Embed Size (px)
Citation preview

International Immunopharmacology xxx (2014) xxx–xxx
INTIMP-03406; No of Pages 5
Contents lists available at ScienceDirect
International Immunopharmacology
j ourna l homepage: www.e lsev ie r .com/ locate / in t imp
Immediate infusion-related adverse reactions to intravenous immunoglobulin in aprospective cohort of 1765 infusions
Danielli C. Bichuetti-Silva ⁎, Fernanda P. Furlan, Fernanda A. Nobre, Camila T.M. Pereira, Tessa R.T. Gonçalves,Mariana Gouveia-Pereira, Rafael Rota, Lusinete Tavares, Juliana T.L. Mazzucchelli, Beatriz T. Costa-Carvalho ⁎Division of Allergy Clinical Immunology and Rheumatology, Department of Pediatrics, Federal University of São Paulo (UNIFESP-EPM), Rua dos Otonis 725, São Paulo, SP 04025–002, Brazil
⁎ Corresponding authors at: Rua dos Otonis 725, São P+55 11 55791590; fax: +55 11 50840285.
E-mail addresses: [email protected] (D.C. [email protected] (F.P. Furlan), aimeenobre@[email protected] (C.T.M. Pereira), tessarachel@[email protected] (M. Gouveia-Pereira), [email protected] (L. Tavares), juliana.mazzucc(J.T.L. Mazzucchelli), [email protected] (B.T. Costa
http://dx.doi.org/10.1016/j.intimp.2014.09.0151567-5769/© 2014 Elsevier B.V. All rights reserved.
Please cite this article as: Bichuetti-Silva DC,cohort of 1765 infusions, Int Immunopharm
a b s t r a c t
a r t i c l e i n f oArticle history:Received 18 June 2014Received in revised form 1 September 2014Accepted 10 September 2014Available online xxxx
Keywords:Intravenous immunoglobulinAntibodyInfusion-relatedAdverse reactionsPrimary immunodeficiency
Intravenous immunoglobulin (IVIG) is increasingly recommended for many diseases apart from primary immu-nodeficiency diseases (PID). Although effective and safe, adverse reactions may occur. We conducted a 2-yearprospective observational study in 117 patientswith PIDwho received regular IVIG replacement therapy at ame-dian dose of 600 mg/kg every 3 to 4 weeks to examine IVIG's adverse effects; 1765 infusions were performed(mean = 15/patient) in 75 males and 42 females (aged 3 months to 77 years) in 3 groups: ≤9 years (34.2%),10–19 years (26.5%), and ≥20 years (39.3%). Fifty patients had common variable immunodeficiency (CVID),11 had X-linked agammaglobulinemia (XLA), and 55 had other immune system disorders. The drugs adminis-tered were Octagam® (49.1%), Tegeline® (17.3%), Imunoglobulin® (18.6%), Flebogama® (12.9%), Vigam®(1.2%), and Kiovig® (0.4%). Immediate infusion-related adverse reactions occurred in the cases of 38 out 1765 in-fusions (2.15%, IC95% 1.53%–2.94%), which were classified as mild (81.6%), moderate (10.5%), or severe (7.9%).Time until reaction ranged from 10 to 240min (mean= 85.7, median= 60). Reaction rates were similar acrossage groups. The most common reactions were malaise, headache, and abdominal pain. Reported severe eventswere tightness of the throat and seizure. All symptoms improved with temporary or complete IVIG interruptionand symptomatic medications. Sixteen of 38 reactions to infusions occurred in the presence of an acute infection(p = 0.09). Tegeline® represented a greater reaction risk factor than Octagam® (p b 0.001). These results indi-cate that IVIG infusion can be considered a safe procedure. Low reaction incidence and few severe immediateinfusion-related adverse reactions were observed.
© 2014 Elsevier B.V. All rights reserved.
1. Introduction
Intravenous immunoglobulin (IVIG) has become increasingly im-portant as a replacement therapy in primary and acquired immunodefi-ciencies, and as an immunomodulatory therapy in autoimmune andauto-inflammatory diseases and transplantation [1, 2]. Themechanismsthrough which IVIG produces effects in these distinct disorders are notfully understood, but multiple potential immunomodulatory functionshave been described, and IVIG has been accepted asmore than a passivereplacement therapy [1].
IVIG is a blood derivative consisting primarily of intact IgGmoleculesfrom pooled plasma of human donors [3]. Despite the introduction ofmanufacturing steps that enhance purity, minimize damage to IgG
aulo, SP 04025–002, Brazil. Tel.:
chuetti-Silva),oo.com.br (F.A. Nobre),il.com (T.R.T. Gonçalves),@hotmail.com (R. Rota),[email protected]).
et al, Immediate infusion-relaacol (2014), http://dx.doi.org
molecules, decrease the frequency of adverse reactions, and result in ahigher concentration of liquid IVIG, some adverse reactions associatedwith its regular administration still occur [4, 5].
