Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Immediate transverse rectus abdominis musculocutaneous(TRAM) flap breast reconstruction in underweight Asian patients
Eun Key Kim • Jin Sup Eom • Chang Heon Hwang •
Sei Hyun Ahn • Byung Ho Son • Taik Jong Lee
Received: 28 February 2012 / Accepted: 8 January 2013
� The Japanese Breast Cancer Society 2013
Abstract
Background TRAM breast reconstruction is commonly
thought to be inadequate for underweight patients and LD
flap with implant is usually recommended. However, it is
often difficult to find an appropriate implant for thin Asian
women with small breasts. The authors present the results
of using TRAM flap alone for immediate breast recon-
struction in underweight Asian patients.
Methods Between September 2001 and October 2006,
564 patients underwent immediate TRAM flap-only
breast reconstruction. Among these, 18 were underweight
(BMI\18.5 kg/m2) and 317 were normal weight (18.5 kg/
m2 B BMI \ 23.0 kg/m2). Complications were classified
as systemic, breast, and donor site. Complication rate,
oncologic outcome and overall satisfaction and recom-
mendation were compared between two groups. Standard-
ized postoperative photographs were also subject to a panel
for cosmetic assessment.
Results the overall complication rate was 22.2 % in
underweight group and 27.1 % in normal weight group
(p = 0.32). There was a tendency that the breast compli-
cation rate was higher in the normal weight group and the
abdominal complication rate was higher in the underweight
group. However, neither of these was statistically signifi-
cant. Mean satisfaction was not statistically different, either
(8.44 vs. 8.60, p = 0.54). Panel assessment for overall
cosmesis, symmetry and scarring showed no significant
between-group differences.
Conclusions Immediate breast reconstruction using
TRAM flap alone can be performed with acceptable com-
plication rates and comparable patients’ satisfaction score
in a well selected underweight Asian women as in a normal
weight group.
Keywords Breast reconstruction � Thinness �Underweight � TRAM flap
Introduction
Since Hartrampf et al. [1] first introduced it more than
30 years ago, the pedicled transverse rectus abdominis
musculocutaneous (TRAM) flap has been a popular and
reliable option in immediate breast reconstruction with its
undefeated merit of relative simplicity [2]. However, many
surgeons hesitate to use TRAM flap breast reconstruction
in underweight patients thinking that they would have
insufficient abdominal tissue. The common autologous
tissue reconstructive procedure in these patients has been
latissimus dorsi (LD) flap combined with implant, and
other sources such as buttock or thigh have also been
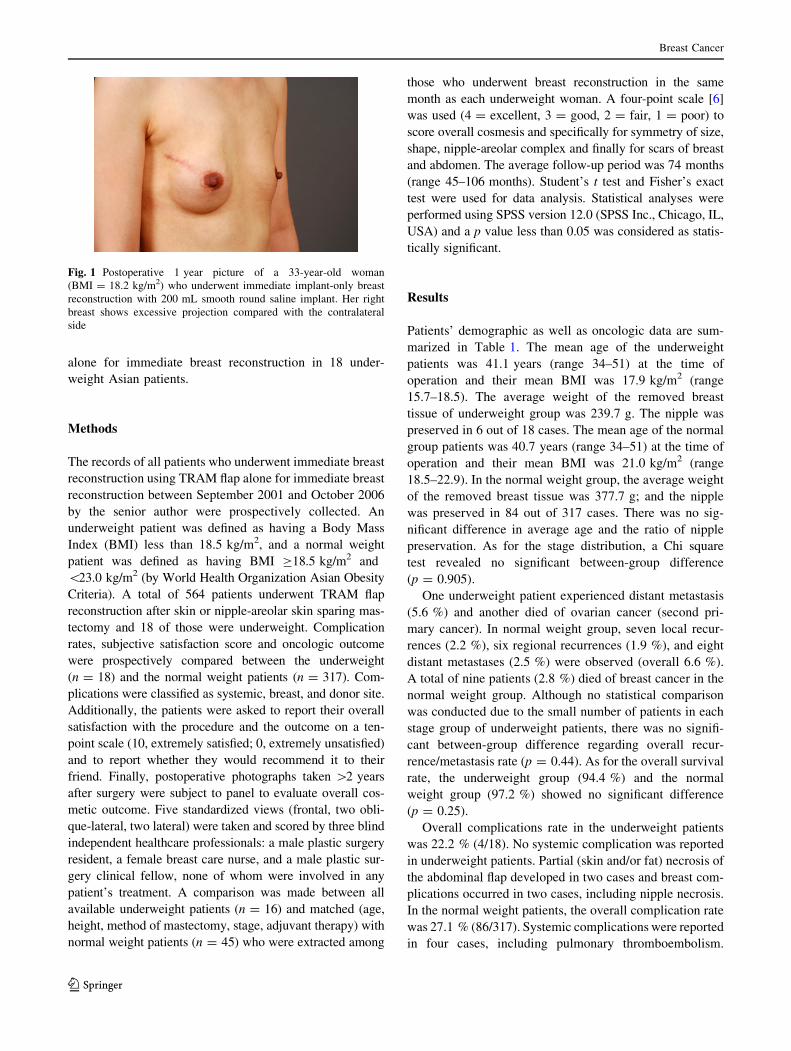
sought [3–5]. However, in lean Asian women with rela-
tively small breasts, it is difficult to find implants with
appropriate width and projection. In our experience, these
patients usually have small dense breasts with minimal
projection. Using conventional implants in these patients
