Embed Size (px)
Citation preview

Imaging Findings in TBI - Part 1
Travis Snyder, D.O. Neuroradiologist
SimonMed Imaging/Touro U/MV HCA Hospital
Moderators: Kyle Kingberger, Hugo Chanez, Hali Marsocci
Nov 4th 2020
Connectionology HMR

Neuro-Imaging in Brain Injury Lecture Outline
• Optimal TBI protocol – Standard – Advanced
• Imaging findings highly specific for head trauma • Imaging findings possibly related to head trauma • Imaging findings more likely relating to head trauma?
– Atrophy • Global • Hippocampal • Cortical
– White Matter Shearing – DTI (Diffusion Tensor Imaging)

TBI Protocol • CT: assess life threatening conditions in ER
– Bleeds, fractures, midline shift
Subdural Hematoma Subarachnoid Hematoma Intraparencheymal Hematomas

Value of CT
• Essentially nondiagnostic for mTBI
• Soft Tissue Swelling! Commonly missed by radiologists
• Some findings on CT will resolve by the time MRI is performed (Subarachnoid Hemorrhage, Subdural hemorrhages)

Value of CT Soft Tissue Swelling! Commonly missed by radiologists
Resolving Left Forehead Contusion
Head CT 2/6/13 Head CT 12/15/14 Head CT 2/23/13

Healing Left Forehead Contusion
Head CT 2/6/13 Head CT 2/23/13 Head CT 12/15/14
Improved Resolved

Prognosis of Subdural and Subarachnoid Hemorrhage (Often only seen on initial CT)
Subdural Hematoma Subarachnoid Hemorrhage
Mortality rate as high as 60%, which has improved recently with recent medical and surgical advances (Alagoz, Yildirim et al. 2017) However, there remains risk for significant morbidity with functional recovery rates from surgically treated acute subdural hematomas ranging from only 19-45% (Bullock, Chesnut et al. 2006, Tallon, Ackroyd-Stolarz et al. 2008).
A high mortality rate of 35-40%, despite neurosurgical treatment advances, has been reported following SA hemorrhage (Pothiawala 2012). Twenty-five percent of patients develop moderate depression, 50% of survivors report that they think that their personality has changed, generally for the worse, the cases reported being mostly weakness, excessive irritability, memory difficulties, daytime drowsiness and insomnia” (Daniere, Gascou et al. 2015).

TBI Protocol
• MRI – Only way to completely assess prognosis, full extent of damage, can be done
as outpatient.
MRI optimal protocol Standard Imaging – 3T magnet (better camera lens) – SWI (hemorrhage) – Thin section, triplane (contusions and shearing) Advanced Imaging – Volumetric Software (atrophy means injury) – DTI (White matter tract damage) – Perfusion (Blood flow) – Other? (MRA, spectroscopy, fMRI) – Time and cost constraints?

Why Advanced Imaging?
Conventional MRI is insensitive for traumatic brain
injury with only 27% of patients demonstrating
findings. (Yuh et al., 2013) Therefore advanced
imaging is indicated which can identify pathology
not present on conventional sequences. (Vanier et
al., 2020) (Osborn, 2017)
Yuh, E. L., Mukherjee, P., Lingsma, H. F., Yue, J.
K., Ferguson, A. R., Gordon, W. A., . . .
Investigators, T.-T. (2013). Magnetic
resonance imaging improves 3-month
outcome prediction in mild traumatic brain
injury. Annals of neurology, 73(2), 224-
235. doi:10.1002/ana.23783
Osborn, A. (2017).
Osborn's Brain
2nd edition. Salt
Lake City, UT:
Elsevier.
Vanier, C., Pandey, T., Parikh, S., Rodriguez, A.,
Knoblauch, T., Peralta, J., . . . Snyder, T.
(2020). Interval-censored survival analysis of
mild traumatic brain injury with outcome
based neuroimaging clinical applications.
Journal of Concussion, 4,
2059700220947194.
doi:10.1177/2059700220947194

SWI (susceptibility weighted sequence) 4-6 x superior to GRE (Gradient Echo) for hemorrhages

SWI (susceptibility weighted sequence) 4-6 x superior to GRE (Gradient Echo) for hemorrhages
Tong KA, Ashwal S, Holshouser BA, Shutter LA, Herigault G, Haacke EM, Kido DK. Hemorrhagic shearing lesions in children and adolescents with posttraumatic diffuse axonal injury: improved detection and initial results. Radiology. 2003 May;227(2):332-9.

