Embed Size (px)
Citation preview

Ultrasound in Med. & Biol., Vol. 33, No. 1, pp. 113–119, 2007Copyright © 2006 World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/07/$–see front matter
doi:10.1016/j.ultrasmedbio.2006.07.025
● Original Contribution
IMAGE-GUIDED ACOUSTIC HEMOSTASIS FOR HEMORRHAGE IN THEPOSTERIOR LIVER
SEAN BURGESS, VESNA ZDERIC and SHAHRAM VAEZY
Department of Bioengineering, University of Washington, Seattle, WA, USA
(Received 24 March 2006, revised 27 June 2006, in final form 13 July 2006)
Abstract—We investigated the use of ultrasound image-guided high intensity focused ultrasound (HIFU) to stopbleeding from injuries in the posterior liver. A HIFU transducer with focal length of 3.5 cm and frequency of 3.2MHz was integrated with an intraoperative high-resolution ultrasound-imaging probe. Wedge tissue extractions,30-mm long, 5-mm wide and 8-mm deep, were made in the posterior liver surface of five pigs to induce bleeding.The device was positioned on the anterior surface of the liver and HIFU was applied using ultrasoundimage-guidance. Hemostasis was achieved in 66 � 18 s (mean � standard deviation) for 17 HIFU treatments.During 7 min of sham HIFU treatment, none of the control incisions (n � 7) became hemostatic. Ultrasoundimage-guided HIFU offers a promising method for hemostasis in surgical settings in which the hemorrhage siteis hidden and/or not accessible. (E-mail: [email protected]) © 2006 World Federation for Ultrasoundin Medicine & Biology.
Key Words: Acoustic hemostasis, High intensity focused ultrasound, Therapeutic ultrasound, Liver trauma,
Hemorrhage control, Ultrasound-guided therapy.INTRODUCTION
Severe liver injury is the most common cause of hem-orrhagic death following abdominal trauma (Cogbillet al. 1988; Hoyt et al. 1994). While low-grade liverinjuries are commonly treated nonoperatively, high-grade injuries often require surgery due to uncontrolledhemorrhage and the potential subsequent development ofseptic complications (Duane et al. 2004). Current surgi-cal methods for hemorrhage control and repair of livertrauma range from hepatic sutures and packing to livertransplantation (Parks et al. 1999). However, significantdifficulty exists for hemostasis of inaccessible locationsof the posterior liver that contain major hepatic andportal veins, lying behind the thickest least-mobile por-tion of the liver (Buckman et al. 2000). Furthermore,attempts to lift and/or rotate the liver to allow access toinjured tissue may increase bleeding (Buckman et al.2000). The development of new methods that canaddress hidden and inaccessible liver injuries isneeded for improved surgical outcomes. We investi-gated the use of ultrasound image-guided high inten-sity focused ultrasound (HIFU) to address hidden in-
Address correspondence to: Shahram Vaezy, PhD, Associate Pro-
fessor, Department of Bioengineering, University of Washington, Box355061, Seattle, WA 98195, USA. E-mail: [email protected]113
juries, due to its ability to treat regions deep within thetissue.
HIFU is being investigated in various fields in-cluding neurosurgery (Hynynen and Jolesz 1998),urology (Gelet et al. 2001), oncology (ter Haar 2001;Wu et al. 2001) and hemorrhage control (Vaezy et al.2001a). Hemorrhage control relies on both thermaland mechanical effects of HIFU. The thermal effectscan result in tissue temperatures exceeding 70°Cwithin seconds of application, effectively cauterizingtissue and sealing blood vessels (ter Haar 1995),whereas the mechanical effects may cause plateletactivation (Poliachik et al. 2001) and the release oftissue coagulation factors (Vaezy et al. 2001a), leadingto faster formation of coagulum. HIFU-induced hemo-stasis has been used previously for the treatment ofvisible bleeding sites in solid abdominal organs (No-ble et al. 2002; Vaezy et al. 1999, 2004). HIFU ther-apy can be extended to include nonvisible bleedingsites through the use of diagnostic ultrasound (US)imaging. We believe that US offers a safe, portableand real-time method of imaging for the detection ofbleeding and visualization of injured tissues. More-over, hyperecho (bright spot) formation at the HIFUfocus in US images provides a valuable guidance and
monitoring of the HIFU treatment (Held et al. 2006).
