Embed Size (px)
Citation preview

Bull. Org. mond. SantJ 1962, 26, 397407Bull. Wld Hlth Org.
Immunization against Tetanusof Patients Given Injections of Antitetanus Serum*
A. TASMAN, Ph.D.' & F. J. A. HUYGEN, M.D.2
The authors report on an investigation conducted in the Netherlands into the best methodofactive immunization of patients treated with antitetanus serum; the active immunizationis conferred by two intramuscular injections of tetanus phosphate toxoid at one month'sinterval.
Trials were carried out on a total of153 patients to determine the relative value of threetreatment schemes: (a) the first vaccination and the serum injection given simultaneouslybut in different sites, (b) the first vaccination and the serum given in a single mixed inocula-tion, and (c) the first vaccination given one month after the serum injection. The resultsshow that with simultaneous administration of vaccine and serum in different sites thepatient acquires a reasonable antitoxin titre more rapidly than with either of the otherschemes. Not only is he quickly protected, but he also receives his first vaccination at apsychologically opportune moment-when he is being treatedfor an accident.
The authors lay special stress on the value ofbooster injections and discuss the differencein immune response between those under and over 20 years of age.
It is an established fact that the administration ofanimal serum in the prevention or treatment oftetanus, diphtheria, leptospirosis, etc. can render thepatient hypersensitive to a subsequent injection ofserum from the same animal species. In some casesthis hypersensitivity may be manifested as a severeanaphylactic shock, sometimes leading to death(Hasche-Klunder & Pichert, 1953; Wright, 1958).The fact that administration of well-purified anti-tetanus serum can also give rise to severe symptomsof shock has been pointed out by such authors asLansberg (1950). A past history of tetanus does notgive the patient immunity to this disease (Seibold &Bachmann, 1955; Regamey, 1955; Eckmann &Bisaz, 1956; Tasman, 1959).
In view of these facts, it is highly advisable, in allcases in which a serum injection is given either
* This investigation was conducted jointly by the NationalInstitute of Public Health, Utrecht, and the Research Com-mittee of the Dutch College of General Practitioners. Thefollowing members of that College participated: B. de Beer,H. D. Boer, M.D., R. S. ten Cate, M.D., J. de Clerq-Zubli,W. Fokkens, A. Fuldauer, G. J. Heringa, A Hofmans,F. J. A. Huygen, M.D., I. Ph. L. Koperberg,. B. S. Polak,J. R. van Reekum, M.D., F. Schreuder and E. van Westree-nen.
1 National Institute of Public Health, Utrecht, Nether-lands.
' Member of the Research Committee of the DutchCollege of General Practitioners.
prophylactically or therapeutically, that the patientbe immunized against tetanus (and in some casesalso against diphtheria) as soon after the seruminjection as possible. In the majority of cases,active immunization can obviate future seruminjections. It is obvious that this holds true in parti-cular for those who, after injuries, are given anti-tetanus serum prophylactically.
In the Netherlands, active immunization is effectedby two intramuscular injections of 0.5 ml of tetanusphosphate toxoid 3 at one month's interval. Thereis as yet no agreement as to the procedure for activeimmunization following serum injection, and particu-larly as to the manner in which and the time at whichthe first vaccine injection must be given.
In principle, there are two possibilities-namely,(a) the first vaccine injection may be given at thesame time as the antitetanus serum (so-called simul-taneous vaccination); or (b) the first vaccine injectionmay be given 4-6 weeks after the serum injection.
In either case, the second vaccine dose is injected4 weeks after the first. Advocates of simultaneousvaccination include such investigators as Gold &Bachers (1943), Regamey (1955), Eckmann &Bisaz (1956), Hubner (1958), Fisher (1956) and
' Tetanus phosphate toxoid consists of 10 Lf purifiedtetanus toxoid adsorbed on to 3 mg AIPO,/ml.
1111 - 397

A. TASMAN & F. J. A. HUYGEN
Eckmann (1958). Simultaneous vaccination is alsoaccepted conditionally (antitoxin doses not toolarge) by Philipson (1959) and Edsall (1959). In1956 the Deutsche Gesellschaft fur Chirurgie opposedsimultaneous vaccination, but in 1957 accepted a
resolution in which this procedure is recommended(Klingenberg & Maresch, 1958).
Simultaneous vaccination has been opposed bysuch authors as Otten & Hennemann (1940), Ramon(1940), Downie et al. (1941, with reference todiphtheria immunization), Cooke & Jones (1943),Scheibel (1957), Parish et al. (1957), Hennicke (1957)and Fulford (1960). In this connexion it must bepointed out, however, that the majority of authorswho reject simultaneous vaccination refer to immuni-zation with fluid toxoid, i.e., an antigen not boundto an adsorbent (AIPO4 or Al(OH)3).Mention must also be made in this respect of an
investigation made by Regamey, Simon & Wantz(1955), who found but a small difference in serum
titres whether the first vaccine injection was simul-taneous, mixed with antitetanus serum or given one
month after injection of antitetanus serum.