Optimal SWI technique -Thin section
- Proper Technique - >Siemens

Triplane 3D SWI technique (enhanced detection and illustrative)

Subtle Left Anterior Frontal Contusion
Why Thin Section, triplane FLAIR/T2?

Subtle Inferior Temporal Contusion (only seen in coronal plane)
Why Thin Section, triplane FLAIR/T2?

Subtle Bilateral Anterior Inferior Frontal Contusions
Why Thin Section, triplane FLAIR/T2?

Subtle Right Anterior Inferior Frontal Contusion
Why Thin Section, triplane FLAIR/T2?

Why Thin Section, triplane FLAIR/T2?
Later Scan

Axial Slice Skipped (Slice too thick)
Why Thin Section, triplane FLAIR/T2?
Earlier Scan

Why Perfusion? (ASL and Contrasted)
Abnormal Perfusion (blood flow) Beyond Contusions

Perfusion and PET Matched Posterior Defects
Byrnes, K. R., Wilson, C. M., Brabazon, F., von Leden, R., Jurgens, J.
S., Oakes, T. R., & Selwyn, R. G. (2014). FDG-PET imaging in
mild traumatic brain injury: a critical review. Front
Neuroenergetics, 5, 13. doi:10.3389/fnene.2013.00013

Imaging findings highly specific for head trauma
• Hemorrhages, Fractures
• Contusions
• Hemorrhagic DAI (Diffuse
Axonal Injury)

Imaging findings highly specific for head trauma
• Hemorrhagic DAI
Literature
L. Amaral, A.A.S.M. Santos, V.E.C. Oliveira, C.A.P. Fontes, T.C.R.S. Santos, M.H. Santos, M.L.O. Santos (2011). "Diffuse axonal injury: a study of patients in neurological intensive care unit, with emphasis on follow up and value of
diffusion weighted imaging." European Society of Radiology EPOS doi: 10.1594/ecr2011/C-1692
Literature
Douglas DB, Muldermans JL, Wintermark M. Neuroimaging of brain trauma.
Curr Opin Neurol. 2018 Aug;31(4):362-370. doi: 10.1097/WCO.0000000000000567.

Imaging findings highly specific for head trauma
• Hemorrhagic DAI

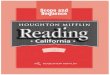
Hemorrhagic Shearing (DAI)
Hemorrhagic Shearing (DAI)

Hemorrhage Shearing Prognosis - Overall Burden
- Corpus Callosum - Brainstem - Midbrain
Rita de Cássia Almeida Vieira, Wellingson Silva Paiva, Daniel Vieira de Oliveira, Manoel Jacobsen Teixeira, Almir Ferreira de Andrade, and Regina Márcia Cardoso de Sousa Diffuse Axonal Injury: Epidemiology, Outcome and Associated Risk Factors Front Neurol. 2016; 7: 178.
Abu Hamdeh S, Marklund N, Lannsjö M, Howells T, Raininko R, Wikström J, Enblad P. Extended Anatomical Grading in Diffuse Axonal Injury Using MRI: Hemorrhagic Lesions in the Substantia Nigra and Mesencephalic Tegmentum Indicate Poor Long-Term Outcome. J Neurotrauma. 2017 Jan 15;34(2):341-352. doi: 10.1089/neu.2016.4426. Epub 2016 Jul 25.
Calvi MR, Beretta L, Dell'Acqua A, Anzalone N, Licini G, Gemma M. Early prognosis after severe traumatic brain injury with minor or absent computed tomography scan lesions. J Trauma. 2011 Feb;70(2):447-51. doi: 10.1097/TA.0b013e3182095e14.

The corpus callosum is the largest white matter fiber tract of the brain and the only significant fiber tract connecting the right and left hemispheres. Without the corpus callosum, the two halves
(hemispheres) of the brain cannot communicate. Injury to this vital structure is a very poor prognostic sign.
Moen KG1, Brezova V, Skandsen T, Håberg AK, Folvik M, Vik A. Traumatic axonal injury: the prognostic value of lesion load in corpus callosum, brain stem,
and thalamus in different magnetic resonance imaging sequences J Neurotrauma. 2014 Sep 1;31(17):1486-96. doi: 10.1089/neu.2013.3258. Epub 2014 Jul 1..
Brain MRI 5/1/19
Prognosis of Damage to the Corpus Callosum

Prognosis of Damage to the Corpus Callosum
The corpus callosum is the largest white matter fiber tract of the brain and the only significant fiber tract connecting the right and left hemispheres. Without the corpus callosum, the two halves
(hemispheres) of the brain cannot communicate. Injury to this vital structure is a very poor prognostic sign.
Moen KG1, Brezova V, Skandsen T, Håberg AK, Folvik M, Vik A. Traumatic axonal injury: the prognostic value of lesion load in corpus callosum, brain stem,
and thalamus in different magnetic resonance imaging sequences J Neurotrauma. 2014 Sep 1;31(17):1486-96. doi: 10.1089/neu.2013.3258. Epub 2014 Jul 1..

