9) 35.1 15.9 27.3 19.7 11.3 16.5 26.5 13.7 21.5
Higher secondary (upto 10) 20.7 11.3 18.1 30.1 32.0 30.7 26.5 25.1 26.1
Higher secondary & above (11 & above) 24.7 22.4 23.0 25.7 31.3 28.1 25.4 26.2 25.8
Caste
General/OBC 29.1 20.4 25.3 25.2 29.2 26.3 26.9 23.8 25.8
Scheduled Castes 16.3 33.8 23.1 27.4 16.8 23.2 25.8 19.3 23.2
Scheduled Tribes 28.6 21.8 26.9 29.2 12.7 26.4 28.7 21.3 26.8
Religion
Hindu 27.6 17.8 24.1 25.0 19.9 23.2 25.6 19.3 23.4
Muslims 28.6 22.2 25.8 32.4 39.0 34.0 29.7 24.9 27.9
Christians/Others 26.0 36.8 28.4 - - - 26.0 36.8 28.4
MPCE
MPCE quintile 1 (Lowest) 18.8 19.0 18.9 29.1 15.5 24.3 24.1 17.3 21.6
MPCE quintile 2 24.8 19.1 22.4 23.5 19.2 22.2 24.0 19.1 22.3
MPCE quintile 3 28.5 22.2 26.3 24.0 22.5 23.5 26.0 22.3 24.8
MPCE quintile 4 27.6 22.0 25.6 29.7 19.5 26.4 28.7 21.1 26.0
MPCE quintile 5 (Higher) 34.9 25.9 31.8 26.1 30.0 26.8 29.5 28.2 28.8
Mass media exposure at HH level
No exposure 29.3 25.3 28.1 27.9 25.3 27.1 28.6 25.3 27.5
Any exposure 24.7 19.2 22.3 23.9 17.9 21.8 24.3 18.7 22.0
Total 27.8 21.9 25.6 26.3 22.3 24.9 26.9 22.1 25.2

Page | 86
Appendix 11. Awareness about schemes that covers hospitalization expenses by selected background characteristics (in %)
Jharkhand West Bengal
Intervention District Non-Intervention
District
Intervention District Non-Intervention
District
Background characteristics Any scheme
that covers
Hospitalization
expenses
RSBY Any scheme
that covers
Hospitalization
expenses
RSBY Any scheme
that covers
Hospitalization
expenses
RSBY Any scheme
that covers
Hospitalization
expenses
RSBY
Highest education level
Illiterate 73.7 89.5 65.5 82.8 32.5 38.6 21.9 23.8
Primary completed 66.7 94.9 52.6 73.7 27.5 29.7 27.3 32.7
Secondary completed 70.8 93.3 60.6 83 34.7 38.9 19.5 20.7
Higher secondary 83.6 97.3 55.9 79.7 52.4 50 21.1 26.3
Higher secondary & above 89.1 91.3 70.5 87.2 31.6 31.6 28.9 26.7
Caste
General/OBC 75.7 95.4 55.3 80.5 26.7 28.8 24.6 27.7
Scheduled Castes 69.4 89.8 67.7 85.5 41.7 50 23.6 26.6
Scheduled Tribes 82.7 93.3 70.1 83.1 48.8 51.3 20 20
Religion
Hindu 76.6 95.3 63.9 83.5 54.9 60.4 24 26.4
Muslims 57.1 85.7 33.3 59.3 23.3 25 23.7 28.9
Christians/Others 82.3 91.9 72.7 95.5 36.1 38.9 0 0
MPCE
MPCE quintile 1 (Lowest) 89.4 95.5 62.3 81.1 30.9 36.8 25 28.6
MPCE quintile 2 76.3 94.9 68.3 86.7 30.4 33.9 23.7 29
MPCE quintile 3 73 98.4 64.3 78.6 25 31.7 29.7 30.8
MPCE quintile 4 76 86 59.4 82.6 36.9 40 17.6 20
MPCE quintile 5 (Higher) 66.1 93.2 55 81.7 48.3 43.1 23.1 25.3
Total 76.4 93.9 61.7 82.2 34.2 37.1 23.9 26.8

Page | 87
Appendix 12. Awareness about specific components of RSBY scheme by selected background characteristics in Jharkhand (in %)
Intervention District Non-Intervention District
Background
characteristics
Eligibili
ty
No. of
enrollme
nt
member
Enrollme
nt
expenses
Amou
nt
spent
per
year
Type of
treatme
nt
Awareness
about
transportati
on
allowance
Eligibili
ty
No. of
enrollme
nt
member
Enrollme
nt
expenses
Amou
nt
spent
per
year
Type of
treatme
nt
Awareness
about
transportati
on
allowance
Highest education
level
Illiterate 78.9 73.7 89.5 68.4 47.4 10.5 62.1 62.1 75.9 41.4 44.8 17.2
Primary completed 71.8 82.1 94.9 53.8 66.7 28.2 73.7 84.2 92.1 55.3 44.7 18.4
Secondary completed 73.3 90.8 91.7 69.2 67.5 18.3 71.3 77.7 89.4 47.9 55.3 18.1
Higher secondary 82.2 90.4 90.4 87.7 76.7 34.2 81.4 74.6 81.4 54.2 55.9 5.1
Higher secondary &
above
84.8 87 89.1 78.3 69.6 41.3 76.9 82.1 87.2 67.9 69.2 14.1
Caste
General/OBC 78.6 89 93.1 69.9 65.9 19.1 78 79.2 88.7 56 59.1 18.2
Scheduled Castes 71.4 85.7 85.7 65.3 63.3 12.2 80.6 87.1 83.9 58.1 59.7 14.5
Scheduled Tribes 78.7 86.7 90.7 85.3 78.7 53.3 61 66.2 83.1 49.4 49.4 6.5
Religion
Hindu 77.1 87.9 92.5 72 66.8 21.5 75.1 78.3 86.3 57 58.6 14.5
Muslims 85.7 90.5 85.7 42.9 57.1 0 81.5 77.8 81.5 29.6 33.3 18.5
Christians/Others 75.8 87.1 88.7 87.1 79 53.2 54.5 68.2 90.9 59.1 63.6 9.1
MPCE
MPCE quintile 1
(Lowest)
86.4 86.4 98.5 90.9 80.3 47 81.1 86.8 92.5 58.5 67.9 17
MPCE quintile 2 81.4 93.2 91.5 79.7 69.5 28.8 73.3 78.3 88.3 58.3 60 18.3
MPCE quintile 3 68.3 88.9 90.5 66.7 65.1 19 67.9 73.2 83.9 57.1 53.6 14.3
MPCE quintile 4 78 88 86 64 64 16 71 75.4 79.7 53.6 49.3 13
MPCE quintile 5
(Higher)
72.9 83.1 88.1 61 62.7 18.6 78.3 75 88.3 46.7 55 10
Total 77.4 87.9 91.2 73.1 68.7 26.6 74.2 77.5 86.2 54.7 56.7 14.4

Page | 88
Appendix 13. Awareness about specific components of RSBY scheme by selected background characteristics in West Bengal (in %)
Intervention District Non-Intervention District
Background Characteristics Eligibility No. of
enrollment
member
Enrollment
expenses
How
much
amount
spent
per
year
Type of
treatment
Awareness
about
transportation
allowance
Eligibility No. of
enrollment
member
Enrollment
expenses
How
much
amount
spent
per
year
Type of
treatment
Awareness
about
transportation
allowance
Highest education level
Illiterate 60 80 99 87 41 5 73 74 96 86 39.3 2.8
Primary completed 59 72 97 80 27 3 70 73 92 76 40.7 3.3
Secondary completed 71 76 97 88 46 7 71 72 97 78 44.3 1.1
Higher secondary 71 74 100 86 45 5 69 76 97 88 36.2 6.9
Higher secondary & above 60 75 75 75 10 10 71 73 93 80 28.9 0
Caste
General/OBC 72 81 96 89 41 5 69 75 93 83 37.4 3.1
Scheduled Castes 61 69 100 78 22 0 73 72 96 80 40.1 3
Scheduled Tribes 46 65 95 77 32 9 62 67 91 71 47.6 0
Religion
Hindu 46 68 95 79 34 7 71 73 95 80 39.1 3.2
Muslims 75 80 97 89 41 5 67 76 93 87 39.5 1.3
Christians/Others 53 72 97 75 22 3 100 100 100 100 100 0
MPCE
MPCE quintile 1 (Lowest) 54 74 99 87 31 6 76 81 100 83 38.1 3.6
MPCE quintile 2 61 80 98 84 43 5 73 67 94 77 37.9 5.3
MPCE quintile 3 62 74 95 82 36 7 65 71 93 79 42.9 2.2
MPCE quintile 4 70 77 96 85 42 2 68 75 97 84 43.5 1.2
MPCE quintile 5 (Higher) 72 72 95 83 31 7 72 72 90 82 34.4 2.2
Total 64 75 96 84 37 5 71 73 95 81 39.3 2.9

Page | 89
Appendix 14. Source of awareness about s RSBY scheme by selected background Characteristics in
Jharkhand
Intervention District Non-Intervention District
Background
Characteristics
Friends/
Relative
s/
Neighbo
rs
Teacher/
Panchayat/
ANM/AW
W
RSB
Y
Mitra
TV/
Radio/
Other
Source
s
Friends/
Relative
s/
Neighbo
rs
Teacher/
Panchayat/
ANM/AW
W
SHG
/
NG
O
TV/
Radio/
Other
Source
s
Highest education
Illiterate 26.3 47.4 52.6 0.0 41.4 65.5 17.2 3.5
Primary completed 12.8 61.5 35.9 5.1 26.3 71.1 10.5 5.3
Secondary completed 23.3 58.3 25.8 7.5 40.4 58.5 7.5 2.1
Higher secondary 13.7 42.5 53.4 1.4 42.4 57.6 3.4 6.8
Higher secondary &
above
15.2 41.3 43.5 10.9 29.5 73.1 7.7 7.7
Caste
General/OBC 19.7 51.5 34.1 5.8 30.8 67.3 10.1 5.7
Scheduled Castes 20.4 61.2 20.4 8.2 61.3 53.2 6.5 3.2
Scheduled Tribes 14.7 45.3 60.0 4.0 27.3 67.5 5.2 5.2
Religion
Hindu 21.5 53.7 33.6 5.6 39.0 64.7 9.2 3.2
Muslim 14.3 71.4 9.5 4.8 18.5 51.9 3.7 25.9
Others 9.7 37.1 64.5 6.5 27.3 77.3 0.0 0.0
MPCE
MPCE quintile 1
(Lowest)
27.3 37.9 62.1 4.6 41.5 71.7 3.8 1.9
MPCE quintile 2 8.5 50.9 42.4 5.1 33.3 63.3 10.0 5.0
MPCE quintile 3 17.5 58.7 27.0 7.9 33.9 69.6 5.4 3.6
MPCE quintile 4 24.0 54.0 22.0 8.0 39.1 62.3 8.7 1.5
MPCE quintile 5 (Higher) 15.3 57.6 33.9 3.4 33.3 56.7 11.7 13.3
Total 18.5 51.5 38.4 5.7 36.2 64.4 8.1 5.0

Page | 90
Appendix 15. Source of awareness about s RSBY scheme by selected background characteristics in West
Bengal
Intervention District Non-Intervention District
Background
Characteristics
Frien
ds/
Relat
ives/
Neig
hbors
Teach
er/
Panch
ayat/
ANM
/
AW
W
PACS
interve
ntions
MLA/P
olitical
leader
TV/
Radio/
Other
Source
s
Friend
s/
Relati
ves/
Neigh
bours
Teach
er/
Panac
hayat/
ANM/
AWW
Mass
Medi
a
Cam
paign
SH
G/
N
G
O
ML
A/
Polit
ical
lead
er
TV/
Rad
io/
Oth
er
Sou
rces
Highest
education
Illiterate 27.7 10.8 51.8 16.9 7.2 12.2 9.4 51.4 9.4 30.8 7.5
Primary
completed
20.7 12.0 54.4 12.0 12.0 24.7 15.3 40.0 4.0 28.7 6.0
Secondary
completed
23.6 2.8 45.8 27.8 8.3 15.9 10.2 29.6 1.1 37.5 4.6
Higher
secondary
28.6 19.1 76.2 9.5 2.4 8.6 10.3 48.3 5.2 22.4 12.1
Higher
secondary &
above
20.0 5.0 65.0 5.0 15.0 15.6 6.7 55.6 0.0 28.9 4.4
Caste
General/OBC 24.0 8.3 48.4 20.8 8.9 16.9 7.2 40.0 2.6 38.0 7.7
Scheduled
Castes
33.3 8.3 52.0 16.7 8.3 15.1 12.9 45.3 6.5 25.0 6.5
Scheduled
Tribes
21.0 14.8 76.5 4.9 8.6 38.1 33.3 52.4 0.0 14.3 0.0
Religion
Hindu 24.7 8.6 64.5 10.8 7.5 15.9 11.9 42.1 4.9 31.0 6.5
Muslim 24.4 9.4 47.2 21.1 8.3 22.4 9.2 48.7 2.6 26.3 7.9
Others 22.2 16.7 72.2 5.6 13.9 0.0 0.0 100.0 0.0 0.0 0.0
MPCE
MPCE quintile 1 19.1 5.9 58.5 14.7 8.8 10.7 9.5 52.4 7.1 28.6 6.0
MPCE quintile 2 23.2 5.4 57.1 10.7 7.1 23.2 9.5 43.2 3.2 26.3 6.3
MPCE quintile 3 23.0 8.2 65.6 13.1 13.1 16.5 15.4 42.9 3.3 26.4 8.8
MPCE quintile 4 31.8 19.7 43.9 19.7 9.1 16.5 11.8 38.8 4.7 31.8 7.1
MPCE quintile 5 24.1 10.3 63.8 22.4 5.2 17.2 10.8 39.8 4.3 37.6 5.4
Total 24.3 10.0 55.3 16.2 8.7 17.0 11.4 43.3 4.5 30.1 6.7

Page | 91

Imact Assessement Study on RSBY
Page | 92
Appendix 16. Source of awareness about s RSBY scheme by selected background characteristics in Jharkhand
Intervention District Non-Intervention District
Backgroun
d
Characteris
tics
Mike
Anno
uncem
ent
Ralli
es/
Proc
essio
ns
Ta
ble
au
Vide
o/Fil
m
Sho
ws
Pu
pp
et
Sh
o
ws
Dra
ma/
Plays
/Stre
ets
Play
Fo
lk
so
ng
s/
Ar
t
W
all
wri
tin
g/
Po
ste
rs
Mike
Anno
uncem
ent
Ralli
es/
Proc
essio
ns
Ta
ble
au
Vide
o/Fil
m
Sho
ws
Pu
pp
et
Sh
o
ws
Dra
ma/
Plays
/Stre
ets
Play
Fo
lk
so
ng
s/
Ar
t
W
all
wri
tin
g/
Po
ste
rs
Highest
education
level
Illiterate 15.8 5.3 0.0 0.0 0.
0
10.5 5.
3
10.
5
6.9 0.0 0.0 0.0 0.
0
3.4 0.
0
0.0
Primary
completed
28.2 2.6 0.0 0.0 0.
0
10.3 2.
6
5.1 5.3 0.0 0.0 0.0 0.
0
2.6 0.
0
0.0
Secondary
completed
38.3 0.8 0.0 0.0 0.
0
5.8 0.
8
8.3 3.2 0.0 0.0 0.0 0.
0
0.0 0.
0
0.0
Higher
secondary
38.4 1.4 0.0 0.0 0.
0
12.3 4.
1
13.
7
5.1 0.0 0.0 0.0 0.
0
1.7 0.
0
3.4
Higher
secondary &
above
28.3 2.2 0.0 0.0 0.
0
6.5 2.
2
17.
4
6.4 1.3 0.0 0.0 0.
0
0.0 0.
0
1.3
Caste
General/OB
C
35.3 1.7 0.0 0.0 0.
0
6.9 2.
9
11.
0
3.8 0.6 0.0 0.0 0.
0
0.0 0.
0
0.6
Scheduled
Castes
55.1 4.1 0.0 0.0 0.
0
8.2 4.
1
20.
4
3.2 0.0 0.0 0.0 0.
0
1.6 0.
0
0.0
Scheduled
Tribes
17.3 0.0 0.0 0.0 0.
0
12.0 0.
0
4.0 9.1 0.0 0.0 0.0 0.
0
2.6 0.
0
2.6
Religion
Hindu 41.6 2.3 0.0 0.0 0.
0
8.4 3.
3
13.
6
5.2 0.4 0.0 0.0 0.
0
0.8 0.
0
1.2
Muslims 19.0 0.0 0.0 0.0 0.
0
0.0 0.
0
4.8 7.4 0.0 0.0 0.0 0.
0
3.7 0.
0
0.0
Others 12.9 0.0 0.0 0.0 0.
0
11.3 0.
0
3.2 0.0 0.0 0.0 0.0 0.
0
0.0 0.
0
0.0
MPCE
MPCE
quintile 1
(Lowest)
13.6 1.5 0.0 0.0 0.
0
18.2 1.
5
9.1 1.9 0.0 0.0 0.0 0.
0
0.0 0.
0
0.0
MPCE
quintile 2
30.5 0.0 0.0 0.0 0.
0
8.5 3.
4
5.1 6.7 0.0 0.0 0.0 0.
0
0.0 0.
0
0.0
MPCE
quintile 3
47.6 0.0 0.0 0.0 0.
0
1.6 0.
0
9.5 7.1 0.0 0.0 0.0 0.
0
1.8 0.
0
3.6
MPCE
quintile 4
44.0 4.0 0.0 0.0 0.
0
6.0 4.
0
18.
0
4.3 1.4 0.0 0.0 0.
0
1.4 0.
0
1.4
MPCE
quintile 5
(Higher)
37.3 3.4 0.0 0.0 0.
0
6.8 3.
4
13.
6
5.0 0.0 0.0 0.0 0.
0
1.7 0.
0
0.0
Media
Exposure
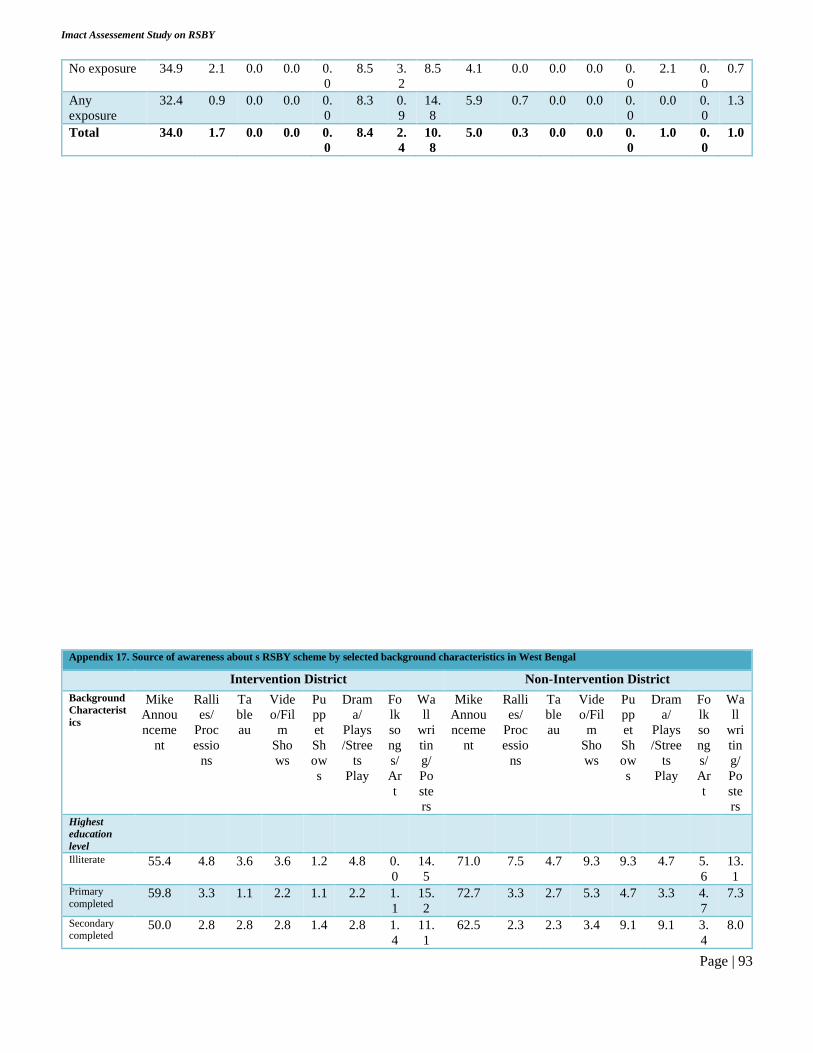
Imact Assessement Study on RSBY
Page | 93
No exposure 34.9 2.1 0.0 0.0 0.
0
8.5 3.
2
8.5 4.1 0.0 0.0 0.0 0.
0
2.1 0.
0
0.7
Any
exposure
32.4 0.9 0.0 0.0 0.
0
8.3 0.
9
14.
8
5.9 0.7 0.0 0.0 0.
0
0.0 0.
0
1.3
Total 34.0 1.7 0.0 0.0 0.
0
8.4 2.
4
10.
8
5.0 0.3 0.0 0.0 0.
0
1.0 0.
0
1.0
Appendix 17. Source of awareness about s RSBY scheme by selected background characteristics in West Bengal
Intervention District Non-Intervention District
Background
Characterist
ics
Mike
Annou
nceme
nt
Ralli
es/
Proc
essio
ns
Ta
ble
au
Vide
o/Fil
m
Sho
ws
Pu
pp
et
Sh
ow
s
Dram
a/
Plays
/Stree
ts
Play
Fo
lk
so
ng
s/
Ar
t
Wa
ll
wri
tin
g/
Po
ste
rs
Mike
Annou
nceme
nt
Ralli
es/
Proc
essio
ns
Ta
ble
au
Vide
o/Fil
m
Sho
ws
Pu
pp
et
Sh
ow
s
Dram
a/
Plays
/Stree
ts
Play
Fo
lk
so
ng
s/
Ar
t
Wa
ll
wri
tin
g/
Po
ste
rs Highest
education
level
Illiterate 55.4 4.8 3.6 3.6 1.2 4.8 0.
0
14.
5
71.0 7.5 4.7 9.3 9.3 4.7 5.
6
13.
1 Primary
completed 59.8 3.3 1.1 2.2 1.1 2.2 1.
1
15.
2
72.7 3.3 2.7 5.3 4.7 3.3 4.
7
7.3
Secondary completed
50.0 2.8 2.8 2.8 1.4 2.8 1.
4
11.
1
62.5 2.3 2.3 3.4 9.1 9.1 3.
4
8.0