Which method of immunization is used is a matterof great importance both to the therapist and to thepatient. The object of these tetanus immunizationsis twofold. First of all, the patient must be givensufficient immunity against tetanus, as rapidly as
possible. In addition, all patients must be completelyimmunized, i.e., they must in fact receive two injec-tions of vaccine. If the simultaneous vaccinationmethod is adopted, the patient need return onlyonce, to receive the second vaccine injection. If thefirst vaccine injection is not given until 4-6 weeksafter the serum, then the patient must return twiceafter treatment of the injury (serum injection) for thetwo vaccine injections. Obviously, the chance ofcomplete immunization of an optimal number ofpatients is smaller the more often they must appear
in the general practitioner's consulting-room or inthe accident clinic during surgery hours.
AIM OF THE STUDY
In view of the great practical importance of thisquestion and of the diversity of opinions on thesubject, an investigation into the relative value ofthe two immunization schemes outlined aboveseemed indicated. Such an investigation cannot bemade with normal subjects because they cannot beinjected with antitetanus serum unless it is urgentlynecessary (for instance, in the case of injury) in view
of the possible sensitization to horse protein that itmay entail. The investigation therefore required anumber of patients who, as a result of an accidentin which the possibility of tetanus infection had tobe considered, were prophylactically treated withantitetanus serum.
MATERIAL AND METHODS
Patients suitable for this purpose were dividedinto three groups in the order of their reporting fortreatment, and immunized as follows:
I. First vaccination and serum injection separatebut simultaneous (simultaneous vaccination, to bereferred to as SV).
II. First vaccination and serum injection mixed (tobe referred to as S+V).
III. First vaccination and serum injection separateand not simultaneous, the first vaccine injection beinggiven one month after serum injection (to be referredto as S_V).One month after the first vaccine injection, all
patients received the second vaccine injection. Sixmonths after the second vaccine injection all patientswere given a third dose of vaccine (0.5 ml) as abooster injection.At institution of treatment (before serum injec-
tion), and subsequently at fixed intervals, tetanusantitoxin titres were determined in blood samplesobtained by venipuncture. An attempt was alsomade to determine the influence of sex and age onthe titre values.The serum injected was enzymatically purified
antitetanus horse serum, in a dose of 1500 AU, witha few exceptions. The serum was injected intra-muscularly. The vaccine used was tetanus phosphatetoxoid (dose 2 x 0.5 ml). The antitetanus serum andthe tetanus toxoid came from the National Instituteof Public Health, Utrecht. The tetanus phosphatetoxoid for both first and second vaccinations wasinjected intramuscularly into the deltoid muscle.The patients of Group II also received the mixtureof 0.5 ml tetanus phosphate toxoid and 1.0 ml ofantitetanus serum for the first injection in thedeltoid muscle.
Vaccinations and serum injections were given to atotal of 172 patients-57 in Group I (SV), 60 inGroup II (S+V), and 55 in Group III (S-+V).The investigation was arranged to include only
patients who had never been immunized againsttetanus. During the investigation, however, it wasfound from the antitoxin titres obtained (see below)
398

TETANUS IMMUNIZATION OF PATIENTS GIVEN ANTITETANUS SERUM INJECTIONS 399
FIG. 1PLAN OF TREATMENT AND BLOOD SAMPLING
b b b b b bgroup I
s , v ,b'
b b b b b bgroupm \ \ \
0 1 2 3 4 5 6 7 8time in months
b = blood sample and antitoxin determination.s = serum injection.v = vaccine injection (basic immunization).b= booster injection of vaccine.
TABLE IAVERAGE INTERVALS BETWEEN VENIPUNCTURES
BetweenTtime- Group I | Group I Group III
points a
1 and Ia 2.06 weeks 2.00 weeks 2.00 weeks
I and 2 4.15 weeks 4.10 weeks 4.26 weeks
2 and 3 4.10 weeks 4.20 weeks 4.20 weeks
2 and 4 8.30 weeks 8.25 weeks
3 and 4 _ _ 4.22 weeks
2 and 5 5.75 months 5.67 months
3 and 5 _ - 8.57 weeks
3 and 6 _ 5.88 months
5 and 6 7.35 days 7.73 days
6 and 7 _ - 7.30 days
a Time-points for Groups I and II:I = before immunization; Ia = 2 weeks after serum;
2 = 1 month after first vaccination; 3 = 1 month after secondvaccination; 4 = 2 months after second vaccination; 5 = 6months after second vaccination; 6 = 1 week after booster.
Time-points for Group III:1 = before immunization; Ia = 2 weeks after serum; 2= 1
month after serum; 3 = I month after first vaccination; 4 = 1month after second vaccination; 5 = 2 months after secondvaccination; 6 = 6 months after second vaccination; 7 = 1 weekafter booster.
that 19 patients had in fact been immunized prior tothe investigation. The observations made on thesecases have consequently been eliminated from thestatistical analysis,' which consequently deals onlywith 52 patients in Group I (SV), 51 patients in
1 Statistical analysis of the findings was performed bythe Nederlandse Stichting voor Statistiek, The Hague.
TABLE 2
SEX DISTRIBUTION OF PATIENTS TREATED
Sex Group I Group II Group IlIl(S V) (S + V) (S-V)
Males 36 35 29
Females 16 16 21
Total ] 52 { 51 [ 50
Group II (S+V), and 50 patients in Group III(S V).For the procedure regarding antitoxin determina-
tions the reader is referred to the publication ofWilkens & Tasman (1959).The times at which serum injections, vaccinations
and blood samplings were carried out are given inFig. 1 and are also shown in Tables 1, 4, 5 and 6.In some cases (not shown in Fig. 1), a blood samplewas obtained two weeks after the serum injectionand used for antitoxin determination. As shown inTable 1, the average interval between venipunctureswas about 2 weeks or a multiple thereof. About oneweek after the booster injection, the last bloodsample was obtained from all patients.The distribution of patients according to sex is
shown in Table 2. The number of women includedin the investigation is too small to warrant a separateanalysis according to sex.
