Embed Size (px)
Citation preview
![Page 1: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/1.jpg)
A
ode©
K
1
sAnitiaa
att
2
ebtio
s
0d
European Journal of Radiology 64 (2007) 3–14
Imaging of blunt cerebrovascular injuries
Clint W. Sliker ∗, Stuart E. Mirvis 1
Department of Diagnostic Radiology, University of Maryland Medical Center, 22 South Greene Street, Baltimore, MD 21043, USA
Received 5 February 2007; accepted 14 February 2007
bstract
Blunt cerebrovascular injuries are uncommon but potentially devastating injuries that can lead to stroke and death. While uncommon, appreciation
f the seriousness of these injuries, a high index of suspicion in high risk patients, and aggressive screening of multitrauma patients leads to earlyiagnosis of asymptomatic lesions that may be amenable to treatment prior to the onset of ischemia. The radiologist can play a vital role in thearly diagnosis, follow-up, and, in some cases, treatment of these challenging injuries.2007 Elsevier Ireland Ltd. All rights reserved.
sis
bsas
3
o[f1TtBr[oBwi
eywords: Blunt trauma; Carotid artery injury; Vertebral artery injury; Diagno
. Introduction
Historically, blunt cerebrovascular injuries (BCVI) were con-idered uncommon in the general blunt trauma population.lthough many of these lesions lead to stroke and death, diag-osis prior to onset of symptoms can be challenging. Withncreased appreciation of these injuries, increasing therapeu-ic options, and increasing access to ever advancing diagnosticmaging modalities, this group of injuries has received greaterttention in the trauma literature and from those caring forcutely traumatized patients.
The purpose of this article is to provide the radiologist withreview of blunt cerebrovascular injuries with special attention
o diagnosis and those clinical factors that impact diagnosis andhe radiologist’s role in patient management.
. Incidence
Blunt cerebrovascular injuries (BCVI) are generally consid-red uncommon injuries. Among all hospital admissions forlunt trauma, blunt carotid artery injuries (BCI) are encoun-
ered in 0.14–1.1% of patients [1–3] and blunt vertebral arterynjuries (BVI) are encountered in 0.4–0.53% [4,5]. Although theverall incidence of BCVI ranges from 1.1 to 1.4% [6,7] of all∗ Corresponding author. Tel.: +1 410 328 7968; fax: +1 410 328 8925.E-mail addresses: [email protected] (C.W. Sliker),
[email protected] (S.E. Mirvis).1 Tel.: +1 410 328 8845; fax: +1 410 328 8925.
tc
4
nt
720-048X/$ – see front matter © 2007 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.ejrad.2007.02.015
lunt trauma patients, it is more frequently diagnosed in moreeverely injured patients. For example, Mutze et al. [8] reportedn incidence as high as 2.7% in blunt patients with an injuryeverity score equal to or greater than 16.
. Outcomes
BCVIs result in high mortality and morbidity. For BCI, theverall mortality and morbidity rates are 17–38 and 32–67%1–3,5,7,9], respectively. Overall mortality and morbidity ratesor BVI are generally lower, although morbidity still ranges from4 to 24% [5,10] and mortality ranges from 8 to 18% [4,9].he high morbidity and mortality are, in part, attributable to
he severity of concurrent injuries frequently associated withCVI, although BCVI-specific mortality itself is high. In one
etrospective review of 22 patients with BCVI, McKevitt et al.11] reported a stroke rate of 60% and BCVI-specific mortalityf 25%. In a prospective study conducted by Cothren et al. [9],CI-specific mortality was 21%, while BVI-related mortalityas 18%. Moreover, reflecting a stroke’s globally deleterious
mpact on a patient, Cothren reported higher overall mortality inhose with BCVI-related stroke (32% for BCI and 18% for BVI)ompared to those without stroke (7% for both BCI and BVI).
. Mechanism of injury
Hyperextension and contralateral rotation of the head andeck, with the cervical internal carotid stretched against theransverse processes of the upper three cervical vertebrae, is
![Page 2: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/2.jpg)
4 C.W. Sliker, S.E. Mirvis / European Journal of Radiology 64 (2007) 3–14
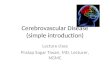
Fig. 1. A 82-year old woman with atlanto-occipital dissociation and bilateral vertebral artery injuries following motor vehicle collision. 3D volume rendered (a) andaxial images (b) obtained with whole-body multidetector computed tomography (WB-MDCT) protocol. Magnetic resonance angiogram (MRA) (c) and T1 weightedspin echo magnetic resonance image (MRI) (d). WB-MDCT demonstrates right vertebral artery segmental occlusion from C1 to foramen magnum (curved arrow),focal left vertebral artery central narrowing from intramural hematoma at level of foramen magnum, and bare occipital condyles (asterisks). MRA demonstratesabsent flow in distal right vertebral artery with focal narrowing of injured left vertebral artery (arrow). Left vertebral artery high T1 signal (arrowhead) indicatesintramural hematoma from dissection.
![Page 3: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/3.jpg)
n Journal of Radiology 64 (2007) 3–14 5
cscie(m
tdstC
5
susHapi
rritaapbv
Table 1Authors’ institutional guidelines for identifying trauma patients at high risk forblunt cerebrovascular injury
1. Cervical spine fracture withA. Foramen transversarium involvement, orB. 30% or more subluxation, orC. Significant rotation or distraction mechanism (e.g. unilateral interfacetal
dislocation, atlanto-occipital distraction, etc.)