Imact Assessement Study on RSBY
Page | 94
Higher secondary
57.1 11.9 9.5 9.5 2.4 9.5 2.
4
31.
0
65.5 0.0 0.0 1.7 1.7 1.7 0.
0
3.4
Higher secondary &
above
55.0 10.0 5.0 5.0 0.0 5.0 5.
0
35.
0
77.8 0.0 0.0 6.7 2.2 2.2 2.
2
4.4
Caste General/OB
C 52.6 3.6 2.6 4.7 1.0 3.1 0.
5
10.
9
68.7 0.5 1.0 2.6 2.6 2.1 1.
5
7.2
Scheduled
Castes 63.9 5.6 5.6 5.6 2.8 2.8 2.
8
19.
4
71.6 6.0 3.9 8.6 9.5 6.9 5.
6
9.5
Scheduled
Tribes 59.3 8.6 4.9 1.2 1.2 7.4 2.
5
32.
1
61.9 0.0 0.0 0.0 0.0 0.0 4.
8
0.0
Religion Hindu 57.0 8.6 3.2 2.2 2.2 5.4 2.
2
25.
8
68.5 4.0 2.7 6.5 7.0 5.1 4.
3
8.1
Muslims 52.8 2.8 2.8 5.6 1.1 3.9 0.
6
11.
7
76.3 0.0 1.3 1.3 1.3 1.3 1.
3
7.9
Others 66.7 8.3 8.3 0.0 0.0 2.8 2.
8
25.
0
100.0 0.0 0.0 0.0 0.0 0.0 0.
0
0.0
MPCE MPCE
quintile 1 (Lowest)
47.1 2.9 2.9 10.3 1.5 5.9 0.
0
16.
2
69.0 7.1 4.8 4.8 8.3 4.8 4.
8
9.5
MPCE
quintile 2 58.9 5.4 5.4 1.8 0.0 3.6 0.
0
10.
7
60.0 4.2 2.1 4.2 5.3 4.2 3.
2
12.
6 MPCE
quintile 3 55.7 3.3 1.6 3.3 3.3 8.2 3.
3
23.
0
70.3 4.4 4.4 11.0 4.4 3.3 3.
3
5.5
MPCE
quintile 4 48.5 4.5 3.0 1.5 1.5 1.5 1.
5
18.
2
76.5 0.0 0.0 0.0 3.5 2.4 3.
5
5.9
MPCE
quintile 5 (Higher)
70.7 10.3 5.2 1.7 0.0 1.7 1.
7
19.
0
74.2 1.1 1.1 7.5 8.6 7.5 4.
3
6.5
Media
Exposure
No
exposure 59.8 4.7 3.6 3.0 0.0 3.6 0.
0
13.
0
67.3 3.0 2.3 4.6 4.6 3.0 3.
8
6.5
Any
exposure 50.7 5.7 3.6 5.0 2.9 5.0 2.
9
22.
9
73.5 3.8 2.7 7.0 8.1 6.5 3.
8
10.
3 Total 55.7 5.2 3.6 3.9 1.3 4.2 1.
3
17.
5
69.9 3.3 2.5 5.6 6.0 4.5 3.
8
8.0

Imact Assessement Study on RSBY
Page | 95
Appendix 18. Frequency of awareness programmers about RSBY scheme by selected background characteristics
Jharkhand West Bengal
Intervention District Non-Intervention
District
Intervention District Non-Intervention
District
Background
Characteristics
Tw
ice
or
mo
re
in
eve
ry
2
mo
nth
Mo
re
tha
n 2
mo
nth
s
On
ce/
twi
ce
in
a
ye
ar
Do
n't
Kn
ow
Tw
ice
or
mo
re
in
eve
ry
2
mo
nth
Mo
re
tha
n 2
mo
nth
s
On
ce/
twi
ce
in
a
ye
ar
Do
n't
Kn
ow
Tw
ice
or
mo
re
in
eve
ry
2
mo
nth
Mo
re
tha
n 2
mo
nth
s
Once/
twice
in a
year
Do
n't
Kn
ow
Tw
ice
or
mo
re
in
eve
ry
2
mo
nth
Mo
re
tha
n 2
mo
nth
s
Once/
twice
in a
year
Do
n't
Kn
ow
Highest
education level
Illiterate 16.
7
25.0 0.0 58.
3
0.0 17.7 0.0 82.
4
5.8 0.0 43.5 50.
7
2.2 0.0 35.5 62.
4
Primary
completed
5.3 26.3 10.
5
57.
9
0.0 15.4 15.
4
69.
2
7.4 1.5 38.2 52.
9
3.5 0.0 39.1 57.
4
Secondary
completed
10.
3
11.5 3.9 74.
4
8.0 16.0 12.
0
64.
0
5.0 3.3 31.7 60.
0
7.3 0.0 39.1 53.
6
Higher
secondary
9.8 17.7 5.9 66.
7
0.0 14.3 0.0 85.
7
5.6 16.7 55.6 22.
2
0.0 0.0 59.1 40.
9
Higher
secondary &
above
10.
7
25.0 0.0 64.
3
10.
0
20.0 10.
0
60.
0
11.
8
0.0 35.3 52.
9
4.9 2.4 41.5 51.
2
Caste
General/OBC 5.9 14.9 2.0 77.
2
5.1 35.9 12.
8
46.
2
5.2 1.3 36.0 57.
5
6.6 0.0 43.5 50.
0
Scheduled
Castes
2.9 11.8 0.0 85.
3
0.0 3.7 0.0 96.
3
10.
7
7.1 28.6 53.
6
1.1 0.6 39.9 58.
4
Scheduled
Tribes
22.
6
26.4 11.
3
39.
6
8.7 0.0 8.7 82.
6
7.3 7.3 55.1 30.
4
0.0 0.0 25.0 75.
0
Religion

Imact Assessement Study on RSBY
Page | 96
Hindu 6.3 13.9 2.1 77.
8
5.2 19.5 9.1 66.
2
13.
3
5.3 49.3 32.
0
2.4 0.3 42.3 55.
0
Muslims 0.0 0.0 0.0 10
0.0
0.0 0.0 0.0 10
0.0
4.1 1.4 33.8 60.
7
9.5 0.0 34.9 55.
6
Others 25.
6
33.3 12.
8
28.
2
0.0 0.0 0.0 10
0.0
0.0 10.0 50.0 40.
0
0.0 0.0 0.0 10
0.0
MPCE
MPCE quintile
1 (Lowest)
18.
4
24.5 6.1 51.
0
0.0 26.3 5.3 68.
4
10.
6
6.4 36.2 46.
8
4.3 1.4 40.0 54.
3
MPCE quintile
2
11.
8
14.7 8.8 64.
7
7.1 35.7 14.
3
42.
9
11.
4
2.3 50.0 36.
4
2.9 0.0 38.6 58.
6
MPCE quintile
3
4.8 19.1 2.4 73.
8
5.9 5.9 17.
7
70.
6
3.6 1.8 32.7 61.
8
1.4 0.0 35.6 63.
0
MPCE quintile
4
6.9 3.5 0.0 89.
7
9.1 9.1 4.6 77.
3
0.0 3.8 39.6 56.
6
4.2 0.0 45.8 50.
0
MPCE quintile
5 (Higher)
5.9 20.6 2.9 70.
6
0.0 11.8 0.0 88.
2
7.8 3.9 45.1 43.
1
5.2 0.0 44.2 50.
7
Media
Exposure
No exposure 6.1 16.5 4.4 73.
0
4.0 18.0 6.0 72.
0
4.5 1.5 37.6 56.
4
4.3 0.5 40.0 55.
2
Any exposure 16.
4
19.2 4.1 60.
3
5.1 15.4 10.
3
69.
2
8.6 6.0 43.6 41.
9
2.6 0.0 42.1 55.
3
Total 10.
1
17.6 4.3 68.
1
4.5 16.9 7.9 70.
8
6.4 3.6 40.4 49.
6
3.6 0.3 40.9 55.
3

Imact Assessement Study on RSBY
Page | 97
Appendix 19. Source of encouragement for enrolling in RSBY scheme by selected background characteristics in
Jharkhand
Background
Characteristics
Intervention District Non-Intervention District
Self
Motiv
ated
Friend
s/
Relativ
es/
Neigh
bors
Teach
er/
ASH
A/
AW
W/
Panca
yat
RSB
Y-
Mitr
a
MLA
/
Politi
cal
leade
r
Othe
r
Sour
ces
Self
Motiv
ated
Friend
s/
Relativ
es/
Neigh
bors
Teach
er/
ASH
A/
AW
W/
Panca
yat
NG
Os/
SH
Gs
MLA
/
Politi
cal
leade
r
Othe
r
Sour
ces
Highest education
level
Illiterate 5.3 26.3 36.8 52.6 0.0 0.0 6.9 48.3 51.7 10.4 3.5 0.0
Primary completed 10.3 35.9 46.2 41.0 0.0 2.6 10.5 39.5 57.9 13.2 0.0 5.3
Secondary
completed
8.3 39.2 57.5 25.8 3.3 6.7 13.8 46.8 52.1 5.3 5.3 1.1
Higher secondary 5.5 28.8 49.3 43.8 2.7 1.4 11.9 47.5 55.9 1.7 1.7 3.4
Higher secondary &
above
6.5 32.6 47.8 45.7 0.0 4.4 11.5 48.7 64.1 7.7 2.6 2.6
Caste
General/OBC 8.7 35.3 51.5 28.3 2.3 4.6 12.6 42.8 61.6 10.7 3.1 1.3
Scheduled Castes 4.1 42.9 63.3 22.5 2.0 2.0 11.3 61.3 37.1 4.8 1.6 1.6
Scheduled Tribes 6.7 26.7 42.7 66.7 1.3 4.0 10.4 42.9 62.3 0.0 3.9 5.2
Religion
Hindu 7.5 38.3 52.3 32.2 2.8 4.2 10.0 48.6 57.4 8.0 2.8 1.6
Muslims 4.8 28.6 66.7 0.0 0.0 29.6 11.1 55.6 0.0 0.0 3.7
Others 8.1 22.6 41.9 66.1 0.0 4.8 9.1 68.2 50.0 0.0 9.1 9.1
MPCE
MPCE quintile 1
(Lowest)
4.6 37.9 48.5 68.2 4.6 4.6 9.4 56.6 56.6 7.6 5.7 3.8
MPCE quintile 2 6.8 28.8 49.2 44.1 3.4 1.7 13.3 50.0 63.3 5.0 3.3 0.0
MPCE quintile 3 6.4 33.3 54.0 23.8 1.6 6.4 10.7 44.6 62.5 5.4 1.8 0.0
MPCE quintile 4 10.0 44.0 48.0 18.0 0.0 2.0 8.7 47.8 52.2 10.2 1.5 4.4
MPCE quintile 5
(Higher)
10.2 28.8 55.9 25.4 0.0 5.1 16.7 35.0 50.0 5.0 3.3 3.3
Media Exposure
No exposure 8.5 36.5 51.9 33.3 2.7 3.2 12.3 50.0 52.1 5.5 2.1 0.7
Any exposure 5.6 30.6 50.0 43.5 0.9 5.6 11.2 43.4 61.2 7.9 4.0 4.0
Total 7.4 34.3 51.2 37.0 2.0 4.0 11.7 46.6 56.7 6.7 3.0 2.4

Imact Assessement Study on RSBY
Page | 98
Appendix 20. Source of encouragement for enrolling in RSBY scheme by selected background characteristics in
Jharkhand
Background
Characteristics
Intervention District Non-Intervention District
Self
Motiv
ated
Friend
s/
Relati
ves/
Neigh
bors
Teac
her/
ASH
A/
AW
W/
Panc
ayat
RSB
Y-
Mit
ra
ML
A/
Politi
cal
leade
r
Othe
r
Sour
ces
Self
Motiv
ated
Friend
s/
Relati
ves/
Neigh
bors
Teach
er/
ASH
A/
AW
W/
Panca
yat
RSB
Y-
Mit
ra
ML
A/
Politi
cal
leade
r
Othe
r
Sour
ces
Highest education
level
Illiterate 5.3 26.3 36.8 52.6 0.0 0.0 6.9 48.3 51.7 10.4 3.5 0.0
Primary completed 10.3 35.9 46.2 41.0 0.0 2.6 10.5 39.5 57.9 13.2 0.0 5.3
Secondary
completed
8.3 39.2 57.5 25.8 3.3 6.7 13.8 46.8 52.1 5.3 5.3 1.1
Higher secondary 5.5 28.8 49.3 43.8 2.7 1.4 11.9 47.5 55.9 1.7 1.7 3.4
Higher secondary
& above
6.5 32.6 47.8 45.7 0.0 4.4 11.5 48.7 64.1 7.7 2.6 2.6
Caste
General/OBC 8.7 35.3 51.5 28.3 2.3 4.6 12.6 42.8 61.6 10.7 3.1 1.3
Scheduled Castes 4.1 42.9 63.3 22.5 2.0 2.0 11.3 61.3 37.1 4.8 1.6 1.6
Scheduled Tribes 6.7 26.7 42.7 66.7 1.3 4.0 10.4 42.9 62.3 0.0 3.9 5.2
Religion
Hindu 7.5 38.3 52.3 32.2 2.8 4.2 10.0 48.6 57.4 8.0 2.8 1.6
Muslims 4.8 28.6 66.7 0.0 0.0 29.6 11.1 55.6 0.0 0.0 3.7

Imact Assessement Study on RSBY
Page | 99
Others 8.1 22.6 41.9 66.1 0.0 4.8 9.1 68.2 50.0 0.0 9.1 9.1
MPCE
MPCE quintile 1
(Lowest)
4.6 37.9 48.5 68.2 4.6 4.6 9.4 56.6 56.6 7.6 5.7 3.8
MPCE quintile 2 6.8 28.8 49.2 44.1 3.4 1.7 13.3 50.0 63.3 5.0 3.3 0.0
MPCE quintile 3 6.4 33.3 54.0 23.8 1.6 6.4 10.7 44.6 62.5 5.4 1.8 0.0
MPCE quintile 4 10.0 44.0 48.0 18.0 0.0 2.0 8.7 47.8 52.2 10.2 1.5 4.4
MPCE quintile 5
(Higher)
10.2 28.8 55.9 25.4 0.0 5.1 16.7 35.0 50.0 5.0 3.3 3.3
Media Exposure
No exposure 8.5 36.5 51.9 33.3 2.7 3.2 12.3 50.0 52.1 5.5 2.1 0.7
Any exposure 5.6 30.6 50.0 43.5 0.9 5.6 11.2 43.4 61.2 7.9 4.0 4.0
Total 7.4 34.3 51.2 37.0 2.0 4.0 11.7 46.6 56.7 6.7 3.0 2.4
Appendix 21. Who informed about the entire enrolment process of RSBY scheme by selected background characteristics in
Jharkhand
Intervention District Non-Intervention District

Imact Assessement Study on RSBY
Page | 100
Background
Characteristics
Self
Moti
vated
Frien
ds/
Relat
ives/
Neig
hbor
s
Teache
r/
ASHA/
AWW/
Pancha
yat
Mass
Medi
a
Cam
paign
SHG
/
PAC
S-
Mob
ilizer
ML
A/
Poli
tical
lead
er
Oth
er
Sou
rces
Self
Moti
vated
Frien
ds/
Relat
ives/
Neig
hbor
s
Teache
r/
ASHA/
AWW/
Pancha
yat
Mass
Medi
a
Cam
paign
SHG
/
PAC
S-
Mob
ilizer
ML
A/
Poli
tical
lead
er
Oth
er
Sou
rces
Highest
education level
Illiterate 0.0 21.1 31.6 0.0 52.6 0.0 0.0 3.5 51.7 51.7 3.5 6.9 0.0 0.0
Primary
completed
7.7 33.3 46.2 0.0 41.0 0.0 2.6 5.3 34.2 63.2 2.6 5.3 2.6 7.9
Secondary
completed
4.2 36.7 56.7 0.0 25.8 5.0 6.7 6.4 46.8 53.2 0.0 6.4 4.3 1.1
Higher
secondary
4.1 23.3 46.6 0.0 49.3 4.1 1.4 3.4 44.1 55.9 0.0 1.7 0.0 8.5
Higher
secondary &
above
2.2 28.3 45.7 0.0 50.0 4.4 6.5 2.6 47.4 65.4 3.9 6.4 2.6 2.6
Caste
General/OBC 4.1 31.2 49.1 0.0 30.6 2.9 5.2 5.7 41.5 61.6 2.5 8.8 1.9 4.4
Scheduled
Castes
2.0 38.8 61.2 0.0 22.5 6.1 2.0 6.5 59.7 38.7 1.6 3.2 3.2 3.2
Scheduled
Tribes
5.3 24.0 42.7 0.0 69.3 4.0 4.0 0.0 41.6 66.2 0.0 0.0 2.6 2.6
Religion
Hindu 4.2 34.6 50.5 0.0 34.1 4.7 4.7 4.4 47.4 58.6 2.0 6.4 2.4 1.6
Muslims 0.0 28.6 66.7 0.0 0.0 0.0 0.0 7.4 11.1 55.6 0.0 0.0 0.0 18.5
Others 4.8 17.7 40.3 0.0 69.4 1.6 4.8 0.0 63.6 54.6 0.0 0.0 4.6 9.1
MPCE
MPCE quintile
1 (Lowest)
3.0 28.8 42.4 0.0 68.2 10.6 4.6 1.9 56.6 58.5 1.9 3.8 3.8 3.8
MPCE quintile
2
3.4 22.0 49.2 0.0 47.5 5.1 1.7 6.7 45.0 68.3 1.7 3.3 1.7 0.0
MPCE quintile
3
1.6 33.3 54.0 0.0 25.4 1.6 7.9 5.4 44.6 62.5 0.0 3.6 0.0 1.8
MPCE quintile
4
4.0 42.0 46.0 0.0 20.0 0.0 2.0 2.9 44.9 53.6 2.9 10.1 2.9 2.9
MPCE quintile
5 (Higher)
8.5 28.8 55.9 0.0 28.8 0.0 5.1 5.0 36.7 48.3 1.7 5.0 3.3 10.0
Media
Exposure
No exposure 4.2 32.8 49.2 0.0 34.4 4.2 3.7 4.1 48.6 52.7 0.7 4.8 2.1 3.4
Any exposure 3.7 26.9 50.0 0.0 47.2 2.8 5.6 4.6 42.1 63.2 2.6 5.9 2.6 4.0
Total 4.0 30.6 49.5 0.0 39.1 3.7 4.4 4.4 45.3 58.1 1.7 5.4 2.4 3.7

Imact Assessement Study on RSBY
Page | 101
Appendix 22. Who informed about the entire enrolment process of RSBY scheme by selected background
characteristics in West Bengal
Backgroun
d
Characteris
tics
Intervention District Non-Intervention District
Self
Mot
ivat
ed
Frie
nds/
Rel
ativ
es/
Nei
ghb
ors
Teacher/
ASHA/A
WW/Panc
hayat
Mas
s
Med
ia
Ca
mpa
ign
SH
G/
PA
CS-
Mo
bili
zer
M
LA
/
Pol
itic
al
lea
der
Ot
her
So
urc
es
Self
Mot
ivat
ed
Frie
nds/
Rel
ativ
es/
Nei
ghb
ors
Teacher/
ASHA/A
WW/Panc
hayat
Mas
s
Med
ia
Ca
mpa
ign
SH
G/
PA
CS-
Mo
bili
zer
M
LA
/
Pol
itic
al
lea
der
Ot
her
So
urc
es
Highest
education
level
Illiterate 1.2 2.4 9.6 0.0 4.8 3.6 2.4 0.9 12.2 17.8 0.0 2.8 11.
2
0.0
Primary
completed
3.3 9.8 8.7 0.0 6.5 5.4 3.3 4.0 5.3 9.3 0.0 1.3 8.0 0.7
Secondary
completed
1.4 5.6 5.6 0.0 8.3 2.8 6.9 2.3 3.4 10.2 1.1 1.1 14.
8
3.4
Higher
secondary
0.0 14.3 4.8 0.0 9.5 4.8 0.0 1.7 8.6 19.0 0.0 3.5 12.
1
1.7
Higher
secondary &
above
10.0 5.0 10.0 5.0 15.0 0.0 5.0 8.9 8.9 31.1 0.0 0.0 8.9 0.0
Caste
General/OB
C
1.0 4.7 6.3 0.0 3.1 2.1 5.2 2.6 7.2 16.4 0.5 1.5 13.
3
1.5
Scheduled
Castes
0.0 5.6 2.8 0.0 8.3 2.8 0.0 1.7 6.9 14.2 0.0 2.2 8.6 0.9
Scheduled
Tribes
6.2 13.6 13.6 1.2 17.3 8.6 1.2 23.8 14.3 9.5 0.0 0.0 9.5 0.0

Imact Assessement Study on RSBY
Page | 102
Religion
Hindu 3.2 11.8 12.9 0.0 16.1 6.5 1.1 3.5 7.0 13.8 0.3 2.2 11.
9
1.4
Muslims 0.6 3.9 6.7 0.0 2.2 2.2 5.6 1.3 9.2 19.7 0.0 0.0 5.3 0.0
Others 8.3 11.1 0.0 2.8 11.1 5.6 0.0 0.0 0.0 100.0 0.0 0.0 0.0 0.0
MPCE
MPCE
quintile 1
(Lowest)
2.9 4.4 4.4 0.0 2.9 1.5 1.5 3.6 10.7 26.2 1.2 1.2 16.
7
0.0
MPCE
quintile 2
1.8 5.4 8.9 0.0 3.6 7.1 1.8 4.2 4.2 14.7 0.0 3.2 13.
7
2.1
MPCE
quintile 3
3.3 4.9 9.8 0.0 6.6 4.9 3.3 2.2 4.4 7.7 0.0 0.0 5.5 1.1
MPCE
quintile 4
1.5 9.1 6.1 0.0 12.1 1.5 9.1 3.5 9.4 12.9 0.0 1.2 7.1 2.4
MPCE
quintile 5
(Higher)
1.7 12.1 10.3 1.7 12.1 5.2 1.7 2.2 8.6 14.0 0.0 3.2 10.
8
0.0
Media
Exposure
No exposure 2.4 4.7 7.1 0.6 4.1 3.6 1.2 2.7 6.5 13.7 0.4 1.5 12.
2
0.0
Any
exposure
2.1 10.0 8.6 0.0 11.4 4.3 6.4 3.8 8.7 16.8 0.0 2.2 8.7 2.7
Total 2.3 7.1 7.8 0.3 7.4 3.9 3.6 3.1 7.4 15.0 0.2 1.8 10.
7
1.1

Imact Assessement Study on RSBY
Page | 103
Appendix 23. Anyone helped during the RSBY enrolment process by selected background characteristics
Jharkhand West Bengal
Intervention District Non-Intervention
District
Intervention District Non-Intervention District
Background
Characteristic
s
Sma
rt
car
d
pro
vide
r
PACS
Interv
ention
s
No
bod
y
Ot
her
s
Sma
rt
car
d
pro
vide
r
NG
Os/
SH
Gs
No
bod
y
Ot
her
s
Sma
rt
car
d
pro
vide
r
PACS
Interv
ention
s
No
bod
y
Ot
her
s
Sma
rt
car
d
pro
vide
r
NGOs
/SHGs
No
bod
y
Ot
her
s
Highest
education level
Illiterate 0.0 37.5 56.
3
6.3 4.0 0.0 96.
0
0.0 0.0 5.6 44.
4
55.
6
2.9 5.9 58.
8
38.
2
Primary
completed
0.0 31.4 65.
7
2.9 0.0 0.0 91.
7
8.3 12.0 24.0 40.
0
40.
0
5.6 0.0 58.
3
36.
1
Secondary
completed
1.0 21.0 73.
3
4.8 0.0 2.4 88.
1
9.5 0.0 25.0 37.
5
50.
0
4.0 0.0 64.
0
32.
0
Higher
secondary
3.0 42.4 54.
6
0.0 0.0 0.0 92.
2
7.8 12.5 50.0 25.
0
25.
0
11.8 0.0 52.
9
35.
3
Higher
secondary &
above
0.0 36.6 51.
2
12.
2
0.0 1.5 94.
1
4.4 0.0 33.3 33.
3
33.
3
5.6 0.0 61.
1
33.
3
Caste
General/OBC 0.7 21.7 73.
7
4.0 0.7 2.1 90.
2
7.0 2.6 13.2 42.
1
50.
0
8.8 0.0 50.
9
40.
4
Scheduled
Castes
0.0 20.9 79.
1
0.0 0.0 0.0 94.
6
5.5 0.0 40.0 40.
0
40.
0
3.1 3.1 67.
2
29.
7
Scheduled
Tribes
2.9 58.8 29.
4
8.8 0.0 0.0 92.
4
7.6 10.0 33.3 33.
3
36.
7
0.0 0.0 55.
6
44.
4
Religion
Hindu 0.5 22.4 71.
9
5.2 0.5 1.4 90.
5
7.7 10.0 40.0 30.
0
43.
3
5.5 1.8 64.
6
30.
0
Muslims 0.0 0.0 100
.0
0.0 0.0 0.0 100
.0
0.0 2.9 11.4 45.
7
42.
9
5.3 0.0 31.
6
63.
2
Others 3.6 70.9 21.
8
3.6 0.0 0.0 94.
7
5.3 0.0 12.5 37.
5
50.
0
0.0 0.0 0.0 100
.0
MPCE