114 Ultrasound in Medicine and Biology Volume 33, Number 1, 2007
In the study presented here, our objective was toachieve hemorrhage control of the bleeding in posteriorliver by applying HIFU from the anterior liver surface,through the liver parenchyma, under the guidance of USimaging. Treatment times, blood loss and gross andmicroscopic examinations were used to evaluate the ef-ficacy and safety of the procedure. To the best of ourknowledge, this is the first image-guided HIFU hemo-stasis study in which ultrasound was used both to targetand to treat nonvisible bleeding from injured solid or-gans.
MATERIALS AND METHODS
Animal modelAll procedures were conducted in accordance with
the guidelines of the National Institutes of Health for useof laboratory animals with the approval of the Universityof Washington Institute of Animal Care and Use Com-mittee. Five pigs (weight of 40–45 kg) were used in theexperiments. The animals were sedated via IM injectionof acepromazine (0.4 mg/kg) and ketamine (20 mg/kg)and then anesthetized using an IV injection of ketamine(20 mg/kg) and xylazine (2.5 mg/kg) dosed to effect, toallow placement of an endotracheal tube. Following in-tubation, the animals were ventilated with oxygen andisoflurane (1% to 3%) to maintain anesthesia. Heparinwas administered (200 units/kg) via an IV injection, 5 to10 min before the experiment and every 30 to 60 minthroughout the experiment, to impede blood coagulation(Di Nisio et al. 2005).
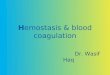
A midline incision was made from the xyphoidprocess to the level of kidneys to open the abdomenallowing access to the liver. Overall, 24 incisions wereproduced in posterior liver parenchyma of the left lateral,left medial and right medial liver lobes (up to 4–5incisions per each animal). No more than two injuries, atleast 3 cm apart, were made in each lobe. The incisionswere randomly assigned to the HIFU-treated (n � 17)and sham-treated (n � 7) group. The lobe was lifted toexpose the posterior side of the liver and cuts were made,30-mm long, 5-mm wide and 8-mm deep, that separateda wedge of tissue that was then removed (Fig. 1). Bloodwas immediately collected by placing a gauze pad overthe incision site for 5 s. The blood loss was determinedby weighing the gauze with blood, subtracting the weightof a gauze without blood, and dividing this value with thedensity of pig blood (1.06 g/mL) (Cornejo et al. 2004).The blood loss rate (mL/min) was found by dividing thevolume of collected blood with the blood collection timeof 0.083 min (5 s).
The injured liver lobe was placed on gauze pads,with its posterior surface facing down, thus concealing
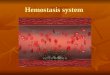
the incision. In the HIFU-treatment group, the incision wastargeted by positioning the US image-guided HIFU device(Fig. 2a) over the anterior surface of the lobe (Fig. 2b) suchthat the incision was within the HIFU target region onthe B-mode US image (Fig. 3a). HIFU treatment wasapplied in 10-s intervals while scanning the device alongthe incision at a rate of approximately 1 mm/s. Through-out the treatment, the incision was maintained at theHIFU focus and lesion formation was monitored usinghyperecho appearance in US images. Following each10-s HIFU application, the lobe was lifted to determinewhether bleeding was still present. The treatment con-tinued until hemostasis was achieved. The time fromproducing the incision to the complete arrest of thebleeding was defined as time to hemostasis, whereas thetime during which HIFU was delivered was defined asHIFU application time.
In control experiments, overall, seven incisionswere made as described above (in four animals, one totwo control incisions per each animal) and the treatmentprocedure was simulated but HIFU was not applied(sham treatment). The average duration of sham treat-ments was 7 min. Blood was collected immediately afterthe incision was produced and then again at the end ofsham treatment for blood loss rate calculations to deter-mine the reduction in bleeding over time. After the shamtreatment was completed, the incision was sealed (usingHIFU), without data collection.