When to Image? (EARLY!)
• 70% of Hemorrhagic DAI resolves on follow-up MRI
• 30% of Non-hemorrhagic DAI resolves
• 30% of contusions resolve on subsequent MRI and a volume reduction of 44% on average one year following trauma.
Wei Liu, Karl Soderlund, Justin S. Senseney, David Joy, Ping-Hong Yeh, John Ollinger, Elyssa B. Sham, Tian Liu, Yi Wang, Terrence R. Oakes, Gerard Riedy Imaging Cerebral Microhemorrhages in Military Service Members with Chronic Traumatic Brain Injury RadiologyVol. 278, No. 2
Brandstack N, Kurki T, Tenovuo O, Isoniemi H. MR imaging of head trauma: Visibility of contusions and other intraparenchymal injuries in early and late stage Brain Inj. 2006 Apr;20(4):409-16.

• Empty Sella
• Cavum Septum Pellucidum
• Chiari I malformation
• Aneurysms
• Dilated Perivascular Spaces
Imaging findings possibly related to head trauma

• Empty Sella
Imaging findings possibly related to head trauma
Schneider HJ, Kreitschmann-Andermahr I, Ghigo E, Stalla GK, and Agha A (2007)."Hypothalamopituitary dysfunction following traumatic brain injury and aneurysmal subarachnoid hemorrhage: a systematic review". JAMA. 298(12): 1429-38.
Salvatore Benvenga Alfredo CampennI Rosaria M. Ruggeri Francesco Trimarchi Hypopituitarism Secondary to Head Trauma J Clin Endocrinol Metab (2000) 85 (4): 1353-1361.
Fatih Tanriverdi and Fahrettin Kelestimur Pituitary dysfunction following traumatic brain injury: clinical perspectives Neuropsychiatr Dis Treat. 2015; 11: 1835–1843.
Patient Normal

• Cavum Septum Pellucidum
Imaging findings possibly related to head trauma
Silk T, Beare R, Crossley L, Rogers K, Emsell L, Catroppa C, Beauchamp M, Anderson V. Cavum septum pellucidum in pediatric traumatic brain injury. Psychiatry Res. 2013 Sep 30;213(3):186-92. doi: 10.1016/j.pscychresns.2013.03.001. Epub 2013 Jun 29 Koerte Inga K., Hufschmidt Jakob, Muehlmann Marc, Tripodis Yorghos, Stamm Julie M., Pasternak Ofer, Giwerc Michelle Y., Coleman Michael J., Baugh Christine M., Fritts Nathan G., Heinen Florian, Lin Alexander, Stern Robert A., and Shenton Martha E. Cavum Septi Pellucidi in Symptomatic Former Professional Football Players Journal of Neurotrauma. February 2016, Vol. 33, No. 4: 346-353
Cavum Septum Very Small Normal

• Chiari I malformation
Imaging findings possibly related to or
exacerbated by head trauma
Wan MJ, Nomura H, Tator CH. "Conversion to symptomatic Chiari I malformation after minor head or neck trauma." Neurosurgery. 2008 Oct;63(4):748-53; discussion 753. doi: 10.1227/01.NEU.0000325498.04975.C0. Mehta, A. I., Grant, G. A., Gray, L., & Sampson, J. H. (2011). Radiographic progression of a Chiari I malformation after minor head trauma: Final increment of obstruction to create pathophysiology. Journal of Surgical Radiology, 2(3), 290-293.
Patient Normal

• Aneurysms
Imaging findings possibly related to head trauma
Jefferson T Miley, MD, Gustavo J Rodriguez, MD, and Adnan I Qureshi, MD Traumatic Intracranial Aneurysm Formation following Closed Head Injury J Vasc Interv Neurol. 2008 Jul; 1(3): 79–82.