Imact Assessement Study on RSBY
Page | 104
MPCE quintile
1 (Lowest)
4.9 39.3 44.
3
11.
5
2.1 2.1 87.
2
8.5 0.0 0.0 40.
0
70.
0
9.1 0.0 8.0 6.7
MPCE quintile
2
0.0 45.5 50.
9
3.6 0.0 0.0 88.
5
11.
5
7.7 7.7 53.
9
30.
8
27.3 23.5 28.
0
25.
3
MPCE quintile
3
0.0 29.1 69.
1
1.8 0.0 0.0 90.
0
10.
0
7.1 21.4 35.
7
42.
9
0.0 0.0 0.0 6.7
MPCE quintile
4
0.0 14.6 82.
9
2.4 0.0 0.0 96.
8
3.2 10.0 30.0 25.
0
40.
0
45.5 70.6 56.
0
132
.0
MPCE quintile
5 (Higher)
0.0 21.6 76.
5
2.0 0.0 3.8 94.
3
1.9 0.0 43.8 43.
8
43.
8
18.2 5.9 8.0 36.
0
Media
Exposure
No exposure 0.6 27.8 67.
5
4.1 0.8 0.0 90.
1
9.2 6.5 9.7 51.
6
38.
7
5.6 1.4 60.
6
33.
8
Any exposure 2.1 37.2 55.
3
5.3 0.0 2.3 93.
2
4.5 4.8 33.3 28.
6
47.
6
5.1 1.7 57.
6
37.
3
Total 1.1 31.2 63.
1
4.6 0.4 1.1 91.
7
6.8 5.5 23.3 38.
4
43.
8
5.4 1.5 59.
2
35.
4
Appendix 24. Post RSBY enrolment visit by selected background characteristics
Jharkhand West Bengal
Intervention District Non-intervention
District
Intervention District Non-Intervention
District

Imact Assessement Study on RSBY
Page | 105
Background
Characteristics
Nobo
dy
PACS
initiati
ves
Oth
ers
Nobo
dy
NG
Os/
SH
Gs
Oth
ers
Nobo
dy
PACS
initiati
ves
Oth
ers
Nobo
dy
NGOs/S
HGs
Oth
ers
Highest education
level
Illiterate 53.3 46.7 0.0 95.2 4.8 0.0 66.7 20.0 40.0 67.9 0.0 32.1
Primary completed 62.5 34.4 3.1 96.6 0.0 3.5 65.4 23.1 19.2 66.7 10.0 23.3
Secondary
completed
80.9 18.1 1.1 97.0 3.0 0.0 69.2 23.1 7.7 52.2 4.4 43.5
Higher secondary 55.4 39.3 5.4 100.0 0.0 0.0 22.2 55.6 55.6 69.2 0.0 30.8
Higher secondary &
above
60.0 36.7 3.3 98.2 1.9 0.0 33.3 33.3 33.3 43.8 6.3 50.0
Caste
General/OBC 75.5 22.3 2.2 95.6 3.5 0.9 75.6 7.3 26.8 51.9 1.9 46.2
Scheduled Castes 86.5 13.5 0.0 100.0 0.0 0.0 50.0 50.0 0.0 67.9 7.6 24.5
Scheduled Tribes 31.4 62.8 5.9 100.0 0.0 0.0 27.3 45.5 36.4 80.0 0.0 20.0
Religion
Hindu 76.2 21.5 2.3 97.2 2.3 0.6 32.0 48.0 36.0 62.8 5.3 31.9
Muslims 100.0 0.0 0.0 100.0 0.0 0.0 79.0 5.3 21.1 46.7 0.0 53.3
Others 15.4 79.5 5.1 100.0 0.0 0.0 33.3 33.3 33.3 100.0 0.0 0.0
MPCE
MPCE quintile 1
(Lowest)
46.3 48.2 5.6 100.0 0.0 0.0 83.3 0.0 16.7 60.7 3.6 35.7
MPCE quintile 2 62.2 37.8 0.0 100.0 0.0 0.0 61.5 0.0 46.2 62.5 4.2 33.3
MPCE quintile 3 79.2 20.8 0.0 97.4 0.0 2.6 44.4 22.2 33.3 62.5 12.5 25.0
MPCE quintile 4 84.2 15.8 0.0 95.5 4.6 0.0 54.6 31.8 27.3 59.1 4.6 36.4
MPCE quintile 5
(Higher)
71.4 21.4 7.1 95.0 5.0 0.0 46.2 53.9 15.4 60.0 0.0 40.0
Media Exposure
No exposure 73.0 26.4 0.7 98.0 1.0 1.0 79.3 3.5 20.7 67.2 1.6 31.2
Any exposure 57.0 36.7 6.3 97.2 2.8 0.0 42.5 37.5 32.5 53.1 8.2 38.8
Total 67.4 30.0 2.6 97.6 1.9 0.5 58.0 23.2 27.5 60.9 4.6 34.6

Imact Assessement Study on RSBY
Page | 106
Appendix 25.Satisfaction of entire RSBY enrolment process by selected background characteristics
Jharkhand West Bengal
Intervention District Non-Intervention District Intervention District Non-Intervention District
Background Characteristics Unsatisfactory Somewhat
unsatisfactory
OK/
Satisfactory
Unsatisfactory Somewhat
unsatisfactory
OK/
Satisfactory
Unsatisfactory Somewhat
unsatisfactory
OK/
Satisfactory
Unsatisfactory Somewhat
unsatisfactory
OK/
Satisfactory
Highest education level
Illiterate 68.8 0.0 31.3 64.0 24.0 12.0 23.5 17.7 52.9 6.5 41.9 48.4
Primary completed 65.7 25.7 8.6 75.0 25.0 0.0 24.0 28.0 36.0 27.8 30.6 33.3
Secondary completed 64.8 20.0 15.2 70.2 27.4 2.4 15.4 30.8 46.2 29.6 25.9 44.4
Higher secondary 71.2 24.2 4.6 43.1 51.0 5.9 25.0 12.5 50.0 21.1 26.3 47.4
Higher secondary & above 73.2 22.0 4.9 57.4 30.9 11.8 0.0 40.0 60.0 5.9 52.9 29.4
Caste
General/OBC 63.8 19.7 16.5 55.2 35.7 9.1 17.1 31.7 43.9 20.7 31.0 43.1
Scheduled Castes 76.7 20.9 2.3 74.6 21.8 3.6 40.0 20.0 40.0 15.4 36.9 41.5
Scheduled Tribes 72.1 23.5 4.4 65.2 33.3 1.5 22.7 13.6 50.0 42.9 42.9 14.3
Religion
Hindu 68.8 18.8 12.5 60.6 32.1 7.2 29.2 12.5 41.7 19.8 37.8 37.8
Muslims 56.3 18.8 25.0 58.3 41.7 0.0 18.4 31.6 44.7 16.7 16.7 61.1
Others 69.1 29.1 1.8 79.0 21.1 0.0 0.0 33.3 66.7 0.0 0.0 0.0
MPCE
MPCE quintile 1 (Lowest) 77.1 19.7 3.3 68.1 27.7 4.3 36.4 9.1 45.5 15.6 28.1 50.0
MPCE quintile 2 70.9 23.6 5.5 67.3 23.1 9.6 16.7 33.3 41.7 12.9 35.5 48.4
MPCE quintile 3 58.2 27.3 14.6 54.0 42.0 4.0 18.2 36.4 45.5 15.8 42.1 36.8
MPCE quintile 4 63.4 22.0 14.6 59.7 35.5 4.8 14.3 23.8 57.1 32.0 24.0 40.0
MPCE quintile 5 (Higher) 68.6 11.8 19.6 60.4 32.1 7.6 23.1 23.1 30.8 21.7 47.8 21.7
Media Exposure
No exposure 62.7 21.3 16.0 67.2 28.2 4.6 25.0 28.6 39.3 23.2 34.8 37.7

Imact Assessement Study on RSBY
Page | 107
Any exposure 77.7 20.2 2.1 56.4 36.1 7.5 17.5 22.5 50.0 14.8 34.4 44.3
Total 68.1 20.9 11.0 61.7 32.2 6.1 20.6 25.0 45.6 19.2 34.6 40.8

Imact Assessement Study on RSBY
Page | 108
Annex 1
Sample Selection& Sampling Design
The study design will follow a multi-stage, stratified design in arriving at the required sample and its selection process.
In order to decide the required sample size, we will use the following formula:
n = [t2*p(1-p)]/m2 (1)
Where,
n = required sample size
t = confidence level at 95% (standard value of 1.96)
p = estimated prevalence of the variable of interest
m = margin of error at 5% (standard value of 0.05)
Generally, to this estimated ‘n’ an adjustment factor for the ‘design-effect’ arising due to the multistage, clustered
design of the sample – usually around 2 – is applied. Accordingly the final sample size is,
N = n*d (2)
As the main ‘variables of interest’, we use two indicators:
i. Average rate/proportion of BPL households enrolled under RSBY scheme – Coverage indicator
ii. Estimated rate of hospitalization among the target population, i.e. BPL households (assumed as double the
observed level for general population) – Need indicator
Based on the above formula, the required sample size for the two states is computed as shown below:
Criteria Jharkhand West Bengal
Hospitalization rate (general pop)# 0.06 0.12
Hospitalization rate (target pop) 0.12 0.24
RSBY coverage rate^ 0.49 0.56
p (Combined average (33% weightage for coverage indicator, 66%
for need indicator)) 0.231 0.336
1-p 0.769 0.664
t2 3.8416 3.8416
m2 0.0025 0.0025
n 273 343
Oversampling/non-response (allowing additional 15%) 314 394
d 1.6 1.6
Round-off 500 625
Non-beneficiary (add 15%) 575 719
PACS-n 288 300
Non-PACS-n 288 425
N 575 725
# Source: NSSO 60th Round (2004-05)
^ www.rsby.gov.in
Note: The split between PACS and non-PACS sample is based on a 50:50 ratio for Jharkhand and 40:60 for WB (using
roughly the district covered in each of these states by PACS)

Imact Assessement Study on RSBY
Page | 109
Hence, we propose a total sample of 1300 households, including 575 (500 beneficiaries, 75 non-beneficiaries)
from Jharkhand and 725 (625 beneficiaries, 100 non-beneficiaries) from West Bengal.
Table 1
Ranking list of Districts
SN District
No. of
Household
(Census2011)
Total
(BPL)
Enrolled
(RSBY)
Proportion
of BPL to
HH
1 Jalpaiguri 868326 619180 222945 71.3
2 Koch Bihar 665720 474461 249920 71.3
3 Maldah 846991 601102 404418 71.0
4 Puruliya 567824 394035 197619 69.4
5 Paschim Medinipur 1301610 747304 450101 57.4
6 Murshidabad 1570759 887260 631003 56.5
7 Bankura 766902 418430 354436 54.6
8 Birbhum 817899 424717 335541 51.9
9 Dakshin Dinajpur 396406 204193 127011 51.5
10 Barddhaman 1730927 833882 619250 48.2
11 Uttar Dinajpur 605674 291349 125830 48.1
12 Nadia 1232282 551647 339750 44.8
13 Hugli 1287423 547375 338785 42.5
14 Purba Medinipur 1114170 461806 277280 41.4
15
South Twenty Four
Parganas 1781221 706669 138719 39.7
16
North Twenty Four
Parganas 2348683 874840 395606 37.2
17 Darjiling 391234 144484 33987 36.9
18 Haora 1061336 238342 85626 22.5
19 Kolkata 1024928 217846 96934 21.3
T WEST BENGAL 20380315 9638922 5424761 47.3
This Colour indicates the PACS Districts

Imact Assessement Study on RSBY
Page | 110
SN District
No. of
Household
(Census2011)
Total
(BPL)
Enrolled
(RSBY)
Proportion
of BPL to
HH
1 Garhwa 254697 274843 86203 107.9
2 Latehar 133381 125653 51124 94.2
3 Saraikela-Kharsawan 221232 184868 86548 83.6
4 Chatra 182271 133289 74867 73.1
5 Palamu 358754 258719 93778 72.1
6 Pakur 182317 129854 74095 71.2
7 Jamtara 155275 109850 52024 70.7
8 Sahibganj 227023 137517 80018 60.6
9 Simdega 118288 71629 30267 60.6
10 Khunti 103700 62763 24795 60.5
11 Pashchimi Singhbhum 302046 174506 79992 57.8
12 Hazaribagh 304749 167290 110060 54.9
13 Deoghar 264347 141175 41517 53.4
14 Ramgarh 179375 95430 53385 53.2
15 Godda 253648 131196 68721 51.7
16 Lohardaga 88638 45555 23556 51.4
17 Giridih 396521 188230 126996 47.5
18 Gumla 188988 87545 55134 46.3
19 Dumka 275019 125287 62276 45.6
20 Kodarma 116155 51638 32210 44.5
21 Ranchi 569444 226006 103400 39.7
22 Purbi Singhbhum 476931 148810 79654 31.2
23 Dhanbad 507064 157825 84546 31.1
24 Bokaro 394918 104886 53973 26.6
T JHARKHAND 6254781 3334364 1629139 53.3

Imact Assessement Study on RSBY
Page | 111
Annex 2 IMPACT ASSESSEMENT STUDY ON RASHTRIYA SWASTHYA BIMA YOJANA (RSBY)
MAIN QUESTIONNAIRE - JHARKHAND
Sponsored by Poorest Area Civil Society Programme [PACS]
INSTITUTE FOR HUMAN DEVELOPMENT NIDM Building, 3rd Floor, IIPA Campus, I.P Estate, Mahatma Gandhi Marg, New Delhi-110 002
Phones – 2335 8166, 2332 1610 / Fax : 23765410
Email: [email protected]
BLOCK 1: Interview Particulars
1. Interview ID 5. Supervisor Name and Signature
2. Supervisor ID 6. DEO Name and Signature
3. Data Entry Operator ID 7. Interview/Re-interview status
4. Interview er Name and Signature 8. Interview Date and Start-time
BLOCK 2: Household Identification Particulars
1 District 7 Gram Panchayat
2 PSU No. (Unique code) 8 Village Name
3 Block 9
Caste Category
(SC=1, ST=2, OBC=3, General=4)
4 Unique Household Identification
No. (UHID) 10
Religion
(Hindu=1, Muslim=2, Christian=3,
Others=4)
5 Name of Household Head 11 Highest educational attainment in
the household
1. SEGMENT 2. SUB-GROUP
A. RSBY Beneficiary Sample A. Minority
B. RSBY Non-Beneficiary sample B. ST
C. SC/OBC
Informed Consent Statement
INTERVIEWER – (Read out): Namaskar. My name is (please say your name here) and I work for Institute for Human Development, a
research institute in New Delhi. Your household has been selected to collect some detailed information on health and health care aspects
and the amount you have spent on health care for your family member, and your use and experience of the national health insurance scheme,
RSBY. It will take about 45 minutes for you to answer the questions. You can choose not to answer any questions or refuse participating in
the interview at any point of time throughout the interview. The information you provide will be confidential and used for research purposes
only. If you can spare the time now, and with your permission, can I start the interview now?

Imact Assessement Study on RSBY
Page | 112
BLOCK 3: HOUSEHOLD MEMBER ROSTER
A. Demographics and Socioeconomics
Details of all family members: In order to determine whom to interview, I need to know who lives at this address. Let me
assure you that any information you provide is strictly confidential. I would like the age, sex, education, marital status and
relationship to you of each of the members of this household who live here. Please include people who may presently be in
an institution due to their health (hospital, nursing home etc.) for a short or long period. All the members in the household
should be entered first, from oldest to youngest.Don’t forget to include yourself in the appropriate order.
1.1
Lin
e No
.
1.2
Name
1.3
Sex
1.4
Relatio
nsh
ip w
ith h
ouseh
old
head
1.5
Age
1.6
Marital statu
s
1.7
Hig
hest ed
ucatio
nal lev
el
1.8
Usu
al activity
status
1.9
Wh
ether su
ffered fro
m an
y
min
or illn
esses durin
g la
st 1 m
on
th
1.1
0 W
heth
er suffers fro
m an
y
chro
nic d
iseases since la
st 12
mo
nth
s?
1.1
1 W
heth
er hosp
italized ev
er
durin
g la
st 12
mon
ths
1.1
2 H
ealth In
suran
ce Coverag
e
1
2
3
4
5
6
7
8
9
CODES
For 1.3: Sex male=1, female=2
For 1.4: Relation to head self=1, spouse of head=2, married child=3, spouse of married child=4, unmarried chiId=5, grand child=6, father/mother/father-in-law/mother-in-law=7, brother/sister/brother-in-law/sister-in-law/other relative=8, servant/employees/other non-relatives=9

Imact Assessement Study on RSBY
Page | 113
For 1.6: Marital status never married=1, currently married=2, widowed=3, divorced/separated=4
For 1.7: Educational level Illiterate=01; literate but never gone to school=02, Upto class 4=03, Upto class=04, Completed class 10=05, completed class 12= 06, completed Graduation= 07, Any higher education above graduation=08
For 1.8: Usual activity status Casual/daily wage laborer=01, Self-employed (including small business & trade)=02, Regular salaried employment=03, Unemployed/seeking work=04, Student=05, Home-maker/household work/domestic duties (unpaid)=06, Disabled/Old/Young=07, Household
entrepreneur (tailoring/weaning/hand wash)=08, Others=99 (Specify)
For Q.1.9 to 1.11: Yes=1, No=0, don’t know/can’t say=99.
For Q. 1.12: RSBY=1, Private insurance=2, Covered by employer=3, Not covered with any scheme=4, DK/CS=99
Note: Q1.9: When suffered from any common/minor/short-term illness in last 30 days (such as – fever/cold & cough/loose motion…….etc.) Q 1.10: Diabetes/cancer/hypertension/heart alignments/heart alignment/respiratory problems/tuberculosis/arthritis/long standing pain in bone/joints)
B. Social Networks
Is anyone in the family presently a member of any of the followings :
10 Self Help Group (SHG)/Credit Cooperatives Yes (1) No (0) DK/CS (99)
11 NGO/MFI (Micro Finance Institution) client Yes (1) No (0) DK/CS (99)
12 Trade unions Yes (1) No (0) DK/CS (99)
13 Political party Yes (1) No (0) DK/CS (99)
14 Religious organization Yes (1) No (0) DK/CS (99)
15 Local CBO’s (Community Based Organizations) Yes (1) No (0) DK/CS (99)
16 Other membership-based organization Yes (1) No (0) DK/CS (99)
17 Do you or your family members personally know the Gram Panchayat/Local MLA/MP/any other elected member of your AREA?
Yes (1) No (0) DK/CS (99)
Number of times you did the following during last 7 days/in last week?
18 Watch TV Never (1) Rarely (2) Daily (3)
19 Listen Radio Never (1) Rarely (2) Daily (3)
20 Read Newspaper/magazines Never (1) Rarely (2) Daily (3)
21
What are your main sources of your information regarding government programmes/schemes?
(Multiple Answers)
[Friends and family-members =1,
Media (A-V/Print)=2,
Local government workers (ANM, AWW =3,
Political party, workers/leaders/elected reps =4,
Religious leaders/places of worship-=5,
Local NGO/CBO members =6,
Others(specify)=98, Don’t Know/CS=99]

Imact Assessement Study on RSBY
Page | 114
BLOCK 4: HEALTH STATUS AND HEALTH CARE UTILIZATION
A. Particulars of non-hospitalized/short-term aliments of household members during the last 30 days
22 Srl. no. of ailment 1 2 3 4 5
23 Srl. no. of member reporting ailment
Number of days within the reference period
24 Nature of ailment (code on page no…)
25 Total duration of ailment (days)
26 Ill
27 On restricted activity
28 Confined to bed
29 Did you/[member] receive any medical treatment for this
ailment? (Yes-1, No-2)
30 If not (Q 43=2), reasons for not seeking/receiving any medical
treatment?
No medical facility available in the neighbourhood - 1,
Facilities available but no treatment sought owing to: lack of
faith - 2,
Long waiting - 3,
Financial reasons - 4,
Ailment not considered serious - 5,
Others - 98
31 If yes (Q 43=1), Type of health service provider/health facility
from where treatment was sought?
Govt. clinic/dispensary-1

Imact Assessement Study on RSBY
Page | 115
Govt hospital-2
Private physician/clinic-3
Private hospital/nursing home (including NGO/trust
hospitals)-4
Quacks/informal providers-5
Medicine shops/pharmacy/old prescriptions-6
Hakim/vaids-7
Other (specify)
32 Please provide reasons for seeking treatment from this
provider/health facility?
Nearest health facility/convenient (including convenient
operational hours)-1
Low cost/financial reasons-2
Usual choice for treatment/past experience of effective
treatment-3
Neighbours/friends advised-4
Others (specify)-98
Not sure/DK/CS) =99
if 1 in item 1
33 If Q___=1 (Ask treatment was sought from any sources,
except govt. health facility) [If Q.61≠1 or Q.61≠2]
Reason for not using services of government
physicians/health facilities
Govt. doctor/facility too far-1,
Not satisfied with medical treatment by Govt. doctor/facility -2
Long waiting -3,
Required specific services not available - 4,
Others – 98
Now, I would like to collect some information on the expenses incurred for your treatment
From the illness you have been describing, I will require expenses incurred on different purposes, and also from where/which sources did
you manage to pay. (In case of multiple episodes, information from the most recent)

Imact Assessement Study on RSBY
Page | 116
Please provide amount spent on
(I)
Total cost
(II)
Amount paid out-of
pocket (own
income/savings)
III
Amount from
other sources
IV
Source
V
34 Doctor’s fee
35 Diagnostic tests
36 Medicine/injections
37 Bed charges
38 Surgery charges
39 Any special diet/other food
40 Follow-up costs
41 Transportation (including ambulance)
42 Any other indirect costs (wage loss of
attendants etc.)
43 Total expenses
Instructions: funsZ”k
For III: Ask respondent whether entire amount was met with self-income/salary/from other household member. If so, copy the
total costs from Col.2 to Col. 3 and skip col.4 & col.5
For IV: Entre the amount that was with supported from other sources:
If Partial support=include amount
If total (entire amount supported by external sources)=copy col. 3.
For V: Other/External sources:
1=Borrow from friend/neighbor/relatives;
2=Loans from office;
3=Paid by the employee
4=Loan (with interest) from money lender
9=Others (specific)
44
How were the expenses met? (Multiple responses
possible)
Note: These questions are to be asked if the respondent
is unable to give break-up of the expenses incurred
(and its financing sources)
Self savings =1
Employer paid =2
Friends/family =3
Health insurance (others)=5
Borrowings from money lenders with interest
Selling of assets =7
Others (specify) =98
DK/CS=99
45
Was it of any difficulty for your family/yourself to
meet the costs associated with your (child’s) treatment,
and spending the amount you mentioned?
1=Extremely difficult
2=Somewhat difficult
3=Not at all
46 Number of days confined to bed/absent in work
CODES FOR AILMENT:

Imact Assessement Study on RSBY
Page | 117
ailment code ailment code Gastro-intestinal Diabetes mellitus 22 Diarrhoea/ dysentery 01 Under-nutrition 23 Gastritis/gastric or peptic ulcer 02 Anaemia 24 Worm infestation 03 Sexually transmitted diseases 25 Amoebiosis 04 Febrile illnesses
Hepatitis/Jaundice 05 Malaria 26 Cardiovascular Diseases Eruptive 27 Heart disease 06 Mumps 28 Hypertension 07 Diphtheria 29 Whooping cough 30 Respiratory including ear/nose/throat ailments 08 Fever of unknown origin 31 Tuberculosis 09
Bronchial asthma 10 Tetanus 32 Disorders of joints and bones 11 Filariasis/Elephantiasis 33 Diseases of kidney/urinary system 12
Prostatic disorders 13 Disabilities Gynaecological disorders 14 Locomotor 34 Neurological disorders 15 Visual including blindness (excluding 35 cataract)
Psychiatric disorders 16 Speech 36 Hearing 37 Eye ailments Diseases of Mouth/Teeth/Gum 38 Conjunctivitis 17 Accidents/Injuries/Burns/
Glaucoma 18 Fractures/Poisoning 39 Cataract 19 Cancer and other tumours 40
Diseases of skin 20 Other diagnosed ailments 41 Goitre 21 Other undiagnosed ailments 99
B. Particulars of medical treatment received as inpatient of a hospital during the last 365 days
47 Sr1. no. of the hospitalisation case 1 2 3 4 5
48 Srl. no. of member (as in HH roster) hospitalized
49 Age (years)
50 Type of hospital (code)
Govt hospital=1
Private hospital/nursing home (including NGO/trust hospitals)=2
Other (specify)=98
51 Nature of ailment (code on page no…)
Disease Code will be added
52 Type of ward (free - 1, paying general - 2, paying special - 3)
53 Duration of stay in hospital (days)

