Embed Size (px)
Citation preview

Iliac compression syndrome and recanalization offemoropopliteal and iliac venous thrombosis: Aprospective study with magnetic resonancevenographyDouglas G. W. Fraser, MRCP,a Alan R. Moody, FRCR,b Paul S. Morgan, PhD,d and Anne Martel,PhD,c Birmingham and Nottingham, England; and Toronto, Canada
Objectives: Poor iliac vein recanalization has been associated with compression of the left common iliac vein by the rightcommon iliac artery (RCIA/LCIV compression); however, this finding has been difficult to confirm. In a baseline study,RCIA/LCIV compression was detected with magnetic resonance imaging in patients with deep venous thrombosis. Wecompared recanalization of left femoropopliteal and iliac thrombosis with and without RCIA/LCIV compression.Methods: This was a prospective blinded study carried out in a 1355-bed university hospital. Thirty-one patients wererecruited from consecutive cohorts of patients with iliofemoral and femoropopliteal DVT who underwent directthrombus magnetic resonance imaging, venous enhanced peak arterial magnetic resonance venography, and magneticresonance arteriography as part of the baseline study relating RCIA/LCIV compression to extent of thrombosis.Magnetic resonance venography was performed 6 weeks, 6 months, and 1 year after diagnosis of deep venous thrombosis.Femoropopliteal and iliac venous segments that were occluded at diagnosis were classified as occluded, partially occluded,or patent on follow-up scans.Results: At 6-week follow-up, recanalization of all segments was incomplete. At both 6-month and 1-year follow-up,recanalization of left iliac segments associated with RCIA/LCIV compression was poorer compared with recanalizationof left iliac segments not associated with compression (6 of 6 occluded vs 1 of 6 occluded and 1 of 6 partially occluded at6 months, P �.015; 6 of 6 occluded vs 5 of 5 patent at 1 year, P � .002). This was due to complete failure of recanalizationof left common iliac veins associated with RCIA/LCIV compression in 6 of 6 cases. All other iliac and femoropoplitealsegments including left external iliac veins associated with RCIA/LCIV compression had high rates of recanalization atboth 6 months and 1 year.Conclusion: RCIA/LCIV compression is associated with persistent occlusion of the left common iliac vein. Therecanalization rate for all other femoropopliteal and iliac segments was high. (J Vasc Surg 2004;40:612-19.)
Obstruction of the proximal lower limb veins has asignificant additive effect with valvular reflux in the devel-opment of ambulatory venous hypertension and post-phle-bitic disease.1-4 Serial duplex ultrasound scanning hasshown high recanalization rates for femoral and poplitealthrombosis.5-7 However, recanalization rates for iliacthrombosis are poor. Studies using radionuclide and con-ventional venography have reported that 65% to 82% ofiliac segments remain obstructed and 35% to 59% remainoccluded 5 to 10 years after deep venous thrombosis(DVT).8-11 Cockett and colleagues12,13 proposed thatcompression of the left common iliac vein by the rightcommon iliac artery (RCIA/LCIV compression) is a fre-
From the Department of Cardiology, Queen Elizabeth Hospital,a Birming-ham, Departments of Medical Imaging,b and Medical Physics,c Sunny-brook and Women’s College Health Sciences Centre, Toronto, andDepartment of Academic Radiology, University Hospital,d Nottingham.
Supported by the British Heart Foundation.Competition of interest: none.Reprint requests: Dr Douglas Fraser, 3 Aboyne Close, Birmingham, UK
(e-mail: [email protected]).0741-5214/$30.00Copyright © 2004 by The Society for Vascular Surgery.doi:10.1016/j.jvs.2004.05.029
612
quent cause of left iliofemoral thrombosis, and causes fail-ure of subsequent recanalization, which leads to persistentiliac vein occlusion. This mechanism has been difficult toconfirm. However, defects attributed to RCIA/LCIVcompression are commonly detected after thrombus re-moval via catheter-directed thrombolysis and thrombec-tomy in acute iliofemoral DVT.10,14,17
In a baseline study, 2 MRI sequences were used todetect RCIA/LCIV compression in patients with acuteDVT. Venous enhanced peak arterial magnetic resonancevenography (VESPA) was used to produce both veno-graphic and arteriographic images (magnetic resonancevenography [MRV] and magnetic resonance angiography[MRA] images) and thereby visualize the anatomy ofpatent iliac veins and the iliac arteries; thrombosed iliacveins were visualized with magnetic resonance directthrombus imaging (MRDTI).18,19 These sequences en-abled RCIA/LCIV compression to be detected noninva-sively in patients with acute iliofemoral thrombosis, andshowed that RCIA/LCIV compression is strongly associ-ated with left iliofemoral DVT in which distal thrombosis iseither absent (isolated iliofemoral DVT) or not contiguouswith the thrombus in the iliac veins (Fig 1).