In the analysis according to age, two groups weredistinguished-those under 20 years of age and those20 years and older. For the sake of completeness, theage distribution of the patients by 10-year age-groups is presented in Table 3.
TABLE 3AGE DISTRIBUTION OF PATIENTS TREATED
Age-group I 1 11 T III(years) ] (S V) j (S + V) (S-_.V)
0-9 5 3 2
10-19 20 17 15
20-29 7 6 3
30-39 5 10 9
40-49 8 10 10
50 and over 7 5 11
Total 52 J 51 50

A. TASMAN & F. J. A. HUYGEN
TABLE 4ANTITOXIN TITRES (AU/ml) IN GROUP I
(FIRST VACCINE INJECTION SIMULTANEOUS WITH SERUM INJECTION)
Before 2 weeks I month 1 month 2 months 6 months 1 weekimmu- after serum after first after 2nd after 2nd after 2nd afternization vaccination vaccination vaccination vaccination booster
(1) (1 a) (2) (3) (4) (5) (6)
<0.001<0.001<0.001<0.001<0.001<0.001<0.0010.001
<0.001<0.001<0.001<0.0010.001
<0.0010.001
<0.001<0.001<0.001<0.001<0.0010.001
<0.001<0.001<0.001
0.001<0.001<0.001<0.0010.001
<0.001<0.0010.002
<0.001<0.001<0.001<0.001<0.0010.001
<0.001
<0.001<0.001<0.0010.001
<0.001<0.001<0.0010.001
<0.001<0.001<0.001<0.001
0.032
0.045
0.2560.0320.2560.320
0.0900.0640.0900.1810.0450.0900.0320.0900.1810.0320.0450.090
0.0060.0010.0040.0030.0060.0450.0160.0110.0160.0160.0080.0060.0080.0160.008
<0.0010.0640.0060.0110.0010.0030.0160.0160.0110.0110.0060.0040.0040.0040.0030.0160.0320.0160.0320.0230.0160.0160.0080.0160.045
0.0640.0040.0900.0110.0040.0020.0110.1280.0110.0110.0040.064
0.0110.1280.0320.181
0.0080.0040.0010.0080.0080.0110.0320.0160.0080.004
0.0320.0010.0900.0060.0040.0040.0080.011
<0.0010.0450.0080.0450.0020.0040.2560.0640.0020.1810.0010.0640.0900.0320.0110.0110.064
0.0450.0640.0160.016
<0.0010.1810.0080.0450.0640.1280.2560.090
0.0450.3200.0230.0900.0640.0230.0160.0080.0640.0160.0160.0900.0230.0160.016
0.0160.0030.2560.0080.0080.0640.0160.0020.0080.0080.0640.0320.0010.0320.0900.0450.0230.1280.0450.2560.1810.0900.0320.1810.090
0.6400.0320.0160.0900.0080.1810.0320.0900.0110.0640.2000.045
0.0080.2560.0900.0640.0640.0640.0320.0450.0600.0320.0010.1280.1280.008
0.1280.1280.3200.0320.0160.0160.0320.0640.0450.1280.0640.0640.0640.0640.0640.0320.2560.5600.2560.4000.1810.3000.2560.5600.800
0.4000.5600.1600.1600.0060.0900.1280.1280.0320.1810.6400.110
2.302.304.504.504.504.503.201.109.000.309.000.560.304.500.64
4.502.302.309.000.562.300.560.309.00
12.8018.109.001.601.102.30
12.804.509.004.509.009.009.002.309.009.00
12.804.504.504.501.102.304.506.402.30
36.204.504.50
400

TETANUS IMMUNIZATION OF PATIENTS GIVEN ANTITETANUS SERUM INJECTIONS
TABLE 5ANTITOXIN TITRES (AU/ml) IN GROUP II
(FIRST VACCINE INJECTION MIXED WITH SERUM INJECTION)
Before 2 weeks I month I month 2 months 6 months 1 weekImmu- after serum after first after 2nd after 2nd after 2nd afternizatlon vaccination vaccination vaccination vaccination booster
(I) (Ia) (2) (3) (4) (5) (6)
<0.001<0.001<0.001<0.001<0.001<0.001<0.001<0.001<0.001<0.0010.002
0.004<0.001<0.001<0.001
0.001<0.001<0.001<0.0010.0010.001
<0.001<0.001<0.001<0.001<0.001<0.001<0.001<0.001
0.001<0.001
0.001<0.001<0.001<0.001<0.001<0.001<0.001<0.001<0.001
0.001<0.001<0.0010.001
<0.001<0.001<0.0010.003
<0.001<0.001
0.0450.0640.2560.0110.0450.2560.2560.0320.1280.1280.0320.0320.0230.0800.064
0.0160.0320.2560.016
0.0060.0010.0080.0160.0040.0110.0020.0110.0040.0060.008
0.0080.0160.0450.064
0.0080.0060.0160.0080.0450.0080.0110.0060.0060.0640.0080.0080.0320.0040.023
0.0320.0060.0060.002
<0.0010.0160.016
0.0160.0160.1810.008
<0.0010.0110.064
<0.0010.0040.0080.0080.0150.002
0.006<0.001<0.0010.0020.0040.016
