Embed Size (px)
Citation preview
PHARMACOEPIDEMIOLOGY Drug Safe1y 11 (6): 44&<162. 1994 01 14-5916/94/0012-{)445/S09.00/0
© Ad~ International Limited. All ngh1s reserved.
Idiosyncratic Drug-Induced Haematological Abnormalities Incidence, Pathogenesis, Management and Avoidance
W Nigel Pattonl and Stephen B. Duffu.ll2
1 Department of Haematology, Christchurch Hospital, Christchurch, New Zealand 2 Department of Clinical Pharmacology, Christchurch Hospital, Christchurch, New Zealand
Contents Summary .......... . 1. Incidence . . . . . . . . . . .
1.1 Individual Case Reports 1.2 Cohort Studies .... 1.3 Case-Control Studies. . 1.4 In Vitro Studies. . . . . .
2. Specific Drugs and Drug-Induced Haematological Dyscrasias 3. Pathogenesis and Influencing Factors.
3.1 Regulation of Haemopoiesis 3.2 Immune-Type Mechanisms ... . 3.3 Toxic-Type Mechanisms ..... . 3.4 Pharmacokinetic and Pharmacodynamic Factors
4. Management. . . . . . 4. 1 Agranulocytosis........ 4.2 Aplastic Anaemia ..... . 4.3 Immune Thrombocytopenia 4.4 Immune Haemolysis . . .
5. Avoidance .......... . 5. 1 Education of Prescribers . 5.2 Restricted Prescribing .. 5.3 Haematological Monitoring . 5.4 Patient Instruction ..... . 5.5 Improved Reporting, Collation and Evaluation of Suspected Severe Adverse
Drug Reactions 6. Conclusion ......................................... .
.445
.446
.446
.448
.448
.449
.450
.450
. 451
. 451
.452
.452
.453
.454
.455
.455
.456
.456
.457
.457
.457 458
458 458
Summary Haematological dyscrasias remain important because they are potentially fatal. Their accurate reporting is required to confirm the cause-effect relationship of suspected adverse drug reactions (ADRs); to estimate their incidence; and, by risk-benefit analysis of such events, to introduce preventive measures to reduce their impact. Limitations within the available data on haematological ADRs are reviewed and some suggestions made for improvement. The drugs most commonly associated with haematological dyscrasias are listed. An understanding of the pathogenesis of haematological dyscrasias is essential for their effective man-

446 Patton & Duffull
agement and these are briefly reviewed. Features common to the management of the different types of haematological dyscrasia include the early involvement of a haematologist and drug information pharmacist and the accurate identification and early withdrawal of any likely offending agent. Guidelines for the management of drug-induced aplastic anaemia, agranulocytosis, thrombocytopenia and haemolytic anaemia are presented and the potential value of granulocyte and granulocyte-macrophage colony-stimulating factors (G-CSF; GM-CSF) in the management of agranulocytosis is specifically mentioned. Finally, general principles are discussed whereby serious haematological ADRs might be prevented. These include: the importance of continuing education for drug prescribers; policies on the restricted prescribing of likely offending agents; the use of written instructions for patients; and, the use of haematological monitoring. The guidelines presented in this article should be adapted to meet local circumstances and would prove suitable subjects for audit of their effectiveness.
Adverse drug reactions (ADRs) continue to be a major cause of morbidity, hospital admission and death.[l-3] Blood dyscrasias account for only a small percentage of total cases reported to ADR authorities, but they assume great importance because they are responsible for a large proportion of those cases associated with a fatal outcome.f4] This is especially important when the drugs involved are commonly prescribed for nonfatal illness. The druginduced haematological dyscrasias associated with a potentially fatal outcome include aplastic anaemia, neutropenia, agranulocytosis, thrombocytopenia and haemolytic anaemia. This article focuses on rare idiosyncratic reactions, as opposed to the predictable, dose-dependent haematological toxicity which occurs, for example, following antineoplastic or anticoagulant therapy.
Readers are referred to excellent previous reviews on this subject.f5-7] The contents remain valid, particularly with regard to incidence estimates for drug-induced haematological dyscrasias, detailed listings and referencing of implicated drugs and for discussion of the pathogenesis involved.
This review focuses on: (i) the limitations of the database on drugs and blood dyscrasias; (ii) possible ways in which it might be improved; (iii) advances in the management ofhaematological adverse drug reactions, particularly for drug-induced agranulocytosis; and (iv) avoidance strategies for the pre-
© Adis Internafional Umited. All rights reserved.
vention of serious drug-induced haematological dyscrasias.
1. Incidence
Accurate reporting of ADRs is important to provide early warning of such events, confirm the cause-effect relationship of a suspected ADR and to provide a basis by which their incidence may be estimated. Risk-benefit analysis of such events enables prevention measures to be introduced to limit the impact of ADRs. Unfortunately, the true incidence and accurate attribution of drug-induced blood dyscrasias are difficult to define because of well recognised limitations within the available data from which such estimates are made. The various sources from which our knowledge of druginduced blood dyscrasias is derived are discussed below.
1.1 Individual Case Reports
By definition, ADRs that are idiosyncratic are unexpected and usually rare, and the detailed reporting of individual cases, as a form of postmarketing surveillance, has proved invaluable in the recognition of rare idiosyncratic ADRs. However, these reporting mechanisms are extremely vulnerable to underreporting, selection bias and difficulties in establishing the cause-effect relationship of a suspected ADR.
Drug Safety 11 (6) 1994

Drug-Induced Haematological Abnormalities
It is well recognised, from using data obtained from population-based case studies, that the incidence of ADRs based on reports to ADR agencies is much lower than the real incidence in clinical practice. Indeed, it is estimated that only 10 to 15% of severe ADRs and as few as 5% of mild-moderate reactions are reported. [81 In one study of druginduced neutropenia, only 29 of the 84 cases which had been identified had been reported to the relevant ADR agency.l9]
Reasons why clinicians may fail to report an ADR include failure to recognise an ADR, lack of familiarity with reporting mechanisms, selection bias and apathy.f IO] Even lower percentages of ADRs are likely to be reported in the medical literature, particularly when a cause-effect relationship has already been established for a given ADR. Furthermore, searches of the medical literature for suspected ADRs are always incomplete due to the restrictions imposed by the number of journals available for searching, their time periods of availability, their language of publication and the time and resources available to, and the expertise of, the searcher. Computer-based searches, which have proved a tremendous advance in recent years, also suffer from these limitations as such data bases only cover a selected but incomplete part of the currently available medical literature.
Selection bias in the reporting of ADRs is also a major problem and can result in both under- and overreporting. Clinicians often fail to report serious ADRs, especially if these have been previously well recognised, or they may be selective in reporting events with newer drugs. Following promptings from their local ADR agency they may report events for a short period only, or report only specific events related to specific drugs. Fear of possible legal repercussions or a reluctance based on a degree of dependence upon a pharmaceutical company might also cause underreporting. False-positive reporting bias may also occur if a few initial reports suggest a causal relationship for a suspected ADR. Each report may encourage others, and such reporting, by assuming a cause-effect relationship, may result in a biased
© Adis I"ter"atio"al Limited. All rights reserved.
447
conclusion being made about the drug involvement or frequency in a suspected ADR.
Unfortunately, many case reports lack the complete information required to judge whether arl association between a drug and an ADR may be either causal or coincidental. It is desirable to have a simple standardised system of high specificity and sensitivity that accurately attributes a cause-effect relationship and avoids identifying spurious or false-positive associations.
Many previous reports have attempted to address this issue by establishing criteria for ranking the probability of causation for a suspected ADR.[ 10-12]
These criteria assess information relating to previous experience with the drug involved, the temporal relation to drug exposure, pharmacokinetic information, clinical progress in relation to drug withdrawal and rechallenge, in vitro or other supportive experimental evidence, and alternative aetiological explanations. Using such criteria, valid and reproducible scoring systems have been devised to assess possible ADRs as being either unlikely, possible, probable or definite.
Although particular difficulties can occur when assessing haematological ADRs,f 13] there is little published evidence that such standardised criteria are regularly being used for this purpose) 14] The further development and use of such systems by ADR agencies and journal editors is to be encouraged.
Once individual reports have been made concerning potential ADRs it is important that such data are collated centrally, analysed and summarised. Conclusions drawn and important messages must be widely promulgated and such data should be made easily available for subsequent use.
When serious ADRs occur, especially in the case of haematological dyscrasias, it is essential that any offending drugs be identified immediately and accurately so that appropriate action can be taken. Individual enquiries are made to the various data sources including individual drug companies, national ADR databases and the medical literature, but in actual practice, such surveys are often slow, usually incomplete and potentially inaccurate.f 15]
Drug Safety 11 (6) 1994

448
However, such surveys may be invaluable sources of useful data which are never subsequently collated onto an international database for the benefit of others. If such data were more readily available important clinical decisions could be made more rapidly and with greater accuracy.
