Embed Size (px)
Citation preview

n CASE HISTORY
12 z Prescriber 19 March 2015 prescriber.co.uk
A56-year-old man presented to thedermatology department with a two-
month history of an itchy rash with wide-spread vesicular erythematous plaquesand some bullae. The patient had a pastmedical history of squamous cell lungcancer, which was in remission, and had been diagnosed with epidermolysisbullosa simplex (EBS, a geneticallyacquired blistering condition) as a child.His EBS had manifested itself with minorblistering at sites of trauma, such as theheels and elbows. His medications wereramipril 5mg once daily and simvastatin40mg once nightly. There were no knowndrug allergies.
The diagnosis was initially unclear,with a working differential of either dis-
coid eczema or an immunobullous disor-der such as linear IgA disease. A biopsywas performed, with tissue samples sentfor histology and immunofluorescence.While awaiting the results, the patientwas given a tapering course of oral pred-nisolone, beginning at 40mg once daily.The biopsy suggested an eczematous pic-ture, with a blistering pattern consistentwith EBS. Immunofluorescence was neg-ative. Correlating the histological findingswith the clinical presentation, the diagno-sis of discoid eczema complicated by EBSblistering was made.
After a month of oral prednisoloneon a tapering regimen, he remained on5mg prednisolone once daily for two tothree weeks, with a super potent topicalsteroid ointment (clobetasol propionate0.05 per cent) on the itchy red areasonce daily for 10–14 day bursts asneeded. He was advised to use soapsubstitutes and emollients to maintainthe integrity of the skin barrier and wasgiven open follow up.
Discoid (nummular) eczema presentsusually in middle age and is characterisedby itchy coin-shaped lesions with a well-demarcated border.1 Unlike dermatophyteinfections, with which it may be confused,the rash does not tend to be annular,lacking a central clearing. Psoriasis isamong the differential diagnoses, buttends to be less itchy and has loose silverscale, rather than adherent crust.Psoriasis may also be associated withnail, scalp or joint changes. Discoideczema can be very florid, with livid erythema, vesicles, crusting and oozing.1
For this reason it can be mistaken for cel-lulitis or severe impetigo, leading to treat-ment with oral antibiotics. However,although the eczema may become super-infected, it will not resolve with antibioticsalone, and requires potent topicalsteroids in addition.2 Over time thelesions tend to become dry and scaly.1
There may be multiple lesions visible atdifferent stages of evolution.
Identifying and treating a florid vesicular rash
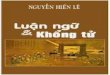
The erythematous, vesicular discoid lesions on the lower limbs

Eczema l CASE HISTORY n
Prescriber 19 March 2015 z 13prescriber.co.uk
Discoid eczema is usually endo genousin aetiology, although patients will oftenseek an allergic cause. However, as withother forms of eczema, patch tests will bepositive in a minority, and relevant insome.3 Swabs for micrsocopy, culture andsensitivity (MC&S) will help direct anti -microbial therapy if needed; nasal swabsmay identify staphylococcal carriage,which can be the source of infection. If thediagnosis is in doubt, skin scrapings formycology should be taken and a biopsyconsidered.2 The advice of a dermatologistshould be sought if there is diagnosticuncertainty or resistant disease.
As with any eczema, irritant avoid-ance (including the use of soap substi-tutes) and barrier repair with emollients,is important. To maximise adherence,patients should be given the choice of theemollient they wish to use.4 The key treat-ment is with potent topical corticosteroids(see Table 1). Mild and moderate potencytopical steroids do not tend to be effectivein discoid eczema. As with all topical cor-ticosteroids, patients should receivecounselling regarding side-effects andappropriate application doses (in termsof fingertip units).5
Steroid/antibiotic combination creamscan be helpful in discoid eczema that isfrequently infected, eg betamethasonevalerate 0.1 per cent plus fucidic acid 2per cent (Fucibet), but care should betaken in areas of fucidic acid resistance.Recalcitrant disease may require systemictherapy with oral prednisolone followed bya steroid-sparing immunosuppressant,such as azathioprine. Anti histamines canbe prescribed to help reduce the itch,although in practice they are rarely effec-tive. If there are signs of cellulitis or lym-phangitis the patient should be treated
with oral antibiotics according to local for-mulary guidelines (see note above regard-ing MC&S). If the history suggests possiblecontact allergy then the patient should bereferred for patch testing.
References1. Burton JL, Holden CA. Pruritus. In: ChampionRH et al. eds. Textbook of Dermatology. 6th ed.Oxford: Blackwell 1998, Pg 646–7.2. Burge S, et al. Oxford handbook of medicaldermatology. 1st edition. Oxford: OxfordUniversity Press 2010.3. Bonamonte D, et al. Nummular eczema andcontact allergy: a retrospective study.
Dermatitis 2012;23:153–7.4. Moncrieff G, et al. Use of emollients in dry-skin conditions: consensus statement. Clin ExpDermatol 2013;38:231–8.5. Royal Pharmaceutical Society of GreatBritain. British National Formulary 68.September 2014.
Declaration of interestsNone to declare.
Dr William Hunt is an FY2 doctor and Dr Emily McGrath is consultant dermatologist at the Royal Devon and Exeter Hospital
Table 1. Steroids for use in discoid eczema in adults5
Strength Drug Price Dose
Potent Beclometasone dipro-pionate 0.025%
30g tube costs£68.00 (creamand ointment)
Thin applicationonce to twicedaily, 7 days
Betamethasone valer-ate 0.1%
30g tube costs£1.43 (cream andointment)
Thin applicationonce to twicedaily, 7 days
Hydrocortisonebutyrate 0.1%
30g tube costs£1.60(cream)
Thin applicationonce to twicedaily, 7 days
Mometasone furoate0.1%
30g tube costs£4.09 cream,£3.36 ointment
Thin applicationonce daily, 7 days
Potent withantimicrobials
Betamethasone asvalerate 0.1%/fusidicacid 2%
30g tube costs£6.38 (Fucibetcream)
Thin applicationonce daily, 7 days
Very potent Clobetasol propionate0.05%(Dermovate)
30g tube costs£2.69 (cream andointment)
Thin applicationonce to twicedaily, 7 days. Max50g/week
If you have any issues you would like to air with your colleagues or comments on articlespublished in Prescriber, the editor would be pleased to receive them and, if appropriate,publish them on our forum page. Please send your comments to:
The editor, Prescriber, The Atrium, Southern Gate, Chichester, West Sussex PO19 8SQ, or e-mail to [email protected]
Share your views