Embed Size (px)
Citation preview


Immunotherapie in oncologie
Lore Decoster
Medische oncologie
Oncologisch Centrum, UZ Brussel


Immuuntherapie
• Definitie:– Gebruik vh immuunsysteem vd patiënt om kanker
te behandelen
• De ‘ideale’ kankerbehandeling– Zeer uitgebreid wapenarsenaal
• T cellen, antilichamen, natural killers, etc
– Precies en doelgericht
– Recall effect: na priming levenslange immuniteit

Immuunsysteem

Immuunsysteem in evenwicht
Te weinig
(infecties, kanker)
Te veel
(autoimmuniteit,weefselschade)
Immuun activatie


Immuunsysteem vs kanker
• Spontane regressie vb in melanoom en RCC
• Immunosuppressie verhoogt kanker risico– Lymfoom x90; huidkanker x29
• Lymfocyten in bloed en in de tumor (TILs)
• Tumoren zijn immunogeen door tumor Ag– HER2, RAS, MAGE

Trafficking of T cells to tumours
CX3CL1, CXCL9, CXCL10CCL5
Killing of cancer cells
IFN- , T-cell granule content
Priming and Activation
CD28/B7.1, CD137/CD137LOX40/OX40L, CD27/CD70HVEM, GITR, IL-2, IL-12
CTLA4/B7.1PD-L1/PD-1PD-L1/B7.1 Prostaglandins
Chen DS and Mellman I. Immunity. 2013 Jul 25;39(1):1-10.
Stimulatory and inhibitory factors in the cancer
immunity cycle
Cancer antigen presentation
TNF-, IL-1IFN-, CD40L/CD40CDN, ATPHMGB1, TLR
IL-10, IL-4, IL-13
Release of cancer cell antigens
Immunogenic cell death
Tolergenic cell death
PD-L1/PD-1PD-L1/B7.1IDOTGF-BTLA
VISTALAG-3ArginaseMICA/MICBB7-H4
Recognition of cancer cells by T cells
T cell receptor
Reduced pMHC on cancer cells
Infiltration of T cells into tumours
LFA1/ICAM1Selectins
VEGFEndothelin-B receptor
4
Stimulatory factors Inhibitors
Lymphnode
Bloodvessel
Tumour
5
6
71
2
3
TIM-3/phospholipids

13
Tumor microenvironment: Immune escape mechanisms
Tumor cells
CD8* T cell Treg
MDSC
CD8* T cell
CD4+
T cell
TGF-β
IL-10
TGF-β
ARG1
iNOS
VEGFAPC
TGF-β
IDO
IL-10
PD-1
P-DL1PD-1
PD-L1
CTLA-4TCR
MHC
Vesely MD, et al, Ann Rev Immunol 2011, 29: 235
A. Ineffective tumor antigen presentation (gp100, MART-1, decreased MHC expression)
B. Recruitment of immunosuppressing cells (regulatory T cells =Tregs, MDSCs, other)
C. Secretion of immunosuppressive signals (e.g. PD-L1, TGF-β, IL-10, and indolamine 2,3-dioxygenase [IDO])
D. T cell checkpoints

Immuuntherapie
• Immuun stimulerende cytokines
• Monoclonale antilichamen
• Kanker vaccins
• Checkpoint inhibitoren
– Anti-cTLA4
– Anti PD1
– Anti PDL1

Immuun checkpoints
• T cel respons geregeld door een evenwicht tussen co-stimulatie en inhibitie signalen (imuun checkpoints)
• ‘normale omstandigheden’:
– Bescherming normaal weefsel tegen schade tijdens immuunrespons op infecties
– Preventie autoimmuniteit