2. Basilar skull fracture crossing carotid canal, foramen lacerum, or cavernoussinus
3. Severe facial fractures (LeFort II or III; naso-orbital ethmoid complex, facialsmash)
4. Carotid or vertebral artery perivascular hematoma by CT or MD-CTA5. Horner’s syndrome6. Glasgow Coma Score ≤ 6 at 24 h after initial assessment7. Neurologic examination incongruent with brain imaging8. Stroke or transient ischemic attack9. Hanging attempt with cervical hematomas or cervical spine fractures
CaC
dI[IcBUwa
Fr(
C.W. Sliker, S.E. Mirvis / Europea
onsidered the most common cause of BCI [12]. Also, exten-ion of basilar skull fractures through the carotid canal mayause petrous carotid injury [12]. Less common causes of BCInclude a direct blow to the neck (e.g. assault, near hanging,tc.) [12] and intraoral trauma from either a hard foreign objecte.g. falling against a toothbrush) [12] or posteriorly displacedandible fracture fragments [13].Since most of the vertebral arteries are fixated within the
ransverse foramina, they are vulnerable to injuries induced byisplaced bone fragments or stretching related to rotation andubluxation [14,15]. In cases of craniocervical junction distrac-ion or dislocation, the vertebral arteries may be crushed against1 [14] or stretched over the dura [16] (Fig. 1).
. Clinical presentation and associated injuries
The diagnosis of BCVI is typically suspected in patients pre-enting with overt signs of fixed neurologic deficits that arenexplained by cerebral computed tomography (CT). Otherigns, such as transient ischemic attacks, neck hematomas,orner’s syndrome, or cervical carotid bruit, also suggest BCVI,
lthough they can be difficult to identify in the acute multitraumaatient [17], especially those with concomitant traumatic brainnjury.
Several studies suggest prompt treatment reduces BCVI-elated stroke and mortality rates [4,5,7,18]. To this end, severaletrospective studies have described numerous clinical andmaging findings that may serve as triggers for screening of bluntrauma patients for BCVI [5,11,12,17,19–22]. Table 1 lists theuthors’ institutional guidelines for predicting BCVI. Despite
lack of consensus regarding the most significant independentredictors for BCVI, it has been shown that the greater the num-er of risk factors, the greater the likelihood of an associatedascular injury [12].snom
ig. 2. A 40-year old with persistent low Glasgow Coma Score following motor vehiestricted diffusion related to diffuse axonal injury (curved arrows). (b) MRA demoarrowheads).
T, Computed tomography; MD-CTA, multidetector computed tomographicngiography. References: Lee et al. [16], Miller et al. [19], Kerwin et al. [20],othren et al. [21], Mirvis et al. [23] and Parbhoo et al. [24].
Many proposed predictors of BCVI can be readily identifieduring routine imaging of acutely injured patients [11,17,22].n a retrospective review of 75 patients with BCVI, Biffl et al.22] identified diffuse axonal injury (DAI) (Fig. 2), LeFort II orII fractures (Fig. 3), and petrous temporal bone fractures witharotid canal extension (Fig. 4) as independent risk factors forCI. Retrospective studies conducted by Berne et al. [25] andtter et al. [17] support the association of skull base fracturesith BCVIs. BVI and cervical spine injury have been strongly
ssociated in several studies [4,7,10,21,17,22,24,26]. In one
tudy [4], 38 patients with BVI were 11 times more likely thanot to have a cervical spine injury. In another study [21], 77%f patients with BVIs demonstrated cervical spine injuries, withost exhibiting either fracture involving a transverse foramencle collision. Diffusion weighted brain MRI (a) demonstrates corpus callosumnstrates distal cervical segment internal carotid artery (ICA) pseudoaneurysm
![Page 4: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/4.jpg)
6 C.W. Sliker, S.E. Mirvis / European Journal of Radiology 64 (2007) 3–14
F h. 3Di ion (MI
(Cts
fi
GB
Fc
ig. 3. A 44-year old male imaged with WB-MDCT following motor cycle crasnclude LeFort II and III patterns (arrowheads). Sagittal multiplanar reconstructCA just distal to carotid bulb (arrow).
Fig. 5), subluxation or dislocation, or injury level at C1 to3. Parbhoo et al. [24] report a high frequency of BVIs among
hose with unilateral facet dislocations, which is an associationupported by the authors’ experience.
Some significant clinical risk factors can be inferred byndings on routine imaging. For example, a very low (≤8)
ita(
ig. 4. A 23-year old with skull base fractures following motor vehicle collision. Carotid canal (arrowheads). (b) Angiogram demonstrates petrous ICA (curved arrow)
volume rendered image (a) of face demonstrates extensive facial fractures thatPR) (b) demonstrates characteristic short-tapered post-traumatic occlusion of
lasgow Coma Score (GCS) [11,22] has been associated withCVI. Severe traumatic brain injury revealed by cerebral
maging may suggest a low GCS, and then allow the radiologisto propose evaluation for BCVI. Similarly, a high (≥3) thoracicbbreviated injury score (AIS) [11] has been linked to BCVIFig. 6). Since imaging plays the primary role in determining
omputed tomography (CT) (a) demonstrates displacement of fragments intoand cavernous ICA (arrow) pseudoaneurysms.