usually results in breasts with insufficient width and
excessive projection (Fig. 1), which may be hard to cam-
ouflage even with covering latissimus dorsi. The intent of
this article is to present the results of using TRAM flap
E. K. Kim � J. S. Eom � C. H. Hwang � T. J. Lee (&)
Department of Plastic Surgery, Asan Medical Center,
University of Ulsan, Pungnap-2 dong, Songpa-gu, Seoul, Korea
e-mail: [email protected]
S. H. Ahn � B. H. Son
Department of Surgery, Asan Medical Center,
University of Ulsan, Seoul, Korea
123
Breast Cancer
DOI 10.1007/s12282-013-0443-9
alone for immediate breast reconstruction in 18 under-
weight Asian patients.
Methods
The records of all patients who underwent immediate breast
reconstruction using TRAM flap alone for immediate breast
reconstruction between September 2001 and October 2006
by the senior author were prospectively collected. An
underweight patient was defined as having a Body Mass
Index (BMI) less than 18.5 kg/m2, and a normal weight
patient was defined as having BMI C18.5 kg/m2 and
\23.0 kg/m2 (by World Health Organization Asian Obesity
Criteria). A total of 564 patients underwent TRAM flap
reconstruction after skin or nipple-areolar skin sparing mas-
tectomy and 18 of those were underweight. Complication
rates, subjective satisfaction score and oncologic outcome
were prospectively compared between the underweight
(n = 18) and the normal weight patients (n = 317). Com-
plications were classified as systemic, breast, and donor site.
Additionally, the patients were asked to report their overall
satisfaction with the procedure and the outcome on a ten-
point scale (10, extremely satisfied; 0, extremely unsatisfied)
and to report whether they would recommend it to their
friend. Finally, postoperative photographs taken [2 years
after surgery were subject to panel to evaluate overall cos-
metic outcome. Five standardized views (frontal, two obli-
que-lateral, two lateral) were taken and scored by three blind
independent healthcare professionals: a male plastic surgery
resident, a female breast care nurse, and a male plastic sur-
gery clinical fellow, none of whom were involved in any
patient’s treatment. A comparison was made between all
available underweight patients (n = 16) and matched (age,
height, method of mastectomy, stage, adjuvant therapy) with
normal weight patients (n = 45) who were extracted among
those who underwent breast reconstruction in the same
month as each underweight woman. A four-point scale [6]
was used (4 = excellent, 3 = good, 2 = fair, 1 = poor) to
score overall cosmesis and specifically for symmetry of size,
shape, nipple-areolar complex and finally for scars of breast
and abdomen. The average follow-up period was 74 months
(range 45–106 months). Student’s t test and Fisher’s exact
test were used for data analysis. Statistical analyses were
performed using SPSS version 12.0 (SPSS Inc., Chicago, IL,
USA) and a p value less than 0.05 was considered as statis-
tically significant.
