Embed Size (px)
Citation preview

FY 2017IN-HOME SUPPORTIVE SERVICES
A N N U A L R E P O R T
S O C I A L S E R V I C E S A G E N C Y DEPARTMENT OF AGING AND ADULT SERVICES

IHSS Annual Report 2017 Page 1
IN-HOME SUPPORTIVE SERVICES (IHSS) ANNUAL REPORT
Presented to the Children, Seniors and Families Committee
Board of Supervisors, Santa Clara County
October 11, 2017
Introduction
The Children, Seniors, and Families Committee last reviewed the IHSS Annual Report in
October 2016. This report will update the Committee as to the status of current
administrative and service issues specific to the IHSS program and the IHSS Public
Authority.
IHSS Program Overview
The IHSS program provides in-home care for persons who cannot safely remain in their
own homes without such assistance. Created in 1973, the core goal of the IHSS program
remains the prevention of premature or unnecessary placement of recipients in
institutions (skilled nursing facilities, community care facilities, or hospitals). IHSS is an
entitlement program and all clients found to be eligible and at risk of out-of-home
placement are accepted. To be eligible, recipients must be assessed and found to be
aged (65 years of age or older), blind or disabled (as determined by the Social Security
Administration) and are unable to remain safely in their own home without assistance.
Recipients must also meet specific income requirements consistent with eligibility for
Medi-Cal. Services offered include: domestic and related tasks such as laundry,
shopping, meal preparation, and light housecleaning; personal care services such as
assistance with feeding, bathing, and ambulating; transportation to and from medical
appointments; and certain paramedical services ordered by a physician. County Social
Workers perform an assessment to determine the number of hours and type of services
to authorize an IHSS recipient. The recipient is responsible for hiring, training,
supervising, and firing a provider. Based on the submittal of timesheets, the IHSS
providers are paid with a combination of state, federal and county funds.
IHSS is a state mandated and regulated program that is operated at the County level in
accordance with the California Welfare and Institutions Code. Both federal and state laws
serve, effectively, to make IHSS an entitlement program. Interested individuals have a
right to apply for IHSS services and are guaranteed services if they meet the financial and
functional eligibility criteria. Consistent with all public entitlement programs, IHSS provides
IHSS Annual Report 2017 Page 2
applicants certain rights—timely decision of eligibility, timely notice of change in eligibility
or service, and an appeals process to dispute eligibility decisions.
The California State Department of Social Services (CDSS) and the counties share
administrative responsibilities for the IHSS program. CDSS oversees the IHSS data and
payroll system known as the Case Management and Information and Payroll
System II (CMIPS II), serves as the payroll agent for the IHSS providers, and writes the
IHSS regulations. Counties are responsible for the day-to-day administration of the IHSS
program. County staff also determines recipients’ program eligibility and the number of
hours and type of services each recipient needs.
Components of IHSS
IHSS Program Funding
IHSS services are provided under four programs: Personal Care Services Program
(PCSP), Federal Plus Waiver Program (converted to State Plus Option in 2009), Residual
Program, and Community First Choice Options (CFCO).
Eligibility
To be eligible for IHSS, a person must be aged, blind or disabled and usually have
monthly income at or below $1005.00 per month for individuals. Those individuals with
income in excess of this grant level may still be eligible for IHSS with a share of cost
(SOC). An IHSS recipient with a SOC must make an out-of-pocket monthly payment
towards the receipt of IHSS services before the IHSS program pays the remainder of the
cost of their services. Eligibility for Medi-Cal is generally limited to individuals with no
more than $2,000 in assets and couples with no more than $3,000 in assets (with certain
exclusions for such assets as homes and vehicles).
Application and Social Worker Assessment
When a prospective IHSS recipient applies for the program, the determination of their
eligibility is a two-step process that takes into account both their income and need for
services. Once verified that an individual is financially eligible for IHSS, a Social Worker
visits the home of the recipient to determine whether there is a need for services. To
perform this assessment, the social worker uses a uniform assessment tool to
determine the number of hours for each type of IHSS service for which a recipient
qualifies in order to remain safely in his/her own home. The uniform assessment tool,
known as the Hourly Task Guidelines (HTGs) assists the Social Worker in ranking the
recipient’s impairment level on a five-point scale known as the Functional Index (FI)
ranking. Figure 1 shows each of the potential FI rankings that may be assessed by a
Social Worker, and what they mean for the impairment level of the recipient.

IHSS Annual Report 2017 Page 3
Figure 1:
Functional
Index
Impairment Implications
1 Able to perform function without human assistance-independent.
2 Able to perform a function, but needs verbal assistance
(reminding, encouraging).
3 Able to perform a function with some human, physical
assistance.
4 Able to perform a function with substantial human assistance.
5 Cannot perform the function with or without human assistance.
Each FI ranking corresponds to an established range of service hours for a particular
task. For example a recipient who receives an FI ranking of 2 on the “feeding” task may
be authorized to receive between 0.7 hours and 2.3 hours of feeding per week. The
corresponding range of hours varies depending on the particular task being assessed.
For example, meal preparation services range from three to seven hours. Also if an
individual is assessed as having an FI ranking of 1 for any given task, he/she will not
receive any authorized hours for that task. The weighted average of the FI rankings for
each task is used to create a total FI score. Although the HTGs provide a standard tool,
the assessment process is individualized. Social Workers may, with written justification,
authorize hours above or below the range established by the HTGs.
Assignment of Hours
Once a Social Worker has determined the number of hours to authorize for a recipient,
the recipient is notified of the number of hours they have been authorized for each task.
Using the HTGs, Social Workers may authorize between 1 and 283 total hours per month
of IHSS services. Recipients who receive over 195 hours of service each month are
considered to be severely impaired. Once it has been determined that a recipient meets
the eligibility criteria for IHSS, that individual is granted those IHSS services. As a result,
there is no waiting list or cap on program enrollment.

IHSS Annual Report 2017 Page 4
Federal and State Legislation Affecting IHSS
Provider Overtime
In February 2016, the state implemented the new federal labor regulations for IHSS
providers following a one-year delay due to federal court action. The federal regulations
required all IHSS programs to (1) pay overtime compensation—at one-and-a-half times
the regular rate of pay—to IHSS providers for all hours worked that exceed 40 hours in a
week; and (2) compensate IHSS providers for time spent waiting during medical
appointments and traveling between the homes of IHSS recipients.
In response to the new program responsibilities, Santa Clara County’s IHSS program
formed the Fair Labor Standards Act (FLSA) Unit in 2016. The FLSA Unit is responsible
for:
1. Implementing and enforcing the workweek, overtime, and travel time requirements;
2. On-going outreach, education, support, guidance, and planning to recipients and
providers regarding FLSA;
3. Reviewing violations that exceed the overtime and travel time limits and counsel
recipients and providers to prevent any further occurrences;
4. Issuing notices to both providers and recipients inform them of any violations and
the penalties (if any) related that violation;
5. Exploring and compiling information related to Exemptions 1 and 2;
6. Assisting recipients and providers-via a telephone hotline or lobby visits-to ensure
mutual understanding regarding responsibilities and the limits related to FLSA; and
7. Having the capability to enter information into the CMIPS II system.
With the goal of being accessible to the IHSS community, on May 2, 2016, IHSS went
Live with the FLSA Hotline to singularly address issues and concerns related to overtime
and travel time. Since its inception, the hotline has continued to average over 100 calls
per week. Topics can include but are not limited to: violations, timecard errors, weekly
hour calculations, flexible hour requests, travel times, forms, and non FLSA related
questions. As a direct result of the FLSA Hotline (with the occasional lobby visit), the
Santa Clara County’s IHSS program is anecdotally experiencing a high number of
providers who have not incurred an additional violation in the past year; these providers’
violation level have all been reduced to zero.