Studies evaluating adverse reactions to IVIG have revealed incidencerates varying from 1% to as high as 81% of patients or infusions, butmostly between 30 and 40% of infusions [6–13]. These reactions canbe mild, moderate, or severe, and immediate or delayed. Adverse reac-tions may be due to the antigenicity of IgG itself, large-molecular-weight IgG aggregates, presence of an antibody to a circulatingmicrobi-al or self-antigens, or complement activation or direct release of cyto-kines from mononuclear cells. IVIG formulations may contain low-molecular-weight kinins or kallikreins, as well as procoagulant factorsthat were not removed during fractionation. The presence of these fac-tors varies considerably from brand to brand, and even from batch tobatch of the same brand [14]. Other risk factors associated with infu-sions and patient characteristics have been well documented, such asa prior history of infusion reaction, first infusion, large dose, rapiddose, no pre-infusion or post-infusion hydration, fever/infection at thetime of infusion, autoimmunity, older age, immobility, hypertension,high lipid levels, diabetes, smoking, prior/current thrombosis, estrogenuse, and change of IVIG brand [5, 14–16].
ted adverse reactions to intravenous immunoglobulin in a prospective/10.1016/j.intimp.2014.09.015

2 D.C. Bichuetti-Silva et al. / International Immunopharmacology xxx (2014) xxx–xxx
This study was conducted to evaluate the frequency, severity, andrisk factors for adverse reactions related to IVIG infusion at replacementdoses in patients with primary immunodeficiency (PID) in a publichealth clinic in Brazil, where this medication is administered with noconsistent brand or batch for patients from month to month, andwhere pump infusion is not available.
2. Methods
2.1. Patients and IVIG infusions
This study was approved by the Institutional Research Ethics Com-mittee andwas conducted in a Brazilian referral center for adult and pe-diatric patients with PID.
All patients included in the study were diagnosed with PID based onthe criteria of the European Society for Immunodeficiency (ESID) andthe Pan-American Group for Immunodeficiency (PAGID) [17]. Patientsin the outpatient servicewith demonstrated impaired antibody produc-tionwere treatedwith antibodies replacement doses of IVIG (median=600 mg/kg) every 3 to 4 weeks under the supervision of the same timeof clinical immunologist and trained nurses.
Every patientwho had received at least 1 infusion of IVIG fromAugust2011 to August 2013 was enrolled. Because an infusion pump was notavailable, the infusion rate was manually regulated according to the pre-scribed drip rate for each patient. The rate of infusion was calculatedbased on the duration of each IVIG infusion and patient weight (infusionrate= dose/infusion period (min)). All patients received 0.9% saline (100and 250 mL for children and adults, respectively) before IVIG infusion,and those with a prior history of adverse reactions received pre-treatment with medications including steroids, antihistamines, non-steroidal anti-inflammatory drugs (NSAIDs), and antiemetics.
Infusion details were recorded by physicians, including brand andbatch preparations, clinical condition of the patient (including vitalsigns), pre-treatment medication, infusion rate, adverse reaction signsand symptoms, medications used to treat reactions, and informationgained during follow-up examinations. Any reaction that occurred dur-ing the infusion and was diagnosed by a physician was considered animmediate infusion-related adverse reaction.
Because IVIG medication is provided by the Government of Brazil, apatient may receive different brands during the course of his or her treat-ment. Six brands of IVIG preparations were administered to the patients:Vigam® (Bio Products Laboratory, Hertfordshire, UK), Kiovig® (BaxterAG, Vienna, Austria), Octagam® (Octapharma, Langenfeld, Germany),Flebogama® (Grifols, S.A., Barcelona, Spain), Imunoglobulin® (GCC,Suwon-City, Korea), and Tegeline® (LFB-Biomedicaments, Les Ulis,France).
2.2. Classification of reactions
Reactions occurring during IVIG infusionwere classified asmild,mod-erate, or severe, based on the classification scheme proposed by Brennanet al. [18]. Mild reactions included headache, fever, chills, nausea, emesis,hypotension, andmuscle cramps. Mild reactions subsidedwhen the infu-sion rate decreased. Moderate reactions included mild reactions that in-creased in severity and necessitated discontinuation of the infusion.Severe reactions included moderate reactions that were persistent or in-creased in severity, or other symptoms, such as tightness of the throat, se-vere shaking, severe breathlessness or wheezing, severe dizziness orfainting, sensation of pressure in the chest, or collapse. A severe reactionrequired the administration of adrenaline and further medical attention[13].