![Page 5: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/5.jpg)
C.W. Sliker, S.E. Mirvis / European Journal of Radiology 64 (2007) 3–14 7
F e follC ow) (bv days
tieri
BABcwsm
atss
6
c
ig. 5. A 22-year old male with vertebral artery injury induced brainstem strok6 left transverse process fractures involving foramen transversarium (black arrertebral artery (white arrow). Diffusion weighted (c) brain MRI performed 10
he thoracic AIS, if the radiologist diagnoses severe thoracicnjuries, he/she may then initiate the appropriate diagnosticvaluation for BCVI. Through awareness of the full spectrum ofisk factors for BCVI, the radiologist may be the first to considerts presence, thereby facilitating early diagnosis and treatment.
It is important to note that a large number of patients withCVI do not manifest any of the reported markers of injury.ccording to Biffl et al., approximately 20% of patients withCVI exhibit no recognized risk factors, and injuries are initially
linically occult [10] (Fig. 7). Supporting Biffl’s data, recentork by Stein et al. [42] found no major craniofacial or cervicalpine injury in 27% of 85 patients diagnosed with BCVI. As aeans to diagnose the large number patients with truly occult
csw(
owing motor vehicle collision. Admission cervical spine CT (a) demonstrates) and angiogram demonstrates associated abrupt occlusion of the proximal left
later demonstrates rostral brain stem infarct (arrowhead).
cute injuries and limit resultant stroke, some [8] have suggestedhe routine use of computed tomographic angiography (CTA) toimultaneously examine the cervical spine and cervical arterialystem during assessment of acute multitrauma patients.
. Location and types of vascular injury
Blunt cerebrovascular injuries may occur anywhere along thearotid and vertebral artery distributions, and evaluation of both
irculations from their origins through their intracranial water-heds is vital. However, coinciding with the frequent associationith cervical spine injuries, most BVIs occur at the foraminali.e. V2) vertebral artery segments [26]. As predicted by the
![Page 6: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/6.jpg)
8 C.W. Sliker, S.E. Mirvis / European Journal of Radiology 64 (2007) 3–14
F r vehd t ICA
dcdb
ig. 6. A 39-year old male scanned with WB-MDCT protocol following motoemonstrate a traumatic aortic injury with pseudoaneurysm (arrowheads), a righ
ominant mechanism of injury, BCIs typically affect the internalarotid artery just below the skull base [C.W. Sliker, unpublishedata], although a significant number occur at or above the skullase [12].
tv[
icle collision. 3D volume rendered image of the chest (a) and neck (b and c)dissection (black arrow), and a right vertebral artery dissection (white arrow).
Notably, a large number of those with BCVI manifest morehan one injured vessel (Figs. 1 and 6). Multiarterial injury, inarious combinations, has been reported in 18–38% of cases18,20,27,28]. Given the violent and complicated force vectors
![Page 7: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/7.jpg)
C.W. Sliker, S.E. Mirvis / European Journal of Radiology 64 (2007) 3–14 9
Fig. 7. A 17-year old with female with femur fracture (not shown) and ICA injury following motor vehicle collision. Admission WB-MDCT (not shown) demonstratednarrowed distal left ICA cervical segment. Coronal maximum intensity projection (MIP) computed tomography angiogram (CTA) image (a) acquired day #2demonstrates left ICA pseudoaneurysm (white arrow) and normal adjacent lumen. Coronal MIP CTA image (b) acquired day #7 and angiogram acquired day #9(c) demonstrate larger pseudoaneurysm (black arrow) and near occlusion of adjacent ICA lumen (white arrowheads). Angiogram acquired after endovascular stentplacement (d) demonstrates normal ICA lumen (black arrowheads) and minimal pseudoaneurysm filling (curved arrow).
![Page 8: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/8.jpg)
10 C.W. Sliker, S.E. Mirvis / European Jour
Table 2Biffl blunt cerebrovascular injury grading system
Injury grade Description
I Luminal irregularity (i.e. intimal injury) or dissection with<25% luminal narrowing
II Dissection or intraluminal hematoma with ≥25% luminalnarrowing, intraluminal thrombus, raised intimal flap, orhemodynamically insignificant AVF
III PseudoaneurysmIV OcclusionV
A
riicalp
atdmaDm(isflitpnst
afwwtppdps
7
7
rt
toweafrpsSBrMCupu
7a
uacptrtlratscft
wCtbpTwaepWcu
7
Transection or hemodynamically significant AVF
VF, Arteriovenous fistula. Reference: Biffl et al. [27].
esponsible for many cases of multitrauma, this is not a surpris-ng injury characteristic. Given the propensity for multivesselnjuries, care should be taken to thoroughly assess all four vas-ular distributions during diagnostic imaging, especially duringngiography when one may be tempted to limit the evaluation toess than a complete four-vessel study in an attempt to avoid theotential consequences of progressive catheter manipulations.
The forms of injuries identified in the carotid and vertebralrteries are similar to those encountered in arteries elsewhere inhe body. Typical types of injury include intimal injury, spasm,issection with intramural hematoma, raised intimal flap, intra-ural hematoma, pseudoaneurysm, occlusion, transection with
ctive hemorrhage, and arteriovenous fistulae (AVF) [16,29,30].issections may vary in degree of luminal compromise frominimal to near occlusion. Combinations of injury can be seen
e.g. pseudoaneurysm with dissection, raised intimal flap withntraluminal thrombus, etc.) in the same artery. With occlu-ion or high grade luminal narrowing, inadequate collateralow and/or hypotension can lead to arterial insufficiency and
schemia, while intimal injury may promote platelet aggrega-ion and embolization [12]. Pseudoaneurysms may promotelatelet aggregation with distal embolization or compress theative vessel lumen [31] with resultant downstream underperfu-ion. Rarely, pseudoaneurysm rupture or transaction may leado ischemia or hemodynamic compromise [12].