IHSS Annual Report 2017 Page 5
From July 1, 2016 to August, 31, 2017, IHSS has reviewed and counselled providers on
3048 instances of violations. Of that total, IHSS has upheld 1352 violations. At least
1696 violations were overridden and, of that number, 357 were overturned via the
provider dispute process. There were 1610 instances of violation which were
automatically overridden as the provider had qualified for an Exemption. Santa Clara
County has 73 providers who qualify under Exemption 1 and 1 provider under Exemption
2.
As the implementation of FLSA continues to be defined at the state level, Santa Clara
County’s IHSS program’s FLSA Unit will continue to provide timely responses to new
developments while simultaneously continuing its prime directive to serve and support
recipients and individual providers.
Coordinated Care Initiative (CCI) Update
Created through a public process involving stakeholders and health care consumers, the
passage of the Coordinated Care Initiative (CCI) marked an important transition towards
transforming California's Medi-Cal delivery system to better serve the state's low-income
seniors and persons with disabilities. The Coordinated Care Initiative (CCI) allowed
persons eligible for both Medicare and Medi-Cal (termed Dual Eligibles) to receive
medical, behavioral health, long term services and supports, and home and community
based services coordinated through a single health plan. CCI also included mandatory
enrollment for most other Dual Eligibles into Medi-Cal managed care and integrated Medi-
Cal long term services and supports (MLTSS), including In-Home Supportive Services
(IHSS), into managed care. As part of CCI, the state assumed bargaining responsibilities
for IHSS. CCI also established a new Maintenance Of Effort (MOE) requirement in place
of the traditional county share of cost for IHSS programs in all counties. This pilot was
implemented through a federal demonstration project and currently operates in seven
counties—Los Angeles, Orange, Riverside, San Bernardino, San Diego, San Mateo, and
Santa Clara. As one of the pilot counties, Santa Clara County’s IHSS program created a
dedicated CCI Unit to execute the mandates of the pilot project.
Under current state law, the CCI pilot project has been determined to be not cost effective
and funding for CCI will cease on January 1, 2018. The termination of the CCI will have
the following impact on the Santa Clara County’s IHSS program:
● Removal of IHSS from Cal MediConnect (CMC) and Medi-Cal funded Long-Term
Services and Supports (MLTSS)
● Removal of IHSS benefits from Medi-Cal managed care plan capitation rates

IHSS Annual Report 2017 Page 6
● Elimination of Statewide Authority responsible for negotiating IHSS providers’
wages and benefits in the seven CCI counties
Of note, the most significant impact is the elimination of the MOE under the CCI pilot
project. The repeal of the CCI MOE would mean that an additional $592.2 million in
funding cost will be shifted from the State to Counties. To mitigate the financial hardship
and cash-flow problems, Senate Bill 90 was passed and the bill instituted a new MOE
funding model that modifies the cost sharing arrangements between the State and
Counties.
SB 90 establishes a new statewide county IHSS MOE base at $1.769 billion and
appropriates $400 million General Fund (GF) in FY18; $330 million GF in FY19; $200
million GF in FY20; and $150 million GF in FY21 and annually thereafter to offset the
additional IHSS costs being shifted to counties. At the time of this report, Santa Clara
County’s Interim MOE requirement stands at $74.6 million.
There will be no inflator to the MOE requirement in FY18 and in FY19, the County IHSS
MOE base will be adjusted by 5%. In FY20 and, annually thereafter, the base will be
adjusted by 7%.
In FY20, a “re-opener” will be conducted with the California Department of Finance
(DOF), California State Association of Counties (CSAC), and stakeholders to re-examine
how the provisions of SB 90 will impact the IHSS programs and the 1991 Realignment
funding structure.
Based upon lessons learned, certain elements of CCI have shown the potential to reduce
the cost of health care for affected individuals and improve health outcome. Thus, the
following components will be funded through December 31, 2019:
● The Cal MediConnect (CMC) program will be extended
● Mandatory enrollment of Dual Eligibles into managed care will be continued
● Integration of MLTSS (except IHSS) into managed care will be continued
During the tenure of the pilot project, Santa Clara County’s IHSS program’s CCI Unit has
worked in tandem with our County’s designated managed health care plans (Anthem Blue
Cross and Santa Clara Family Health Plan) to achieve the stated goals of CCI. As
conveyed by both health plans, this affiliation enabled significant reductions in turn-
around time for the most at risk IHSS applicants and diverted calls that would have
otherwise gone through the main IHSS telephone line. This was achieved through the
timely processing and screening of new referrals and reassessment requests from the
health plans, participating in Interdisciplinary Care Team (ICT) meetings, telephone

IHSS Annual Report 2017 Page 7
screenings, conducting assessments on expedited applications and reassessments on
high touch cases, engaging in follow up care as needed, and frequent communication
between all entities.
In FY17, the CCI Unit received 1021 inquiries from the health plans (e.g., new IHSS
referrals, ICT requests, general information, etc.). Of that number, 127 were for
reassessments and 82 resulted in a change of authorized hours. The CCI Unit received
approximately 25 new expedited referrals each month that were initiated by either the
health plans or through IHSS’ Application Readiness Unit. These referrals were
assessed by the CCI unit within 15 calendar days and hospice referrals were seen-on an
average of-15 calendar days. The CCI Unit completed 170 requests for additional
assistance on behalf of recipients enrolled in either Anthem Blue Cross or Santa Clara
Family Health Plan.
Figure 2
Fiscal Year 2015-2016 Coordinated Care Initiative Data
Total
Inquiries from Health Plans
(new referrals, ICTs, general info,
etc.)
1021
Reassessment requests 127
Reassessment requests resulting in
change of authorizations
82
Requests for Health Plan assistance
from IHSS
170
Expedited Referrals by Health Plans
from the Application Readiness Unit
Assessed in 15 calendar days
Hospice Referrals Assessed in 15 calendar days