The animals were euthanized at the end of theexperiment using an injection of euthasol (1 mL per 4.5kg animal weight) followed by 20 mL of concentrated KCl.Following euthanasia, tissue samples were collected for
Fig. 1. Injury in the posterior liver. The incisions, 30-mm long,5-mm wide and 8-mm deep, created a wedge of tissue that was
subsequently removed.
histologic examination. The samples were fixed in for-

in the
HIFU hemostasis in posterior liver ● S. BURGESS et al. 115
malin, embedded in paraffin, stained with hematoxylinand eosin, and examined using light microscopy.
Image-guided HIFU deviceA single element 3.2 MHz HIFU transducer (SU-
107, Sonic Concepts, Woodinville, WA, USA) was cou-pled to a broadband B-mode ultrasound imaging probe(CL10-5, HDI-1000, Philips Ultrasound, Bothell, WA,USA) via a custom-designed holder (Fig. 2a) (Foleyet al. 2004). The holder maintained a 45° angle betweenthe HIFU transducer and imaging probe, such that theHIFU focus remained fixed within the US imaging plane(Fig. 2a). The spherically curved HIFU transducer had afocal length of 3.5 cm and f-number of 1. The focalregion dimensions (�6 dB) in the axial and lateral di-rections, 0.51 cm and 0.08 cm, respectively, were mea-sured by mapping the pressure field of the transducerwith a needle hydrophone (TNU001A, NTR Systems,Inc., Seattle, WA, USA). The acoustic power was mea-
Fig. 2. a) Schematic drawing of US image-guided HIFmechanically coupled such that the HIFU focus remainedapplication. The HIFU device was positioned on the an
bleeding incision
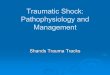
Fig. 3. Sequence of US images for a typical HIFU applicthe HIFU focus was on or a few millimeters beneath thwhich a lesion progressed toward the HIFU transducer.length of the incision. The lesion formation and progress
using hyperecho
sured using a reflective radiation force balance (Chris-tensen 1988). The free-field acoustic intensity, calculatedas the acoustic power divided by the �6 dB focal area of0.0045 cm2, was 21800 W/cm2. The in situ focal acousticintensity, accounting for 2 cm of attenuation through theliver (0.15 Np/cm) (Christensen 1988) and a 75% HIFUduty cycle, was 2300 W/cm2 (spatial-average temporal-average). The actual in situ acoustic intensity was larger(by less than two times) as compared with the calculatedvalue due to the reflection of ultrasound waves from theliver–gauze interface in the postfocal region, resulting inan increased energy delivery at the injury site (Muratet al. 2004).
Coupling between the HIFU transducer and liverwas achieved by a custom-made polyurethane water pil-low (Fig. 2b) with degassed water circulation for provid-ing cooling of the transducer. Synchronization of USimaging and HIFU therapy was achieved using a previ-ously reported method (Vaezy et al. 2001b). By utilizing
ice. The HIFU transducer and US imaging probe werein the US image plane. b) Experimental set-up for HIFUsurface of the liver. US imaging was used to target the
posterior liver.
) The wedge incision was located and targeted such thation site. b) HIFU was applied for 10-s intervals, duringg HIFU application, the device was scanned along thes monitored through a window in the interference bands
U devfixed
terior
ation. ae incis
Durinion wa
formation.

116 Ultrasound in Medicine and Biology Volume 33, Number 1, 2007
a 75% HIFU duty cycle, an observation window wascreated between interference bands (Fig. 3b). The win-dow location was adjustable and positioned such that theHIFU focal region could be viewed during the treatment.Since the geometric relationship between the US imag-ing probe and HIFU transducer was held constant, theHIFU focus remained fixed at a marked position on theUS image screen.
RESULTS
A typical sequence of treatment events, observedusing US imaging, is shown in Fig. 3. Discontinuity inthe posterior liver surface (Fig. 3a), at the incision site,was used as an indicator to locate and target theincision before HIFU treatment. During HIFU appli-cation (Fig. 3b), the treatment was monitored in theinterference-free window. A hyperechoic region (arrow,Fig. 3b) formed at the HIFU focus located at the incisionsite. As the HIFU treatment progressed, the hyperechoicregion propagated toward the HIFU transducer.
Hemostasis was achieved in all HIFU-treated inci-sions (n � 17). HIFU application times were 66 � 19 s(mean � standard deviation), with a range from 32 s to95 s. The overall time needed to achieve hemostasis fora single incision was 6 � 3 min (mean � standarddeviation). This time includes the time required to targetthe incision site, apply HIFU, and check whether hemo-stasis was achieved after each 10-s application.
