Embed Size (px)
Citation preview

Harpreet Singh, PhDCo-Founder & CSO
immatics biotechnologies GmbH, Tuebingen (Germany)
iSBTc 2007, Boston MA
IMA901- a novel multi-peptide vaccinefor treatment of renal cell carcinoma

2 TUMAPs = tumor-associated HLA-binding peptides
© Hans-Georg Rammensee (1991)
3 immatics biotechnologies
Approach
• Develop therapeutic cancer vaccines based on multiple peptides derived from tumor-associated antigens
• Use novel peptides confirmed to be naturally presented on primary tumor tissue
• Multi-peptide vaccines are fully synthetic and provided as stable, lyophilized formulation
• Perform multi-centre clinical trials with centralized and highly standardized immunomonitoring

4
1 2 3 4 5R1
R30
5
10
15
20
XPRESIDENT™ platform for identification of novel and naturally presented tumor-associated pepties
blood
Tumor cellsNormal cells
mRNA
Over-expression tumor vs. healthy
Gene Chips
HLA peptides
TUMAPsequences
LC-MS/MS
T cells
Selection of strongly immunogenic TUMAPs from
relevant tumor antigens
Synthesis of candidate TUMAPs
Collection of tissue samples
Correlation
ELISpot HLA tetramers
Immunoassays

A novel HLA-A*02-biding tumor-associated peptide fromc-met proto-oncogene
5
0.00.00.10.00.22.1
0.10.90.60.71.01.72.8
1.1 0.50.20.20.90.10.30.40.01.00.80.2
7.5
13.0
9.8
12.113.9
13.0
26.0
6.5
4.3
8.0
16.0
22.6
5.3
13.0
16.0
0.7
9.88.6
24.3
leukocytes
CD
3+
cells
CD
19
+cells
den
dritic cells
adren
al glan
d
blad
der
bon
e marrow
wh
ole brain
colon
heart
kidn
ey
liver
lun
g
placen
ta
prostate
salivary glan
d
small in
testine
skeletal mu
scle
spleen
stomach
testis
thym
us
thyroid
trachea
uteru
s
RC
C0
04
4T
RC
C0
06
8T_
a
RC
C0
07
0T
RC
C0
07
3T
RC
C0
07
5T
RC
C0
09
8T
RC
C0
10
3T
RC
C0
10
8T
RC
C0
11
2T
RC
C0
11
5T
RC
C0
11
6T
RC
C0
06
8T_
b
RC
C0
10
0T
RC
C0
11
9T
RC
C0
13
0T
RC
C0
13
3T
RC
C0
13
5T
RC
C0
14
6T
RC
C0
14
9T
rela
tive
expr
essi
on
203510_at
Healthy tissues RCC tumors
% S
peci
fi c L
ysi s
E:T
Croft (A2+Met-)
HCT 116 (colon)
K 562 (NK-sensitive)
SK-OV-3 (A2-Met+)
MZ 1257 (renal)MEL 1479 (melan.)SK-OV-3 (A2-Met+)
% S
peci
fi c L
ysi s
-10
0
10
20
30
40
0,1 1 10 100
-100
102030405060
0,1 1 10 100
E:T
A 498 (renal)
SK-OV-3 (A2-Met+)
K 562 (NK-sensitive)
Croft (A2+Met-)
MCF-7 (breast)
U 266 (myelom.)
K 562 (NK-sensitive)
SK-OV-3 (A2-Met+)
-20
0
20
40
60
80
0,1 1 10 100
0
10
20
30
40
50
0,1 1 10 100

6 TUMAP Development Platform
1. Shotgun Identification *
~100 promisingTUMAPs
7. Pharmaceutical development
2000-5000 peptides associated with selected type of cancer
Pre-clinical Development
Month 24 Month 12
Phase 1
Month 0
Product candidate comprising 10-12 TUMAPs
2. Expression analysis *3. Functional analysis4. TUMAP re-detection **5. TUMAP quantification **6. TUMAP validation *
8. GMP manufacturing9. Filing of IMPD/IND
~20 high-potentialTUMAPs
* patented / ** proprietary know how
Screen – Hit – Lead – Drug Candidate