2.3. Study design and statistical analysis
This studywas a prospective observational studywith 2 years of fol-low up observation. Initially, the data was analyzed descriptively. To
Please cite this article as: Bichuetti-Silva DC, et al, Immediate infusion-relacohort of 1765 infusions, Int Immunopharmacol (2014), http://dx.doi.org
verify the association between the occurrence of adverse reactionsand possible risk factors (acute infection, pre-treatment medication,PID diagnosis, IVIG brand, rate of infusion, age, and number of batches),while considering the possible influence of multiple infusions from aparticular patient, logistic regressions (multivariate analysis) were ad-justed to consider the effect of patient identity as a random effect. Inthese regressions, the adverse reaction was the dependent variableand each factorwas an explanatory variable. Time until reaction accord-ing to severity of the reaction was compared using the non-parametricMann–Whitney U test. For all statistical tests, a significance thresholdof b0.05 was used. Statistical analyses were performed using SPSS soft-ware package version 20.0 (IBM, Tokyo, Japan) and Stata version 12(STATA Corp., College Station, TX, USA).
3. Results
3.1. Patient and infusion features
One hundred and seventeen patients with PID at antibodies replace-ment doses of IVIG (aged 3 months to 77 years) were included in thestudy, of which 42 were women and 75 were men. Stratification byage group resulted in the following groups: ≤9 years (n = 40, 34.2%),10–19 years (n = 31, 26.5%), and ≥20 years (n = 46, 39.3%). Four pa-tients weremore than 60 years old. Fifty patients had immunodeficien-cy (CVID), 11 had X-linked agammaglobulinemia (XLA), and 55 hadother immune system disorders, such as hypogammaglobulinemia,DiGeorge syndrome, Hyper-IgM syndrome, Hyper-IgE syndrome, com-bined immunodeficiency, ataxia-telangiectasia, Bloom syndrome andWiskott–Aldrich syndrome.
During the study period, a total of 1765 infusions were administered(mean = 15/patient, range = 1–36/patient): 558 (31.6%) in patientsaged under 9 years, 505 (28.6%) in patients aged between 10 and19 years, and 702 (39.7%) in patients older than 20 years (60 in the 4 pa-tients older than 60 years). Per diagnosis, infusions were distributed asfollows: 783 (44.4%) in CIVD, 164 (9.3%) in XLA, and 818 (46.3%) inother PID disorders. Each patient received different brands of IVIG ac-cording to availability of the government supply. Preparations usedwere as follows: Octagam® (867, 49.1%), Tegeline® (306, 17.3%),Imunoglobulin® (329, 18.6%), Flebogama® (228, 12.9%), Vigam® (21,1.2%), and Kiovig® (7, 0.4%). Three patients received 2 different brands(Flebogama® and Octagam®, Flebogama® and Imunoglobulin®, orImunoglobulin® and Octagam®) in the same infusion. The brands werenot documented for 7 infusions. Most infusions (1531, 86.7%) werefrom 1 preparation batch, 227 (12.8%) were from 2 or more batches,and for 7 infusions the number of batches were not recorded. Nearly athird (504, 28.5%) of infusions occurred in the presence of an acute infec-tion, most of which were upper (351, 69.5%) and lower (110, 21.8%) re-spiratory tract infections, followed by gastrointestinal infections (58,11.5%). Pre-treatment medication was used in 625 (35.4%) infusions,and included: NSAIDs (569, 90.9%), steroids (79, 12.6%), antiemeticdrugs (55, 8.8%), type I antihistamines (7, 1.1%), and other drugs (28,4.5%) such as type II antihistamines, bronchodilators, or diuretics. Combi-nations of 2 or more medications were used in 93 infusions. The infusionrate was ≤4 mg/kg/min in 859 (48.6%) infusions, and N4 mg/kg/min in644 (36.5%) infusions, of which 47 (2.7%) were administered at ratesN8 mg/kg/min. This data was not recorded for 262 infusions (14.8%).