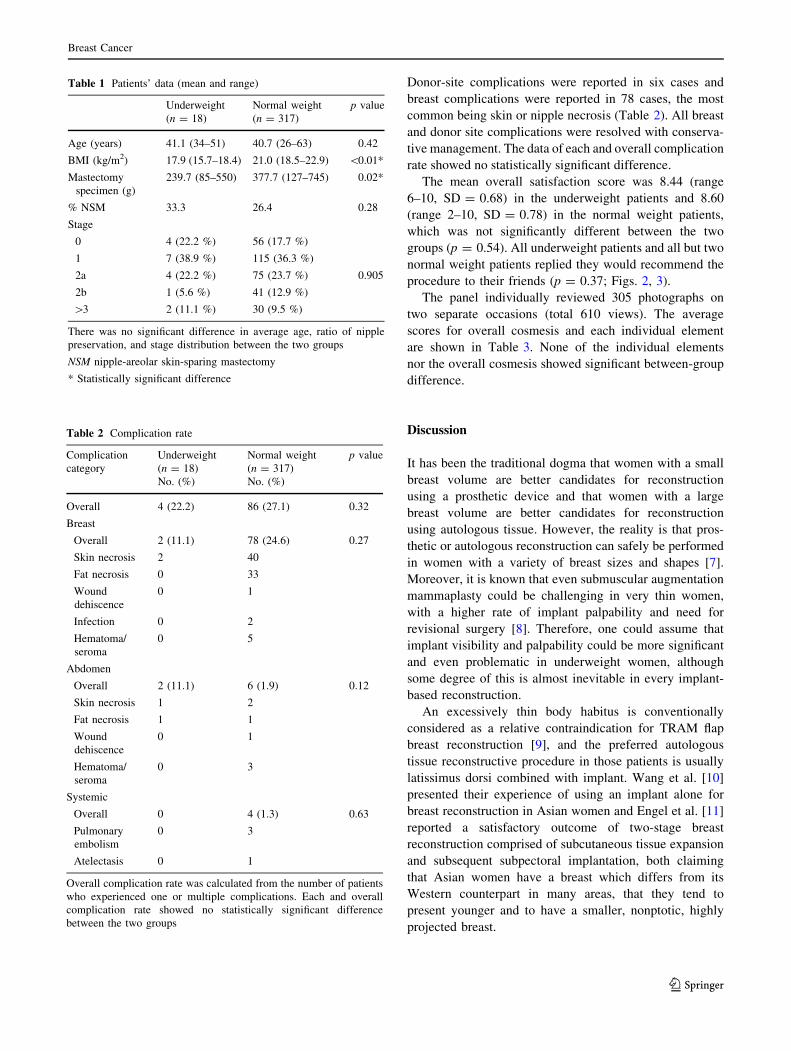
Results
Patients’ demographic as well as oncologic data are sum-
marized in Table 1. The mean age of the underweight
patients was 41.1 years (range 34–51) at the time of
operation and their mean BMI was 17.9 kg/m2 (range
15.7–18.5). The average weight of the removed breast
tissue of underweight group was 239.7 g. The nipple was
preserved in 6 out of 18 cases. The mean age of the normal
group patients was 40.7 years (range 34–51) at the time of
operation and their mean BMI was 21.0 kg/m2 (range
18.5–22.9). In the normal weight group, the average weight
of the removed breast tissue was 377.7 g; and the nipple
was preserved in 84 out of 317 cases. There was no sig-
nificant difference in average age and the ratio of nipple
preservation. As for the stage distribution, a Chi square
test revealed no significant between-group difference
(p = 0.905).
One underweight patient experienced distant metastasis
(5.6 %) and another died of ovarian cancer (second pri-
mary cancer). In normal weight group, seven local recur-
rences (2.2 %), six regional recurrences (1.9 %), and eight
distant metastases (2.5 %) were observed (overall 6.6 %).
A total of nine patients (2.8 %) died of breast cancer in the
normal weight group. Although no statistical comparison
was conducted due to the small number of patients in each
stage group of underweight patients, there was no signifi-
cant between-group difference regarding overall recur-
rence/metastasis rate (p = 0.44). As for the overall survival
rate, the underweight group (94.4 %) and the normal
weight group (97.2 %) showed no significant difference
(p = 0.25).
