Embed Size (px)
Citation preview

375
C H A P T E R 1 0
Patients with autoimmunehemolytic anemia (AIHA)often present with anemia ofsufficient severity to suggest aneed for blood transfusion.When anemia of such severityis discovered, physicians fre-quently refer a sample ofblood to the blood transfusionlaboratory while simultane-
ously initiating diagnostic studies to determine thecause of the anemia. Indeed, a diagnosis of AIHA isoften first made by the blood transfusion service whenautoantibodies are detected during the performanceof the compatibility test.
Transfusion of patients with AIHA presents a uniqueset of potential problems. The indications for transfu-sion must be considered in light of the following facts:
• The risks of transfusion are somewhat increaseddue to the difficulty of compatibility testing.
• The patient’s autoantibody can be expected tocause a shortened life span of transfused red bloodcells (RBCs).
Nevertheless, blood should never be denied to apatient with a justifiable need, even though the com-patibility test might be strongly positive.1-5
In this chapter, we first discuss the principlesconcerning indications for blood transfusions for
patients with AIHA. We next review the methodsthat should be employed for the optimal selection ofblood for patients with autoantibodies. Finally, wediscuss the optimal volume of blood to be transfused(which can be of critical importance in safely treatingpatients with severe hemolytic anemia), in vivocompatibility testing, the use of warm blood forpatients with cold antibody AIHAs, the use of RBC substitutes, the use of washed or leukocyte-reduced RBCs, and the use of autologous blood fortransfusion.
ASSESSING THE NEED FORTRANSFUSION IN PATIENTS WITHAUTOIMMUNE HEMOLYTIC ANEMIA
As with all clinical decisions concerning therapy, thepossible benefits must be weighed in relationship topotential risks. The advisability of blood transfusion isrelated to the severity of the anemia, to the determi-nation of whether the anemia is rapidly progressive,and especially to the associated clinical findings.Although, as indicated previously, the risks associatedwith transfusion for patients with AIHA are greaterthan for patients without immunohematologic abnor-malities, the risk of not transfusing is even greater formost patients with severe anemia, and transfusion ismandatory in patients with life-threatening anemia.
Blood Transfusion inAutoimmune HemolyticAnemias

376 Immune Hemolytic Anemias
A major difference between transfusing patientswith AIHA and those without RBC autoantibodies isthat the clinician must consider the time that isrequired by the transfusion service to do complexserologic tests to assure that the optimal RBC productis obtained. The clinician and the transfusion servicemust be in contact with one another so that the trans-fusion service understands the urgency of the situa-tion and the clinician understands the complexity ofthe serologic studies to be undertaken. In a largemajority of cases, adequate time can be taken to com-plete appropriate antibody identification studies andcompatibility tests. In extremely urgent situations, itcould be necessary to take added risks, but even here,cautionary measures can minimize these risks.
Nowhere in the management of patients withimmune hemolytic anemias is the communicationbetween clinician and laboratory personnel moreimportant than with regard to blood transfusion.Because the serologic evaluation potentially can betime consuming, notification of the potential need fortransfusion and initiation of work-up should occur assoon as transfusion is considered.6,7 Results of evalua-tions performed at other facilities (e.g., prior identi-fication of alloantibodies or determination of thepatient’s RBC phenotype) can expedite the prepara-tion of blood. The knowledge of recent transfusions isalso important for the transfusion service laboratoryto determine the optimal serologic procedures foridentifying RBC alloantibodies in the presence ofbroadly reactive autoantibodies.
Other important information should include ahistory of pregnancy and of prior transfusions.Clinicians frequently forget that the presence of RBCalloantibodies is extremely unlikely if the patient hasnever been pregnant or previously received a transfu-sion. Transfusion medicine specialists are reluctant todepend on such information because the medicalhistory might not be reliable. Indeed, hospitalizedpatients may have been transfused without havingbeen aware of the transfusion. Nevertheless, withsome patients one can be quite sure that there havebeen no previous transfusions or pregnancies, andthis information reassures the physician that noalloantibody-induced hemolytic transfusion reactionwill occur.
Finally, it must be emphasized that the decision totransfuse should depend not on the serologic findingsbut rather on an evaluation of the patient’s clinicalstatus. The patient’s physician should assess theacuteness of onset and the rapidity of progression ofthe anemia, the patient’s symptoms and signs causedby the anemia, and the probable effectiveness oftherapy other than transfusion (see Chapter 11).
Reluctance to Transfuse Patients with AIHA
Perhaps one of the most common mistakes in themanagement of patients with AIHA is the reluctance
to transfuse even those with severe anemia. Examplesof such cases have been reported by Conley and asso-ciates,8,9 who described five patients with AIHA andreticulocytopenia who developed life-threateninganemia but were not transfused because physicianswere concerned that compatible blood could not beobtained. This was true even though the patients’hematocrits were at levels of 8%–10%. After transferto a tertiary care medical center, the patients werepromptly transfused—a measure that the authors feltwas unquestionably life saving.
Patients with AIHA and reticulocytopenia are in a particularly precarious position. Crosby andRappaport10 reported on 15 such patients who werenot transfused; 12 of the 15 patients died. Numerousother authors have described reticulocytopenia inpatients with AIHA.11-15 In some instances, the reticu-locytopenia is caused by human parvovirus B19.16-18
In other cases, it could have an immune basis, and inmany instances there is no identifiable cause19,20 (seealso Chapter 3).
Assessing the Acuteness of Onset and Rapidity of Progression of AIHA
When a patient presents with AIHA and a moderatelysevere anemia, it is not possible to predict with cer-tainty whether the anemia will rapidly become moresevere. Thus, serial determinations of the hemoglobinand hematocrit should be performed at intervalsdetermined by the evaluation of the severity of theillness. In particular, the physician should notewhether the patient appears acutely ill with symp-toms attributable to acute hemolysis—fever, malaise,and pain in the back, abdomen, and legs.21 It is alsoimportant to note whether hemoglobinuria andhemoglobinemia are present. These findings areusually manifestations of severe hemolysis.
If a patient is acutely ill or has a history of an abruptonset of the illness, or if visual inspection of serum andurine indicate hemoglobinemia and/or hemoglobin-uria, the hematocrit level should be determined every 2to 4 hours initially. In less acutely ill patients, initialtesting may take place at 12- to 24-hour intervals. Thefrequency of testing may soon be decreased if the sever-ity of the anemia proves to be essentially constant. Insome cases of fulminant hemolysis, a significant fall inthe hematocrit can occur within hours, whereas in amajority of patients with AIHA, the anemia is moreslowly progressive.
THE APPROPRIATE USE OF BLOOD IN VARIOUS CLINICAL SETTINGS IN PATIENTS WITH AIHA
Stable Anemia during Initial Evaluation
Patients with an anemia that is essentially stableduring the initial period of evaluation often need not

Blood Transfusion in Autoimmune Hemolytic Anemias 377
be transfused, even though they might have symp-toms such as a decrease in exercise tolerance or palpi-tations with exertion. Furthermore, the response totherapy or spontaneous improvement might be rapid.For example, 50% of the patients with warm-antibodyautoimmune hemolytic anemia (WAIHA) will respondto adequate doses of corticosteriods during the firstweek of therapy (Chapter 11), and acute paroxysmalcold hemoglobinuria (PCH) seldom lasts longer than 7 to 10 days.22
Progressively Severe Anemia
Some patients have an anemia that is steadily pro-gressive in severity, leading to the development ofsymptoms of hypoxemia. In association with an eva-luation of the clinical status of the patient, laboratoryvalues offer some guidance as to the necessity fortransfusion (Table 10-1). If the hemoglobin level isabove 10 g/dL, transfusion therapy is almost neverindicated. Even at a level of 8–10 g/dL, transfusion israrely necessary or desirable. Clinical judgment ismost critical at a hemoglobin level of 6–8 g/dL. At alevel of hemoglobin level below 6 g/dL, most patientsrequire transfusion.
Manifestations of life-threatening anemia can occur,such as progressively severe angina, cardiac decom-pensation, or neurologic symptoms that includemarked lethargy, weakness, somnolence, and mentalconfusion. These symptoms usually occur when thehemoglobin level is below 5 g/dL but can developeven with less severe anemia. The presence of suchsymptoms indicates an urgent need for transfusion,but transfusion should be not be withheld until thosesymptoms arise. For patients with anemia of suchseverity, or for those patients whose rate of progres-sion of anemia indicates that this level of severity willprobably be reached, RBCs are needed urgently.Indeed, death could result from progressive anemia.In the management of these acutely ill patients, thetransfusion of RBCs sufficient to maintain a modestincrease in hematocrit until therapy for the AIHAbecomes effective is probably optimal.
Chronic Stable Anemia
Many patients (especially those with cold agglutininsyndrome) are able to compensate partially for theirshortened RBC survival and maintain a relativelystable (albeit occasionally quite severe) degree ofanemia. For such patients, for whom transfusion maybe considered as a means of relieving symptoms, theadvantages and disadvantages of such managementmust be weighed carefully. The hazards and incon-venience of long-term transfusions must be consi-dered, and it is often preferable for the patient to livewith some symptoms of anemia rather than to face thehazards of long-term transfusion therapy.23
In some patients, in spite of adequate therapy,hemolysis proceeds chronically at a rate greater thanthat of their RBC production. In this situation, chronictransfusion is necessary to sustain life, and the atten-dant risks, cost, and inconvenience must be accepted.Transfusions will at least partially suppress erythro-poiesis, and the frequency of transfusions will need tobe determined arbitrarily and will depend on the rateof hemolysis. It is usually convenient to give two tothree units of packed RBCs at a time when necessary.It is not advisable to correct the anemia completely,and transfusion to a level of hemoglobin of 8–11 g/dLis perhaps optimal.23
Fulminant Hemolytic Anemia
Least common among the indications for transfusionin AIHA is rapidly progressive anemia caused byacute massive hemolysis. Nevertheless, such fulmi-nant hemolysis does occur, and such patients mighteven be hypotensive.
Patients who have AIHA of such severity are likelyto have gross evidences of hemolysis, particularlyhemoglobinuria and hemoglobinemia. Diagnosessuch as PCH, Clostridium perfringens (welchii) sep-ticemia, and drug-induced immune hemolyticanemia should be investigated quickly. The onset canbe so acute that a reticulocytosis might not bepresent, as the bone marrow might not have hadtime to compensate. Indeed, an increase in the retic-ulocyte count in response to a sudden decrease inRBC mass can require 7 to 10 days.24
Although such patients are uncommon, transfusionfor them is urgent. If manifestations of shock arepresent, the immediate aim of transfusion is toimprove vital signs, which can be restored temporar-ily by the use of electrolyte or colloid solutions.Simultaneously, the physician should communicate asense of urgency to the blood transfusion laboratoryto find RBCs for transfusion. Rarely will these RBCsbe “compatible,” but, nevertheless, transfusion ismandatory in this acute, life-threatening context. Apossible alternative to RBC transfusion is the use ofeffective oxygen-carrying solutions, should theybecome available and practical (also see p. 395).25,26
TABLE 10-1. GUIDELINES FOR ASSESSING PHYSIO-LOGICAL IMPAIRMENT OF THE ANEMIC PATIENTAND PRESCRIBING TRANSFUSION STRATEGY
Average Probability ofHemoglobin SignificantLevel (g/dL) Impairment Transfusion Strategy
≥10 Very low Avoid8–10 Low Avoid; transfuse only if demonstrably
better after transfusion trial6–8 Moderate Try to avoid by decreased activity;
if impossible, transfuse≤6 High Frequently requires transfusion
From Petz LD: Blood transfusion in acquired hemolytic anemia. In Petz LD,Swisher SN, Kleinman S, Spence RK, Strauss RG (eds): Clinical Practice ofTransfusion Medicine, 3rd ed. New York: Churchill Livingstone, 1996:469–499.

378 Immune Hemolytic Anemias
THE RISKS OF TRANSFUSION FORPATIENTS WITH AUTOIMMUNEHEMOLYTIC ANEMIA
Risks Caused by the Patient’sAutoantibody
For patients with AIHA, the risks of blood transfusionbeyond the usual risks relate to the presence of thepatient’s RBC autoantibody. Autoantibodies usuallyreact with all normal RBCs, with the result that anytransfused RBCs are likely to have a shorter-than-normal life span. This reaction cannot be avoided,assuming that optimal therapeutic measures are beingused to treat the AIHA. The RBC autoantibody mightreact strongly in vitro (e.g., 2+ to 4+ by indirectantiglobulin test [IAT]) with all available donor RBCsto be transfused, thus making it impossible to obtaincompatible blood for transfusion. Nevertheless, acutesymptomatic transfusion reactions occur only infre-quently.27,28 Survival of transfused RBCs is about asgood as survival of the patient’s own RBCs, and thenet result is that transfusion generally causes tempo-rary benefit.
Although this finding is generally true, somepatients appear to derive no benefit from transfusion29
or, in very unusual instances, they develop significantcomplications such as acute renal failure,30,31 dissemi-nated intravascular coagulation, or post-transfusionhemoglobinuria.33-36 Such complications are probablymost likely to occur if relatively large volumes ofblood are given and if the patient has brisk hemolysis.
Risks Caused by Alloantibodies
When the patient’s serum reacts with all RBCs inroutine compatibility and antibody identificationtests, the blood transfusion laboratory must use addi-tional techniques in an attempt to demonstrate RBCantibodies other than the autoantibody. This is a criti-cal aspect of selection of donor blood because, if thepatient has previously been transfused or has beenpregnant and has developed RBC alloantibodies (e.g.,anti-D, anti-K, anti-Jka), donor RBCs lacking suchantigens must be selected for transfusion to prevent asevere alloantibody-induced hemolytic transfusionreaction. Such compatibility testing procedures are attimes complex and can be difficult to resolvedefinitively.
Risks Caused by the Increase in RBCMass as a Result of Transfusion
Post-transfusion hemoglobinemia and hemoglobinuriahave generally been attributed to an increased rate ofhemolysis, although they could more commonlyoccur as a result of the increase in the total mass ofRBCs available for destruction.33-35 Awareness of thisrisk has led to strong warnings against overtransfu-
sion of patients with AIHA (see the section on theoptimal volume of blood to be transfused).3,34,37
COMPATIBILITY TESTING IN WARM-ANTIBODY AIHA
The selection of blood for transfusion to patients withWAIHA is one of the most difficult tasks faced by ablood transfusion laboratory. A significant commit-ment of time can be required to resolve the problemspresented by a patient with broadly reactive autoanti-bodies. We have divided the discussion of these prob-lems into a consideration of RBC phenotyping, thedetection of alloantibodies, and the significance ofautoantibody specificity.
Red Cell Phenotyping and Genotyping
Techniques for ABO and Rh cell typing and extendedphenotyping in patients with AIHA are discussed inChapter 6. For all patients with WAIHA who requiretransfusion, we strongly recommend determining theextended RBC phenotype of the patient prior to theinitial transfusion. If time does not allow, it is never-theless advisable to obtain a blood specimen from thepatient for subsequent typing. This information is par-ticularly useful in the management of AIHA.7 Onemust keep in mind that determining the patient’s RBCphenotype can be impossible after the patient hasreceived a transfusion. Therefore, one should not missthe opportunity when the patient is first examined.
Knowledge of the patient’s extended RBC phenotypeprovides valuable information when techniques toidentify serum alloantibodies cannot be performed orproduce inconclusive results. Blood for transfusion canpotentially be selected that lacks those antigens againstwhich the patient could have produced a clinicallysignificant antibody. For example, if the patient’s Rhphenotype is known, it is usually feasible to selectdonor units of the same phenotype to avoid alloanti-body-induced hemolysis. Also, if the patient is, forexample, Jk(a+), one need not be concerned about anti-Jka alloantibodies; if the patient is K negative, the use ofK-negative blood would eliminate concern about thepossible presence of anti-K4 (also see the section later inthis chapter on the use of phenotpyically matched RBCfor transfusion). Also, knowledge of the patient’s RBCphenotype can make selection of RBCs for allogeneicadsorption studies significantly easier (see the discus-sion later in this chapter).
Unfortunately, phenotyping for all RBC antigens canbe difficult when the direct antiglobulin test (DAT) ispositive. The use of monoclonal typing reagents is ofsignificant assistance, as are special techniques with theintent of removing the autoantibody without alteringantigen expression (see Chapter 6).38
In the case of previously transfused patients, onemay separate reticulocytes from the other RBCs andperform typing on them to determine the patient’s phe-

