Embed Size (px)
Citation preview

J Clin Pathol 1984;37:1114-1118
Immunohistochemical demonstration of leucocyteelastase in human tissuesJ CROCKER,* RACHEL JENKINS,* D BURNETTt
From the *Histopathology Department, East Birmingham Hospital, Bordesley Green East, BirminghamB9 SST, and the tUniversity Department ofImmunology and the General Hospital, Birmingham
SUMMARY A polyclonal antiserum, produced in sheep and reactive against purified human leuco-cyte elastase, has been applied to paraffin sections from a range of human tissues by means of theindirect immunoperoxidase method. Striking and consistent results have been obtained. Normalor inflammatory granulocytes were intensely positive, the reaction being "blocked" by pureelastase. Activity was not seen in other sites, including histiocytic reticulum and lymphoid cells,although some weaker reaction was present in gastric and ileal lining epithelium. Strong reactivitywas also seen in the cells of acute and chronic myeloid leukaemia and in extramedullaryhaemopoiesis. The advantages of this technique are compared with those for muramidase(lysozyme), a,-antitrypsin, and naphthol-AS-D-chloroacetate esterase.
Mature myeloid cells are generally readily identifiedin conventional paraffin sections of human tissues.More primitive varieties, however, may be less read-ily recognised and their distinction from, for exam-ple, primitive lymphoid or monocytic cells may bedifficult.The naphthol-AS- D-chloroacetate esterase
(NCAE) azocoupling technique shows fully ornearly mature granulocytes in sections of paraffinembedded material,' but the reaction is not alwaysreliable and is highly dependent on fixation. Theimmunohistochemical techniques for muramidase(lysozyme)23 and a,-antitrypsin4 are unsatisfactoryas a means of demonstrating granulocytes, since his-tiocytic cells also contain these molecules.
Accordingly, in a series of human tissues we haveinvestigated the value of immunohistochemicallocalisation of the enzyme leucocyte elastase (EC3.4.21.11), which is a serine protease. This has beenextracted from malignant granulocytes. Severalspecimens of acute and chronic myeloid leukaemiahave been included to test the usefulness of elastasestaining as a means of showing these neoplasms.
Material and methods
PREPARATION OF ANTISERUMPurified leucocyte elastase was supplied by Dr AJBarrett, Strangeways Laboratories, Cambridge. Theenzyme was isolated from cells obtained by
Accepted for publication 4 July 1984
leucophoresis of patients with chronic myeloidleukaemia.5 The purified enzyme was injectedintramuscularly into a sheep as a suspension inFreund's complete adjuvant. Three injections weregiven at intervals until a desired titre of antibodies toelastase was detected in the sheep serum. A desiredtitre was that resulting in a strong precipitation lineon immunoelectrophoresis. The sheep was bled andthe immunoglobulin fraction of the serum was iso-lated by ion exchange chromatography on DE 52cellulose (Whatman Ltd); the whole sheep serumwas applied to the column, which was eluted with0-03 M phosphate buffer, pH 7-2. The non-adherent, IgG rich fraction was collected and thespecificity of the antiserum was verified byimmunoelectrophoresis.
TISSUES EXAMINEDThirty five specimens of normal human tissues,obtained as surgical or fresh postmortem excisions,.were studied (Table 1). These comprised: brain (2),skin (3), myocardium (1), oesophagus (1), stomach(2), ileum (2), colon (2), liver (2), spleen (2),skeletal muscle (2), bone marrow trephine (3),palatine tonsil (2), thyroid (2), adrenal (1), kidney(4), pancreas (1), and lung (3). In addition, 15specimens showing inflammatory or other non-malignant changes were studied. These were: acuteappendicitis (2), ulcerative colitis (2), pilonidal sinus(1), pulmonary tuberculosis (2), and inflammatorynasal polyps (2), together with three lymph -nodesshowing reactive hyperplasia and one exhibiting
1114
copyright. on A
pril 19, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.37.10.1114 on 1 O
ctober 1984. Dow
nloaded from

Immunohistochemical demonstration of leucocyte elastase in human tissues
Table 1 Elastase activity in human dssues
Tissue Elastase activity
Brain (matrix and cells)Skin (dermis and epidermis)MyocardiumOesophagus (wall and epithelium)Liver (all constituent cells)Skeletal musclePalatine tonsil,.(all cells)ThyroidAdrenalKidney (all cells)PancreasLungStomach (epithelial cells) +Ileum (epithelial cells) +Colon (epithelial cells)Bone marrow
Granulocyte series cells + + +Other cells
Bone (cells and matrix)Acute appendicitis (granulocytes) + + +Ulcerative colitis (granulocytes) + + +Pilonidal sinus (granulocytes) + + +Tuberculosis (histiocytes; giant cells)Nasal polyps (eosinophil polymorphs) +"Reactive' lymph nodes (lymphoid cells,
histiocytes, sinus lining cells)Extramedullary haemopoiesis
Granulocyte series +++Other cells
+ = positive; +++ = intensely positive; - - negative.