7 IMA901
IMA901: renal cell cancer• status: phase 2 started in September 2007
• >200,000 new incidences worldwide (approx. 3% of all cancers),thereof approx. 60% late-stage
• 5-year survival rate <10% in stage IV disease
• Approved therapies: cytokines, TKIs (sorafenib, sunitinib, temsirolimus)
• RCC known as immunogenic tumor
• HLA class I and class II expression directly by tumor cells
HLA class II expression in healthy renal tisusue (endothelial cells and monocytes)
HLA class II expression in RCC
Histology by Karin Klingel, Tübingen

8Composition of IMA901 for treatment of renal cell carcinoma
# Peptide ID Allele Antigen Common acronyms and synonyms
1 IMA-ADF-001 HLA-A*02 Adipophilin adipose differentiation-related protein, ADRP
2 IMA-APO-001 HLA-A*02 Apolipoprotein L1 APOL1
3 IMA-CCN-001 HLA-A*02 Cyclin D1 CCND1, PRAD1, parathyroid adenomatosis 1, BCL-1
4 IMA-GUC-001 HLA-A*02 GUCY1A3 guanylate cyclase 1-soluble-alpha 3
5 IMA-K67-001 HLA-A*02 KIAA0367 --
6 IMA-MET-001 HLA-A*02 c-met proto-oncogene MET, HGF (hepatocyte growth factor) receptor, HGFR
7 IMA-MUC-001 HLA-A*02 MUC1 mucin, CD227, episialin, epithelial membrane antigen
8 IMA-RGS-001 HLA-A*02 RGS-5 regulator of G-protein signalling 5
9 IMA-ADF-002 HLA-A*02 Adipophilin adipose differentiation-related protein, ADRP
10 IMA-MMP-001 HLA-DR MMP7 matrix metalloproteinase 7
11 IMA-HBV-001 HLA-A*02 HBV core Antigen HBc, HBcAg, cAg

9
An open label study to evaluate safety and immunogenicity
of the peptide based therapeutic cancer vaccine IMA901injected intradermally with GM-CSF as adjuvant
in patients with renal cell carcinoma
Phase 1
Study Code IMA901-101
A. Stenzl, University Hospital of TübingenM. Stähler / Ch. Stief, Klinikum Grosshadern, Munich
P.Y. Dietrich, University Hospital of GenevaA. Haferkamp / M. Hohenfellner, University of Heidelberg
J. Beck, University of MainzT. Eisen, Royal Marsden Hospital, London
IMA901 Phase 1 Study

10 IMA901 Phase 1 Study
IMA901 phase 1 study outline• Design multi-centre, single arm phase 1
• Patients 28 patients with advanced renal cell carcinoma (HLA-A*02-positive)
• Scope 6 centers, 3 countries (DE, CH, UK)
• Dose 4.5 mg (400 µg per peptide) IMA901 i.d. 8x75 µg GM-CSF i.d. 8x
• Primary Endpoint Systemic safety, local tolerability
• Secondary Endpoints - Immunogenicity of IMA901- Pharmacokinetics intradermal GM-CSF- Any evidence of anti-tumor response
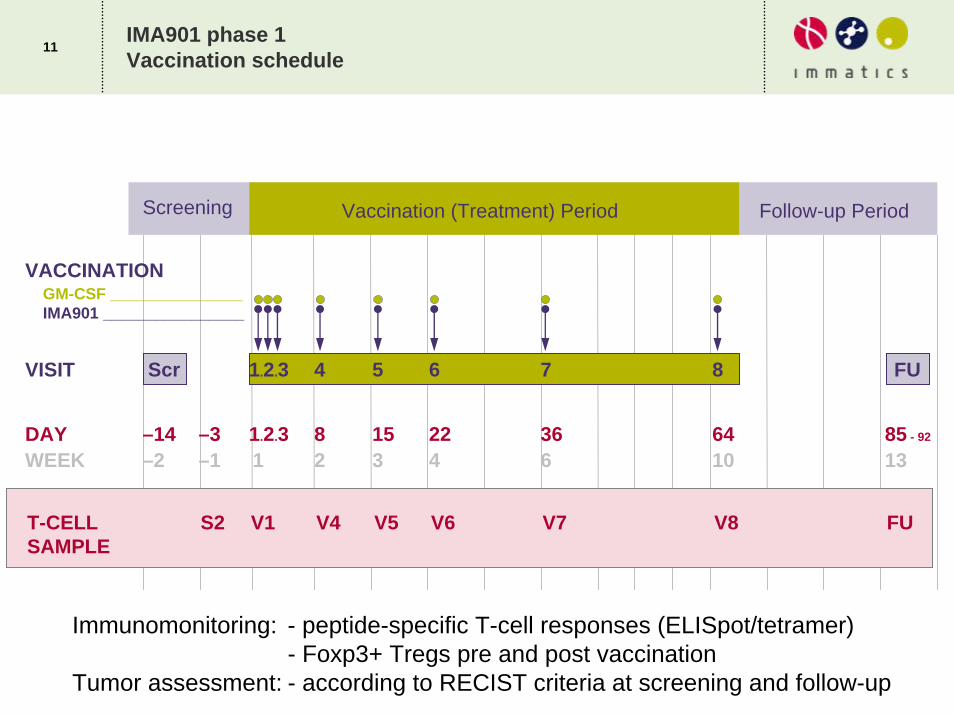
11IMA901 phase 1 Vaccination schedule
VACCINATIONGM-CSF _______________IMA901 ________________
WEEKDAY 85 - 92
Follow-up Period
VISIT 1.2.3 4 5 6 7 8
1 2 3 4 6 10–1–2 131.2.3 8 15 22 36 64–3–14
Screening Vaccination (Treatment) Period
Scr FU
T-CELLSAMPLE
FUV1 V4 V5 V6 V7 V8S2
Immunomonitoring: - peptide-specific T-cell responses (ELISpot/tetramer)- Foxp3+ Tregs pre and post vaccination
Tumor assessment: - according to RECIST criteria at screening and follow-up