• Dilated Perivascular Spaces
Imaging findings possibly related to head trauma
Inglesea, M., Bomsztyka, E., et al "Dilated Perivascular Spaces: Hallmarks of Mild Traumatic Brain Injury" AJNR 2005 26: 719-724
Normal Basal Ganglia Normal Vertex Post Traumatic

Imaging findings more likely relating to head trauma?
– Atrophy
• Global
• Hippocampal
• Cortical
– White Matter Shearing
– DTI (Diffusion Tensor Imaging)

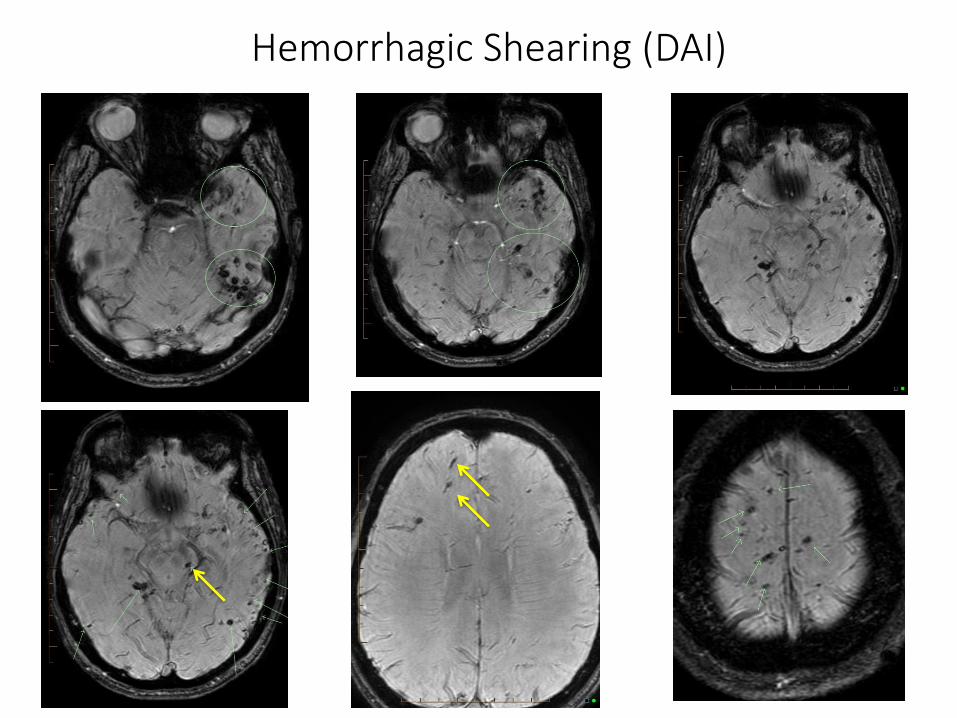
Imaging findings more likely than not relating to head
trauma?
– Atrophy
• Global

- Post Traumatic Ventricular enlargement
indicates diffuse brain injury
- Lateral ventricle size is best predictor of
cognitive outcome
- More prognostic even than severity of original TBI
Himanen, Portin et al
Cognitive functions in relation to MRI findings 30 years after traumatic brain injury.
Brain Inj. 2005 Feb;19(2):93-100.
Timming R, Orrison WW, Mikula JA.
Computerized tomography and rehabilitation outcome after severe head trauma.
Arch Phys Med Rehabil. 1982 Apr;63(4):154-9.
Ventricle Volume and TBI

9/21/09 9/22/11 7/25/18
Abnormal Ventricular Volumes (Diffuse Post Traumatic Brain Injury and Poor Prognosis)
MVC 9/20/09

Brain CT 9/21/09, 9/22/11, 7/25/18 Actual Increase
vs. Anticipated Increase with Normal Aging
Scahill, R. I., C. Frost, R. Jenkins, J. L. Whitwell, M. N. Rossor and N. C. Fox (2003). "A longitudinal study of brain volume changes in normal aging using serial registered magnetic resonance imaging.”
Arch Neurol 60(7): 989-994.
20
21
22
23
24
25
26
27
28
29
30
9/1
/09
8/1
/18
cm3
Anticipated
Actual
MVC 9/20/09
Abnormal Ventricular Volumes (Diffuse Post Traumatic Brain Injury and Poor Prognosis)

Abnormal Ventricular Volumes (Volumetric Tracing Technique)
Arnold Tóth,Ilona Schmalfuss, Shelley C. Heaton, Andrea Gabrielli, H. Julia Hannay, Linda
Papa, Gretchen M. Brophy, Kevin K.W. Wang, András Büki, Attila Schwarcz, Ronald L.
Hayes, Claudia S. Robertson, and Steven A. Robicsek
Lateral Ventricle Volume Asymmetry Predicts Midline Shift in Severe Traumatic Brain Injury
J Neurotrauma. 2015 Sep 1; 32(17): 1307–1311.