<0.001<0.0010.0640.0110.011
0.0010.0020.003
0.0080.008
<0.0010.0160.0320.0020.0080.0060.0010.0230.0020.0030.1280.0160.001
0.0010.0230.0030.0080.0030.0040.016
0.002<0.0010.0040.0020.0080.0040.0040.0060.0030.0040.0020.0640.003
0.0160.002
<0.0010.0060.0110.0160.0020.0040.0320.0080.016
0.0060.0110.0600.004
0.0160.0030.0030.1100.1100.0080.0900.0110.0040.0320.0110.0010.2560.0230.006
0.0060.0900.0640.0080.0030.0640.032
0.0060.0110.006
0.1280.1280.0160.006
0.0030.0110.3200.023
0.2560.0080.0040.0230.0320.0110.0060.0080.0640.064
0.0320.0900.1810.023
0.1810.0320.2560.2300.3200.0640.0640.1280.0080.2560.0800.0160.4000.256
0.0640.3000.2560.0450.0060.1810.045
0.2300.0110.1280.0160.0110.5600.0450.006
0.0110.0640.6400.090
6.401.101.60
18.104.502.300.572.300.56
18.104.50
1.104.509.002.30
9.002.301.10
12.809.00
18.1018.1018.102.303.20
18.100.309.009.000.80
1.609.006.404.500.563.209.00
6.400.569.001.109.002.302.301.10
1.103.209.009.00
I__ _* .I_
401

A. TASMAN & F. J. A. HUYGEN
TABLE 6ANTITOXIN TITRES (AU/ml) IN GROUP III
(FIRST VACCINE INJECTION ONE MONTH AFTER SERUM INJECTION)
Before 2 weeks 1 monthimmu- after afternization serum serum
(1) (Ia) (2)
<0.001 0.006<0.001 0.0110.001 0.016
<0.001 0.023<0.001 0.005<0.001 0.006<0.001 <0.001<0.001 0.016<0.001 0.008<0.001 0.004<0.001 0.008<0.001 <0.001<0.001 0.023<0.001 0.008<0.001 0.016<0.001 0.011<0.001 0.0060.001 0.016
<0.001 0.016<0.001 0.032<0.001 0.008<0.001 0.002<0.001 0.008<0.001 0.008<0.001 0.004<0.001 0.011<0.001 0.004<0.001 0.016<0.001 0.032<0.001 0.0320.001 0.0110.001 0.008
<0.001 0.016<0.001 0.045 0.0160.001 0.023 <0.0010.001 0.128 0.016
<0.001 <0.001<0.001 0.004<0.001 0.090 0.064<0.001 0.045 0.011<0.001 0.256 0.008<0.001 0.064 <0.001<0.001 0.008<0.001 0.181 0.003<0.001 0.032 <0.0010.001 0.181 0.020
<0.001 0.090 0.023<0.001 0.008 0.002<0.001 0.064 0.008<0.001 0.090 0.032
I month I month 2 months 6 months I weekafter first after 2nd after 2nd after 2nd aftervaccination vaccination vaccination vaccination booster
(3) (4) (5) (6) (7)
<0.0010.008
<0.0010.002
<0.0010.0230.0010.0010.008
<0.001<0.0010.0020.0110.0010.0010.002
<0.001<0.001<0.0010.003
<0.001<0.001<0.0010.0160.0230.0010.0160.0080.002
<0.0010.0080.0160.0080.032
<0.0010.0320.0020.0020.0020.0010.0010.0080.0010.003
0.0030.0030.0010.2560.002
0.181 0.2301.280 0.3200.090 0.0400.450 0.1600.008 0.0040.256 0.0320.001 0.0040.181 0.2560.032 0.0230.032 0.0640.006 0.0230.362 0.1284.500 4.5000.016 0.0080.128 0.3200.090 0.0640.128 0.1600.008 0.0640.128 0.3200.045 0.0640.064 0.0320.128 0.3200.460 0.2560.045 0.0900.128 0.0640.064 0.0320.256 0.0450.045 0.0640.016 0.0450.090 0.0230.450 2.3000.181 0.1289.000 2.3000.032 0.0900.023 0.0320.128 0.4000.320 0.2300.128 0.2560.181 0.2560.128 0.2560.064 0.1280.090 0.0900.045 0.0160.064 0.032
1.100 0.2560.064 0.0450.016 0.0321.100 0.9000.045 0.032
0.0640.256
0.0900.0040.0110.0160.4500.0320.0640.0320.3201.2800.0450.230
<0.0010.0800.0230.5600.5600.0600.5600.0900.1280.2560.0110.0640.2560.0900.0320.5600.1500.3000.2560.0450.5600.3000.4000.3200.3000.1810.2300.0160.160
0.5600.1600.0301.1000.128
2.3012.80
2.300.573.200.57
18.102.309.002.309.009.001.606.409.004.500.206.403.200.804.504.501.606.400.564.509.002.30
9.009.002.309.004.509.001.104.500.562.309.00
12.800.302.30
51.204.504.5012.802.30
_ _
An')

TETANUS IMMUNIZATION OF PATIENTS GIVEN ANTITETANUS SERUM INJECTIONS
The titres at various times before and after immu-nization in the 153 patients not previously immunizedagainst tetanus are shown for each group in Tables4, 5 and 6.