Blood loss rates, measured immediately after theincision was produced, were 19.8 � 10.8 mL/min and20.4 � 16.8 mL/min for the HIFU- and sham-treatmentgroups, respectively. Blood loss rates following treat-ment were 0 � 0 mL/min and 16.2 � 7.8 mL/min for theHIFU- and sham-treatment groups, respectively. Aftersham treatment (n � 7), the blood loss rate of the controlgroup was reduced by 22%; however, the control inci-sions continued to bleed.
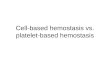
The gross examination of the HIFU-treated posteriorliver showed grey-tan discoloration of the tissue at thetreatment site, indicating coagulation necrosis (Fig. 4a). Theanterior liver, where the image-guided HIFU device wasplaced, varied in color among incisions from the normalmaroon (healthy tissue) for shorter HIFU applications to thegrey-tan discoloration (coagulated tissue) for the six inci-sions that received long HIFU applications (greater than78 s) resulting in extensive coagulation necrosis. Figure4b shows a cross-sectional view of a HIFU-treated inci-sion. An occluded artery (black arrow, Fig. 4b) can beseen within the grey-tan region surrounding the incision(white arrow, Fig. 4b).
Figure 5 shows light micrographs of a HIFU-treatedincision. Figures 5a-d correlate with the regions of gross
examination labeled �, �, �, and � in Fig. 4b. Region “�”(Fig. 5a) is tissue from the anterior side of the liver at theplace where the US-guided HIFU device was locatedduring the treatment. This region showed normal ma-roon-colored tissue under gross examination and normalhepatic parenchyma structure when viewed microscopi-cally. Individual hepatocytes (Fig. 5a) had round nuclei,with the surrounding sinusoids containing evenly distrib-uted red blood cells similar to untreated healthy tissue.Region “�” (Fig. 5b) is the dark maroon area surround-ing the treated grey-tan colored tissue. The light micro-graph (Fig. 5b) shows intact hepatocytes with the sur-rounding sinusoids congested with red blood cells. Thecongestion of red blood cells is thought to cause thedarker maroon discoloration observed under gross exam-ination (Vaezy et al. 2004). Region “�” (Fig. 5c) is anarea along the inner edge (toward the HIFU-sealed inci-sion) of the congested zone. The light micrograph (Fig.5c) shows a reduction in the number of red blood cellsnear the treated tissue. This micrograph also shows thatthe hepatocytes adjacent to the congestion zone remainedintact and therefore differed from those within the treatedregion. HIFU-treated tissue at the incision site is shownin region “�”. Under light microscopy, this HIFU-treatedliver section (Fig. 5d) was observed to have distortedhepatic structure consistent with coagulative necrosis(Ng et al. 2005). The darkly stained elongated nuclei anddetached individual hepatocytes were indicative of coag-ulative necrosis.
DISCUSSION
The use of B-mode US imaging to target the inci-sions and guide the treatment presented several chal-
Fig. 4. a) Posterior liver showing HIFU-treated incision. b)Cross-section of the HIFU-treated liver. The white arrow indi-cates the HIFU-sealed wedge incision, surrounded by necrosedtissue. The dark area (black arrow) is an occluded artery. (�)Normal hepatic tissue in the region between the necrosed tissueand the HIFU device. (�) Congestion zone caused by red bloodcells collecting in the region surrounding the treated tissue. (�)Transition region from congestion zone to the region of coag-ulation necrosis. (�) HIFU-treated tissue (grey-tan colored)surrounding the incision. Regions �, �, � and � are shown at
higher magnification in Fig. 5.