In an effort to the predict risk of stroke, Biffl et al. [29] devisedblunt carotid artery injury grading scale based on the anatomic
eatures of injury. In a subsequent report [27], the scale (Table 2)as revised to include AVFs, and it was used to grade BVIs asell as BCIs. When BCVIs are reported with the Biffl scale,
he highest grade injury identified determines the score for thatarticular vessel. At the authors’ institution, all injuries in aarticular vessel are described, although only one may be used toetermine overall grade of injury. In addition to providing somerognostic information, the grading scale is a useful reportinghorthand that is easily understood by the traumatologist.
. Diagnosis of BCVI
.1. Angiography
Four-vessel cervicocerebral angiography is considered theeference standard for diagnosing BCVI [10,20]. As an invasiveest, angiography carries an inherent risk of serious complica-
a
o
nal of Radiology 64 (2007) 3–14
ions, including stroke and hemorrhage. Yet, with experiencedperators, routine angiographic assessment of trauma patients,ho are generally young and without pre-existing vascular dis-
ase, is a safe procedure. For example, in one report by Cothren etl. [9], 727 blunt trauma patients were angiographically screenedor BCVI, and there was one instance (0.1%) of angiography-elated stroke and two cases (0.3%) of conservatively-manageduncture-site hematomas. In those in whom BCVI is stronglyuspected clinically, the risks would seem to be tolerable.till, in a screening population without hard clinical signs ofCVI, many may consider potential complications of angiog-
aphy unacceptable given the relative rarity of these injuries.oreover, angiography is also expensive and resource intensiveonsequently, other diagnostic modalities, including Dopplerltrasound, magnetic resonance angiography (MRA), and com-uted tomographic angiography (CTA), are being increasinglysed to diagnose BCVI.
.2. Multidetector computed tomographicngiography—scanning options
Computed tomography (CT) is an important tool commonlysed to evaluate multitrauma patients for head, spine, chest,bdomen, and pelvic injuries. With the advances in multidetectoromputed tomography (MDCT) technology, multidetector com-uted tomographic angiography (MD-CTA) is increasingly usedo evaluate the arterial systems throughout the body, and, recenteports describe it use to diagnose BCVI [6,7,17,32,33]. Withhe use of MDCT, routine diagnosis of BCVI does not need to beimited only to scans targeted to the craniocervical region. Cur-ent MDCT scanners, used in concert with contrast bolus timing,llow continuous scanning through all regions of interest in theypical multitrauma patient. Utilization of whole-body MDCTcanning techniques permits simultaneous detection of cranio-ervical vascular, skeletal, thoracic, and organ injuries whileorgoing the scanning time and excess radiation [34] inherent toraditional segmental scanning techniques.
In the authors’ trauma center, targeted neck MD-CTA andhole-body MDCT have been performed for over 3 years.urrently, both 16- and 40-detector row scanners are in use,
hough the 40-detector row scanner is preferred for most whole-ody and neck MD-CTA scans (Table 3). In most multitraumaatients, the whole-body scanning protocol is routinely used.he targeted neck MD-CTA protocol is utilized in those caseshere clinical interest is directed entirely to the cranicocervical
rterial system, in addition to cases where the patient is consid-red at risk for harboring a BCVI and the whole-body MDCTrovided suboptimal or equivocal evaluation of the neck vessels.ith both protocols, advanced post-processing techniques (e.g.
urved multiplanar reconstructions, volume rendering, etc.) aresed liberally on an as needed basis.
.3. Multidetector computed tomographic
ngiography—diagnostic accuracyThe relatively few studies that have investigated the accuracyf CTA when used to diagnose BCVI are limited by small cohorts
![Page 9: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/9.jpg)
C.W. Sliker, S.E. Mirvis / European Journal of Radiology 64 (2007) 3–14 11
Table 3A 40-detector row MDCTa scanning protocols for evaluating craniocervical arterial system
Parameter Whole-body MDCT protocol Neck MD-CTA protocol
Patient positioning Arms extended superiorly over head Arms at his/her sidesDetector configuration and collimation 40 mm × 0.625 mm 40 mm × 0.625 mmPitch 0.926 0.67Rotation time 0.5 s 0.5 skV 120 120mA 250 400Area scanned Circle of Willis to lung bases (or ischial tuberosities) Vertex to aortic archContrast Iohexol (350 mg I/mL) Iohexol (300 mg I/mL)Contrast volume 100 mL contrast, 50 mL saline push 100 mL contrast, 50 mL saline pushContrast injection rate 6 mL/s for 60 mL, then 4 mL/s for 40 mL
(contrast followed by saline push)4 mL/s (contrast followed by saline push)
Scan trigger threshold 90 HUb Time to peak cervical ICA enhancement + 2 sc
Axial images (thickness × interval) 2 mm × 2 mm 1 mm × 0.5 mmSagittal and coronal MPR images (thickness × interval) 2 mm × 2 mm 2 mm × 2 mmSagittal and coronal MIP images (thickness × interval) n/a 5 mm × 2 mmThin section axial images to independent workstation
(thickness × interval)2 mm × 1 mm 1 mm × 0.5 mm
n/a, MIP images through neck not part of routine whole-body MDCT protocol. MDCT, Multidetector computed tomography; MD-CTA, multidetector computedtomographic angiography; MPR, multiplanar reconstruction; MIP, maximum intensity projection.