1 .2 Cohort Studies
Cohorts of selected patients exposed to a particular drug for a given time have been studied either retrospectively or prospectively to determine the incidence of ADRs. Selection bias may be introduced by reporting only those studies in which the ADR was actually observed. Extremely rare events may not occur even in large cohort studies, thus limiting their value further.
1 ,3 Case-Control Studies
In case control studies, a large number of cases of a given problem, such as a rare ADR, are identified from a source population over a given time period and compared with a control population.l 16] This epidemiological approach, which is well suited to rare events, has much greater statistical power than cohort studies.
Methodological drawbacks include problems of case definition and access to complete case details, the selection of appropriately matched controls, the misclassification of risk because of difficulties in judging the relevant time period of drug exposure, and difficulty in controlling for compounding variables such as the concomitant use of multiple drugs.[I3,16, 171 Such studies are also limited by the size and geographic location of the popUlation studied, the pattern of drug usage within that population and the duration of the study period. The statistical power of such studies will be low in situations where drugs are used infrequently, such as with newer agents, and where the events under study occur extremely rarely.
Despite these caveats, one population casecontrol study, the International Agranulocytosis and Aplastic Anaemia Study (IAAAS), deserves special mention.l 13,18-221 This independent multidisciplinary group has explored new ground in the
© Adis International Limited. All rights reserved.
Patton & Duffull
conduct of major epidemiological studies, and such a detailed study is unlikely to be repeated. By studying prospectively and most thoroughly a population of 23 million in 6 countries in Europe and Israel for an average period of 5 years between 1980 and 1986, the IAAAS has provided arguably the most accurate data on the incidence of druginduced agranulocytosis and aplastic anaemia.l 13,17] The summary data for agranulocytosis are shown in table I.l13]
The overall incidence of agranulocytosis was 4.7 cases per million population per year. The incidence increased dramatically with age, especially for those over 60 years of age. Women outnumbered men 2 to 1. Detailed data were available from 270 cases, from which 21 significant drug associations with agranulocytosis were identified. Nearly all the drugs involved had already been reported to cause agranulocytosis, one notable exception being digitalis glycosides. The authors concluded that the estimates for risks of agranulocytosis associated with exposure to all drugs identified were low - 'so low as to have only minor implications for drug safety and consequently for the need for regulatory action'.
The greatest risks for agranulocytosis were associated with exposure to antithyroid drugs, where the multivariate relative risk estimate (with 95% confidence interval) was 97 (36 to 262), and where the excess risk estimate was 5.3 cases per million users for any exposure during a I-week period. Agranulocytosis caused by antithyroid drugs is still associated with significant mortality,l23] and we would advise that patients on these drugs should be the target of specific preventive measures.
The IAAAS incidence estimate for drug-induced agranulocytosis is similar to previous estimates generated from predominantly Scandinavian studies.l9,24-281 These other studies employed less rigorous criteria for case definition, analysed cases retrospectively and produced estimates similar to the IAAAS in the range of 2.5 to 10 per million per year. The overall fatality rate of agranulocytosis reported by IAAAS of 9% is much lower than has been reported in earlier case studies.l25-27,29,301
Drug Safety 11 (6) 1994

Drug-Induced Haematological Abnormalities 449
Table I. Summary data on agranulocytosis from the International Agranulocytosis and Aplastic Anaemia Study (IAAAS)113]
No. of cases identified
Hospital acquired
Community acquired
Population studied
Overall estimated incidence rate
Overall estimated incidence rate attributed to drug-induced causes
Overall mortality rate
Influence of age on incidence rates and mortality
537
157
380 115.9 million person·years
4.7 per million per year"
3.1 per million per year'
9.0%
Age range (years) Incidence rate (per million per year) Mortality (%)e
2·24 1.1
25·59
>60
2.7
9.5
5
9
12 a These figures mask significant regional variations, which ranged from 1.5 per million per year in Milan, Italy to 5.5 per million per year in
Budapest, Hungary.
b Calculated estimate based on study authors' estimate that following multiple logistic regreSSion analysis, 64 to 66% of cases could be attributed to drug-induced causes. The drug associations identified with agranulocytosis were dipyrone (some regions only), butazones, indomethacin, salicylates, cotrimoxazole (trimethoprim-sulfamethoxazole), ~-Iactams, macrolides, antithyroid drugs, propranalol, aprindine, procainamide, dipyridamole, cinepazide, digoxin, acetyldigoxin, sulfasalazine, thenalidine, troxerutin and corticosteroids.
c Data supplied on community·acquired cases only where overall mortality was 10%.
However, more recent estimates of fatality rates have been much closer to that reported by the IAAASJ31 l It is likely the reduction in fatality rates in recent years largely reflects improvements in supportive care measures, but it is also likely that selective reporting of fatal cases may have contributed to higher fatality rates reported in the past. It is anticipated that newer preventative and supportive care measures should reduce the mortality of drug-induced agranulocytosis further.
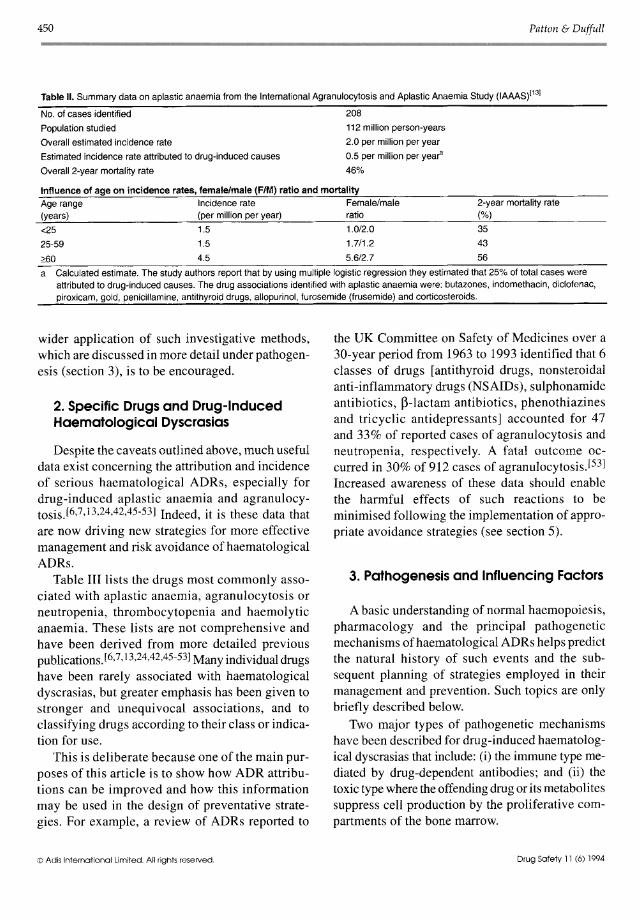
The IAAAS summary data for aplastic anaemia are shown in table nJ13l Detailed data were available from 152 cases from which 10 significant drug associations with aplastic anaemia were identified, including one possible previously unrecognised association with furosemide (frusemide). Again, all estimates of excess risks for aplastic anaemia associated with all identified drugs were low. The high confirmed mortality for drug-induced aplastic anaemia warrants consideration of preventative measures. The incidence rate in this study (2.0 per million per year) compares favourably with that (1.5 per million per year) of another large prospective population-based study in France which also employed rigorous criteria for the identification of casesJ32l
© Adis International Limited. All rights reserved.
A similar, but much smaller study, in Bangkok has reported an overall incidence estimate for aplastic anaemia of 3.7 per million per yearJ33l In the Bangkok study, however, the highest incidence (8.4 per million per year) was observed amongst males in the 15 to 24 year age group. Incidence estimates for aplastic anaemia, derived from less rigorous retrospective popUlation based surveys are reviewed by the IAAAS authors.l34-39l
1 .4 In Vitro Studies
In vitro studies using cells and/or plasma from patients affected by an idiosyncratic ADR, tested with and without the presence of the implicated drug, may be helpful in confirming the presence and the pathogenesis of the ADR for that patient. Such investigation may be especially helpful in cases of multidrug administration, may prevent the need to consider drug rechallenge and may be used to predict an individual's in vivo response to a related drug.l40-44l Unfortunately, such in vitro investigations may not be applicable in many circumstances, are technically demanding and often require facilities and technical expertise that are expensive and not routinely available.f7l However,
Drug Safety 11 (6) 1994
450 Patton & Duffull
Table II. Summary data on aplastic anaemia from the International Agranulocytosis and Aplastic Anaemia Study (lAAAS)113]
No. of cases identified
Population studied
Overall estimated incidence rate
Estimated incidence rate attributed to drug-induced causes
Overall 2-year mortality rate
208
112 million person-years
2.0 per million per year
0.5 per million per yeara
46%
Influence of age on incidence rates, female/male (FIM) ratio and mortality Age range Incidence rate Female/male 2-year mortality rate
(%) (years) (per million per year) ratio
d5 1~ 1.M~ 35
43 56
25-59 1.5 1.7/1.2
260 4.5 5.6/2.7
a Calculated estimate. The study authors report that by using multiple logistic regression they estirnated that 25% of total cases were attributed to drug-induced causes. The drug associations identified with aplastic anaemia were: butazones, indomethacin, diclofenac, piroxicam, gold, penicillamine, antithyroid drugs, allopurinol, furosemide (frusemide) and corticosteroids.
wider application of such investigative methods, which are discussed in more detail under pathogenesis (section 3), is to be encouraged.