IHSS Annual Report 2017 Page 8
In addition to the work that was performed under the auspices of CCI, the CCI Unit also
assumes other duties within IHSS:
● The CCI Unit has been utilized as the de facto unit to partner with many community
based organizations desiring a more direct relationship with IHSS. In the past year,
the CCI Unit has worked closely with the following agencies to affect the best
outcome for mutually served recipients: Institute On Aging-Community Living
Connection (CLC); Santa Clara County’s Office of Supportive Housing’s Care
Coordination and Transitions Program (CCTP); Santa Clara County’s Health and
Hospital System’s Valley Specialty Center’s Public Hospital Redesign & Incentives
in Medi-Cal (PRIME); and Valley Medical Center’s Social Work staff.
● The CCI Unit provided guidance to Medi-Cal recipients as whether it would be more
beneficial to obtain cash aid [Supplemental Security Income (SSI)] or in-kind
benefits [IHSS] via the completion of the Authorization for Non-Medical Out of
Home Care (Board and Care) form (SSP 22).
● Lastly, the CCI Unit maintained a half caseload of continuing IHSS cases in order to
assist with the IHSS reassessment compliance rate.
While the CCI pilot project may have fallen shy of full implementation, it is incontrovertibly
that the Santa Clara County’s IHSS program demonstrated how effective collaboration
and coordination with internal and external stakeholders can ensure the delivery of vital
services and support to our most vulnerable community members. The end result was
that individuals who enrolled in CCI expressed an increased satisfaction with their health
care services over time. The Santa Clara County’s IHSS program has been proud to
have been a participant in the CCI pilot project as it truly laid the groundwork to deliver
the right care, at the right place, and at the right time.
Santa Clara County’s IHSS Program
Housed within the Social Services Agency, IHSS is one of five programs along with Adult
Protective Services, Senior Nutrition, Office of the Public Administrator/ Guardian/
Conservator and Seniors’ Agenda that together comprise the Department of Aging and
Adult Services.
Currently, the IHSS program employs 155.5 full time equivalent positions and is staffed as
follows: Managers: 6; Quality Assurance: 6; Social Work Supervisors: 9; Case
Management Social Workers: 77; Fair Labor Standards Act/Coordinated Care Initiative:
11; Application Readiness: 10; Payroll/Data Specialists: 17; and Clerical support: 19.5.