Overall complications rate in the underweight patients
was 22.2 % (4/18). No systemic complication was reported
in underweight patients. Partial (skin and/or fat) necrosis of
the abdominal flap developed in two cases and breast com-
plications occurred in two cases, including nipple necrosis.
In the normal weight patients, the overall complication rate
was 27.1 % (86/317). Systemic complications were reported
in four cases, including pulmonary thromboembolism.
Fig. 1 Postoperative 1 year picture of a 33-year-old woman
(BMI = 18.2 kg/m2) who underwent immediate implant-only breast
reconstruction with 200 mL smooth round saline implant. Her right
breast shows excessive projection compared with the contralateral
side
Breast Cancer
123
Donor-site complications were reported in six cases and
breast complications were reported in 78 cases, the most
common being skin or nipple necrosis (Table 2). All breast
and donor site complications were resolved with conserva-
tive management. The data of each and overall complication
rate showed no statistically significant difference.
The mean overall satisfaction score was 8.44 (range
6–10, SD = 0.68) in the underweight patients and 8.60
(range 2–10, SD = 0.78) in the normal weight patients,
which was not significantly different between the two
groups (p = 0.54). All underweight patients and all but two
normal weight patients replied they would recommend the
procedure to their friends (p = 0.37; Figs. 2, 3).
The panel individually reviewed 305 photographs on
two separate occasions (total 610 views). The average
scores for overall cosmesis and each individual element
are shown in Table 3. None of the individual elements
nor the overall cosmesis showed significant between-group
difference.
Discussion
It has been the traditional dogma that women with a small
breast volume are better candidates for reconstruction
using a prosthetic device and that women with a large
breast volume are better candidates for reconstruction
using autologous tissue. However, the reality is that pros-
thetic or autologous reconstruction can safely be performed
in women with a variety of breast sizes and shapes [7].
Moreover, it is known that even submuscular augmentation
mammaplasty could be challenging in very thin women,
with a higher rate of implant palpability and need for
revisional surgery [8]. Therefore, one could assume that
implant visibility and palpability could be more significant
and even problematic in underweight women, although
some degree of this is almost inevitable in every implant-
based reconstruction.
An excessively thin body habitus is conventionally
considered as a relative contraindication for TRAM flap
breast reconstruction [9], and the preferred autologous
tissue reconstructive procedure in those patients is usually
latissimus dorsi combined with implant. Wang et al. [10]
presented their experience of using an implant alone for
breast reconstruction in Asian women and Engel et al. [11]
reported a satisfactory outcome of two-stage breast
reconstruction comprised of subcutaneous tissue expansion
and subsequent subpectoral implantation, both claiming
that Asian women have a breast which differs from its
Western counterpart in many areas, that they tend to
present younger and to have a smaller, nonptotic, highly
projected breast.
Table 1 Patients’ data (mean and range)
Underweight
(n = 18)
Normal weight
(n = 317)
p value
Age (years) 41.1 (34–51) 40.7 (26–63) 0.42
BMI (kg/m2) 17.9 (15.7–18.4) 21.0 (18.5–22.9) \0.01*
Mastectomy
specimen (g)
239.7 (85–550) 377.7 (127–745) 0.02*
% NSM 33.3 26.4 0.28
Stage
0 4 (22.2 %) 56 (17.7 %)
1 7 (38.9 %) 115 (36.3 %)
2a 4 (22.2 %) 75 (23.7 %) 0.905
2b 1 (5.6 %) 41 (12.9 %)
[3 2 (11.1 %) 30 (9.5 %)
There was no significant difference in average age, ratio of nipple
preservation, and stage distribution between the two groups
NSM nipple-areolar skin-sparing mastectomy
* Statistically significant difference
Table 2 Complication rate
Complication
category
Underweight
(n = 18)
No. (%)
Normal weight
(n = 317)
No. (%)
p value
Overall 4 (22.2) 86 (27.1) 0.32
Breast
Overall 2 (11.1) 78 (24.6) 0.27
Skin necrosis 2 40
Fat necrosis 0 33
Wound
dehiscence
0 1
Infection 0 2
Hematoma/
seroma
0 5
Abdomen
Overall 2 (11.1) 6 (1.9) 0.12
Skin necrosis 1 2
Fat necrosis 1 1
Wound
dehiscence
0 1
Hematoma/
seroma
0 3
Systemic
Overall 0 4 (1.3) 0.63
Pulmonary
embolism
0 3
Atelectasis 0 1
Overall complication rate was calculated from the number of patients
who experienced one or multiple complications. Each and overall
complication rate showed no statistically significant difference
between the two groups
Breast Cancer
123

Our experiences revealed that thin Asian women usually
have small breasts with less projection. Using conventional
implants in these patients usually results in asymmetry with
insufficient width and excessive projection, which is hard
to camouflage even with a covering latissimus dorsi flap.