Ways to keeping the T cells “active”
Presented By Michael Postow at 2015 ASCO Annual Meeting
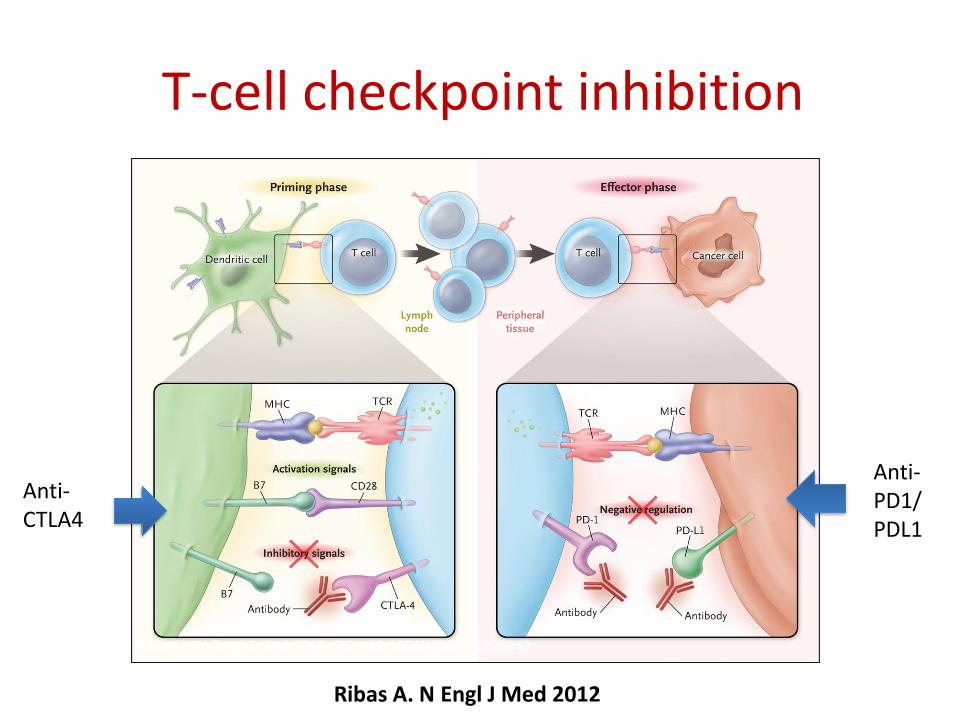
Ribas A. N Engl J Med 2012. DOI: 10.1056/NEJMe1205943
Ribas A. N Engl J Med 2012
T-cell checkpoint inhibition
Anti-CTLA4
Anti-PD1/PDL1
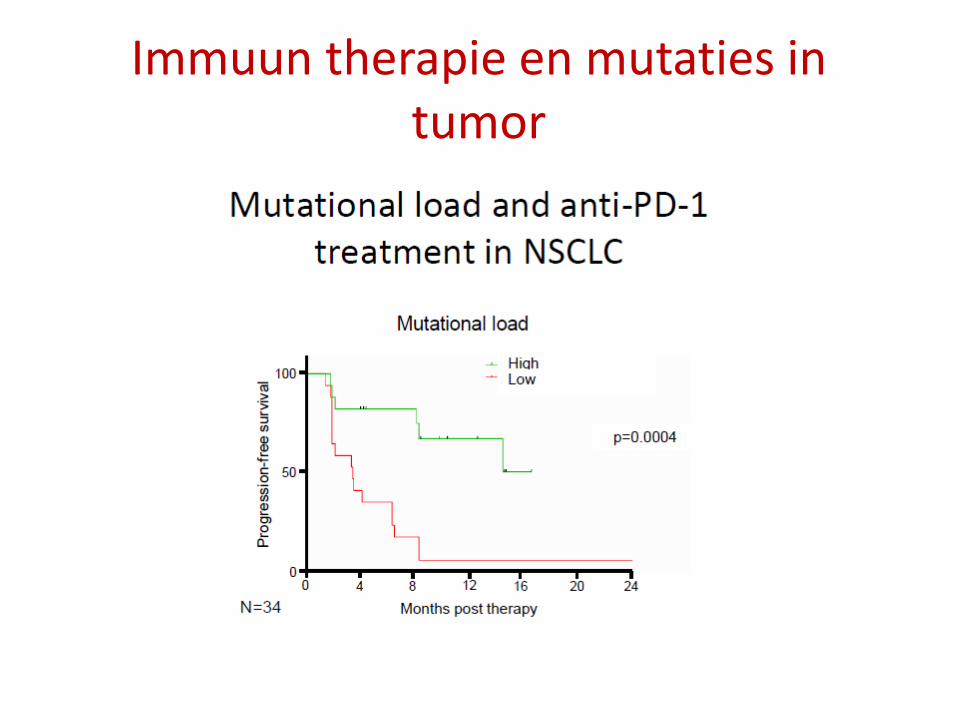
Immuun therapie en mutaties in tumor