IHSS Annual Report 2017 Page 9
Also as part of the MOE, IHSS augmented its staff by 10 full time equivalent positions
through the FY17 budget. IHSS received approval to hire 1 Social Services Program
Manager I/II, 6 Social Worker I/II’s, 2 Office Specialists II’s, and 1 Administrative
Assistant. We were successful in hiring all of these positions. For the Social Worker
recruitment, efforts were made to best reflect the IHSS recipient population regarding
language and ethnicity.
As of this writing, the number of IHSS recipients in Santa Clara County is approximately
23,592. The county’s IHSS population reflects the community’s cultural and ethnic
diversity. Attachment 1 provides an overview of the county’s IHSS recipient population by
city. Since the last report to CSFC the county’s IHSS caseload has increased by 6.4%.
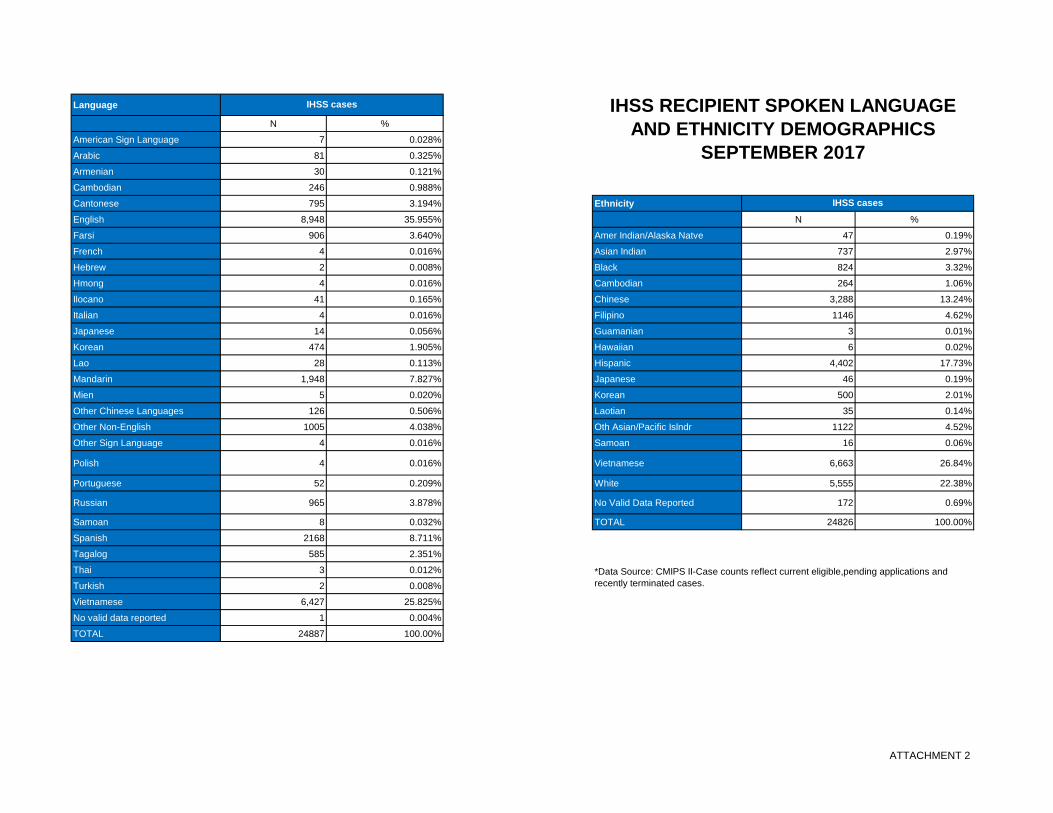
Attachment 2 provides an overview of the county’s IHSS recipient population by the
spoken language/ethnicity breakdown of the recipient population.
Effective May 1, 2013 Santa Clara County launched the CMIPS II database application
that significantly changed the daily administration of the program. CMIPS II, a much
anticipated update of the legacy CMIPS system that had been utilized throughout the
State for the past 25 years, rolled out successfully after several years of intense work at
the State, vendor and local level. Due to significant changes (both legislative and
regulatory) as well as caseload and management needs, CMIPS II provides an enhanced,
efficient and user-friendly system to support the IHSS program. Several features of the
new system include: real-time data updates, on demand printing reports, pre-populated
State mandated IHSS forms, and less reliance on codes and commands in plain
language. Additionally, CMIPS II supports staff by automatically applying hourly task
guidelines, automatic calculation of IHSS authorized hours, on-line case notes, and on-
line review and approval by supervisory staff. Most significantly, the IHSS provider
payroll (which had historically been processed by county staff) is now processed by
CMIPS II via a central processing facility in Chico. County staff still handle exception
timesheets and provide error resolution as needed, however, payroll processing is
handled much more efficiently due to this changeover resulting in a significant decrease
in complaints regarding payroll processing.
Also of note is the negotiated change in the case carrying model of IHSS cases. As
CMIPS II requires that every IHSS case be assigned to a “case owner” the previous
model which incorporated a “banked” caseload was eliminated prior to the CMIPS II
launch. All 77 social work staff now shares an equitable distribution of the IHSS
caseload as well as receive an equitable distribution of the monthly intake applications
received to conduct an initial assessment. Caseload size is approximately 327 cases per
Social Worker. Ongoing meetings are scheduled between management and labor to
address efficiencies wherever possible.
IHSS Annual Report 2017 Page 10
With the implementation of the Telework Policy, all Case Management Social Workers
are able to work from home as many as a couple days a week by entering necessary data
into CMIPS II, thus reducing office distractions and increasing work output and
compliance with CDSS.
Remote Access is also another project that IHSS implemented. All Case Management
Social Workers received County issued laptops, Smartphones, hot spots, head sets, and
docking stations. This equipment is now considered mandatory in order for Social
Workers to complete their daily work.
In addition to Telework and Remote Access, IHSS began a project with the agency’s
Information Systems (IS) Division to implement a scanned document system called
Integrated Document Management (IDM), eliminating the need for paper case files. IHSS
implemented IDM in July 2016 and the work plan included scanning all of the active cases
by December 2016 and the closed cases by December 2017. As of the writing of this
report, all of the active cases were scanned by March 2017 and the closed cases are still
being scanned. Having IDM in place has improved the service delivery by providing case
document access to staff who are assisting recipients and providers. IHSS is working
with IS to improve IDM by adding a search feature so that documents can be located in
an even shorter amount of time.
IHSS Quality Assurance/Quality Improvement
Training
As part of the continued commitment to Quality Assurance/Quality Improvement, CDSS in
conjunction with the University of San Diego, statewide training is offered in order to
increase consistency in the assessment process used by IHSS Social Workers from all
counties. New staff is required to participate in all three modules of the training program
including: IHSS 101, Comprehensive Assessment Concepts (CAC), and Medical
Implications/Program Integrity/State Hearings. The module series are now offered in the
Central Region quarterly.
Santa Clara County continues to offer a CMIPS II Web-Based Training on SCC Learn
where staff can take advantage of on-line courses. New staff is asked to complete
Module 1 which gives a basic orientation and then they are asked to take relevant
Modules that pertain to their classification and job function.
Santa Clara County continues to offer in-house trainings series to orient staff to local level
policy and procedures. These trainings are coordinated by Staff Development. The
IHSS Annual Report 2017 Page 11
trainings topics are facilitated by Managers, Social Work Supervisors, Lead Social Worker
staff, and Quality Assurance (QA) coordinators. Topics include: IHSS Overview, State
Hearings, QA Roles and Responsibilities, Case Management Tools/Tips, CMIPSII, Medi-
Cal Eligibility and IHSS, Inter-County Transfers, Provider Enrollment and the Public
Authority, Payroll Functions and Timesheets, APS Overview and Mandated Reporting,
Protective Supervision, Proration, Assessing Minor Children, Able and Available Spouse,
Paramedical, and Medical Supplies.
State Monitoring Review
In December 2016, staff from the Quality Assurance Bureau of CDSS, Adult Programs
branch, reviewed 70 of Santa Clara County’s IHSS case files and accompanied county
QA staff on three home visits. Santa Clara County participated in an entrance
interview, hosted the review team, cooperated and supported the review process, and
participated in an exit Interview on the last day with the IHSS Leadership and Quality
Assurance team.
The final monitoring review report dated 1/11/17, confirmed that Santa Clara County was
found to be 100% compliant in the following areas:
1. Request for Order and Consent-Paramedical Services forms (SOC 321s) were in
the case file when required and signed by a Licensed Health Care Professional;
2. When a need for Protective Supervision was identified, there was sufficient
3. documentation for the service, the need was addressed at each reassessment, and
the Assessment of Need for Protective Supervision forms (SOC 821s) were in the
case files or documented as sent;
4. When available, the source and services of the Alternate Resources were
documented.
Reassessment Compliance Rate
Santa Clara County IHSS was commended for sustaining a high reassessment
compliance rate. Fifty-four of the 60 cases reviewed had timely reassessments.
Conducting timely reassessments continues to be a high priority in Santa Clara County,
as evidenced by the CMPIS II data from July 2017, showing that 86% of recipients
received timely reassessments.
Santa Clara QA Reviewed Cases
Twenty-four cases that our Santa Clara County Quality Assurance team reviewed were
also re-reviewed by the CDSS Monitoring team. CDSS revealed that:
1. When County QA staff identified areas to be addressed, regulations were applied
correctly in all 24 cases;

IHSS Annual Report 2017 Page 12
2. In 21 out of 24 cases reviewed, County QA staff identified most inaccuracies and
omissions present at the time of the Desk Review;
3. The remediation process outlined in the County’s QA/QI plan was clear and the
Desk Review Tool included completion timeline and appropriate signatures.
In 23 of 24 cases reviewed, the remediation process was followed;
4. In the seven county QA home visit cases reviewed, all issues identified during the
home visit were addressed appropriately.
Home Visits with County QA Staff
State monitoring staff accompanied count QA staff on three home visits for cases which
were identified as requiring a home visit. The County’s QA staff performed a thorough
assessment and addressed all of the required areas as outlined in ACL 130110.
Best Practices
The CDSS QA team reported that it was demonstrated throughout the monitoring review,
both in documentation and observed interactions that Santa Clara County strives to
provide quality service to clients. As a result of the last monitoring review Santa Clara
County developed several guides, processes and is working on the development of a
Web Application to assist in needs assessment process and to ensure uniformity in
authorization of cases and accurate assessment of needs and hours.
Areas of Concern/Santa Clara’s response
The following areas were identified as areas of concern by the monitoring review team:
1. Paramedical Services
Of the 16 cases reviewed with Paramedical services authorized, six cases had
authorized hours that did not match the hours the licensed health care professional
(LHCP) indicated in the Request for Order and Consent Paramedical Services
Form (SOC 321). If the County determines that the Paramedical tasks take more or
less time than the time indicated on the SOC 321, the county should contact the
LHCP to discuss their concerns. A new form should be obtained (ACL 08-18),
otherwise, the time indicated on the SOC 321 should be authorized.
2. Cases with Unmet Need
In three of the seven cases reviewed with unmet needs, there was no
documentation to verify that either the Social Worker had assessed the availability
of other resources or made referrals to address those unmet needs when
there are resources available (ACL 13-66). As stated in the Assessment
Narrative template, Social Workers are required to document what resources are in
place or referrals provided to attempt to address determined unmet need.