JOURNAL OF VASCULAR SURGERYVolume 40, Number 4 Fraser et al 613
The purpose of this study was to use MRV to assess therelationship between RCIA/LCIV compression detectedin the baseline study and subsequent femoropopliteal andiliac vein recanalization.
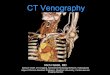
Fig 1. Number of thrombosed segments at baseline dleft-sided deep venous thrombosis (DVT) associated comiliac artery (RCIA/LCIV compression) and in patienRCIA/LCIV compression. Details of the presence of calffrom the calf (*) are shown. Patients with left ileofemdifferent pattern of thrombosis than did patients with ile
MATERIAL AND METHODSThe ethical committee at our institution granted ap-
proval for the study, and all patients gave written informedconsent. Inclusion criteria included treatment with antico-
d according to pattern of thrombosis in patients withsion of the left common iliac vein by the right commonith left-sided or right-sided DVT in the absence ofbosis and details of whether thrombosis was contiguousVT associated with RCIA/LCIV compression had a
oral DVT not associated with such compression.
ivideprests wthromoral Dofem

JOURNAL OF VASCULAR SURGERYOctober 2004614 Fraser et al
agulation and willingness to undergo repeat magnetic res-onance imaging (MRI). Exclusion criteria included previ-ous ipsilateral femoropopliteal or ileofemoral DVT,treatment with thrombolysis or thrombectomy, recurrentipsilateral DVT during the study period, and advancingcancer.
MRV at diagnosis was used to assess the presence ofoccluded venous segments. Venous segments with nonoc-clusive thrombus were not recorded. Recanalization of theoccluded segments was assessed with repeat MRV at 6weeks, 6 months, and 12 months. Once full recanalizationoccurred, repeat scans were not obtained and continuedpatency was assumed. Femoropopliteal and iliac venoussegments with occlusive thrombus were graded as patent,partially occluded, or occluded on follow-up studies.
Further analysis included separate assessment of recan-alization within popliteal, femoral, common femoral, exter-nal iliac, and common iliac veins. Recanalization of venoussegments in the left leg associated with RCIA/LCIV com-pression was then compared with recanalization of venoussegments in the left or right leg not associated with suchcompression.
Detection of RCIA/LCIV compression in baselinestudy. Patent left common iliac veins (LCIVs) were visu-alized with multiplanar reconstruction of the MRV data-sets, and thrombosed LCIVs were visualized with multipla-nar reconstruction of the MRDTI datasets. The positionsof the right common iliac artery (RCIA) and LCIA werevisualized in relation to stenoses of the LCIV by overlayingthe corresponding MRA images. RCIA/LCIV compres-sion was defined as greater than 50% reduction in luminalcross-sectional area of the LCIV at the point where theLCIV was crossed by the RCIA. A threshold of 50% luminalnarrowing has previously been used for angioplasty ofvenous spurs thought to be caused by RCIA/LCIV com-pression after catheter-directed thrombolysis.15 Image in-terpretation was performed by 2 reviewers at the time ofacquisition.
Assessment of femoropopliteal and iliac vein reca-nalization. Recanalization was determined with MRV. Ateach study, unblinded image interpretation was performedby reviewer A, and if persistent occlusion was present,repeat scanning was arranged as per protocol. After com-pletion of the study, repeat interpretation of all scans wasperformed by reviewer B, who was unaware of the time ofeach study or of other test results. The latter interpretationis reported in this study. Interobserver variability of theinterpretations made by reviewers A and B was calculated.