2. Specific Drugs and Drug-Induced Haematological Dyscrasias
Despite the caveats outlined above, much useful data exist concerning the attribution and incidence of serious haematological ADRs, especially for drug-induced aplastic anaemia and agranulocytosis.l6,7,13,24,42,45-53] Indeed, it is these data that are now driving new strategies for more effective management and risk avoidance ofhaematological ADRs.
Table III lists the drugs most commonly associated with aplastic anaemia, agranulocytosis or neutropenia, thrombocytopenia and haemolytic anaemia. These lists are not comprehensive and have been derived from more detailed previous publications.f6,7, 13,24,42,45-53] Many individual drugs have been rarely associated with haematological dyscrasias, but greater emphasis has been given to stronger and unequivocal associations, and to classifying drugs according to their class or indication for use.
This is deliberate because one of the main purposes of this article is to show how ADR attributions can be improved and how this information may be used in the design of preventative strategies. For example, a review of ADRs reported to
© Ads International limited. All rights reserved
the UK Committee on Safety of Medicines over a 30-year period from 1963 to 1993 identified that 6 classes of drugs [antithyroid drugs, nonsteroidal anti-inflammatory drugs (NSAIDs), sulphonamide antibiotics, p-lactam antibiotics, phenothiazines and tricyclic antidepressants] accounted for 47 and 33% of reported cases of agranulocytosis and neutropenia, respectively. A fatal outcome occurred in 30% of 912 cases of agranulocytosis,f53] Increased awareness of these data should enable the harmful effects of such reactions to be minimised following the implementation of appropriate avoidance strategies (see section 5).
3. Pathogenesis and Influencing Factors
A basic understanding of normal haemopoiesis, pharmacology and the principal pathogenetic mechanisms ofhaematological ADRs helps predict the natural history of such events and the subsequent planning of strategies employed in their management and prevention. Such topics are only briefly described below.
Two major types of pathogenetic mechanisms have been described for drug-induced haematological dyscrasias that include: (i) the immune type mediated by drug-dependent antibodies; and (ii) the toxic type where the offending drug or its metabolites suppress cell production by the proliferative compartments of the bone marrow.
Drug Safety 11 (6) 1994

Drug-Induced Haematological Abnormalities
In immune cases, the mechanism whereby idiosyncrasy is achieved is immediately apparent, but in other cases the circumstances are less obvious. In toxic reactions, large drug doses for prolonged periods, or altered pharmacokinetics, e.g. inhibition of drug clearance, which could be due to genetic or acquired factors, are implicated. In others, pre-existing damage or undue sensitivity to damage of host haemopoietic precursors may be involved.L6,7,41] The incidence of drug-induced haematological dyscrasias increases with age, and many of the above factors, such as age-related impairment of renal or hepatic function and agerelated damage to the haemopoietic stem cells, are consistent with this observation.
3.1 Regulation of Haemopoiesis
The haemopoietic system is maintained by pluripotential haemopoietic stem cells (PHSCs) that are capable of generating, throughout life, the terminally differentiated and widely diverse functional cells of the peripheral blood.l54,55] Toxic damage to PHSCs, which may occur following exposure to such drugs as gold, phenylbutazone or chloramphenicol, results in aplastic anaemia, the most serious drug-induced dyscrasia. Such damage is usually profound, irreversible and associated with a high mortality.
PHSCs give rise to intermediate precursor cells, called progenitors or colony-forming cells, which are transit amplifying popUlations of cells committed to a restricted range of lineages which generate
451
colonies of more differentiated progeny in response to appropriate colony-stimulating factors (CSFs).£56,57] Progenitor cells eventually become restricted to a single lineage, and generate the morphologically recognisable haemopoietic precursor cells seen in the bone marrow. These recognisable marrow precursors undergo further proliferation and maturation within the marrow before becoming the terminally differentiated functional cells of the peripheral blood.
Damage to the precursor or progenitor cell compartment of the marrow is usually reversible as by definition, the pluripotential stem cell compartment remains unaffected. Damage to the latest precursors is associated with early recovery within a few days, whereas damage to the earliest progenitors is associated with much longer recovery times of more than 2 weeks.L58-601 Many haemopoietic CSFs that drive the proliferation and differentiation of precursor cells have been identified and cloned, and are available for clinical use. Evidence is mounting that in certain circumstances selected CSFs can accelerate marrow recovery following drug-induced damage to the progenitor/precursor marrow compartment.[15,61-72]
3.2 Immune-Type Mechanisms
The classical model of immune agranulocytosis is the acute form induced by the now rarely used pyrazolones, amidopyrine and dipyrone.[41] In previously exposed and sensitised individuals further drug exposure triggers an immunologically-
Table III. Drugs commonly associated with haematological dyscrasias (in approximate descending order of incidence)
Aplasia Agranulocytosis Thrombocytopenia Haemolyfic anaemia
Gold Antithyroid drugs Gold J3-lactams Phenylbutazone Phenylbutazone Heparin Quinine/quinidine Chloramphenicol Sulphonamides Quinine/quinidine Thiazides Penicillamine Clozapine Sulphonamides Sulphonamides Nonsteroidal Phenothiazines Anticonvulsants NSAIDs anti-inflammatory drugs Mianserin NSAIDs Rifampicin (NSAIDs) NSAIDs Diuretics Isoniazid
Sulphonamides j3-lactams Rifampicin (rifampin) Phenothiazines Antithyroid drugs Captopril Sulphonylureas Sulphonylureas Sulphonylureas H2-antagonists Cimetidine Nomifensine Phenothiazines Allopurinol
© Adis International Umited. All rights reserved. Drug Safety 11 (6) 1994

452
mediated hypersensitivity reaction, which results (often within a few hours) in the disappearance of neutrophils from the blood. In idiosyncratic individuals, the drug induces the production of an antibody which combines with the drug or its metabolites in vivo and which can then also react with the leucocytes of any individual in vivo.
In cases of drug-induced haemolytic anaemia, 3 main pathogenetic mechanisms have been described.l44.48,73] These include: (i) the hapten (penicillin) type, where an antibody binds to an erythrocyte membrane-drug antigen complex; (ii) the circulating immune complex, or innocent bystander type, where a drug antigen-antibody-complement complex is adsorbed onto the erythrocyte membrane; and (iii) the autoantibody type, e.g. the methyldopa type, where the drug triggers the formation of an anti-red cell antibody.
Similar mechanisms are responsible for drug-induced immune thrombocytopenias, where hapten type and innocent bystander type reactions commonly occur.l50-52,74] In an analogous way to methyldopa, gold therapy can induce platelet autoantibody production to produce a classical immune thrombocytopenic purpura (ITP) syndrome.l751
Common to all of these immune type dyscrasias are the normal effector processes which mediate cell destruction, e.g. complement-mediated cell lysis and adherence, and phagocytosis by cells of the reticuloendothelial system.
The factors responsible for idiosyncratic immune reactivity remain poorly understood, but a genetic basis has been suggested in some individuals by the more frequent occurrence of specific human leucocyte antigen (HLA) antigens. For example, the development of gold-induced ITP is linked to HLA DR-3 positivityV6]
3.3 Toxic-Type Mechanisms
Direct toxicity to haemopoietic cells is suggested by a slow decline in haemopoietic cells, dose-dependency and the lack of immediate relapse if the offending drug is reintroduced in small doses after recovery. For agranulocytosis, these have been described as type II reactions, in contrast
© Adis International limited. All rights reserved.
Patton & Ouffull
to the acute type I reactions that can occur in immunosensitised patients rechallenged with only a small amount of the offending drug)41]
An example of a toxic type agranulocytosis reaction is that mediated by chlorpromazine. Chlorpromazine is a powerful electron donor that profoundly affects a number of cellular functions, including the proliferative capacity of the haemopoietic system in vitro. Chlorpromazine produces dose-dependent inhibition of granulopoiesis.l41,77]
While there is some relationship to the administered dosage, chlorpromazine-induced agranulocytosis has been considered to be an idiosyncratic reaction. Interestingly, all of these cases show greatly enhanced susceptibility to the antiproliferative effects of chlorpromazine when compared with normal controlsV8] The recent decline in the incidence of chlorpromazine-induced agranulocytosis has been attributed to a general reduction in the doses administered)13]
3.4 Pharmacokinetic and Pharmacodynamic Factors
In some circumstances, idiosyncratic druginduced blood dyscrasias may be related to various patient specific pharmacokinetic parameters. There seems to be some evidence that although idiosyncratic in nature, these reactions may have some dose-dependency due to an impairment in the clearance of a drug or its metabolite. This, in conjunction with other factors (yet to be determined), may increase the risk of such reactions. More work needs to be undertaken to determine if pharmacokinetic differences are present in patients who experience idiosyncratic reactions. It could be that many of the previously considered idiosyncratic reactions are not dose-independent at all.