IHSS Annual Report 2017 Page 13
3. Alternative Resources
Although alternative resources were appropriately identified and documented where
applicable, in four of the nine cases reviewed, the hours authorized for purchase
were not reduced to reflect the availability of these resources. Santa Clara County
is aware of the inconsistency of how alternate resources are reflected in these
cases. A future All Staff training will ensure that all staff is completing this correctly.
State QA findings including the identified areas of concerns were shared with all levels of
the program at the April 2017 All Staff meeting. Areas of concerns identified continue to
be discussed at monthly IHSS Leadership Team meetings. This information has also
been incorporated into monthly All Staff training sessions with the Social Worker staff. In
September 2016, the IHSS All Staff meeting/training was primarily focused on
strengthening case documentation and assessment narratives when Social Workers are
assessing recipients. This training covered several identified areas of improvement
including paramedical services, cases with unmet need, and alternate resources.
Santa Clara County’s next CDSS review is scheduled to occur December 5-8, 2017. We
will have 60 cases reviewed and three home visits conducted with the CDSS QA
reviewers.
Quality Assurance Activities and Efforts
Internal Reviews
QA Social Work Coordinators were required to complete 584 desk reviews and 117 home
visits as required by standards set forth by CDSS. The results of these reviews were
given to the Social Work Supervisors who then review the findings with their social work
staff. Corrective actions are completed within 30 days of receipt. When QA staff note
trends, trainings and/or reminder memorandums are created. At monthly All Staff
meetings, we continue to train or retrain on a variety of identified QA training topics.
Currently, IHSS has three IHSS QA Social Work Coordinators. The number of yearly
reviews are assigned by CDSS based on county caseload size. Santa Clara
County is considered a large county and assignments are given based on 3.0 FTE staff.
Targeted Reviews
Pending Case Monitoring
This year’s activity was focused on identifying cases that had been in pending
status and assigned to a Social Worker for assessment more than one month.
Supervisors requested additional support in being able to monitor their staff
caseload based on assessment date.

IHSS Annual Report 2017 Page 14
QA receives a file once a month from Santa Clara County Information Systems (IS)
and is able to run a variety of program reports for follow-up and review. A pending
case report was created to pull each case that has been assigned to a Social
Worker with an outstanding pending status. The first report was generated in
February of 2017 and provided to Social Work Supervisors for review and
feedback. The feedback was received and incorporated in the report, which was
generated monthly for Social Work Supervisors to review and respond. Social
Workers are expected to input their assessment and data within seven business
days of a completed home visit. The timeframe this report is generated is to ensure
that staff have had sufficient time to input their data and have made a determination
in the month it was assigned. The reports were reviewed monthly by the Case
Management Social Service Program Manager II to ensure that the determinations
have been made, or if extenuating circumstances were present and outlined in the
case notes. The reports were reviewed at supervision each month with Social
Work Supervisors. Social Work Supervisors were required to review the report
earlier in the month, follow up with their respective staff and provide updates to their
Manager at supervision.
In the first month that the report was created there were 71 identified cases, by the
second month there were 20 cases identified, which was significantly less. This
report was instrumental in helping Social Work Supervisors manage the timeliness
of assessments and determinations on intake assignments in their units.
This targeted review will continue ongoing. The pending case assignment reports
assists management in holding mid management accountable and Social Workers
accountable for their intake assignments. Timely initial assessments are key in
providing essential services to keep our recipients safely in their home. This
continued oversight will ensure that assessments are taking place in a timely
manner.
Paid Claims
When the Medi-Cal system determines there was a potential out of home expense paid
for during an IHSS eligibility period, a paid claim task is initiated in the CMIPS II
application. The QA Coordinators respond to and investigate potential overpayments.
Confirmation is made directly with the identified facility or through provider confirmation.
During FY17, there were 113 confirmed overpayments as a result of this effort, initiating
overpayment recovery for $85,954.
Fair Hearing Compliance
In the appeals process, Social Workers are responsible for completing their own

IHSS Annual Report 2017 Page 15
responses to administrative law judge decisions. The Quality Assurance Manager
continues to manage the program’s compliance with response times for ordered actions.
Regional Meetings/Leadership Roles
In FY17, Santa Clara’s QA Coordinators continue to co- chair the Central Regional IHSS
QA Meetings, held bi-monthly throughout the Central Region of CA. This meeting
provides an opportunity to collaborate with other Central Regional county partners in the
implementation of QA activities. They will continue to fulfill this role for the remainder of
FY17.
In addition, the monthly CWDA Central Regional meeting provides an opportunity to build
relationships with County partners, various CDSS contacts, and generates ideas to best
improve our local program. In this meeting, Central Regional QA Manager/Social Work
Supervisors gather to discuss new regulations, policy and procedures, and various QA
efforts. Meetings are held in surrounding Central Regional counties throughout California.
Quality Improvement Efforts
Assessment Narrative and Service Evidence Documentation Training
Quality Assurance (QA) Coordinators noticed in their reviews that there were
inconsistencies in Social Worker documentation and suggested implementing a training to
address these concerns. This effort was created to provide an opportunity for a transfer
of learning experience and ongoing reference.
A documentation work group was created and they met for several months to plan,
organize and develop the training material and transfer of learning tool. The training
consisted of two parts, an All Staff meeting and a transfer of learning opportunity to
promote learning in small group settings. The initial training was provided at the IHSS All
Staff meeting in September of 2016, which included an overview of the changes, new
expectations and an introduction of the transfer of learning tool. The transfer of learning
tool provided specific examples of strong and weak documentation for discussion and
understanding. Copies of the transfer of learning tool were provided to each unit. Social
Work Supervisors were encouraged to go over the tool with their staff and QA
Coordinators were available to Social Work Supervisors to help facilitate this transfer of
learning opportunity. QA Coordinators attended most unit meetings to support this
process.
The outcome of this effort was very positive. County QA staff saw an overall
improvement in stronger documentation across the program. During our December 2016
Monitoring Review, the CDSS monitoring review team also acknowledged a significant