Imact Assessement Study on RSBY
Page | 118
Details of medical services received (not received - 1; received: free - 2, partly free - 3, on payment - 4)
54 Bed charges
55 Attendant/Nursing
56 Food
57 Surgery charges
58 medicine
59 X-ray/ECG/EEG/Scan
60 other diagnostic tests
61 Did [member] receive any treatment before hospitalisation for
the ailment mentioned in Q 5 (yes - 1, no - 2)
62
If 1 in
item 15
Source of treatment
Govt. clinic/dispensary=1; Govt hospital =2; Private
physician/clinic=3; Private hospital/nursing home
(including NGO/trust hospitals)=4; Quacks/informal
providers=5; Medicine shops/pharmacy/old
prescriptions=6; Other (specify)=98
63 Duration of treatment (days)
64 whether treatment continued after discharge from hospital (yes -
1, no - 2)
65
If 1 in
item 18
Source of treatment (code)
Govt. clinic/dispensary=1; Govt hospital =2; Private
physician/clinic=3; Private hospital/nursing home
(including NGO/trust hospitals)=4; Quacks/informal
providers=5; Medicine shops/pharmacy/old
prescriptions=6; Other (specify)=98
66 Duration of treatment (days)
Now, I would like to collect some information on the expenses incurred for all episodes/events of Hospitalization for all members of this
household, on all diseases DURING LAST 12 MONTHS
From the illnesses and hospitalizations you have been describing, I will require expenses incurred on different purposes, and also from
where/which sources did you manage to pay. (In case of multiple episodes, information from the most recent)
Please provide amount spent on
(I)
Total cost
(II)
Amount paid out-
of pocket (own
income/savings)
III
Amount from
other sources
IV
Source
V
Amount provided
under RSBY
VI
67 Doctor’s fee
68 Diagnostic tests
69 Medicine/injections
70 Bed charges
71 Surgery charges
72 Any special diet/other food
73 Follow-up costs
74 Transportation (including
ambulance)

Imact Assessement Study on RSBY
Page | 119
75 Any other indirect costs (wage loss
of attendants etc.)
76 Total expenses
Instructions: For III: Ask respondent whether entire amount was met with self-income/salary/from other household member. If
so, copy the total costs from Col.2 to Col. 3 and skip col.4 & col.5
For IV: Enter the amount that was with supported from other sources:
If Partial support=include amount ;
If total (entire amount supported by external sources)=copy col. 3.
For V: Other/External sources: 1=Borrow from friend/neighbor/relatives; 2=Loans from office/ place of work; 3=Paid by the
employee; 4=Loan (with interest) from money lender; 5=Sold household assets/jewelry; 9=Others (specific)
77
Ask only if respondent cannot provide break-up of the
expenses incurred (and its financing sources
How were the expenses met? (Multiple responses
possible)
Self savings =1
Employer paid =2
Friends/family =3
Health ins-RSBY - =4
Health insurance (others)=5
Borrowings from money lenders with interest =6
Selling of assets =7
Others (specify) =98
DK/CS=99
78
Loss of household income, if any, due to
hospitalization of [member] (Rs)
Instruction: Include loss of wage for the hospitalized member
(if working)
79
Was it of any difficulty for your family/yourself to
meet the costs associated with the hospitalizations of
your household members, and spending the amount you
mentioned?
1=Extremely difficult
2=Somewhat difficult
3=Not at all
C. Accidental Injury, Treatment and Financing
80 Did you/any household member suffer from any accidents or an injury in the
past 12 months that required medical treatment?
(Ignore minor cuts/bruises; include those that required medical treatment)
Yes
(1)
No
(0)
If no, Skip to next
Section
81
82
Indicate which members suffered such injuries
(Only include currently surviving members; for dead members record in
Block___): [ADD ADDITIONAL SHEET IN CASE OF MORE THAN TWO]
(Instruction – copy Member Line Number from Block-___)
ID-1 ID-2
83 Type of accident/Mechanism of Injury
(1=motor vehicle, 2=pedestrian-vehicle crash, 3=motorcycle, 4=bicycle,
5=fall , 6=gunshot/firearms, 7=stab/cuts, 8=fire/burn s, 9=poisoning,
10=drowning , 11=others , 98=Others (specify); 99=DK/CS)
84 Where did the injury occur?

Imact Assessement Study on RSBY
Page | 120
(1=home , 2=school, 3=streets/highways/railways, 4=trade & service areas
(shops, offices), 5=water bodies, 6=industrial/construction, 98=others
(specify); ; 99=DK/CS)
85 When (in the last 12 months) did the accident happen?
(1=within last 30 days, 2=last 3 months , 3=3-6 months , 4=6-12 months f,
98=Others (specify); 99=DK/CS)
86 Which body parts/organs were injured/affected by the accident? (Head flj =1;
Limb =2; Chest =3; Shoulder/neck/back =4; Internal organ =5)
87 Did any other family members/friends accompany you/member at the time of
the accident/injury?
(0=No, 1=Yes, 99=DK/CS)
88 How you /your family did come to know about the accident/injury of the
member?
(1=police, 2=hospital authorities, 3=friends/neighbors, 4=unknown
strangers; 98=Others (specify)
89
Did you/member receive any medical attention/treatment at the
accident/injury site?
(0=No, 1=Yes, 99=DK/CS)
90 Were you/member taken/went to any hospital/clinic to receive treatment after
the injury/accident? (0=No, 1=Yes, 99=DK/CS)
91 Name of the hospital
92
Type of the facility
Govt. clinic/dispensary =01;
Govt hospital =02;
Private physician/clinic =03;
Private hospital/nursing home (including NGO/trust hospitals) =04;
Quacks/informal providers =05;
Hakim/vaids=07;
Other (specify) =98)
93 How were you/member taken/went to the hospital/clinic/physician mentioned
in Q 198?
(1=Govt ambulance, 2=pvt. Ambulance, 3=pvt vehicles 4=police vehicles
5=rickshaw/vans, 98= Others (specify); 99=DK/CS)
94 Are you aware of the ambulance service OR the helpline number xxxxxx for
emergency medical transportation service of the Delhi Government?
(0=No, 1=Yes, 98= Others (specify); 99=DK/CS)
95 Reasons for seeking care/treatment from the particular facility?
Nearest health facility/convenientworking hours =01;
Low cost/financial reasons =02;
Usual choice for treatment/past experience of effective treatment=03;
neighbours/friends advised=04
taken by police/other
persons/ambulance=05
98=Others
(specify);
99=Not
sure/DK/CS)))

Imact Assessement Study on RSBY
Page | 121
96 Did you/member receive immediate treatment (including examination,
dressing of the wound, applying bandages/casts) after arriving at the health
facility?
(0=No, 1=Yes, 99=DK/CS)
97 Were any diagnostic tests/scans conducted
(0=No, 1=Yes, 99=DK/CS)
98 How satisfied were you by the overall quality of treatment/care received
while being treated for the accident/injury at the health facility?
Rate in a scale of 1-5, with 1=Extremely dissatisfied and 5=Very Satisfied
99 Did the accident/injury require any hospitalization/in-patient stay of the
member?
(0=No, 1=Yes, 99=DK/CS)
100 Days of stay
101 Total duration of treatment (include hospitalizations and any follow-up visits)
Total expenditure incurred on account of treatment and related expenses due to the accident/injury of the member in last 12
months?
Please provide amount spent for
(i)
Total cost
(II)
Amount paid
out-of pocket
(own
income/savings)
III
Amount from
other sources
IV
Source
V
Amount
provided under
RSBY scheme
VI
102 Doctor’s fee
103 Diagnostic tests
104 Medicine/injections
105 Bed charges
106 Surgery charges
107 Any special diet/other food
108 Follow-up costs
109 Transportation (including
ambulance)
110 Any other indirect costs (wage loss
of attendants etc.)
111 Total expenses
Instructions:
For III: Ask respondent whether entire amount was met with self-income/salary/from other household member. If so, copy the
total costs from Col.2 to Col. 3 and skip col.4 & col.5
For IV: Entre the amount that was with supported from other sources:
If Partial support=include amount
If total (entire amount supported by external sources)=copy col. 3.
For V: Other/External sources: 1=Borrow from friend/neighbor/relatives; 2=Loans from office; 3=Paid by the employee; 4=Loan
(with interest) from money lender; 9=Others (specific)
112 What has been the major source of finance for the treatment? [Note: These
questions are to be asked if the respondent is unable to give break-up of the
expenses incurred (and its financing sources]
Self savings =1,
Employer paid=2,
Friends/family =3,

Imact Assessement Study on RSBY
Page | 122
Health ins-RSBY =4,
Health insurance (others vU;)=5,
Borrowings from money lenders with interest =6,
Selling of assets =7,
Others =8, Others (specify)=98;
DK/CS=99
113 Was it of any difficulty for your family/yourself to meet the costs associated
with your (child’s) treatment, and spending the amount you mentioned?
1=Extremely difficult
2=Somewhat difficult
3=Not at all
114 Are you/hh member restricted in any of the following areas as a result of this
accident / injury?
(a) Attending work on a full-time/pre-accident/injury leaves
(b) Attending school regularly
(c) Attend daily living activities (bathing/driving/walking/using toilets)
(d) Attend daily household chores (outing/shopping/managing
household finance etc.)
Yes
(1)
A
B
C
d
No
(2)
A
B
C
d
DK/CS
(99)
A
B
C
d
115 Have you/hh member missed work due to this accident / injury?
(0=No, 1=Yes, 99=DK/CS)
116 Number of days lost/confined to bed:
117 Did the accident/injury cause any permanent/semi-permanent disability?
(loss of limb, eyesight, hearing. Cognition etc)
(0=No, 1=Yes, 98= Others (specify); 99=DK/CS)
118 How difficult you found to adjust with the loss of work / financial hardships,
following the accident?
Rate in a scale of 1-3, with 1=Extremely difficult;2=Somewhat difficult; Not
difficult at all=3
119 How would you rate the current health status/condition of the member, with
respect to the accident/injury
Rate in a scale of 1-5, with Very poor=1; Poor=2; Somewhat
OK/moderate=3; Good=4 and 5=Excellent
D. Welfare Impacts Of Health Shocks & Coping Mechanisms

Imact Assessement Study on RSBY
Page | 123
120 Considering all events of diseases/illnesses, hospitalizations, accidents,
injury experienced by your family members in last 1 year, how would
you rate the impact of all these events taken together, on the economic
status/capacity of your household?
Very severe impact 1
Sever impact 2
Moderate impact 3
Partial impact 4
No effect 5
121 Do you consider that your family has fully recovered, partially
recovered, or not at all recovered from the financial impacts of the
health shocks - taking all of these adverse health events together?
Completely recovered 1
Partially recovered 2
Not at all recovered 3
122 For some families, health shocks/adverse health events have been seen
to be responsible for making families poorer, and impoverished in
some cases.
Now, considering the economic status of your household during same
time of last year (March, 2013/ Last Holi) and the health
shocks/adverse health events your family has faced since then, do you
think that the economic status/capacity of your household have:
Deteriorated considerably 1
Deteriorate somewhat 2
More or less remained the same 3
Improved somewhat 4
Substantially improved 5
Do you think that your household/any family member had to do any of the following to cope with/manage the financial impacts
arising out of all these ill-health/diseases events taken together?
(1=Severe impact, 2=High, but not severe impact, 3=Somewhat/little impact, 4=No impact)
122 Postpone marriages in the family 1 2 3 4
123 Withdraw children from schools 1 2 3 4
124 Children required to work 1 2 3 4
125 Elderly members required to work 1 2 3 4
126 Adults forced to take up additional working hours 1 2 3 4
127 Reduce food consumption (e.g. adults skipping meals, buy cheaper/less quality
food) 1 2 3 4
128 Reduce other non-food consumption expenditure (on clothing, festival-spending,
travel to native places, entertainment etc) 1 2 3 4
129 Postpone/defer purchase of assets 1 2 3 4
130 Delay/Ignore/Avoid non-critical health care needs of household members 1 2 3 4
131 Would you be able to raise Rs. 10,000 in one week if you needed it for some
emergency?
Yes
(1)
No
(0)
DK/CS
(99)
132 How would you raise Rs. 10,000?
Mention top 3 sources in the order you would follow
(Selling durable goods/equipment =1, Selling land/house =2 , From
savings=3, From relatives/friends =4, From employer=5, From
moneylender=6, Taking extra work=7, From any
MFI/cooperative/NBFI=8; Others (specify) =98; DK/CS=99 )
1st 1 2 3 4 5 6 7 8 9 99
2nd 1 2 3 4 5 6 7 8 9 99
3rd 1 2 3 4 5 6 7 8 9 99
E. Quality Of Medical Services/Quality Of Care

Imact Assessement Study on RSBY
Page | 124
133 (a) Have you visited/accompanied patient to
any health provider/ hospital/clinic for out-
patient care (OPD) in last 12 months
(b)Have you been hospitalized/spent time
with other family members during
hospitalization in- patient care in last 12
months
Yes (1)
If yes, complete the full
column
No (0)
If no, move to
(b)
Yes (1)
If yes, complete the
full column
No (0)
If no, Skip to
next section
134 Type of health facility used Government hospital (1)
Private hospital/nursing/clinics (2)
Private practitioner (3)
Informal providers/Jhola chap etc.(4)
Government hospital (1)
Private hospital/nursing/clinics (2)
Private practitioner (3)
Informal providers/Jhola chap etc. (4)
Rank the top three services, which you liked/found best during your last visit to a hospital/ nursing home/clinic
Rank (1,2,3)
OPD IPD
135 Skill and Competency of the staff/physician
136 Overall Cleanliness
137 Friendliness and courtesy of the staff
138 Effectiveness of the treatment and medicine prescribed
139 Cost of the treatment
140 Ease of communicating treatment/ therapy
141 Any other aspects (Specify)
Rank the top three services, which you disliked/found worst during your last visit to a hospital/ nursing home/clinic
Rank (1,2,3)
142 OPD IPD
143 Distance
144 Waiting Time
145 Cleanliness/ Environment
146 Lack of Privacy during consultation/ overcrowding
147 Behaviour of staff/ physician
148 Cost of treatment
149 Effectiveness of the treatment and medicine prescribed
150 Any other aspects (Specify)
Now, I am going to ask you a few questions on the health services
You have received/experienced while you were at the hospital clinic and your overall experience.
Domains
For out- patient care
(OPD)
For in- patient
care/hospitalization
151 How approachable/friendly was the doctor?
1=Very much; 2=somewhat; 3=not at all
152 How approachable/friendly was the other staff
(nurses/technicians/clerks)? 1=Very much; 2=somewhat; 3=not at
all
153 Did you find the working hours convenient to you, given your
normal daily tasks/duties?
1=Very convenient; 2=Somewhat convenient; 3=Inconvenient;
4=Very inconvenient
154 How convenient/accessible was the location of the facility/clinic
from your residence?
1=Very convenient; 2=Somewhat convenient; 3=Inconvenient;
4=Very inconvenient
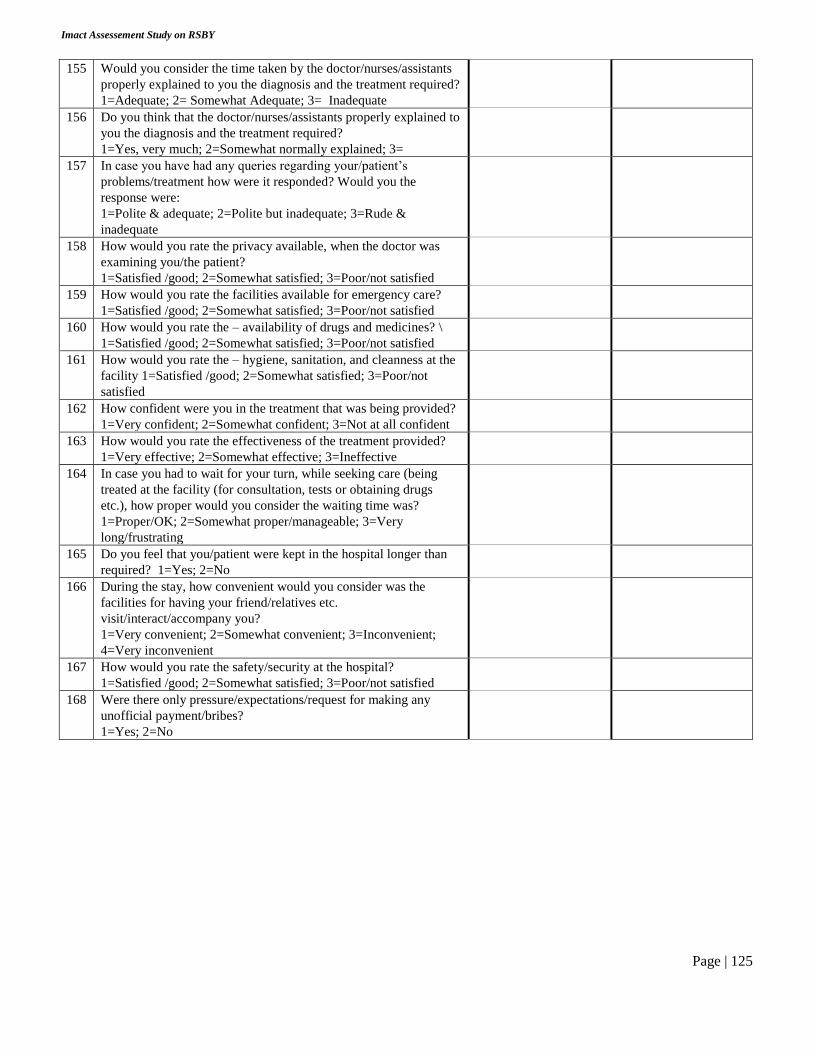
Imact Assessement Study on RSBY
Page | 125
155 Would you consider the time taken by the doctor/nurses/assistants
properly explained to you the diagnosis and the treatment required?
1=Adequate; 2= Somewhat Adequate; 3= Inadequate
156 Do you think that the doctor/nurses/assistants properly explained to
you the diagnosis and the treatment required?
1=Yes, very much; 2=Somewhat normally explained; 3=
157 In case you have had any queries regarding your/patient’s
problems/treatment how were it responded? Would you the
response were:
1=Polite & adequate; 2=Polite but inadequate; 3=Rude &
inadequate
158 How would you rate the privacy available, when the doctor was
examining you/the patient?
1=Satisfied /good; 2=Somewhat satisfied; 3=Poor/not satisfied
159 How would you rate the facilities available for emergency care?
1=Satisfied /good; 2=Somewhat satisfied; 3=Poor/not satisfied
160 How would you rate the – availability of drugs and medicines? \
1=Satisfied /good; 2=Somewhat satisfied; 3=Poor/not satisfied
161 How would you rate the – hygiene, sanitation, and cleanness at the
facility 1=Satisfied /good; 2=Somewhat satisfied; 3=Poor/not
satisfied
162 How confident were you in the treatment that was being provided?
1=Very confident; 2=Somewhat confident; 3=Not at all confident
163 How would you rate the effectiveness of the treatment provided?
1=Very effective; 2=Somewhat effective; 3=Ineffective
164 In case you had to wait for your turn, while seeking care (being
treated at the facility (for consultation, tests or obtaining drugs
etc.), how proper would you consider the waiting time was?
1=Proper/OK; 2=Somewhat proper/manageable; 3=Very
long/frustrating
165 Do you feel that you/patient were kept in the hospital longer than
required? 1=Yes; 2=No
166 During the stay, how convenient would you consider was the
facilities for having your friend/relatives etc.
visit/interact/accompany you?
1=Very convenient; 2=Somewhat convenient; 3=Inconvenient;
4=Very inconvenient
167 How would you rate the safety/security at the hospital?
1=Satisfied /good; 2=Somewhat satisfied; 3=Poor/not satisfied
168 Were there only pressure/expectations/request for making any
unofficial payment/bribes?
1=Yes; 2=No

Imact Assessement Study on RSBY
Page | 126
BLOCK 5: RSBY-INTERVENTION: WEST BENGAL
Section A: Screening and Non-beneficiaries
Now, I would like to ask you a few questions regarding your Knowledge with the RSBY scheme.
169 Are you aware of a government scheme/programme that covers hospitalization expenses for
families such as yours?
Yes
(1)
No
(2)
170 Have you ever heard of a scheme called Rashtriya Swasthya Bima Yojana (RSBY)?
Yes
(1)
No
(2)
171 Have you ever seen any of your neighbours/relatives/friend having a card such as this? [SHOW
RSBY CARD]
Yes
(1)
No
(2)
IF ANSWER “NO” to all of the 3 questions above, Skip to next BLOCK 6
IF ANSWER “YES” to any of the 3 questions above go to next question
172 Do you/hh posses a RSBY smart card? Yes No

Imact Assessement Study on RSBY
Page | 127
(1)
Skip to Q. 176
(2)
173 Why have you/your family not enrolled in the programme/RSBY?
Unsure about enrolment process; =1
Do not have required documents; =2
Lack of time to visit enrolment centre/get enrolled =3
Was refused enrolment; =4
Was told that the scheme is no longer operational;-=5
Unaware about the actual benefit; =6
Considers that the benefit will be too little -=7
Unsatisfactory experience of friends/neighbours =8
98=Others (Specify)
99=Can’t say/DK
174
Do you consider that it will be useful/helpful for your family if you are enrolled under
RSBY/and can avail of the facilities/financial support it provided? Would you say it will
be:
Very useful 1
Somewhat useful 2
Not useful at all 3
175
For families such as yours, what kind of help/support do you think the government should provide, with regards to
healthcare/medical treatment needs of your family and the financial implications associated with it?
(OPEN ENDED QUESTION/Note down)
Section B: Awareness and Knowledge about RSBY – Relevant Intervention Assessments
176 Have you heard about the RSBY scheme?
Yes
(1)
No
(2)
177 Did anyone come to your house to inform you about the RSBY scheme?
Yes
(1)
No
(2)
Others
(98)
178 Do you know the organisation name of the person who visited you regarding RSBY
scheme? --------------------------------
179
Where did you first come to know about the RSBY scheme?
Neighbours/friends=1
Relatives=2
Local school teacher=3
Employer=4
Govt. workers=5
Local health worker=6

Imact Assessement Study on RSBY
Page | 128
Local NGO=7
MLAs/other political workers=8
Newspaper/magazines=9
TV/films=10
Others (specify)=98
180
Do you know who is eligible for the scheme?
Everyone in the family=1
BPL families=2
Antyoday Anna Yojana families=3
NREGA card holders=4
Others(specify)=5
Don’t know=99
181
How many family members can be enrolled?
At most 5 members=1
All household members=2
Others (specify)=98
Don’t know=99
182
Which members of the family are compulsory to enroll in RSBY scheme?
183 How much does it cost to enroll in this scheme? (in Rs.)
184 What is the maximum amount per year that can be spent under RSBY scheme?
185
What kind of treatment is provided free of cost under RSBY/Smart Card? (Prompt)
Hospitalized treatment=1
Home based treatment=2
Both=3
Don’t know=98
186 Are transportation allowances provided to the patient under RSBY scheme?
Yes
(1)
No
(2)
DK
(99)
187
Do you have to pay for the diagnostic tests (Examples: X-ray/ECG/EEG/Scan)during
hospitalisation if you enroll in this scheme?
Yes=1
No=2
Don’t know=99
188
Do you have to pay for medicines and drugs in case of hospitalisation if you enrol in this
scheme?
Yes=1
No=2
Don’t know=99
189
Have you noticed/observed any of the following activities related with awareness
generation/information on RSBY taking place in your village/community?
(Read all options one-by-one)
Mike announcements in the community/village=1
Rallies=2
Tableau=3
Video shows=4
Puppet shows=5
Street plays=6
Wall writing=7
Others (specify)=98
190
How often have you noticed such awareness related activities on RSBY scheme in your
community?
Twice or more in a month=1
Monthly=2
Every two months=3

Imact Assessement Study on RSBY
Page | 129
More than two months=4
Others (specify)=98
Don’t know=99
Show IEC materials and Test Familiarity
191
Have you seen?
Exhibit 1
Exhibit 2
Exhibit 3
Exhibit 4
Exhibit 5
192
How useful do you think these materials are?
Exhibit 1
Exhibit 2
Exhibit 3
Exhibit 4
Exhibit 5
Section C: Enrolment and Orientation
193
Do you have a RSBY smart card?
Yes=1
No=2
Don’t know=99
194 In which year did enrolment take place?
195
Please show your RSBY/Smart card.
Showed=1
Did not want to show=2
Other (specify)=98
196
Who encouraged you to apply for the RSBY scheme?
Self=1
Neighbours/friends=2
Relatives=3
Local school teacher=4
Employer=5
Govt. workers=6
Local health worker=7
Local NGO=8
MLAs/other political workers=9
Others (specify)=98
197
Who informed you about the RSBY enrolment process?
Neighbours/friends=1
Relatives=2
Local school teacher=3
Employer=4
Govt. workers=5
Local health worker=6
Local NGO=7
MLAs/other political workers=8
Others (specify)=98
198 Where did you apply for RSBY scheme?