Interpretation of MRV images was performed withstandard image reconstruction techniques together withanalysis of source data. Venous segments were classified asoccluded in the presence of nonfilling of part or the entiresegment. Partial occlusion was defined qualitatively asmarked narrowing of the lumen visually estimated to beequivalent to a reduction in cross-sectional area of 70% orgreater.
MRI sequences. MRDTI is a high-resolution, T1-weighted, magnetization–prepared 3-dimensional gradi-
ent-echo sequence.19 Fat and blood signals are suppressedby using a selective water-excitation pulse, and an inversiontime is chosen to null blood signal. Acute thrombus isvisualized as high signal against a suppressed background.
VESPA is a 3-dimensional contrast material–enhancedgradient-echo sequence. Sequential acquisitions before andafter a contrast material bolus produce background images,early arterial phase images, and late venous phase images.MRA images are produced by using post-processing toremove background signal from early arterial phase images.MRV images are produced by using post-processing toremove arterial and background signal from late venousphase images. In this way selective MRV and MRA imagesare produced.18 In most patients a single field of view wassufficient to visualize the popliteal, femoral, and iliac veins,with 20 mL of contrast (gadopentate dimeglumine; Mag-nevist, Berlex Laboratories). Cases in which a single field ofview did not provide adequate coverage were scanned with2 imaging blocks, covering the popliteal and femoral veinsand the femoral and iliac veins, respectively; 10 mL ofcontrast material was given with the first (distal) set ofmeasurements, and 30 mL was given with the second(proximal) set of measurements.
Statistical analysis. The following comparisons weremade at 6 weeks, 6 months, and 1 year, with the 2-sidedFisher exact test: (1) overall rate of femoropopliteal com-pared with iliac vein recanalization; (2) recanalization of leftiliac veins associated with RCIA/LCIV compression com-pared with recanalization of left iliac veins not associatedwith RCIA/LCIV compression; and (3) recanalization ofleft femoral and popliteal veins associated with RCIA/LCIV compression compared with recanalization of leftand right femoral and popliteal veins not associated withRCIA/LCIV compression.
RESULTS
The baseline study included 18 consecutive patientswith ileofemoral thrombosis and 28 consecutive patientswith femoropopliteal thrombosis. Four patients with fem-oropopliteal thrombosis in the baseline study were ex-cluded because of either nondiagnostic MRDTI, nondiag-nostic MRV, or discordance between these tests andconventional venography. Another 11 patients were ex-cluded from follow-up because of advancing cancer (n �5), unwillingness to undergo further scanning (n � 4),ipsilateral rethrombosis (n � 1), and treatment with throm-bolysis (n � 1). The remaining 19 patients with femoro-popliteal DVT (7 left-sided, 12 right-sided) and 12 patientswith ileofemoral DVT (all left-sided) underwent serialMRV. The pattern of thrombosis in these patients is shownin Fig 1. All patients received anticoagulation therapy for 3months.
Follow-up was incomplete in 3 patients. One patientwith occluded femoral and popliteal segments at 6 weeksand RCIA/LCIV compression died before imaging at 6months. One patient with partially occluded femoral andpopliteal segments in the absence of RCIA/LCIV com-pression declined to undergo imaging at 6 months and 1

JOURNAL OF VASCULAR SURGERYVolume 40, Number 4 Fraser et al 615
year. One patient with occluded common iliac and femoralveins and partially occluded external iliac and commonfemoral veins at 6 months declined to undergo imaging at1 year.
The overall rates of femoropopliteal and iliac recanali-zation were not significantly different at 6 weeks (9 of 12iliac segments occluded and 1 of 12 partially occluded,compared with 17 of 31 femoropopliteal segments oc-cluded and 3 of 31 partially occluded; P � .54). At 6months, recanalization of the iliac segments was poorerthan recanalization of the femoropopliteal segments (7 of12 iliac segments occluded and 1 of 12 partially occluded,compared with 6 of 29 femoropopliteal segments occludedand 0 of 29 partially occluded; P � .011). This differencewas maintained at 1 year (6 of 11 iliac segments occludedand 0 of 11 partially occluded, compared with 3 of 28femoropopliteal segments occluded and 1 of 28 partiallyoccluded; P � .007).