3.2. Adverse reactions
An incidence rate of 2.15% of infusions (IC95% = 1.53–2.94%) and23.9% of patients (IC95% = 16.5%–32.7%) for adverse reactions was re-ported. Thirty-eight reactions occurred in 28 patients (12 females and16 males aged from 3–51 years). Six patients had 2 reactions, and 2 pa-tients had 3 reactions. The median dose of IVIG was 700 mg/kg(140–860 mg/kg). Out of those 28 patients, 15 had CVID, 2 had XLAand 11 other immune system disorders (4 ataxia-telangiectasia, 3
ted adverse reactions to intravenous immunoglobulin in a prospective/10.1016/j.intimp.2014.09.015

3D.C. Bichuetti-Silva et al. / International Immunopharmacology xxx (2014) xxx–xxx
combined immunodeficiency, 2 hypogammaglobulinemia, 1 Wiskott–Aldrich syndrome and 1 Bloom syndrome). According to infusionswith reactions were distributed as follows: 18/783 (2.3%) in CIVD, 5/164 (3.0%) in XLA, and 15/818 (1.8%) in other PID disorders. Regardingthe 31 first infusions that occurred during the study, in 2 there weresome adverse reactions (6.45%). History of previous reaction was pres-ent in 18 (69.2%) patients. Infusions with reactions by age groupwere: 13/558 (2.3%) in patients aged under 9 years, 13/505 (2.6%) inpatients aged between 10 and 19 years, and 12/702 (1.7%) in patientsolder than 20 years (no statistical difference among these groups).
Distribution of infusions by the presence of acute infection, use ofpre-treatment medication, IVIG preparation, rate of infusion, and num-ber of batches are shown in Table 1. Odds ratios were used to analyzethe associations of these factors with the incidence of adverse reactions,and the only significant factor found was the preparation of IVIG. Therewas a higher incidence of adverse reactions in patients using Tegeline®compared to Octagam® (p b 0.001). Of the 8 patients who had morethan 1 reaction, 5 presented at least 1 from Tegeline®, and 2 patientshad multiple reactions with this brand.
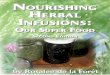
All reactionswere reversed with temporary (31) or complete (4) in-terruption of drug infusion and treatment with symptomatic medica-tions. Frequency of signs and symptoms observed in all reactions areshown in Fig. 1.
3.2.1. Severity of reactionsObserved adverse reactions weremild in 31 (81.6%) infusions, mod-
erate in 4 (10.5%), and severe in 3 (7.9%). The latency until reactionranged from 10 to 240min after the start of infusion (mean= 85.7,me-dian = 60). The distribution of latency by severity of reaction is shownin Fig. 2, and no significant association was detected (p = 0.241).
One moderate reaction (wheezing and dyspnea) occurred in a51 year-old female with CVID on her first infusion. She improved withtemporary interruption, hydration and symptomatic medications. Thebrand used was Octagam® and during the study she received this brandthree more times without recurrence of reaction. Another patient withone moderate reaction was a 16 year-old male with XLA who had threereactions during the study, all with Tegeline®. The first reaction wasmild (malaise and tachycardia); the second, moderate (dyspnea and sen-sation of pressure in the chest), and the third reaction, mild again and the
Table 1Distribution of infusions and adverse reaction according to potential risk factors.
Adverse reaction
No Yes
N (%) N
Acute infectionNo 1.239 (98.3%) 22Yes 488 (96.8%) 16
Pre-treatment medicationNo 1.118 (98.1%) 22Yes 609 (97.4%) 16
PreparationFLEBOGAMA® 222 (97.4%) 6IMUNOGLOBULIN® 326 (99.1%) 3ENDOBULIN KIOVIG® 7 (100%) 0OCTAGAM® 855 (98.6%) 12TEGELINE® 289 (94.4%) 17VIGAM® 21 (100%) 0
Infusion rate (mg/kg/min)≤4 836 (97.3%) 23N4 635 (98.6%) 9
Number of batches1 1.501 (98.0%) 30≥2 219 (96.5%) 8
a Logistic regression with random effect. CI95%: confidence interval of 95%. (1) No adverse r
Please cite this article as: Bichuetti-Silva DC, et al, Immediate infusion-relacohort of 1765 infusions, Int Immunopharmacol (2014), http://dx.doi.org
only one pre-treated with NSAID and steroids. The patient had no furtherreaction to this brand in the following pre-treated infusions. One severereaction (tightness of throat) occurred in a CVID adult patient on her sec-ond infusion. She received Octagam®, after prophylaxis with NSAID andantiemetic drug because of a previousmild reaction to this brand at an in-fusion rate ofN8 mg/kg/min. Themost severe adverse eventwas a seizurethat occurred in a CVID patient with a previous history of herpetic en-cephalitis. He received Flebogama®, at a slow rate (b2 mg/kg/min) andwas not infected at the time of that infusion.
Out of 28 patients, 24 received the same brands that had caused pre-vious reaction during the study without reproducibility of the events.
4. Discussion
IVIG is a complex therapy that can cause numerous-us side effectsand additional adverse consequences [19, 20]. Safe and effective admin-istration of IVIG, as well as the diagnosis and management of adverseevents, are complex tasks that demand expert practice.