IHSS Annual Report 2017 Page 16
improvement in documentation compared to previous years.
Program Integrity
Potential fraud is detected several ways using resources provided by CDSS/CMIPS II.
Reviews of all fraud complaints submitted by Social Workers, county staff, collaterals, and
the community are required by CDSS. In addition to the review of fraud complaints, our
other program integrity efforts include: error rate study reviews, directed mailings,
unannounced home visits to verify services are being received or provided, reviewing all
identified overpayments and underpayments, reviewing the County Vital Statistics Report
for recipients that are deceased, and completing the Death Match Report.
Directed Mailings
The purpose of directed mailings is to reach out to providers associated with cases which
appear to suggest some program integrity concern (whether or not the concern is
founded) and proactively educate those providers concerning common program integrity
mistakes. The goal is to increase the participants’ knowledge and create a better informed
provider of IHSS services in an effort to reduce errors, fraud, and abuse in the IHSS
program. This year our identified category was Protective Supervision authorized cases
not reassessed in more than two years. Twenty-five cases were identified. Mailings were
sent to recipients and their individual providers in this effort.
Unannounced Home Visits
Unannounced home visits (UHVs) were conducted by our Program Integrity Coordinator
to ensure that the services authorized are consistent with the recipient’s needs at a
level which allows him/her to remain safely in his/her home, and to validate the
information in the case file. A UHV monitoring tool is used in efforts to safeguard a
recipient’s well-being by verifying that they are receiving appropriate levels of services
and to ensure program integrity by reminding recipients of program rules and
requirements and the consequences for failure to adhere to them, including the potential
loss of services. This year our indicator was eligible recipients (as of September 30, 2016)
who applied to the program before March 1, 2016 and did not have an assigned provider.
There were 38 assigned unannounced home visits. UHV efforts confirmed that nine
recipients had no identified program integrity concerns and 29 recipient cases were
determined to have substantiated program integrity concerns. Out of the substantiated
cases, 19 were terminated due to recipient’s services authorized beyond need or services
not sufficiently provided and eight were sent to the Social Worker for reassessment or
sent to QA for further action. Both the Social Worker and Social Work Supervisor were
notified to conduct an early reassessment to ensure the recipient received an appropriate
assessment or the QA Coordinators were notified to conduct a case review to ensure the
Social Worker’s assessment followed State regulations and County policies.

IHSS Annual Report 2017 Page 17
Fraud Review and Investigation
For FY17, a total of 355 fraud complaints were received. Five cases were sent to the
Department of Health Care Services Investigations for further investigation and
consideration for prosecution. Most of these cases are still pending prosecution. When
cases are prosecuted, this results in arrests, convictions, and restitutions to IHSS
ordered by the Court. In addition, 178 fraud complaints were reviewed internally by the
Quality Assurance Manager, IHSS Program Integrity Social Work Coordinator I, and the
Quality Assurance/Program Integrity Associate Management Analyst during the fraud
triage process. Presently, the Program Integrity unit triages the reports of suspected
fraud complaints and assigns them to an investigative agency based on amount threshold
and investigator availability. From these review efforts, cases were forwarded for criminal
investigation/prosecution, recipients and providers were educated about how to avoid
common fraud issues, or the cases were sent for identified overpayment processing.
Overpayment Recovery
The IHSS program has a dedicated Senior Account Clerk on staff responsible for
reviewing all terminated IHSS cases and auditing the case for either outstanding
overpayments or underpayments. Additionally, cases involving suspected fraud,
timesheet inactivity, Vital County Statistics, death reviews, paid claims, unannounced
home visits, or death matches are also submitted to the Quality Assurance/Program
Integrity Associate Management Analyst for a review audit. For FY17, $451,811 was
identified and processed for overpayment recovery to the IHSS program.
IHSS Public Authority
The Santa Clara County IHSS Public Authority is managed via contract by Sourcewise,
with a final amended FY17 budget of $2,036,051.
The primary role of the Public Authority is to offer services that assist recipients with
greater access to providers. This has been accomplished by:
1. creating a provider registry;
2. establishing the Public Authority as the employer of record for collective bargaining;
3. maintaining benefits administration for qualified independent providers;
4. providing access to training for consumers and providers of IHSS and;
5. providing enrollment processes for all new providers.

IHSS Annual Report 2017 Page 18
The provider registry is a computerized database listing of screened and qualified IHSS
providers. The Public Authority implemented mandatory criminal background checks for
independent providers prior to becoming eligible to be listed on the registry. As of June
2017, the registry had 549 active providers available to work. These services provide
recipients with a greater level of confidence when hiring providers referred by the registry.
Additionally, the Public Authority administers benefits which include: health, dental, vision
and VTA Eco-Pass Clipper Cards for eligible providers. The ability of the Public Authority
to maintain an adequate number of qualified screened providers on the registry correlates
to the wages and benefits offered in Santa Clara County. The Public Authority also gives
recipients a voice in how IHSS services are provided via the IHSS Public Authority
Advisory Board. The Advisory Board is also a state mandated function of the Public
Authority. It is composed of eleven members of whom at least 50% are individuals who
are current or past users of personal care assistance services. The Advisory Board
studies, reviews, evaluates and makes recommendations to the IHSS Public Authority
Governing Board and Sourcewise staff relative to any matters affecting persons receiving
IHSS.
Public Authority provides access to training for recipients and providers as part of its
mandate. The Public Authority implemented training for providers in partnership with Adult
Education programs in Santa Clara County and now offers classes in five different
locations. Classes are designed to enhance the skill set of providers in providing quality
care for their IHSS recipients maintaining a consumer directed model.
Public Authority Services provides training classes for providers through a curriculum
developed specifically to follow and reinforce the IHSS based recipient directed model of
care. In FY17, Public Authority Services provided training for 1,876 providers and issued
69 certificates of completion to providers who finished all nine Series 1 certificate classes.
In June 2017, Public Authority Services began issuing a Series 2 certificate of completion
to providers who have completed the six most recently incorporated class subjects. The
Series 2 certificates were issued to all 10 providers who have completed those classes to
date. Fewer classes were offered to providers during the FY17 due to a lower number of
registrants and the continued high rate of absence for classes. However, the ratio of
certificates earned by providers increased from 3.6% in FY16 to 4.2% in FY17.
In Fall 2016, Public Authority renamed several classes to better reflect the purposes and
intentions of the subjects, while the content of the classes largely remained the same.
IHSS Annual Report 2017 Page 19
The curriculum offers 15 classes:
Series 1 Certificate classes:
CPR Nutrition
First Aid Personal Care
Understanding Diabetes Safety and Infection Prevention
Last Phase of Life Safe Lifting and Transferring
Mental Health
Series 2 Certificate classes:
Alzheimer’s Basics Caregiver Stress Management
Cancer Care Basics Emergency and Disaster Preparedness
The Skilled Care Provider Falls Prevention
The Public Authority is also mandated to provide access to training for IHSS recipients. A
newly developed training called “Call and Connect” was launched in February 2016 on a
monthly basis. Recipients are pre-registered for the sessions, emailed or mailed class
materials ahead of time and given a call-in number to join the session. Feedback from
recipients who have participated indicates they find them informative and quite valuable.
Session topics provided were:
Finding and Using Community Resources
Understanding and Using the Public Authority Registry
Independent Living and Consumer Rights
Living with Memory Loss
Disaster and Emergency Preparedness
Falls Prevention
Tips for Training a New Care Provider
Understanding Roles: IHSS, Social Workers, Care Providers, and the Public Authority
Tips for Improved Communication
Understanding IHSS Authorized Services
Additional training resources are available on the Public Authority website www.pascc.org
including videos and training modules in multiple languages on the following topics:
• IHSS System Introduction
• Obtaining Your Independent Provider
• Managing Your Independent Provider
• Assessment, Reassessment and the Appeal Process