a Philips Brilliance-40 scanner (Philips Medical Systems, Cleveland, OH, USA).b Bolus Pro triggering system (Philips Medical Systems) with region of interest at the distal ascending aorta.
t plac
oey4iBsspwirwniiapdatpmM4vwpisMa
felde
7
nw1aawdwB1tt
Bnimat
c Based on test injection of 15 mL of contrast at 4 mL/s with region of interes
f injured patient and varied study designs. Compared to the ref-rence standard, angiography, reports of single-slice spiral CTAielded disappointing results; sensitivities for BCI and BVI were7–68% [10,19] and 53% [10], respectively. Recently, studiesnvestigating the accuracy of MD-CTA have emerged. In 2006,iffl et al. [32] and Berne et al. [6] reported their experience
creening 331 and 435 patients, respectively, for BCVI with 16-lice MD-CTA. In both studies, injuries (combined total of 42atients) were confirmed with angiography while those patientsith normal (i.e. no BCVI) MD-CTA results were followed clin-
cally for signs of neurovascular complications. Neither groupeported delayed neurological complications of BCVI in thoseith normal MD-CTA examinations, though neither followedormal MD-CTA examinations with angiography. Therefore,n both reports, true accuracy of 16-slice MD-CTA for detect-ng BCVI was not determined. In a prospective study that alsoppeared in 2006, Eastman et al. [33] evaluated 146 at-riskatients with both 16-slice MD-CTA and angiography, and theyetermined 16-slice MD-CTA to have a sensitivity of 97.7%nd specificity of 100% when used to diagnose BCVI. Despitehese impressive results, the BCVI cohort consisted of only 43atients [33], which is a small number when studying an uncom-on entity; this is a limitation shared by the other two studies.oreover, Eastman et al. [33] report only 46 injuries in the
3 patients diagnosed with BCVI, which is far from the pre-iously reported multivessel injury rate of 18–32% in patientsith BCVI [18,20,28], Although the results of this study areromising, the small cohort of injured patients and the atyp-
cally small number of patients with multiple injured vesselsuggest the data may not reflect the true accuracy of 16-sliceD-CTA when used to evaluate to the blunt trauma populationt large for BCVI. Controversies not withstanding, the authors
pnCt
ed over internal carotid artery at C4 level.
eel that MD-CTA (16-slice or greater) plays a valuable role invaluating patients with suspected BCVI, but, until proven by aarge (preferably multicenter and prospective) trial, the authorso not think that MD-CTA should be considered diagnosticallyquivalent to angiography.
.4. Magnetic resonance angiography
Few studies have assessed the diagnostic accuracy of mag-etic resonance angiography (MRA) relative to angiographyhen used to detect BCVI. In one study by Biffl et al. [10],6 patients at risk for BCVI were examined with both MRA andngiography. Angiography confirmed BCVI in three patients,nd the collective sensitivity and specificity of MRA for BCVIere 75 and 67%, respectively. In a slightly larger study con-ucted by Miller et al. [19] 21 at-risk patients were examinedith both MRA and angiography. Among the four patients withCI, the sensitivity of MRA was 50% and its specificity was00%. Vertebral artery injuries were found in 17 patients, andhe sensitivity and specificity of MRA were 47 and 97%, respec-ively.
Though its sensitivity is limited, the use MRA to diagnoseCVI has several potential advantages relative to other diag-ostic options. Among them, the examination does not utilizeonizing radiation or require intravenous contrast. However, in
ost centers, magnetic resonance (MR) imaging is not as rapidlyccessible as CT. In addition to the time and personnel requiredo transport the patient to the MR suite, which is remote from
atient care areas in many centers, the MR environment itself isot conducive to the management of the acutely injured patient.onsequently, even if future well-designed studies demonstratehat contemporary MRA techniques have diagnostic accuracies
![Page 10: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/10.jpg)
1 n Jour
cpMutti
7
pDmuetiibsadoaosuomiu
8
liratfbCptItfirm
arap
imficfmitdrm
9
ftmiltmoatcc6(htpo
srts[pwnadp2dwsatc
2 C.W. Sliker, S.E. Mirvis / Europea
omparable or exceeding those of CTA, the authors feel that thehysical limitations of MRA should limited it use in favor ofD-CTA (16 detector row or greater) or angiography, with the
se of MRA relegated to instances when the other two diagnos-ic options are unavailable, their results are equivocal, or whenhe use of iodinated contrast material and/or ionizing radiations contraindicated.
.5. Sonography
Although operator dependent, ultrasound is a portable, inex-ensive tool in common use by traumatologists, and Duplexoppler techniques are established means for diagnosing andonitoring non-traumatic cerebrovascular disease. Therefore,
ltrasound is an attractive option for diagnosing BCVI. How-ver, since the intracranial internal carotid arteries and most ofhe vertebral arteries are encompassed by bony canals, the abil-ty of ultrasound to detect potentially significant injuries (e.g.ntimal flaps, pseudoaneurysms) without associated flow distur-ances can be limited. The few studies that have discussed theensitivity of Doppler ultrasound for detecting BCVI report dis-ppointing results. In one early study [35], Doppler ultrasoundiagnosed 14 patients with BCI within the neck for a sensitivityf 86%, although it missed two injuries near the skull base. Inmore recent study, Mutze et al. [8] detected BCVI in 0.9%
f 1471 patients screened with Doppler ultrasound with sen-itivity of only 38.5%. The eight patients in whom Dopplerltrasound missed injury came to clinical attention as resultf cerebrovascular ischemia, supporting the notion that injuriesissed by sonography are potentially significant. Given its lim-
tations, Doppler ultrasound should only be utilized when these of other imaging techniques is impossible.