Recanalization of left iliac segments associated withRCIA/LCIV compression (Fig 2) was poorer comparedwith recanalization of left iliac segments not associated withsuch compression at both 6 months (P � .015) and 1 year(P � .002). Iliac occlusions were not observed at 1 year inthe absence of RCIA/LCIV compression. Separate analysisof the external iliac and common iliac veins showed that the
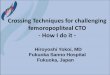
Fig 2. Patency of femoropopliteal and iliac veins duringof the left common iliac vein by the right commonfemoropopliteal and iliac segments not associated with Rwhereas left iliac segments associated with RCIA/LCIVvein recanalization associated with RCIA/LCIV comprthrombosis at presentation and persistent occlusion of adj
site of persistent iliac vein occlusion in cases associated withRCIA/LCIV compression was the left common iliac veinin 6 of 6 cases at 6 months and at 1 year (Fig 3;Table).Recanalization of the left external iliac vein in these cases,though poor at 6 weeks, was successful at 6 and 12 months.
Recanalization of left femoropopliteal segments associ-ated with RCIA/LCIV compression was poorer comparedwith recanalization of left or right femoropopliteal seg-ments not associated with RCIA/LCIV compression at 6weeks (P � .035, figure 2). However, at 6 and 12 months,recanalization of left femoropopliteal segments associatedwith RCIA/LCIV compression was similar to recanaliza-tion of left or right femoropopliteal thrombi not associatedwith compression. Separate analysis of popliteal, femoralvein, and common femoral vein recanalization showed thatthe only occluded segments observed at 12 months werefemoral vein occlusions that were well collateralized byeither the deep femoral vein (n � 2) or a patent duplicatedsecond branch of the femoral vein that was visible at diag-nosis (n � 1).
Interobserver variability between the unblinded andblinded interpretations by reviewers A and B for patent,partially occluded, and occluded segments was 0.84(weighted � statistic).
w-up divided according to the presence of compressionartery (RCIA/LCIV compression). Recanalization ofLCIV compression was high at both 6 and 12 months,
pression remained occluded. Failure of femoropoplitealn at 6 weeks may have been related to more extensiveiliac veins. Fempop, femoropopliteal; NS, nonsignificant.
folloiliac
CIA/comessioacent

JOURNAL OF VASCULAR SURGERYOctober 2004616 Fraser et al
DISCUSSIONIliac vein recanalization was poorer than femoropop-
liteal vein recanalization. This was due to completefailure of recanalization of the left common iliac vein in
Fig 3. Patency of popliteal, superficial femoral, commoaccording to the presence of compression of the left comcompression). Follow-up was at 6 weeks, 26 weeks (6 moassociated with RCIA/LCIV compression was compareassociated with RCIA/LCIV compression. Recanalizatiexcept left common iliac veins associated with RCIA/LC
Recanalization at 6 weeks, 6 months, and 1 year of individthrombus at baseline, according to presence of compressioiliac vein*
6 Weeks
Patentpartly
occluded O
Left or right DVT, no compressionPopliteal 13 1Femoral 11 1Common femoral 5 1External iliac 3Common iliac 1 1
Left DVT with RCIA/LCIV compressionPoplitealFemoralCommon femoral 1External iliac 1Common iliac
DVT, Deep venous thrombosis; RCIA/LCIV, right common iliac artery co*Once full recanalization occurred, repeat imaging was not performed anperformed in 1 patient with occluded femoral and popliteal veins and 1 patiwas not performed in 1 patient with occluded common iliac and femoral ve
cases associated with RCIA/LCIV compression. Recan-alization rates at 6 and 12 months were high for all otheriliac and femoropopliteal segments. This study thereforesuggests that poor iliac vein recanalization is due to
oral, external iliac, and common iliac segments dividediliac vein by the right common iliac artery (RCIA/LCIV, and 52 weeks (1 year). Patency of left venous segmentsh recanalization of right and left venous segments nottes were high at 6 months and 1 year for all segmentsompression.