12IMA901 Phase 1 ImmunomonitoringExample for raw data in tetramer assay
20060517a.039
FL2-H
010
110
210
310
410
FL4-
H
010
110
210
310
410
0.01%99.98%
0.00%0.01%
20060517a.039
FL1-H
010
110
210
310
410
FL2-
H
010
110
210
310
410
20060517a.039
FL1-H
010
110
210
310
410
FL4-
H
010
110
210
310
410
20060517a.040
FL2-H
010
110
210
310
410
FL4-
H
010
110
210
310
410
0.09%99.57%
0.00%0.34%
20060517a.040
FL1-H
010
110
210
310
410
FL2-
H
010
110
210
310
410
20060517a.040
FL1-H
010
110
210
310
410
FL4-
H
010
110
210
310
410
20060502a.044
FL2-H
010
110
210
310
410
FL4-
H0
10
110
210
310
410 0.04% 0.00%
99.96% 0.01%
20060502a.044
FL1-H
010
110
210
310
410
FL2-
H
010
110
210
310
410
20060502a.044
FL1-H
010
110
210
310
410
FL4-
H
010
110
210
310
410
20060503a.029
FL2-H
010
110
210
310
410
FL4-
H
010
110
210
310
410 0.01% 0.00%
99.55% 0.44%
20060503a.029
FL1-H
010
110
210
310
410
FL2-
H
010
110
210
310
410
20060503a.029
FL1-H
010
110
210
310
410
FL4-
H0
10
110
210
310
410
05-001 S2+V1FL1: CD8FL2: rK67-001FL4: rCCN-001
05-001 V4+V5FL1: CD8FL2: rK67-001FL4: rCCN-001
03-003 V4+V5FL1: CD8FL2: rK67-001FL4: MET-001
03-008 V6+V7FL1: CD8FL2: MUC-001FL4: ADF-002

13T-cell Responses in Phase 1IMA901-101 Immunomonitoring
Vaccine-induced T-cell responses
• N=27 patients evaluable for immune response• T-cell response measured with ELISpot and tetramer assays
0%
52%
85%
74%
30%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Negative controlpeptide (HIV)
Viral marker peptide(HBV)
At least 1 response toany TUMAP or HBV
At least 1 response toany TUMAP
Multi-TUMAPresponses
Vacc
ine-
indu
ced
imm
une
resp
onde
rs

14IMA901 Phase 1 ImmunomonitoringKinetics
T-cell response kinetics (representative patient)
Patient 03004
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
S2 V1 V4 V5 V6 V7 V8 FU
Scheduled timepoint (scale in weeks)
% T
etra
mer
+ am
ong
CD
8+ T
-cel
ls
TUMAP PoolHBV-001HIV-001

