Embed Size (px)
Citation preview
Immuno-chemotherapy
A new standard in the first-line treatment of advanced indolent (follicular) lymphoma?
Michael Herold
HELIOS – Klinikum Erfurt
Germany
Kuala-Lumpur, Malaysia 11.3.06

Non-Hodgkin‘s lymphoma: most frequent (important) entities
Entity Cases (%) 5-year survival (%)
DLBCL 30 46
Follic. lymphoma 22 72
Marginal-Zone B 8 74
(MALT-Type)
B-CLL 7 51
Mantle-Cell L. 6 27
Armitage, Blood 1997

Survival of patients with indolent lymphoma: the Stanford experience 1960–1996
Adapted from Horning. Semin Oncol 1993;20 (5 Suppl. 5):75–88
Pat
ien
ts (
%)
1987–1996
1976–1986
1960–1975
5-year 80%10-year 60%15-year 45%
Years
100
80
60
40
20
00 5 10 15 20 25 30
Median survival ~ 11y!

Expanding treatment options in advanced follicular lymphoma
# Watch and wait
# Mono-chemotherapy
# Combination chemotherapy
# New cytotoxic drugs
# High-dose-chemotherapy +/- TBI + APBSCT
# Biological therapy: monoclonal antibodies
+/- chemotherapy

Rationale for combining chemotherapy and rituximab
Single agent activity
No cross resistance
No over-lapping toxicities
Synergistic effects in vitro
Sensitisation of NHL cell lines by rituximab against cytotoxic drugs in vitro

Rituximab + CHOP in low-grade NHL: efficacy
Czuczman M, et al. Blood 2003;102:411a (Abstract 1493),up date 2005
Previously untreated patients (n=29)
Previously treated patients (n=9)
CR (%) 59 56
PR (%) 41 44
TTP (range, months) 84.9+ (4.5–105.6+)
47.4 (6.8–95.5+)
Duration of response (range, months)
83.5+ (2.9–105.1+)
46.1 (4.1–94+)

Rituximab + CHOP in low-grade NHL: conclusions from a phase II study
Rituximab plus CHOP results in an overall response rate of 100%
Time to progression is prolonged
Combination therapy is safe and does not cause significant added toxicity
Results have to be confirmed in large scale prospective randomized trials
Czuczman M, et al. Blood 2003;102:411a (Abstract 1493)

Chemotherapy +/- rituximab first-line
M 39021 CVP vs R-CVP
GLSG CHOP vs R-CHOP
FL 2000 GELA CHVP vs R-CHVP
M 39023 (OSHO) MCP vs R-MCP

Rationale/questions of all studies:
Can we improve the outcome of patients with advanced indolent NHL/follicular lymphoma by combining chemotherapy with rituximab?
End points :
# response rates, especially complete
responses
# time to progression (PFS) and event-free
survival (EFS), resp. time to
next treatment
# is it even possible to prolong survival,
is cure possible??

M39021: study design
•Follicular NHL (IWF B,C, D)•Stage III-IV•> 18 yrs.•No prior Rx•Measurable Dz•Central histology review
RANDOMIZE
CVP x 4 cycles(q 3 weeks)
R-CVP x 4 cycles (q 3 weeks)
RESTAGING
CVP x 4 cycles(q 3 weeks)
R-CVP x 4 cycles (q 3 weeks)
SD,PD off treatment
R. Marcus, 2005
CR, PR
rituximab 375 mg/m2 IV d1cyclophosphamide 750 mg/m2 IV d1vincristine 1.4 mg/m2 IV d1prednisone 40 mg/m2 PO d1–5

Patient characteristics Characteristic
CVP (n=159)
R-CVP
(n=162)
Median age (years) 53 52
Stage III−IV (%) 99 99
Histology − Follicular NHL (%)
Grade 1, 2 89 90
Grade 3 8 9
Elevated LDH level (%) 26 26
Bulky disease (%) 46 39
Extranodal sites > 1 (%) 17 17
FLIPI 3−5 (poor prognosis) (%) 50 47
FLIPI 2 (intermediate prognosis) (%) 43 40
FLIPI 0−1 (good prognosis) (%) 7 13
Note: central review of pathology performed on 90% of patients, diagnosis of FL confirmed for 95% of patients