moropopliteal and iliac segments, with occlusiveright common iliac artery by left common
6 Months 1 Year
ed PatentPartly
occluded Occluded Patentpartly
occluded Occluded
21 2016 5 17 3
9 1 95 1 52 1 1 3
1 12 24 1 4 14 1 4 1
6 6
sed by left common iliac vein.tinued patency was assumed. Follow-up at 6 months and 1 year was notth partially occluded femoral popliteal veins at 6 weeks. Follow-up at 1 yeard partially occluded external iliac and common femoral veins at 6 months.
n femmonnths)d witon raIV c
ual fen of
cclud
910
432
23446
mpresd conent wiins an

JOURNAL OF VASCULAR SURGERYVolume 40, Number 4 Fraser et al 617
RCIA/LCIV compression, as proposed by Cockett etal.13
Despite the small study size, a strong association be-tween RCIA/LCIV compression and persistent occlusionof the left common iliac vein was found. Patency of the iliacveins has been difficult to study noninvasively with conven-tional techniques, and thus has not been extensively stud-ied. The multiplanar capabilities of MRI make it ideallysuited for visualization of the pelvic veins, and severalauthors have considered it the standard noninvasive test forthis indication.20 Furthermore, the VESPA MRV tech-nique is an improvement on time-of-flight techniques incurrent use, which suffer from long imaging times and flowartifacts at the origin of the inferior vena cava and commoniliac veins.21,22 In a recent study of 55 patients, femoral andiliac vein thromboses were detected with VESPA MRV,with sensitivity and specificity of 97% to 100% and � valuesfor interobserver variability of 0.85 and 0.97, respective-ly.18 Contrast-enhanced MRV has also shown excellentagreement with conventional venography and computedtomography (CT) venography in the setting of venousanomalies and chronic thrombosis.23-25 Intravascular ultra-sound is the most accurate test for assessment of iliac veinanatomy, and shows that single-plane femoral venographymay significantly underestimate the severity of eccentricstenoses.26 MRV lacks the resolution of these invasivetechniques, but enables cross-sectional areas of stenoses tobe measured directly.
MRDTI used in the baseline study directly imagesthrombus as high signal, and thus differs from conventionalCT and MRI techniques that visualize flowing blood, withthrombus detected as filling defects. This sequence is there-fore uniquely able to visualize the structure of thrombosedvenous segments in 3 dimensions and at high resolution.This enabled RCIA/LCIV compression in the baselinestudy to be detected in patients with thrombosed iliacveins. In a study of 101 patients with acute thrombosisMRDTI detected femoral and iliac thrombosis with sensi-tivity and specificity of 97% to 100% and � values forinterobserver variability of 0.96 and 0.98, respectively;accuracy was also maintained below knee.19
To our knowledge, this is the first prospective study touse MRV to assess iliac vein recanalization and to relaterecanalization to the presence of RCIA/LCIV compres-sion. Although patients with ileofemoral DVT and femo-ropopliteal DVT were consecutively recruited, there wereno patients with right iliac thrombosis. This was relatedboth to the small study size and the left-sided predomi-nance of iliofemoral DVT in the population studied. Left-sided predominance of ileofemoral DVT has been reportedin several other series.13,16
Cockett and colleagues12,13 described poor recanaliza-tion of the iliac veins in association with RCIA/LCIVcompression in patients with severe post-phlebitic diseaseand a history of ileofemoral DVT. They examined thesepatients with iliac phlebography, and concluded thatRCIA/LCIV compression was not only the cause of theiliac thrombosis but also prevented its recanalization. These
findings have been difficult to reproduce with noninvasivetechniques, and have therefore remained unconfirmed.However, defects attributed to RCIA/LCIV compressionare detected in as many as 60% of cases of ileofemoral DVTafter thrombectomy and catheter-directed thrombolysis,and are successfully treated with angioplasty and stent-ing.10,14-17 After such treatment high patency rates areachieved, which persist up to 5 years after presentation.10,17
Endothelial lesions in the left common iliac vein associatedwith RCIA/LCIV, such as intraluminal webs andspurs13,27, were not clearly evident in the baseline study,but may have contributed to the reduction of luminal arearecorded.