Imact Assessement Study on RSBY
Page | 130
In the village=1
Outside the village=2
Others (specify)=98
199 How far was the enrolment centre from your house? (in kms)
200
How did you come to know about RSBY enrolment venue?
Self=1
Neighbours/friends=2
Relatives=3
Local school teacher=4
Employer=5
Govt. workers=6
Local health worker=7
Local NGO=8
Announcements=9
MLAs/other political workers=10
Others (specify)=98
201
What documents did you produce for the enrolment?
BPL Card=1
MNEREGA ID Proof=2
Others (Specify)=98
202
Did anyone told you about the essential documents that are required to enrol under
RSBY?
Neighbours/friends=1
Relatives=2
Local school teacher=3
Employer=4
Govt. workers=5
Local health worker=6
Local NGO=7
Corporators/MLAs/other political workers=8
Others (specify)=98
203 Did anyone help you during the enrolment process apart from the RSBY enrolment team
members?
204
Did you face any problem in obtaining the card?
Yes
(1)
No
(2)
205
What problems did you face in obtaining the card?
206
Did you get the RSBY smart card instantly?
Yes
(1)
No
(2)
207 If no, when did you receive your smart card? (in days)
208 Did you make any payments to receive the RSBY smart card? (in Rs)
209 Did you receive any documents with the card?
Yes
(1)
No
(2)
210
What information was provided on the documents?
List of hospitals =1
How to use the card=2
Whom to contact in case of any query=3
Information about district kiosk=4

Imact Assessement Study on RSBY
Page | 131
Other (specify)=98
Don’t remember=99
211 Did you receive any information on RSBY/Smart Card verbally?
Yes
(1)
No
(2)
212 Who provided you the information?
213
What information was conveyed to you? (Read out options)
List of hospitals=1
How to use the card=2
Who to contact in case of any query=3
Information about district kiosk=4
No information was conveyed=5
Other (Specify)=98
Don’t remember=99
214 Did you ask any for any doubts/clarifications related to RSBY scheme during enrolment?
Yes
(1)
No
(2)
215 Did anyone respond to your doubts/clarifications?
Yes
(1)
No
(2)
216 Who was the person/organization that responded to your doubts/clarifications?
217 Did anyone visit your home after acquiring RSBY smart card for detail description related to its usage and others?
218
Were you told about the date when you could start using the smart card?
Yes
(1)
No
(2)
219
How long did it take you to complete the whole enrolment process?
Less than one hour=1
One or more than one hour=2
If more than one hour, please specify=3
220
What was your experience of the enrolment process (How satisfactory….)?
Complicated/difficult/long-waiting/v. unsatisfactory=1
Somewhat unsatisfactory=2
OK/satisfactory/no problem=3
Others (specify)=98
DK/CS=99
201 Are you aware of the three nearest RSBY empanelled hospital nearby your locality?
Yes
(1)
No
(2)
202 If yes, please name the hospitals?
1……………………..
2………………………
3………………………
203 Have you ever be a part of any hospital exposure visits conducted by any organisation?
Yes
(1)
No
(2)
204
Who approached you prior to hospital exposure visits?
Friends/relatives=1
Any PRI member=2
Local health worker=3

Imact Assessement Study on RSBY
Page | 132
Local NGO/CBO=4
Others (Specify)=98
205 Did anyone tell you about the purpose of hospital exposure visits?
206 How many people from you community were accompanying you during hospital
exposure visit?
207
Which hospital did you visit?
208 How much time did you spent on exposure visit? (in hrs.)
209
To whom did you interact during hospital exposure visit?
Doctors=1
Nurses=2
Hospital administrative staff=3
RSBY help desk=4
Others (Specify)=98
210
Did you visit different departments/locations inside the hospitals?
Registration desk=1
Patient waiting hall=2
Doctors room=3
X-ray room=4
Drug distribution centre=5
Toilets/Wash room=6
Others (Specify)=98
211 What was the major issue that was raised during the hospital exposure visits?
212 Did your confident improve after the hospital exposure visit?
Yes
(1)
No
(2)
Can’t
say
(99)
213
Did hospital exposure visit change your perception towards?
Doctors=1
Nurses=2
Staff=3
Others (Specify)=98
214 Did you share you hospital exposure visit to anyone in the community?
Yes
(1)
No
(2)
Section D: Utilization and Satisfaction
215 Screener Check: Did you use your RSBY Smart Card for medical treatment-
related payments for any of your ill family members during last 12 months:
Yes
(1)
No
(2)
216 Type of aliment/disease for which hospitalization was required?
217 Which RSBY-empanelled hospital did you visit?
218 How far is the hospital from your house/village? (in kms)
218
How did you reach the RSBY empanelled hospital?
Ambulance=1
Public transport=2
Private transport=3
Others (Specify)=98

Imact Assessement Study on RSBY
Page | 133
219 Was there a RSBY helpdesk/counter at the hospital
Yes
(1)
No
(2)
220
Whether the RSBY help desk was Separate=1
Shared=2 Don’t know=98
201 Did you find any staff member at the RSBY help desk?
Yes
(1)
No
(2)
202 Did anybody help you/informed you about how to use your RSBY card regarding the
admission/treatment processes?
Yes
(1)
No
(2)
203
How long did you/the patient have to wait before being attended by the Help-Desk staff?
(In hrs.)
204
Was fingerprint verification done through a fingerprint scanner?
Yes
(1)
No
(2)
Don’t
know
(99)
205 Were you informed about the costs of treatment or given an estimate in advance/at the
time of admission?
Yes
(1)
No
(2)
206 Were you informed about the amount that can be charged/paid from your RSBY Card?
Yes
(1)
No
(2)
207
How was the behavior of staff at RSBY help-desk?
Polite=1
Rude=2
No separate helpdesk available=3
208
Did you face any type of discrimination on RSBY help desk based on?
Caste/social group=1
Religion=2
Place=3
Others (Specify)=98
209 What was the total expenditure (Kharcha) on the hospitalization? (in Rs.)
210 What was the amount paid/cost of treatment supported by the RSBY Card? (in Rs.)
211 On discharge was discharge summary provided to the family?
Yes
(1)
No
(2)
Don’t
know
(99)
212 Was the fingerprint verification done at the time of discharge?
Yes
(1)
No
(2)
Don’t
know
(99)
213
When did you get the RSBY/Smart card back?
After swiping at the time of admission=1
On discharge=2
Next day=3
Two days later=4
Others (specify)=98
214 Were you told about the amount of money left in the card at the time of discharge?
Yes
(1)
No
(2)
Don’t
know
(99)

Imact Assessement Study on RSBY
Page | 134
215
How would you rate the behaviour and overall help/support of the staff dealing with
your admission/use of your RSBY Card.
(Please provide your response in a scale of 1-5 where 1=most dissatisfied/very poor and
5=Very satisfied/excellent)
216 Were you told the amount of money available in your Card at the time of discharge?
217
Was any other post-hospitalization expenses covered under RSBY?
No=0
Some medicines provided from hospital=1
Free ambulance/transport to return home=2
Free tests/scan etc on follow-up visits=3
Dressing of wounds etc.=4
Others (specify)=98
218
How would you rate your overall experience in using the RSBY Card at the hospital?
(Please provide your response in a scale of 1-5 where 1=most dissatisfied/very poor
and 5=Very satisfied/excellent)
219
Did you have any complaint/problems during hospital visit?
Use of RSBY card=1
Lack of adequate cost of treatment/amount covered under RSBY=2
For that you were by cheated/mislead in somewhat or the other=3
Others (specify)=98
220 Did you lodge any complaint regarding your grievances?
Yes
(1)
No
(2)
DK/CS
(99)
221
If yes, place of lodging grivabces?
Hospital authorities=1
CSO=2
Others (specify)=3
222 Are you aware about any measures/action taken on the basis of your graviances/
Yes
(1)
No
(2)
DK/CS
(99)
223
Is there any post hospitalization expenses covered under RSBY?
224 Was the patient prescribed any medicines after the discharge?
Yes
(1)
No
(2)
Don’t
know
(99)
225
For how many days the medicines needed to be taken after discharge?(based on discharge summary)
Days=1
Weeks=2
Months=3
Don’t know=98
226 Were these medicines provided by the hospital?
Yes
(1)
No
(2)
Don’t
know
(99)
227 Was the patient prescribed any tests after discharge?
Yes
(1)
No
(2)
Don’t
know
(99)
228 Were facilities for those tests organized by hospital free of cost?
Yes
(1)
No
(2)
Don’t
know
(99)
229
How is health of patient now comparing when he was admitted to the hospital?
Has died=1

Imact Assessement Study on RSBY
Page | 135
No improvement=2
Partially recovered=3
Has recovered completely=4
230
How significant would you consider the financial support you have received under
RSBY, by being a card-holder?
Insignificant/little help/support=1
Somewhat useful/helpful=2
Very useful/helpful=3
BLOCK 6: A. INCOME & LIVELIHOOD
231 What is the major income-earning activity of this household? (Formal sector employment/salaried service=1, Business/petty-trade=2, Self-employment=3, Manual/Wage-labour=4, Traditional
semi-skilled trade=5, Remittance/Doles=6, Others (specify)=98)
Do the household/any members of the household own the following?
232 Mobile phone Yes (1) No (0) DK/CS (99)
233 Motorcycles/scooters Yes (1) No (0) DK/CS (99)
234 Cycle Yes (1) No (0) DK/CS (99)
235 Coolers Yes (1) No (0) DK/CS (99)
236 Television Yes (1) No (0) DK/CS (99)
237 Television with cable/satellite TV connection Yes (1) No (0) DK/CS (99)
238 Any land (in Delhi/native place) Yes (1) No (0) DK/CS (99)
239
Thinking of all the income-earning individuals in this household,
which category would you say the household falls, taking the total
MONTHLY household income/earning?
>5000 1
5000-7500 2
7500-10000 3
10000-15000 4
15000-30000 5
30000-50000 6
50000 & above 7
DK/CS 99
B. Consumption Expenditure
How much money was spent by your household – on
240 (a) Food – during last 7 days
241 (b) Electricity/Water Supply – during last 30 days
242 (c) Transportation (to school/works) – during last 30 days
243 (d) Education of children (including tuition) – during last 30 days
244 (e) Medical care/treatment (all diseases/injuries/by staying illness etc.) during last 30
days
245 (f) Rent/Taxes (for housing) – during last 30 days
(g) Clothing/entertainment (movies/cable rent)/communications(mobile)/travels – during
last 30 days
(h) Domestic durables (TV/bicycle/furniture) – during last 1year
(i) Home repair/constructions – during last 1year
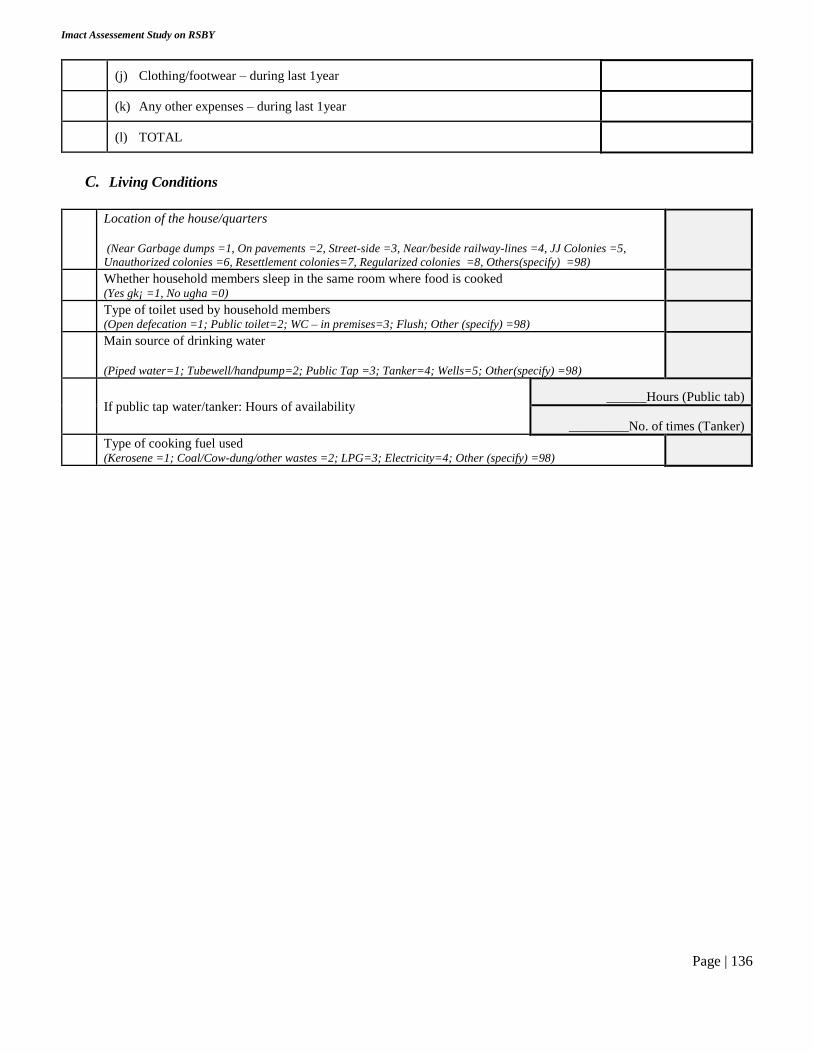
Imact Assessement Study on RSBY
Page | 136
(j) Clothing/footwear – during last 1year
(k) Any other expenses – during last 1year
(l) TOTAL
C. Living Conditions
Location of the house/quarters
(Near Garbage dumps =1, On pavements =2, Street-side =3, Near/beside railway-lines =4, JJ Colonies =5,
Unauthorized colonies =6, Resettlement colonies=7, Regularized colonies =8, Others(specify) =98)
Whether household members sleep in the same room where food is cooked (Yes gk¡ =1, No ugha =0)
Type of toilet used by household members (Open defecation =1; Public toilet=2; WC – in premises=3; Flush; Other (specify) =98)
Main source of drinking water
(Piped water=1; Tubewell/handpump=2; Public Tap =3; Tanker=4; Wells=5; Other(specify) =98)
If public tap water/tanker: Hours of availability ______Hours (Public tab)
_________No. of times (Tanker)
Type of cooking fuel used (Kerosene =1; Coal/Cow-dung/other wastes =2; LPG=3; Electricity=4; Other (specify) =98)

Imact Assessement Study on RSBY
Page | 137
Annex 3 IMPACT ASSESSEMENT STUDY ON RASHTRIYA SWASTHYA BIMA YOJANA (RSBY)
MAIN QUESTIONNAIRE – WEST BENGAL
Sponsored by Poorest Area Civil Society Programme [PACS]
INSTITUTE FOR HUMAN DEVELOPMENT NIDM Building, 3rd Floor, IIPA Campus, I.P Estate, Mahatma Gandhi Marg, New Delhi-110 002
Phones – 2335 8166, 2332 1610 / Fax : 23765410
Email: [email protected]
BLOCK 1: INTERVIEW PARTICULARS
1. Interview ID 5. Supervisor Name and Signature
2. Supervisor ID 6. DEO Name and Signature
3. Data Entry Operator ID 7. Interview/Re-interview status
4. Interview er Name and Signature 8. Interview Date and Start-time
BLOCK 2: HOUSEHOLD IDENTIFICATION PARTICULARS
1 District 7 Gram Panchayat
2 PSU No. (Unique code) 8 Village Name
3 Block 9
Caste Category
(SC=1, ST=2, OBC=3, General=4)
4 Unique Household Identification
No. (UHID) 10
Religion
(Hindu=1, Muslim=2, Christian=3,
Others=4)
5 Name of Household Head 11 Highest educational attainment in
the household
1. SEGMENT 2. SUB-GROUP
A. RSBY Beneficiary Sample A. Minority
B. RSBY Non-Beneficiary sample B. ST
C. SC/OBC
Informed Consent Statement
INTERVIEWER – (Read out): Namaskar. My name is (please say your name here) and I work for Institute for Human Development, a
research institute in New Delhi. Your household has been selected to collect some detailed information on health and health care aspects
and the amount you have spent on health care for your family member, and your use and experience of the national health insurance scheme,
RSBY. It will take about 45 minutes for you to answer the questions. You can choose not to answer any questions or refuse participating in
the interview at any point of time throughout the interview. The information you provide will be confidential and used for research purposes only. If you can spare the time now, and with your permission, can I start the interview now?

Imact Assessement Study on RSBY
Page | 138
BLOCK 3: HOUSEHOLD MEMBER ROSTER
C. Demographics and Socioeconomics
Details of all family members: In order to determine whom to interview, I need to know who lives at this address. Let me
assure you that any information you provide is strictly confidential. I would like the age, sex, education, marital status and
relationship to you of each of the members of this household who live here. All the members in the household should be
entered first, from oldest to youngest.
1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9 1.10 1.11 1.12
1.1
Lin
e No
.
1.2
Name
1.3
Sex
1.4
Relatio
nsh
ip
with
hou
seho
ld
head
1.5
Age
1.6
Marital
status
1.7
Hig
hest
edu
cation
al
level
1.8
Usu
al
activity
status
1.9
Wh
ether
suffered
from
any
min
or
illnesses
durin
g la
st 1
mo
nth
1.1
0
Wh
ether
suffers fro
m
any
chro
nic
diseases
since la
st 12
mo
nth
s?
1.1
1
Wh
ether
hosp
italized
ever d
urin
g
last 1
2
mo
nth
s
1.1
2 A
ny
health
schem
e/insu
r
ance
1
2
3
4
5
6
7
8
9
CODES
For 1.3: Sex male=1, female=2
For 1.4: Relation to head self=1, spouse of head=2, married child=3, spouse of married child=4, unmarried chiId=5, grand child=6, father/mother/father-in-
law/mother-in-law=7, brother/sister/brother-in-law/sister-in-law/other relative=8, servant/employees/other non-relatives=9
For 1.6: Marital status never married=1, currently married=2, widowed=3, divorced/separated=4
For 1.7: Educational level Illiterate=01; literate but never gone to school=02, Upto class 4=03, Upto class=04, Completed class 10=05, completed class 12=
06, completed Graduation= 07, Any higher education above graduation=08

Imact Assessement Study on RSBY
Page | 139
For 1.8: Usual activity status Casual/daily wage laborer=01, Self-employed (including small business & trade)=02, Regular salaried employment=03,
Unemployed/seeking work=04, Student=05, Home-maker/household work/domestic duties (unpaid)=06, Disabled/Old/Young=07, Household
entrepreneur (tailoring/weaning/hand wash)=08, Others=99 (Specify)
For Q.1.9 to 1.12: Yes=1, No=0, don’t know/can’t say=99.
Note: Q1.9: When suffered from any common/minor/short-term illness in last 30 days (such as – fever/cold & cough/loose motion…….etc.) Q 1.10: Diabetes/cancer/hypertension/heart alignments/heart alignment/respiratory problems/tuberculosis/arthritis/long standing pain in bone/joints)
D. Social Networks
Is anyone in the family presently a member of any of the followings :
B1 Self Help Group (SHG)/Credit Cooperatives Yes (1) No (0) DK/CS (99)
B2 NGO/MFI (Micro Finance Institution) client Yes (1) No (0) DK/CS (99)
B3 Trade unions Yes (1) No (0) DK/CS (99)
B4 Political party Yes (1) No (0) DK/CS (99)
B5 Religious organization Yes (1) No (0) DK/CS (99)
B6 Local CBO’s (Community Based Organizations) Yes (1) No (0) DK/CS (99)
Do you or your family members personally know the Gram Panchayat/Local MLA/MP/any other elected member of your AREA?
Yes (1) No (0) DK/CS (99)
Number of times you did the following during last 7 days/in last week?
B7 Watch TV Never (1) Rarely (2) Daily (3)
B8 Listen Radio Never (1) Rarely (2) Daily (3)
B9 Read Newspaper/magazines Never (1) Rarely (2) Daily (3)
B10
What are your main sources of your information regarding government programmes/schemes?
(Multiple Answers)
Friends and family-members =1,
Media (Audio-Visual/Print)=2,
Local government workers (ANM, AWW) =3,
Political party, workers/leaders/elected representatives =4,
Religious leaders/places of worship-=5,
Local NGO/CBO members =6,
Others(specify)=98, Don’t Know/CS=99

Imact Assessement Study on RSBY
Page | 140
BLOCK 4: HEALTH STATUS AND HEALTH CARE UTILIZATION
Minor Ailments during last 30 days (Non-Hospitalized)
4.1 Srl. no. of ailment 1 2 3 4 5
4.2 Srl. no. of member reporting ailment (COPY LINE NUM. – Q
1.1)
4.3 Nature of ailment (code on page no 4)
4.4 Total duration of ailment (days): Days Ill
4.5 Total duration of ailment (days): Days of restricted activity
4.6 Total duration of ailment (days): Days confined to bed
4.7 Did you/[member] receive any medical treatment for this ailment?
(Yes-1, No-2)
4.8 If not (Q 4.7=2)
Reasons for not seeking/receiving any medical treatment:
No medical facility available in the neighbourhood - 1
Lack of faith - 2
Long waiting - 3
Financial reasons - 4
Ailment not considered serious – 5
Others – 98
4.9 If yes (Q 4.7=1)
Type of health service provider/health facility from where
treatment was sought?
Govt. clinic/dispensary-1
Govt hospital-2
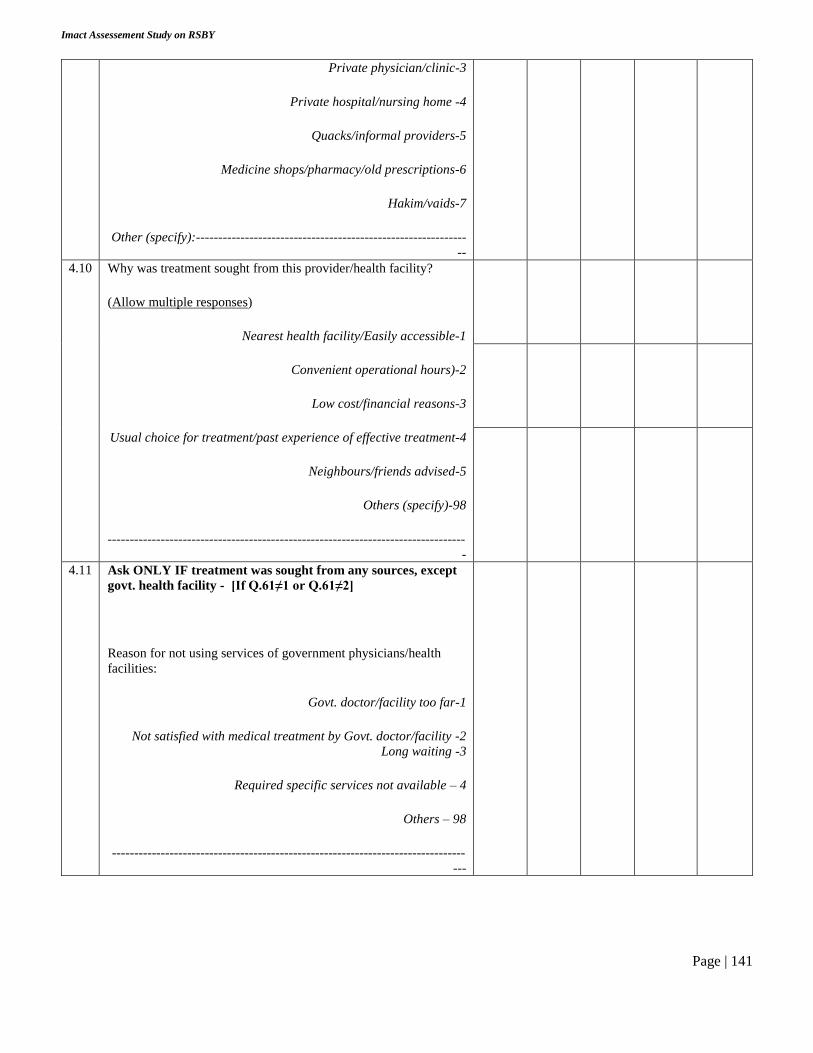
Imact Assessement Study on RSBY
Page | 141
Private physician/clinic-3
Private hospital/nursing home -4
Quacks/informal providers-5
Medicine shops/pharmacy/old prescriptions-6
Hakim/vaids-7
Other (specify):-------------------------------------------------------------
--
4.10 Why was treatment sought from this provider/health facility?
(Allow multiple responses)
Nearest health facility/Easily accessible-1
Convenient operational hours)-2
Low cost/financial reasons-3
Usual choice for treatment/past experience of effective treatment-4
Neighbours/friends advised-5
Others (specify)-98
---------------------------------------------------------------------------------
-
4.11 Ask ONLY IF treatment was sought from any sources, except
govt. health facility - [If Q.61≠1 or Q.61≠2]
Reason for not using services of government physicians/health
facilities:
Govt. doctor/facility too far-1
Not satisfied with medical treatment by Govt. doctor/facility -2
Long waiting -3
Required specific services not available – 4
Others – 98
--------------------------------------------------------------------------------
---