Blood Transfusion in Autoimmune Hemolytic Anemias 379
notype. Branch and colleagues39 described a rapid tech-nique for the age-fractionation of human RBCs intoreticulocyte-enriched (young) RBCs and reticulocyte-poor (old) RBCs. Using this method, it was possible toperform accurate RBC typing for six patients within 12 hours after transfusion of 4 to 29 units of bloodwithin a 12-hour period. Other methods for reticulo-cyte separation using microhematocrit centrifugationhave also been described.40-42 In patients with a positiveDAT, one might also need to first remove IgG from thesurface of the RBC before typing. These complexitiesshould inspire one to perform phenotyping prior to thefirst transfusion.
More recently, methods for genotyping RBCs usingDNA typing have become available.43-45 Castilho andcoworkers45 tested RBCs from 15 patients withWAIHA, all of whom had been phenotyped byhemagglutination for Rh, Kell, Kidd, and Duffy afterantibody dissociation with chloroquine diphosphate.The results for all 15 patients using hemagglutinationwere unclear, probably due to insufficient dissociationof antibodies by the chloroquine treatment. In con-trast, genotyping results were clear, even for patientswho had been transfused because the large excess ofpatients’ DNA prevented detection of DNA fromtransfused leukocytes.
Detection of Alloantibodies
If the patient’s autoantibody reacts with all normalRBCs, several available techniques allow one to detectalloantibodies that might also be present. These pro-cedures are quite practical and should be performedin all cases except when extreme emergency precludesadequate evaluation before transfusion.
The Incidence of Alloantibodies in Patients with AIHA Who Require Transfusion
In seven reported studies of randomly selected seracontaining warm autoantibodies, investigators havefound alloantibodies of potential clinical significancein 12%–40% of samples (Table 10-2).46-53 In someinstances, the alloantibodies are evident even in thepresence of broadly reacting autoantibodies becauseof variable reactivity when tested against an RBCpanel. Three reports, however, indicated that, in42%–77% of sera, alloantibodies were not evidentbefore adsorption.49-51 Because alloantibodies weredetected in 209 of 647 sera (32%) (see Table 10-2), thereis an obvious need for a method to detect these antibo-dies to prevent alloantibody-induced hemolytic trans-fusion reactions. Indeed, undetected alloantibodiescould be the cause of increased hemolysis followingtransfusion, which might falsely be attributed to anincrease in the severity of AIHA.4
Two reports were not included in the foregoingsummary. Sokol and colleagues28 reported finding
clinically significant alloantibodies in 10% of sera.This study is impossible to compare with otherreports because it included sera with both warm- and cold-reactive autoantibodies. Also, the authorspointed out that their policy is to issue K-negativeblood of matched Rh phenotype, and they speculatethat this could have contributed to the relatively lowoccurrence of alloantibodies in their series. For thesereasons, their data were not included in Table 10-2.
So and associates54 reported a rate of alloimmuniza-tion of 11.3% in a Chinese population. They suggestedthat the comparatively low rate of alloimmunizationprobably reflects the genetic homogeneity amongChinese people with respect to RBC phenotypes.
Methods for Detection of RBCAlloantibodies in Patients withAutoantibodies
COMPARISON OF DIRECT AND INDIRECTANTIGLOBULIN TESTS
A comparison of the DAT and IAT sometimes affordsextremely valuable information. In patients withWAIHA, the IAT caused by the autoantibody is gen-erally weaker than the DAT. Apparently, most of theautoantibody is adsorbed to the patient’s RBCs invivo. A coexisting alloantibody will not, of course, beadsorbed by the patient’s RBCs and might result in astrongly positive IAT. Thus, if the IAT is significantlystronger than the DAT, the presence of an alloanti-body in association with the autoantibody is stronglysuspected.
If the DAT is equally strong or stronger than theIAT, no conclusion can be reached concerning thepresence or absence of alloantibodies.
TABLE 10-2. RBC ALLOANTIBODIES IN PATIENTSWITH WARM AUTOANTIBODIES
Number of PercentageAlloantibodies Found/ of Sera with
Reference Number of Sera Tested Alloantibodies
Morel et al47 8/20 40Branch and Petz48 5/14 36Wallhermfechtel et al49* 19/125 16Laine and Beattie50* 41/109 38James et al51* 13/41 32Issitt et al (alloadsorptions)52† 13/34 38Issitt et al (autoadsorptions)52† 5/41 12Leger and Garratty53‡ 105/263 40
Totals 209/647 32
* Forty-two to 77 percent of alloantibodies were not evident before adsorption.† Calculations excluded autoantibodies that mimicked alloantibodies.‡ Sera were first tested for autoantibodies using low-lonic-strength salinesolution. When autoantibodies were initially detected using PEG, 47 percentof sera contained alloantibodies.From Branch DR, Petz LD: Detecting alloantibodies in patients withautoantibodies. Transfusion 1999;39:6–10.

380 Immune Hemolytic Anemias
TESTING PATIENT’S SERUM AGAINST A RED CELL PANEL
If the screening tests for serum antibody reveal anantibody reactive at 37°C, the serum should be testedagainst a panel of phenotyped RBCs, as is routine inany determination of alloantibody specificity. If aweakly reactive autoantibody and a strongly reactivealloantibody are present, the differences in thestrength of the reaction of various cells of the panelwill make this evident. For example, Table 10-3 showsa strong anti-K together with a weak autoantibody.One has no assurance, however, that a patient’salloantibody will react more strongly than the autoan-tibody, so additional tests to detect alloantibody arenecessary.
DILUTION TECHNIQUE
One may select a dilution of the patient’s serum thatreacts approximately 1+ in the IAT, and then test thatdilution against a panel of RBCs. Table 10-4 illus-trates the results obtained in a case in which thealloantibody of anti-c specificity had a titer of 64 andthe autoantibody a titer of only 16. When the undi-luted serum was tested, all cells reacted 3+, but a 1:64dilution of the patient’s serum reacted only with c+RBCs. Although this technique frequently providesuseful information, it is informative only when thealloantibody is of higher titer than the autoantibody,and therefore one cannot rely on it.
Oyen and Angeles55 recommended that sera withautoantibodies be diluted 1-in-5 to screen for under-lying alloantibodies. The success of this approachrequires not only that the autoantibody be in lowertiter than the alloantibody but also that the autoanti-body be essentially nonreactive at the suggesteddilution. Leger and Garratty53 evaluated the effec-tiveness of this method and reported that only 5 of 26(19%) potentially clinically significant alloantibodieswere identifiable (Table 10-5). Fourteen potentiallyclinically significant alloantibodies (54%) were notidentified because they continued to be masked bythe autoantibody after dilution. In addition, 7 of the26 alloantibodies (27%) were not detected becausecompletely negative results were obtained in thediluted serum. Alloantibodies missed by the dilutionmethod included Rh system antibodies, anti-Jka, -Jkb, -Fya, -s, and -Kn/McC. Also, only 20 of 93 sera(22%) containing warm autoantibodies withoutalloantibodies were nonreactive after dilution at aratio of 1:5, indicating that the method is not widelyapplicable. (Oyen and Angeles55 had reported that 50of 119 sera [42%] were nonreactive after dilution to 1-in-5.) Thus, it is preferable to select a dilution of thepatient’s serum that reacts approximately 1+ in theIAT, rather than using an arbitrarily selected dilutionsuch as 1-in-5.
ADSORPTION PROCEDURES—OVERVIEW
Adsorption with autologous RBCs (”warm autoadsorp-tion”) is the optimal method for the detection of allpotentially significant alloantibodies, as it uses thepatient’s RBCs to adsorb the autoantibody from theserum, leaving only the alloantibodies. This is parti-cularly important when clinically significant alloanti-bodies to high-frequency antigens are present. Afurther advantage of adsorption with autologousRBCs compared with allogeneic adsorptions is thatadsorption with only one sample of RBCs is needed.This results in a greater volume of serum remainingafter adsorption than is the case after adsorption withmultiple cells, as is generally necessary with allo-geneic adsorptions. Indeed, unless one begins with agenerous supply of serum, it can be difficult toperform specificity tests and cross-match tests withthe small volume of serum remaining after adsorptiontests with multiple samples of allogeneic RBCs. Theseadvantages are balanced by the fact that it might bedifficult to obtain a sufficiently large sample of RBCsfor autoadsorption studies from severely anemicpatients. This is a particular problem for referencelaboratories, which, therefore, often must rely on theallogeneic adsorption procedure.
It is of no value to incubate patient’s serum and RBCsin vitro to adsorb autoantibody, as this has occurred invivo. It is assumed that autoantibody is present in theserum because all autoantigen sites on the patient’sRBCs are saturated. For effective autoadsorption, someof the antibody coating the patient’s RBCs should beremoved before the procedure. To accomplish this, aheat-elution technique was used originally; the patient’sheat-eluted RBCs were then enzyme-treated to enhanceadsorption of autoantibody.47,56 Currently, the mostwidely used procedure uses “ZZAP” reagent.48 ZZAPconsists of a mixture of 0.1 M dithiothreitol (DTT) plus0.1% cysteine-activated papain or 0.1% ficin; it effec-tively dissociates IgG from RBCs and simultaneouslyresults in their treatment with a proteolytic enzyme.
A less labor-intensive option would be autoadsorp-tion without prior treatment of the patient’s RBCs;this could be feasible using polyethylene glycol(PEG).53,57,58 Although Liew and Duncan57,58 did findthe method effective in their study of six patients, theadsorbing RBCs that they used were also pretreatedwith papain.46 Cheng and coworkers59 commentedthat the method “awaits standardization.” Indeed,Champagne and Moulds60 reported that an autoad-sorption using untreated autologous RBCs mixedwith PEG failed to detect an alloanti-K that wasdetected when the adsorptions were performed withficin-treated autologous RBCs.
Adsorption with allogeneic RBCs (allogeneic adsorp-tion) is necessary when adsorption studies are to beperformed on a patient who has had a recent transfu-sion, or when an adequate supply of the patient’s RBCsis not available. Allogeneic adsorptions may be per-formed using ZZAP-treated RBCs48 or by using PEG

381
TAB
LE 1
0-3
.R
EAC
TIO
NS
OB
TAIN
ED W
ITH
A S
ERU
M C
ON
TAIN
ING
ALL
O A
NTI
-K A
ND
AN
UN
DEF
INED
AU
TOA
NTI
BO
DY
W
HEN
REA
CTE
D W
ITH
A P
AN
EL O
F R
ED C
ELLS
Don
orR
hS
exN
o.P
heno
type
Rh
Kel
lD
uffy
Kid
dLe
wis
MN
SP
1Lu
ther
anLi
nked
Res
ults
CD
Ec
ef
Cw
VK
kK
paK
pbJs
aJs
bFy
aFy
bJk
aJk
bLe
aLe
bM
NS
sP
1Lu
aLu
bX
gaIC
37
IAT
1rr
00
0+
++
00
0+
0+
0+
+0
++
+0
+0
+0
00
++
00
1+2
rr0
00
++
+0
0+
00
+0
+0
++
00
++
0+
0+
0+
+0
03+
3rr
00
0+
++
00
++
0+
0+
++
+0
+0
0+
0+
++
++
00
3+4
r′r+
00
++
+0
00
+0
+0
+0
++
+0
+0
+0
++
0+
+0
01+
5r″
r0
0+
++
+0
00
+0
+0
++
+0
+0
++
++
++
0+
+0
01+
6R 1
wR 1
++
00
+0
+0
++
0+
0+
0+
0+
0+
+0
0+
00
++
00
3+7
R 1R 1
++
00
+0
00
0+
0+
++
+0
+0
0+
++
0+
+0
+0
00
1+8
R 00
+0
++
+0
+0
+0
+0
++
0+
+0
0+
++
++
0+
00
01+
9R 2
R 20
++
+0
00
00
+0
+0
++
0+
+0
0+
0+
++
0+
00
01+
10R 2
R 20
++
+0
00
00
+0
+0
+0
+0
++
00
++
0+
0+
00
01+
IC =
Imm
edia
te C
entri
fuga
tion;
37
= A
gglu
tinat
ion
at 3
7°C
; IA
T =
Indi
rect
Ant
iglo
bulin
Tes
t.N
ote
that
3+
reac
tions
are
obt
aine
d w
ith K
pos
itive
RBC
s; a
ll ot
her c
ells
yiel
d 1+
reac
tions
.
TAB
LE 1
0-4
.R
ESU
LTS
OF
DIL
UTI
ON
TEC
HN
IQU
E TO
DET
ERM
INE
PR
ESEN
CE
OF
ALL
OA
NTI
BO
DY
Dilu
tion
s of
Pat
ient
’s S
erum
24
81
63
26
412
82
56
512
10
24
IAT
on s
cree
ning
cel
ls (p
oole
d)3+
3+3+
2+2+
1+0
00
0
Pan
el o
f G
roup
O C
ells
rrrr
r′r
R1R
1R
1R
1R
2R
2R
2R
2r″
r″
Und
ilute
d se
rum
3+3+
3+3+
3+3+
3+3+
Seru
m d
ilute
d 1:
641+
1+1+
00
1+1+
1+
Agg
lutin
atio
n re
actio
ns a
re g
rade
d as
1+
to 4
+.