caseous tuberculosis. The final two specimens in thisgroup were lymph node and a liver affected byextramedullary'haemopoiesis (Table 1).A second group, consisting of 15 specimens
infiltrated by diagnostically established leukaemias,was studied. This comprised spleen, liver, or bonemarrow. specimens containing, acute lymphoblasticleukaemia (2), chronic lymphocytic leukaemia,acute myeloid leukaemia (3), and chronic myeloidleukaemia (6) (Table 2).Thus 65 specimens from the same number of
patients were submitted to staining for leucocyteelastase.
FIXATION AND STAININGAll specimens, other than bone marrow trephines,were fixed in 10% formol-saline. The trephinespecimens were fixed in 5% acetic acid in 10%formol-saline.6 After fixation, all tissues were proces-
Table 2 Elastase activity in leukaemic specimens
Type of leukaemia Elastase acnvity ofmalignantcells
Acute lymphoblasticChronic lymphocyticAcute myeloid +++Chronic myeloid + + +
+ + + = intensely positive; - = negative.
sed to paraffin wax, sectioned at 3 ,m, and thenstained for elastase activity, having been taken toTris buffer at pH 7-8. Endogenous peroxidase activ-ity was blocked by 0a1% hydrochloric acid inmethanol for 30 min. The indirect peroxidase label-led second antibody routine was utilised. Sheepantihuman elastase was applied, at a titre of 1/100,for 45 min. After a thorough wash in Tris buffer, pH7-8, peroxidase conjugated rabbit antisheepimmunoglobulins were applied, at a concentrationof 1/50. After a further wash in Tris buffer, pH 7*8,the peroxidase was shown in the usual way, bymeans of the 3, 3'-diaminobenzidine reaction. Sec-tions were counterstained in Mayers haemalum,dehydrated, cleared, and mounted in syntheticmedium.The usual controls were performed: the optimum
titre was sought in the first stage, the first antiserumwas replaced by normal sheep serum and both ofthe two stages, respectively, were omitted. The reac-tion was completely "blocked" by pure antigen at aconcentration of 2 mg/ml and the 3, 3' diaminoben-zidine reaction applied direct to the sections wasnegative. (Trypsinisation, before immunostaining,was unnecessary, resulting in no improvement instaining response.)
Results
The results of immunostaining for elastase are sum-marised in Tables 1 and 2. Certain generalisationsmay be made.
NORMAL TISSUESIn all but a limited number of tissues, positivity wasseen only in polymorphonuclear leucocytes. In thesecells, staining was uniformly intense and highlygranular. The only other site in which activity wasdetected was in the basal part of the lining cells ofthe stomach and ileum, where weaker but finelygranular staining was seen (Fig. 1). No otherepithelia were positive. Connective tissue elements,including smooth and striated muscle, fibroblasts,cartilage (cells and matrix), and bone (cells and mat-rix) were uniformly negative, as were histiocytes andendothelial cells. In lymphoid tissues (for example,tonsils and gut associated lymphoid tissue), histio-cytic reticulum cells, fibroblasts, and all lymphoidcells themselves were negative. Squamous andglandular epithelia (apart from the gastric and ileallinings) were uniformly negative. In bone marrow,only granulocyte series cells were positive (Fig. 2).