. Injury evolution
Both blunt carotid and vertebral arteries tend to be dynamicesions. That is, over the course of days or weeks, the sever-ty of both treated and untreated lesion may either progress oregress. In their review of 114 carotid artery and 65 vertebralrtery injuries followed with angiography 7–10 days after sus-aining injury, Biffl et al. [27] noted that grade I and II injuriesrequently healed by initial follow-up, and therapy could thene discontinued in 57% of grade I and 8% of grade II lesions.onversely, 8% of grade I lesions and 43% of grade II lesionsrogressed, leading to more aggressive therapeutic interven-ions. Ninety-three percent of grade III injuries and 82% of gradeV injuries were unchanged, although in the authors’ experience,hese lesions, especially carotid injuries, change with greaterrequency. Notably, Biffl et al. noted no significant differencen injury progression or regression among patient populationseceiving systemic anticoagulation, antiplatelet therapy, or noedical therapy [27].At the authors’ trauma center, blunt cerebrovascular injuries
re followed with the imaging modality that most satisfacto-ily characterized it during the initial work-up; this is usuallyn MDCT angiogram. The first follow-up imaging is typicallyerformed between 24 and 72 h after initial diagnosis. Dur-
fudo
nal of Radiology 64 (2007) 3–14
ng this brief interval, BCVI frequently change enough to alteranagement, which is particularly important given the relative
requency of coexisting injuries (e.g. unstable cervical spinenjury requiring surgery, major visceral injury, etc.) that mayomplicate treatment with anti-thrombotic agents. A secondollow-up examination is usually obtained within 1 week to 1onth (Fig. 7a and b). Beyond this point, the timing of repeat
maging is generally based on injury morphology and responseo management. Uncommonly, rapid morphologic changes ren-er differentiation between injury progression and vascularemodeling associated with healing difficult, and, in these cases,ore frequent follow-up imaging can be especially useful.
. Treatment
Though treatment of some BCVI may be impossible orruitless due to early extensive stroke or other contraindica-ions (e.g. intracranial hemorrhage, spinal cord injury) [36],
ultiple authors have suggested that treatment with either med-cal therapy or endovascular techniques can either prevent orimit BCVI-related neurologic deficits [2–5,18,19,37,38]. Tohis date, the optimum treatment regimen has yet to be deter-
ined, but the current trend is towards medical therapy asption of choice. Many consider anticoagulation first line ther-py [2–5,9,18,19,29], with antiplatelet therapy reserved forhose with contraindications to anticoagulation. In one studyonducted by Miller et al. [5], timely treatment with either anti-oagulation or antiplatelet therapy lowered stroke incidence to% in patients diagnosed with BCI and to 0% in those with BVIcompared to 50% for both untreated BCI and BVI). Antiplateletas been proposed by others [37] to exhibit efficacy comparableo anticoagulation while reducing the risk of hemorrhagic com-lications. At this time, the superiority of one approach over thether is unproven.
Of special interest to radiologists, endovascular repair withtent placement has been used to treat BCIs when lesions areefractory to medical therapy [31,38] (Fig. 7c and d), medicalherapy is contraindicated [38], or either angiography or perfu-ion imaging demonstrates evidence of cerebral hypoperfusion38]. In a study reported by Cohen et al. [38], 10 patients withost-traumatic cervical internal carotid artery (ICA) dissectionsere treated with endovascular stent placement. There wereo procedure-related complications or stent occlusions, andt a mean clinical follow-up time of 16 months four patientsemonstrated no deterioration in neurologic status while sixatients improved. In contrast, Cothren et al. [39] reported a1% complication rate (three strokes and one subclavian arteryissection) and an occlusion rate of 45% among 23 patientsith post-traumatic cervical ICA pseudoaneurysms treated with
tents. In a cohort of 18 patients who received only medical ther-py, none suffered stroke or progressive deficit after initiation ofreatment, and one suffered carotid artery occlusion despite anti-oagulation. Interestingly, this report contradicts an earlier one
rom the same institution, in which Coldwell et al. [31] describedncomplicated endovascular treatment of cervical ICA pseu-oaneurysms in 14 patients in whom a mean clinical follow-upf 16 months revealed no evidence of stroke or delayed stent![Page 11: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/11.jpg)
n Jour
crwrasCB
dtmirarptaaepsoa
1
aiiBiBltrooiatpeti
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
C.W. Sliker, S.E. Mirvis / Europea
omplication. It must be noted that in Cohen’s study, all patientseceived antiplatelet therapy with aspirin and clopidogrel [38],hile those suffering stent occlusion in Cothren’s study only
eceived anticoagulation [39], thereby suggesting that thentiplatelet therapy either alone or in combination with thetents contributed to the more promising results reported byohen. Clearly, the role and methods of endovascular repair ofCI remain areas in need of continued investigation.