382 Immune Hemolytic Anemias
in the procedure. The use of PEG for differentialadsorption procedures has been proposed by severalgroups of investigators.53,59,61,62 There is general agree-ment that the use of PEG reduces the time required forallogeneic adsorptions and is as effective as usingZZAP-treated RBCs.53
Some precautions and qualifying statements aboutthe use of PEG have also been made. Some have sug-gested that weak alloantibodies cannot be detectedusing PEG,60,63-66 whereas in other studies this has notbeen the case.53,59,62 Further, some of these differencesof opinion might be because the methods describedhave varied among investigators regarding suchdetails as the source and composition of PEG and theserum:PEG:RBCs ratio that is used.
Finally, the savings in time when using PEG ratherthan ZZAP is, at least in part, lost by the more exten-sive phenotyping that is necessary for selecting RBCsto be used for the adsorptions.46 ZZAP denatures anti-gens in the Kell and Duffy systems as well as S, andsubstantially denatures s so that one need not be con-cerned about the phenotype of adsorbing cells regard-ing these antigens.48 It might be less labor intensive todetermine the Rh, Kell, and Kidd (and possibly Duffyand Ss) system phenotypes of the patient (whichshould be done in any case) and to minimize thenumber of RBCs used for adsorptions than toroutinely use multiple (e.g., three) samples of RBCsfor adsorptions. Indeed, if one determines the Rh,Kell, and Kidd system phenotypes of the patient, it isoften a simple matter to select one or two examples ofRBCs that would be appropriate for allogeneicadsorptions.40,46,59
In planning ahead for management of patients whowill need allogeneic adsorptions, large volumes ofphenotyped RBCs may be obtained, treated withZZAP or ficin if desired, and stored in the liquid statein Alsever’s solution, ACD, or CPD. If the cells are tobe treated with ZZAP reagent, one merely needs toselect R1R1, R2R2, and rr cells, one of which is Jk(a–)and one Jk(b–). Experience in reference laboratoriesindicates that RBCs for allogeneic adsorption proce-dures can be stored in the liquid state for about one totwo months, with or without prior treatment withZZAP or proteolytic enzymes. Alternatively, if theneed for them is infrequent, they can be glycerolizedand cryopreserved in appropriate sized aliquots.40,67
The foregoing comments point out that critical aspectsof managing patients with autoantibodies who requiretransfusion are to develop a detailed protocol and ob-tain appropriate reagents and cells for adsorptions inadvance, rather than waiting until the arrival of a patientwith AIHA who has an urgent need for transfusion.
Technical information regarding adsorption proce-dures have been published,48,68 and further details areprovided in Chapter 6.
WARM AUTOADSORPTION TECHNIQUE
The optimal adsorption technique, when feasible, iswarm autoabsorption. With this technique, one absorbsthe autoantibody from the patient’s serum at 37°C usingthe patient’s own RBCs after first eluting some of theautoantibody. The procedure can be modified byenzyme treatment of the patient’s RBCs after the elutionprocedure.47 Alternatively, one can use ZZAP reagent,which dissociates IgG from RBC and simultaneouslyresults in their treatment with a proteolytic enzyme.48
After adsorption of the autoantibodies, the serum canthen be tested for alloantibodies, as alloantibodies willnot be adsorbed onto the patient’s own RBCs.
It has been our experience that most autoantibodieshave IAT titers of less than 16 with saline suspendedRBCs, and two autoadsorptions often removes allautoantibody present in the serum. If the autoantibodytiter is higher than 16 by the IAT, more autoadsorp-tions could be necessary to remove all autoantibody.
An even simpler rule of thumb is as follows: If theIAT is 1+, one adsorption is usually all that is required;if the IAT is 2+, two adsorptions should be performed;for a 3+ IAT, three adsorptions are likely to be needed.When the IAT is 4+, three or more adsorptions are gen-erally necessary to remove all autoantibody.
Following the autoadsorptions, the adsorbed serumis retested. It is recommended that potentiators suchas PEG (which enhances autoantibody reactivity) arenot used at this stage. If a negative reaction isobtained, it is assumed that all the serum reactionswere due to the autoantibody. If a positive reactionstill occurs, the adsorbed serum should be testedagainst a panel of RBCs to determine whether alloan-tibody is present or whether autoantibody is stillpresent, thus requiring further autoadsorptions.
In some instances, not all serum antibody is removedeven after multiple adsorptions.54 This could bebecause the autoantibody is so strong that furtheradsorptions are necessary or because the autoantibodymight be reactive against antigens that are destroyedby enzymes or ZZAP. If the latter is the case, thenadsorptions with untreated RBCs may be necessary.
WARM AUTOADSORPTION TECHNIQUE FORRECENTLY TRANSFUSED PATIENTS
We have long recommended that the warm autoad-sorption technique not be used in recently transfused
TABLE 10-5. RESULTS AFTER 1-IN-5 DILUTION OF 119 SERA
Antibody(ies) All CellsNonreactive Identified Reactive
Warm autoantibodies only 20 (22%) 73 (78%)Warm autoantibodies + 7 (27%) 5 (19%) 14 (54%)
alloantibodies
From Leger RM, Garratty G: Evaluation of methods for detecting alloantibodiesunderlying warm autoantibodies. Transfusion 1999;39:11–16.

Blood Transfusion in Autoimmune Hemolytic Anemias 383
patients; it seems possible that donor RBCs that arestill circulating could adsorb both alloantibody andautoantibody from the patient’s serum in vitro.69
There were no published data to substantiate such anopinion, however, and the percentage of a minor pop-ulation of RBCs that would invalidate an autoadsorp-tion procedure was unknown.
To resolve this question, Laine and colleagues70 per-formed in vitro experiments in which D, E, K, Fya, andJka antibodies were absorbed with mixtures ofantigen-positive and antigen-negative RBCs to deter-mine the lowest concentration of antigen-positiveRBCs capable of removing all alloantibody reactivity.The percentage of antigen-positive RBCs in eachmixture was determined using flow cytometry.
Table 10-6 shows the breakpoints of the percentagesof antigen-positive RBCs at which antibody was andwas not detected after three adsorptions with themixtures. Small amounts (2%–6%) of antigen-positiveRBCs completely removed anti-D, -E, and -Fya.Reactivity of two examples of anti-K was removed by11% and 17% of K+ RBCs, respectively. Anti-Jka reac-tivity was completely removed by 4%–5% of Jk(a+)RBCs using a PEG adsorption, although not by 11% ofJk(a+) RBC in a ZZAP absorption procedure. Thepreadsorption titers for all antibodies were notsignificantly different from the titers after adsorptionwith antigen-negative RBCs.
The authors concluded that small amounts ofantigen-positive RBCs are generally capable of remov-ing all alloantibody reactivity, thus providing scientific
evidence that the autoadsorption procedure shouldnot be used in recently transfused patients.Adsorptions using allogeneic RBCs should be used forpatients who have received transfusions within thelast 3 months.70
DETERMINING THE TIME NEEDED FOLLOWING ATRANSFUSION BEFORE AN AUTOADSORPTIONPROCEDURE IS APPROPRIATE
Some investigators have suggested that it is possibleto determine whether an autoadsorption would beaccurate in a recently transfused patient by perform-ing antigen typing to see whether transfused cellswere still circulating. Laine and associates70 studied invitro mixtures of RBCs to determine whether smallamounts (2%–6%) of “transfused” RBCs could bedetected directly by antigen typing. Small percentagesof RBC positive for E, K, and Jka could not be detectedwith monoclonal reagents by macroscopic reading(Table 10-7). Thus, if antigen typing was used to lookfor the presence of circulating transfused RBCs, theresults could be misleading. This procedure shouldnot be relied on to determine whether autoadsorptionwould be “safe.”
Although Laine and associates70 determined that anautoadsorption test is not indicated following a recenttransfusion, their study does not provide insight intohow far removed from transfusion such a test couldbe done. In healthy subjects, RBCs live for about110–120 days.71 For a patient who has autoantibodies
TABLE 10-6. ANTIBODY TITRATION RESULTS AFTER ADSORPTION WITH DIFFERENTPERCENTAGES OF ANTIGEN-POSITIVE RBCs
Antigen-Positive Percentage of Antibody TiterAntibody RBCs Antigen-Positive RBCs after Adsorption
ZZAP PEG
Anti-D R,r 0 8 8–161 0–1 0–22 0 0
Anti-E E+e– 0 4 161 1* 0–13 NT 0
Anti-KExample 1 K+k+ 0 NT 32
13 NT 117 NT 0
Example 2 K+k+ 0 NT 32–6410 NT 111 NT 0
Anti-Fya Fy(a+b–) 0 NT 645 NT 26 NT 0
Anti-Jka Jk(a+b–) 0 32 32–644 4 0–15 8 0
11 4* NT
* Higher percentage of antigen-positive RBCs not used for adsorption studies.From Laine EP, Leger RM, Arndt PA, Calhoun L, Garratty G, Petz LD: In vitro studies of the impact of transfusion on the detection ofalloantibodies after autoadsorption. Transfusion 2000;40:1384–1387.

384 Immune Hemolytic Anemias
without hemolytic anemia, in whom transfused andautologous RBCs would be expected to have normalsurvival, waiting for 3 to 4 months after a transfu-sion before doing autologous adsorption would beappropriate.
In patients with AIHA, transfused RBCs can beexpected to have a shortened survival time.71
Therefore, autoadsorption would seem appropriate ata time interval much shorter than 3 months forpatients with severe hemolysis and a markedly abnor-mal RBC survival time who need repeated transfu-sions. The significance of this finding, however, isnegated by the fact that such patients are also likely toneed repeated transfusions at short intervals. An accu-rate determination of the time when all allogeneiccells have been eliminated is not feasible.
Although waiting for 3 months after transfusionbefore allowing an autoadsorption would seem to bea conservative approach, it might be the most appro-priate policy. Accordingly, the allogeneic adsorptiontechnique is generally the optimal method for detect-ing alloantibodies for patients with WAIHA who needrepeated transfusions.
STORAGE OF AUTOLOGOUS CELLS FOR FUTURE AUTOADSORPTIONS
Because the warm autoadsorption technique is souseful, we recommend storing some of the patient’sRBCs that are obtained before the first transfusionepisode so that they can be used in future autoab-sorptions in the event that continued transfusions arerequired.69 The RBCs may be stored in ACD, CPD, orthe frozen state if facilities are available. Reid and
Toy72 described simple and rapid techniques for pre-serving RBCs using PVP-methanol or formaldehydefixation. Using these methods, RBCs could be storedfor six months and, when used for autoadsorption, theresults were comparable to those using fresh cells.
ALLOGENEIC ADSORPTION
As indicated previously, the warm autoadsorptiontest is not feasible if a patient has been transfusedrecently or if an adequate volume of the patient’s pre-transfusion RBCs is not available. In either of thesecircumstances, the optimal procedure is the allo-geneic adsorption technique—adsorption of autoanti-body from the patient’s serum using allogeneic RBCsof varying phenotypes.
For example, performing an adsorption using aJk(a-) cell of a serum containing a warm autoantibodyand an anti-Jka removes the autoantibody but not theanti-Jka. As with the warm autoadsorption technique,the allogeneic RBCs can be enzyme- or ZZAP-treated.The major practical limitation to the use of the allo-geneic adsorption technique is obtaining an adequatesupply of RBCs of appropriate types for the adsorp-tion (several mL of packed RBCs of each type areneeded).
We suggest using three samples of allogeneicRBCs—one rr, one R1R1, and one R2R2; one sampleshould be Jk(a-) and one should be Jk(b-). We prefer touse ZZAP-treated RBCs, as these will not adsorb anyantibodies to any antigens in the MNS, Kell, Lutheran,and Duffy systems but will adsorb autoantibodiesefficiently. On rare occasions, however, autoantibodieshave specificities that are directed against antigensdestroyed by ZZAP (e.g., Ge, Ena, Kell system anti-gens). Thus, if one is unsuccessful after many adsorp-tions, one should consider adsorbing with untreatedRBCs. The adsorption procedure using allogeneicRBCs is similar to that for using autologous RBCs. Byobserving the pattern of reactivity left in the serum inrelationship to the phenotype of the adsorbing RBCs,one can determine the specificity of the alloantibody.
Disadvantages of adsorbing with allogeneic RBCsare that large volumes of phenotyped RBCs are needed,and that alloantibodies to high-frequency antigens willbe adsorbed by all three RBC samples, leading to a falseassumption that no alloantibody is present. Never-theless, allogeneic adsorption provides the greatestsafety of any procedure other than autoadsorption forselection of blood. Although the possible presence ofalloantibodies of some specificities is ignored, the prob-ability of an alloantibody-induced hemolytic transfu-sion reaction is minimal.
Transfusion services should plan ahead to circum-vent the problem of availability of cells for adsorption,as indicated previously.
In some situations, fewer samples of adsorbing RBCsmay be required. Because the patient’s extended phe-notype should be determined prior to the first trans-fusion, one may select RBCs for adsorption on the
TABLE 10-7. DETECTION OF ANTIGEN-POSITIVECELLS BY USING MONOCLONAL AND POLYCLONAL REAGENTS
Percentage of Monoclonal ReagentAntigen-Positive (Direct Polyclonal
Antibody RBCs Agglutination) Reagent (IAT)
Anti-E 100 4+ NT11 1+mf* NT6 0 NT3 0 NT2 0 NT
Anti-K 100 4+ 4+10 0 Micro†
5 0 Micro2 0 01 0 0
Anti-Jka 100 3+ 3+9 0 1⁄2+mf6 0 Micro2 0 0
* Mixed field.† Microscopic.From Laine EP, Leger RM, Arndt PA, Calhoun L, Garratty G, Petz LD: In vitrostudies of the impact of transfusion on the detection of alloantibodies afterautoadsorption. Transfusion 2000;40:1384–1387.

Blood Transfusion in Autoimmune Hemolytic Anemias 385
basis of these results. For example, if the patient isR1R1, K-negative, Jk(a-), Jk(b+), one may simplyadsorb with ZZAP-treated RBCs that are R1R1 andJk(a-). It could be less labor intensive to determine theRh, Kell, and Kidd system phenotypes of the patientand to minimize the number of RBCs used for adsorp-tions than to routinely use multiple samples of RBCfor adsorptions. But because phenotyping for all rele-vant antigens might not be feasible for a patient whohas a positive DAT, it is prudent to have available asupply of the three examples of RBCs previously sug-gested, which can be used for adsorption regardless ofthe patient’s RBC phenotype.
Autoantibody Specificity
Defining the specificity of the autoantibody73,74 is notas important as excluding the presence of alloantibo-dies, but if time allows and if blood lacking the puta-tive antigens can be found expeditiously, it mightpromote the survival of transfused RBCs. If theautoantibody shows a well-defined specificity (e.g.,anti-e), compatible blood should be obtained unlessthis would delay transfusion significantly.
AUTOANTIBODIES WITH RH SPECIFICITY OR “RELATIVE SPECIFICITY”
Serologists are frequently vague regarding the criteriaused to report an autoantibody as having Rhspecificity. Most warm autoantibodies react with allRBCs of common Rh phenotypes, but they might failto react with gene deletion cells, such as Rhnull cells.Other autoantibodies react with all RBCs tested butreact to a higher titer or score against RBCs bearing aparticular Rh antigen. In either case, the autoantibodyis usually said to have Rh specificity without distin-guishing such reactions from each other or from theclear-cut specificity of Rh alloantibodies, wherein cellslacking the appropriate antigen yield strictly negativereactions. We will use the term relative specificity torefer to antibodies that react with all normal RBCsbearing common Rh antigens but react consistently toa higher titer or score against RBCs containing one oranother Rh antigen.
Tests for determining “relative specificity” ofautoantibody should be performed if time allows, as
RBCs lacking the more strongly reactive antigensurvive significantly better than RBCs that do containit. The dilution technique may be used for determin-ing Rh-relative specificity. In essence, one need onlytitrate the patient’s serum or eluate against R1R1, R2R2,and rr RBCs. Table 10-8 shows results of an eluate thatwould be interpreted as showing “relative specificity”against the e antigen. Such reactions should beconfirmed by testing against several examples ofRBCs with and without the appropriate antigenbefore making clinical decisions based on the “relativespecificity” of the autoantibody.
SIGNIFICANCE OF AUTOANTIBODY SPECIFICITY
Several investigators have studied the in vivo survivalof RBCs of varying Rh phenotypes among patientswho have warm autoantibodies with Rh “specificity.”In most instances, detailed serologic data are notgiven, and the autoantibodies are likely to havedemonstrated “relative specificity.”
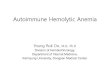
Mollison75,76 described a case in which survival ofthe patient’s own e-positive RBCs was shortenedmarkedly, whereas transfused e-negative RBCs sur-vived almost normally. The patient’s serum containedan autoantibody that reacted preferentially with e+RBCs (Fig. 10-1).
Salmon77 described two patients who had anti-e andanti-nl autoantibodies. In the first case, the T50 of 51Cr-labeled RBCs was 23 days for -D-/-D- RBCs (e-, nl-), 24 days for cDE/cDE RBCs (e-, nl+), and 12.5 daysfor cde/cde RBCs (e+, nl+). In the second case, the T50was 14 days for cDE/cDE RBCs but only 4 days forCDe/cde RBCs.
von dem Borne and colleagues78 reported on apatient who had autoanti-e and anti-nl antibodies.The 51Cr half-time of CDe/CDe RBCs was 1.9 days,and that of cDE/cDE RBCs was 4.0 days.
In Höllander’s patient, the autoantibodies had anti-D specificity; whereas cde/cde blood survived for atleast 31 days, CDe/cde blood survived for only 3days.79 In Crowley and Bouroncle’s patient, two auto-antibodies—anti-D and anti-E—were present, andcde/cde cells survived normally.80 In the patient ofWiener, Gordon and Russow,81 the autoantibodyreacted to highest titers with cells containing the rh’(C) factor; when transfused with blood lacking this
TABLE 10-8. ELUATE SHOWING ANTI-E “RELATIVE SPECIFICITY”
Dilutions of Eluate
2 4 8 16 32 64 128 256
rr(cde/cde) 4+ 3+ 3+ 2+ 2+ 1+ 0 0R1R1(CDe/CDe) 4+ 3+ 3+ 2+ 2+ 1+ 0 0R2R2(cDE/cDE) 3+ 2+ 1+ 0 0 0 0 0
Agglutination reactions are graded as 1+ to 4+.