Captopril-induced neutropenia is a well defined example. Although idiosyncratic in nature, and probably not a class effect of ACE inhibitors, evidence from postmarketing studies has established a relationship between the dosage of captopril (>150 mg/day) and neutropenia.[79] The incidence of captopril-induced neutropenia also appears to be much higher in those with impaired renal function
Drug Safety 11 (6) 1994

Drug-Induced Haematological Abnormalities
(i.e. reduced clearance) and in those with collagen vascular disease.f80-82]
Other examples include: (i) penicillin-induced agranulocytosis, which occurs in 5 to 15% of patients treated with high doses and for prolonged periods (cumulative dose >120g)[83] and which also occurs more frequently in those with hepatic dysfunction;l84] (ii) amrinone-induced thrombocytopenia, which has been linked to peak concentrations in excess of 0.4 mg/L, and possibly also to the ratio of amrinone to its N-acetyl metabolite;[85] (iii) carbamazepine-induced neutropenia, which has been attributed to the accumulation of toxic drug metabolites in individuals who are unable to clear these products normally;[41] and (iv) phenylbutazone-induced aplastic anaemia, which may be linked to reduced drug clearance. [86]
Drug interactions may also be important. There is evidence suggesting that clozapine-induced agranulocytosis is related to a toxic metabolite that suppresses haemopoiesis.f87] Of interest is the observation of cases of agranulocytosis occurring in patients previously stabilised on clozapine, who were given carbamazepine.l88] It is possible that this phenomenon could be due to the additive myelosuppressive effects of each agent, but it is also conceivable that carbamazepine (an enzyme inducer) might increase the metabolism of clozapine to its toxic metabolite. The concomitant use of drugs known to cause bone marrow suppression by toxic mechanisms is potentially problematical as the combination may interact either additively or synergistically to increase the risk or severity of the bone marrow suppression.
Some idiosyncratic drug-induced adverse haematological effects are known to be genetically determined. For example, idiosyncratic druginduced oxidative haemolysis occurs in genetically susceptible individuals who are predisposed to the oxidant stress induced by such drugs.l89] Normal individuals can counteract this oxidant stress, but individuals with unstable haemoglobins and deficiencies in the enzymes that generate reducing power within the erythron may develop acute
© Adis International Limited. All rights reserved.
453
intravascular haemolysis with renal failure when treated with such oxidant drugs.
Antimalarials and sulphonamide antibiotics can commonly cause oxidative haemolysis in individuals with glucose-6-phosphate dehydrogenase (G6PD) deficiency, a sex-linked disorder. In certain situations, for example before commencing primaquine therapy, screening for G6PD deficiency has been recommended.l90j Dapsone is strongly oxidant and is capable of producing oxidative haemolysis in non-G6PD-deficient individuals, although this is rarely seen with dosages less than 200 mg/day.l89]
In addition to patient-related factors there is evidence to implicate certain chemical structures within the drug classes that are associated with an increased incidence of blood dyscrasias. [91] These chemical structures mayor may not be related to the functional components of the drugs involved. The most notable potential examples are sulphurcontaining drugs which include captopril, penicillamine, sulfasalazine, the sulphonamide antibiotics, sulphonylureas, antithyroid drugs, H2-antagonists, diuretics and phenothiazines. Interestingly, gold compounds and many ~-lactam antibiotics also contain sulphur moieties.
The development of H2-antagonists illustrates how differences in drug structure may affect the incidence of drug-induced haematological dyscrasias. Metiamide, the first H2-antagonist used in humans, was withdrawn because of its unacceptably high incidence of agranulocytosis, but its successor, cimetidine, which differs from metiamide by its lack of a thiourea side chain, is rarely associated with agranulocytosis. In vitro, both metiamide and cimetidine can block the H2-receptors on haemopoietic stem cells, but animal studies have shown that metiamide and not cimetidine is taken up by the bone marrow, thus possibly explaining the relative safety of cimetidine compared with metiamide.l6]
4. Management
There are many common features to the management of the different types of drug-induced
Drug Safety 11 (6) 1994

454
Table IV. Guidelines forthe management of patients with suspected drug-induced agranulocytosis
1. Early liaison with haematologisVdrug information pharmacist
2. Assess severity of problem:
• peripheral blood neutrophil count • bone marrow findings
3. Consider investigation/cryopreservation of diagnostic material
4. Discontinue (if possible) likely offending drug(s)
5. Is infection present?: No - institute prophylaxis measures:
• reverse barrier isolation • antimicrobial prophylaxis • observation for infection
Yes - treat urgently and appropriately
6. Accelerate marrow recovery with a cOlony-stimulating factor:
• established infection • severe marrow granulopoietic hypoplasia
7. Monitor progress:
• clinical • neutrophil count, marrow findings
8. Avoid future exposure to likely offending drug
9. Report findings to adverse drug reaction authority
haematological dyscrasias (tables IV and V). These reactions are potentially fatal, and appropriate early action may be life saving. Important steps include the early involvement of a haematologist and drug information pharmacist and/or clinical pharmacologist.
The drug information pharmacist, who may be located at a regional centre, plays a pivotal role in the early and accurate identification of any likely offending drug so that it may be discontinued. There is evidence to show that failure to stop an offending drug can be associated with a much greater mortality, and that early discontinuation can be associated with a good chance of recovery.l231 A haematologist is needed for help in diagnosis, the assessment of the severity of the problem and for advice on subsequent management.
4.1 Agranulocytosis
In assessing the severity of agranulocytosis, it is not only the absolute level of circulating neutrophils which is important, but also the bone marrow findings. The infection risk associated with severe neutropenia and the high mortality associated with prolonged neutropenia have long been recogn
© Adis International limited All rights reserved.
Patton & Duffull
ised.l921 There is also evidence that the speed of neutrophil recovery following agranulocytosis depends on the degree of granulocyte compartment depletion within the marrow.[931 For example, in those cases where, at diagnosis, promyelocytes and myelocytes can be found in the bone marrow, it can be expected that neutrophil recovery will occur relatively promptly (i.e. within 4 to 7 days) following withdrawal of the offending drug. However, in those cases where granulopoiesis is completely absent, neutrophil recovery cannot be expected for at least 14 days. [58-60] These latter cases resemble more closely the pattern of neutrophil recovery occurring following myeloablative chemotherapy, which can be accelerated using the myeloid colony stimulating factors granulocyte CSF (G-CSF) or granulocyte-macrophage CSF (GM-CSF))94,951
The cells involved are haemopoietic precursor cells within the neutrophil lineage, and it seems likely that the neutrophil precursor cells left within the bone marrow after such drug-induced damage should respond to either G-CSF or GM-CSF ther-
Table V. Guidelines for the management of patients with suspected drug-induced aplastic anaemia
1. Confirm diagnosis:
• early involvement of haematologisVdrug information officer • peripheral blood/ bone marrow aspirate and trephine findings • exclusion of other causes of pancytopenia
2. Discontinue (if possible) likely offending drug
3. Institute appropriate supportive care measures for bone marrow failure:
• infection prophylaxis/treatment • transfusion support; may need filtered,
cytomegalovirus-negative, human leucocyte antigen (HLA)-matched products
4. Early exploration of marrow transplant option: • assess age, severity/potential reversibility of aplasia and
sibling/unrelated donor availability • review with local haematologisVmarrow transplant centre • if relevant, proceed with transplant workup e.g. tissue typing
studies
5. Plan specific aplasia management:
• supportive care • transplantation • androgens • immunosuppression
6. Avoid future exposure to likely offending drug(s)
7. Report findings to adverse drug reaction authority
Drug Safety 11 (6) 1994

Drug-Induced Haematological Abnormalities
apy. Therefore, in drug-induced agranulocytosis, where myeloid precursor cells are still present within the bone marrow, accelerated neutrophil recovery would be expected within 1 to 4 days following CSF therapy. If myeloid precursors are absent from the bone marrow neutrophil recovery would be expected to take correspondingly longer, but to still occur before the time taken in the absence of a CSF.
Rapid neutrophil recovery following G-CSF or GM-CSF therapy for drug-induced agranulocytosis has recently been reported.l 15,61-71] In view ofthese results and the risk of mortality in druginduced agranulocytosis it appears reasonable to consider the use of G-CSF or GM-CSF in these cases. This practice is unlikely to have major financial consequences in view of the rarity and short term nature of this conditionVO,71] It should be realised that neutrophil recovery is a surrogate marker of morbidity and mortality in drug-induced agranulocytosis, and that presenting clinical features such as impaired renal function and bacteraemia, especially if Gram-negative, are other important prognostic factors)}l]
We would normally use G-CSF or GM-CSF only in cases of severe neutropenia associated with either established clinical infection or absent granulocyte precursors in the bone marrow when neutrophil recovery can be predicted to be prolonged. Repeat bone marrow examination can be used to monitor the progress of granulocyte recovery. It is anticipated that the co-ordinated response outlined above, along with the use of myeloid CSFs, will help to reduce further the mortality from this condition.
