Embed Size (px)
DESCRIPTION
IMAGING CONTRIBUTION IN THE DIAGNOSIS OF MAXILLOMANDIBULAR LESIONS. A NEFFATI, K BOUZAÏDI, I KECHAOU, K AYACHI*, F JABNOUN, M MAAMOURI * Radiology service, MT Maamouri Hospital, Nabeul , Tunisia *ORL service, MT Maamouri Hospital, Nabeul , Tunisia . HEAD AND NECK : HN 6. INTRODUCTION. - PowerPoint PPT Presentation
Citation preview

IMAGING CONTRIBUTION IN THE DIAGNOSIS OF MAXILLOMANDIBULAR LESIONS
A NEFFATI, K BOUZAÏDI, I KECHAOU, K AYACHI*, F JABNOUN, M MAAMOURI *
Radiology service, MT Maamouri Hospital, Nabeul, Tunisia *ORL service, MT Maamouri Hospital, Nabeul, Tunisia
HEAD AND NECK : HN 6

INTRODUCTION
There are a variety of cysts and tumors that affect the osseous marrow and cortex of the jaw bones, which may be uniquely derived from the tissues of developing teeth.
It is important as a radiologist to know the different types of maxillo-mandibular lesions, their semiological presentation, and to guide the otolaryngologist before any treatment.

SUBJECTS AND METHODS
Study of radio-clinical cases of 6 patients 4 men and 2 women with an average age of 37.6
years ranging from 18 to 58 years. The clinical call signs were bone pain, tooth
mobility and maxillomandibular tumefaction. All patients were investigated by means of:
- Dental Panoramic X-Ray- Facial CT scan
Pathologically confirmed by surgery or biopsy.

RESULTS
The Dental Panoramic X-Ray shows a radiolucent lesion located in- The maxilla (1case)
- The mandible (5 cases)
The CT scan shows these osteolytic lesions and specify their anatomical relationship with adjacent structures.
Histological examination identified:- Radicular cyst (4 cases)- Ameloblastoma (1 case)- Mandibular bone localization of Langerhans cell histiocytosis (LCH) (1 case).

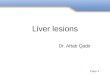
MK, 20 years
CT scan shows Multilocular radiolucent lesion with undefined borders of the maxilla. Ameloblastoma

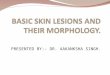
BM, 54 years
-Panoramic radiograph shows large, unilocular, expansile lesion on left molar region of mandible.Root of third molar Is partly absorbed.

MK, 20 years
CT shows same lesion with root resorption and thinned cortex. Pathologically,
radicular cyst was proven.

AH, 18 years
periapical radiolucency on right molar region of mandible .Radicular Cyst

Patient known to have a LCH.Panoramic radiograph shows large, unilocular, expansile lesion of the mandible. Biopsy: Bone localization of Langerhans cell histiocytosis.

Radicular (Periapical) Cyst
The most common odontogenic cyst (65%) It is thought to arise from the epithelial cell rests
of Malassez in response to inflammation. In fact, practically all radicular cysts originate in
preexisting periapical granulomas. Clinic: The cyst is painless when sterile and
painful when infected. Microscopically, the cyst is described with a
connective tissue wall that may vary in thickness, a stratified squamous epithelium lining, and foci of chronic inflammatory cells within the lumen.

Radicular (Periapical) Cyst
Radiographic findings consist of a pulpless, nonvital tooth that has a small well-defined periapical radiolucency at its apex.
Large cysts may involve a complete quadrant with some of the teeth occasionally mobile and some of the pulps nonvital.
Root resorption may be seen.
Treatment is extraction of the affected tooth and its periapical soft tissue or root canal if the tooth can be preserved.

Ameloblastoma
The most common odontogenic tumor. Young adults without sex predilection. Originates from epithelial remnants of dental
embryogenesis, without the participation of the odontogenic ectomesenchyme.
It is a benign but locally invasive neoplasm.

Ameloblastoma Three different clinicopathologic subtypes:
multicystic (86%), unicystic (13%) and peripheral (extraosseus – 1%).
It is characterized by a progressive growth rate and, when untreated, may reach enormous proportions.
Early symptoms are often absent, but late symptoms may include a painless swelling, loose teeth, malocclusion, or nasal obstruction.

Ameloblastoma Any location in the mandible or maxilla, but the
regions of the inferior molars and mandibular ramus are the most prevalent anatomical locations (80%).
The most common radiographic findings are unilocular and multilocular masses, septation, association with unerupted teeth, loss of lamina dura and root resorption.
In solid or multicystic ameloblastomas, a multilocular radiolucent lesion with undefined borders is the most characteristic radiographic aspect (soap bubble or honeycomb appearance).

Ameloblastoma In the unicystic type, the lesions usually appear as
radiolucent areas with relatively well-defined borders that surround the crown of an impacted inferior third molar, resembling a dentigerous cyst.
In addition to these osteolytic lesions, CT scan shows the loco-regional extension and their content: Cystic type with liquid content, often voluminous, thick
walled, enhanced after contrast injection. Furthermore, it can be associated to a tissue
formation.

Langerhan’s cell histiocytosis
Langerhan’s cell histiocytosis is defined as an abnormal proliferation of Langerhans cells in various organs and tissues (bone, skin, lymph nodes…)
Maxillo-mandibular localisation is the most commun, it represents 20,8% of non odontogenic tumors.
Among facial locations, mandibular involvement is the most frequent and occurs in young people less than 20 years.

Langerhan’s cell histiocytosis
It is characterized by multiple radiolucent lesions, well defined, circular or oval without bone condensation reaction giving the appearance of floating teeth.
CT confirms these informations and may shows a cortical rupture in places without invasion of the soft tissues.
However, only the pathological examinationcan confirm the diagnosis.

Others Beside these lesions there other many lesions.
In fact, tumoral and pseudotumoral (odentogenic) pathology of the maxilla forms a large diverse group with three types of tumors: Those derived from odontogenic device Tumors and pseudotumors of bone origin Epithelial cysts of the maxilla
They can be devided also in:

Others
Odontogenic Cysts: Inflammatory Cysts:
Radicular (periapical) Cyst, paradental Cyst Developmental Cysts:
Dentigerous (follicular) Cyst, developmental Lateral Periodontal Cyst, odontogenic Keratocyst, glandular Odontogenic Cyst (GOC).

Others Nonodontogenic cysts
Incisive Canal Cyst, stafne Bone Cyst, traumatic Bone Cyst, surgical Ciliated Cyst (of Maxilla)
Odontogenic Tumors Epithelial Odontogenic Tumors
Ameloblastoma Calcifying Epithelial Odontogenic Tumor
Mesenchymal Odontogenic Tumors Odontogenic Myxoma Central Odontogenic Fibroma Cementoblastoma
Mixed Odontogenic Tumors

Others And then we can find other related Jaw
Lesions: Giant Cell Lesions:Central Giant Cell Granuloma, Brown Tumor of Hyperparathyroidism, Aneurysmal Bone Cyst
Fibroosseous Lesions: Fibrous Dysplasia, Ossifying Fibroma,
Condensing Osteitis

In general, well-demarcated lesions outlined by sclerotic borders suggest benign growth, while aggressive lesions tend to be ill-defined lytic lesions with possible root resorption.
With larger more aggressive lesions, CT may more clearly identify bony erosion and/or invasion into adjacent soft tissues.

CONCLUSION
The Dental Panoramic X-Ray and facial CT scan
can often guide the diagnosis of
maxillomandibular lesions, specify the
relationship with adjacent structures and
monitor its progress.
The ultimate diagnosis is still histological.