The definition of partial occlusion was greater than 70%reduction of the luminal cross-sectional area in the absenceof occlusion. This definition was chosen because we haveobserved that MRV with the VESPA technique may showapparent minor stenoses due to underfilling of vessels withcontrast material when the patient is supine (Fig 4). Occlu-sion was defined as complete absence of visible lumen. Theinterobserver variability for patent, partially occluded, andoccluded venous segments with these definitions was satis-factory. The level at which venous stenoses are functionallysignificant is incompletely understood, and functional test-ing was not performed.28 However, studies have shownsignificant clinical improvement if iliac stenoses greaterthan 50% are treated with stenting, and some authors haveconsidered that stenoses greater than 30% may be signifi-cant.29,30 This study may therefore have underestimatedthe proportion of patients with significant venous obstruc-tion in the absence of occlusion.
The functional significance of iliac vein occlusion interms of the venous function of the leg was also not assessedin this study. Iliac vein occlusion is frequently well collat-eralized, and is not likely to cause significant venous hyper-tension in the absence of valvular reflux. However, incombination with valvular reflux venous obstruction signif-icantly exacerbates venous hypertension and post-phlebiticcomplications, and the importance of iliocaval chronic ve-nous obstruction is being increasingly recognized.2-4,29
Furthermore, interventional treatment for ileofemoralDVT with catheter-directed thrombolysis and angioplastywith stenting maintains long-term iliac vein patency andreduces post-phlebitic symptoms, compared with anticoag-ulation therapy alone.10 It remains therefore to be testedwhether interventional treatment has greater benefit inpatients with left ileofemoral DVT associated with RCIA/LCIV compression, in whom this study suggests low spon-taneous patency rates can be expected. Conversely, inter-ventional treatment may be less beneficial in patients withileofemoral DVT not associated with RCIA/LCIV com-pression, in whom high spontaneous patency rates wouldbe expected.
The study protocol had several limitations. First, theprotocol assumed continued patency of the femoropopli-teal and iliac segments once full patency had been achieved,and further MRV scans were not performed. This protocoltended to overestimate the patency at 6 months and 1 year

the ab
JOURNAL OF VASCULAR SURGERYOctober 2004618 Fraser et al
when patients with previous occlusion dropped out. How-ever, the dropout rate was low, and did not significantlyaffect the conclusions of this study. Second, recanalizationof femoral and iliac segments was assessed individually, andaccount was not taken of either the extent of thrombosiswithin each segment or the occurrence of thrombosis inadjacent segments. Adjacent occlusive iliac vein thrombosisand extensive thrombosis at presentation in 6 of 7 patientswith femoropopliteal thrombosis associated with RCIA/LCIV compression may have caused the poor femoropop-liteal vein recanalization observed in these patients at 6weeks (Fig 2). However, at 6 and 12 months these effectsare unlikely to have been significant, because recanalizationof all segments, except left iliac segments associated withRCIA/LCIV compression, was high, irrespective of theextent of thrombosis within that segment or the occurrenceof adjacent occlusion. Furthermore, at 1 year the onlysegments that remained occluded were LCIVs associatedwith RCIA/LCIV compression and femoral segments thatwere well- collateralized. Follow-up was terminated at 1year, and it is possible that further recanalization occurredsubsequently. However, prospective studies with follow-up
Fig 4. a, Magnetic resonance venogram at diagnosis shiliac veins into the inferior vena cava (arrows) in a patientthe right common iliac artery. b, After 1 year, recanalizMagnetic resonance venogram at diagnosis shows dispara(solid arrow) in a patient with compression of the LCrecanalization of the femoral segments has occurred (opeIncomplete filling of the right common femoral vein in
to 5 years after DVT have shown only minor changes in iliacvein recanalization from 6 months to 5 years.8
In conclusion, this study showed that persistent occlu-sion of the LCIV occurred in cases of left ileofemoral DVTassociated with RCIA/LCIV compression. All other iliacand femoropopliteal segments became recanalized in a highproportion of cases. Persistent iliac vein occlusion in theformer patients could have an important influence on thedevelopment of subsequent post-phlebitic disease andtherefore the potential benefit of acute interventional treat-ment.