4.2 Aplastic Anaemia
Aplastic anaemia is more serious than other haematological dyscrasias because of the high mortality related to the severity of the underlying aplasia.l45,96] It is important to discontinue promptly any likely offending agent, as some early onset drug-induced hypoplasias are completely reversible following drug withdrawal, and because
© Adis International Limited. All rights reserved.
455
many patients may survive marrow hypoplasia if the stem cell damage is incomplete.l97,98]
Chelation therapy with either dimercaprol or acetylcysteine has been advocated for the treatment of gold-induced aplastic anaemia, but the evidence for their efficacy remains limited.l97,99] In severe cases, an early bone marrow transplant may be life saving. The early involvement of a haematologist is essential to help plan supportive care and to evaluate the prospects for transplantation. Many cases of severe drug-induced aplasia have been treated successfully by marrow transplantation, but this option is restricted to a minority of younger patients with suitable donors.l lOO] Important factors likely to increase the chances of a successful transplantation outcome include the early involvement of the transplant centre, the early identification of a suitable donor, good quality supportive care measures which avoid alloimmunisation and cytomegalovirus (CMV) transmission, and early transplantation. [45, 101]
In the absence of a transplant option, supportive care measures become the mainstay of therapy. Androgen therapy may be useful, but this appears most likely to benefit the less severe cases of hypoplastic anaemia.l45 ,102-104] There are few published data on the potential benefits of immunosuppressive and haemopoietic cytokine therapy for drug-induced aplasia. Limited benefit might be expected if the aplasia is caused by toxic damage to pluripotential haemopoietic stem cells. However, occasional reports have cited marrow recovery of gold-induced aplasia following treatment with either anti-human thymocyte globulin or high doses of steroids.l 105,106] Some preliminary data suggest that GM-CSF may be of value in neutropenic patients with idiopathic aplastic anaemiaJ721
4.3 Immune Thrombocytopenia
Cessation of the offending agent is the most important aspect of the management of druginduced immune thrombocytopenia. Platelet recovery usually occurs within a few days. In severe, life-threatening situations, treatment with high dose intravenous immunoglobulin G (IgG), to
Drug Safety 11 (6) 1994

456
block the reticuloendothelial system, and platelet transfusion should be considered) I 07] Quinine and quinidine may cause severe thrombocytopenia associated with fatal haemorrhage,l108] but platelet transfusion in these cases may be ineffective for 2 to 3 days after cessation of therapy because of delayed drug metabolism and the persistence of drugantibody complexesV4] Rarely, quinine-induced thrombocytopenia may be associated with disseminated intravascular coagulation (DIC) or haemolytic uraemic syndrome)109,1l0]
Thrombocytopenia that persists beyond 2 weeks is probably not related to a drug-induced platelet antibody. Further use of an offending drug in a sensitised individual is contraindicated)lll]
Heparin-induced thrombocytopenia and/or associated thrombosis, which is mediated by a drugdependent IgG antiplatelet antibody, and usually occurs after 7 days of therapy, warrants specific mention)112,113] The syndrome often goes unrecognised as it has only recently been characterised and because: (i) it can occur with low dose heparin therapy given to prevent thrombosis of intravenous catheters,l1l4] which might not even appear on a patient's drug chart; and (ii) because it may be attributed to dilution or other consumptive causes of thrombocytopenia such as sepsis.
Laboratory testing for heparin-induced thrombocytopenia is helpful in distinguishing this from other causes,f IIS-117] Heparin should be discontinued in suspected cases, and the indications for anticoagulation should be reviewed. If patients require continuing anticoagulation, options include the introduction of warfarin, the heparinoid danaparoid sodium (Org 10172)[118,119] or the defibrinogenating venom, ancrod)120]
Low molecular weight heparins, although associated with a reduced incidence of thrombocytopenia, should probably not be used as they may result in persistent thrombocytopenia and thrombosis,f121] Platelet transfusions are also contraindicated because of the risk of precipitating thrombotic complications. Following heparin withdrawal, platelet recovery usually occurs within a few days.
© Adis International Limited. All rights reserved.
Patton & Ouffull
4.4 Immune Haemolysis
The natural history and management of drug-induced immune haemolysis is dependent upon the pathogenetic mechanism involved. The most serious reactions, which can be fatal, are associated with the immune complex type reactions where intravascular haemolysis, renal failure and DIC can occur)122-126] An offending drug must be discontinued immediately and in patients with mild haemolysis, no further action may be necessary. In more serious cases, supportive care measures identical to those for a severe intravascular haemolytic transfusion reaction, renal failure and DIC are required. Cross-matching blood may be difficult, and further transfusions must be given with caution because rapid destruction of the transfused cells may occur, producing further complications. Corticosteroids are unlikely to be of value in this situation, and additional measures such as exchange transfusion or plasma exchange should only be considered as a last resort. The offending drug should not be reintroduced) 126)
5. Avoidance
Idiosyncratic ADRs are by nature unpredictable, but their incidence and severity can be reduced if lessons learned from previous experience can be put into practice (table VI),f127,I28]It must be emphasised that this is an ongoing process
Table VI. Strategies for the prevention of severe drug-induced haematological dyscrasias
Education of prescribers on likely offending agents
Restricted prescription of commonly offending drugs: • withdrawal of drug license • for specific indications only • to individual specialists experienced in their use • quantity of drug prescribed • general restrictions
Haematological monitoring of commonly offending drugs
Verbal/written instructions for patients prescribed drugs where serious reactions are possible
Improved recognition and management of individual cases
Improved reporting, collation, in vitro investigation and evaluation of suspected severe adverse drug reactions for existing drugs and new agents
Drug Safety 1 1 (6) 1994

Drug-Induced Haematological Abnormalities
requiring continued vigilance. The incidence of ADRs may remain at its current level if the numbers of cases prevented by such actions are replaced by additional cases caused by newer drugs. However, following adherence to such guidelines, it is likely that offending drugs, which have other important therapeutic benefits, can be used with increasing margins of safety.
5.1 Education of Prescribers
The continued education of prescribers on likely offending drugs and the circumstances in which such ADRs occur is an essential prerequisite for the design of any preventive strategy. Such information should be reviewed regularly by expert groups such as national drug safety committees and specialist task forces, so that guidelines on drug prescription and the management of specialist problems can be produced and regularly updated.l 129]
5.2 Restricted Prescribing
Management guidelines may recommend some policy of restricted prescribing. In extreme circumstances this could involve the withdrawal of a drug. In other situations it may be appropriate to restrict the prescription of the drug for well defined specific indications where there is no alternative safer treatment, or to restrict the prescription of the drug to a small number of specialists, who could be registered, who are highly experienced in the use of that agent, alternative therapies and the management of the diseases concerned. For example, chloramphenicol could be reserved for the treatment oflife-threatening infections[130j and be prescribed by an infectious disease physician. Similarly, phenylbutazone could be reserved for ankylosing spondylitis, as second-line therapy. Gold, penicillamine and sulfasalazine could be reserved as second-line therapies for rheumatoid arthritis, and the use of these drugs could be supervised by approved rheumatologists.
In these and other situations it is also appropriate to prescribe limited quantities of a specific drug so that the patient returns for assessment prior to
© Adis International Limited. All rights reseNed.
457
Table VII. Drugs for which haematological monitoring is recommended
Gold Phenylbutazone (~ 7 days' therapy) Chloramphenicol Penicillamine Sulfasalazine Clozapine Mianserin Heparin (~ 5 days' therapy) Benzylpenicillin (penicillin G) [prolonged intravenous therapy,
> 1 OOg total dose]
further prescription. In situations where a drug may be prescribed by clinicians in different specialities for a variety of conditions it may be more appropriate to advise more general restrictions on drug usage, based on general awareness of specific problems. For example, more discriminate use of NSAIDs should be encouraged, as these agents are responsible for many serious adverse effects (in addition to haematological ones) that occur more commonly in the elderly and in those with impaired renal, cardiac or hepatic function.l 131]
5.3 Haematological Monitoring
In some situations, the incidence of severe haematological dyscrasias is so high that haematological monitoring is warranted (table VII). There is good evidence that such monitoring, by identifying early warning signals, helps prevent severe ADRs, greatly improves the therapeutic margins for such treatments and reduces patient mortality.l98,128] In these situations, it is important that the recommended guidelines on clinical and laboratory monitoring are accurately followed, and the responsible attitude adopted by many drug companies in educating prescribers and supervising therapy is to be applauded.