IHSS Annual Report 2017 Page 20
The Consumer Connection quarterly newsletter was mailed to all IHSS recipients. The
purpose of the newsletter is to inform recipients of important information regarding the
IHSS program and to provide informative articles as additional training tools to better
equip them in their role as employers of IHSS homecare workers. Newsletters and
training materials are also posted on the Public Authority website at www.pascc.org.
The Public Authority implemented Care Coaching July 1, 2015 as part of the Registry
services. Care Coaching provides help for IHSS recipients who require assistance with
the responsibilities of being an employer. Three Care Coordinators are assigned cases as
referrals come in. They help IHSS recipients with scheduling provider interviews, coach
recipients on how to conduct interviews, establish work schedules, set expectations and
problem solve. Establishing relationships with the recipients and providers to help them
when they need it but also to teach them how to do this on their own if they are able. This
program is an essential component of the registry for those who are unable to handle
these responsibilities on their own and do not have a friend or family member to assist
them. Care Coaching received 271 referrals during fiscal year 2017. Referrals primarily
come from APS, IHSS and the two health plans, Anthem Blue Cross and Santa Clara
Family Health Plan. Of the total referrals to the program 10 came from the health plans.
FLSA Overtime
The IHSS program began paying overtime and travel time to providers under the FLSA
regulations beginning with the February 2016 pay periods. Providers working more than
40 hours per week are paid time and a half for all hours over 40. There are a number of
regulations that limit the amount of overtime that a provider may claim and providers may
be issued “violations” if they exceed the allowed limits. Multiple violations can lead to
termination of the provider from the program for up to one year.
Public Authority Services continues to offer training on the topics of overtime and travel
time both in-class and via telephone to providers and recipients. Between July and
December 2016, 13 providers completed classroom training for overtime and travel time.
Due to declining interest for classroom training, overtime and travel time training is now
offered individually via telephone as needed. In person training is available for providers
requiring additional assistance. In FY17, Public Authority Services provided assistance to
109 providers via telephone.
In May 2017, Public Authority Services released a timesheet training video to assist
providers and recipients to better understand how to correctly complete and submit their
timesheets and how to avoid common mistakes that may delay pay or result in an
overtime violation. Between the release date on May 10, 2017 and June 30, 2017, the

IHSS Annual Report 2017 Page 21
video had 3,049 views.
IHSS Provider Enrollment Process
Sourcewise, and IHSS collaborated on developing a local methodology to implement the
four new mandated functions. The Provider Enrollment mandates for counties are:
1. all providers must submit fingerprints and undergo a criminal background check by
the California Department of Justice;
2. providers must attend a provider orientation/watch a video providing rules,
regulations and requirements for being an IHSS provider;
3. providers must sign a provider agreement stating they understand and agree to the
rules of the program and responsibilities of being a provider; and
4. providers must provide a current, original government issued ID and their
original Social Security card to the county or Public Authority to be
electronically scanned.
An additional change to IHSS provider enrollment was enacted pursuant to SB 878 adds
WIC section 12301.24(e) which requires that, no later than April 1, 2015: The provider
orientation shall be an onsite orientation that all prospective providers shall attend in
person. Representatives of the recognized employee organization in the county shall
be permitted to make a presentation of up to thirty minutes at the provider orientation.
The Public Authority developed a one hour IHSS provider orientation session with
an additional thirty minutes at the end for SEIU representatives to present the union to
attendees. The group orientation was added to requirements for individuals to complete
the IHSS enrollment process to become eligible to be paid as an IHSS provider. Sessions
are offered two times per week typically with a Friday morning and afternoon option.
IHSS contracts with Sourcewise to provide the mandated functions which require
providers be processed prior to them becoming eligible to be paid through IHSS. The
enrollment process in Santa Clara County has been successful in meeting the mandate
and all providers who took action to complete the process have been provided the
opportunity. There were 5,668 new providers processed through enrollment during the
2017 fiscal year which is an increase of 8.4% over last year.
Public Authority continues to use REVA (Registration, Enrollment, Verification,
Appointment) exclusively for provider enrollment with an alternative plan in place for
anyone unable to access the web-based process.

IHSS Annual Report 2017 Page 22
MOA with SEIU Local 2015
The Memorandum of Agreement (MOA) with the union expired February 1, 2017, with no
successor agreement the previous one was automatically extended for 12 months. With
the discontinuance of CCI, the State disbanded the Statewide Authority effective January
10, 2017 and returned collective bargaining responsibilities to the Public Authority.
Negotiations have not been initiated by either the union or the Public Authority as of June
30, 2017.
Community Outreach is conducted in the community to increase awareness about
IHSS. A volunteer IHSS staff member and a representative from SEIU participate in local
health fairs, and community group sessions to share basic information regarding IHSS
and eligibility for the program. The Public Authority purchases materials necessary
for these outreach activities. Nine outreach events were attended throughout the year
providing informational flyers, magnets with the IHSS phone number and answering
questions about the program.
The MOA agreement includes language regarding a new or modified VHP plan being
adopted. A change to the VHP benefit was incorporated effective September 1, 2014
creating two plans, the Classic (original wide network) and the Preferred Plan (new
narrow network). As of June 2017 there were 5,975 providers enrolled in the Classic Plan
and 4,777 providers enrolled in the Preferred Plan. This translates into a 12.5% reduction
of enrollment in the Classic Plan and a 32% increase in the Preferred Plan over the
previous year.
All new enrollees are only eligible to enroll in the Preferred Plan. Any provider who was
enrolled in VHP prior to the creation of two plans remains in the Classic Plan as long as
continue as IHSS providers. If they terminate benefits for any reason and later decide to
return and re-enroll in VHP they are only able to enroll in the Preferred Plan.
Health, dental and vision benefits continue to be offered to providers who work at least
35 hours a month for the most recent two consecutive months. There is a $25 portion of
the premium cost to providers enrolled in Valley Health Plan (VHP). Growth of the
number of providers enrolled in benefits increased over the previous fiscal year.
IHSS Annual Report 2017 Page 23
Figure 3:
Valley Health Plan Liberty (dental)/VSP (vision)
June 2015 10,078 10,692
June 2016 10,752 11,436
Percent Growth 6.27% 6.5%
The Public Authority is also responsible for administering and issuing the VTA Eco Pass
benefit for IHSS providers. The Eco Pass was transitioned to a Clipper Pass by VTA as of
January 1, 2015. The Public Authority has issued 18,729 Eco Pass/Clipper Cards this
calendar year.
IHSS Future Planning
The Social Services Agency has been deeply involved in developing a strong
labor/management partnership to promote improved outcomes for our recipients. Unit
Based Teams (UBT’s) were initiated in the Health and Hospital System and have since
begun in Social Services Agency as well. IHSS requested to be considered for a UBT
and received approval in late 2016.
During the January 2017 mandatory IHSS All Staff Meeting, UBT Facilitators educated
our staff about the UBT process and how a group of frontline employees, Social Work
Supervisors, Managers, and labor would work collaboratively to solve a problem, improve
performance, and enhance quality for measurable results. During this All Staff Meeting,
we asked for volunteers to form a committee within IHSS to determine a project, goal, and
present a deliverable. Ultimately, we formed a committee of volunteers from IHSS staff,
sought input from all of the staff by seeking project ideas from all of the 14 unit meetings
within IHSS, and chose a project based on the most popularly selected idea. The idea
selected was the long phone wait times for our outside callers.
The IHSS UBT committee has been meeting twice a month since February 2017 and
there are additional meetings outside of IHSS that are also required. The IHSS UBT goal
is to reduce the provider phone wait time by 25% of an average of 30 minutes from the
May 2017 baseline by October 31, 2017. Based on one of the most common ideas
collected from staff and stakeholders, we implemented the voice mail option on August 4,
2017. Outside callers now have the option of holding on the line or pressing the pound
sign to leave a message. Since we implemented the voice mail option, we have been
receiving an average of 100 voice mails per day and we have also surpassed our UBT
goal of reducing the phone wait time by more than 25%.