LB Alexandrov et al. Nature 000, 1-7 (2013) doi:10.1038/nature12477
The prevalence of somatic mutations across human cancer types.

Ribas A. N Engl J Med 2012. DOI: 10.1056/NEJMe1205943
Ribas A. N Engl J Med 2012
T-cell checkpoint inhibition
Anti-CTLA4
Anti-PD1/PDL1

Anti-cTLA4

Anti-cTLA4
• Ipilimumab (Yervoy)
– Geregistreerd en terugbetaald in melanoma
• Tremelimumab
– In studie in verschillende tumoren

Hodi et al. N Eng J Med 2010
Robert et al N Eng J Med 2011

Ipilimumab in melanoom

Ipilimumab in melanoom
• 2e lijn na chemo:
– DCR 20-28% vs 11%
– Mediane OS 10 vs 6,4 m
– 1 jaar S: 25% vs 15%
– 2jaar S: 22% vs 14%
Hodi et al. N Eng J Med 2010
Na 3j 20% in leven!

Kaplan–Meier Curves for Overall Survival, Progression-free Survival, and Duration of Response.
Robert C et al. N Engl J Med 2011;364:2517-2526.
• 1e lijn vs chemo:
– Mediane OS 11 vs 9 m
– 1j OS 47 vs 36%
– 3j OS 21 vs 12%

Ribas A. N Engl J Med 2012. DOI: 10.1056/NEJMe1205943
Ribas A. N Engl J Med 2012
T-cell checkpoint inhibition
Anti-CTLA4
Anti-PD1/PDL1

Anti-PD1

Anti-PD1
• Nivolumab (Opdivo)– Geregistreerd en terugbetaald in melanoom
– Geregistreerd en terugbetaald tweede lijn in NSCLC
– Geregistreerd en terugbetaald in niercelcarcinoom
– Geregistreerd en terugbetaald in Hodgkin lymfoom
• Pembrolizumab (Keytruda)– Geregistreerd en terugbetaald in melanoom
– Geregistreerd in PDL1 positief NSCLC (1e en 2e lijn)
– Evidentie in Merkelcelcarcinoom, Head and neck,…

Anti-PDL1
• Atezolizumab– FDA blaasCA
– FDA NSCLC
• Durvalumab– FDA PDL1+ blaasCA
• Avelumab– FDA Merkel cel CA

Anti-PD1 in melanoom
• Pembrolizumab fase 1 na ipilimumab
Robert Lancet 2014

Robert C et al. N Engl J Med 2015;372:320-330.
• Nivolumab 1e lijn bij BRAF wild typeSurvival End Points.