lenges. A clear discontinuity in the posterior liver could

HIFU hemostasis in posterior liver ● S. BURGESS et al. 117
not always be observed on the US image, making itdifficult to locate the incision. The observation of adiscontinuity was believed to be hindered by the softliver parenchyma conforming to the surface it was placedon. In addition, it was not possible to determine fromB-mode US images whether the incisions were stillbleeding after the HIFU treatment. Therefore, the inci-sions required visual inspection following HIFU appli-cation to determine whether bleeding was still present,which is not a feasible option in the treatment of nonac-cessible injuries. We are currently investigating differentUS-based methods for detection of bleeding that mayhelp in solving the above-mentioned problems. For ex-ample, contrast agent-enhanced US was shown previ-ously to aid in bleeding detection of injuries in solidorgans (Catalano et al. 2003; Liu et al. 2002) and bloodvessels (Luo et al. 2006). In addition, color Doppler mayprovide localization of active bleeding. Synchronizationof color Doppler with HIFU application for treatmentguidance that we have recently developed (Rabkin et al.2005) allows real-time visualization of the hemorrhagecontrol from hidden bleeding sites. Overall, incorporat-ing color Doppler or contrast-enhanced US imaging inour system may help in the assessment of bleeding andbetter targeting of the incisions, and subsequent reduc-tion in HIFU application times.
Current surgical methods to treat liver injuries in-clude the use of sutures, fibrin sealants, packing, elec-
Fig. 5. Micrographs of a representative HIFU-treated liver lobestained with hematoxylin and eosin. a) Region that was closestto the HIFU device showed normal hepatic architecture. b)Region in the proximity of necrosed tissue. A dark, red ringsurrounded the treatment site as sinusoids were congested withred blood cells. c) Transition toward the HIFU-treated tissue.No red blood cells were observed in the HIFU-treated region.d) HIFU-treated tissue at the incision site. Darkly stained,distorted nuclei (as compared with normal nuclei seen in (a))
were prevalent, with detached individual hepatocytes.
trocautery and argon beam coagulation (Trunkey 2004).
Drawbacks to the use of sutures to control liver bleedinginclude tissue tearing, foreign body response and contin-ued slow oozing of blood (Blair et al. 1988; Tovar et al.1998). Topical agents, such as fibrin glue, have beenshown to control hepatic bleeding, but with limitations.Since fibrin glue applied to actively bleeding injuriesmay be washed away by blood leaving the wound, it canonly be applied after bleeding is reduced by other mech-anisms (Cohn et al. 1998). Electrocautery and argonbeam coagulation are able to treat nonprofuse surfacebleeding (Gananadha et al. 2005; Wadia et al. 2000), but,like other conventional hemostatic techniques, they areunable to address hidden injuries in solid organs. Inaddition, the maximum ablation depth reported for elec-trocautery and argon beam coagulation was less than 1cm (Gananadha et al. 2005). Therefore, bleeding sitesdeep beneath the surface cannot be treated using argonbeam coagulation, electrocautery or other conventionalmethods without exposing the bleeding site and riskingadditional blood loss. US image-guided HIFU offers theadvantages of treating actively bleeding tissues and treat-ing injuries deep beneath the surface, all without directvisual observation. In addition to treatment of posteriorliver injuries, HIFU treatment of intraparenchymalbleeding in which the liver capsule is intact is alsopossible (Deng et al. 2004).
Published studies on conventional surgical treat-ment of porcine livers with visible lacerations of similarlength to those produced in our study, reported an aver-age hemostasis time of 3.0 min (Dowling et al. 1991).The average time to achieve hemostasis in our study was5.7 min, of which 1.1 min was HIFU on-time. A directcomparison of hemostasis times is difficult, due to theadditional challenges of targeting associated with the treat-ment of occult injuries. However, in a previous study inwhich HIFU was applied directly to visibly bleedingliver incisions, the average time to hemostasis was 1.3min (Vaezy et al. 2004), less than half the time ofconventional methods. Future studies should be aimed atreducing hemostasis times by optimizing HIFU parame-ters and improving the image-guided targeting. Suchimprovements could reduce the overall time to hemosta-sis of nonvisible injuries and minimize damage to adja-cent tissues.
A critical criterion for the placement of an incisionin the posterior liver was the thickness of the tissue. Thiswas due to the fixed focal depth of our single-elementHIFU device. If a multiple-element HIFU phased arrayconfiguration is used, the focus may be electronicallyrepositioned, allowing treatment of injuries throughoutthe liver. Treatment could also benefit from integratingHIFU phased array with 3-D US imaging. In our study,3-D mapping of the injured surface while holding the
device stationary would allow the HIFU phased array to
118 Ultrasound in Medicine and Biology Volume 33, Number 1, 2007
be applied with minimal movement of the device. Thiswould reduce the dependency on the operator to targetthe incision correctly and would likely further reduce thetime to hemostasis.