Abnormal Ventricular Volumes (Diffuse Post Traumatic Brain Injury and Poor Prognosis)
Actual Increase vs.
Anticipated Increase with Normal Aging
Scahill, R. I., C. Frost, R. Jenkins, J. L. Whitwell, M. N. Rossor and N. C. Fox (2003). "A longitudinal study of brain volume changes in normal aging using serial registered magnetic resonance imaging.”
Arch Neurol 60(7): 989-994.
0
5
10
15
20
25
30
35
40
45
9/1
/07
3/1
/08
9/1
/08
3/1
/09
9/1
/09
3/1
/10
9/1
/10
3/1
/11
9/1
/11
3/1
/12
9/1
/12
3/1
/13
9/1
/13
3/1
/14
9/1
/14
3/1
/15
9/1
/15
3/1
/16
9/1
/16
3/1
/17
9/1
/17
cm3
Actual
Anticipated
Date of Injury
Imaging findings more likely than not relating to head
trauma? – Atrophy
• Hippocampal
Severe Right and Mild Left HA Normal
David F. Tate and Erin D. Bigler Fornix and Hippocampal Atrophy in Traumatic Brain Injury doi:10.1101/lm.33000 Learn. Mem. 2000. 7: 442-446
John D. MacKenzie, Faez Siddiqi, James S. Babb, Linda J. Bagley, Lois J. Mannon, Grant P. Sinson and Robert I. Grossman Brain Atrophy in Mild or Moderate Traumatic Brain Injury: A Longitudinal Quantitative Analysis American Journal of Neuroradiology October 2002, 23 (9) 1509-1515
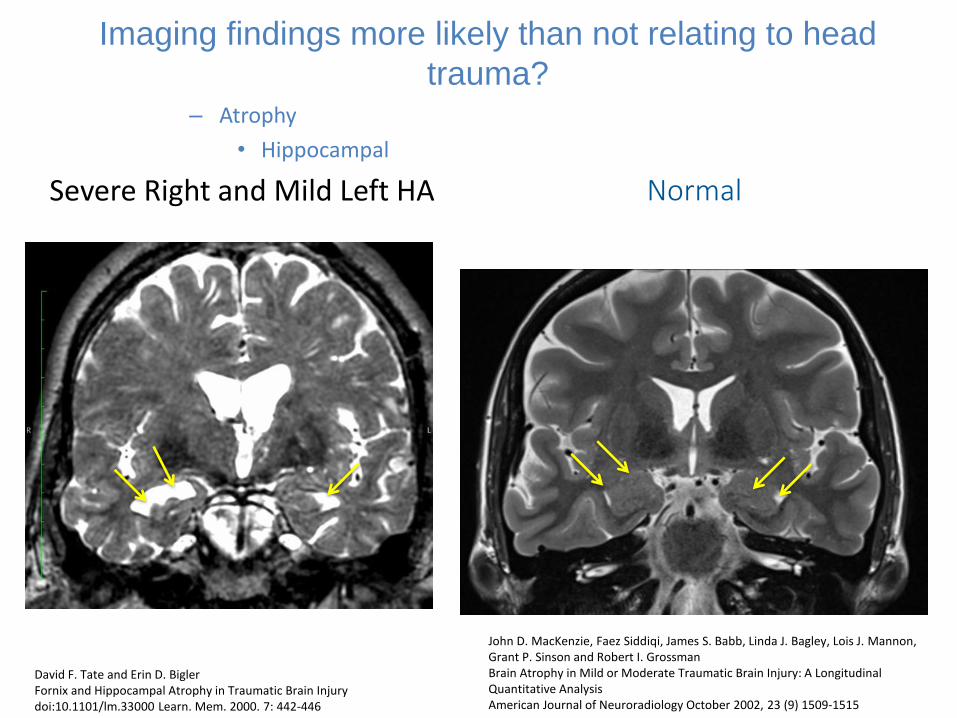
Imaging findings more likely relating to head trauma? – Atrophy
• Hippocampal
Ross DE, Ochs AL, DeSmit ME, Seabaugh JM, Havranek MD; Alzheimer’s Disease Neuroimaging Initiative. Man Versus Machine Part 2: Comparison of Radiologists' Interpretations and NeuroQuant Measures of Brain Asymmetry and Progressive Atrophy in Patients With Traumatic Brain Injury. J Neuropsychiatry Clin Neurosci. 2015;27(2):147-52