Robert N Eng J Med 2015
Anti-PD1 vs anti-cTLA4

Anti-PD1 in long

2e lijn NSCLC:4 fase 3 studies in 2e lijn
Key patient inclusion criteria• Previously treated
with a first line platinum-based regimen
Differences between studies: • PD-L1 status• PD-L1 cut off
R
Docetaxel
PD-(L)1 inhibitor
PD or toxicity
PD or toxicity
Primary endpoint: OSSecondary endpoint: PFS, RR, QOL
Geen vergelijking met:- Docetaxel + nintedanib in adenoca- Docetaxel + ramucirumab

Checkmate 017: Nivo in sqNSCLCBrahmer et al N Eng J Med 2015
Checkmate 057: Nivo in nonsqNSCLCBorghaei H et al N Eng J Med 2015
Keynote 010: Pembro in NSCLC (PDL1≥ 1%)Herbst RS et al Lancet 2016;387:1540-50
OAK: atezolizumab in NSCLC


Impact op QoL Checkmate 017

Tumor PD-L1 expressie?
Prevalentie 40% 35% 25% RR 10.7% 16.5% 45.2%
Garon et al.
N Eng J Med 2015

PD-L1 expressie: beperkingen
Verschillende technieken: Ab als IHC platformVerschillende cut offPD-L1 expressie is heterogeenPD-L1 expressie is dynamisch
CONCLUSIE: PDL1 IH lijkt een ‘enrichment biomarker’

Pembrolizumab 1e lijn vs chemotherapie in PDL1>50% NSCLC

CHECKMATE 026:Nivolumab PDL1≥5% NSCLC
Nivolumab
n = 211
Chemotherapy
n = 212
Median PFS, months
(95% CI)
4.2
(3.0, 5.6)
5.9
(5.4, 6.9)
1-year PFS rate, % 23.6 23.2
HR = 1.15 (95% CI: 0.91, 1.45), P = 0.2511
Months
OS
(%)
2421181512963 30
100
80
60
40
0
20
0 27
Nivolumab
Chemotherapy
Nivolumab
n = 211
Chemotherapy
n = 212
Median OS,
months
(95% CI)
14.4
(11.7, 17.4)
13.2
(10.7, 17.1)
1-year OS rate, % 56.3 53.6
HR = 1.02 (95% CI: 0.80, 1.30)
No benefit for subgroup PDL1≥50%
Socinski et al ESMO 2016

AntiPD1 (Nivolumab) in niercelcarcinoom
Motzer RJ et al. N Eng J Med 2015;373
Response rate:25 vs 5%
Median OS:25 vs 19,6 maand

Anti (PD1) Nivolumab in Hodgkin lymfoom
Ansell SM et al. N Engl J Med 2015;372:311-319
Response 87%

Pembrolizumab in Merkel cel carcinoom
Nghiem PT et al. N Engl J Med 2016;374:2542-2552.
Phase 2, treatment naiveResponse 56%6 maand PFS 67%

Avelumab in Merkel cel carcinoom
Kaufman HL et al. Lancet Oncol 2016;17:1374-1385
Phase 2 previously treated
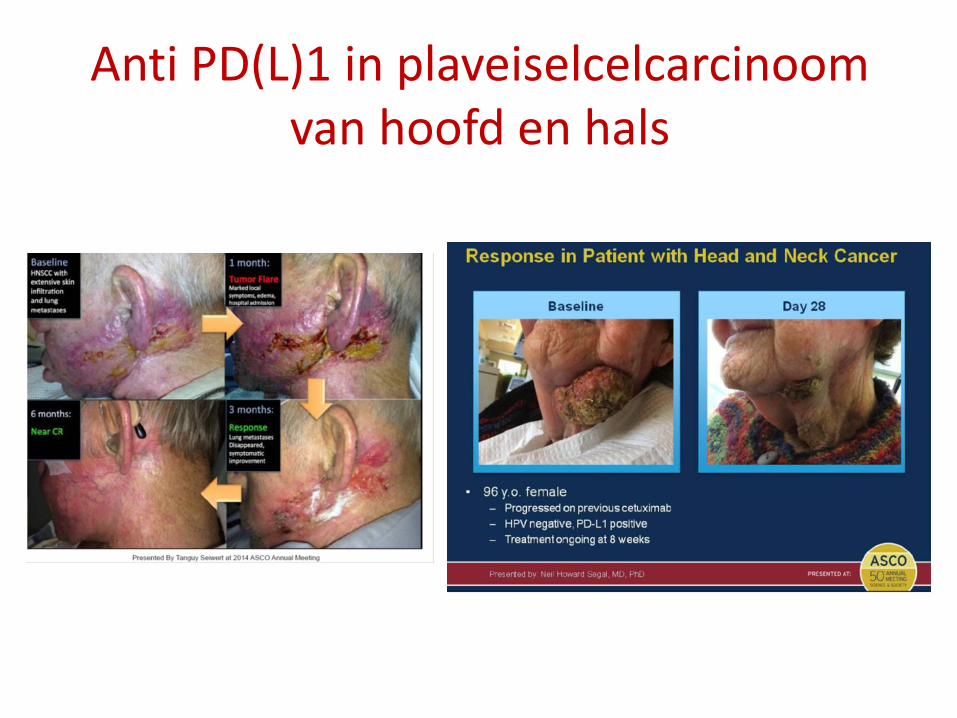
Anti PD(L)1 in plaveiselcelcarcinoom van hoofd en hals