TISSUES AFFECTED BY BENIGN CONDITIONSThe specimens selected showed uniformly intensegranular staining of polymorphonuclear neutrophils
1115
copyright. on A
pril 19, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.37.10.1114 on 1 O
ctober 1984. Dow
nloaded from

Crocker, Jenkins, Burnett
I _R .
:
I~~~~~~~~~~~~~~~~~~~~~
It _v
*ffi: E~~~~~~~~~~~~~~~~~~~~~~~~~~~~~& t~~~~~:.,.c~~~~~~~~~~~~1;,N
.-
4r k-
*C
ew i
r
p
*
'I
i4 N s
,.
:. .:4."IlkS
.:.Pt-4
itC
4.
4
i*S }
5~~~~~~~
&~~~~'*:9 w *
a&>t r. a;
Fig. 2 Bone marrow. Numerous positve cells, which wereofgranulocytic series. Peroxidase-antiperoxidase techniquefor elastase; haemalum counterstain x 310.
, a
X'-A
.
I
Fig. 1 Ileal lining epithelium. Fine, moderate staining forelastase activity is seen in a supranuclear position in theepithelial cells. Peroxidase-antiperoxidase technique forelastase; haemalum counterstain x 270.
and, less strongly, eosinophils (Fig. 3) in acuteinflammatory areas. In granulomatous lesions,histiocytes, epithelioid cells, and multinucleategiant cells were negative. In extramedullaryhaemopoiesis, the granulocytic component stainedintensely (Fig. 4); the other cellular moieties werenegative. Reactive lymph nodes possessed no elas-tase activity in lymphoid cells, histiocytic reticulumcells, or sinuses (Fig. 5); some positive structures,probably corresponding to mast cells, were seenwithin and beneath the marginal sinus.
LEUKAEMIC SPECIMENSIn all specimens of myeloid leukaemia, whetheracute or chronic, there was intense granular stainingof the majority of malignant cells for elastase. Thiswas seen in liver, spleen, and bone marrow (Figs. 6and 7) and in a case of "chloroma." In contrast, thespecimens of acute lymphoblastic and chronic lym-phocytic leukaemia were uniformly negative.
.4* ,.§§
;4lbM..
,.I .t_ 9*j.,
% ig
...
j .
Fig. 3 Acute appendicitis. A heavy neutrophilpolymorphonuclear leucocyte infitrate is present in themucosa, submucosa, and wall; the constituent cells areintensely positive with the elastase technique. Two lymphoidfollicles are negative. Peroxidase-antiperoxidase techniquefor elastase; haemalum counterstain x 120.
1116
i`4
copyright. on A
pril 19, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.37.10.1114 on 1 O
ctober 1984. Dow
nloaded from
1117Immunohistochemical demonstration of leucocyte elastase in human tissues
aNt.-W,
;^;C ),.44AN u -
N; *'W" 't9 , .9 * I
lw~
a node. - -iFig. 4 Lymph node. The interfollicular area is infitratedby extramedullary haemopoietic tissue. The granulocyteseries component cells are intensely positive for elastase.Peroxidase-antiperoxidase technique for elastase;haemalum counterstain x 140.
CONTROLSAll negative controls gave appropriately negativestaining results. Elastase staining was totally"blocked" by preadsorption of the antiserum withpurified elastase.
Discussion
A not infrequent problem in diagnostic histopathol-ogy is that of recognising myeloid series cells or ofdistinguishing them from lymphoid cells. This can be
' 4 e* ',4. r*
444.. ~ ~ ~ 4,..,~+, %>s|l 4
*v; '% 4..# + et^
(.. A,; -' a
. - 4-* 9:'s ..4 X ,4.,-- ''.9 4i
Fig. 5 Follicle from "reactive" lymph node. Elastaseactvity is absent from lymphoid and histocytic cells.Peroxidase-antiperoxidase technique for elastase;haemalum counterstain X 520.
*
A4v'.4fi
'S.
''4a
v' TiJF4
;..t * vf
it'. 4',, 4 v1#6
9'.0,
w
4% <I
I.,. '*'.og
.* it,;, 4
A*9v
^, b' ] #a ''
4sf.