RESULTS
GeneralThe geometrical mean of the titres given in
Tables 4, 5 and 6 was determined for each of the timepoints shown in those tables. The titre values<0.001 were read as 0.00025. The results arepresented in Table 7 and Fig. 2. The margin ofaccuracy of a mean titre value is about 30% of thetitre value (P <0.05).From Fig. 2 it will be seen that the passive immun-
ity resulting from serum injection (the degree ofwhich was not measured immediately after injection)gradually decreases and disappears after about twomonths. Active immunity does not occur untilabout one month after the second vaccine injection.The figure also includes a curve showing the courseof titre values in controls immunized against tetanuswho were not treated with serum; this curve is basedon an investigation by Tasman, Bangna & Smith(1961).
Fig. 2 shows that, after SV treatment (Group I),the titre first decreases but that, after about a month,
TABLE 7GEOMETRICAL MEAN VALUES OF TITRES SHOWN IN
TABLES 4, 5 AND 6
Group I Group II Group iITime I
(S V) (S+V) (S-+V)
At institution of treatment _ a _ a - a
After 2 weeks b 0.082 0.057 0.067
After I month 0.010 0.009 0.007
After 2 months 0.017 0.004 0.002
After 3 months 0.035 0.010 0.096
After 4 months - - 0.091
Before booster injection 0.084 0.054 0.092
1 week after booster injection 3.1 3.3 3.2
Number of subjects 52 51 { 50
a At institution of treatment, this value was <0.001 AU/mlfor all groups. Immediately after serum injection, however, itincreased to a considerably higher level in all patients. Thisvalue was not determined.
b The number of observations after 2 weeks was 18 for Group I,19 for Group II and 14 for Group Ill.
log. titre
II0
-
-3 L0
FIG. 2MEAN TITRE VALUES IN TREATED PATIENTS
t~~~~~~~~~~~~~~~~~~~~s v
- -. group IL s5vg- . group m s_v
- controls,not treated
'4 with serum
2 3 4 5 6 7 8time in months
active immunity prevails over passive immunity.After two months there is an unmistakable increasein titre values.
After S+V treatment (Group II), in which antigenand antibody probably influence each other in themixture, the titre after a month had decreased to thesame level as for Group I, but the decrease con-tinued until about 2 months after institution oftreatment. At that time the titre value rises againowing to active immunity. It always, however,remains below the level seen in Group I.S-+V treatment (Group III) shows an entirely
different picture. Immediately after serum injectionthe titre value shows a marked increase (as inGroups I and II). After a month, when the firstvaccine injection is given, the titre value has decreasedto slightly below the level found in Groups I and IIabout a month after the first vaccine injection.Another month later, passive immunity has disap-peared almost completely; active immunity is notyet discernible, so that the antitoxin titre is virtuallyzero. After this, however, the titre value very rapidlyrises in Group III (which in this respect is compara-ble to the control group), to a level which in Groups Iand II is not even fully reached seven months afterthe institution of treatment. Considering the situa-tion about six months after institution of treatment,we find only slight differences in mean titre valuesbetween the three modes of treatment. The reactionto the booster injection, too, is about the same in thethree groups (a very marked rise to a level of3 AU/ml.).The differences between the three groups in the
course of the mean titre values can also be demon-strated by correlation with the so-called " level ofprotection ", i.e., the antitoxin titre (expressed in
11.
4()3
I

A. TASMAN & F. J. A. HUYGEN
AU/ml) which protects a patient from the sequelaeof infection by tetanus bacilli.
Opinions as to the height of this level vary widely.It has been estimated at 0.01 AU/ml by Sneath(1936), at 0.1 AU/ml by Gold (1938), at 0.01-0.2AU/ml by Bigler & Werner (1941), at 0.007-0.01 AU/ml by Wolters & Dehmel (1943), at 0.001-0.01 AU/mlby Cooke & Jones (1943), at 0.2 AU/ml by Bigler(1951) and by Morl (1954), at 0.03-0.06 AU/ml byTurner, Stafford & Goldman (1954), at 0.05 AU/mlby Regamey (1959), at 0.005-0.01 AU/ml by Scheibel(1955), at 0.01-0.1 AU/ml by Wright (1958), and at0.1 AU/ml by Cruickshank (1960). The titre valuesgiven thus vary between 0.001 and 0.2 AU/ml. Ofcourse, an estimate of this titre value can only bemade on the basis of highly speculative considera-tions. Only Wolters & Dehmel (1943) attempted todetermine this level by means of an experiment on
themselves. They immunized themselves activelyagainst tetanus with fluid tetanus toxoid and thentolerated 2-3 " fatal " doses of tetanus toxin (also, ofcourse, a relative quantity). Before the toxin injec-tion their serum titres were 0.007 and 0.01 AU/ml,respectively.
In view of the above we selected 0.011 AU/ml-avalue included in our titration series-as the " levelof protection ". It was then possible to calculate foreach point of time the percentage of patients whowere or were not protected (Table 8 and Fig. 3).
FIG. 3
PERCENTAGE OF TREATED PATIENTS PROTECTED ATA PRESUMED LEVEL OF PROTECTION
OF 0.011 AU/ml
* I~~~~~~~~~~~~~~~~~~~I. J
, _ _ ,~~~~~~~~~~~~.