CVP ± rituximab in previously untreated FL: response rates
Response
CVP (n=159)
Rituximab + CVP (n=162)
p value
ORR (%) 57.2 80.9 <0.0001
CR (%) 7.5 30.2
CRu (%) 2.5 10.5
CR/CRu (%) 10.0 40.7 <0.0001
PR (%) 47.2 40.1

159CVP
R–CVP
Patients at risk:Study month
162
Ev
en
t-fr
ee
pro
ba
bil
ity
06 12 18 24 30 36 42 48 540 60
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
86
123
51
113
34
98
30
93
21
76
16
66
5
36
1
15
0
5
0
0
Primary endpoint: time to treatment failuremedian FU 42 months
Primary endpoint: time to treatment failuremedian FU 42 months
R-CVP: median 27.0 months
CVP: median 6.6 monthsp <0.0001

Overall survival median FU 42 months
159CVP
R–CVP
Patients at risk:Study month
162
Ev
en
t-fr
ee
pro
ba
bil
ity
p = 0.0553
06 12 18 24 30 36 42 48 540 60
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
155
162
151
160
141
155
136
150
132
144
122
135
72
82
38
43
7
14
0
0
R-CVP: median not reached
CVP: median not reached
89 % vs 81 %
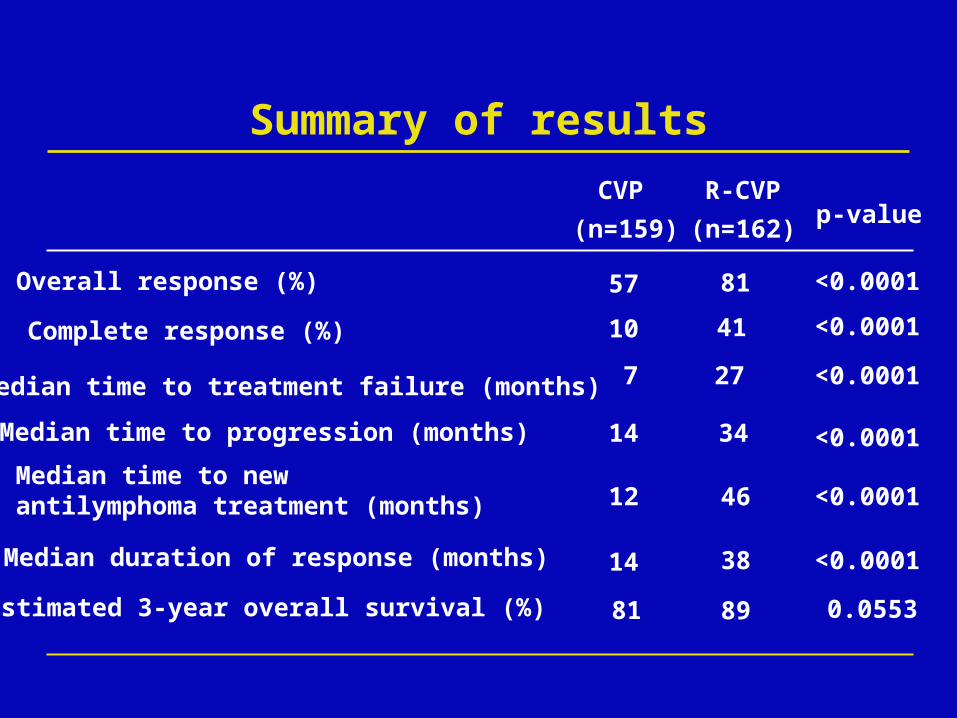
Summary of results
10 41
7 27
14 34
CVP
(n=159)
R-CVP
(n=162)
81
p-value
<0.0001
<0.0001
<0.0001
<0.0001
Median time to treatment failure (months)
Median time to progression (months)
Median time to new antilymphoma treatment (months)
Overall response (%)
Median duration of response (months)
Estimated 3-year overall survival (%)
Complete response (%)
12
14
81
57
46
38
89
<0.0001
<0.0001
0.0553