386 Immune Hemolytic Anemias
factor, the patient made a complete and lasting recov-ery. Previously, she had been treated with randomlyselected Rh-positive donors and had failed toimprove. Ley, Mayer, and Harris’s82 patient was group0 cde/cde. RBCs of phenotype cDE/cDE survivednormally (51Cr T50 = 25 days), but cde/cde cells sur-vived even less well than the patient’s own cells (51CrT50 5 days and 13–14 days, respectively).
Hogman, Killander and Sjolin’s case was a 13-year-old child of phenotype CDe/CDe who had formedautoanti-e antibody and an apparent “nonspecific”component.83 The latter component did not appear tobe of much importance, as cDE/cDE RBCs survivednormally.
Bell and coworkers84 mentioned one patient withanti-e who tolerated two e-negative units with theexpected rise and maintenance of hemoglobin levels.No further details are given.
Habibi and associates29 transfused cDE/cDE RBCsto six patients with autoantibodies of e, ce, or Cespecificities. The blood “proved normally efficient invivo,” but two of six homozygous e+ patients devel-oped anti-E.
Although the preceding data are scanty, we feel thatif an autoantibody demonstrates “relative specificity”(e.g., if the titer against RBCs containing the e antigenis consistently two tubes higher than when testedagainst cells lacking the e antigen), it is preferable toavoid transfusion of blood containing the antigen inquestion, even though this could involve the deliber-ate administration of RBCs containing Rh antigensthat the patient lacks. An exception to this course is
generally made if it would be necessary to give D-positive blood to a D-negative patient.
In contrast to our approach, some immunohemato-logists recommend ignoring the specificity of theautoantibody. This recommendation is based on twoconsiderations. First, the evidence indicating good sur-vival related to autoantibody “relative specificity” isnot extensive. Indeed, in some reports no difference insurvival in vivo can be demonstrated,85 and in others,the benefit has been minimal.78 In other instances,good survival of donor blood lacking the more reactiveantigen has not been shown to be due to the autoanti-body specificity, as survival of transfused RBCs con-taining the more reactive antigen has not beenstudied.29,80,83,84 Second, if one transfuses RBCs thatlack an antigen with which an autoantibody reacts,one might need to use RBCs containing an antigen notfound on the patient’s own RBCs, thus causing thepotential for alloimmunization. This does not seem tobe a critical argument, as typing for Rh antigens otherthan the D antigen is not part of routine blood transfu-sion practice. Such a precaution might be warranted,however, as some data suggest that patients withAIHA have an increased incidence of development ofRBC alloantibodies after transfusion (see the earliersection on the incidence of alloantibodies in patientswith AIHA who require transfusion).
“LEAST INCOMPATIBLE UNITS”
The term least incompatible unit is not an official termin transfusion medicine and is not defined in themedical literature.86 It appears to mean the selectionof a unit of blood that gives weaker reactions in thecompatibility test than other incompatible units. Thatis, one may perform cross-match tests using a numberof donor units that are ABO- and Rh-matched with thepatient and then select the one that reacts leaststrongly. The rationale for using “least incompatible”units appears to be that the stronger reactions couldbe caused by an alloantibody. The use of this termapparently lingers on from the days before effectiveand practical serologic tests were devised for theidentification of alloantibodies in the presence ofautoantibodies that react with all RBCs.
Selecting “least incompatible” units must not beconsidered an acceptable alternative to the techniquesdescribed earlier in this chapter for selecting donorunits for transfusion. Reliance on “least incompatible”units instead of performance of appropriate serologicstudies is a dangerous practice and should be aban-doned, except in extremely urgent settings when timeto perform adequate serologic tests is insufficient.
Some transfusion services appear to use the term“least incompatible unit” in another context. Theyselect donor units for transfusion after adequatelyaccounting for RBC alloantibodies or select units onthe basis of extended phenotyping. Nevertheless, anyunit selected is incompatible with the patient’s
100
75
50
25
00 10 20 30
Days
Per
cent
age
of s
urvi
val
FIGURE 10-1. Survival, in a ddccee patient with autoimmunehaemolytic anaemia of e+ (DCCee) red cells (•), estimated by differen-tial aggultination, and of e– (DccEE) cells (×), estimated by 51Cr-labelingand corrected for Cr elution. The patient’s serum contained anautoantibody reacting preferentially with e+ cells. (From Mollison PL:Measurement of survival and destruction of red cells in haemolyticsyndromes. Brit Med Bull 1959;15:59.)

Blood Transfusion in Autoimmune Hemolytic Anemias 387
autoantibody. Transfusion services might choose tocross-match the selected units with the patient’sserum, although all such cross-matches are incompat-ible. Choosing the “least incompatible unit” fromamong those that have been selected might provide alevel of comfort to the transfusion service personneland can do no harm, but this provides no knownbenefit to the patient. Some variability in reactivitycaused by an autoantibody can be expected to occurwhen a number of units are cross-matched with thepatient’s serum; this phenomenon is due simply to thelimitations of precision of serologic reactions.
The term “least incompatible” unit should beplaced in the garbage heap of serologic terminology. Itis not defined in transfusion medicine nomenclature;it is undoubtedly used differently by various transfu-sion services; its use does not convey informationregarding the extent of compatibility testing per-formed; and finally, the term implies that this is anacceptable alternative to adequate serologic evalua-tion prior to transfusion of patients with AIHA.86
AUTOIMMUNE HEMOLYTIC ANEMIA WITHOUTSERUM AUTOANTIBODY
In contrast to the previously described problems fre-quently encountered among patients with AIHA, itshould also be pointed out that in some patients, theautoantibody does not interfere with compatibilitytesting. This is true because the autoantibody mightbe undetectable in the patient’s serum (apparentlybecause it is entirely adsorbed onto the patient’sRBCs) or is detectable only by techniques more sensi-tive than are used in routine compatibility tests. Even
though the donor blood appears to be compatible, thetransfused RBCs cannot be expected to survive nor-mally. Indeed, Mollison71 has stated that in all thoseconditions in which a hemolytic anemia is due tosome extrinsic mechanism rather than to any intrinsicRBC defect, transfused normal RBCs are expected toundergo accelerated destruction.
Selection of Blood: Summary
With regard to selection of blood for transfusion topatients with WAIHA, we feel that it is most impor-tant to determine the extended RBC phenotype of thepatient, to save some of the patient’s RBCs for futurewarm autoadsorption tests, to compare the strengthof the DAT and IAT, to test for antibody specificityusing a routine RBC panel, and to perform the warmautoadsorption test. In a recently transfused patient,an allogeneic adsorption test should replace thewarm autoadsorption test unless pretransfusionRBCs are available. If time allows, one may also testfor autoantibody specificity (e.g., Rh “relative specifi-city”). Table 10-9 summarizes our recommendations.
The Optimal Frequency of Tests forAlloantibodies in a Patient with AIHAWho Is Transfused Repeatedly
The question frequently arises as to how often a searchfor alloantibodies using adsorption procedures mustbe performed in a patient with AIHA who is beingtransfused repeatedly. As pointed out by Leger andGarratty,53 patients who have autoantibodies shouldreceive the same protection from hemolytic transfusion
TABLE 10-9. SUMMARY OF METHODS USED IN SELECTION OF BLOOD FOR TRANSFUSION TO PATIENTS WITHWARM ANTIBODY AUTOIMMUNE HEMOLYTIC ANEMIA*
A. Patient not recently transfused (within previous 3 months)1. Determine patient’s ABO and Rh phenotype.2. Determine the patient’s extended RBC phenotype (e.g., K, Jka, Jkb, Fya, Fyb, S), if feasible.3. Compare strength of DAT and IAT. If IAT is stronger, the presence of an alloantibody is highly suspected.4. Test patient’s serum against a panel. If an alloantibody causes stronger reactions than the autoantibody, the alloantibody specificity might
be evident.5. Obtain RBCs for autoadsorption tests; save as many RBCs as practical in anticoagulant or in frozen state for use in subsequent warm
autoadsorption tests, should repeated transfusions be required.6. Perform autoadsorptions for detection of alloantibodies.7. If RBCs are not available for the autoadsorption test, perform allogeneic adsorptions for detection of alloantibodies.8. If the IAT is strongly reactive and adsorptions are not possible (lack of time or lack of autologous or allogeneic RBCs), prepare a dilution
of the patient’s serum that reacts about 1+ by IAT and test against a panel.B. Patient recently transfused (within previous 3 months)
1. Pretransfusion RBCs are available for warm autoadsorption test.a) Follow steps 1–5, above (accurate determination of the patient’s RBC phenotype could be difficult or impossible)b) Perform warm autoadsorption for detection of alloantibodies, using pretransfusion RBCs.
2. Pretransfusion RBCs are not available for warm autoadsorption test.a) Follow steps 1–4, above (accurate determination of patient’s RBC phenotype could be difficult or impossible)b) Perform allogeneic adsorptions for detection of alloantibodies or, if extended RBC phenotype of the patient is known, one may use
phenotypically matched RBC units, if available. Using partially matched units (e.g., units matched for Rh and K) will provide only partial safety (see text).
* If a patient has never been transfused or pregnant, it is highly unlikely that clinically significant alloantibodies are present.Testing the patient’s autoantibody for specificity could provide additional benefit (see text).

388 Immune Hemolytic Anemias
reactions as other patients. In particular, the AmericanAssociation of Blood Banks’ Standards indicate that ifa patient has received a transfusion or been pregnantwithin the preceding 3 months, the sample must beobtained from the patient within 3 days of the sche-duled transfusion.87 Indeed, Shulman and colleagues88
have published data indicating that 13 of 60 retrospec-tively studied patients developed newly detectableantibodies within 83 hours of a sample reported to benegative for the new antibody. Thus, after a patientwith autoantibodies receives a transfusion, compati-bility test procedures, including adsorption studies,should be performed on samples obtained within 3 days of subsequent transfusions.
The Use of Phenotypically MatchedRBCs for Transfusion
As the frequent performance of adsorptions is laborintensive, there is a never-ending search for less techni-cally demanding but safe approaches to providingblood for patients with AIHA. Some investigatorssuggest the transfusion of RBCs that are prophylacti-cally antigen matched (PAM) with the patient’s, ratherthan performing adsorption studies to detect and iden-tify alloantibodies.89 Providing phenotypically matchedRBCs can provide a significant measure of safety,90 butsome caveats and precautions should be noted.
Performing an autoadsoption provides protectionagainst the presence of antibodies against high-incidence antigens, whereas providing blood selectedon the basis of the patient’s phenotype or by thealloadsorption technique does not. Therefore, autoad-sorption should be considered a preferable approachwhen feasible.
To provide adequate safety, the patient’s extendedphenotype must be determined (D, C, E, c, e, K, Jka,
Jkb, Fya, Fyb, S, and s antigens), and all donor unitsmust be matched with the patient’s. If the patient’sRBCs can be phenotyped for all of these antigens, andif the blood supplier can provide units that are nega-tive for all of these antigens not present on thepatient’s RBC, this method of selecting blood wouldappear to be about as safe as using an allogeneicadsorption procedure. Although performing anextended phenotype is a labor-intensive and expen-sive procedure, it need be done only once per patient,and the information can be used for all subsequenttransfusions. This might not be a significant advan-tage, however, as data from the Los Angeles RedCross (LARC) Reference Laboratory (unpublished)shows that only 90 of 418 patients (22%) needed morethan the initial set of adsorptions, evidently becausethe patients responded to therapy and repeated trans-fusions were not required. Further, one must keep inmind that even in the most skilled hands, extendedphenotyping of RBCs that have a strongly positivedirect antiglobulin test might not be possible. Indeed,Shirey and coworkers89 could not obtain a reliablephenotype from 40% of their patients, and in thesecases, adsorption procedures were necessary foralloantibody detection and identification.
Data from the LARC Reference Laboratory91 sug-gests that the use of phenotypically matched RBCsprevents most of the alloantibody-induced hemolytictransfusion reactions that potentially would occur inpatients with AIHA. Table 10-10 shows the specificitiesof 202 alloantibodies detected in the sera of 418patients with AIHA. Anti-E was by far the mostcommon alloantibody detected, being twice ascommon as the next most common specificity, anti-K.The next most common group included anti-C, -Fya, -Jka, and anti-c, in that order. A third group of alloanti-bodies—anti-Jkb, -S, -D, -e, “HTLA”, -M, -V, -Jsa, -Cw,
TABLE 10-10. ALLOANTIBODY SPECIFICITIES OF 202 ANTIBODY-CONTAINING SERA FROM 418 AIHA PATIENTS
Specificity* n Percentage Present in Antibody-Containing Sera Percentage Present in Total AIHA Patients
Anti-E 92 46 22-K 45 22 10.8-C 36 18 8.7-Fya 30 15 7.8-Jka 21 10 5.0-c 20 10 4.8-Jkb 19 9.4 4.6-S 17 8.4 4.0-D 14 7 3.4-e 10 5 2.4
“HTLA” 9 4.5 2.2-M 9 4.5 2.2-V 8 4 1.9-Jsa 7 3 1.7-Cw 7 3 1.7-Lea 7 3 1.7-Wra 5 2.5 1.2-s 4 2 1.0-rhi 4 2 1.0
* Other specificities detetected in only 1 or 2 sera included anti-Kpa, -VS, -P1, -Ch, -G, -N, -Dia, -Ce, -KnMca, -U, -Lua, -Lu14, -He, -Xga, -Mit, -Fy5.From Garratty G, Petz LD: Approaches to selecting blood for transfusion to patients with auto-immune hemolytic anemia. Transfusion 2002;42:1390–1392.