The current study was designed as an efficacy studyof US image-guided HIFU treatment of nonvisible liverbleeding. To replicate more closely inaccessible liverinjuries seen in trauma patients, future studies shouldinclude treatment of thicker regions closer to the hilumof porcine liver. Treatment of these regions would re-quire a device with a long and variable focal length aswell as high acoustic intensities to account for the addi-tional tissue attenuation losses. We have been developinghigh-power HIFU applicators for treatment through thicktissue layers (�10 cm) as well as treatment of largeblood vessels (�1 cm). These devices may prove valu-able in sealing high-grade occult liver injuries.
SUMMARY
The results of this study indicate that US image-guided HIFU can successfully arrest nonvisible bleedingin the posterior liver parenchyma. HIFU has the ability toinduce hemostasis via cauterization of a select volume oftissue situated deep beneath the surface of a solid organ.This unique capability allows image-guided HIFU totreat injured tissue regions that are difficult to access,thereby providing a means of remote hemorrhage con-trol.
Acknowledgements—This work was supported by US Army RemoteAcoustic Hemostasis grant DAMD17-02-2-0014, National Institutes ofHealth grant R01 EB00292 and National Space Biomedical ResearchInstitute Postdoctoral Fellowship PF00505 through NASA NCC 9-58.The authors thank Frank Starr for his expert help during animalexperiments.
REFERENCES
Blair SD, Backhouse CM, Harper R, Matthews J, McCollum CN.Comparison of absorbable materials for surgical haemostasis. Br JSurg 1988;75:969–971.
Buckman RF Jr, Miraliakbari R, Badellino MM. Juxtahepatic venousinjuries: A critical review of reported management strategies.J Trauma 2000;48:978–984.
Catalano O, Lobianco R, Sandomenico F, D’Elia G, Siani A. Real-timecontrast-enhanced ultrasound of the spleen: Examination techniqueand preliminary clinical experience. Radiol Med (Torino) 2003;106:338–356.
Christensen DA. Ultrasonic bioinstrumentation. New York: Wiley,1988:235.
Cogbill TH, Moore EE, Jurkovich GJ, et al. Severe hepatic trauma: Amulti-center experience with 1,335 liver injuries. J Trauma 1988;28:1433–1438.
Cohn SM, Cross JH, Ivy ME, Feinstein AJ, Samotowka MA. Fibringlue terminates massive bleeding after complex hepatic injury.J Trauma 1998;45:666–672.
Cornejo CJ, Vaezy S, Jurkovich GJ, et al. High-intensity ultrasoundtreatment of blunt abdominal solid organ injury: An animal model.
J Trauma 2004;57:152–156.Deng CX, Dogra V, Exner AA, et al. A feasibility study of highintensity focused ultrasound for liver biopsy hemostasis. Ultra-sound Med Biol 2004;30:1531–1537.
Di Nisio M, Middeldorp S, Buller HR. Direct thrombin inhibitors.N Engl J Med 2005;353:1028–1040.
Dowling RD, Ochoa J, Yousem SA, Peitzman A, Udekwu AO. Argonbeam coagulation is superior to conventional techniques in repair ofexperimental splenic injury. J Trauma 1991;31:717–720.
Duane TM, Como JJ, Bochicchio GV, Scalea TM. Reevaluating themanagement and outcomes of severe blunt liver injury. J Trauma2004;57:494–500.
Foley JL, Little JW, Starr FL, Frantz C, Vaezy S. Image-guided HIFUneurolysis of peripheral nerves to treat spasticity and pain. Ultra-sound Med Biol 2004;30:1199–1207.
Gananadha S, Daniel S, Zhao J, Morris DL. An experimental evalua-tion of ablation devices for the local treatment of the liver resectionedge. Eur J Surg Oncol 2005;31:528–532.
Gelet A, Chapelon JY, Bouvier R, et al. Transrectal high intensityfocused ultrasound for the treatment of localized prostate cancer:factors influencing the outcome. Eur Urol 2001;40:124–129.