Imact Assessement Study on RSBY
Page | 142
Now, I would like to collect some information on the expenses incurred for treatment of the illnesses of all your family members you
have just described, during the last 30 days.
I will require expenses incurred on different purposes and also from where/which sources did you manage to pay.
Please provide amount spent on
(Column 1)
Total cost
(Column 2)
Amount paid
out-of pocket
(own income and
savings)
(Column 3)
Amount from
other sources
(Column 4)
Source
(Column 5)
4.12 Doctor’s fee
4.13 Diagnostic tests
4.14 Medicine/injections
4.15 Bed charges
4.16 Surgery charges
4.17 Any special diet/other food
4.18 Follow-up costs
4.19 Transportation (including
ambulance)
4.20 Any other indirect costs (wage loss
of attendants etc.)
4.21 Total expenses
Instructions:
For Column 2: Ask respondent whether entire amount was met with self-income/salary/from other household member. If so,
copy the total costs from Col.2 to Col. 3 and skip col.4 & col.5
For Column 4: Include amount that was supported/financed by other sources
For Column 5: Include the source for the amount included in (IV).
Codes:
1=Borrow from friend/neighbor/relatives (without interest)
2=Loans from office/employer (without interest)
3=Paid by the employer, not t be paid back
4=Loan (with interest) from money lenders or others
5=Selling any assets
98=Others (specific)
----------------------------------------------------------------------------------------------------------------------------- ---------------------------
4.22
If the respondent is unable to give break-up of the
expenses incurred (and its financing sources), ASK
THE FOLLOWING QUESTION:
How were the expenses met?
(Multiple responses possible)
Self savings 1
Employer paid 2
Friends/family 3
Health insurance (others) 4
Borrowings from money lenders with
interest 5
Selling of assets 6
Others (specify):
4.23
Was it of any difficulty for your family/yourself to
meet the costs associated with the treatment, and
spending the amount you mentioned, for the
diseases during last 30 days?
Extremely difficult 1
Somewhat difficult 2
Not at all 3
4.24 Number of days confined to bed/absent in work

Imact Assessement Study on RSBY
Page | 143
CODES FOR DISEASES:
Disease code Disease code
Diarrhoea/ dysentery 01 Diphtheria 21
Gastritis/gastric or peptic ulcer 02 Whooping cough 22
Hepatitis/Jaundice 03 Fever of unknown origin/Other fevers 23
Heart disease 04 Cough and cold 24
Hypertension 05 Filariasis/Elephantiasis 25
Respiratory including ear/nose/throat ailments 06 Diseases of Mouth/Teeth/Gum 26
Tuberculosis 07 Accidents/Injuries/Burns/ 27
Bronchial asthma 08 Fractures/Poisoning 28
Disorders of joints and bones 09 Cancer and other tumours 29
Diseases of kidney/urinary system 10 Disabilities
Prostatic disorders 11 Locomotor 30
Gynaecological disorders 12 Visual including blindness (excluding 31
Psychiatric disorders 13 cataract) 32
Eye ailments (Conjunctivitis/Cataract) 14 Speech 33
Diabetes mellitus 15 Hearing 34
Anaemia 16 Other diagnosed ailments 100
Sexually transmitted diseases 17
Malaria 18
Typhoid 19
Encephalitis 20
BLOCK 5: HEALTH STATUS AND HEALTH CARE UTILIZATION Hospitalized Illnesses During Last 365 Days
5.1 Sr1. no. of the hospitalisation case 1 2 3 4 5
5.2 Srl. no. of member hospitalized (COPY LINE NO.- Q 1.10)
5.3 Type of hospital
Any Govt hospital=1

Imact Assessement Study on RSBY
Page | 144
Private hospital/nursing home (including NGO/trust hospitals)=2
Other (specify)=98
5.4 Nature of ailment (code above)
5.5 Type of ward (free - 1, paying general - 2, paying special - 3)
5.6 Duration of stay in hospital (days)
5.7 Did [member] receive any treatment before hospitalisation for the
ailment mentioned in Q 5.4 (Yes - 1, No - 2)
5.8
If 1
in
item
5.7
Source of treatment:
Govt. clinic/dispensary-1
Govt hospital-2
Private physician/clinic-3
Private hospital/nursing home -4
Quacks/informal providers-5
Medicine shops/pharmacy/old prescriptions-6
Hakim/vaids-7
Other (specify):---------------------------------------------
5.9 Duration of treatment (days)
5.10 Current status of the member:
(Fully cured-1, Partially cured, under treatment-2, Partially
cured, but no treatment ongoing-3 )

Imact Assessement Study on RSBY
Page | 145
Now, I would like to collect some information on the expenses incurred for all episodes/events of Hospitalization for all members of this household, on all diseases
DURING LAST 12 MONTHS
From the illnesses and hospitalizations you have been describing, I will require expenses incurred on different purposes, and also from where/which sources did you manage to
pay. (In case of multiple episodes, information from the most recent)
Please provide amount spent on
(Column 1)
Total cost
(Column 2)
Amount paid
out-of pocket
(own income and
savings)
(Column 3)
Amount from
other sources
(Column 4)
Source
(Column 5)
Amount
provided under
RSBY
(Column 6)
5.11 Doctor’s fee
5.12 Diagnostic tests
5.13 Medicine/injections
5.14 Bed charges
5.15 Surgery charges
5.16 Any special diet/other food
5.17 Follow-up costs
5.18 Transportation (including ambulance)
5.19 Any other indirect costs (wage loss of
attendants etc.)
5.20 Total expenses
Instructions:
For Column 2: Ask respondent whether entire amount was met with self-income/salary/from other household member. If so, copy the total costs from Col.2
to Col. 3 and skip col.4 & col.5
For Column 4: Include amount that was supported/financed by other sources
For Column 5: Include the source for the amount included in (IV). If answers ‘6’ (RSBY) complete the entries for Q 5.20 for Column 6
Codes:
1=Borrow from friend/neighbor/relatives (without interest)
2=Loans from office/employer (without interest)
3=Paid by the employer, not t be paid back
4=Loan (with interest) from money lenders or others

Imact Assessement Study on RSBY
Page | 146
5=Selling any assets
6=RSBY
98=Others (specific)
----------------------------------------------------------------------------------------------------------------------------- ---------------------------
5.23
If the respondent is unable to give break-up of the expenses incurred
(and its financing sources), ASK THE FOLLOWING QUESTION:
How were the expenses met?
(Multiple responses possible)
Self savings 1
Employer paid 2
Friends/family 3
RSBY 4
Health insurance (others) 5
Borrowings from money lenders with
interest 6
Selling of assets 7
Others (specify)
5.24
Loss of household income, if any, due to hospitalization of [member]
(Rs)
Instruction: Include loss of wage for the hospitalized member (if working)
5.25
Was it of any difficulty for your family/yourself to meet the costs
associated with the hospitalizations of your household members, and
spending the amount you mentioned?
Extremely difficult 1
Somewhat difficult 2
Not at all 3
BLOCK 6: Accidental Injury, Treatment and Financing During Last 365 Days
6.1
Did you/any household member suffer from any accidents or an injury in the
past 12 months that required medical treatment?
(Ignore minor cuts/bruises; include those that required medical treatment)
Yes
(1)
No
(0)
If no, Skip to next
Section
6.2 Indicate which members suffered such injuries: ID-1 ID-2

Imact Assessement Study on RSBY
Page | 147
(Instruction – Copy Member Line Number from Block- 3, Q 1.1)
6.3
Type of accident/Mechanism of Injury
Codes:
1=motor vehicle, 2=pedestrian-vehicle crash, 3=motorcycle, 4=bicycle,
5=fall, 6=gunshot/firearms, 7=stab/cuts, 8=fire/burns, 9=poisoning,
10=drowning , 11=others , 98=Others (specify); 99=DK/CS)
6.4
Where did the injury occur?
Codes:
1=home , 2=school, 3=streets/highways/railways, 4=trade & service areas
(shops, offices), 5=water bodies, 6=industrial/construction
6.5
Which body parts/organs were injured/affected by the accident?
Codes:
Head =1; Limb =2; Chest =3; Shoulder/neck/back =4; Internal organ =5
6.6
How you /your family did come to know about the accident/injury of the
member?
(1=police, 2=hospital authorities, 3=friends/neighbors, 4=unknown
strangers; 98=Others (specify)
6.7
Did you/member receive any medical attention/treatment at the
accident/injury site?
(0=No, 1=Yes, 99=DK/CS)

Imact Assessement Study on RSBY
Page | 148
6.8 Were you/member taken/went to any hospital/clinic to receive treatment after
the injury/accident? (0=No, 1=Yes, 99=DK/CS)
6.9
Type of the facility
Govt. clinic/dispensary =01;
Govt hospital =02;
Private physician/clinic =03;
Private hospital/nursing home (including NGO/trust hospitals) =04;
Quacks/informal providers =05;
Hakim/vaids=07;
Other (specify) =98)
6.10
How were you/member taken/went to the hospital/clinic/physician mentioned
in Q 198?
Codes:
1=Govt ambulance, 2=pvt. Ambulance, 3=pvt vehicles 4=police vehicles
5=rickshaw/vans, 98= Others (specify); 99=DK/CS
6.11
Reasons for seeking care/treatment from the particular facility?
Nearest health facility/convenientworking hours =01
Low cost/financial reasons =02
Usual choice for treatment/past experience of effective treatment=03
Neighbours/friends advised=04
Taken by police/other persons/ambulance=05
98=Others
6.12
Did you/member receive immediate treatment (including examination,
dressing of the wound, applying bandages/casts, diagnostic tests/scans) after
arriving at the health facility?
(1=Yes,2=No, 99=DK/CS)

Imact Assessement Study on RSBY
Page | 149
6.13
How satisfied were you by the overall quality of treatment/care received
while being treated for the accident/injury at the health facility?
Rate in a scale of 1-5, with 1=Extremely dissatisfied and 5=Very Satisfied
6.14
Did the accident/injury require any hospitalization/in-patient stay of the
member?
(0=No, 1=Yes, 99=DK/CS)
6.15 Days of stay
6.16 Total duration of treatment (include hospitalizations and any follow-up visits)
Total expenditure incurred on account of treatment and related expenses due to the accident/injury of the member in last 12
months?
Please provide amount spent on
(Column 1)
Total cost
(Column 2)
Amount paid
out-of pocket
(own income and
savings)
(Column 3)
Amount from
other sources
(Column 4)
Source
(Column
5)
Amount
provided under
RSBY
(Column 6)
6.17 Doctor’s fee
6.18 Diagnostic tests
6.19 Medicine/injections
6.20 Bed charges
6.21 Surgery charges
6.22 Any special diet/other food
6.23 Follow-up costs
6.24 Transportation (including
ambulance)
6.25 Any other indirect costs (wage loss
of attendants etc.)
6.26 Total expenses
Instructions:
For Column 2: Ask respondent whether entire amount was met with self-income/salary/from other household member. If so, copy
the total costs from Col.2 to Col. 3 and skip col.4 & col.5
For Column 4: Include amount that was supported/financed by other sources
For Column 5: Include the source for the amount included in (IV). If answers ‘6’ (RSBY) complete the entries for Q 5.20 for
Column 6
Codes:
1=Borrow from friend/neighbor/relatives (without interest)

Imact Assessement Study on RSBY
Page | 150
2=Loans from office/employer (without interest)
3=Paid by the employer, not t be paid back
4=Loan (with interest) from money lenders or others
5=Selling any assets
6=RSBY
98=Others (specific)
----------------------------------------------------------------------------------------------------------------------------- ---------------------------
6.27
What has been the major source of finance for the treatment?
[Note: These questions are to be asked if the respondent is unable to give
break-up of the expenses incurred (and its financing sources]
Self savings =1, Employer paid=2, Friends/family =3, Health ins-RSBY =4,
Health insurance (others;)=5, Borrowings from money lenders with interest
=6, Selling of assets =7, Others =8, Others (specify)=98; DK/CS=99
6.28
Was it of any difficulty for your family/yourself to meet the costs associated
with member’s treatment, and spending the amount you mentioned?
1=Extremely difficult , 2=Somewhat difficult, 3=Not at all
6.29
Are you/hh member restricted in any of the following areas as a result of this accident / injury?
Codes: Completely=1, Partially/somewhat=2, Not at all=3

Imact Assessement Study on RSBY
Page | 151
a) Attending work on a full-time/pre-accident/injury leaves
b) Attending school regularly
c) Attend daily living activities (bathing/driving/walking/using toilets)
d) Attend daily household chores (outing/shopping/managing
household finance etc.)
e) Any disability
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
6.30
Total number of days missed at work due to this accident / injury?
(Include number of days. If not lost any days include ‘0’)
6.31
How difficult you found to adjust with the loss of work / financial hardships, following the accident?
Rate in a scale of 1-3, with 1=Extremely difficult;2=Somewhat difficult; Not difficult at all=3
6.32
How would you rate the current health status/condition of the member, with respect to the
accident/injury
Rate in a scale of 1-5, with
Very poor=1; Poor=2; Somewhat OK/moderate=3; Good=4 and 5=Excellent
BLOCK 7: Welfare Impacts Of Health Shocks & Coping Mechanisms
7.1
Considering all events of diseases/illnesses, hospitalizations,
accidents, injury experienced by your family members in last 1
year, how would you rate the impact of all these events taken
together, on the economic status/capacity of your household?
Instruction to Investigator: If answers ‘No effect’=5, SKIP TO
Q 7.13
Very severe impact 1
Severe impact 2
Moderate impact 3
Partial impact 4
No effect 5
7.2
Do you consider that your family has fully recovered, partially
recovered, or not at all recovered from the financial impacts of
the health shocks - taking all of these adverse health events
together?
Completely recovered 1
Partially recovered 2
Not at all recovered 3
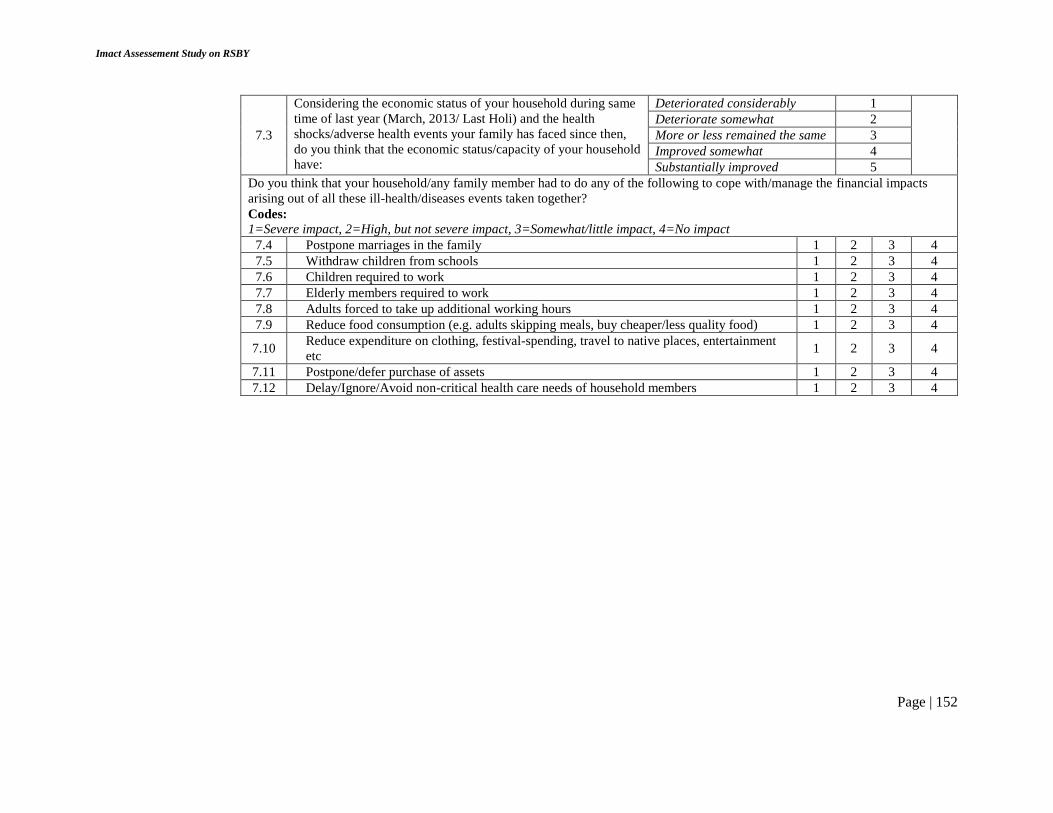
Imact Assessement Study on RSBY
Page | 152
7.3
Considering the economic status of your household during same
time of last year (March, 2013/ Last Holi) and the health
shocks/adverse health events your family has faced since then,
do you think that the economic status/capacity of your household
have:
Deteriorated considerably 1
Deteriorate somewhat 2
More or less remained the same 3
Improved somewhat 4
Substantially improved 5
Do you think that your household/any family member had to do any of the following to cope with/manage the financial impacts
arising out of all these ill-health/diseases events taken together?
Codes:
1=Severe impact, 2=High, but not severe impact, 3=Somewhat/little impact, 4=No impact
7.4 Postpone marriages in the family 1 2 3 4
7.5 Withdraw children from schools 1 2 3 4
7.6 Children required to work 1 2 3 4
7.7 Elderly members required to work 1 2 3 4
7.8 Adults forced to take up additional working hours 1 2 3 4
7.9 Reduce food consumption (e.g. adults skipping meals, buy cheaper/less quality food) 1 2 3 4
7.10 Reduce expenditure on clothing, festival-spending, travel to native places, entertainment
etc 1 2 3 4
7.11 Postpone/defer purchase of assets 1 2 3 4
7.12 Delay/Ignore/Avoid non-critical health care needs of household members 1 2 3 4

Imact Assessement Study on RSBY
Page | 153
7.13 Would you be able to raise Rs. 10,000 in one week if you needed it for some
emergency?
Yes
(1)
No
(0)
DK/CS
(99)
7.14
How would you raise Rs. 10,000?
Mention top 3 sources in the order you would follow
(Selling durable goods/equipment =1, Selling land/house =2 , From
savings=3, From relatives/friends =4, From employer=5, From
moneylender=6, Taking extra work=7, From any
MFI/cooperative/NBFI=8; Others (specify) =98; DK/CS=99 )
1st 1 2 3 4 5 6 7 8 9 99
2nd 1 2 3 4 5 6 7 8 9 99
3rd 1 2 3 4 5 6 7 8 9 99

Imact Assessement Study on RSBY
Page | 154
BLOCK 8: Quality Of Medical Services/Quality Of Care
8.1
Have you PERSONALLYvisited/accompanied any
patient to any health provider/ hospital/clinic for
out- patient care (OPD) in last 12 months?
(A) (B)
Yes
(1)
No
(2)
If - Yes (1), type of provider/health facility
Government hospital (1)
Private hospital/nursing/clinics (2)
Private practitioner (3)
Informal providers/Jhola chap etc.(4)
8.2
Have you been hospitalized/spent time with other
family members during hospitalization in- patient
care in last 12 months? Yes
(1)
No
(2)
If - Yes (1), type of provider/health facility
Government hospital (1)
Private hospital/nursing/clinics (2)
Private practitioner (3)
Informal providers/Jhola chap etc.(4)
INSTRUCTION TO THE INVESTIGATOR:
In the space provided below, write the type of provider/health facility for both OPD and In-patient care.
Copy the codes for OPD from Q 8.1 (B) and for In-patient care from Q 8.2 (B).
Then continue asking the questions in Column 2, and insert the answers in Column 3 (OPD) and Column 4 (IPD). First
complete all Column 3 (OPD) entries before starting asking the responses for Column 4 (IPD)
For each of the following aspects of treatment, and your experience at the health facility, or about the physician, please rank the provider or health
facility in Column 3/Column 4 in a scale of 1 to 5, where
1=Very good or Very satisfactory, and 5=Very Poor or Very unsatisfactory
Column 2
Column 3 Column 4
OPD Code:
IPD Code:

Imact Assessement Study on RSBY
Page | 155
8.3 Skill and Competency of the staff/physician 1 2 3 4 5 1 2 3 4 5
8.4 Overall Cleanliness 1 2 3 4 5 1 2 3 4 5
8.5 Friendliness and courtesy of the staff 1 2 3 4 5 1 2 3 4 5
8.6 Effectiveness of the treatment and medicine prescribed 1 2 3 4 5 1 2 3 4 5
8.7 Cost of the treatment 1 2 3 4 5 1 2 3 4 5
8.8 Ease of communicating treatment/ therapy 1 2 3 4 5 1 2 3 4 5
8.9 Distance/Accessibility 1 2 3 4 5 1 2 3 4 5
8.10 Waiting Time 1 2 3 4 5 1 2 3 4 5
8.11 Cleanliness/ Environment 1 2 3 4 5 1 2 3 4 5
8.12 Lack of Privacy during consultation/ overcrowding 1 2 3 4 5 1 2 3 4 5
8.13 Behaviour of staff/ physician 1 2 3 4 5 1 2 3 4 5
8.14 Cost of treatment 1 2 3 4 5 1 2 3 4 5
8.15 Effectiveness of the treatment and medicine prescribed 1 2 3 4 5 1 2 3 4 5
8.16 Friendliness of the doctor 1 2 3 4 5 1 2 3 4 5
8.17 Friendliness of nurses/other staff 1 2 3 4 5 1 2 3 4 5
8.18 Convenience of working hours 1 2 3 4 5 1 2 3 4 5
8.19 Explanation of diagnosis and treatment 1 2 3 4 5 1 2 3 4 5
8.20 Facilities for emergency treatment 1 2 3 4 5 1 2 3 4 5
8.21 Availability of drugs and medicines 1 2 3 4 5 1 2 3 4 5
8.22 Confidence in the treatment provided 1 2 3 4 5 1 2 3 4 5
8.23 Effetiveness of of the treatment provided 1 2 3 4 5 1 2 3 4 5
BLOCK 9: RSBY-INTERVENTION: WEST BENGAL
Section A: Screening and Non-beneficiaries
ASK TO ALL HOUSEHOLDS
Now, I would like to ask you a few questions regarding your Knowledge with the RSBY scheme.
9A.1 Are you aware of a government scheme/programme that covers hospitalization expenses for
families such as yours?
Yes
(1)
No
(2)
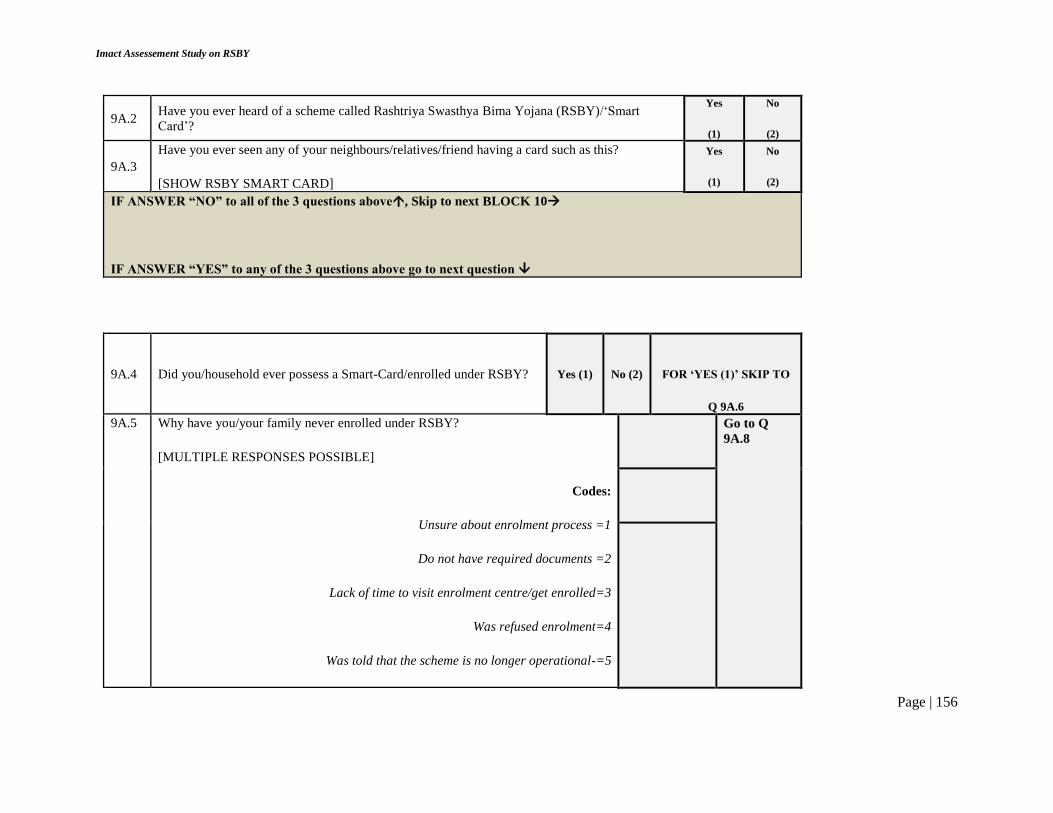
Imact Assessement Study on RSBY
Page | 156
9A.2 Have you ever heard of a scheme called Rashtriya Swasthya Bima Yojana (RSBY)/‘Smart
Card’?
Yes
(1)
No
(2)
9A.3
Have you ever seen any of your neighbours/relatives/friend having a card such as this?
[SHOW RSBY SMART CARD]
Yes
(1)
No
(2)
IF ANSWER “NO” to all of the 3 questions above, Skip to next BLOCK 10
IF ANSWER “YES” to any of the 3 questions above go to next question
9A.4 Did you/household ever possess a Smart-Card/enrolled under RSBY?
Yes (1)
No (2)
FOR ‘YES (1)’ SKIP TO
Q 9A.6
9A.5 Why have you/your family never enrolled under RSBY?
[MULTIPLE RESPONSES POSSIBLE]
Codes:
Unsure about enrolment process =1
Do not have required documents =2
Lack of time to visit enrolment centre/get enrolled=3
Was refused enrolment=4
Was told that the scheme is no longer operational-=5
Go to Q
9A.8

Imact Assessement Study on RSBY
Page | 157
Unaware about the actual benefit =6
Considers that the benefit will be too little=7
Unsatisfactory experience of friends/neighbours =8
Name not included in the BPL lists= 9
98=Others (Specify)
99=Can’t say/DK
9A.6
Is your RSBY Smart Card currently valid (enrolled during the last
phase)?
Instruction: If respondent is not sure, check Smart Card to confirm
Yes
(1)
No
(2)
For ‘Yes (1)’ skip to
Q 9A.8
Reasons for not renewing the Smart-Card for current year?
[MULTIPLE RESPONSES POSSIBLE]
Codes:
Considered RSBY of little/no use = 1
Lack of time to visit enrolment centre/get enrolled=3
Was refused enrolment=4
Was told that the scheme is no longer operational-=5
Did not receive any information on renewal/enrolment =6
Unsatisfactory experience of using Card by self/friends/neighbours =7
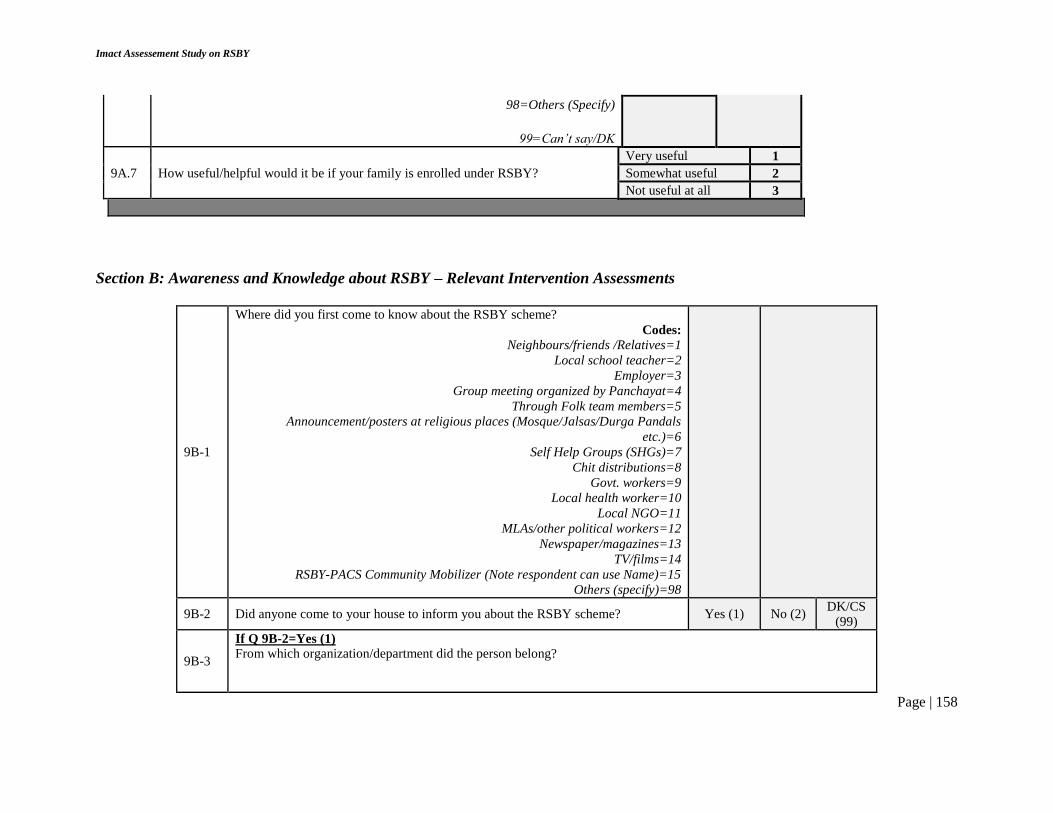
Imact Assessement Study on RSBY
Page | 158
98=Others (Specify)
99=Can’t say/DK
9A.7 How useful/helpful would it be if your family is enrolled under RSBY?
Very useful 1
Somewhat useful 2
Not useful at all 3
Section B: Awareness and Knowledge about RSBY – Relevant Intervention Assessments
9B-1
Where did you first come to know about the RSBY scheme?
Codes:
Neighbours/friends /Relatives=1
Local school teacher=2
Employer=3
Group meeting organized by Panchayat=4
Through Folk team members=5
Announcement/posters at religious places (Mosque/Jalsas/Durga Pandals
etc.)=6
Self Help Groups (SHGs)=7
Chit distributions=8
Govt. workers=9
Local health worker=10
Local NGO=11
MLAs/other political workers=12
Newspaper/magazines=13
TV/films=14
RSBY-PACS Community Mobilizer (Note respondent can use Name)=15
Others (specify)=98
9B-2 Did anyone come to your house to inform you about the RSBY scheme? Yes (1) No (2) DK/CS
(99)
9B-3
If Q 9B-2=Yes (1)
From which organization/department did the person belong?

Imact Assessement Study on RSBY
Page | 159
9B-4
Who is eligible for this scheme?
Everyone=1
BPL families=2
Antyoday Anna Yojana families=3
NREGA card holders with 15 days of work=4
Others(specify)=5
Don’t know=98
9B-5
How many family members can be enrolled?
At most 5 members=1
All household members=2
Others (specify)=98
Don’t know=99
9B-6 Which members of the family are compulsory to enroll in RSBY scheme?
9B-7 How much does it cost to enroll in this scheme? (in Rs.)
9B-8 What is the maximum amount per year that can be spent under RSBY scheme?
9B-9
What kind of treatment is provided free of cost under RSBY/Smart Card? (Prompt)
Hospitalized treatment=1
Home based treatment=2
Outdoor/Clinic visits=3
Others (specify)=98
Don’t know=99
9B-10 Are transportation allowances provided to the patient under RSBY scheme? Yes
(1)
No
(2)
Don’t know
(99)
9B-11 Do you pay for the diagnostic tests (Examples: X-ray/ECG/EEG/Scan) during
hospitalisation if you enroll in this scheme?
Yes
(1)
No
(2)
Don’t know
(99)
9B-12 Do you pay for medicines and drugs in case of hospitalisation if you enrol in this
scheme?
Yes
(1)
No
(2)
Don’t know
(99)
9B-13
From where did you get the information related to the different provisions of the
RSBY scheme?
Codes:
Neighbours/friends /Relatives=1
Local school teacher=2
Employer=3
Group meeting organized by Panchayat=4
Through Folk team members=5

Imact Assessement Study on RSBY
Page | 160
Announcement/posters at religious places (Mosque/Jalsas/Durga Pandals
etc.)=6
Self Help Groups (SHGs)=7
Chit distributions=8
Govt. workers=9
Local health worker=10
Local NGO=11
MLAs/other political workers=12
Newspaper/magazines=13
TV/films=14
RSBY-PACS Community Mobilizer (Note respondent can use Name)=15
Others (specify)=98
Have you noticed/observed any of the following activities in your village/community that had provided any
information on RSBY (such as, enrolment process, how to use the card etc)?
Codes: Yes=1, No=2, Can’t say/Not sure=3
9B-14 Mike announcements in the community/village 1 2 99
9B-15 Rallies/Processions 1 2 99
9B-16 Tableau 1 2 99
9B-17 Video shows/Film shows 1 2 99
9B-18 Puppet shows 1 2 99
9B-19 Drama/Plays/Street plays 1 2 99
9B-20 Folk-song (Bhawaiya)/Folk-art (Patachitra) Teams 1 2 99
9B-21 Wall writing/Posters 1 2 99
9B-22
How often have you noticed such awareness related activities on RSBY scheme in
your community?
Twice or more in a month=1
Monthly=2
Every two months=3
More than two months=4
Once/twice in the last 1 year=5
Others (specify)=98
Don’t know=99
Show IEC materials and test familiarity.
Show the exhibits provided according to the number, and ask the questions:
9B-23 Have you seen the following?
Exhibit 1
Yes (1), No (2), Not sure (99)
1 2 99

Imact Assessement Study on RSBY
Page | 161
Exhibit 2
Exhibit 3
Exhibit 4
Exhibit 5
1 2 99
1 2 99
1 2 99
1 2 99
9B-24
How useful do you think these materials are in providing required information
about enrolment and using different facilities and provisions under RSBY?
Exhibit 1
Exhibit 2
Exhibit 3
Exhibit 4
Exhibit 5
Very useful (1), Somewhat
useful (2), Not at all useful (3),
DK/CS (99)
1 2 3 99
1 2 3 99
1 2 3 99
1 2 3 99
1 2 3 99
9B-25
Have you seen or heard any mike announcements/posters and banners at/from any
of the following places related to information on RSBY?
Mosque/Dargaah/Temple/etc.=1
Durga puja pandals=2
Kirtans=3
Jalsas/Cultural functions=4
Not seen any announcements in any of the above palces =5
Put the codes for which
answers ‘Yes’
9B-26
If Q 9B-25=1,2,3,or 4 (Seen/Heard the announcements)
What information did you get on RSBY scheme from these announcements/mass-
media? (Read out each)
Eligibility criteria=1
Benefits of the scheme=2
No. of person in a family to get the benefit=3
Amount needed for registration=4
Hospitalization criteria=5
Process of transaction=6
Put the codes for which
answers ‘Yes’
9B-27 Did you find it useful? Yes
(1)
No
(2)
9B-28
Were any of the following initiatives taken
by the local Panchayat or Govt.
Departments to raise the awareness on
RSBY scheme?
Yes(1) No(2) DK/CS (99)
Community gatherings
Gram Sabha/VHND meetings
Workshops

Imact Assessement Study on RSBY
Page | 162
Home visits by ANM/AWW
Public announcements
Distributing leaflets
If at least for one of the options of 9B-28, answer is ‘Yes (1)’ continue with next question, otherwise SKIP TO Q
9B-29
How often have you noticed such activities by Panchayat/Govt departments?
Twice or more in a month=1
Monthly=2
Every two months=3
More than two months=4
9B-30
What information did you get on RSBY scheme from the initiatives taken by the
Panchayat/govt departments?
Codes:
Eligibility criteria=1
Benefits of the scheme=2
No. of person in a family to get the benefit=3
Amount needed for registration=4
Hospitalization criteria=5
How to use the Card=6
What to do in case of any problems/complaints=7
Put the codes for which answers
‘Yes’
9B-31 Have you heard about RSBY Sahayata Kendra? Yes
(1)
No
(2)
If ‘No (2)’ SKIP TO
Section C
9B-32
How did you come to know about RSBY Sahayata Kendra?
Self=1
Neighbours/Friends/Relatives=2
Local school teacher=4
Employer=5
Govt. workers=6
Local health worker=7
Local NGO=8
MLAs/other political workers=9
RSBY-PACS Community mobilize=10
Others (specify)=98

Imact Assessement Study on RSBY
Page | 163
Section C: Enrolment and Orientation
Instruction for Investigators: Please collect the information for first enrolment only, and make it clear that we are not looking for information related to
renewal.
9C-1
Who encouraged you to apply for the RSBY scheme?
[MULTIPLE RESPONSES POSSIBLE]
Codes:
Self-motivated/nobody in particular=1
Relatives/ Neighbours/Friends/Interpersonal communication = 2
Group meeting organized by Panchayat/Gram Sabha/Govt Departments=3
Local folk-art/IEC team members=4
Announcement at religious places (Mosque/Temple etc.)=5
Self Help Groups (SHGs)=6
Chit distributions=7
ANM/ASHA/AWW durng Home visits=8
Local school teacher=9
Employer=10
Govt. workers=11
MLAs/other political workers=12
RSBY-PACS Community mobilizer=13
Others (specify)=98
9C-2
Who informed you about the RSBY enrolment process?
[MULTIPLE RESPONSES POSSIBLE]
Codes: Self-motivated/nobody in particular=1
Relatives/ Neighbours/Friends/Interpersonal communication = 2
Group meeting organized by Panchayat/Gram Sabha/Govt Departments=3
Local folk-art/IEC team members=4
Announcement at religious places (Mosque/Temple etc.)=5
Self Help Groups (SHGs)=6
Chit distributions=7
ANM/ASHA/AWW durng Home visits=8
Local school teacher=9
Employer=10
Govt. workers=11
MLAs/other political workers=12
RSBY-PACS Community mobilizer=13

Imact Assessement Study on RSBY
Page | 164
Others (specify)=98
9C-3 How far was the enrolment centre from your house? (in kms)
Were you provided/did you have the following information before you went for enrolment?
(Yes=1, No-2, DK/CS/Not sure=99)
9C-5 Venue/timings for enrolment/photography & biometrics 1 2 99
9C-6 Carry BPL Card/ Carry MNEREGA ID Proof 1 2 99
9C-7 Registration fee (Rs. 30) 1 2 99
9C-8 All five members present during enrolement 1 2 99
9C-9
From where did you get these informations on RSBY enrolment venue and other
details?
Codes:
Self =1
Relatives/ Neighbours/Friends/Interpersonal communication = 2
Group meeting organized by Panchayat/Gram Sabha/Govt Departments=3
Local folk-art/IEC team members=4
Announcement at religious places (Mosque/Temple etc.)=5
Self Help Groups (SHGs)=6
Chit distributions=7
ANM/ASHA/AWW durng Home visits=8
Local school teacher=9
Employer=10
Govt. workers=11
MLAs/other political workers=12
RSBY-PACS Community mobilizer=13
Others (specify)=98
9C-10
What documents did you produce for the enrolment?
BPL Card=1
MNEREGA ID Proof=2
Others (Specify)=98
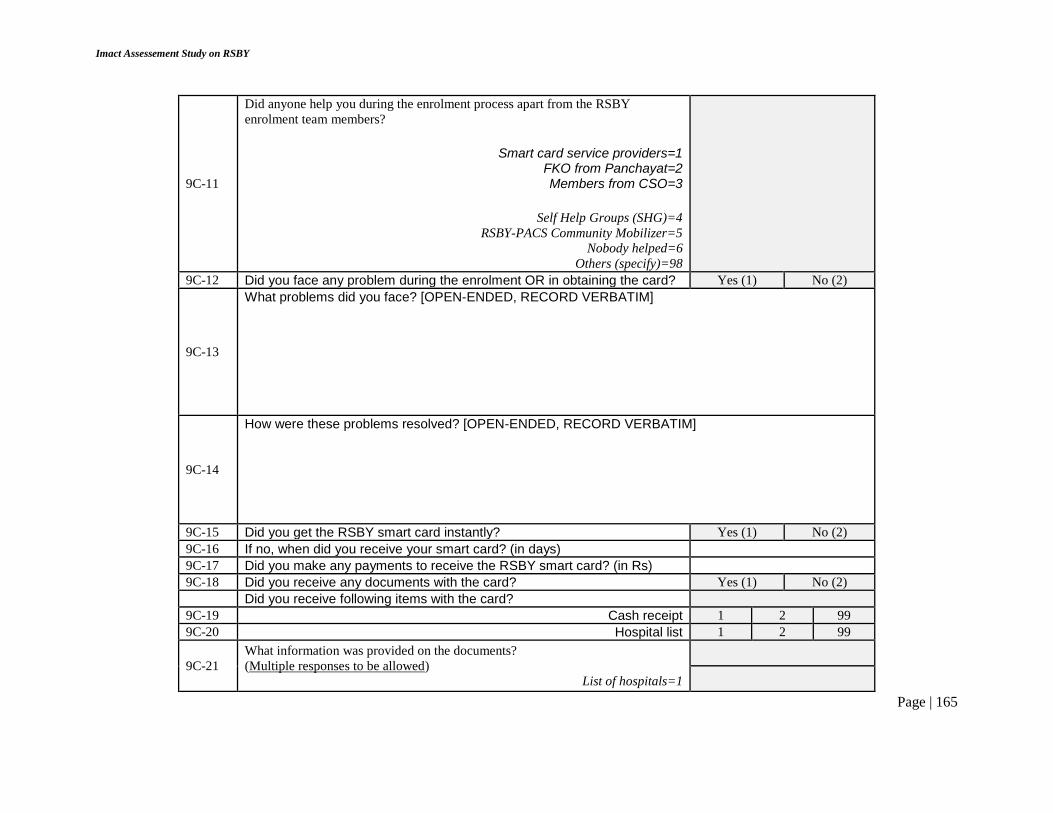
Imact Assessement Study on RSBY
Page | 165
9C-11
Did anyone help you during the enrolment process apart from the RSBY
enrolment team members?
Smart card service providers=1 FKO from Panchayat=2 Members from CSO=3
Self Help Groups (SHG)=4
RSBY-PACS Community Mobilizer=5
Nobody helped=6
Others (specify)=98
9C-12 Did you face any problem during the enrolment OR in obtaining the card? Yes (1) No (2)
9C-13
What problems did you face? [OPEN-ENDED, RECORD VERBATIM]
9C-14
How were these problems resolved? [OPEN-ENDED, RECORD VERBATIM]
9C-15 Did you get the RSBY smart card instantly? Yes (1) No (2)
9C-16 If no, when did you receive your smart card? (in days)
9C-17 Did you make any payments to receive the RSBY smart card? (in Rs)
9C-18 Did you receive any documents with the card? Yes (1) No (2)
Did you receive following items with the card?
9C-19 Cash receipt 1 2 99
9C-20 Hospital list 1 2 99
9C-21
What information was provided on the documents?
(Multiple responses to be allowed)
List of hospitals=1

Imact Assessement Study on RSBY
Page | 166
How to use the card=2
Whom to contact in case of any query=3
Information about district kiosk=4
Other (specify) =98. _____________________________________
Don’t remember=99
9C-22 Did you receive any information on RSBY/Smart Card verbally?
Yes (1) No (2)
9C-23
Who provided you the information?
9C-24
What information was conveyed to you? (Read out options)
List of hospitals=1
How to use the card=2
Who to contact in case of any query=3
Information about district kiosk=4
No information was conveyed=5
Other (Specify)=98
Don’t remember=99
9C-25
Did you ask any for any doubts/clarifications related to RSBY scheme during enrolment?
Yes
(1)
No
(2)
9C-26
Did anyone respond to your doubts/clarifications?
Yes
(1)
No
(2)
9C-27
Who was the person/organization that responded to your doubts/clarifications?
9C-28
Did anyone visit your home after acquiring RSBY smart card for detail description related to its usage and others?
Smart card service providers=1 FKO from Panchayat=2 Members from CSO=3

Imact Assessement Study on RSBY
Page | 167
Self Help Groups (SHG)=4
RSBY-PACS Community Mobilizer=5
Nobody helped=6
Others (specify)=98
9C-29
Were you told about the date when you could start using the smart card?
Yes
(1)
No
(2)
9C-30
How long did it take you to complete the whole enrolment process?
Less than one hour =1
One or more than one hour=2
If more than one hour, please specify=3
9C-31
What was your experience of the enrolment process (How satisfactory….)?
Complicated/difficult/long-waiting/v. unsatisfactory=1
Somewhat unsatisfactory=2
OK/satisfactory/no problem=3
Others (specify)=98
DK/CS=99
9C-32
Are you aware of the three nearest RSBY empanelled hospital nearby your
locality?
Yes
(1)
No
(2)
9C-33
If yes, please name the hospitals?
1.
2.
3.
9C-34
Have you ever be a part of any hospital exposure visits conducted
by any organisation?
Yes (1) No (2) If ‘No (2)’
SKIP TO
Section D