Post Traumatic Left Hippocampal Atrophy
Normal Patient’s Scan
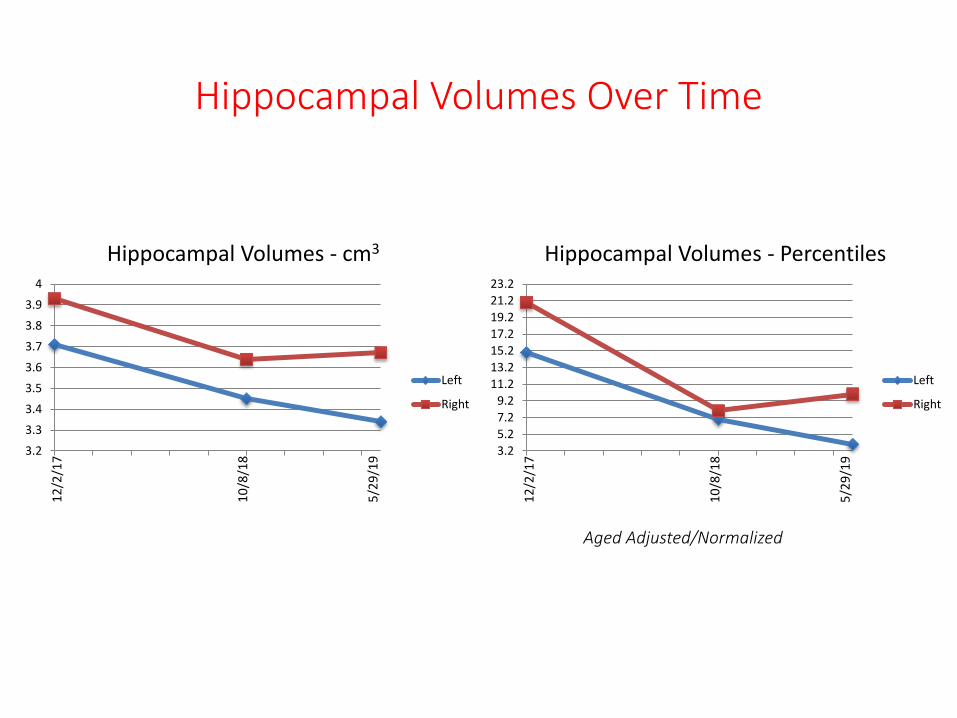
Hippocampal Volumes Over Time
3.2
3.3
3.4
3.5
3.6
3.7
3.8
3.9
4
Hippocampal Volumes - cm3
Left
Right
3.2
5.2
7.2
9.2
11.2
13.2
15.2
17.2
19.2
21.2
23.2
Hippocampal Volumes - Percentiles
Left
Right
10
/8/1
8
5/2
9/1
9
12
/2/1
7
10
/8/1
8
5/2
9/1
9
12
/2/1
7
Aged Adjusted/Normalized

Imaging findings more likely relating to head trauma? – Atrophy
• Cortical
Chong CD, Berisha V, Chiang CC, Ross K, Schwedt TJ. Less Cortical Thickness in Patients With Persistent Post-Traumatic Headache Compared With Healthy Controls: An MRI Study. Headache. 2018 Jan;58(1):53-61. doi: 10.1111/head.13223. Epub 2017 Nov 15.
Koushik A. Govindarajan, Ponnada A. Khader M. Hasan, Elisabeth A. Wilde, Harvey S. Levin, Jill V. Hunter, Emmy R. Miller, Vipul Kumar S. Patel, Claudia S. Robertson, and James Cortical Thickness in Mild Traumatic Brain Injury J. McCarthy J Neurotrauma. 2016 Oct 15; 33(20): 1809–1817.

Would you like to learn more? Please stay tuned for Part 2.If you have questions, please contact us at:
Travis Snyder DO SimonMed Imaging/Touro U/ MV HCA hospital
Thanks to Moderators: Kyle Kingberger [email protected] and Hugo Chanez
[email protected] and Hall Marocci [email protected]
[email protected] [email protected] [email protected]
Acknowledgements:
Cheryl Vanier PhD, Shaunaq Parikh DO, Alan Rodriguez MD, Logan Razenberger DO, Trisha Pandley DO, students of Touro U, Michael Lobatz MD, Enricco Fazzini DO, Lindell Weaver
MD, Jeff Lewine PhD, and William Orrison MD