Conclusions
The addition of rituximab to each of 8 courses of CVP demonstrates major improvement in all clinical endpoints
R-CVP is an effective, short and very low toxicity regimen
R-CVP shows superior efficacy to any other chemotherapy regimen published in a large scale clinical trial

R-CHOP versus CHOP in previously untreated follicular NHL and MCL: protocol
RANDOMISATION
CHOP x 4–6
CHOP x 4–6 +
rituximab
CR, PR
RANDOMISATION
Peripheral blood stem cell transplant
2 x CHOP (+ MabThera) +standard IFN-maintenance
2 x CHOP (+ MabThera) +intensive IFN-maintenance
2 x CHOP (+ MabThera) +standard IFN-maintenance
CR, PR
Hiddemann W, et al. Blood 2004;104:50a (Abstract 161)
<60 years
≥60 years

R-CHOP versus CHOP in previously untreated follicular NHL: response
CHOP (%) (n=272)
R-CHOP (%) (n=284)
ORR 91 97
CR 17 20
PR 74 77
MR 3 1
SD 2 1
PD 3 1
Excluded 1 1
Hiddemann W, et al. Blood 2005
p=0.005

0 1 2 3 4 5
100
80
60
40
20
0
Years
Pat
ien
ts (
%)
R-CHOP (231/285)
CHOP (164/272)
R-CHOP versus CHOP in previously untreated follicular NHL: TTF
Hiddemann W, et al. Blood 2005
p<0.0001

R-CHOP versus CHOP in previously untreated follicular NHL: overall survival
100
80
60
40
20
Years
Pat
ien
ts (
%)
R-CHOP (272/285)
CHOP (249/272)
0 1 2 3 4 5
Hiddemann W, et al. Blood 2005
P=0,016

FL2000 study design
D1 Cyclophosphamide 600 mg/m2
D1 Doxorubicin 25 mg/m2 D1 Etoposide 100 mg/m2 D1-D5 Prednisone 40 mg/m2
α-IFN 2b (Roferon) : 4.5 MU t. i. w for 18 months (3MU if aged > 70)
Rituximab : 375 mg/m2every month for 6 months (arm A &
B) then every 2 months in arm A
R
Arm A
Arm B
Staging including CT-scan and bone marrow biopsy
12 months6 months

Arm A
(n= 183)
Arm B
(n=175)p
CR + CRu 109 (60%) 132 (75%)
.0046
Partial Response 22 (12%) 10 (6%)
Stable/PD/Death 52 (28%) 33 (19%)
FL2000: response at the end of planned therapy
(18 months - 358 patients)
G. Salles - December 2004 ASH Meeting
Cheson criteria

FL2000 : event-free survivalMedian follow-up 31 months
Arm B
Arm A
GS - December 2004 ASH Meeting
Log-Rank P= 0.0031
63%
78%Arm B
Arm A