Blood Transfusion in Autoimmune Hemolytic Anemias 389
Lea, -Wra, -s, and –rhi—were present in 1% to 10% ofthe alloantibody containing sera. A fourth group ofvarious specificities was associated with only one ortwo of the patients. Approximately 40% of the seracontained alloantibody of only a single specificity; 30%contained two specificities; and 16% contained threespecificities. Approximately 10% of the alloantibody-containing sera contained alloantibodies of four ormore specificities.
Providing PAM RBCs might present a significantproblem for hospitals and smaller blood suppliers.The phenotypes of the 12 patients who received PAMRBCs (listed in Table 2 of Shirey and associates89)range from 0.0002 to 0.09 (mean = 0.04), meaning that51,000–65,000, or a total of 76,300 random unitswould have to be screened to obtain the 149 PAMRBCs that were transfused to these patients. Even ifthe frequency of the rarest of the phenotypes, E–, K–,Fy(a–b–), S– (patient #9, who was probably AfricanAmerican) is removed from the calculation (as thisphenotype could be obtained more easily by screen-ing African Americans), 51–6714, or a total of 11,306random donors would have to be screened to obtainthe 136 PAM RBCs transfused to 11 patients.91
Nevertheless, Lau and colleagues90 have suggestedthat, with the use of a sophisticated computerprogram, it is feasible and cost effective in a rela-tively homogeneous population in Hong Kong toobtain phenotype-matched blood for all patientswithout need for pretransfusion antibody screening.
Partial phenotyping (e.g., for Rh, K and Jka anti-gens) would not provide protection against alloim-munization by antigens of other blood group systemsthat can cause hemolytic transfusion reactions, andtherefore, it would not preclude the necessity of pre-transfusion adsorption studies.71,92,93 Determining thepartial genotype of patients’ RBCs using DNA tech-nology might be helpful in identifying at least someRBC antigens (see the earlier discussion of red cellphenotyping and genotyping).
Whether implementation of this approach is feas-ible and cost effective at many blood centers has notbeen determined. If the intention is to place emphasison providing phenotype-matched units, one mustdetermine that the blood supplier could provide suchunits reliably, and one must recognize that adsorptionstudies will be required in cases in which a patient’sRBCs cannot be phenotyped and/or when the bloodsupplier cannot provide matched units.
COMPATIBILITY TESTING IN COLD-ANTIBODY AIHAs
Cold Agglutinin Syndrome
PERFORMING COMPATIBILITY TESTING AT 37°CUSING SALINE-SUSPENDED RBCs
There are several approaches to compatibility testingfor patients with CAS. One method is to perform the
compatibility test strictly at 37°C and to use onlysaline-suspended RBCs (i.e., without potentiators).Cold agglutinins from only 7% of patients with coldagglutinin syndrome react at 37°C using saline-sus-pended RBCs, although we found positive reactionsin 30% of cases in albumin media.94,95 If positive reac-tions occur at 37°C with saline-suspended RBCs, onemust first suspect faulty technique. If cells and serumare not prewarmed before mixing, if centrifugation isperformed at a temperature lower than 37°C, or if theinitial washes of the cells after incubation do not usesaline at 37°C, reactions can occur within seconds.Even if direct agglutination is not evident, comple-ment might be bound by the antibody reactivity andresult in a positive IAT using polyspecific antiglobu-lin serum (one molecule of IgM antibody might bindseveral hundred molecules of complement). Thisreaction may be circumvented by using anti-IgGantiglobulin serum.
The advantages of this method are that time-consuming autoadsorptions of the patient’s serum arenot necessary and that the method can be used even ifthe patient has recently received a transfusion.
Several disadvantages are also apparent. First, it isobvious that RBC alloantibodies reacting at tempera-tures lower than 37°C will not be detected. Thisfinding is of little consequence, as alloantibodies thatdo not react in vitro at temperatures less than 37°C arerarely, if ever, clinically significant. Indeed, theStandards for Blood Banks and Transfusion Servicesof the American Association of Blood Banks does notrequire a room temperature incubation phase of thecrossmatch but instead states that methods for testingfor unexpected antibodies “shall include 37°C incuba-tion preceding an antiglobulin test using reagentRBCs that are not pooled.”87
It is also true that potentiator-dependent antibodieswill be missed, but here, again, the risk is minimalbecause such antibodies are quite unusual.96 Becausecompatibility testing at 37°C is quicker than othermethods, it can be used even if the patient hasrecently received a transfusion, and because it resultsin a low risk of missing clinically significant allo-antibodies, we believe it is the method of choice.Attention to certain technical details is crucial,however, to be certain that one is truly working strictlyat 37°C.
One must validate that procedures are actuallybeing carried out strictly at 37°C. A heated centrifugeor a centrifuge in a 37°C warm room may be used, acentrifuge may be placed in an incubator, or the tubesmay be placed in centrifuge cups containing warmwater. Samples transferred from a 37°C water bathand centrifuged immediately at room temperaturedrop by approximately 7–8°C after only one minute ofcentrifugation. One must be aware that, if one usessaline at 40–45°C, the temperature will drop by a fewdegrees when it enters a test tube and by a few moredegrees when centrifuging is in progress. A fewsimple experiments are all that is required to deter-mine the appropriate conditions.

390 Immune Hemolytic Anemias
COLD AUTOADSORPTION AND ALLOGENEIC ADSORPTION
An alternative approach is to adsorb the cold autoan-tibody from the patient’s serum before performingthe compatibility test. If facilities are not available towork strictly at 37°C, one or two cold autoadsorp-tions will frequently remove enough of the coldagglutinin so that compatibility tests can be per-formed with less stringent control of the incubationtemperature. It is interesting that cold autoadsorp-tions remove antibody reactive at 30–37°C before allantibody reactive at 4°C is adsorbed, thus makingcompatibility testing feasible without adheringstrictly to 37°C temperatures.
Even if the transfusion service can work strictly at37°C, cold autoadsorptions might be necessary in thesmall percentage of patients whose antibody is reac-tive at 37°C, even in saline. If a patient has a veryhigh-titer cold agglutinin, one should not attempt toremove all of the antibody by adsorption. Doing sowould require multiple adsorptions even whenenzyme-treated RBCs are being used and is not neces-sary. Table 10-11 shows the results of autoadsorbing aserum with a cold-agglutinin titer of 2048 (saline) and8096 (albumin). After three adsorptions for one-halfhour each at 4°C using the patient’s papainized RBCs,the serum still reacted strongly (4+ with undilutedserum) at room temperature (25°C), but it no longerreacted at 37°C.
In recently transfused patients, allogeneic adsorp-tion studies can be performed as for warm-antibodyAIHA. This is rarely necessary if compatibility testsare carried out as described previously.
OTHER METHODS
An alternative approach to compatibility testing is toadsorb the serum with rabbit erythrocyte stroma,which can be used to adsorb anti-I and –IH40 butmight also remove clinically significant alloantibodies(notably anti-B, -D, -E, and others).97
Still another approach to compatibility testing incold agglutinin syndrome is to inactivate the IgM coldagglutinin with 2-mercaptoethanol (2ME) or DTT.98,99
Pirofsky and Rosner100 described the use of DTT ata concentration of 0.01 M in a rapid 15-minute, 37°Cincubation test system. Dialysis was not required.They reported that this procedure caused at least afourfold or greater decrease in IgM antibody titerswithout affecting the activity of IgG antibodies.
Olson and associates101 used DTT in a concentrationof 0.01 M, added equal volumes to test sera, and incu-bated for 30 minutes at 37°C. Thirty sera that con-tained RBC antibodies reactive by the IAT showedvirtually no alteration in activity after DTT treatment,while 20 sera containing cold-reactive RBC antibodiesshowed almost total elimination of activity. However,none of the cold-reactive antibodies tested werepathologic high-titer cold agglutinins from patientswith CAS.
Freedman and colleagues102 reviewed the optimalconditions for the use of sulphydryl compounds indissociating RBC antibodies. They noted that incuba-tion at 37°C with 0.2 M 2ME provided the best con-ditions for inactivating IgM antibodies. Incubationstill failed to inactivate completely the extremelypotent autoanti-I (titer of 1,024,000) that was used,however. False-positive reactions in the IAT usinganti-IgG or anticomplement antiglobulin serum wereobtained consistently when sera that had beentreated with 2ME were not subsequently dialyzed.Although in many cases dialysis for as short as 30 minutes was sufficient, in others overnight dialy-sis was found to be necessary. Incubation of serumwith DTT produced a slower effect than did incuba-tion with 2-mercaptoethanol, and incubation for 2.5 hours was necessary to reduce the anti-I titerfrom 1,024,000 to 1024.
Using either reagent, IgM alloantibodies will, ofcourse, be inactivated in addition to the cold autoag-glutinins. Other disadvantages are that blood banktechnologists are often unfamiliar with the use of suchreagents, and both reagents can inactivate or diminishcomplement activity.
TRANSFUSION OF ADULT-i RBCs
Some investigators have suggested that adult-i RBCsbe used for transfusion of patients with cold agglutinin
TABLE 10-11. ABSORPTION OF COLD AGGLUTININ BY PATIENT’S OWN RBCs AT 4°C
Titer against Adult OI RBCs
4°C 25°C 37°C
Saline Albumin Saline Albumin Saline Albumin
Unadsorbed 2048 8098 1024 8098 0 32Absorbed × 1 1024 2048 256 1024 0 16Absorbed × 2 256 256 128 256 0 8Absorbed × 3 128 128 16 64 0 0

Blood Transfusion in Autoimmune Hemolytic Anemias 391
syndrome who have anti-I autoantibodies. vanLoghem and associates103 studied the survival of I andi RBCs labeled with 51Cr in one patient with chronicCAS. They demonstrated normal survival for the idonor RBCs with greatly shortened survival of both thepatient’s I RBCs and donor I RBCs. Woll and cowork-ers104 reported one patient with transient CAS whoresponded to transfusion of warmed, freeze-thawedadult-i RBCs. These researchers did not test the sur-vival of adult I RBCs, however. Bell and colleagues84
reported unfavorable experiences transfusing twopatients with CAS with adult-i RBCs. Two adult-i unitsgiven to a patient with strong anti-I survived forapproximately the same period of time (i.e., 3 to 4 days)as several adult-I units given subsequently. In a secondpatient with anti-I, no elevation of hematocrit wasnoted after transfusion of two units of adult-i blood.These authors suggested that the minimal I antigenpresent on adult-i RBCs seemed sufficient to renderthem biologically incompatible.
Our own experience indicates that transfusion ofadult-I RBCs to patients with chronic CAS usuallyresults in an appropriate rise in hemoglobin. Unusualpatients might fail to respond to transfusion of adult-IRBCs, but a majority of available data indicate that theuse of adult-i cells is not a solution to the problem. Inpatients with chronic CAS, the repeated use of i RBCsis certainly not feasible because of their extreme rarity.
Paroxysmal Cold Hemoglobinuria
Transfusion of compatible blood for patients withparoxysmal cold hemoglobinuria (PCH) might bepossible if the rare p or Pk cells are available througha rare donor file. Although the routine cross-matchtest could appear to be compatible with other RBCsbecause the antibody reacts only in the cold (usually<15°C), there are some suggestions that p or Pk RBCswill survive better.22,105
Rausen and colleagues22 reported on two childrenwith PCH who were severely anemic. The firstpatient, a 4-year-old boy with blood type A1, wastransfused with two 100-mL aliquots of frozen-thawed RBCs from a compatible type O, Tj(a-) donor5 days after the sudden onset of hemolytic anemia.The blood was administered at room temperature,and the hematocrit level rose from 11% to 19% follow-ing the transfusions. Although the hematocrit hadbeen expected to reach 28%, the authors determinedthat the post-transfusion blood contained fewer than5% type A RBCs and therefore concluded that the lackof an appropriate rise in the hematocrit was becausethe patient’s own cells were rapidly being hemolyzed.Within 2 more days, hemoglobinuria subsided, andthe patient’s hemoglobin rose progressively.
The second child, a 21⁄2-year-old boy with blood typeAB, was treated with intravenously administeredhydrocortisone on the first day of hospitalization, andsubsequently he was transfused with 100 mL of typeAB RBCs that were incompatible with the Donath-
Landsteiner antibody. The hematocrit temporarilyimproved from 13.5% to 20% but decreased over thenext 36 hours to 11.5%. A second incompatible transfu-sion of 130 mL again resulted in a temporary rise inhematocrit to 24.5% but with a drop to 15% over thenext 36 hours. The urine then abruptly became clearand at this point, 100 mL of frozen-thawed RBCs froma compatible type O, Tj(a-) donor were transfusedthrough a warming coil adjusted to 37°C. Followingthis transfusion, the hematocrit rose to 20%, and thepatient’s hemolytic anemia stabilized and then gradu-ally resolved. The authors state that these were the firstrecorded cases of successful compatible transfusiontherapy in PCH. One should note, however, that bothpatients’ hemolysis spontaneously subsided soon afterthe transfusions of compatible blood and that onecannot determine the comparative efficacy of the com-patible and incompatible transfusions from the dataprovided.
Sabio and associates105 reported on a 41⁄2-year-oldgirl with PCH who was transfused twice withABO/Rh (D)-compatible, P+-incompatible RBCs.These transfusions only worsened the patient’s hemo-globinuria without increasing the hemoglobin con-centration significantly. Transfusion with RBC of therare p phenotype was attempted successfully with arise in hemoglobin and amelioration of symptoms.The patient was also treated with 2 mg/kg prednisone“without any effect” following the first transfusions.
Nordhagen and colleagues106 reported on four chil-dren with acute PCH who required transfusion in spiteof aggressive therapy with corticosteroids. One patientreceived three transfusions of P-positive blood duringthe first 3 days of hospitalization. One week later, thepatient became febrile again, with increasing hemolysisand a hemoglobin that dropped from 7.3 to 4.6 g/dL.He was given another transfusion on the 10th day andthe last on the 14th day. The last transfusion consistedof washed, P-negative (pp) erythrocytes, after whichthe patient’s condition stabilized.
Patients are likely to require transfusion beforeRBCs of the p phenotype are available. Generally,transfusion of RBCs of common P types should beprovided, as patients with PCH often have severehemolysis, and waiting for availability of p or Pk RBCis likely to delay a needed transfusion. Successfultransfusion of patients with PCH has been reportedby numerous authors and, almost certainly, the trans-fusions were of P-positive blood.33,106-112
Although there are some reports of Donath-Landsteiner antibodies having other specificities,these are extraordinarily rare (see Chapter 5).
OPTIMAL VOLUME OF BLOOD TO BE TRANSFUSED
The optimal volume of blood to be transfused topatients with AIHA varies with the clinical setting. Inpatients who have severe hemolysis but who might

392 Immune Hemolytic Anemias
require transfusion only temporarily until therapybecomes effective, the transfusion of modest volumesof RBCs just sufficient to maintain a tolerable hema-tocrit level appears advisable. In patients with severeanemia, however, there is a tendency to transfuselarge volumes of blood to restore the hemoglobin andhematocrit to near-normal levels quickly. Thisapproach can lead to tragic consequences.
Indeed, Rosenfield and Jagathambal37 point out thatthe salutary effect of just 100 mL of packed RBCs canbe quite remarkable when given to a patient with car-diopulmonary embarrassment from anemia. Theysuggest that 100 mL may be given as needed (perhapstwice daily, depending on the severity of hemolysis)and that there is generally no need to increase thehemoglobin even to a level of 8 g/dL. The aim of suchtransfusions is to supply just enough RBCs to preventhypoxemia while avoiding dangerous reactionsresulting from overtransfusion.
Complications of Aggressive TransfusionTherapy in Patients with AIHA
VOLUME OVERLOAD
The dangers of overtransfusion among patients withAIHA are several. If the anemia is very severe (hema-tocrit 10–15%, hemoglobin 3.5–5.0 g/dL), and espe-cially if the patient is elderly or if cardiac reservemight be reduced, transfusion can overload the circu-lation easily and precipitate cardiac failure. In slowlydeveloping anemia, total blood will not be as severelyreduced as are hemoglobin and hematocrit values, sothat even modest volumes of transfused RBCs willresult in hypervolemia. Not only should the totalvolume that is transfused be kept modest but RBCsshould also be administered slowly, the total volumetransfused not exceeding 1 mL/kg/hour. One mustlook for evidence of congestive heart failure duringand following the transfusion—particularly elevatedvenous pressure and the presence of rales on auscul-tation of the chest. Cardiac failure after the adminis-tration of as little as 200 mL of RBCs can develop upto 6 to 12 hours later and can be fatal. Althoughdiuretics are of value and probably should be given topatients with diminished cardiac reserve, responsesvary, and their administration must not replace closeclinical observation of the patient.
POST-TRANSFUSION HEMOGLOBINEMIA,HEMOGLOBINURIA, AND DISSEMINATEDINTRAVASCULAR COAGULATION
An additional danger for patients with AIHA relatesto the fact that the kinetics of RBC destruction alwaysdescribe an exponential curve of decay, indicating thatthe number of cells removed in a unit of time is a per-centage of the number of cells present at the start ofthis time interval.37 Thus, the more cells present atzero time, the greater the absolute number of RBCsthat will be destroyed in the unit time span. Indeed,
Chaplin113 indicates that the most common cause ofpost-transfusion hemoglobinuria in AIHA might notbe alloantibody-induced hemolysis but rather thequantitative effect of transfusion in increasing theRBC mass subjected to ongoing autoantibody-mediated destruction. Such marked post-transfusionhemoglobinemia and hemoglobinuria have the poten-tial for a significant degree of associated morbidityand possibly, mortality. Indeed, Gürgey and cowork-ers114 pointed out that two children who were treatedwith exchange transfusions died of profound hemoly-sis shortly after the procedure (although Heidemannand colleagues115 reported successful exchange trans-fusion in one patient).
Patients undergoing severe post-transfusion intra-vascular hemolysis can develop disseminated intravas-cular coagulation (DIC), possibly as a result ofprocoagulant substances present in RBC lysates.36,116
These potential problems emphasize the need forrestraint in the volume of blood transfused per trans-fusion episode to patients with AIHA.
CASE SUMMARIES
An example of such a complication of transfusiontherapy was reported by Bilgrami and associates.116
They described a patient who was infected withhuman immunodeficiency virus (HIV) who hadsevere AIHA. His hemoglobin was 2.9 g/dL; hema-tocrit, 8%; corrected reticulocyte count, 1.2%; whitecell count, 12,500/μL; platelet count, 101,000/μL;total bilirubin, 3 mg/dL; direct bilirubin, 0.7 mg/dL;lactate dehydrogenase, 1902 U/L; prothrombin time, 11.8 seconds (normal 11–13 seconds); andpartial thromboplastin time 20.8 seconds (normal,25–35 seconds). The urine was grossly red but withno intact RBCs. The peripheral smear demonstratedspherocytes, polychromasia, and nucleated RBCs.The DAT was positive using polyspecific AGS, anti-IgG, and anti-C3. “Least incompatible” (w+ to 2+)units were selected for transfusion using differen-tially adsorbed sera for cross-matching. Before trans-fusion, immune complexes were detected in theserum by several techniques.
The patient underwent aggressive transfusion,receiving 8 units of packed RBCs over the course of 24hours, as shown in Figure 10-2. The patient was trans-fused to a hematocrit level of greater than 25%. Signs ofDIC developed, however, with the platelet countdemonstrating a progressive decline and the prothrom-bin time and partial thromboplastin times showing anupward trend within 24 hours. One-half hour before thepatient’s death, the following laboratory results wereobtained: prothrombin time, 16.8 seconds; partialthromboplastin time, 81 seconds; serum fibrinogen, 130mg/dL (normal, 150–400 mg/dL); thrombin time, 45seconds (control, 16.5 seconds); fibrin degradationproducts titer, greater than 40 mg/mL; and D-dimer,greater than 1 μg/mL. A diagnosis of DIC was made.The patient became hypotensive shortly thereafter andcould not be resuscitated.