We found the incidence of adverse reactions to be surprisingly low:2.15% of infusions (38/1765). Reported rates vary considerably from 1to 81%, depending on the patients studied and the brand of immunoglob-ulin used [6–13]. Although higher rates of systemic reactions are reportedin non-PID patients, we presume that the low rates described here wereobtained due to infusion adjustment that have been made for most pa-tients prior to the study, the enrollment of experienced recipients,i.e., with exposure tomultiple brands of IVIG thatmight have desensitizedsome of them, and the choice to include adverse reactions occurred onlyduring the infusion to avoid patient's bias. Therefore, our data did not in-clude adverse reactions captured for 72 hpost infusion such as headaches,which are themost commonly reported symptom inmost licensing stud-ies of new IVIG products [14, 21–23]. Andres et al. reported delayed head-aches in 24% of patients and 13% of infusions [24].
No significant differenceswere observed in the rates of adverse reac-tions between children, adolescents, and adults. In a recent publication,old age was considered as a risk factor for adverse reactions [14]. Ourstudy was underpowered to evaluate these differences because of thesmall sample size that we considered (only 4 patients more than60 years old), but all patients in this study aged 60 or greater presentednormal kidney and liver functions.
Odds ratio (OR)a
(%) Estimative CI95% p-Value
(1.7%) 1.00 – –
(3.2%) 1.80 0.91–3.56 0.090
(1.9%) 1.00 – –
(2.6%) 1.27 0.62–2.58 0.517
(2.6%) 2.41 0.79–7.35 0.123(0.9%) 0.60 0.16–2.27 0.450
(0%) (1) (1) (1)(1.4%) 1.00 – –
(5.6%) 7.32 2.80–19.10 b0.001(0%) (1) (1) (1)
(2.7%) 2.09 0.93–4.71 0.075(1.4%) 1.00 – –
(2.0%) 1.00 – –
(3.5%) 1.82 0.80–4.13 0.152
eaction was found in this category.
ted adverse reactions to intravenous immunoglobulin in a prospective/10.1016/j.intimp.2014.09.015

Fig. 1. Signs and symptoms observed during mild, moderate, and severe reactions. Mild reactions presented with a variety of symptoms, the most common of which were chill, malaise,headache, and abdominal pain. Moderate reactionswere characterized bywheezing, a sensation of pressure in the chest, andmouth angioedema, while severe reactions included seizureand tightness of the throat. Black = severe reactions; grey = moderate reactions; white = mild reactions.
4 D.C. Bichuetti-Silva et al. / International Immunopharmacology xxx (2014) xxx–xxx
The highest proportion of adverse reactions occurred in 5 of 154 in-fusions in patients with XLA (3.0%). This result differs from the litera-ture, which shows greater susceptibility to adverse reactions inpatients with CIVD due to the development of autoantibodies and IgG/anti-IgA antibodies [25–29].
Active infection during infusion is an important risk factor for ad-verse reactions to IVIG [8]. In infected patients, high rates of adverseevents are related to the formation of antigen–antibody complexes,and rates can be reduced if the patient is apyrexial or receiving anti-biotics. The antigenic load should be reduced with an appropriateantibiotic for 2 to 7 days before IVIG infusion. Therefore, awarenessof underlying infections during the administration of IVIG is impor-tant for the prevention of adverse reactions [8, 30]. Furthermore, itis known that PIDs patients have a chronic underlying inflammatorycondition [31–33]. In our cohort, patients with an underlying infec-tion had a 2-fold higher frequency of adverse reactions than that inpatients without infection, but this difference was not significant(p = 0.09). All patients underwent a medical evaluation prior to in-fusion; no patients had severe infections, all were afebrile when theyreceived infusions and 53% were under chronic prophylactic antibi-otic therapy.
Fig. 2. Time until reaction compared to severity of the reaction. Mild reactions occurredfrom 10 to 240 min after starting IVIG infusion (median= 60 min). Moderate and severereactions occurred from 10 to 150 min after starting IVIG infusion (median = 30 min).