St ,* i' ' 8
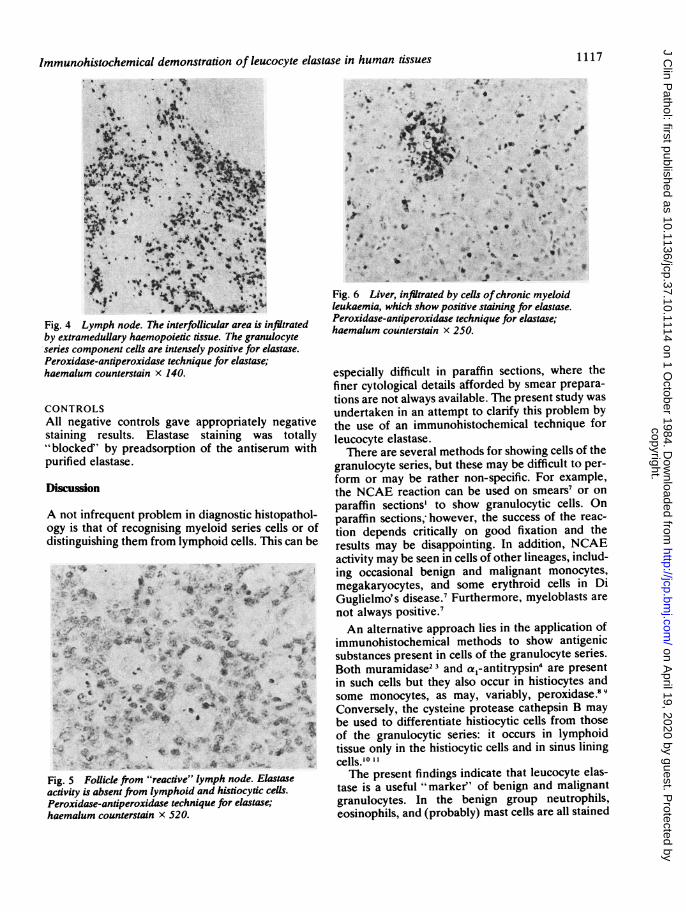
Fig. 6 Liver, infitrated by cells ofchronic myeloidleukaemia, which show positive staining for elastase.Peroxidase-antiperoxidase technique for elastase;haemalum counterstain x 250.
especially difficult in paraffin sections, where thefiner cytological details afforded by smear prepara-tions are not always available. The present study wasundertaken in an attempt to clarify this problem bythe use of an immunohistochemical technique forleucocyte elastase.There are several methods for showing cells of the
granulocyte series, but these may be difficult to per-form or may be rather non-specific. For example,the NCAE reaction can be used on smears7 or onparaffin sections' to show granulocytic cells. Onparaffin sections,- however, the success of the reac-tion depends critically on good fixation and theresults may be disappointing. In addition, NCAEactivity may be seen in cells of other lineages, includ-ing occasional benign and malignant monocytes,megakaryocytes, and some erythroid cells in DiGuglielmo' s disease.7 Furthermore, myeloblasts are
not always positive.'An alternative approach lies in the application of
immunohistochemical methods to show antigenicsubstances present in cells of the granulocyte series.Both muramidase23 and ao-antitrypsin4 are presentin such cells but they also occur in histiocytes andsome monocytes, as may, variably, peroxidase.89Conversely, the cysteine protease cathepsin B maybe used to differentiate histiocytic cells from thoseof the granulocytic series: it occurs in lymphoidtissue only in the histiocytic cells and in sinus liningcells.' 1' lThe present findings indicate that leucocyte elas-
tase is a useful "marker' of benign and malignantgranulocytes. In the benign group neutrophils,eosinophils, and (probably) mast cells are all stained
1. -I
0 . .