Conventional smaller-volume implants with lower projec-
tions have insufficient width, and larger ones with suffi-
cient width have excessive projections. Moreover, implants
with larger volumes increase tension, raising the risk of
wound dehiscence, mastectomy flap necrosis, and implant
exposure. Recently with the advance of reconstructive
microsurgery, more sophisticated surgical options such as
multiplying and/or stacking the flaps are also suggested
for extreme cases [12, 13]. However, in our experience,
the greater part of underweight Asian women could be
reconstructed with TRAM flap alone, which usually have
adequate dimension with matching projection. In this
study, we demonstrated that immediate breast reconstruc-
tion using TRAM flap alone in underweight Asian patients
yielded comparable outcomes with acceptable complica-
tion rates. It is true that underweight patients have less
abdominal tissue, but their smaller breasts usually allow for
satisfactory reconstruction. An LD or extended LD flap
alone could also be considered if the surgeon and the
patient prefer it, as an LD flap can be done without an
implant for women with a small breast [14]. However,
when an extended LD flap is planned, it should be con-
sidered that the fatty tissue under the fascia is even scantier
in the back of underweight patients.
There are some pitfalls in using TRAM flaps in under-
weight patients which may lead to unsatisfactory aesthetic
results. First, these patients commonly have a vague
inframammary fold. Careful reconstruction of the lateral
portion of the tunnel may reduce the related aesthetic
problem. Second, the thin subcutaneous tissue of under-
weight patients makes epigastric bulging more noticeable.
Sufficient back-cut at the lateral muscle belly and severing
of the eighth intercostal nerve are required to minimize the
bulging [15]. Tension on the abdominal closure site is
another problem in underweight patients with less
abdominal tissue, but most breast cancer patients are in
their 30s or more and usually have enough abdominal tis-
sue for breast reconstruction. The abdominal complication
rate showed a higher tendency in underweight patients (one
fat necrosis and one skin necrosis) which may be the result
of higher tension. Hypertrophic scarring did not differ
between the two groups, having an incidence of about 5 %
in both groups. On the contrary, breast fat necrosis did not
develop in any of our 18 underweight patients, which
probably resulted from their smaller, thin flap. These
findings failed to show a statistically significant difference
in both breast and abdominal complication rates; still the
small number in the underweight group remains as the
major limitation of our study. Further data with more
underweight patients would be required to verify these
assumptions. At any rate, it is true that hypertrophic
Fig. 2 A 41-year old woman (BMI = 17.5 kg/m2) who underwent
immediate breast reconstruction after nipple-areolar skin-sparing
mastectomy with TRAM flap. The photograph was taken 1 year after
the surgery
Fig. 3 Postoperative 1 year picture of a 33-year old woman
(BMI = 15.7 kg/m2) who underwent immediate breast reconstruction
with TRAM flap after nipple-areolar skin-sparing mastectomy
Breast Cancer
123

scarring of the donor site could be problematic in lean
Asian patients [16, 17] and the possibility of developing
such a complication should be consulted with the patient
preoperatively. We think that careful patient selection may
reduce the donor site problems in underweight patients: we
do not recommend TRAM flap breast reconstruction for
patients with a tight abdomen who are too young or
nulliparous.
In conclusion, TRAM flap can be performed with
acceptable complication rates and comparable cosmetic
outcome as well as patients’ satisfaction score in well
selected underweight Asian women as in a normal weight
group, and it should not be preexcluded in planning a
breast reconstruction.
Conflict of interest The authors report no financial or other conflict
of interest relevant to the subject of this article.
References
1. Hartrampf CR, Scheflan M, Black PW. Breast reconstruction with
a transverse abdominal island flap. Plast Reconstr Surg.