IHSS Annual Report 2017 Page 24
While we are ecstatic that we have surpassed our goal prior to the UBT project
completion date of October 31, 2017, we still have a lot of work to do internally. Some
IHSS staff perceive the forwarded voice mail as an additional workload duty and have
shared their ideas with the UBT Committee, management, and labor about what changes
should take place in order to make this project successful overall.
Once the workload issues have been resolved, we are hoping to implement the email
option effective as early as October 1, 2017. This would allow recipients, providers, and
the community to send us an email in addition to coming to our office in person, calling,
leaving a voice mail, or even sending a fax. We believe that by implementing the email
option, the phone wait times will reduce even more.
Even though the UBT project is expected to end October 31, 2017, we still have plans to
work beyond and improve the wait time even more. We plan to put some of the most
commonly used IHSS forms online so that users may either submit the forms online or
print them out and send them via fax or email to our office to be processed. We have
already begun the revamping of the IHSS lobby to make it more efficient for our recipients
and providers so that they may fill out the most commonly used forms in our lobby and
drop them in a locked drop box on their way out which eliminates the need to wait in line
to speak to a receptionist.
In addition to UBT, the implementation of Electronic Timesheets (E-Timesheets) is brand
new to IHSS. E-Timesheets will enable recipients and providers to submit timesheets via
their smart phone, lap top, or iPad which would replace the paper timesheets that are
currently in place. CDSS began with a small pilot of three counties on June 5, 2017 and
after a successful pilot, all of the remaining counties will Go Live in different waves.
Santa Clara is part of Wave 3 and will Go Live with E-Timesheets on October 11, 2017.
Based on the pilot counties, Waves 1 and 2, we expect that recipients and providers will
be pleased with what E-Timesheets has to offer including making edits electronically,
making fewer errors due to system pop ups and calculations, and having a reduced need
to contact our office because recipients and providers will be able to check the status of
payment with their electronic devices.
The only thing of concern Santa Clara County has at this point is the increase of lobby
visits and phone wait times just prior to Go Live and immediately following Go Live.
However, it has been reported by previous counties that the increase of activity lasts only
about a month or two and that staff do not otherwise see an increase of workload.

IHSS Annual Report 2017 Page 25
Attachments
Attachment 1: IHSS Recipients by City
Attachment 2: IHSS Recipient Spoken Language/Ethnicity Demographics
Attachment 3: Quality Assurance Monitoring Review

Santa Clara County IHSS Recipients Distribution By City
September 2017
Morgan Hill 1.64%
Palo Alto
Campbell 2.56%
2.74%
Saratoga 1.02%
Cupertino
1.86%
Los Gatos 0.80%
Los Altos 0.40%
San Martin 0.28%
Alviso 0.06% Los Altos Hills
0.02%
Gilroy 3.23%
Mountain View
3.06%
Santa Clara 4.38%
Sunnyvale
4.82%
Milpitas 5.41%
San Jose 67.69%
Total IHSS Population: 23,212
City IHSS Recipients San Jose 15702 Milpitas 1257
Sunnyvale 1119 Santa Clara 1017
Mountain View 711 Gilroy 752
Cambell 637 Palo Alto 596 Cupertino 432
Morgan Hill 381 Saratoga 238
Los Gatos 188 Los Altos 95
San Martin 65 Alviso 16
Los Altos Hills 06
Data Source: IHSS QA Dashboard‐case count reflects eligible cases (9/24/17)
ATTACHMENT 1
ATTACHMENT 2
Language
N %
American Sign Language 7 0.028%
Arabic 81 0.325%
Armenian 30 0.121%
Cambodian 246 0.988%
Cantonese 795 3.194% EthnicityEnglish 8,948 35.955% N %
Farsi 906 3.640% Amer Indian/Alaska Natve 47 0.19%
French 4 0.016% Asian Indian 737 2.97%
Hebrew 2 0.008% Black 824 3.32%
Hmong 4 0.016% Cambodian 264 1.06%
Ilocano 41 0.165% Chinese 3,288 13.24%
Italian 4 0.016% Filipino 1146 4.62%
Japanese 14 0.056% Guamanian 3 0.01%
Korean 474 1.905% Hawaiian 6 0.02%
Lao 28 0.113% Hispanic 4,402 17.73%
Mandarin 1,948 7.827% Japanese 46 0.19%
Mien 5 0.020% Korean 500 2.01%
Other Chinese Languages 126 0.506% Laotian 35 0.14%
Other Non-English 1005 4.038% Oth Asian/Pacific Islndr 1122 4.52%
Other Sign Language 4 0.016% Samoan 16 0.06%
Polish 4 0.016% Vietnamese 6,663 26.84%
Portuguese 52 0.209% White 5,555 22.38%
Russian 965 3.878% No Valid Data Reported 172 0.69%
Samoan 8 0.032% TOTAL 24826 100.00%
Spanish 2168 8.711%
Tagalog 585 2.351%
Thai 3 0.012%
Turkish 2 0.008%
Vietnamese 6,427 25.825%
No valid data reported 1 0.004%
TOTAL 24887 100.00%
IHSS cases IHSS RECIPIENT SPOKEN LANGUAGE AND ETHNICITY DEMOGRAPHICS
SEPTEMBER 2017
*Data Source: CMIPS II-Case counts reflect current eligible,pending applications and recently terminated cases.
IHSS cases



