REFERENCES
1. Shull KC, Nicolaides AN, Fernandes e Fernandes J, Miles C, Horner J,Needham T, et al. Significance of popliteal reflux in relation to ambu-latory venous pressure and ulceration. Arch Surg 1979;114:1304-6.
2. Franzeck UK, Schalch I, Bollinger A. On the relationship betweenchanges in the deep veins evaluated by duplex sonography and thepostthrombotic syndrome 12 years after deep vein thrombosis. ThrombHaemost 1997;77:1109-12.
3. Raju S, Fredericks RK. Late hemodynamic sequelae of deep venousthrombosis. J Vasc Surg 1986;4:73-9.
4. Johnson BF, Manzo RA, Bergelin RO, Strandness DE Jr. Relationshipbetween changes in the deep venous system and the development of the
leofemoral thrombosis extending from left femoral andut compression of the left common iliac vein (LCIV) byof all thrombosed segments has occurred (arrows). c,
ombosis in the left femoral veins (open arrows) and LCIVy the right common iliac artery. d, After 1 year, fullows), whereas the LCIV remains occluded (solid arrow).sence of thrombosis is also seen (double arrow).
ows iwithoationte thrIV b
n arr

JOURNAL OF VASCULAR SURGERYVolume 40, Number 4 Fraser et al 619
postthrombotic syndrome after an acute episode of lower limb deep veinthrombosis: a one- to six-year follow-up. J Vasc Surg 1995;21:307-12;discussion 313.
5. Saarinen J, Kallio T, Lehto M, Hiltunen S, Sisto T. The occurrence ofthe post-thrombotic changes after an acute deep venous thrombosis: aprospective two-year follow-up study. J Cardiovasc Surg (Torino)2000;41:441-6.
6. van Haarst EP, Liasis N, van Ramshorst B, Moll FL. The developmentof valvular incompetence after deep vein thrombosis: a 7 year follow-upstudy with duplex scanning. Eur J Vasc Endovasc Surg 1996;12:295-9.
7. Meissner MH, Manzo RA, Bergelin RO, Markel A, Strandness DE Jr.Deep venous insufficiency: the relationship between lysis and subse-quent reflux. J Vasc Surg 1993;18:596-605; discussion 606-8.
8. Akesson H, Brudin L, Dahlstrom JA, Eklof B, Ohlin P, Plate G. Venousfunction assessed during a 5 year period after acute ilio-femoral venousthrombosis treated with anticoagulation. Eur J Vasc Surg 1990;4:43-8.
9. Plate G, Akesson H, Einarsson E, Ohlin P, Eklof B. Long-term results ofvenous thrombectomy combined with a temporary arterio-venous fis-tula. Eur J Vasc Surg 1990;4:483-9.
10. AbuRahma AF, Perkins SE, Wulu JT, Ng HK. Iliofemoral deep veinthrombosis: conventional therapy versus lysis and percutaneous trans-luminal angioplasty and stenting. Ann Surg 2001;233:752-60.
11. Plate G, Einarsson E, Ohlin P, Jensen R, Qvarfordt P, Eklof B. Throm-bectomy with temporary arteriovenous fistula: the treatment of choicein acute iliofemoral venous thrombosis. J Vasc Surg 1984;1:867-76.
12. Cockett FB, Thomas ML. The iliac compression syndrome. Br J Surg1965;52:816-21.
13. Cockett FB, Thomas ML, Negus D. Iliac vein compression: its relationto iliofemoral thrombosis and the post-thrombotic syndrome. Br Med J1967;2:14-9.
14. Juhan CM, Alimi YS, Barthelemy PJ, Fabre DF, Riviere CS. Late resultsof iliofemoral venous thrombectomy. J Vasc Surg 1997;25:417-22.
15. Semba CP, Dake MD. Iliofemoral deep venous thrombosis: aggressivetherapy with catheter-directed thrombolysis. Radiology 1994;191:487-94.