Endovascular therapy of vertebral artery injuries is also aiagnostic option. Although emergent coil embolization of ver-ebral artery transections is an appropriate approach [40], the
erits of a comparable approach to less severe injuries remainncompletely explored. Since Biffl et al. [27] suggest the highestate of BVI-related stroke (38%) occurs with grade II injuries,nd up to 75% of traumatic vertebral artery occlusions canecanalize [24], coil embolization of occluded vessels has beenroposed [41] to prevent reconstitution and the risk of dis-al thromboembolization. While this approach may pose nodditional harm to the patient, its long term merits measuredgainst those of medical therapy and the immediate risks of anndovascular procedure are unproven. Although dissections andseudoaneurysms can be addressed with endovascular occlu-ion, this should be done with caution with documentationf adequate collateral flow through the contralateral vertebralrtery and circle of Willis established.
0. Conclusion
Blunt cerebrovascular injuries are infrequently encountered,nd a high index of suspicion coupled with understanding ofnjury mechanism and recognition of associated injuries facil-tates early diagnosis and treatment of asymptomatic lesions.ased on available resources, each institution must determine
n what setting and with what means will the evaluation forCVI be initiated. Although its accuracy remains unproven,
iberal screening with 16-slice (or higher) MD-CTA facili-ates early diagnosis and treatment. In cases where MD-CTAesults are suspicious, equivocal or normal in high-risk patients,r clearly positive in those whom endovascular therapy is anption, prompt follow-up with four-vessel cerebral angiographys recommended. Regardless of the diagnostic and therapeuticpproaches utilized to address blunt cerebrovascular injuries,he authors advocate that institutions caring for blunt traumaatients adopt a coordinated and systematic approach in orderfficiently utilize resources while optimizing the outcomes ofhose diagnosed with these uncommon but potentially devastat-ng injuries.
eferences
[1] Carillo EH, Osborne DL, Spain DA, et al. Blunt carotid artery injuries:difficulties with the diagnosis prior to neurologic event. J Trauma1999;46(6):1120–5.
[2] Fabian TC, Patton JH, Croce MA, et al. Blunt carotid injury: importance ofearly diagnosis and anticoagulant therapy. Ann Surg 1996;223(5):513–25.
[3] Biffl WL, Moore EE, Ryu RK, et al. The unrecognized epidemic of bluntcarotid arterial injuries: early diagnosis improves neurologic outcome. AnnSurg 1998;228(4):462–70.
[
nal of Radiology 64 (2007) 3–14 13
[4] Biffl WL, Moore EE, Elliott JP, et al. The devastating potential of bluntvertebral arterial injuries. Ann Surg 2000;231(5):672–81.
[5] Miller PR, Fabian TC, Bee TK, et al. Blunt cerebrovascular injuries: diag-nosis and treatment. J Trauma 2001;51(2):279–85.
[6] Berne JD, Reuland KS, Villarreal DH, et al. Sixteen-slice multi-detectorcomputed tomographic angiography improves the accuracy of screeningfor blunt cerebrovascular injury. J Trauma 2006;60(6):1204–9.
[7] Schneidereit NP, Simons R, Nicolaou S, et al. Utility of screening for bluntvascular neck injuries with computed tomographic angiography. J Trauma2006;60(1):209–15.
[8] Mutze S, Rademacher G, Matthes G, Hosten N, Stengel D. Blunt cere-brovascular injury in patients with blunt multiple trauma: diagnosticaccuracy of duplex Doppler US and early CT angiography. Radiology2005;237(3):884–92.
[9] Cothren CC, Moore EE, Ray Jr EC, et al. Screening for blunt cerebrovas-cular injuries is cost-effective. Am J Surg 2005;190(6):845–9.
10] Biffl WL, Ray Jr CE, Moore EE, et al. Noninvasive diagnosis of bluntcerebrovascular injuries: a preliminary report. J Trauma 2002;53(5):850–6.
11] McKevitt EC, Kirkpatrick AW, Vertesi L, Granger R, Simon RK. Bluntvascular neck injuries: diagnosis and outcomes of extracranial vessel injury.J Trauma 2002;53(3):472–6.
12] Biffl WL, Moore EE, Offner PJ, Burch JM. Blunt carotid and vertebralarterial injuries. World J Surg 2001;25(8):1036–43.
13] Yang WG, Chen CT, de Villa GH, Lai JP, Chen YR. Blunt internalcarotid artery injury associated with facial fractures. Plast Reconstr Surg2003;111(2):789–96.
14] Schneider RC, Crosby EC. Vascular insufficiency of brain stem and spinalcord in spinal trauma. Neurology 1959;9:643–56.
15] Carpenter S. Injury of neck as cause of vertebral artery thrombosis. JNeurosurg 1961;18:849–53.
16] Lee CL, Woodring JH, Walsh JW. Carotid and vertebral artery injury insurvivors of atlanto-occipital dislocation: case reports and literature review.J Trauma 1991;31(3):401–7.
17] Utter GH, Hollingworth W, Hallam KD, Jarvik JG, Jurkovich GJ. Sixteen-slice CT angiography in patients with suspected blunt carotid and vertebralartery injuries. J Am Coll Surg 2006;203(6):838–48.
18] Cothren CC, Moore EE, Biffl WL, et al. Anticoagulation is the gold stan-dard therapy for blunt carotid injuries to reduce stroke rate. Arch Surg2004;139(5):540–5.
19] Miller PR, Fabian TC, Croce MA, et al. Prospective screening for bluntcerebrovascular injuries: analysis of diagnostic modalities and outcomes.Ann Surg 2002;236(3):386–93.