7 atime In months
Assuming that a level of protection of about0.011 AU/ml is the closest approximation to thetrue situation, it can be seen from Table 8 and Fig. 3that in each of the three groups about 50% ofpatients are protected about one month after serum
injection. This, then, is a protection which remainsfrom the passive immunity conferred by'the initialadministration of antitetanus serum. A month later,however, it is found that about 60% of the patients inGroup I are protected, while this percentage is only24 and 18 in Group 11 and Group 111, respectively.These results, therefore, are considerably less favour-
TABLE 8
PERCENTAGE OF TREATED PATIENTS PROTECTED AT A PRESUMED LEVEL OF PROTECTION OF 0.011 AU/ml
At After After After After Before AfterTreatment group institution of 1 month a 2 months a 3 months a 4 months a booster booster
treatment injection injection
Group I (S V):Protected 100 56 61 83 - 92 100
Not protected 0 44 39 17 8 0
Group 11 (S+V):Protected 100 42 24 56 85 100
Not protected 0 58 76 44 15 0
Group III (S--*V):Protected 93 46 18 92 94 96 100
Not protected 7 54 82 8 6 4 0
a It should be borne In mind that, for Group I and Group 11, the figures In the column 11 After 1 month " refer to titre valuesdetermined one month after first vaccination, while for Group III they Indicate the titre values determined one month after the admi-nistration of serum but before the first vaccine Injection. This time difference also holds for the columns 11 After 2 months After3 months " and " After 4 months ".
404
TETANUS IMMUNIZATION OF PATIENTS GIVEN ANTITETANUS SERUM INJECTIONS
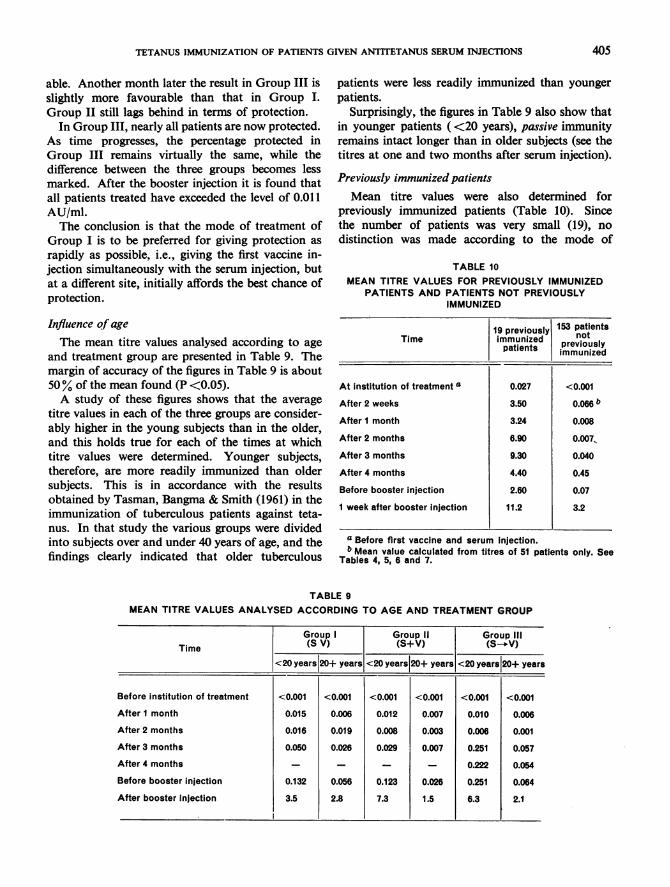
able. Another month later the result in Group III isslightly more favourable than that in Group I.Group II still lags behind in terms of protection.
In Group III, nearly all patients are now protected.As time progresses, the percentage protected inGroup III remains virtually the same, while thedifference between the three groups becomes lessmarked. After the booster injection it is found thatall patients treated have exceeded the level of 0.011AU/ml.The conclusion is that the mode of treatment of
Group I is to be preferred for giving protection asrapidly as possible, i.e., giving the first vaccine in-jection simultaneously with the serum injection, butat a different site, initially affords the best chance ofprotection.
Influence of ageThe mean titre values analysed according to age
and treatment group are presented in Table 9. Themargin of accuracy of the figures in Table 9 is about50% of the mean found (P <0.05).A study of these figures shows that the average
titre values in each of the three groups are consider-ably higher in the young subjects than in the older,and this holds true for each of the times at whichtitre values were determined. Younger subjects,therefore, are more readily immunized than oldersubjects. This is in accordance with the resultsobtained by Tasman, Bangma & Smith (1961) in theimmunization of tuberculous patients against teta-nus. In that study the various groups were dividedinto subjects over and under 40 years of age, and thefindings clearly indicated that older tuberculous
patients were less readily immunized than youngerpatients.
Surprisingly, the figures in Table 9 also show thatin younger patients (<20 years), passive immunityremains intact longer than in older subjects (see thetitres at one and two months after serum injection).