The current regulations governing the use of the antipsychotic agent clozapine warrant specific mention. This agent, which has been hailed as a significant advance for the treatment of schizophrenia,[132] is associated with a high incidence of agranulocytosis. It is only licensed for use in developed countries under the auspices of the Sandoz Clozapine Patient Monitoring Service,
Drug Safety 11 (6) 1994

458
which requires that the patient, prescriber and supplying pharmacist register with the service and comply with the therapy and monitoring guidelines.l 133] Sandoz, who market a GM-CSF, also supply free GM-CSF for the treatment of any identified severe cases of clozapine-induced agranulocytosis, as part of this service. Following such responsible practices this agent is currently being used with a high margin of safety.l 128, 132]
Other indications for haematological monitoring are less well established, Further guidelines may appear in future, but it may be appropriate to consider haematological monitoring in circumstances where potentially offending agents are prescribed for prolonged periods, especially in the elderly.l131]
5.4 Patient Instruction
In situations where serious haematological dyscrasias occur more frequently, it is also appropriate to offer patients both verbal and written instructions as to likely possible symptoms and the appropriate action that needs to be taken. This is common practice in haematology departments, e.g. for postsplenectomy advice and for complications following antineoplastic and anticoagulant therapy. Such written protocols should be encouraged and extended, for example, to patients commencing antithyroid drugs.
5.5 Improved Reporting, Collation and Evaluation of Suspected Severe Adverse Drug Reactions
Improvements are also required in the quality and quantity of ADR reporting, the collation of such material, the risk-benefit analysis of such events and the subsequent delivery of appropriate information to prescribers. Journal editors and directors of ADR agencies should be encouraged to adopt operational criteria for ranking the probability of causation in suspected ADRs and to promote the advantages of the benefits generated by the revolution in information technology and communications.
© Adis International Limited. All rights reserved.
Patton & Duffull
Information contained within global networks are now accessible via modem links to personal computers, and competition between international telecommunications companies is resulting in decreasing prices for such access. Interested parties such as central ADR authorities could commission regular peer review articles on the evidence linking specific drugs with ADRs, which could then be placed on file within the global network. Once on file, such information could then be available on demand on a 24-hour basis, thereby greatly improving the accuracy and speed of information back to individual clinicians. Such a system may seem Utopian, but with appropriate vision, resources and management skills it could become reality in the not too distant future. Many problems in these areas have been identified (lR Edwards, personal communication), but the further development of such systems is to be encouraged.
6. Conclusion
Although progress has been made in the recognition and management of drug-induced haematological dyscrasias, many ofthe problems identified in the concluding remarks of a previous review remain valid today)7] Of these, the limitations within the available data on drugs and blood dyscrasias remain the most important, and further improvements in the reporting mechanisms for ADRs, as outlined in section 5.5, are to be encouraged. The information generated can be used to devise avoidance strategies to limit the impact of ADRs. The management and avoidance guidelines presented in this article should enable further progress to be made. These guidelines can be adapted to meet local circumstances and should prove suitable subjects for audit of their effectiveness.
Acknowledgements
We are grateful to Evan Begg for helpful comments on this article, and to Helena Le Gallais for typing the manuscript.
Drug Safety 11 (6) 1994
Drug-Induced Haematological Abnormalities
References I. Steel K, Gertman PM, Crescenzi C, et al. Iatrogenic i11ness on
a general medical service at a university hospital. N Engl 1 Med 1981; 304: 638-42
2. Lakshmanan ML, Hershey CO, Breslau D. Hospital admissions caused by iatrogenic disease. Arch Intern Med 1986; 146: 1931-4
3. Faich GA. Adverse-drug-reaction monitoring. N Engl 1 Med 1986; 314: 1589-92
4. Bottiger LE, Furhoff AK, Holberg L. Fatal reactions due to drugs. A study of 10 years material from the Swedish Adverse Drug Reaction Committee. Acta Med Scand 1979; 205: 457-61
5. Young GAR. Drug-induced haematological disorders. Curr Ther 1984; 25: 61-9
6. Vincent Pc. Drug-induced aplastic anaemia and agranulocytosis. Drugs 1986; 31: 52-63
7. Heimpel H. Drug-induced agranulocytosis. Med Toxicol1988; 3: 449-62
8. Dukes MNG. The importance of adverse reactions in drug regulation. Drug Saf 1990; 5: 3-6
9. Arneborn P, Palmblad 1. Drug-induced neutropenia: a survey for Stockholm 1973-1978. Acta Med Scand 1982; 212: 289-92
10. Keith MR, Bellanger-McCleery RA, Fuchs lE. Multidisciplinary program for detecting and evaluating adverse drug reactions. Am 1 Hosp Pharm 1989; 46: 1809-12
II. Kramer MS, Leventhal 1M, Hutchinson TA, et al. An algorithm for the operational assessment of adverse drug reactions. lAMA 1979; 242: 623-32
12. Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther 1981; 30: 239-45
13. Kaufman DK, Kelly IP, Levy M, et al. The drug etiology of agranulocytosis and aplastic anaemia. Monographs in epidemiology and biostatistics. No 18. New York: Oxford University Press, 1991
14. Edwards IR, Lindquist M, Wiholm B-E, et al. Quality criteria for early signals of possible adverse drug reactions. Lancet 1990;336: 156-8
15. Patton WN, Holyoake TL, Yates 1M, et al. Accelerated recovery from drug-induced agranulocytosis following G-CSF therapy. Br 1 Haematol 1992; 80: 564-5
16. Schlesselman 11. Case control studies: design, conduct, analysis. Monographs in epidemiology and biostatistics. No 2. New York: Oxford University Press, 1982
17. Kramer MS, Lane DA, Hutchinson TA. Analgesic use, blood dyscrasias and case control pharmacoepidemiology: a critique of the International Agranulocytosis and Aplastic Anaemia Study. 1 Chron Dis 1987; 40: 1073-81
18. International Agranulocytosis and Aplastic Anaemia Study (IAAAS). The design of a study of the drug etiology of agranulocytosis and aplastic anaemia. Eur 1 Clin Pharmacol1983; 24: 833-6
19. The International Agranulocytosis and Aplastic Anemia Study. Risks of agranulocytosis and aplastic anaemia: a first report of their relation to drug use with special reference to analgesics. lAMA 1986; 256: 1749-57
20. International Agranulocytosis and Aplastic Anaemia Study. Risk of agranulocytosis and aplastic anaemia in relation to use of antithyroid drugs. BMl 1988; 297: 262-5
© Adis International Limited. All rights reserved.
459
21. A report from the International Agranulocytosis and Aplastic Anemia Study. Anti-infective drug use in relation to the risk of agranulocytosis and aplastic anemia. Arch Intern Med 1989; 149: 1036-40
22. Kelly IP, Kaufman DW, Shapiro S. Risks of agranulocytosis and aplastic anemia in relation to the use of cardiovascular drugs. Clin Pharmacol Ther 1991; 49: 330-41
23. Committee on Safety of Medicines. Neutropenia and agranulocytosis with carbimazole - may be fatal if the drug is not withdrawn promptly. CUff Probl 1991; 32: 2
24. Bottiger LE, Westerholm B. Drug-induced blood dyscrasias in Sweden. BMl 1973; 3: 339-43
25. Arneborn P, Palmblad J. Drug-induced neutropenia in the Stockholm region 1971-1975: frequency and causes. Acta Med Scand 1978; 204: 283-6
26. Arneborn P, Palmblad J. Drug-induced neutropenias in the Stockholm region 1976-1977. Acta Med Scand 1979; 206: 241-3
27. Paiva IP, Mustala 00. Drug-induced agranulocytosis II. The role of medication in a fatal outcome. I Adults. Acta Med Scand 1972; 191: 121-4