15IMA901 Phase 1 ImmunomonitoringEx vivo phenotyping
Phenotyping of T-cell response (ex vivo, N=1)
• Pre-vaccine T cells are of naïve phenotype
• Post-vaccine T cells are of effector memory phenotype
20060727a.021
FL3-H
010
110
210
310
410
FL4-
H
010
110
210
310
410
20060727a.021
FL1-H
010
110
210
310
410
FL2-
H
010
110
210
310
410
20060727a.022
FL1-H
010
110
210
310
410
FL2-
H
010
110
210
310
410
20060727a.022
FL3-H
010
110
210
310
410
FL4-
H
010
110
210
310
410
20060727a.023
FL1-H
010
110
210
310
410
FL2-
H
010
110
210
310
410
20060727a.023
FL3-H
010
110
210
310
410
FL4-
H
010
110
210
310
410
01-009 V1FL1: CD45RAFL2: CCR7FL3: CD8FL4: rCCN-001
01-009 V5FL1: CD45RAFL2: CCR7FL3: CD8FL4: rCCN-001
01-009 V7FL1: CD45RAFL2: CCR7FL3: CD8FL4: rCCN-001

16IMA901 Phase 1 ImmunomonitoringExample for Treg quantification
20060725a.044
FSC-H0 256 512 768 1024
SS
C-H
0
256
512
768
1024
lymphocytes
20060725a.044
FL1-H
010 110 210 310 410FL
3-H
010
110
210
310
410 CD45+ CD4+ CD45+
20060725a.044
FL1-H
010 110 210 310 410
FL2-
H
010
110
210
310
410
39,71%57,39%
2,72%0,18%
20060725a.050
FSC-H0 256 512 768 1024
SS
C-H
0
256
512
768
1024
lymphocytes
20060725a.050
FL1-H
010 110 210 310 410
FL3-
H
010
110
210
310
410 CD45+ CD4+ CD45+
20060725a.050
FL1-H
010 110 210 310 410FL
2-H
010
110
210
310
410
36,25%56,54%
7,02%0,18%
Gated on CD45+ lymphocytes -> automatic quadrant setting!
Patient 03-003pre-vacc.
Patient 03-006pre-vacc.
FL1: CD4FL2: Foxp3FL3: CD45
Gated on all cells. Gated on lymphocytes.

17IMA901 phase 1 immunomonitoringRegulatory T cells and T-cell response
Patients with multiple TUMAP responses have significantly lower TREGlevels in the periphery than patients with 0-1 TUMAP responses (p=0.016 Wilcoxon Test, N=26 pts)
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
-1 0 1 2 3 4
No. of TUMAP responses in patients
% F
oxp3
+ Tr
egs
of C
D45
+ ly
mph
ocyt
es
Pre-vaccinationPost-vaccinationAverage Pre-v.Average Post-v.

18Efficacy - Change of tumor size and T-cell response (ITT, n=28)
17 158
0024 2 0 0 0 0 00
52
145
25
46
10
263133
-27-38
-9-6-3
-60
-40
-20
0
20
40
60
80
100
120
140
16004
-001
05-0
05
03-0
12
03-0
13
01-0
07
05-0
02
01-0
01
01-0
10
05-0
04
03-0
04
03-0
06
03-0
02
01-0
11
03-0
15
03-0
05
03-0
09
03-0
16
01-0
02
01-0
03
01-0
08
02-0
01
03-0
01
05-0
01
03-0
03
06-0
04
01-0
09
03-0
08
03-0
14
patient numbers
% c
hang
e fr
om b
asel
ine
% increase % decrease
New
lesi
ons
New
lesi
ons
New
lesi
ons
New
lesi
ons
New
lesi
ons
New
lesi
ons
New
lesi
ons
New
lesi
ons
New
lesi
ons
New
lesi
ons
New
lesi
ons
MET
-001
MU
C-0
01, G
UC
-001
CC
N-0
01
ADF-
002
CC
N-0
01
CC
N-0
01, M
ET-
001
CC
N-0
01, K
67-0
01
CN
N-0
01
CC
N-0
01
CC
N-0
01
CC
N-0
01, A
DF-
001,
GU
C-0
01
CC
N-0
01, M
ET-
001,
GU
C-0
01
MU
C-0
01,
CC
N-0
01, A
DF-
001
CC
N-0
01, K
67-0
01
CC
N-0
01
AD
F-00
2, A
PO
-001
CC
N-0
01
MET
-001
not e
valu
able
ADF-
002
CC
N-0
01
No
FU tu
mor
ass
essm
ent
New
lesi
ons
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r
HBV
resp
onde
r