Previously immunized patientsMean titre values were also determined for
previously immunized patients (Table 10). Sincethe number of patients was very small (19), nodistinction was made according to the mode of
TABLE 10MEAN TITRE VALUES FOR PREVIOUSLY IMMUNIZED
PATIENTS AND PATIENTS NOT PREVIOUSLYIMMUNIZED
19 previously 153 patientsTime immunized not
patients peiul
At institution of treatment a 0.027 <0.001
After 2 weeks 3.50 0.066 b
After 1 month 3.24 0.008
After 2 months 6.90 0.007,After 3 months 9.30 0.040
After 4 months 4.40 0.45
Before booster injection 2.60 0.07
1 week after booster Injection 11.2 3.2
a Before first vaccine and serum Injection.b Mean value calculated from titres of 51 patients only. See
Tables 4, 5, 6 and 7.
TABLE 9MEAN TITRE VALUES ANALYSED ACCORDING TO AGE AND TREATMENT GROUP
Group I Group II Group IlIlTime (S V) (S+V) (S-_V)
<20 years|20+ years <20 years|20+ years <20 years|20+ years
Before institution of treatment <0.001 <0.001 <0.001 <0.001 <0.001 <0.001
After I month 0.015 0.006 0.012 0.007 0.010 0.006
After 2 months 0.016 0.019 0.008 0.003 0.006 0.001
After 3 months 0.050 0.026 0.029 0.007 0.251 0.057
After 4 months - - - - 0.222 0.054
Before booster injection 0.132 0.056 0.123 0.026 0.251 0.064
After booster Injection 3.5 2.8 7.3 1.5 6.3 2.1
405
A. TASMAN & F. J. A. HUYGEN
treatment. For comparison the mean titre values ofTable 7 (averaged for the three modes of treatment)are also presented.
Table 10 shows that the average titre value inpreviously immunized patients, determined twoweeks after institution of treatment, has alreadyreached the level attained by other patients onlyafter the booster injection. It appears that for thepreviously immunized group the vaccine injectionsat the beginning of treatment (active immunization)have been fundamentally nothing but boosterinjections.
DISCUSSION AND CONCLUSIONS
A survey of the results reported above would seemto warrant the following conclusions.As to the scheme of vaccination of patients
treated with antitetanus serum, it has been shownthat simultaneous vaccination (Group I) is definitelypreferable to the mode of immunization used in theother groups. The first vaccine injection givensimultaneously with the serum but at a different sitehas the following advantages.
1. Patients relatively rapidly attain a reasonableantitoxin titre and, as compared with other modes ofimmunization, relatively rapidly acquire an accept-able degree of protection.
2. Patients receive the first vaccine injection at apsychologically opportune moment-the time oftreatment for a wound-at which they are undoubt-edly more inclined to submit themselves to activeimmunization than they would be if the first vaccineinjection were not given until 4-6 weeks later.
3. Patients need return only once to complete thisactive immunization. As a result the total number ofpatients ccmpletely immunized will be considerablylarger (more patients will in fact receive both antigeninjections).
4. Treatment by simultaneous vaccination alsosaves the practitioner one consultation or one treat-ment at an accident clinic.
We found that about 10% of treated patients hadin fact been actively immunized against tetanus inthe past. This fact was unknown to the practitionerat the time of treatment. These patients thereforereceived a presumably unnecessary injection ofantitetanus serum. A booster injection of 0.5 mltetanus phosphate toxoid would have been sufficient.In this connexion mention must be made again ofthe great importance of full and proper recordingof all active immunizations performed, particularlyof those against tetanus (Giesberger, de Rover &Tasman, 1958).The enormous effect of the booster injection should
be emphasized once again (Tables 4, 5, 6, 7 and 10and Fig. 2), and we strongly recommend that thisbooster injection be given to all actively immunizedsubjects (who received their last vaccine injectionnot longer than four years previously) on the occasionof any injury which may even remotely entail arisk of tetanus infection.
Excessive reliance on such immunity as maysubsist from active immunization in the past canentail grave and unnecessary risks. Boyd & Mac-Clennan (1942), Simon & Patey (1940) and Boyer etal. (1953) have described a number of cases of tetanusin patients previously actively immunized againsttetanus (for the most part war wounds in militarypersonnel) but not given a booster injection. Someof these patients had been actively immunizedagainst tetanus only one year before the time of theinjury!
Referring again to the figures in Table 9, it must bereiterated that the mean titre values for each of thethree modes of treatment are considerably higher inyounger subjects (up to 20 years) than in olderpatients (20 years and over). As stated earlier, thismeans that younger subjects show a more favourableand more rapid response to the antigen stimulusthan do the older. But it also shows that youngsubjects retain the passive immunity caused byserum injection for a longer period than do oldersubjects.
RItSUMIt
Cet article expose les r6sultats d'une enque'e visant Asavoir quel est, chez des sujets traites par le serum anti-tetanique (AT), le meilleur mode d'immunisation active.Cette derniere a ete realis6e au moyen de deux injectionsintramusculaires d'anatoxine tetanique phosphatee, faitesA un mois d'intervalle.
La premiere injection d'antigene peut s'effectuer selontrois modalit6s: a) en meme temps que le serum AT,mais en un point different; b) en meme temps que lesdrum AT, et melang6e a ce dernier; c) un mois oudavantage apres l'injection de serum AT.