Nivolumab in SCHNC
Ferris et al. N Eng J Med 2016

Atezolizumab in transitioneel cel carcinoom
Rosenberg et al. Lancet 2016;387:1909-20

Combinatie anti-cTLA4 en anti-PD1

Slide 9
Presented By Michael Postow at 2015 ASCO Annual Meeting

Immune related toxiciteit

Toxiciteit
Frequency of irAE
Ipilimumab Pembrolizumab Nivolumab
Diarrhoea 37 (6.9) 18 (2) 13 (1)
Colitis 8 (4.9) 1 (0.2) 2 (1)
Rash 33.2 (2.5) <1 15 (0)
Hepatotoxicity 0.7 (0.7) 0.5 (0.2) 1 (<1)
Hypophysitis 2.7 (2.1) 0.5 (0.2) <1 (<1)
Pneumonitis <2 2.9 (0.2) 3 (1)
Thyroid dysfunctionHypo 1.8 (0.1)
Hyper 1.2 (0.2)
Hypo 8.3 (0.2)
Hyper 1 (<1)
Hypo 4 (<1)
Nephritis <2 0.7 (0.5) 1 (0)
Neuropathies <1 <1 <1
All % (G3/4 %)
Ibrahim JCO 2011Pembrolizumab PI, 2014Nivolumab, safety management BMS, 2014
Data obtained from different studies and not directly comparable

J.M. Michot, et al
European Journal of Cancer, Volume 54, 2016, 139–148

Toxiciteit

Diarrhea and Colitis
Presented By Michael Postow at 2015 ASCO Annual Meeting


Ipilimumab Rashes
Presented By Michael Postow at 2015 ASCO Annual Meeting

PD-1 Rashes
Presented By Michael Postow at 2015 ASCO Annual Meeting



Hypophysitis Endocrinopathy
Presented By Michael Postow at 2015 ASCO Annual Meeting



Pneumonitis
Presented By Michael Postow at 2015 ASCO Annual Meeting


• Uveitis and episcleritis
– Evaluatie door oogarts
– Oogdruppels met corticoïden
Tarhini et al

Toxiciteit
• Efficiënte behandeling van bijwerkingen igv:
– Informeren van de patiënt
– Monitoring
– Vroegtijdig herkennen
– Tijdig opstarten immuunsuppressieve behandeling
– Behandelingsalgoritmen

Future prospects
80
Adapted from Ribas A, presented at WCM, 2013; Ribas et al, Clin Cancer Res. 2012; 18: 336; Drake CG, Ann
Oncol. 2012; 23(suppl 8): viii41.
Where are we now? Where do we want to go?
Surv
ival
Time
Control
Targeted therapies
Immune checkpoint blockade
Combinations
?
Surv
ival
Time





