Blood Transfusion in Autoimmune Hemolytic Anemias 393
The autopsy demonstrated widespread multiplepulmonary thrombi. There was widespread thrombo-sis of small arterioles of both lungs. Some of thethrombi had begun to organize and others were veryacute, a presentation most consistent with the forma-tion of thrombi in situ rather than secondary to throm-boembolic disease. The extensive pulmonary thrombiresulted in acute right ventricular failure, which wasthe immediate cause of death. The authors pointedout that less aggressive transfusion therapy wouldhave sufficed to meet the patient’s tissue oxygenneeds and concluded that the most likely etiology ofthe patient’s DIC was the aggressive transfusiontherapy. They concluded that their case illustrates theneed to consider the possibility of serious transfusioncomplications for patients with AIHA (even whenalloantibodies have been excluded) and underscoresthe value of the judicious use of transfusion forspecific indications in this group of patients.5
Additional examples of unfavorable outcomes oftransfusion are indicated in the following two casesummaries (Patient 1, Patient 2), which were suppliedby Dr. Hugh Chaplin, Jr (Chaplin H Jr, personalcommunication).
P AT I E N T 1 : A 34-year-old white gravida-1, para-1,with relapsing primary autoimmune hemolytic anemia for4 months, was admitted to the hospital with a hemoglo-bin level of 5.0 g/dL; reticulocytes of 16%; DAT stronglypositive for C3d, moderately positive for IgM, and nega-tive for IgG; and all crossmatches deemed “incompati-ble.” Despite high-dose therapy with corticosteroids, she
required 1 to 2 units of packed RBCs daily to maintain herhemoglobin level at 4.5 to 6.0 g/dL. She experiencedincreasingly severe hemoglobinemia and hemoglobinuriaassociated with transfusions, clearing within a few hours.No alloantibodies were demonstrable. On the 10th hos-pital day, a splenectomy was performed without benefit.On the 12th hospital day, several hours following a trans-fusion, she developed acute respiratory distress followedby cardiopulmonary arrest, which did not respond toresuscitative measures. Autopsy revealed a single largepara-aortic lymph node diagnosed as plasmacytoidmalignant lymphoma; death was attributed to multiplefresh small pulmonary emboli.
P AT I E N T 2 : A 56-year-old white female, never previ-ously pregnant or transfused, was semistuporous at thetime of admission to the hospital. She had a hemoglobinlevel of 1.6 g/dL; hematocrit level 6.2%; reticulocytes19%; DAT strongly positive for C3d, moderately positivefor IgG, and weakly positive for IgM; and all crossmatches“incompatible.” She was given corticosteroids and 3 unitsof packed group O, Rh-negative RBCs and developedfever and striking hemoglobinemia and hemoglobinuria,which improved over the ensuing 3 hours. Her state ofconsciousness improved, and the hemoglobin level rosetransiently to 5.7 g/dL but was declining rapidly whenshe developed severe respiratory distress followed by car-diopulmonary arrest, which did not respond to resuscita-tion. At autopsy, no underlying cause for the AIHA wasfound; death was attributed to multiple fresh small pul-monary emboli.
Hours
Pla
tele
t cou
nt(×
109 /
L)P
T (
seco
nds)
Hem
atoc
rit (
%)
PT
T (
seco
nds)
Transferred to UCHC
Steroids
FFP TxPlatelet TxPRBC TxIVIG
20
10
0
20
30
80
100
10
15
20
00 24 48 72 96 120
80
40
200
160
120
FIGURE 10-2. Clinical course of AIHA andDIC in a patient with HIV infection PT, pro-thrombin time; PTT, partial thromboplastintime; PRBC, packed red blood cell; FFP, fresh-frozen plasma; Tx, transfusion;UCHC, University of Connecticut HealthCenter. (From Bilgrami S, Cable R, PisciottoP, Rowland F, Greenberg B: Fatal dissemi-nated intravascular coagulation andpulmonary thrombosis following bloodtransfusion in a patient with severeautoimmune hemolytic anemia and humanimmunodeficiency virus infection.Transfusion 1994;34:248–252.)

394 Immune Hemolytic Anemias
Saif and coworkers117 reported a complication oftransfusion in a patient with HIV-associated AIHA.Following transfusion of 1 unit of RBCs, the patientdeveloped a pulmonary embolism. The authors citedtwo other reports of thromboembolism in patientswith HIV-associated AIHA118,119 and also cited thecase of Bilgrami and associates (reviewed previously),although the latter case described DIC rather thanthromboembolism.
These complications of transfusion patients withAIHA are not common, as emphasized by Salama andassociates,27 who found no instances of a definiteincrease in signs of hemolysis among 53 patients withAIHA who received blood transfusions. Nevertheless,for patients with AIHA, RBCs must be transfused cau-tiously and for appropriate indications.5
IN VIVO COMPATIBILITY TESTING
In vivo compatibility testing has been advocated bysome and is based on testing the survival of an aliquotof RBCs from a unit that has been selected for transfu-sion.56,120 Although such tests are potentially of valuein determining the clinical significance of somealloantibodies in patients without AIHA, we feel thatsuch studies are of limited value for patients withAIHA and should never be considered a substitute formeticulous serologic evaluation and detailed compat-ibility testing. This is particularly true because theoriginal use of in vivo survival studies in patientswith AIHA occurred at a time when less effectivemethods were available for the detection of RBCalloantibodies in such patients. Using the moderncompatibility tests described previously, little is to begained from in vivo survival studies.
Some investigators have measured the survival ofan aliquot of RBCS using 51Cr-tagged cells.120,121 Inthis procedure, 0.5 to 1 mL of RBCs from a donor unitare labeled with 51Cr. If the amount of radioactivity inthe plasma, both at 10 and 60 minutes, does notexceed 5% of the radioactivity injected, and if RBCsurvival at 60 minutes is not less than 70%, the expec-tation was that donor RBCs could be transfused withminimum hazard.71,121 The potential value of thisprocedure according to available data is that anacceptable result in an in vivo compatibility test seemsto preclude the possibility of an immediate sympto-matic hemolytic reaction when cells from the wholeunit subsequently are transfused.120-122 If the in vivotest is performed after detailed compatibility testingusing modern techniques, however, and if it demon-strates short survival of the test cells, it is difficult tounderstand what should be done next to select a unitof RBC different from the one used for the in vivo test.
Indeed, Meyer and colleagues123 presented data on11 patients with AIHA who had an in vivo survival of51Cr-tagged donor red blood cells of less than 70% in1 hour but who nevertheless required transfusion.Only one of these patients had a complication directly
attributable to the transfusion.123 Also, Mollison124
points out that the survival of a small volume ofincompatible RBCs might be different from the sur-vival of a larger volume of the same RBCs. Data arenot available to determine the rate of destruction of atest dose of RBCs that would predict an acute symp-tomatic hemolytic reaction.
Also, the results of an in vivo compatibility testcould impart a false sense of security, as only a smallpercentage of transfused RBCs might survive in the 16to 24 hours following acceptable results in an in vivosurvival study.120,125
For example, Silvergleid and coworkers120 des-cribed patients with WAIHA who had adequate 1-hour RBC survival of a test dose of RBCs and whodid not evidence an acute transfusion reaction, butwho had short survival of the transfused RBCs insubsequent hours. One such patient had a pretrans-fusion hematocrit level of 10.5%, a post-transfusionhematocrit level of 20.6%, but a hematocrit level ofonly 10% just 16 hours after transfusion. Anotherpatient with PCH had a 1-hour survival of Tj (a+)RBCs of 87%, but only 53% of the radiolabeled cellssurvived to 48 hours after transfusion. Still anotherpatient with an alloantibody (anti-Jkb) had 94% sur-vival of tagged cells at 1 hour but only 10% survivalat 24 hours after transfusion. Similar data werereported by Peters and associates,125 who described apatient with anti-Lub; survival of radiolabeledLu(b+) RBCs was 84.4% at 1 hour but only 48% at 5 hours and 8.5% at 24 hours after transfusion.
At the present time, in vivo compatibility testsusing radiolabeled RBC seem to be rarely, if ever, per-formed in clinical services on patients with AIHA.
An alternative method for determining in vivosurvival of transfused RBCs in a patient with AIHAis to infuse over a period of 20–30 minutes an aliquotcontaining 20–30 mL of RBCs from the unit to betransfused. The patient is observed for symptoms ofa hemolytic transfusion reaction, and a blood sampleis obtained after the infusion of the “test dose” tolook for hemoglobinemia (and urine, if available, isobserved for hemoglobinuria). The intravascularlysis of as little as 5 mL of RBCs will raise the plasmahemoglobin concentration of an adult by about 50 mg/100 mL, an amount easily detected by visualinspection.113 One merely needs to obtain an antico-agulated specimen of blood, centrifuge it, and visu-ally compare it to the plasma obtained prior to theinfusion. Absence of hemoglobinemia and hemoglo-binuria suggests that an acute hemolytic transfusionreaction will not occur with infusion of the entireunit of blood.
One benefit of this technique is that the test requiresevaluation of the patient’s status during the earlyphase of a transfusion. Close observation of thepatient is critical, although it obviously should becarried out in any case. As a modification of this pro-cedure, one can merely transfuse slowly until theequivalent of about 20–30 mL of RBCs have been

Blood Transfusion in Autoimmune Hemolytic Anemias 395
infused, and then obtain a blood sample for visualinspection of the plasma. One need not stop the trans-fusion if the patient remains asymptomatic.
An acute hemolytic transfusion serious enough tocause immediate hemoglobinemia is not likely tooccur except as a result of ABO incompatibility. Thus,little information, if any, is provided about the pres-ence of other alloantibodies that have the potential tocause a hemolytic transfusion reaction. Even if noimmediate adverse effects are noted, the survival ofthe full unit is not likely to be better than that of thepatient’s own RBCs.
More important, if a careful serologic study has beendone using the techniques and principles alreadydescribed to select the best possible blood for transfu-sion, and if an in vivo test nevertheless demonstrates avery short RBC survival, there is no logical way toselect an alternative unit. Certainly, a patient shouldnever be denied a needed transfusion because labora-tory data (whether from a compatibility test or from anRBC survival study) suggest that the transfused bloodwill not survive well. If the patient requires transfusion,such incompatible blood must still be given in the hopeof obtaining temporary benefit.
In conclusion, we feel that the significance of in vivosurvival studies with respect to transfusion of patientswith AIHA has been overemphasized.
THE USE OF WARM BLOOD FORPATIENTS WITH COLD AGGLUTININSYNDROME AND PAROXYSMAL COLD HEMOGLOBINURIA
Eminent authorities offer sharply differing opinionsconcerning the need for warm blood when transfu-sing patients with CAS. Dacie33 states that properlycrossmatched blood can probably be transfused withsafety if run in at a slow drip rate, in which case thereis probably no need to attempt to warm it above room temperature. By contrast, Rosenfield andJagathambol37 state that patients with cold agglutinindisease must receive warmed blood. Mollison andcolleagues71 state that blood should be warmed beforetransfusion to patients with cold agglutinin syn-drome, and they also recommend that the patient bekept warm. Wallace126 comments that hemolytic reac-tions are unlikely, provided that the donor blood iswarmed to body temperature and the recipient is keptwarm. As is evident, the question has not beenstudied in much depth, and no RBC survival studiesare available comparing survival of blood transfusedat various temperatures.
With regard to PCH, Rausen22 does report that evencompatible Tj(a-) blood needs to be warmed to 37°Cbefore transfusion. Wallace126 states that transfusion ofRBCs of the common P groups is unlikely to precipitatean acute hemolytic transfusion reaction in PCH pro-vided that the blood is warmed to 37°C and the patient
is maintained at a warm temperature. Johnsen andcoworkers107 reported the results of transfusion of 150 mL of prewarmed, packed RBCs (P-positive) to an18-month-old boy with PCH. The transfusion was fol-lowed by a temperature rise and passage of red-coloredurine. The hemoglobin improved from 4.7 g/dL to 12.4 g/dL and remained at that level.
In the absence of extensive data, logic must prevail.Our experience in CAS has been consistent withDacie’s view, although in some instances we haveempirically used an in-line blood warmer for seriouslyill patients. The use of an in-line blood warmer wouldappear indicated if the patient has either severe PCH orflorid CAS. It is also logical to keep the patient warm,even if the efficacy of such a maneuver has not beenproven.
If blood is to be warmed, it must be done properly.Unmonitored or uncontrolled heating of blood isextremely dangerous and should not be attempted.RBCs heated too much are rapidly destroyed in vivoand can be lethal.37 Very efficient in-line bloodwarmers are available that are simple, efficient, andsafe to use. Guidelines for the use of blood warmingdevices have been published.127
THE USE OF RBC SUBSTITUTES
Considerable progress has been made in the develop-ment of RBC substitutes, and the availability of O2-carrying therapeutic agents for clinical use couldaffect the practice of transfusion medicine.25,26,128-132
Mullon and associates26 described the use of a poly-merized bovine hemoglobin in a patient with severeAIHA. The patient had life-threatening AIHA thatwas refractory to treatment with high doses of gluco-corticoids, plasmapheresis, splenectomy, and intra-venous immune globulin. To maintain a hematocritgreater than 12% and a hemoglobin level greater than4.0 g/dL, as many as 8 units of RBC per day wereneeded; she received a total of 53 units of RBCs beforeinitiation of therapy with the hemoglobin solution.During RBC transfusions, the patient developedsymptoms attributed to acute hemolysis, includingfever, nausea, and back pain. Ischemic changes werepresent in the electrocardiogram when the hemoglo-bin was at a level of about 4.0 g/dL.
A total of 11 units of a sterile solution of gluteralde-hyde-polymerized bovine hemoglobin were trans-fused over a 7-day period. Five units wereadministered in response to clinical evidence ofischemia, three as part of volume resuscitation duringan episode of septic shock, and three to maintain thetotal hemoglobin level above 4 g/dL. This therapyresulted in relief of ischemia, and no clinically impor-tant adverse hemodynamic responses occurred. Shereceived further treatment for her AIHA withcyclophosphamide and developed profound neutro-penia, gram-negative septic shock, and gram-negativepelvic osteomyelitis. Subsequent immunosuppressive