Please cite this article as: Bichuetti-Silva DC, et al, Immediate infusion-relacohort of 1765 infusions, Int Immunopharmacol (2014), http://dx.doi.org
Higher infusion rates are strongly associatedwithmost common ad-verse reactions [34]. These events can be avoided by beginning the infu-sion slowly (0.5 mg/kg/min of 5% IVIG solution or 1 mg/kg/min of 10%IVIG solution) and gradually increasing the rate, as tolerated by the pa-tient. In general, infusion rates should not exceed 0.08 mL/kg/min(equivalent to 4 mg/kg/min of 5% solution or 8 mg/kg/min of 10% solu-tion) [7, 34]. Nevertheless, a survey ofmore than 1000 patients with PIDconducted by the Immune Deficiency Foundation (IDF) found that 44%reported experiencing adverse reactions that were not related to rateof infusion [35]. Moreover, because infusion pumps are expensiveitems for home use, Brennan et al. showed that the rate of infusioncould be calculated based on an individual patient's weight and the con-centration of the immunoglobulin product, and patients selected to starthome-based therapywere easily taught to count the drip rate [7]. At ourcenter, reactions were more common at low rates of infusion, whichwas unexpected. Because our service does not have infusion pumps,rates of infusion were regulated manually by adjusting the drip, and in-fusion rates were recorded based on the duration of each IVIG infusion.This was an important limitation of our study and may have caused ourunexpected results. However, the absence of infusion pumps did notcause a higher rate of adverse reactions.
Adverse reactions are particularly likely in patients naïve to IVIG re-placement. A survey by the IDF showed that approximately 30% of reac-tions occurred during a patient's first IVIG infusion [35]. The reasons forinitial high reaction rates that decrease with subsequent doses of thesame product are unknown. Therefore, the first infusion must be givenslowly as a 3% or 5% solution at a dose of 0.5 to 1.0 mg/kg/min [36]. Inour study, 31 patients received IVIG for the first time, and in these pa-tients the incidence of infusion-related adverse reactions (2/31, 6.45%)was 3 times higher than the overall incidence.
Reported rates of adverse events vary considerably depending onthe group of patients studied and the brand of immunoglobulin used.Brands of IVIG, and batches of a particular brand, are not equally toler-ated. A recent study advised caution when IVIG preparation brandsare changed, because of an increased risk of adverse reactions [37].However, it is unusual for an entire population of immunodeficient pa-tients to receive the same preparation of IVIG. Patients that start on aparticular preparation may be changed to another for reasons of costor availability [29]. This is especially true in Brazil, where the govern-ment supports PID patients and supplies IVIG. Patients are given theirdoses every 3 to 4 weeks according to themedical prescription. Howev-er, the brand provided is often inconsistent and switching brands is very
ted adverse reactions to intravenous immunoglobulin in a prospective/10.1016/j.intimp.2014.09.015

5D.C. Bichuetti-Silva et al. / International Immunopharmacology xxx (2014) xxx–xxx
common. Our patients received 6 different brands of IVIG and brandswitching was nearly universal. In our study, the reactions were signif-icantly associatedwith infusionwith Tegeline®. The 2 patients who suf-feredmultiple reactions (5)with Tegeline® had been on IGIV treatmentfor more than 10 years, and had received all the cited brands, as well asothers, but experienced reactions only to Tegeline® (data not shown).In these 5 reactions, 1 had an underlying infection (conjunctivitis)while the other 4 had no other risk factors. These data agree with pub-lished data showing that preparations are not equally tolerated [38, 39].Tegeline® is the only lyophilized IVIGbrand and contains a high amountof sucrose. Higher prevalence of reactions from lyophilized products di-luted before use is associated with the presence of immunoglobulin ag-gregates and high amounts of sucrose. Dilution of such productsrequires careful regulation of temperature and observation of the prod-uct prior to initiating infusion [34].
Similar to the literature, the majority of adverse reactions were con-sidered mild (81.6%). Moderate and severe events occurred in muchlower proportions of 10.5% and 7.9%, respectively. Themost common im-mediate reactions reported in the literature were chills, fever, headache,nausea, malaise, and myalgia. These reactions were usually mild, oc-curred in the first hour of infusion, and disappeared within 6 h [18, 24,40–42]. In general, the symptoms observed in our research did not differ,and chill, malaise and headache were the most common symptoms.
Considering our low observed reaction rate and the predominanceofmild events, it seems appropriate to consider the safety of home ther-apy programs for selected patients. Previous studies have demonstrateda low overall reaction rate in patients self-infusing IVIG at home afterformal training programs at approved centers, and such home-basedadministration had a positive effect on quality the of life [7, 43, 44].
This study has shown that adverse reactions during IVIG infusion areinfrequent and that IVIG preparations are not equally tolerated. There-fore, recognition of risk factors, appropriate selection and adjustmentof IVIG treatment regimens, use of adjunctive therapies, and trainedmedical supervision should allow for the safe use of this medication.
References
[1] Kaveri SV, Maddur MS, Hegde P, Lacroix-Desmazes S, Bayry J. Intravenous immuno-globulin in immunodeficiencies: more than mere replacement therapy. Clin ExpImmunol 2011;164(2):2–5.
[2] Looney RJ, Huggins J. Use of intravenous immunoglobulin G (IVIG). Best Pract ResClin Haematol 2006;19:3–25.