4p4b
I
copyright. on A
pril 19, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.37.10.1114 on 1 O
ctober 1984. Dow
nloaded from

Crocker, Jenkins, Burnett
Fig.-7 Spleen, infitrated by cells ofacute mye1aid;oleukaemia, which are intensely positively stained.Peroxidase-antiperoxidase technique for elastase;haemalum counterstain x 550.
but neutrophil polymorphonuclear leucocytes areespecially active. The intense positivity encounteredin acute and chronic myeloid leukaemias and theabsence of staining in acute lymphoblastic andchronic lymphocytic leukaemias, together with alack of staining in histiocytes, suggest that onepotentially useful diagnostic role of leucocyte elas-tase staining would be that of differentiatingleukaemias of granulocyte type from those of lym-phoid origin. The technique seems to offer consider-able advantages in relation to the other means ofshowing granulocytes, as described above.
It is of interest that neutrophil type elastase hasbeen shown in extracts from U937 cells, which aremonocyte like.'2 Of course, this may represent a dif-ferent elastase from that shown in the current studyor may be a finding related to the different sen-sitivities of the techniques applied. Certainly, mac-rophage type cells were uniformly negative with ourtechnique. The finding of leucocyte elastase activityin some gut lining cells is also of interest and mayrelate functionally to luminal digestive activity. Inthe diagnosis of leukaemia it is, of course, of littleimportance.We now intend to carry out a prospective study of
leucocyte elastase activity in bone marrow smearsand trephines with a view to distinguishing betweenmyeloid and lymphoid leukaemias.
We are grateful to Mrs Pamela Jackson for secretar-ial help and word processing. Mr MJ Chard gaveexpert photographic assistance, and Dr Catherine BCrocker kindly read the manuscript. This work wassupported by a generous financial grant from the
West Midlands Regional HealthResearch Committee.
Authority
References
Li CY, Yam LT, Crosby WH. Histochemical characterisation ofcellular and structural elements of the human spleen. J His-tochem Cytochem 1972;20:1049-58.
2 Mason DY, Taylor CR. The distribution of muramidase(lysozyme) in human tissues. J Clin Pathol 1975;28: 124-32.
Crocker J. The enzyme histochemistry of lymphomas. Cam-bridge: University of Cambridge, 1983, MD Thesis.
Isaacson P, Jones DB, Millward-Sadler GH, Judd MA, Payne S.Alpha-l-antitrypstn in human macrophages. J Clin Pathol1981;34:982-90.
Saklatvala J, Barrett AJ. Identification of proteinases inrheumatoid synovium. Detection of leucocyte elastase, cathep-sin G and another serine proteinase. Biochim Biophys Acta1980;615: 167-77.
6 Crocker J, Curran RC. Quantitative study of theimmunoglobulin-containing cells in trephine samples of bonemarrow. J Clin Pathol 1981;34: 1080-2.
Hayhoe FGJ, Quaglino D. Haematological cytochemistry. Edin-burgh: Churchill-Livingstone, 1980:146-68.
8Hayhoe FGJ, Quaglino D. Haematological cytochemistry. Edin-burgh: Churchill-Livingstone, 1980:195.
van der Meer JWM, Beelen RHJ, Fluitsma DM, van Furth R.Ultrastructure of mononuclear phagocytes developing in liquidbone marrow cultures. A study on peroxidatic activity. J ExpMed 1979; 149:17-26.
'° Burnett D, Crocker J, Vaughan ATM. Synthesis of cathepsin Bby cells derived from the HL60 promyelocytic leukaemia cellline. J Cell Physiol 1983; 115:249-54.
Crocker J, Burnett D, Jones EL. Immunohistochemical demon-stration of cathepsin B in the macrophages of benign andmalignant lymphoid tissues. J Pathol 1984; 142: 87-94.
12 Senior RM, Campbell EJ. Cathepsin G in human mononuclearphagocytes: comparisons between monocytes and U937monocyte-like cells. J Immunol 1984 (in press).
Requests for reprints to: Dr J Crocker, Department ofHistopathology, East Birmingham Hospital, BordesleyGreen East, Birmingham B9 5ST, England.
1118
AoO"i
.Vt'
copyright. on A
pril 19, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.37.10.1114 on 1 O
ctober 1984. Dow
nloaded from





