L'etude d'un materiel clinique assez nombreux (153
406

TETANUS IMMUNIZATION OF PATIENTS GIVEN ANTITETANUS SERUM INJECTIONS 407
sujets) a montre que la premiere de ces techniques est laplus efficace. C'est alors, en effet, que le titre d'antitoxineatteint une valeur suffisante dans le meilleur delai. Plusrapidement proteg6, le blesse regoit aussi la premiereinjection de vaccin au moment psychologique le plus favo-rable puisqu'il est trait6 a l'occasion d'un accident. Parla suite, il ne doit se deplacer qu'une seule fois pourrecevoir la seconde injection de vaccin. En statistique, ilest indeniable qu'un nombre beaucoup plus eleve desujets est completement immunise contre le tetanos(2 injections d'antigene) si l'on utilise la methode a) quise revele superieure a toute autre.Une analyse detaillee des chiffres a montre qu'un certain
nombre de sujets avaient et immunises activement contrele tetanos dans le passe. Le fait etant ignore du medecintraitant au moment de l'accident, ces sujets ont reocu une
injection de serum antit6tanique qui 6tait superflue-,alors qu'une simple injection de rappel d'anatoxine teta-nique phosphatee aurait suffi. Les auteurs signalent a cepropos qu'il est important- surtout en ce qui concerne letetanos - de tenir un fichier des immunisations. Six moisapres la seconde injection de vaccin, les vaccines ont tousrequ une injection de rappel faite avec 0,5 ml d'anatoxinetetanique phosphatee. Les titres d'antitoxine ont atteintchaque fois un niveau de 3 UA/ml environ. Ce fait incitea mentionner l'importance de l'injection de rappel dansle cas de sujets immunises activement contre le tetanos.
Jusqu'a 20 ans, les sujets observ6s ont reagi aux injec-tions d'antigene d'une maniere plus efficace et plus rapideque les sujets plus ag6s. II est interessant de noter que lesindividus jeunes ont conserve plus longtemps l'immunitepassive consecutive a l'injection de serum antit6tanique.
REFERENCES
Bigler, J. A. (1951) A.M.A. Amer. J. Dis. Child., 81, 226Bigler, J. A. & Werner, M. (1941) J. Amer. med. Ass.,
116, 2355Boyd, J. S. K. & MacClennan, J. D. (1942) Lancet, 2,
745Boyer, J., Corre Hurst, L., Sapin Jaloustra, H. & Tissier,M. (1953) Presse med., 61, 701
Cooke, J. V. & Jones, F. C. (1943) J. Amer. med. Ass.,121, 1201
Cruickshank, R. (1960) Rev. Immunol. (Paris), 24, 221Downie, A. W., Glenny, A. T., Parish, H. J., Smith, W.& Wilson, G. S. (1941) Brit. med. J., 2, 717, 759
Eckmann, L. (1958) Prakt. Arzt, 12, 101Eckmann, L. & Bisaz, E. (1956) Schweiz. med. Wschr.,
86, 641Edsall, G. (1959) J. Amer. med. Ass., 171, 417Fisher, J. (1956) Dtsch. Z. Chir., 284, 749Fulford, G. E. (1960) Lancet, 1, 1121Giesberger, H. A. V., de Rover, G. & Tasman, A. (1958)
Ned. T. Geneesk., 102, 1100Gold, H. J. (1938) J. Lab. clin. Med., 23, 903Gold, H. J. & Bachers, H. (1943) J. Immunol., 47, 345Hasche-Klunder, R. & Pichert, M. (1953) Dtsch. med.
Wschr., 78, 1499Hennicke, W. (1957) Dtsch. Gesundh.- Wes., 12, 305Hubner, A. (1958) Dtsch. med. Wschr., 83, 555Klingenberg, H. G. & Maresch, W. (1958) Wien. klin.
Wschr., 70, 606
Lansberg, H. P. (1950) Ned. T. Geneesk., 94, 2201Morl, F. (1954) Dtsch. Z. Chir., 279, 209Otten, L. & Hennemann, I. P. (1940) Geneesk. T. Ned.-
Ind., 80, 194Parish, H. J., Laurent, L. J. M. & Moynihan, N. H.
(1957) Brit. med. J., 1, 639Philipson, L. (1959) Acta. path. microbiol. scand., 45, 203Ramon, G. (1940) J. Amer. med. Ass., 114, 2366Regamey, R. H. (1955) Praxis, 44, No. 12, p. 268;No. 13, p. 288
Regamey, R. H. (1959) Ergebn. Hyg. Bakt., 32, 270Regamey, R. H., Simon, K. & Wantz, M. (1955) Schweiz.
Z. allg. Path., 18, 1157Scheibel, I. (1955) Bull. Wid Hlth Org., 13, 381Scheibel, (1957) Zbl. Bakt., L Abt. Ref., 163, 263Seibold, M. & Bachmann, H. (1955) Dtsch. med. Wschr.,
80, 1188Simon, R. & Patey, G. A. (1940) Presse med., 48, 935Sneath, P. A. (1936) J. roy. Army. med Cps, 66, 311Tasman, A. (1959) Ann. Inst. Pasteur, 97, 835Tasman, A., Bangma, P. J. & Smith, L. (1961) Antonie
v. Leeuwenhoek (in press)Turner, T. B., Stafford, E. S. & Goldman, L. (1954)
Bull. Johns Hopk. Hosp., 94, 204Wilkens, R. L. & Tasman, A. (1959) Brit. med. J., 2, 1305Wolters, L. K. & Dehmel, H. (1943) Z. Hyg. Infekt.-Kr.,
124, 326Wright, G. P. (1958) Proc. roy. Soc. Med., 51, 997





