Held RT, Zderic V, Nguyen TN, Vaezy S. Annular phased-arrayhigh-intensity focused ultrasound device for image-guided therapyof uterine fibroids. IEEE Trans Ultrason Ferroelectr Freq Control2006;53:335–348.
Hoyt DB, Bulger EM, Knudson MM, et al. Death in the operatingroom: an analysis of a multi-center experience. J Trauma 1994;37:426–432.
Hynynen K, Jolesz FA. Demonstration of potential noninvasive ultra-sound brain therapy through an intact skull. Ultrasound Med Biol1998;24:275–283.
Liu JB, Merton DA, Goldberg BB, et al. Contrast-enhanced two- andthree-dimensional sonography for evaluation of intra-abdominalhemorrhage. J Ultrasound Med 2002;21:161–169.
Luo W, Zderic V, Starr F, Paun M, Vaezy S. Contrast-enhancedbleeding detection of punctured femoral artery. J Ultrasound Med2006;25:1169–1177.
Murat F, Lafon C, Gelet A, Martin X, Cathignol D. Bloodless partialnephrectomy through application of non-focused high-intensityultrasound. In: ter Haar GR, Rivens, IH, eds. Therapeutic Ultra-sound: Proceedings of 4th International Symposium on Thera-peutic Ultrasound. Melville, NY: American Institute of Physics,2004:181–184.
Ng KK, Lam CM, Poon RT, et al. Porcine liver: Morphologiccharacteristics and cell viability at experimental radiofrequencyablation with internally cooled electrodes. Radiology 2005;235:478 – 486.
Noble ML, Vaezy S, Keshavarzi A, et al. Spleen hemostasis usinghigh-intensity ultrasound: Survival and healing. J Trauma 2002;53:1115–1120.
Parks RW, Chrysos E, Diamond T. Management of liver trauma. Br JSurg 1999;86:1121–1135.
Poliachik SL, Chandler WL, Mourad PD, Ollos RJ, Crum LA. Acti-vation, aggregation and adhesion of platelets exposed to high-intensity focused ultrasound. Ultrasound Med Biol 2001;27:1567–1576.
Rabkin B, Zderic V, Vaezy S. Real-time color-Doppler guidance ofHIFU for the selective avoidance or occlusion of blood vessels.In: ter Haar GR, Rivens, IH, eds. Therapeutic Ultrasound: Pro-ceedings of 4th International Symposium on Therapeutic Ultra-sound. Melville, NY: American Institute of Physics, 2004:65–67.
ter Haar G. Ultrasound focal beam surgery. Ultrasound Med Biol1995;21:1089–1100.
ter Haar GR. High intensity focused ultrasound for the treatment oftumors. Echocardiography 2001;18:317–322.
Tovar MC, Sanchez-Valverde MA, Agut A, Laredo FG, Murciano J.Comparative study of air coagulation, fibrin sealant, and suture in
experimental liver injury. Eur J Surg 1998;164:57–63.
HIFU hemostasis in posterior liver ● S. BURGESS et al. 119
Trunkey DD. Hepatic trauma: Contemporary management. Surg ClinNorth Am 2004;84:437–450.
Vaezy S, Martin R, Kaczkowski P, et al. Use of high-intensity focusedultrasound to control bleeding. J Vasc Surg 1999;29:533–542.
Vaezy S, Martin R, Crum L. High intensity focused ultrasound: Amethod of hemostasis. Echocardiography 2001a;18:309–315.
Vaezy S, Shi X, Martin RW, et al. Real-time visualization of high-intensity focused ultrasound treatment using ultrasound imaging.
Ultrasound Med Biol 2001b;27:33–42.Vaezy S, Noble ML, Keshavarzi A, et al. Liver hemostasis withhigh-intensity ultrasound: Repair and healing. J Ultrasound Med2004;23:217–225.
Wadia Y, Xie H, Kajitani M. Liver repair and hemorrhage control byusing laser soldering of liquid albumin in a porcine model. LasersSurg Med 2000;27:319–328.
Wu F, Chen WZ, Bai J, et al. Pathological changes in human malignantcarcinoma treated with high-intensity focused ultrasound. Ultra-
sound Med Biol 2001;27:1099–1106.