16. Mewissen MW, Seabrook GR, Meissner MH, Cynamon J, LabropoulosN, Haughton SH. Catheter-directed thrombolysis for lower extremitydeep venous thrombosis: report of a national multicenter registry.Radiology 1999;211:39-49.
17. Mickley V, Schwagierek R, Rilinger N, Gorich J, Sunder-Plassmann L.Left iliac venous thrombosis caused by venous spur: treatment withthrombectomy and stent implantation. J Vasc Surg 1998;28:492-7.
18. Fraser DG, Moody AR, Davidson IR, Martel AL, Morgan PS. Deepvenous thrombosis: diagnosis by using venous enhanced subtractedpeak arterial MR venography versus conventional venography. Radiol-ogy 2003;226:812-20.
19. Fraser DG, Moody AR, Morgan PS, Martel AL, Davidson I. Diagnosisof lower-limb deep venous thrombosis: a prospective blinded study ofmagnetic resonance direct thrombus imaging. Ann Intern Med 2002;136:89-98.
20. Spritzer CE, Arata MA, Freed KS. Isolated pelvic deep venous throm-bosis: relative frequency as detected with MR imaging. Radiology2001;219:521-5.
21. Dupas B, el Kouri D, Curtet C, Peltier P, de Faucal P, Planchon B, et al.Angiomagnetic resonance imaging of iliofemorocaval venous thrombo-sis. Lancet 1995;346:17-9.
22. Montgomery KD, Potter HG, Helfet DL. Magnetic resonance venog-raphy to evaluate the deep venous system of the pelvis in patients whohave an acetabular fracture. J Bone Joint Surg Am 1995;77:1639-49.
23. Thornton MJ, Ryan R, Varghese JC, Farrell MA, Lucey B, Lee MJ. Athree-dimensional gadolinium-enhanced MR venography techniquefor imaging central veins. AJR Am J Roentgenol 1999;173:999-1003.
24. Ruehm SG, Wiesner W, Debatin JF. Pelvic and lower extremity veins:contrast-enhanced three-dimensional MR venography with a dedicatedvascular coil-initial experience. Radiology 2000;215:421-7.
25. Shinde TS, Lee VS, Rofsky NM, Krinsky GA, Weinreb JC. Three-dimensional gadolinium-enhanced MR venographic evaluation of pa-tency of central veins in the thorax: initial experience. Radiology 1999;213:555-60.
26. Neglen P, Raju S. Intravascular ultrasound scan evaluation of theobstructed vein. J Vasc Surg 2002;35:694-700.
27. Negus D, Fletcher EW, Cockett FB, Thomas ML. Compression andband formation at the mouth of the left common iliac vein. Br J Surg1968;55:369-74.
28. Comerota AJ. Myths, mystique, and misconceptions of venous disease.J Vasc Surg 2001;34:765-73.
29. Neglen P, Raju S. Balloon dilation and stenting of chronic iliac veinobstruction: technical aspects and early clinical outcome. J EndovascTher 2000;7:79-91.
30. Neglen P, Berry MA, Raju S. Endovascular surgery in the treatment ofchronic primary and post-thrombotic iliac vein obstruction. Eur J VascEndovasc Surg 2000;20:560-71.
Submitted Apr 6, 2004; accepted May 30, 2004.Available online Jul 8, 2004.
BOUND VOLUMES AVAILABLE TO SUBSCRIBERS
Bound volumes of the Journal of Vascular Surgery for 2003 are available to subscribers only. They maybe purchased from the publisher at a cost of $119 for domestic, $147.66 for Canadian, and $138 forinternational subscribers for Vol 37 (January to June) and Vol 38 (July to December). Price includesshipping charges. Each bound volume contains subject and author indexes. The binding is durablebuckram with the journal name, volume number, and year stamped in gold on the spine. Payment mustaccompany all orders. Contact Mosby, Subscription Customer Service, 6277 Sea Harbor Dr, Orlando, FL32887; phone 800-654-2452 or 407-345-4000.
Subscriptions must be in force to qualify. Bound volumes are not available in place of a regular Journalsubscription.