28. Inman MHW. Study offatal bone marrow depression with special reference to phenylbutazone and oxyphenbutazone. BMl 1977; 6: 1500-5
29. Pisciotta AV, Ebbe S, Lennon EJ, et al. Agranulocytosis following administration of phenothiazine derivatives. Am 1 Med 1958; 25: 210-23
30. Pretty HM, Gosselin G, Colpron G, et al. Agranulocytosis: a report of 30 cases. Can Med Assoc J 1965; 93: 1058-64
31. Julia A, 010na M, Bueno 1, et al. Drug-induced agranulocytosis: prognostic factors in a series of 168 episodes. Br 1 Haematol 1991; 79: 366-71
32. Mary JY, Baumelou E, Guiget M, et al. Epidemiology of aplastic anaemia in France: a prospective multicentre study. Blood 1990; 75: 1646-53
33. Issaragrisil S, Sriratanasatavorn C, Piankijagum A, et al. Incidence of aplastic anaemia in Bangkok. The Aplastic Anaemia Study Group. Blood 1991; 77: 2166-8
34. Szklo M, Sensenbrenner L, Markowitz 1, et al. Incidence of aplastic anemia in metropolitan Baltimore: a populationbased study. Blood 1985; 66: 115-9
35. Linet MS, McCaffrey LD, Morgan WF, et al. Incidence of aplastic anemia in a three county area in South Carolina. Cancer Res 1986; 46: 426-9
36. Clausen N. A population study of severe aplastic anemia in children: incidence, etiology and course. Acta Paediatr Scand 1986; 75: 58-63
37. Davies SM, Walker DJ. Aplastic anaemia in the northern region 1971-1978 and follow-up of long term survivors. Clin Lab Haematol 1986; 8: 307-13
38. Cartwright RA, McKinney PA, Wi11iams L, et al. Aplastic anaemia incidence in parts of the United Kingdom in 1985. Leuk Res 1988; 12: 459-63
39. Aggio Me, Alverez RV, Bartomioli MA, et al. Incidence and etiology of aplastic anemia in a defined population of Argentina (1966-1977). Medicina (B Aires) 1988; 48: 231-3
40. Irvine AE, French A, Daly A, et al. Drug-induced neutropenia due to direct effects on CFU-C: ten years of culture experience. Eur 1 Haematol 1994; 52: 21-7
41. Pisciotta AY. Drug-induced agranulocytosis. Peripheral destruction of polymorphonuclear leukocytes and their marrow precursors. Blood Rev 1990; 4: 226-37
Drug Safety 11 (6) 1994
460
42. Stroncek OF. Drug-induced immune neutropenia. Transfus Med Rev 1993; 7: 268-74
43. McFarland JG. Laboratory investigation of drug-induced immune thrombocytopenias. Transfus Med Rev 1993; 7: 275-87
44. Garratty G, Petz LD. Drug-induced immune hemolytic anemia. Am J Med 1975; 58: 398-407
45. Williams OM. Pancytopenia, aplastic anaemia and pure red cell aplasia. In: Lee GR, Bithell TC, Foerster J, et aI., editors. Wintrobe's clinical haematology. Philadelphia: Lea and Febiger, 1993: 911-43
46. Champlin RE. Aplastic anaemia. In: Bick RL, editor. Hematology, clinical and laboratory practice. St Louis: Mosby, 1993: 471-94
47. Athens JW. Neutropenia. In: Lee GR, Bithell TC, Foerster J, et aI., editors. Wintrobe's clinical haematology. Philadelphia: Lea and Febiger, 1993: 1589-612
48. Foerster J. Autoimmune hemolytic anaemias. In: Lee GR, Bithell TC, Foerster J, et aI., editors. Wintrobe's clinical haematology. Philadelphia: Lea and Febiger, 1993: 1170-96
49. Lee RG. Acquired hemolytic anaemias resulting from direct effects of infectious, chemical or physical agents. In: Lee GR, Bithell TC, Foerster J, et aI., editors. Wintrobe's clinical haematology. Philadelphia: Lea and Febiger, 1993: II 97-2 10
50. Bithell TC. Thrombocytopenia caused by immunological platelet destroction: idiopathic thrombocytopenic purpura (ITP), drug-induced thrombocytopenia and miscellaneous forms. In: Lee GR, Bithell TC, Foerster J, et al., editors. Wintrobe's clinical haematology. Philadelphia: Lea and Febiger, 1993: 1329-55
51. Bick RL. Quantitative platelet defects. In: Bick RL, editor. Hematology, clinical and laboratory practice. St Louis: Mosby, 1993: 1337-68
52. Chong BH. Drug-induced immune thrombocytopenia. Platelets 1991; 2: 173-81
53. Committee on Safety of Medicines. Drug-induced neutropenia and agranulocytosis. CUIT Prob11993; 19: 10-1
54. Baum CM, Uchida N, Peault B, et al. Isolation and characterization of hematopoietic progenitor and stem cells. In: Forman ST, Blume KG, Thomas ED, editors. Bone marrow transplantation. Boston: Blackwell Scientific Publications, 1994: 53-71
55. Gordon MY. Human haematopoietic stem cell assays. Blood Rev 1993; 7: 190-7
56. Clark SC, Kamen R. The human hematopoietic colony-stimulating factors. Science 1987; 236: 1229-37
57. Nathan DG. Regulation of hematopoiesis. Pediatr Res 1990; 27: 423-43
58. Lekbakula A, Swasdikul D. Drug-induced agranulocytosis: experience in two university hospitals. J Med Assoc Thai 1991; 74: 121-30
59. Treleaven T, Barrett J. Drugs and the bone marrow. Br J Hosp Med 1990; 44: 245-50
60. Ruvidic R, Jelic S. Haematological aspects of drug-induced agranulocytosis. Scand J HaematoI1972; 9: 18-27
61. Muroi K, Ito K, Sasaki R, et aI. Treatment of drug-induced agranulocytosis with granulocyte colony-stimulating factor. Lancet 1989; 2: 55
62. Heinrich B, Gross M, Goebel FD. Methimazole-induced agranulocytosis and granulocyte colony-stimulating factor. Ann Intern Med 1989; Ill: 621-2
63. Delannoy A, Gehenot M. Colony-stimulating factor and druginduced agranulocytosis. Ann Intern Med 1989; 110: 942-3
© Adis Intemational Umited. All rights reserved.
Patton & Duffull
64. Sonada Y, Yashige H, Fujii H, et al. Treatment of idiopathic neutropenia in the elderly with recombinant human granulocyte colony-stimulating factor. Acta Haematol1991; 85: 146-52
65. Nand S, Bayer R, Prinz RA, et al. Granulocyte-macrophage colony stimulating factor for the treatment of drug induced agranulocytosis. Am J Hematol 1991; 37: 267-9
66. Weide R, Koppler H, Heymanns J, et al. Successful treatment of clozapine-induced agranUlocytosis with granulocyte-colony stimulating factor. Br J Haematol1992; 80: 557-9
67. Yokoyama K, SatoT, Nakijima S, etal. Successful treatment of methimazole-induced agranUlocytosis by granulocyte colony-stimulating factor. Am J Hematol 1992; 40: 76-7
68. Delannoy A. GM-CSF therapy for drug induced agranulocytosis. J Intern Med 1992; 231: 269-71
69. Kendra JR, Rugman FP, Flaherty TA, et al. First use ofG-CSF in chlorpromazine-induced agranUlocytosis: a report of two cases. Postgrad Med J 1993; 69: 885-7
70. Patton WN, Bradford CR, Cappellari G, et al. Use of colony stimulating factors for the treatment of drug-induced agranulocytosis [letter]. Br J Haematol1993; 182-5
71. Mani S, Barry M, Concato J. Granulocyte-colony stimulating factor therapy in drug-induced agranulocytosis. Arch Intern Med 1993; 153: 2500-1
72. Kurzrock R, Talpaz M, Gutterman JU. Very low doses ofGMCSF administered alone or with erythropoietin in aplastic anaemia. Am J Med 1992; 93: 41-8
73. Petz LD. Drug-induced autoimmune hemolytic anemia. Transfus Med Rev 1993; 7: 242-54
74. Shulman NR, Jordan JV. Platelet immunology. In: Colman RW, Hirsh J, Marder VJ, et aI., editors. Hemostasis and thrombosis. 2nd ed. Philadelphia: Lippincott, 1987: 452-529
75. Deren B, Masi R, Weksler M, et al. Gold-associated thrombocytopenia. Arch Intern Med 1974; 134: 1012-5
76. Coblyn JS, Weinblatt M, Holdsworth D, et al. Gold-induced thrombocytopenia. A clinical and immunogenetic study of twenty-three patients. Ann Intern Med 1981; 95: 178-81
77. Pisciotta AV, Kaldahl J. Studies on agranulocytosis IV. Effects of chlorpromazine on nucleic acid synthesis of bone marrow cells in vitro. Blood 1962; 20: 364-76
78. Pisciotta AV, Pawlowski N, Peterson L, et al. Studies on agranulocytosis IX. A biochemical defect in chlorpromazine sensitive marrow cells. J Lab Clin Med 1971; 78: 435-48
79. Breckenridge A. Adverse effects of ACE inhibitors and the quality of life. In: MacGregor GA, Sever PS, editors. Current advances in ACE inhibition. Proceedings of an International Symposium on ACE inhibition, Feb 14-17 1989, London. Edinburgh: Churchill Livingstone, 1989: 123-7
80. Cooper RA. Captopril-associated neutropenia. Arch Intern Med 1983; 143: 659-60
81. Irvin JD, Viau JM. Safety profiles of the angiotensin-converting enzyme inhibitors captopril and enalapril. Am J Med 1986; 81 Suppl. 4C: 46-50
82. D Bianco R. Adverse reactions with ACE inhibitors. New Ethicals 1986; 23: 181-208
83. Neftel KA, Hauser Sp, Muller MR. Inhibition of granulopoiesis in vivo and in vitro by beta-Iactam antibiotics. J Infect Dis 1985; 152: 90-8