19IMA901 Clinical Study Phase 1Conclusions
IMA901 is safe and well tolerated (data not shown)
IMA901 is immunogenic
• Vaccine-induced immune responses in 74% of pts.
• Multiple vaccine-induced responses in 30% of pts.
Multiple vaccine-induced immune responses to IMA901
• seem to inversely correlate with the level of regulatory T cells prior to vaccinaton (p=0.016)
• seem to correlate with the clinical outcome (partial response and stable disease according to RECIST) (p=0.015)
Next: multi-centre phase 2 trial in Europe (started Sept 2007)
• ~70 met RCC pts., 2nd line after TKI or cytokine therapy failure
• continous vaccination for 9 months, evaluation of the disease control rate at 6 months
• Evaluation of the impact of low-dose cyclophosphamide on Tregs, MDSC and immune responses in a randomized fashion (+/- CY)

20
Broad-spectrum tyrosine kinase inhibitors (TKIs) were recently approved for treatment of metastatic RCC pts
Question: can TKIs be combined with vaccination simultaneously or sequentially?
Assessment of impact of sorafenib and sunitinib on immune cells in vitro and in vivo
Impact of sunitinib and sorafenib on immune cells

21 Impact of sunitinib and sorafenib on immune cells
Sorafenib but not sunitinib inhibits human T-cell activation in (allogeneic) mixed lymphocyte culture
• Data not shown: very similar observation for CD4+ T cells
CD8+
0,0%
10,0%
20,0%
30,0%
40,0%
50,0%
60,0%
70,0%
A2+ A2+ A2+ A2+ A2+ A2+ A2+ A2+ A2+ A2+ A2+ A2+ A2+ A2+
none A2+ A2+ A2+ A2- A2- A2- A2- A2- A2- A2- A2- A2- A2-
DMSO none Sorafenib13 µM
Sunitinib250 nM
none DMSO Sorafenib1.6 µM
Sorafenib3.3 µM
Sorafenib6.5 µM
Sorafenib13 µM
Sunitinib31 nM
Sunitinib63 nM
Sunitinib125 nM
Sunitinib250 nM
Effector / Target / TKI
% C
FSE-
/ A
2+ C
D8+
Lym
phoc
ytes

22 Impact of sunitinib and sorafenib on immune cells
Sorafenib and sunitinib have no impact on human T-cell activation by artificial peptide-presenting APCs in vitro
Melan-A-specific CD8+ T-cell in vitro priming
HBC-133
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
Mock Mock Sunitinib250 nM
Sunitinib125 nM
Sunitinib63 nM
Sunitinib31 nM
Sorafenib13 µM
Sorafenib6.5 µM
Sorafenib3.3 µM
Sorafenib1.6 µM
DDX5-001HD
MLA-001HD
MLA-001HD
MLA-001HD
MLA-001HD
MLA-001HD
MLA-001HD
MLA-001HD
MLA-001HD
MLA-001HD
% M
LA-0
01+