20] Kerwin AJ, Bynoe RP, Murray J, et al. Liberalized screening for bluntcarotid and vertebral artery injuries is justified. J Trauma 2001;51(2):308–14.
21] Cothren CC, Moore EE, Biffl WL, et al. Cervical spine fracture pat-terns predictive of blunt vertebral artery injury. J Trauma 2003;55(5):811–3.
22] Biffl WL, Moore EE, Offner PJ, et al. Optimizing screening for bluntcerebrovascular injuries. Am J Surg 1999;178(6):517–22.
23] Mirvis SE, Shanmuganathan S, Buell J, Rodriguez A. Use of spiral com-puted tomography for the assessment of blunt trauma patients with potentialaortic injury. J Trauma 1998;45(5):922–30.
24] Parbhoo AH, Govender S, Corr P. Vertebral artery injury in cervical spinetrauma. Injury 2001;32(7):565–8.
25] Berne JD, Norwood SH, McAuley CE, Vallina VL, Creath RG, McLartyJ. The high morbidity of blunt cerebrovascular injury in an unscreenedpopulation: more evidence of the need for mandatory screening protocols.J Am Coll Surg 2001;192(3):314–21.
26] Torina PJ, Flanders AE, Carrino JA, et al. Incidence of vertebral arterythrombosis in cervical spine trauma: correlation with severity of spinalcord injury. AJNR Am J Neuroradiol 2005;26(10):2645–51.
27] Biffl WL, Ray CE, Moore EE, et al. Treatment-related outcomes from blunt
cerebrovascular injuries: importance of routine follow-up arteriography.Ann Surg 2002;235(5):699–706.28] Berne JD, Norwood SH, McAuley CE, Villareal DH. Helical computedtomographic angiography: an excellent screening test for blunt cerebrovas-cular injury. J Trauma 2004;57(1):11–7.
![Page 12: Imaging of blunt cerebrovascular injuriesh24-files.s3.amazonaws.com/110213/294865-HiWHX.pdfclinically occult [10] (Fig. 7). Supporting Biffl’s data, recent work by Stein et al](https://reader033.dokumen.tips/reader033/viewer/2022060217/5f0670797e708231d4180063/html5/thumbnails/12.jpg)
1 n Jour
[
[
[
[
[
[
[
[
[
[
[
[
[
4 C.W. Sliker, S.E. Mirvis / Europea
29] Biffl WL, Moore EE, Offner PJ, Brega KE, Franciose RJ, Burch JM. Bluntcarotid arterial injuries: implications of a new grading scale. J Trauma1999;47(5):845–53.
30] Nunez Jr DB, Torres-Leon M, Munera F. Vascular injuries of the neckand thoracic inlet: helical CT-angiographic correlation. RadioGraphics2004;24(4):1087–98.
31] Coldwell DM, Novak Z, Ryu RK, et al. Treatment of posttraumatic inter-nal carotid arterial pseudoaneurysm with endovascular stents. J Trauma2000;48(3):470–2.
32] Biffl WL, Egglin T, Benedetto B, Gibbs F, Cioffi WG. Sixteen-slicecomputed tomographic angiography is a reliable noninvasive screeningtest for clinically significant blunt cerebrovascular injuries. J Trauma2006;60(4):745–51.
33] Eastman AL, Chason DP, Perez CL, McAnulty AL, Minei JP. Com-puted tomographic angiography for the diagnosis of blunt cervical vascularinjury: is it ready for primetime? J Trauma 2006;60(5):925–9.
34] Ptak T, Rhea JT, Novelline RA. Radiation dose is reduced with a
single-pass whole-body multi-detector row CT trauma protocol comparedwith a conventional segmented method: initial experience. Radiology2003;229(3):902–5.35] Cogbill TH, Moore EE, Meissner M, et al. The spectrum of blunt injury tothe carotid artery: a multicenter perspective. J Trauma 1994;37(3):473–9.
[
nal of Radiology 64 (2007) 3–14
36] Mayberry JC, Brown CV, Mullins RJ, Velmahos GC. Blunt carotid arteryinjury: the futility of aggressive screening and diagnosis. Arch Surg2004;139(6):609–12.
37] Wahl WL, Brandt MM, Thompson BG, Taheri PA, Greenfield LJ.Antiplatelet therapy: an alternative to heparin for blunt carotid injury. JTrauma 2002;52(5):896–901.
38] Cohen JE, Ben-Hur T, Rajz G, Umansky F, Gomori JM. Endovascularstent-assisted angioplasty in the management of traumatic internal carotidartery dissection. Stroke 2005;36(4):e45–7.
39] Cothren CC, Moore EE, Ray CE, et al. Carotid artery stents for bluntcerebrovascular injury: risks exceed benefits. Arch Surg 2005;140(5):480–5.
40] Atar E, Griton I, Barchar GN, Bartal G, Klugar Y, Belenky Y. Embolizationof transected vertebral arteries in unstable trauma patients. Emerg Radiol2005;11(5):291–4.
41] Veras LM, Pedraza-Gutierrez S, Castellanos J, Capellades J, CasamitjanaJ, Rovira-Canellas A. Vertebral artery occlusion after acute cervical spine
trauma. Spine 2000;25(9):1171–7.42] Stein DM, Boswell S, Sliker CW, Lui F, Scalea TM. Blunt cerebrovascularinjuries: does treatment really matter? Eastern Association for the Surgeryof Trauma 20th Annual Scientific Assembly. Fort Myers, FL. January 8,2007.