[3] Sacher RA, the IVIG Advisory Panel. Intravenous immunoglobulin consensus state-ment. J Allergy Clin Immunol 2001;108:139–46.
[4] Ballow M. Intravenous immunoglobulins: clinical experience and viral safety. J AmPharm Assoc 2002;42:449–58.
[5] Fasano MB. Risks and benefits of intravenous immunoglobulin treatment in chil-dren. Curr Opin Pediatr 1995;7:688–94.
[6] Skull S, Kemp A. Treatment of hypogammaglobulinaemia with intravenous immu-noglobulin, 1973–93. Arch Dis Child 1996;74:527–30.
[7] Brennan VM, Cochrane S, Fletcher C, Hendy D, Powell P. Surveillance of adverse re-actions in patients self-infusing intravenous immunoglobulin at home. J ClinImmunol 1995;15:116–9.
[8] Pautard B, Hachulla E, Bagot d'Arc M, Chantreuil L. Intravenous immunoglobulin(Endobulin) clinical tolerance: prospective therapeutic follow-up of 142 adultsand children. Rev Med Interne 2003;24:505–13.
[9] Al Wahadneh AM, Khriesat IA, Kuda EH. Adverse reactions of intravenous immuno-globulin. Saudi Med J 2000;21:953–6.
[10] Benesh M, Kerbl R, Lackner H, Berghold A, Schwinger W, Triebl-Roth K, et al. Low-dose versus high-dose immunoglobulin for primary treatment of acute immunethrombocytopenic purpura in children: results of a prospective, randomizedsingle-centre trial. J Pediatr Hematol Oncol 2003;25:797–800.
[11] Dashti-Kahavidaki S, Aghamohammadi A, Farshadi F, Movahedi M, Parvaneh N,Pouladi N, et al. Adverse reactions of prophylactic intravenous immunoglobulin; a13-year experience with 3004 infusions in Iranian patients with primary immuno-deficiency diseases. J Investig Allergol Clin Immunol 2009;19(2):139–45.
[12] Wasserman RL, Church J, Stein M, Moy J, White M, Strausbaugh S, et al. Safety, effi-cacy and pharmacokinetics of a new 10% liquid intravenous immunoglobulin (IVIG)in patients with primary immunodeficiency. J Clin Immunol 2012;32:663–9.
[13] Katz U, Achiron A, Shere Y, Shoenfeld Y. Safety of intravenous immunoglobulin(IVIG) therapy. Autoimmun Rev 2007;6:257–9.
Please cite this article as: Bichuetti-Silva DC, et al, Immediate infusion-relacohort of 1765 infusions, Int Immunopharmacol (2014), http://dx.doi.org
[14] Stiehm ER. Adverse effects of human immunoglobulin therapy. Transfus Med Rev2013;27:171–8.
[15] Costa-Carvalho BT, Solé D, Condino-Neto A, Rosário Filho N. I Brazilian Consensusabout use of human immunoglobulin in patients with primary immunodeficiencyBrazilian Society of Allergy and Immunopathology. Rev Bras Alerg Imunopatol2010;33(3):104–16.
[16] Siegel J. The product: all intravenous immunoglobulins are not equivalent. Pharma-cotherapy 2005;25(11):78–84.
[17] Primary immunodeficiency diseases. Report of a WHO scientific group. Clin ExpImmunol 1997;109(1):1–28.
[18] Brennan VM, Salome-Bentley NJ, Chapel HM. Prospective audit of adverse reactionsoccurring in 459 primary antibody-deficient patients receiving intravenous immu-noglobulin. Clin Exp Immunol 2003;133:247–51.
[19] Chapel H, Geha R, Rosen F. Primary immunodeficiency diseases: an update. Clin ExpImmunol 2003;132:9–15.
[20] Wittstock M, Benecke R, Zettl UK. Therapy with intravenous immunoglobulins:complications and side-effects. Eur Neurol 2003;50:172–5.
[21] Pierce LR, Jain N. Risks associated with use of intravenous immunoglobulin. TransfusMed Rev 2003;17:241–51.
[22] BallowM. Clinical and investigational considerations for the use of IVIG therapy. AmJ Health Syst Pharm 2005;62(Suppl. 3):S12–8.
[23] Silvergleid AJ, Berger M. Intreavenous immune globulin: adverse effects. UpToDate,2013. Available from: www.uptodate.com. [Accessed February 28, 2014].
[24] Singh-Grewal D, Kemp A, Wong M. A prospective study of the immediate and de-layed adverse events following intravenous immunoglobulin infusions. Arch DisChild 2006;91:651–4.