396 Immune Hemolytic Anemias
therapy with cyclosporine led to sustained improve-ment in her AIHA, transfusions were no longer neces-sary, and 8 months after discharge the patient waswell, with a hematocrit consistently greater than 35%.
There are indications that cell-free hemoglobin sub-stances might support bacterial virulence by offeringa ready supply of iron, thus sustaining bacterial repli-cation and inhibiting neutrophil function.133,134 In thecase of this patient, however, it is unclear what rolethe hemoglobin solution might have had in promot-ing infectious complications, given her neutropeniaand preexisting AIHA.
Raff and colleagues128 reported a 40-year-old allo-immunized woman with sickle cell anemia who under-went hip replacement surgery. Periopertively, shereceived 4 units of matched frozen RBCs. Seven dayspostoperatively, however, she was readmitted withgeneralized pain, fever, dyspnea, and positive bloodand urine cultures. Hemoglobin decreased to 2.8 g/dL, with no improvement after transfusion of 5matched units, findings suggestive of the sickle cellhemolytic transfusion reaction syndrome (see Chapter14). She was treated with antibiotics, IVIG, corticos-teroids, erythropoietin, and iron. In addition, shereceived five daily 1-unit transfusions of PolyHeme, apolymerized human hemoglobin. Pain and dyspneaimproved markedly, and she was discharged 10 daysafter the start of treatment with a hemoglobin level of7.8 g/dL. The authors commented that the multipletherapeutic interventions make it difficult to assess thecontribution of the hemoglobin solution. Nevertheless,they suggested that hemoglobin-based oxygen carrierscould be a valuable contribution to treatment “in thesecases that are every blood banker’s worst nightmare.”
Other reviews have been published of the use ofartificial oxygen carriers, primarily in the setting ofacute blood loss.129-132 Such reports are generallyenthusiastic, although Tremper,131 whose editorialregarding perfluorochemical compounds bears thesubtitle, “The continued search for an indication,”submits a note of caution. Nevetheless, he remainshopeful that the broader utility of such compoundsmight be proven.
USE OF LEUKOCYTE-REDUCED RBCs
Some investigators recommend using leukocyte-reduced RBCs for patients with AIHA to avoid afebrile nonhemolytic transfusion reaction, whichwould confound an evaluation of a possible hemolyticreaction. The interpretation of a febrile reaction in aseriously ill patient with AlHA is difficult and couldlead to unnecessary cessation or delay of transfusion.These reactions could be reduced in incidence by theuse of leukocyte-reduced RBCs. Such a situation pro-vides a justification for their use in AIHA, as the com-patibility test procedures could be labor intensive andtime consuming. Thus, unnecessary cessation of thetransfusion is more costly because of the additional
technical procedures, and there could be a longerdelay in selecting an alternative unit.
USE OF WASHED RBCs
Previously, washed RBCs have been used to reducethe incidence of febrile nonhemolytic transfusionreactions for the same reason indicated for the use ofleukocyte-reduced RBCs. Washed RBCs have alsobeen suggested as possibly being of benefit topatients with AIHA because they are free of comple-ment components that will be in any plasma-containing blood product. The data supporting thisjustification for the washed RBCs is inconclusive,however, and we do not recommend washed RBCsbased on this rationale.
The recommendation for the use of washed RBCsfor transfusion of patients with AIHA is largelybased on the data of Evans and coworkers,35,135 whoreported their experience using packed RBCs orwashed RBCs in transfusing one patient with CAS.The cold antibody agglutinated RBCs to a titer of500,000 at 4°C and caused lysis of normal RBCs bothat room temperature and at 37°C (maximal at roomtemperature). A transfusion of 2 units of packedRBCs was given without subjective reaction,although hemoglobinuria occurred following com-pletion of the transfusion. A subsequent transfusionof 3 units of washed RBCs was given without rise inplasma hemoglobin. The patient’s serum comple-ment was “always low.” Although the data are farfrom conclusive, the authors speculated that thesmall amount of plasma present in the first transfu-sion of RBCs provided the necessary complement forthe hemolysis that followed.
Further studies by Evans and associates35 indicatedthat transfusion of large volumes of RBCs to patientswith CAS caused a lowering of serum complement.51Cr-labeled normal RBCs survived longer after RBCtransfusions than before, and the authors suggestedthat the reduction in serum complement levels mighthave been responsible for the improved survival.
The phenomenon reported by Evans requires moredata for documentation. Serum complement is ordi-narily not reduced in patients with warm- or cold-antibody AIHA, and we would not recommend theuse of washed RBCs based on this rationale because ofthe limited information available.
AUTOLOGOUS BLOOD TRANSFUSION IN AIHA
Three brief reports have suggested the use of autolo-gous RBCs for transfusion of patients with AIHA.Goldfinger and colleagues136 demonstrated that auto-logous frozen-stored RBCs could be practical for somepatients with AIHA. In one patient with IgM-mediated AIHA, normal in vivo recovery was demon-

Blood Transfusion in Autoimmune Hemolytic Anemias 397
strated, although in vitro RBC loss was 40%. Inpatients who had positive DATs but not hemolyticanemia, in vitro RBC loss was only 2% to 14%, and invivo recovery and survival were normal. StoringRBCs in the frozen state may be considered forpatients who go into remission while on therapy forAIHA. In the event of later relapse, the RBCs may betransfused without fear of alloantibody-inducedhemolysis. Because of autoantibody in the patient’sserum, however, RBC survival is not likely to be betterthan that of an allogeneic unit.
Parr and Ballard137 reported on a patient withmethyldopa-induced positive DAT and IAT whorequired surgery. The patient had equivocal evidenceof hemolysis, consisting of an elevated LDH with anormal hemoglobin and hematocrit. The patient’sserum antibody reacted with all normal RBCs tested.Rather than wait for a fall in the autoantibody titer fol-lowing cessation of the drug, 3 units of autologousblood were stored in the liquid state and used duringsurgery. A similar approach was used by Snyder andSpivack138 for two patients. Although evidence indi-cates that drug-induced autoantibodies will not causeshortened survival of homologous blood if thepatient’s own RBC survival is normal, the use ofautologous blood ensures that no alloantibody-induced transfusion reaction will occur. In instancesin which it is inconvenient or impossible to delaysurgery until an adequate number of autologous unitsare collected, the warm autoadsorption technique orother serologic methods as described previously forpatients with warm-antibody AIHA may be used toexclude the presence of alloantibody.
R E F E R E N C E S
1. Petz LD, Garratty G: Acquired Immune Hemolytic Anemias,1st ed. New York: Churchill Livingstone, 1980.
2. Petz LD: Red cell transfusion problems in immunohemato-logic disease. Annu Rev Med 1982;33:355–361.
3. Petz LD: Blood transfusion in hemolytic anemias. Immuno-hematology 1999;15:15–23.
4. Petz LD: Blood transfusion in acquired hemolytic anemia. InPetz LD, Swisher SN, Kleinman S, Spence RK, Strauss RG(eds): Clinical Practice of Transfusion Medicine, 3rd ed. NewYork: Churchill Livingstone, 1996:469–499.
5. Garratty G, Petz LD: Transfusing patients with autoimmunehaemolytic anaemia. Lancet 1993;341:1220.
6. Petz LD: Transfusing the patient with autoimmune hemolyticanemia. Clin Lab Med 1982;2:193–210.
7. Jefferies LC: Transfusion therapy in autoimmune hemolyticanemia. Hematol Oncol Clin North Am 1994;8:1087–1104.
8. Conley CL, Lippman SM, Ness P: Autoimmune hemolyticanemia with reticulocytopenia: A medical emergency. JAMA1980;244:1688–1690.
9. Conley CL, Lippman SM, Ness PM, Petz LD, Branch DR,Gallagher MT: Autoimmune hemolytic anemia with reticulo-cytopenia and erythroid marrow. N Engl J Med 1982;306:281–286.
10. Crosby WH, Rappaport H: Reticulocytopenia in autoimmunehemolytic anemia. Blood 1956;11:929–936.
11. Liesveld JL, Rowe JM, Lichtman MA: Variability of the ery-thropoietic response in autoimmune hemolytic anemia:Analysis of 109 cases. Blood 1987;69:820–826.
12. Hauke G, Fauser AA, Weber S, Maas D: Reticulocytopenia insevere autoimmune hemolytic anemia (AIHA) of the warmantibody type. Blut 1983;46:321–327.
13. Carapella de Luco E, Stegagno M, Morino G, Ballati G,Lorenzini F: Prolonged reticulocytopenia and transient ery-throid hypoplasia in a child with autoimmune haemolyticanaemia. Haematologica 1984;69:315–320.
14. Greenberg J, Curtis-Cohen M, Gill FM, Cohen A: Prolongedreticulocytopenia in autoimmune hemolytic anemia of child-hood. J Pediatr 1980;97:784–786.
15. Cazzola M, Barosi G, Ascari E: Cold haemagglutinin diseasewith severe anaemia, reticulocytopenia and erythroid bonemarrow. Scand J Haematol 1983;30:25–29.
16. Brown KE: Haematological consequences of parvovirus B19infection. Baillieres Best Pract Res Clin Haematol2000;13:245–259.
17. Bertrand Y, Lefrere JJ, Leverger G, et al: Autoimmune hae-molytic anaemia revealed by human parvovirus linkederythroblastopenia. Lancet 1985;ii:382–383.
18. Chitnavis VN, Patou G, Makar YF, Kendra JR: B19 parvovirusinduced red cell aplasia complicating acute cold antibodymediated haemolytic anaemia. Br J Haematol 1990;76:433–434.
19. Mangan KF, Besa EC, Shadduck RK, Tedrow H, Ray PK:Demonstration of two distinct antibodies in autoimmunehemolytic anemia with reticulocytopenia and red cell aplasia.Exp Hematol 1984;12:788–793.
20. Meyer RJ, Hoffman R, Zanjani ED: Autoimmune hemolyticanemia and periodic pure red cell aplasia in systemic lupuserythematosus. Am J Med 1978;65:342–345.
21. Todd D: Diagnosis of haemolytic states. Clinics Haematol1975;4:63–81.
22. Rausen AR, LeVine R, Hsu TC, Rosenfield RE: Compatibletransfusion therapy for paroxysmal cold hemoglobinuria.Pediatrics 1975;55:275–278.
23. Swisher SN, Petz LD: Transfusion therapy for chronic anemicstates. In Petz LD, Swisher SN, Kleinman S, Spence RK,Strauss RG (eds): Clinical Practice of Transfusion Medicine,3rd ed. New York: Churchill Livingstone, 1996:451–467.
24. Hillman RS: Blood-loss anemia. Postgrad Med 1978;64:88–94.25. Klein HG: The prospects for red-cell substitutes. N Engl J Med
2000;342:1666–1668.26. Mullon J, Giacoppe G, Clagett C, McCune D, Dillard T:
Transfusions of polymerized bovine hemoglobin in a patientwith severe autoimmune hemolytic anemia. N Engl J Med2000;342:1638–1643.
27. Salama A, Berghofer H, Mueller-Eckhardt C: Red blood celltransfusion in warm-type autoimmune haemolytic anaemia.Lancet 1992;340:1515–1517.
28. Sokol RJ, Hewitt S, Booker DJ, Morris BM: Patients with redcell autoantibodies: Selection of blood for transfusion. ClinLab Haematol 1988;10:257–264.
29. Habibi B, Homberg JC, Schaison G, Salmon C: Autoimmunehemolytic anemia in children: A review of 80 cases. Am J Med1974;56:61–69.
30. Pirofsky B: Autoimmunization and the AutoimmuneHemolytic Anemias. Baltimore: Williams & Wilkins, 1969.
31. Pirofsky B, Bardana EJ Jr: Autoimmune hemolytic anemia. II.Therapeutic aspects. Ser Haematol 1974;7:376–385.
32. Audet AM, Popovsky MA, Andrzejewski C: Current transfu-sion practices in orthopedic surgery patients: A multi-institutional study [abstract]. Blood 1995;86(Suppl.):853a.
33. Dacie JV: Autoimmune Haemolytic Anaemias (AIHA):Treatment. In The Haemolytic Anaemias, 3rd ed. vol. 3, TheAuto-Immune Haemolytic Anaemias. New York: ChurchillLivingstone, 1992:452–520.
34. Masouredis SP, Chaplin H: Transfusion Management ofautoimmune hemolytic anemia. In Chaplin H (ed): ImmuneHemolytic Anemias. New York: Churchill Livingstone,1985:177–205.
35. Evans RS, Turner E, Bingham M, Woods R: Chronic hemolyticanemia due to cold agglutinins. II. The role of C’ in red celldestruction. J Clin Invest 1968;47:691–701.