1982;69:216–25.
2. Buck DW 2nd, Fine NA. The pedicled transverse rectus abdo-
minis myocutaneous flap: indications, techniques, and outcomes.
Plast Reconstr Surg. 2009;124:1047–54.
3. Blondeel PN. The sensate free superior gluteal artery perforator
(S-GAP) flap: a valuable alternative in autologous breast recon-
struction. Br J Plast Surg. 1999;52:185–93.
4. Werdin F, Peek A, Martin NC, Baumeister S. Superior gluteal
artery perforator flap in bilateral breast reconstruction. Ann Plast
Surg. 2010;64:17–21.
5. Wechselberger G, Schoeller T. The transverse myocutaneous
gracilis free flap: a valuable tissue source in autologous breast
reconstruction. Plast Reconstr Surg. 2004;114:69–73.
6. Fortin AJ, Cheang M, Latosinsky S. Cosmetic outcomes fol-
lowing breast conservation therapy: in search of a reliable scale.
Breast Cancer Res Treat. 2006;100:65–70.
7. Nahabedian MY. Breast reconstruction: a review and rationale
for patient selection. Plast Reconstr Surg. 2009;124:55–62.
8. Stokes RB. Breast augmentation in thin women: patient satis-
faction with saline-filled implants. Aesthetic Plast Surg. 2004;28:
153–7.
9. Han SH, Cho JH, Ahn SH. Immediate breast reconstruction after
mastectomy. J Korean Soc Plast Reconstr Surg. 1995;22:843–51.
10. Wang HY, Ali RS, Chen SC, Chao TC, Cheng MH. One-stage
immediate breast reconstruction with implant following skin-
sparing mastectomy in Asian patients. Ann Plast Surg.
2008;60:362–6.
11. Engel H, Huang JJ, Lin CY, Lam WL, Gazyakan E, Cheng MH.
Subcutaneous tissue expansion and subsequent subpectoral
implantation for breast reconstruction in Asian patients: safety
and outcome. Ann Plast Surg. 2012 (Epub ahead of print).
12. DellaCroce FJ, Sullivan SK, Trahan C. Stacked deep inferior
epigastric perforator flap breast reconstruction: a review of 110
flaps in 55 cases over 3 years. Plast Reconstr Surg. 2011;127:
1093–9.
13. DellaCroce FJ, Sullivan SK, Trahan C, Jenkins CE. Body lift
perforator flap breast reconstruction: a review of 100 flaps in 25
cases. Plast Reconstr Surg. 2012;129:551–61.
14. Lee CN, Foster RD. Breast reconstruction after mastectomy in
young women. Breast Dis. 2005;2006(23):47–52.
15. Kim EK, Eom JS, Ahn SH, Son BH, Lee TJ. Evolution of the
pedicled TRAM flap: a prospective study of 500 consecutive
cases by a single surgeon in Asian patients. Ann Plast Surg. 2009;
63:378–82.
16. Minn KW, Hong KY, Lee SW. Preoperative TRAM free flap
volume estimation for breast reconstruction in lean patients. Ann
Plast Surg. 2010;64:397–401.
17. Yan XQ, Yang HY, Zhao YM, You L, Xu J. Deep inferior epi-
gastric perforator flap for breast reconstruction: experience with
43 flaps. Chin Med J (Engl). 2007;120:380–4.
Table 3 Average panel assessment score of postoperative photo-
graph evaluation (standard deviation)
Underweight
(n = 16)
Matched normal weight
(n = 45)
p value
Overall
cosmesis
3.38 (0.65) 3.30 (0.55) 0.27
Symmetry of
size
3.22 (0.65) 3.20 (0.67) 0.81
Symmetry of
shape
3.42 (0.83) 3.29 (0.76) 0.17
Symmetry of
NAC
3.44 (0.71) 3.33 (0.71) 0.22
Breast scar 3.50 (0.73) 3.57 (0.67) 0.39
Abdomen
scar
3.33 (0.76) 3.20 (0.63) 0.10
None of the individual elements nor overall cosmesis showed a sig-
nificant between-group difference
NAC nipple-areolar complex
Breast Cancer
123





