MCP ± rituximab Rituximab 375mg/m2 IV d 1Mitoxantrone 8 mg/m² IV d 3 + 4Chlorambucil 3 x 3mg/m² PO d 3–7Prednisolone 25 mg/m² PO d 3–7
• Advanced FL, IC and MCL
• 18–75 years• No prior Rx• Central
histology review
• Written informed consent
RANDOMIZE
MCP x 6 cycles(q 4 weeks)
R-MCP x 6 cycles (q 4 weeks)
RESTAGING
MCP x 2 cycles(q 4 weeks)
R-MCP x 2 cycles (q 4 weeks)
SD, PD off treatment
CR, PR
IFN-maintenance for FL
M 39023: study design
ASH, San Diego 12/049. ICML, Lugano 6/05
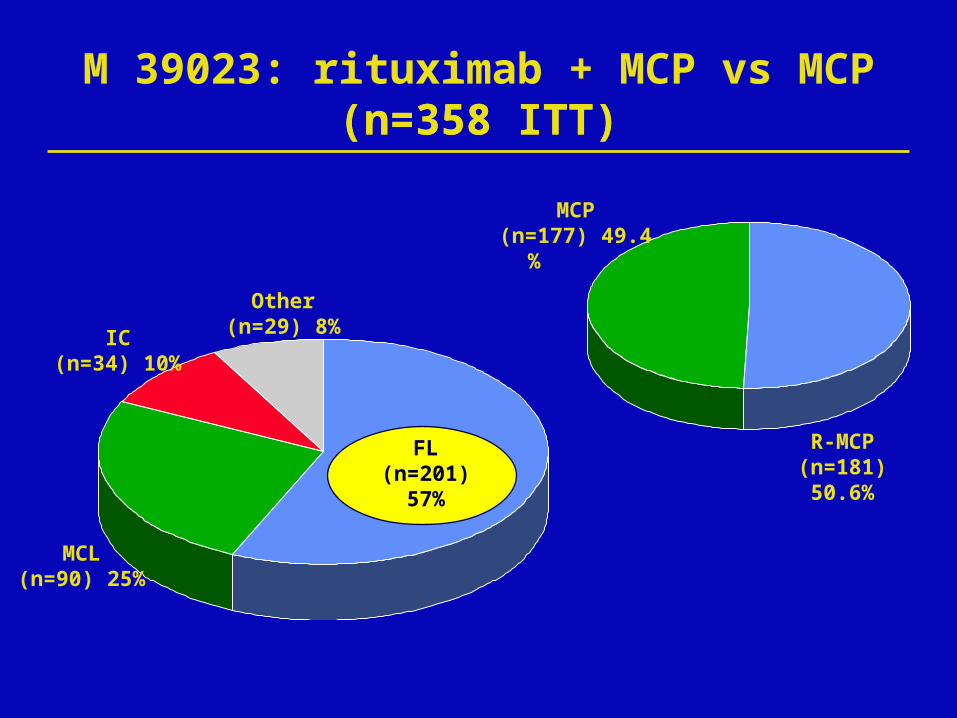
MCP(n=177) 49.4 %
R-MCP(n=181) 50.6%
MCL(n=90) 25%
IC(n=34) 10%
Other(n=29) 8%
M 39023: rituximab + MCP vs MCP(n=358 ITT)(n=358 ITT)
FL(n=201)
57%

M 39023: demographic characteristics follicular lymphoma
R-MCP (105) MCP (96)
Age median 60 (33–78) 57 (31–76)
Sex m/f 53/52 36/60FLIPI (low/interm./high)
8/38/59 6/37/53
Median f/u 7/05 43 (37)
31 mo.
ECOG (0/1/2/3) 68/29/7/1 54/36/6/0
Stage III/IV 30/75 22/74
Bone marrow 73 71

M 39023 toxicity (all SP patients)
R-MCP(n = 183) events/pt.
AE total 1.839/180 (98%)
SAE total 58/34 (19%)
AB-inf.reaction 1/1 (0,5%) (CTC 3)
WBC CTC 3+4 457/130 (71%)
PLT CTC 3+4 20/19 (11%)
Infection CTC 3+4 9/9 (5%)
FUO CTC 3 9/14 (8%)
MCP(n = 177) events/pt.
1.589/157 (89%)
69/41 (23%)
0/0 (0%)
342/96 (54%)
32/18 (10%)
16/14 (8%)
2/2 (1%)

M 39023: remission rates FL patients (ITT population)
RR (%)
CR (%)
92.4 75 0.0009
49.5 25 0.0004
R-MCP MCP pn = 105 n = 96

M39023: progression-free survivalFL patients (ITT population)
median f/u 37 months
Pro
gre
ssio
n-f
ree
surv
ival
1.00
0.75
0.50
0.25
00 10 20 30 40 50 60
Time (months)
3y PFS 77.4%
3y PFS 44%R-MCP: median 54.3 months
MCP: median 27.8 months
p<0.0001CensoredEvents 27 vs 54