398 Immune Hemolytic Anemias
36. Haemolytic Transfusion Reactions. In Mollison PL, EngelfrietCP, Contreras M (eds): Blood Transfusion in ClinicalMedicine, 10th ed. Oxford: Blackwell Science, 1997:358–389.
37. Rosenfield RE, Jagathambal: Transfusion therapy for autoim-mune hemolytic anemia. Semin Hematol 1976;13:311–321.
38. Edwards JM, Moulds JJ, Judd WJ: Chloroquine dissociation ofantigen-antibody complexes: A new technique for typing redblood cells with a positive direct antiglobulin test. Transfusion1982;22:59–61.
39. Branch DR, Hian AL, Carlson F, Maslow WC, Petz LD:Erythrocyte age-fractionation using a Percoll-Renografindensity gradient: Application to autologous red cell antigendeterminations in recently transfused patients. Am J ClinPathol 1983;80:453–458.
40. Brecher M (ed): Technical Manual, 14th ed. Bethesda, MD:American Association of Blood Banks, 2002.
41. Reid ME, Toy PT: Simplified method for recovery of autolo-gous red blood cells from transfused patients. Am J ClinPathol 1983;79:364–366.
42. Vengelen-Tyler V, Gonzales B: Reticulocyte rich RBCs willgive weak reactions with many blood typing antisera[abstract]. Transfusion 1985;25:476.
43. Wenk RE, Chiafari PA: DNA typing of recipient blood aftermassive transfusion. 1997;37:1108–1110.
44. Reid ME, Rios M, Powell VI, Charles-Pierre D, Malavade V:DNA from blood samples can be used to genotype patientswho have recently received a transfusion. Transfusion2000;40:48–53.
45. Castilho L, Rios M, Pellegrino J, Rodrigues A, Costa FF: Bloodgroup genotyping for the management of patients with“warm” antibody-induced hemolytic anemia (WAIHA)[abstract]. Blood 2001;98:62a.
46. Branch DR, Petz LD: Detecting alloantibodies in patients withautoantibodies. Transfusion 1999;39:6–10.
47. Morel PA, Bergen MO, Frank BA: A simple method for thedetection of allo-antibody in the presence of warm autoanti-body [abstract]. Transfusion 1978;18:388.
48. Branch DR, Petz LD: A new reagent ZZAP having multipleapplications in immunohematology. Am J Clin Pathol1982;78:161–167.
49. Wallhermfechtel MA, Pohl BA, Chaplin H: Alloimmunizationin patients with warm autoantibodies: A retrospective studyemploying three donor alloabsorptions to aid in antibodydetection. Transfusion 1984;24:482–485.
50. Laine ML, Beattie KM: Frequency of alloantibodies accompa-nying autoantibodies. Transfusion 1985;25:545–546.
51. James P, Rowe GP, Tozzo GG: Elucidation of alloantibodies inautoimmune haemolytic anaemia. Vox Sang 1988;54:167–171.
52. Issitt PD, Combs MR, Bumgarner DJ, Allen J, Kirkland A,Melroy-Carawan H: Studies of antibodies in the sera ofpatients who have made red cell autoantibodies. Transfusion1996;36:481–486.
53. Leger RM, Garratty G: Evaluation of methods for detectingalloantibodies underlying warm autoantibodies. Transfusion1999;39:11–16.
54. So CC, Wong KF, Yu PH, Kwan AM, Lee AW: Alloimmunizationin Chinese with warm autoimmune haemolytic anaemia–Incidence and characteristics. Transfus Med 2000;10:141–143.
55. Oyen R, Angeles ML: A simple screening method to evaluatethe presence of alloantibodies with concomitant warmautoantibodies. Immunohem 1995;11:85–87.
56. Dorner IM, Parker CW, Chaplin H Jr: Autoagglutinationdeveloping in a patient with acute renal failure: Character-ization of the autoagglutinin and its relation to transfusiontherapy. Br J Haematol 1968;14:383–394.
57. Liew YW, Duncan N: Polyethylene glycol in autoadsorption ofserum for detection of alloantibodies. Transfusion 1995;35:713.
58. Liew YW, Duncan N: Autoadsorptions for the detection ofalloantibodies—Should polyethylene glycol be used? Trans-fusion 1996;36:384.
59. Cheng CK, Wong ML, Lee AW: PEG adsorption of autoanti-bodies and detection of alloantibodies in warm autoimmunehemolytic anemia. Transfusion 2001;41:13–17.
60. Champagne K, Moulds MK: Autoadsorptions for the detec-tion of alloantibodies—Should polyethylene glycol be used?Transfusion 1996;36:384.
61. Miller R, Unger P, Shapiro A: Rapid adsorption of warmautoantibodies using polyethylene glycol [abstract]. Trans-fusion 1996;36(Suppl.):20S.
62. Hernandez-Jorda M, Zamora C, Duarte R, et al: Polyethyleneglycol (PeG) in microadsorption procredures to detect red cellalloantibodies in the presence of autoantibodies. TransfusMed 1998;8:278.
63. Barron CL, Brown MB: The use of polyethylene glycol (PEG)to enhance the adsorption of autoantibodies. Immumno-hematology 1997;13:119–122.
64. Judd WJ, Dake L: PEG adsorption of autoantibodies csauseloss of concomitant allo-antibody. Immunohematology2002;17:82–85.
65. Overbeeke MAM, Porcelijn L: The detection of alloantibodiesagainst red cells in patients with warm-type autoimmunehaemolytic anaemia. International Forum. Vox Sang 2000;78:203–204.
66. Combs MR, Eveland D, Jewett-Keefe B, Telen MJ: The use ofPolyethylene Glycol in adsorptions: More evidence that anti-bodies may be missed. Transfusion 2001;41:30S.
67. Tocci LJ, Reeves CT: Cost saving method for the preparationof differential adsorbing cells [abstract]. Transfusion 1998;38(Suppl.):89S.
68. Petz LD, Branch DR: Serological tests for the diagnosis ofimmune hemolytic anemias. In McMillan R (ed): Methods inHaematology: Immune Cytopenias. New York: ChurchillLivingstone, 1983:9–48.
69. Petz LD, Garratty G: Blood Transfusion in AutoimmuneHemolytic Anemias. In Petz LD, Garratty G (eds): AcquiredImmune Hemolytic Anemias, 1st ed. New York: ChurchillLivingstone, 1980:358–391.
70. Laine EP, Leger RM, Arndt PA, Calhoun L, Garratty G, PetzLD: In vitro studies of the impact of transfusion on the detec-tion of alloantibodies after autoadsorption. Transfusion2000;40:1384–1387.
71. Mollison PL, Engelfriet CP, Contreras M (eds): Blood Transfusionin Clinical Medicine, 10th ed. Oxford: Blackwell Science, 1997.
72. Reid ME, Toy PT: Use of preserved autologous red blood cellsto absorb warm autoantibodies from the serum of patientsreceiving blood transfusion therapy. Vox Sang 1984;46:355–359.
73. Garratty G: Autoimmune hemolytic anemia. In Garratty G(ed): Immunobiology of Transfusion Medicine. New York:Marcel Dekker, 1994:493–521.
74. Garratty G: Target antigens for red cell-bound autoantibodies.In Nance SJ (ed): Clinical and serological aspects of immuno-hematology. Arlington, VA: American Association of BloodBanks, 1991:33.
75. Mollison PL: Measurement of survival and destruction of redcells in haemolytic syndromes. Br Med Bull 1959;15:59.
76. Red cell antibodies against self antigens, bound antigens andinduced antigens. In Mollison PL, Engelfriet CP, Contreras M(eds): Blood Transfusion in Clinical Medicine, 10th ed. Oxford:Blackwell Science, 1997:213–240.
77. Salmon C: Autoimmune hemolytic anemia. In Bach J,Swenson RS, Schwartz RS (eds): Immunology. New York:Wiley & Sons, 2001:675.
78. Borne AE von dem, Engelfriet CP, Beckers D, Van Loghem JJ:Autoimmune haemolytic anaemias. IV. Biochemical studies ofred cells from patients with autoimmune haemolytic anaemiawith incomplete warm autoantibodies. Clin Exp Immunol1971;8:377–388.
79. Hollander L: Study of the erythrocyte survival time in a caseof acquired haemolytic anaemia. Vox Sang 1954;4:164.
80. Crowley LV, Bouroncle BA: Studies on the specificity of autoan-tibodies in acquired hemolytic anemia. Blood 1956;11:700.
81. Wiener AS, Gordon EB, Russow E: Observations on the natureof the autoantibodies in a case of acquired hemolytic anemia.Ann Int Med 1957;47:1.
82. Ley AM, Mayer K, Harris JP: Observations on a “specific autoan-tibody.” Proc 6th Congr Int Soc Blood Trans, Boston, 1958:148.

Blood Transfusion in Autoimmune Hemolytic Anemias 399
83. Hogman C, Killander J, Sjolin S: A case of idiopathic autoim-mune haemolytic anaemia due to anti-e. Acta Paediat1960;49:270.
84. Bell CA, Zwicker H, Sacks HJ: Autoimmune hemolyticanemia: Routine serologic evaluation in a general hospitalpopulation. Am J Clin Pathol 1973;60:903–911.
85. Dacie JV. The Haemolytic Anaemias. Part II. AutoimmuneHaemolytic Anaemias, 2nd ed. London: J. & A Churchill,1962.
86. Petz LD. Transfusing patients with autoimmune hemolyticanemia: How should a clinician deal with “least incompatible”units? Education Manual of the American Society ofHematology 2002;449–454.
87. Standards for Blood Banks and Transfusion Services, 22nd ed.Bethesda, MD: American Association of Blood Banks, 2003.
88. Shulman IA, Nelson JM, Nakayama R: When should antibodyscreening tests be done for recently transfused patients?Transfusion 1990;30:39–41.
89. Shirey RS, Boyd JS, Parwani AV, Tanz WS, Ness PM, King KE:Prophylactically antigen-matched donor blood for patientswith warm autoantibodies: An algorithm for transfusionmanagement. Transfusion 2002;42:1435–1441.
90. Lau FY, Wong R, Chan NPH, et al: Provision of phenotype-matched blood units: No need for pre-transfusion antibodyscreening. Haematologica 2001;86:742–748.
91. Garratty G, Petz LD: Approaches to selecting blood for trans-fusion to patients with autoimmune hemolytic anemia.Transfusion 2002;42:1390–1392.
92. Shirey RS, Ness PM: New concepts of delayed hemolytictransfusion reactions. In Nance SJ (ed): Clinical and BasicScience: Aspects of Immunohematology. Arlington, VA:American Association of Blood Banks, 1991:179.
93. Shirey RS, King KE: Alloimmunization to blood group anti-gens. In Anderson KE, Ness PM (eds): Scientific Basis ofTransfusion Medicine: Implications for Clinical Practice.Philadelphia: WB Saunders, 2000:393–400.
94. Garratty G, Petz LD, Hoops JK: The correlation of cold agglu-tinin titrations in saline and albumin with haemolyticanaemia. Brit J Haemat 1977;35:587–595.
95. Giblett ER: Blood group alloantibodies: An assessment ofsome laboratory practices. Transfusion 1977;17:299–308.
96. Stroup M, MacIlroy M: Evaluation of the albumin antiglobu-lin technique in antibody detection. Transfusion 1965;5:184.
97. Dzik WH, Yang R, Blank J: Rabbit erythrocyte stroma treat-ment of serum interferes with recognition of delayedhemolytic transfusion reaction. Transfusion 1986;26:303–304.
98. Deutsch HF, Morton JI: Dissociation of human serummacroglobulins. Science 1957;125:600.
99. Grubb R, Swahn B: Destruction of some agglutinins but not ofothers by two sulfhydryl compounds. Acta Path MicrobiolScand 1958;43:305.
100. Pirofsky B, Rosner ER: DTT test: A new method to differen-tiate IgM and IgG erythrocyte antibodies. Vox Sang 1974;27:480–488.
101. Olson PR, Weiblen BJ, O’Leary JJ, Moscowitz AJ, McCulloughJ: A simple technique for the inactivation of IgM antibodiesusing dithiothreitol. Vox Sang 1976;30:149–159.
102. Freedman J, Masters CA, Newlands M, Mollison PL: Optimalconditions for the use of sulphydryl compounds in dissociat-ing red cell antibodies. Vox Sang 1976;30:231–239.
103. Van Loghem JJ, Peetom F, Van der Hart M, et al: Serologicaland immunochemical studies in hemolytic anemia with high-titer cold agglutinins. Vox Sang 1963;8:33.
104. Woll JE, Smith CM, Nusbacher J: Treatment of acute coldagglutinin hemolytic anemia with transfusion of adult i RBCs.JAMA 1974;229:1779–1780.
105. Sabio H, Jones D, McKie VC: Biphasic hemolysin hemolyticanemia: Reappraisal of an acute immune hemolytic anemia ofinfancy and childhood. Am J Hematol 1992;39:220–222.
106. Nordhagen R, Stensvold K, Winsnes A, Skyberg D, Storen A:Paroxysmal cold haemoglobinuria: The most frequent acuteautoimmune haemolytic anaemia in children? Acta PaediatrScand 1984;73:258–262.
107. Johnsen HE, Brostrphom K, Madsen M: Paroxysmal coldhaemoglobinuria in children: 3 cases encountered within aperiod of 7 months. Scand J Haematol 1978;20:413–416.
108. O’Neill BJ, Marshall WC: Paroxysmal cold haemoglobinuriaand measles. Arch Dis Child 1967;42:183–186.
109. Bird GW, Wingham J, Martin AJ, et al: Idiopathic non-syphilitic paroxysmal cold haemoglobinuria in children. J ClinPathol 1976;29:215–218.
110. Wolach B, Heddle N, Barr RD, Zipursky A, Pai KR, BlajchmanMA: Transient Donath-Landsteiner haemolytic anaemia. Br JHaematol 1981;48:425–434.
111. Sokol RJ, Hewitt S, Stamps BK: Autoimmune haemolysisassociated with Donath-Landsteiner antibodies. ActaHaematol 1982;68:268–277.
112. Lindgren S, Zimmerman S, Gibbs F, Garratty G: An unusualDonath-Landsteiner antibody detectable at 37 degrees C bythe antiglobulin test. Transfusion 1985;25:142–144.
113. Chaplin H Jr: Special problems in transfusion management ofpatients with autoimmune hemolytic anemia. In Bell CA (ed):A seminar on Laboratory Management of Hemolysis.Washington, DC: American Association of Blood Banks,1979:135–150.
114. Gurgey A, Yenicesu I, Kanra T, et al: Autoimmune hemolyticanemia with warm antibodies in children: Retrospectiveanalysis of 51 cases. Turk J Pediatr 1999;41:467–471.
115. Heidemann SM, Sarniak SA, Sarniak AP: Exchange transfu-sion for severe autoimmune hemolytic anemia. Amer J PediatrHematol Oncol 1987;9:302–304.
116. Bilgrami S, Cable R, Pisciotto P, Rowland F, Greenberg B: Fataldisseminated intravascular coagulation and pulmonarythrombosis following blood transfusion in a patient withsevere autoimmune hemolytic anemia and human immuno-deficiency virus infection. Transfusion 1994;34:248–252.
117. Saif MW, Morse EE, Greenberg BR: HIV-associated autoim-mune hemolytic anemia complicated by pulmonaryembolism following a red blood cell transfusion: Case reportand review of the literature. Conn Med 1998;62:67–70.
118. David A, Thomas M: Upperextremity arterial thrombosisassociated with immunohemolytic anemia. Surgery1996;119:354–355.
119. Ries M, Simon S, Hummer HP, Leipold G: Acute mesentericvein thrombosis: A rare complication after splenectomy due toautoimmune hemolytic anemia in childhood. MonatsschKinderheilkd 1993;141:779–781.
120. Silvergleid AJ, Wells RF, Hafleigh EB, et al: Compatibility testusing chromium-labeled red blood cells in crossmatch posi-tive patients. Transfusion 1978;18:8–14.
121. International Committee for Standardization in Haematology:Recommended methods for radioisotope red cell survivalstudies. Blood 1971;38:378.
122. Mayer K, Bettigole RE, Harris JP, D’Amaro J: Test in vivo todetermine donor blood compatibility. Transfusion 1968;8:8–32.
123. Meyer K, Chin B, Magnes J, Harris JP, Tegoli J: Further experi-ences with the in vivo crossmatch and transfusion of Coombsincompatible red cells [abstract]. XVII Congress ofInternational Society of Hematology and XV Congress ofInternational Society of Blood Transfusion Book of Abstracts,1978;49.
124. Red cell incompatability in vivo. In Mollison PL, EngelfrietCP, Contreras M (eds): Blood Transfusion in ClinicalMedicine, 10th ed. Oxford: Blackwell Science, 1997:315–357.
125. Peters B, Reid ME, Ellisor SS, Avoy DR: Red cell survivalstudies of Lub incompatible blood in a patient with anti-Lub[abstract]. Transfusion 1978;18:623.
126. Wallace J: Blood Transfusion for Clinicians. New York:Churchill Livingstone, 1977.
127. AuBuchon JP: Guidelines for the Use of Blood WarmingDevices. Bethesda, MD: American Association of BloodBanks, 2001.
128. Raff JP, Dobson CE, Tsai HM: Transfusion of polymerisedhuman haemoglobin in a patient with severe sickle-cellanaemia. Lancet 2002;360:464–465.

400 Immune Hemolytic Anemias
129. Spahn DR: Artificial oxygen carriers: Status 2002. Vox Sang2002;83 (Suppl. 1):281–285.
130. Spahn DR, Waschke KF, Standl T, et al: Use of perflubronemulsion to decrease allogeneic blood transfusion in high-blood-loss non-cardiac surgery: Results of a European phase 3study. Anesthesiology 2002;97:1338–1349.
131. Tremper KK: Perfluorochemical “red blood cell substitutes”:The continued search for an indication. Anesthesiology2002;97:1333–1334.
132. Gould SA, Moore EE, Hoyt DB, et al: The life-sustainingcapacity of human polymerized hemoglobin when red cellsmight be unavailable. J Am Coll Surg 2002;195:445–452.
133. Griffiths E, Cortes A, Gilbert N, Stevenson P, MacDonald S,Pepper D: Haemoglobin-based blood substitutes and sepsis.Lancet 1995;345:158–160.
134. Litwin MS, Walter CW, Ejarque P, Reynolds ES: Synergistictoxicity of gram-negative bacterial and free colloidal hemo-globin. Ann Surg 1963;157:485–493.
135. Evans RS, Bingham M, Turner E: Autoimmune hemolyticdisease: Observations of serologic reactions and disease activ-ity. Ann NY Acad Sci 1965;124:422.
136. Goldfinger D, Connelly M, Kellum S, Rosenbaum D: Transfu-sion of frozen autologous red cells in patients with positivedirect antiglobulin tests [abstract]. Blood 1979;54(Suppl. 1):123a.
137. Parr GV, Ballard JO: Autologous blood transfusion withmethyldopa induced positive direct antiglobulin test. Trans-fusion 1980;20:119.
138. Snyder EL, Spivack M: Clinical and serologic management ofpatients with methyldopa-induced positive antiglobulin tests.Transfusion 1979;19:313–316.