[25] Andres E, Limbach FX, Kurtz JE, Kurtz-Illig V, Schaeverbeke T, Pflumio F, et al. Prima-ry humoral immunodeficiency (late-onset common variable immunodeficiency)with antinuclear antibodies and selective immunoglobulin deficiency. Am J Med2001;111:489–91.
[26] Cunningham-Rundles C, Bodian C. Common variable immunodeficiency: clinical andimmunological features of 248 patients. Clin Immunol 1999;92:34–48.
[27] Eisenstein EM, Sneller MC. Common variable immunodeficiency: diagnosis andmanagement. Ann Allergy 1994;73:285–92 [quiz 93–4].
[28] de Albuquerque Campos R, Sato MN, da Silva Duarte AJ. IgG anti-IgA subclasses incommon variable immunodeficiency and association with severe adverse reactionsto intravenous immunoglobulin therapy. J Clin Immunol 2000;20:77–82.
[29] Stangel M, Kiefer R, Pette M, Smolka MN, Marx P, Gold R. Side effects of intravenousimmunoglobulins in neurological autoimmune disorders—a prospective study. JNeurol 2003;250:818–21.
[30] Berger M, Pinciaro PJ. Flebogamma 5% Investigators. Safety, efficacy and pharmaco-kinetics of Flebogamma 5% for replacement therapy in primary immunodeficiencydiseases. J Clin Immunol 2004;24:389–96.
[31] Vieira DG, Costa-Carvalho BT, Silva R, HIX S, Sarni ROS. Evaluation of lipid profile andapolipoprotein A–T: relationship with enzymes associated with cardiovascular riskin patients with hypogammaglobulinaemia. 2014 CIS annual meeting: Primary Im-mune Deficiency Diseases North American Conference 2014, 34. , Journal of ClinicalImmunology; 2014. p. 357.
[32] Valente ECS, Paulina TL, Rafael MN, Sarni ROS, Costa-Carvalho BT, Silva R. Nutricionalstatus and food intake of patients with common variable immunodeficiency. RevBras Nutr Clin 2013;28(2):136–41.
[33] Lucas M, Lee M, Lortan J, Lopez-Granados E, Misbah S, Chapel H. Infection outcomesin patients with common variable immunodeficiency disorders: relationship to im-munoglobulin therapy over 22 years. J Allergy Clin Immunol 2010;125(6):1354–60.
[34] Berger M. Principles of and advances in immunoglobulin replacement therapy forprimary immunodeficiency. Immunol Allergy Clin North Am 2008;28:413–37.
[35] IDF. Immune Deficiency Foundation patient survey 2002. Available from: http://www.primaryimmune.org. [Accessed January 20, 2014].
[36] Orange JS, Hossny EM, Weiler CR, Ballow M, Berger M, Bonilla FA, et al. Use of intra-venous immunoglobulin in human disease: a review of evidence by members of thePrimary Immunodeficiency Committee of the American Academy of Allergy, Asthmaand Immunology. J Allergy Clin Immunol 2006;117(4):525–53.
[37] Fasth A. European Society for Immune Deficiency; October 2006 [Budapest,Hungary] - Oral Presentation.
[38] Gelfand EW, Winkelstein J. Are all IGIVs the same? J Allergy Clin Immunol 2002;110:938.
[39] Feldemeyer L, Benden C, Haile SR, Boehler A, Speich R, French LE, et al. Not all intra-venous immunoglobulin preparations are equally well tolerated. Acta DermVenereol 2010;90:494–7.
[40] Orbach H, Katz U, Sherer Y, Shoenfeld Y. Intravenous immunoglobulin. Adverse ef-fects and safe administration. Clin Rev Allergy Immunol 2006;29:173–84.
[41] Bonilla FA. Intravenous immunoglobulin: adverse reactions and management. J Al-lergy Clin Immunol 2008;122:1238–9.
[42] Shroeder Jr HW, Dougherty CJ. Review of intravenous immunoglobulin replacementtherapy trials for primary humoral immunodeficiency patients. Infection 2012;40:601–11.
[43] Ochs HD, LeeML, Fischer SA, Delson ES, Chang BS, Wedgwood RJ. Self-infusion of in-travenous immunoglobulin by immunodeficient patients at home. J Infect Dis 1987;156:652–4.
[44] Nicolay U, Kiessling P, Berger M, Gupta S, Yel L, Roifman CM, et al. Health-relatedquality of life and treatment satisfaction in North American patients with primaryimmunodeficiency diseases receiving subcutaneous IgG self-infusions at home. JClin Immunol 2006;26(1):65–72.
ted adverse reactions to intravenous immunoglobulin in a prospective/10.1016/j.intimp.2014.09.015