M39023: overall survivalFL patients (ITT population)
median f/u 37 months
Ove
rall
su
rviv
al
1.00
0.75
0.50
0.25
0 0 10 20 30 40 50 60 Time (months)
3y OS 88%
3y OS 74%
R-MCP: median not reachedMCP: median not reached
P=0.0140CensoredEvents 14 vs 24
Cause specific deaths: R-MCP 7 vs MCP 16 p=0.0261

Phase III trials of chemo versus R-chemo in previously untreated advanced follicular NHL
Study Treatment, n median FU (mos)
ORR (%)
CR (%)
TTP
(median, mos)
OS
Solal-Celigny et al. [2005]
CVP, 159
R-CVP, 162
42 57
81
10
41
14
34
(p<0.0001)
81%
89%
(est. 3-yr; p=0.0553)
Hiddemann et al. [2005]
CHOP, 205
R-CHOP, 223
18 90
96
17*
20*
29
NR
(TTF; p<0.001)
90%
95%
(est. 2-yr; p=0.016)
Herold et al. [2005]
MCP, 96
R-MCP, 105
37 75
92
25*
50*
25
54
(TTF;p<0.0001)
74%
88%
(36 mos; p=0.014)
Salles et al. [2004]
CHVP-IFN, 175
R-CHVP-IFN, 184
30 73
84
63
79
62%
78%
(EFS; p=0.003)
N/A
*patients who fulfilled CR criteria but had no evaluable negative BM biopsy defined as PR, not CRu

Antibody based therapy - conclusions
New and promising treatment option for NHL including follicular lymphoma,
# effective
# very well tolerated
# but expensive!! ?
Combination of AB with chemotherapy improves the outcome significantly and is a new standard in 2005
Curative potential ??
More, and new, moAB and AB-conjugates will be introduced soon

Treatment costs M 39023
* Active treatment includes the cost of managing adverse events.† Observation includes the costs associated with disease progression, complications, new therapies and other costs.
Type MCP R-MCP p-value
Active treatment*
€ 21,500 € 35,600 < 0.01
Observation† € 30,700 € 17,900 < 0.01
Total € 52,200 € 53,500 0.6

Cumulative treatment costs – per period analyses M 39023
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
90,000
the
rap
yo
bs
1o
bs
2o
bs
3o
bs
4o
bs
5o
bs
6o
bs
7o
bs
8o
bs
9o
bs
10
ob
s 1
1o
bs
12
ob
s 1
3
ob
s 1
4
MCP
R-MCP
21 months after end of initial therapyC
um
ula
tive
tre
atm
en
t c
ost
s (
€)
Unpublished data

Antibody based therapy - conclusions
New and promising treatment option for NHL including follicular lymphoma,
# effective# very well tolerated# but expensive !! ?
Combination of AB with chemotherapy improves the outcome significantly and is a new standard in 2006
Curative potential ??
More, and new, moAB and AB-conjugates will be introduced soon
European study perspectives

R – MCP x 6 + 2 R
R – CHOP x 6 + 2 R
R – FCM x 6 + 2 RCR+PR
RANDOMIZE
Observation
R–maintenance (SAKK):375 mg/m² q 2 mo. x 2 y
OSHO # 70 Study (>65)
PRIMA = Primary Rituximab and Maintenance
ChRx x 6-8Rituximab x 8
European CooperationOSHO # 70 (only G) + PRIMA Study (EU)
RANDOMIZE

Advanced FL (<65 J.)RI-CHOP
R-CHOP x 6 +
2 x R
CR, PR
RANDOMISATION
HD-ChRx + APBSCT+
Rituximab–maintenance375 mg/m² q 2 months/2y.
Rituximab–maintenance375 mg/m² q 2 months/2 y.

P
atie
nts
(%
)
1987–1996
1976–1986
1960–1975
Years
100
80
60
40
20
00 5 10 15 20 25 30
2000 – 2010??
Perspectives for follicular lymphoma?