84. Singh N, Yu VL, Mieles LA, et al. ~-Lactam antibiotic-induced leukopenia in severe hepatic dysfunction: risk factors and implications for dosing in patients with liver disease. Am J Med 1993; 94: 251-6
Drug Safety 11 (6) 1994
Drug-Induced Haematological Abnormalities
85. Ross MP, Allen-Webb EM, Pappas JB, et al. Amrinone-associated thrombocytopenia: pharmacokinetic analysis. Clin Pharmacol Ther 1993; 53: 661-7
86. Cunningham JL, Leyland MJ, Delamore IW, et al. Acetanilide oxidation in phenylbutazone-associated hypoplastic anaemia. BMJ 1974; 3: 313-7
87. Gerson SL, Arce C, Meltzer HY. N-desmethylclozapine: a c10zapine metabolite that suppresses haemopoiesis. Br J Haematol 1994; 86: 555-61
88. Gerson SL, Lieberman JA, Friedenberg WR, et al. Polypharmacy in fatal clozapine-associated agranulocytosis. Lancet 1991;338:262
89. Gordon-Smith EC. Drug-induced oxidative haemolysis. Clin Haematol1980; 9: 557-85
90. British Medical Association and Royal Pharmaceutical Society of Great Britain. Antiprotozoal drugs: primaquine. In: Prasad AB, editor. British National Formulary No. 26. London: Pharmaceutical Press, 1993: 239
91. Uetrecht J. Mechanism of hypersensitivity reactions: proposed involvement of reactive metabolites generated by activated leukocytes. Trends Pharmacol Sci 1989; 10: 463-7
92. Bodey GP, Buckley M, Sathe YS, et al. Quantitative relationships between circulating leukocytes and infection in patients with acute leukaemia. Ann Intern Med 1966; 64: 328-40
93. Dale DC. Neutrophil disorders: benign quantitative abnormalities of neutrophils; neutropenia. In: Williams WJ, Beutler E, Erslev AJ, et aI., editors. Haematology. 4th ed. New York: McGraw Hill, 1990: 807-16
94. Crawford J, Ozer H, Johnson 0, et al. Reduction by granulocyte colony-stimulating factor of fever and neutropenia induced by chemotherapy in patients with small-cell lung cancer. New EnglJMed 1991;325: 164-70
95. Nemunaitis J. Granulocyte-macrophage-colony stimulating factor: a review from preclinical development to clinical application. Transfusion 1993; 33: 70-83
96. Camitta BM, Storb R, Thomas ED. Aplastic anaemia. Pathogenesis, diagnosis, treatment and prognosis. N Engl J Med 1982;306:645-52,712-8
97. Kay AGL. Myelotoxicity of gold. BMJ 1976; I: 1266-8 98. Patton WN, Murray JA, Blake DR, et al. How should we mon
itor gold therapy? Lancet 1988; I: 581-2 99. Bower JS. Aplastic anaemia due to gold therapy unsuccessfully
treated with BAL. N C Med J 1952; 13: 340 100. Gluckman E, Horowitz MH, Champlin RE, et al. Bone marrow
transplantation for severe aplastic anaemia: influence of conditioning and graft-versus-host disease prophylaxis regimens on outcome. Blood 1992; 79: 269-75
10 I. Storb R. Bone marrow transplantation for aplastic anemia. In: Forman SJ, Blume KG, Thomas ED, editors. Bone marrow transplantation. Boston: Blackwell Scientific, 1994: 583-94
102. French Co-operative Group for the Study of Aplastic and Refractory Anaemias. Androgen therapy in aplastic anaemia: a comparative study of high and low doses of 4 different androgens. Scand J Haematol 1986; 36: 346-52
103. Najean Y. Androgen therapy of aplastic anaemia in a prospective study of 352 cases. Scand J Haematol 1979; 22: 342-56
104. Bacigalupo A, Chaple M, Hows J, et al. Treatment of aplastic anaemia (AA) with antilymphocyte globulin (ALG) and methylprednisolone (MPred) with or without androgens: a randomized trial from the EBMT SAA working party. Br J Haematol 1993; 83: 145-51
© Adis International Limited. All rtghts reserved.
461
105. Doney K, Storb R, Buckner CD, et al. Treatment of gold-induced aplastic anemia with immunosuppressive therapy. Br J Haematol 1988; 68: 469-72
106. Hansen RM, Csuka ME, McCarty OJ, et al. Gold-induced aplastic anaemia: complete response to corticosteroids, plasma pheresis and N-acetyIcysteine infusion. J Rheurnatol 1985; 12: 794-7
107. Ray JB, Brereton WF, Nullet FR. Intravenous immune globulin for the treatment of presumed quinidine-induced thrombocytopenia. Ann Pharmacother 1990; 24: 693-5
108. Freiman JP. Fatal quinine-induced thrombocytopenia. Ann Intern Med 1990; 112: 308-9
109. Spearing RL, Hickton CM, Sizeland P, et al. Quinine-induced disseminated intravascular coagulation. Lancet 1990; 336: 1535-7
110. Gottschall JL, Elliot W, Lianos E, et al. Quinine-induced immune thrombocytopenia associated with hemolytic uremic syndrome: a new clinical entity. Blood 1991; 77: 306-10
III. Gruel Y, Lang M, Darnige L, et al. Fatal effect of re-exposure to heparin after previous heparin-associated thrombocytopenia and thrombosis. Lancet 1990; 336: 1077-8
112. King OJ, Kelton JG. Heparin-associated thrombocytopenia. Ann Intern Med 1984; 100: 535-40
113. Warkentin TE, Kelton JG. Heparin-induced thrombocytopenia. Annu Rev Med 1989; 40: 31-44
114. Laster JL, Nichols WK, Silver D. Thrombocytopenia associated with heparin-coated catheters in patients with heparin associated antibodies. Arch Intern Med 1989; 149: 2285-7
115. Sheridan 0, Carter C, Kelton JG. A diagnostic test for heparininduced thrombocytopenia. Blood 1986; 67: 27-30
116. Warkentin TE, Hayward CPM, Smith CM, et al. Determinants of donor platelet variability when testing for heparin-induced thrombocytopenia. J Lab C1in Med 1992; 120: 371-9
117. Keeling OM, Richards EM, Baglin TP. Platelet aggregation in response to four low molecular weight heparins and the heparinoid Org (10172) in patients with heparin-induced thrombocytopenia. Br J Haematol 1994; 86: 425-6
118. Chong BH, Ismail F, Cade J, et al. Heparin induced thrombocytopenia: studies with a low molecular weight heparinoid, Org 10172. Blood 1989; 73: 1592-6
119. Ortel TL, Gockerman JP, CaliffRM, et al. Parenteral anticoagulation with the heparinoid Lomoparin (Org 10172) in patients with heparin induced thrombocytopenia and thrombosis. Thromb Hemost 1992; 67: 292-6
120. Demers C, Ginsberg JS, Brill-Edwards P, et al. Rapid anticoagulation using ancrod for heparin-induced thrombocytopenia. Blood 1991; 78: 2194-7
121. Warkentin TE, Kelton JG. Heparin-induced thrombocytopenia. Prog Hemost Thromb 1991; 10: 1-34
122. Worlledge SM. Immune drug-induced hemolytic anaemias. Semin Hematol1969; 6: 181-200
123. Garratty G, Postoway N, Schwellenbach J, et al. A fatal case of ceftriaxone (Rocephin)-induced hemolytic anaemia associated with intravascular immune hemolysis. Transfusion 1991; 31: 176-9
124. Garratty G, Nance S, Lloyd M, et al. Fatal immune hemolytic anaemia due to cefotetan. Transfusion 1992; 32: 269-71
125. Johnson FP, Hamilton HE, Liesch MR. Immune hemolytic anaemia associated with sulindac. Arch Intern Med 1985; 145: 1515-6
Drug Safety 11 (6) 1994
462
126. Tofani 0, Mazzoli M, Landini G, et al. Fatal acute immune haemolytic anaemia caused by nalidixic acid. BMJ 1982; 285: 936-7
127. Idanpaan-Heikkila J, Alhava E, Olkinura M. Agranulocytosis during treatment with c1ozapine. Eur J Clin Pharmacol 1977; 11: 193-8
128. Alvir JM, Lieberman JA, Safferman AZ, et al. Clozapine-induced agranulocytosis. Incidence and risk factors in the United States. N Engl J Med 1993; 329: 162-7
129. Walker 10, Walker JJ, Colvin BT, et aI. Investigation and management of haemorrhagic disorders in pregnancy. J Clin Pathol 1994; 47: 100-8
130. British Medical Association and Royal Pharmaceutical Society of Great Britain. Antibacterial drugs: chloramphenicol. In: Prasad AB, editor. British National Formulary No. 26. London: Pharmaceutical Press, 1993: 219
© Adis Intemational Limited. All rights reserved.
Patton & Duffull
131. British Medical Association and Royal Pharmaceutical Society of Great Britain. Non-steroidal anti-inflammatory drugs (NSAID's): indomethacin. In: Prasad AB, editor. British National Formulatary No 26. London: Pharmaceutical Press, 1993:353,356
132. Hirsch SR, Purl BK. Clozapine: progress in treating refractory schizophrenia [editorial). BMJ 1993; 306: 1427-8
133. Clozaril Patient Monitoring Service. Sandoz Pharmaceuticals, FrimIey, Camberley, Surrey, UK
Correspondence and reprints: Dr W Nigel Patton, Department of Haematology, Canterbury Health Laboratories, PO Box 151, Christchurch, New Zealand.
Drug Safely 11 (6) 1994





