23 Impact of sunitinib and sorafenib on immune cells
Sorafenib but not sunitinib inhibits the LPS-mediated maturation of human mDCs in vitro
• Data not shown: no effect of sunitinib on maturation of mDCs
• Data not shown: sorafenib but not sunitinib affects the migrations capacities of mDCs and downmodulates CCR7
Hipp et al., submitted
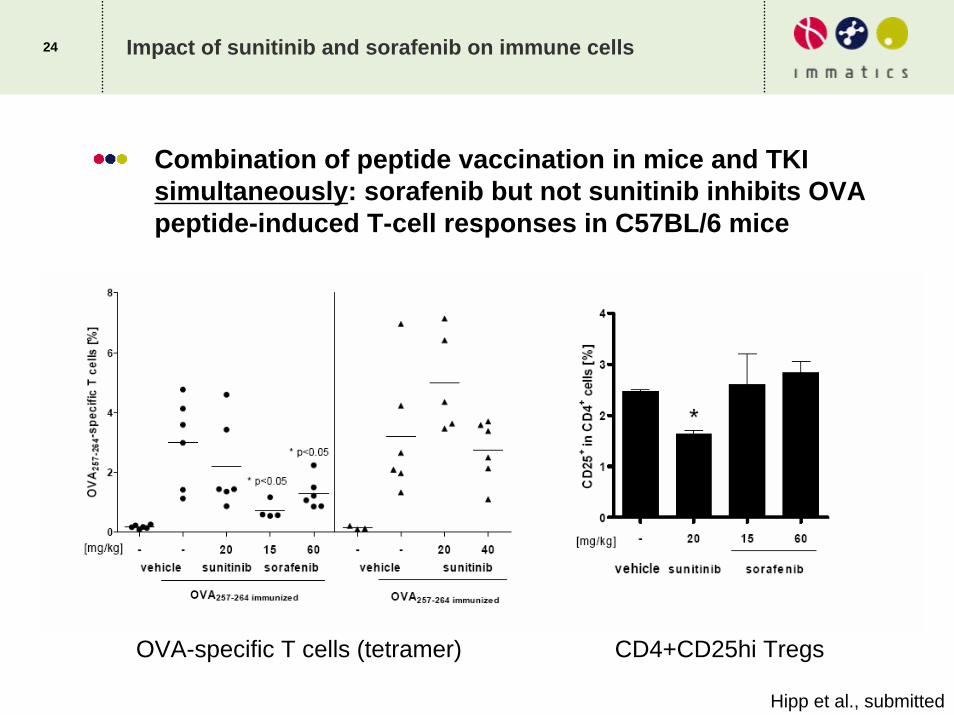
24 Impact of sunitinib and sorafenib on immune cells
Combination of peptide vaccination in mice and TKI simultaneously: sorafenib but not sunitinib inhibits OVA peptide-induced T-cell responses in C57BL/6 mice
Hipp et al., submitted
OVA-specific T cells (tetramer) CD4+CD25hi Tregs

25
Sunitinib is compatible with• in vitro antigen-induced T-cell expansion (human and
mouse)
• in vitro TLR-mediated DC maturation (human)
• in vivo peptide-induced T-cell proliferation (mouse)
On the other hand, sorafenib significantly inhibits all of these immunological endpoints• but: the inhibition by sorafenib is reversible within days in
mice (not shown)
Sunitinib but not sorafenib slightly decreases regulatory T cell levels in miceSorafenib but not sunitinib affects MyD88-dependent and MyD88-independent signaling pathways in APCs (not shown)
Impact of sunitinib and sorafenib on immune cellsConclusions

26
Peter BrossartMadeleine HippDaniela WerthKatharina Brauer
Arnulf StenzlMarkus KuczykSusan FeyerabendJörg Hennenlotter
Hans-Georg RammenseeStefan StevanovicCécile Gouttefangeas
Co-workers and CollaboratorsIMA901 Pre-clinical and Phase 1 / TKI project
IMA901 Discovery TeamToni WeinschenkClaudia LemmelJörn DengjelOliver SchoorNorbert HilfMartin PriemerSilvia RothBettina StreileSylvia ZwickerAntje ArthurColette Song
IMA901-101 Immuno-monitoring TeamSteffen WalterNicole ArnoldMonique GoerlVerona Vass
IMA901-101 CMC TeamPeter LewandrowskiWerner StüberJessica BergmannChristian FlohrVerena Beyer
IMA901-101 Clinical TeamJürgen FrischAndrea MayerAnnette SchmidTamara SpürginAngela Arena
Scientific Advisory BoardHans-Georg RammenseeCornelius MeliefChristoph HuberPedro RomeroCraig Slingluff Jr.






![ComputationalVaccinology:AnImportantStrategyto … · 2011. 6. 1. · DNA vaccine ND IgG, IgG1 > IgG2a ND 38.1% ND [33] Sm 25 Peptide vaccine ND IgG No significative difference](https://img.dokumen.tips/doc/110x75/609fc21e5f4e7561c46ccc5b/computationalvaccinologyanimportantstrategyto-2011-6-1-dna-vaccine-nd-igg.jpg)






![WT1 Peptide Cancer Vaccine for Patients with Hematopoietic ...downloads.hindawi.com/journals/tswj/2007/394078.pdfsyndromes (MDS), and solid cancers[8,910,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25]](https://img.dokumen.tips/doc/110x75/6040cd2c0d0058478d0de4dc/wt1-peptide-cancer-vaccine-for-patients-with-hematopoietic-syndromes-mds.jpg)