Imact Assessement Study on RSBY
Page | 168
9C-35
Who approached you prior to hospital exposure visits?
Smart card service providers=1 FKO from Panchayat=2 Members from CSO=3
Self Help Groups (SHG)=4
RSBY-PACS Community Mobilizer=5
Nobody helped=6
Others (specify)=98
9C-36 Did anyone tell you about the purpose of hospital exposure visits?
Yes (1) No (2)
9C-37
How many people from you community were accompanying you during hospital
exposure visit?
9C-38 Which hospital did you visit?
9C-39 How much time did you spent on exposure visit? (in hrs.)
9C-40
With whom did you interact during hospital exposure visit?
Doctors=1
Nurses=2
Hospital administrative staff=3
RSBY help desk=4
Others (Specify)=98
9C-41
Did you visit different departments/locations inside the hospitals?
Registration desk=1
Patient waiting hall=2
Doctors room=3
X-ray room=4
Drug distribution centre=5
Toilets/Wash room=6
Put the codes for which
answers ‘Yes’
Were you informed about the following during hospital exposure visits?
9C-42 RSBY Help Desk and its role 1 2 99
9C-43 Package rates 1 2 99
9C-44 Facilities available and entitled during hospital stay 1 2 99
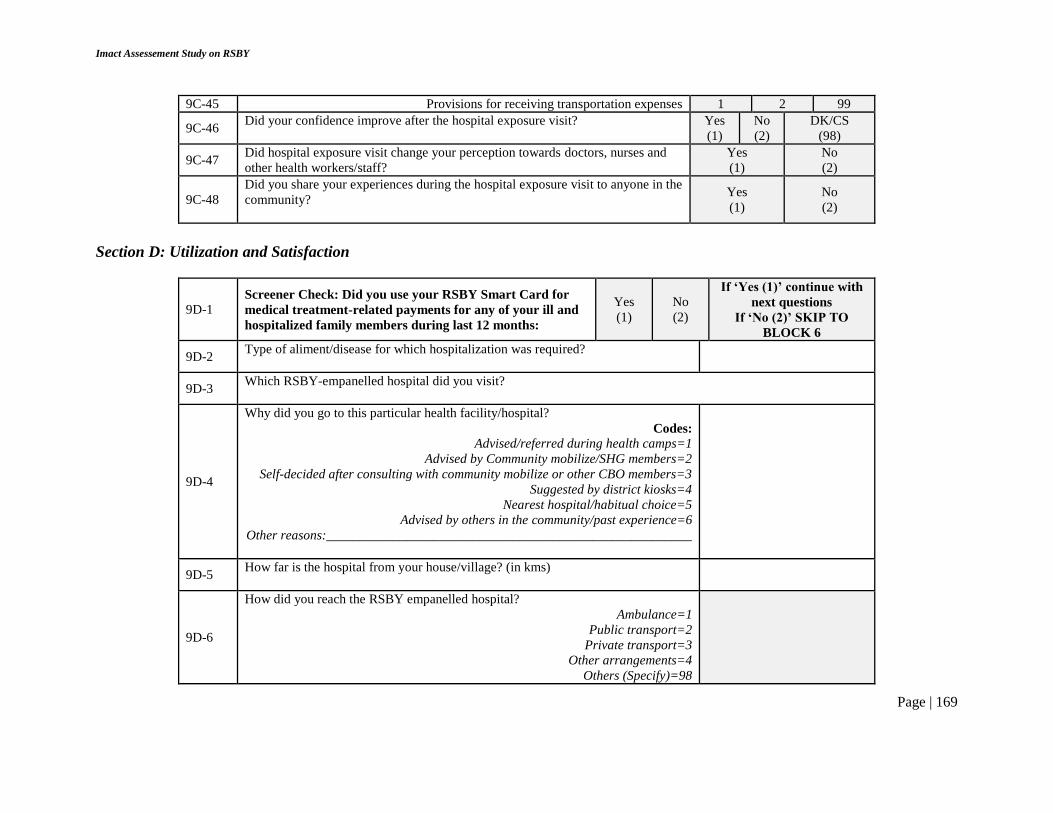
Imact Assessement Study on RSBY
Page | 169
9C-45 Provisions for receiving transportation expenses 1 2 99
9C-46 Did your confidence improve after the hospital exposure visit?
Yes
(1)
No
(2)
DK/CS
(98)
9C-47 Did hospital exposure visit change your perception towards doctors, nurses and
other health workers/staff?
Yes
(1)
No
(2)
9C-48
Did you share your experiences during the hospital exposure visit to anyone in the
community?
Yes
(1)
No
(2)
Section D: Utilization and Satisfaction
9D-1 Screener Check: Did you use your RSBY Smart Card for
medical treatment-related payments for any of your ill and
hospitalized family members during last 12 months:
Yes
(1)
No
(2)
If ‘Yes (1)’ continue with
next questions
If ‘No (2)’ SKIP TO
BLOCK 6
9D-2 Type of aliment/disease for which hospitalization was required?
9D-3 Which RSBY-empanelled hospital did you visit?
9D-4
Why did you go to this particular health facility/hospital?
Codes:
Advised/referred during health camps=1
Advised by Community mobilize/SHG members=2
Self-decided after consulting with community mobilize or other CBO members=3
Suggested by district kiosks=4
Nearest hospital/habitual choice=5
Advised by others in the community/past experience=6
Other reasons:_______________________________________________________
9D-5 How far is the hospital from your house/village? (in kms)
9D-6
How did you reach the RSBY empanelled hospital?
Ambulance=1
Public transport=2
Private transport=3
Other arrangements=4
Others (Specify)=98

Imact Assessement Study on RSBY
Page | 170
9D-7
Was there a RSBY helpdesk/counter/Enquiry at
the hospital?
Yes
(1)
No
(2)
DK/CS
(99) If ‘No (2) or ‘99’ SKIP TO
Q 9D-16
9D-8 Did you find any staff member at the RSBY help desk?
Yes
(1)
No
(2)
9D-9
At the Help-desk, did anybody help you/informed you about how to use your
RSBY card regarding the admission/treatment processes?
Yes
(1)
No
(2)
9D-10
How long did you/the patient have to wait before being attended by the Help-Desk
staff? (In hrs.)
9D-11
Was fingerprint verification done through a fingerprint scanner?
Yes
(1)
No
(2)
DK/CS
(99)
9D-12
Were you informed about the costs of treatment or given an estimate in advance/at
the time of admission?
Yes
(1)
No
(2)
9D-13
Were you informed about the amount that can be charged/paid from your RSBY
Card?
Yes
(1)
No
(2)
9D-14 How was the behavior of staff at RSBY help-desk? Codes: Polite=1, Rude=2
9D-15
Did you face any type of discrimination on RSBY help desk?
Yes
(1)
No
(2)
9D-16 What was the total expenditure (Kharcha) on the hospitalization? (in Rs.)
9D-17
What was the amount paid/cost of treatment supported by the RSBY Card? (in Rs.)
9D-18
On discharge was discharge summary provided to the family?
Yes
(1)
No
(2)
DK/CS
(99)
9D-19
Was the fingerprint verification done at the time of discharge?
Yes
(1)
No
(2)
DK/CS
(99)

Imact Assessement Study on RSBY
Page | 171
9D-20
When did you get the RSBY/Smart card back? Codes:
After swiping at the time of admission=1, On discharge=2 , Next day=3, Two days
later=4, Others (specify)=98
9D-21
Were you told about the amount of money left in the card at the time of discharge?
Yes
(1)
No
(2)
DK/CS
(99)
9D-22
How would you rate the behaviour and overall help/support of the staff dealing
with your admission/use of your RSBY Card
(Please provide your response in a scale of 1-5 where 1=most dissatisfied/very
poor and 5=Very satisfied/excellent)
1 2 3 4 5
9D-23 Were you told the amount of money available in your Card at the time of
discharge?
Yes
(1)
No
(2)
DK/CS
(99)
9D-24
Was any other post-hospitalization expenses covered under RSBY?
No=0
Some medicines provided from hospital=1
Free ambulance/transport to return home=2
Free tests/scan etc on follow-up visits=3
Dressing of wounds etc.=4
Others (specify)=98
9D-25
How would you rate your overall experience in using the RSBY Card at the
hospital?
(Please provide your response in a scale of 1-5 where 1=most dissatisfied/very
poor and 5=Very satisfied/excellent)
1 2 3 4 5
Did you have any complaint/problems regarding the hospitalization and use of RSBY Card?
Instruction: Read out the options
9D-26 Proper use of RSBY card Yes (1) No (2)
9D-27 Lack of adequate cost of treatment/amount covered under RSBY Yes (1) No (2)
9D-28 For that you were by cheated/mislead in somewhat or the other Yes (1) No (2)
SKIP TO Q 287 IF all answers are ‘No (2)’
9D-29 Did you lodge any complaint regarding your grievances?
Yes
(1)
No
(2)
DK/CS
(99)

Imact Assessement Study on RSBY
Page | 172
9D-30
If yes, place of lodging grievances?
Hospital authorities=1
CSO representatives=2
District kiosks=3
Others (specify)=98
9D-31 Are you aware about any measures/action taken on the basis of your grievances?
Yes
(1)
No
(2)
DK/CS
(99)
9D-32
Is there any post hospitalization expenses covered under RSBY?
9D-33
Was the patient prescribed any medicines after the discharge?
Yes
(1)
No
(2)
DK/CS
(99)
9D-34
Were these medicines provided by the hospital?
Yes
(1)
No
(2)
DK/CS
(99)
9D-35 Was the patient prescribed any tests after discharge?
Yes
(1)
No
(2)
DK/CS
(99)
9D-36
Were facilities for those tests organized by hospital free of cost?
Yes
(1)
No
(2)
DK/CS
(99)
9D-37
How significant would you consider the financial support you have received under
RSBY, by being a card-holder?
Codes:
Insignificant/little help/support=1
Somewhat useful/helpful=2
Very useful/helpful=3
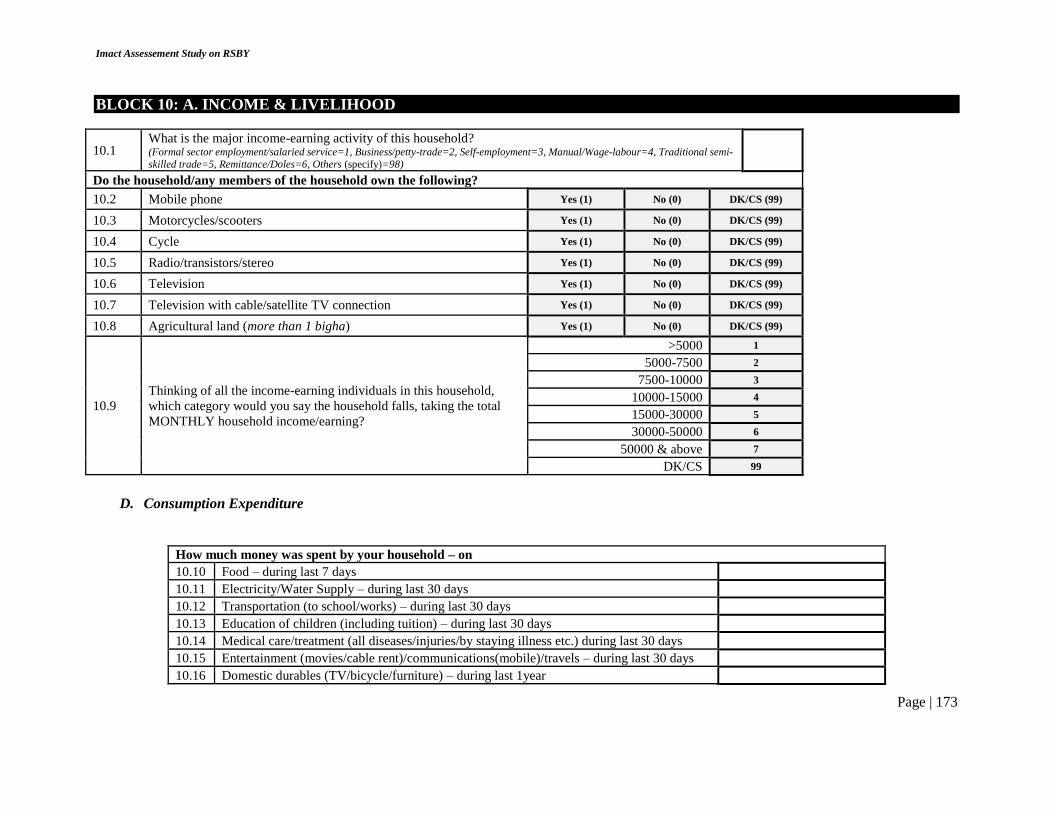
Imact Assessement Study on RSBY
Page | 173
BLOCK 10: A. INCOME & LIVELIHOOD
10.1 What is the major income-earning activity of this household? (Formal sector employment/salaried service=1, Business/petty-trade=2, Self-employment=3, Manual/Wage-labour=4, Traditional semi-
skilled trade=5, Remittance/Doles=6, Others (specify)=98)
Do the household/any members of the household own the following?
10.2 Mobile phone Yes (1) No (0) DK/CS (99)
10.3 Motorcycles/scooters Yes (1) No (0) DK/CS (99)
10.4 Cycle Yes (1) No (0) DK/CS (99)
10.5 Radio/transistors/stereo Yes (1) No (0) DK/CS (99)
10.6 Television Yes (1) No (0) DK/CS (99)
10.7 Television with cable/satellite TV connection Yes (1) No (0) DK/CS (99)
10.8 Agricultural land (more than 1 bigha) Yes (1) No (0) DK/CS (99)
10.9
Thinking of all the income-earning individuals in this household,
which category would you say the household falls, taking the total
MONTHLY household income/earning?
>5000 1
5000-7500 2
7500-10000 3
10000-15000 4
15000-30000 5
30000-50000 6
50000 & above 7
DK/CS 99
D. Consumption Expenditure
How much money was spent by your household – on
10.10 Food – during last 7 days
10.11 Electricity/Water Supply – during last 30 days
10.12 Transportation (to school/works) – during last 30 days
10.13 Education of children (including tuition) – during last 30 days
10.14 Medical care/treatment (all diseases/injuries/by staying illness etc.) during last 30 days
10.15 Entertainment (movies/cable rent)/communications(mobile)/travels – during last 30 days
10.16 Domestic durables (TV/bicycle/furniture) – during last 1year

Imact Assessement Study on RSBY
Page | 174
10.17 Home repair/constructions – during last 1year
10.18 Clothing/footwear – during last 1year
10.19 Any other expenses – during last 1year
10.20 TOTAL
E. Living Conditions
10.21 Whether household members sleep in the same room where food is cooked (Yes =1, No =2)
10.22 Type of toilet used by household members (Open defecation =1; Public toilet=2; WC – in premises=3; Flush; Other (specify) =98)
10.23 Main source of drinking water (Piped water=1; Tubewell/handpump=2; Public Tap =3; Tanker=4; Wells=5; Other(specify) =98)
10.24 Type of cooking fuel used (Kerosene =1; Coal/Cow-dung/other wastes =2; LPG=3; Electricity=4; Other (specify) =98)

Imact Assessement Study on RSBY
Page | 175
Annex 4 Qualitative Tools – FGD Guidelines and In-Depth/Key Informant Interviews Outlines
Guidelines for Focus Group Discussion (FGD)
Group Category
Adult Women Group Tribal Male Group Minority Male Group
DISCUSSANT NAME
Date of FGD Signature Start time End time
Locality Details:
Village/Gram Panchayat Block District
Group Members’ Details:
Name
Sex (M/F)
Age
Completed level (class) of education
Occupation
Knows about RSBY (Y/N)

Imact Assessement Study on RSBY
Page | 176
Has RSBY Smart Card (Y/N) 1 2 3 4 5 6 7 8
Consent Statement:
Signatures of Participating Group Members:
1. 2. 3. 4.
5. 6. 7. 8.
1. What do you know about the RSBY Programme?
2. How did you get to know about the programme?
3. How can a family benefit from this programme?
4. Do you consider that RSBY can be helpful for poor families?
5. Have you noticed something different regarding your experience with the health system after RSBY has started?
6. From where did you know about the different features of the RSBY program?
7. Have you or anyone you know in your locality, ever used the RSBY Smart Card for any hospitalization needs? How was the experience?
8. For what type of diseases/illnesses were the RSBY smart Cards used? Did anybody advised you in this regard?
9. Were any problems faced? If yes, how were the problems resolved?
10. Are any SHGs/CBOs/NGOs active in your village/community? If yes, what are the different activities and interventions these organizations support?

Imact Assessement Study on RSBY
Page | 177
11. Are you aware about any activities undertaken by [PARTNER NGO NAME/NAME OF COMMUNITY MOBILIZER] regarding RSBY? If yes, can you describe the different activities which you have seen?
12. Have these activities/programs in any way helped you to know better about RSBY program? In what ways?
13. Did anybody other than [PARTNER NGO NAME/NAME OF COMMUNITY MOBILIZER] such as panchayat members, doctors, ANM/ASHA/anganwadi worker, political leaders ever told you anything about RSBY, or have helped in getting hospitalizations under RSBY? Please describe.
14. What would you expect from a scheme such as RSBY, so that it is most beneficial/useful to a family such as yours?
Thank you for your time and kind cooperation
Guidelines and Discussion Points for In-Depth/Key-Informant Interviews
CATEGORY ‘A’: RSBY FUNCTIONARIES - GOVERNMENT
Interviewer’s Name
Date of Interview Signature Start time End time
Respondent Characteristics: 1 Name 2 Sex Male Female 3 Age 4 Designation/Role 5 Full contact details (with mobile number and email) 6 Educational Qualifications 7 Professional Training (if any) 8 Years in present position
1. What are the main activities that you/your office/department are engaged in the context of promoting better awareness and utilization of RSBY?
2. Who are the other key associates/partners/stakeholders whom you involve in these activities? How do you identify your potential stakeholders?

Imact Assessement Study on RSBY
Page | 178
3. How important, in your view, is to involve communities and other non-governmental stakeholders such as CBOs/NGOs to improve the functionings and desired impacts of the RSBY programme?
4. Are you aware of any activities or interventions undertaken by PACS in the state/district on RSBY? If so, can you please briefly state them? Which of these activities/interventions you consider to be most appropriate and why? Which of the activities do you consider not effective enough and needs to be modified? Are there any specific areas or issues where you would have liked PACS to concentrate its activities and interventions, in view of any local issues or challenges that you may have faced?
5. How would you describe your interactions with the program personnel of PACS and its partnering organizations regarding different operational and functional aspects of the RSBY program? Do you think that the existing processes of the interactions needs to be revised, or modified? If so, how do you think such changes should happen?
6. Do you have any suggestions, regarding how the overall RSBY program can be strengthened or modified, when you think of the most disadvantaged or vulnerable beneficiary who is in need of the support? Please explain your reasons.
Thank you for your time and kind cooperation
Guidelines and Discussion Points for In-Depth/Key-Informant Interviews
CATEGORY ‘B’: PACS/PARTNER CBO’s FUNCTIONARIES
Interviewer’s Name
Date of Interview Signature Start time End time
Respondent Characteristics: 1 Name 2 Sex Male Female 3 Age 4 Affiliation/Organization 5 Designation/Role 6 Full contact details (with mobile number and email) 7 Educational Qualifications 8 Professional Training 9 Years in present Organization
1. What are the main activities that your organization (PACS/partner CSO, e.g. CINI, SHS) is engaged in the context of promoting better awareness and utilization of RSBY?

Imact Assessement Study on RSBY
Page | 179
2. How would you describe your role in these activities? How are you involved?
3. Who are the other key associates/partners/stakeholders whom you involve in these activities? How do you identify your potential stakeholders?
4. How would you describe your interactions with the government (including the respective nodal agency/officer, and other key government officials in the state/district) functionaries/institutions related to the operation of RSBY? Do you think that the existing processes of the interactions needs to be revised, or modified? If so, how do you think such changes should happen?
5. How would you describe your interactions with or experience about other supporting institutions/individuals related to the operation of RSBY (TPA, insurance agency, district kiosks/helplines etc.)? Do you think that the existing processes of the interactions, or the current system of operations needs to be revised, or modified? If so, how do you think such changes should happen?
6. ONLY FOR NON-PACS RESPONDENTS (CSO PARTNERS): How do you consider the help and support you have received from PACS and its representatives? Please also consider how useful were the different orientations, capacity-building events (e.g. training, workshops) that were organized, in helping you to conduct your regular activities in a better way. Do you have any suggestions how these interactions with PACS can be further strengthened?
7. Do you have practical experience of working among the communities where the PACS interventions are in place? If so, how would you describe the communities’ acceptance of or reaction to the major intervention strategies or components that were introduced?
8. What do you think were/are the most successful strategies/interventions that were introduced? Why do you think so?
9. Which strategies/interventions/program components do you think were not as successful as it was initially thought of? What were the barriers that you think were responsible for such outcomes/results?
10. Thinking of a time when the PACS programme no longer continues, do you think that the existing interventions/activities/strategies ongoing in the community are sustainable in the long-run? If yes, who or what processes or institutions do you think are critical to make the interventions self-sustaining? If not, which are the main challenges that you can think of?
11. Do you have any suggestions, regarding how the overall RSBY program can be strengthened or modified, when you think of the most disadvantaged or vulnerable beneficiary who is in need of the support? Please explain your reasons.

Imact Assessement Study on RSBY
Page | 180
Thank you for your time and kind cooperation
Guidelines and Discussion Points for In-Depth/Key-Informant Interviews
CATEGORY ‘C’: COMMUNITY-LEVEL STAKEHOLDERS
Interviewer’s Name Date of Interview Signature Start time End time
Respondent Characteristics: 1 Name 2 Sex Male Female 3 Age 4 Affiliation/Organization/GP 5 Designation/Role 6 Full contact details (with mobile number and email) 7 Educational Qualifications 8 Professional Training (if any) 9 Years in present Organization OR Years in office (for PRI members)
COMMON SECTION 15. How would you describe the progress and achievements in improving enrolment under the RSBY programme in your village/community? Do you consider that the achievements or performance in terms of enrolment, have improved recently? If yes, what do you think were the main reasons for such positive improvements? If not, what were the challenges that prevented better achievement or performances?
16. What is your opinion regarding the functioning of the RSBY programme, in general, in your village/community? Are there any major issues which you think requires to be addressed in this regard? ASK ONLY TO PRI MEMBERS
1. Are you aware of any organizations/individuals/groups working on improving the functioning and impacts of the RSBY programme in your village/community? If yes, please name them. IF PACS/PARTNER CBOs ARE NOT MENTIONED, TRY TO PROBE WITH SPECIFIC NAMES (Are you aware of any activities by [PACS/PARTNER CBOs NAME])
2. Can you please tell me something more about your opinion about the different activities undertaken by the organization(s)? How important or effective do you think are the different activities to improve performance of RSBY program, in view of the local needs and problems? Do you have any suggestions on how the activities and/or interventions being provided by the organization could be modified?
3. Did you ever participate in any programmes/events that involved elected people’s representatives or other government functionaries, where issues related to RSBY were discussed? If yes, can you please describe some of the issues that were discussed? Who provided/organized

Imact Assessement Study on RSBY
Page | 181
the programmes? How useful do you consider were the events/programmes in improving your own understanding about the RSBY programme and your roles and responsibilities in improving its performance?
ASK OTHER RESPONDENTS
1. Are you involved in any activities (awareness generation, counselling, facilitating enrolment etc) in your village/community regarding RSBY programme? If yes, what are the main activities in which you are involved in?
2. Who are the other key associates/partners/stakeholders whom you involve in these activities? Is there any way through which you prioritize your activities (for e.g. focusing more on local challenges, identifying more vulnerable families etc)? Please describe.
3. How would you describe your interactions with the local government officials and the PRI members related to the operation of RSBY? How would you describe your interactions with the [NAME OF PACS PARTNERING NGO/CBO] and its representatives?
4. ONLY FOR NON-PACS RESPONDENTS (CSO PARTNERS): How do you consider the help and support you have received from PACS and its representatives? Please also consider how useful were the different orientations, capacity-building events (e.g. training, workshops) that were organized, in helping you to conduct your regular activities in a better way. Do you have any suggestions how these interactions with PACS can be further strengthened?
5. How would you describe the communities’ acceptance of or reaction to the major intervention strategies or activities that you are involved in regarding the RSBY programme? Do you have any suggestions on how these activities could be modified according to the local needs and challenges?
6. What do you think were/are the most successful strategies/interventions that were introduced? Why do you think so? Which strategies/interventions/program components do you think were not successful? What were the barriers that you think were responsible for such outcomes/results?
Thank you for your time and kind cooperation