-
Original ResearchPediatric Otolaryngology
Identification of Hearing Loss in PediatricPatients with Down
Syndrome
OtolaryngologyHead and Neck Surgery146(1) 135140 American
Academy ofOtolaryngologyHead and NeckSurgery Foundation
2012Reprints and permission:sagepub.com/journalsPermissions.navDOI:
10.1177/0194599811425156http://otojournal.org
Albert H. Park, MD1, Matt A. Wilson, MD1, Paul T.
Stevens2,Richard Harward, AuD3, and Nancy Hohler, AuD4
No sponsorships or competing interests have been disclosed for
this article.
Abstract
Objective. To determine the type of hearing loss, incidence
ofthe lost to follow-up rate, and the time to diagnose
sensori-neural hearing loss (SNHL) in children with Down syn-drome
(DS) identified from a statewide database.
Study Design. Case series with chart review.
Setting. Pediatric referral center.
Subjects and Methods. Three hundred forty-four patientswith DS
born in Utah between January 2002 and December2006 were identified
using the Utah Department of HealthsNewborn Hearing Screening
database and birth defectsregistry.
Results. Three hundred thirty-two patients were included inthe
study. Eighty-seven infants (26.2%) did not pass theirnewborn
hearing screening (NBS). Thirty-three of thesechildren (37.9%) had
a conductive hearing loss attributed toserous otitis media. Five
infants had SNHL; 3 children werediagnosed with a mixed hearing
loss (MHL). The averagetime to diagnose a sensorineural hearing
loss was 485 6601 days. One child who passed his NBS was
subsequentlyfound to have an SNHL. More than 43% of the
newbornswith DS who passed their NBS developed a conductivehearing
loss requiring insertion of ventilation tubes. Eighty-four percent
of newborns with DS who did not undergoNBS did not have any
apparent subsequent audiologictesting.
Conclusion. Patients with DS present with a relatively
highincidence of conductive hearing loss, MHL, and SNHL and ahigher
lost to follow-up rate compared to patients withoutDS. The authors
were not able to diagnose SNHL withinthe 90-day period recommended
by the Joint Committeeon Infant Hearing.
Keywords
newborn hearing screening, Down syndrome, sensorineuralhearing
loss
Received September 20, 2010; revised August 25, 2011;
accepted
September 9, 2011.
Down syndrome (DS) is estimated to occur in 1 in
700 to 1 in 1000 live births, making it one of the
most common genetic syndromes.1 Common mani-
festations of this syndrome include external ear canal
steno-
sis, chronic ear disease, and hearing loss, conditions many
otolaryngologists, audiologists, and primary care physicians
regularly face.2 Stenotic ear canals occur in up to 50% of
newborns with DS, making the diagnosis of otitis media
with effusion challenging.3 Several studies have cited the
increased incidence of chronic ear disease in this popula-
tion.3,4 Estimates of hearing loss range from 38% to 78% of
all DS patients.5-9
Much of this information had been presented before the
advent of universal newborn hearing screening. Because
many of these cited articles reporting the relatively high
incidence of conductive and sensorineural hearing loss
(SNHL) have been in the literature for several decades, it
would be informative to determine whether universal new-
born screening programs have been successful in diagnosing
these patients expeditiously. The purpose of this study is
to
determine whether a statewide newborn screening program
provides identification of sensorineural hearing loss by 3
months of age, the distribution of hearing loss type in this
program, and the lost to follow-up rate. We hypothesize that
the time to diagnosis of DS infants with sensorineural hear-
ing loss will not be within the guidelines mandated by the
Joint Committee on Infant Hearing (JCIH) and that the inci-
dence of conductive hearing loss, SNHL, mixed hearing
loss, and indeterminant loss, as well as the lost to
follow-up
rate, is high.10
1Division of OtolaryngologyHead and Neck Surgery, University of
Utah,
Salt Lake City, Utah, USA2University of Utah School of Medicine,
Salt Lake City, Utah, USA3Utah Department of Health, Salt Lake
City, Utah, USA4Audiology, Primary Childrens Medical Center, Salt
Lake City, Utah, USA
This article was presented at the 2010 AAO-HNSF Annual Meeting
& OTO
EXPO; September 26-29, 2010; Boston, Massachusetts.
Corresponding Author:
Albert H. Park, MD, Division of OtolaryngologyHead and Neck
Surgery,
University of Utah, 50 North Medical Drive, 3C 120, Salt Lake
City, UT
84132, USA
Email: [email protected]
at IMSS on May 26, 2015oto.sagepub.comDownloaded from
-
Methods
Subjects
Three hundred forty-four newborns with DS born in Utah
between 2002 and 2006 were identified using the Utah Birth
Defects Registry. Several outcome measures were determined
using the Utah Department of Health Hi*Track
informationmanagement system and the Intermountain Healthcare
(IHC)
electronic medical record system. The Utah Newborn
Hearing Screening Program has been considered a very suc-
cessful initiative, with more than 97% of the 53,080 new-
borns delivered being screened for 2010 with an overall
initial state pass rate of 95.8%. The Utah Department of
Health is responsible for data collection and management,
follow-up, and technical assistance for the state screening
program. It helped establish several audiological diagnostic
sites throughout the state that can provide complete
diagnos-
tic services to newborns and infants. The IHC is the largest
health care provider in the Intermountain West. More than 20
hospitals, including the only childrens hospital in Utah,
Primary Childrens Medical Center, are owned by the IHC. It
provides insurance to 19% of all Utah residents.
Outcome measures included newborn hearing screening
results, otoscopic examinations, behavioral audiometry, tym-
panometry/immitance, otoacoustic emissions, auditory brain-
stem response (ABR) testing thresholds, magnetic resonance
and computed tomography temporal bone imaging, time to
diagnosis of hearing loss, time to hearing loss treatment,
and
surgical treatment. Institutional review board (IRB)
approval
was obtained from the Utah Department of Health,
University of Utah, and Primary Childrens Medical Center.
The measures of hearing were categorized as normal hear-
ing, conductive hearing loss, sensorineural hearing loss,
mixed hearing loss, indeterminant hearing result, and lost
to
follow-up. Normal hearing results included behavioral
thresh-
olds at 500, 1000, 2000, and 4000 Hz better than 20 dB or
ABR thresholds better than 30 dB. Conductive hearing loss
was confirmed with the presence of an air-bone (AB) gap
greater than 10 dB based on ABR or behavior testing.
Sensorineural hearing loss was defined as a greater than a
20-dB threshold on behavioral testing at 500, 1000, 2000,
and 4000 Hz or greater than 30-dB thresholds on ABR click
and/or tone burst thresholds with no AB gap present. Mixed
hearing loss included a combination of sensorineural and
con-
ductive hearing loss. Indeterminant hearing loss included
sub-
jects whose hearing loss type was not determined (eg, lack
of
bone conduction testing). Lost to follow-up patients were
those whose audiologic and otoscopic testing could not be
found in the medical records (or in the Hi*Track database).
ResultsNewborn Hearing Screening Data for DS and Non-DSNewborns
in Utah
Of 258,289 children born in the state of Utah between 2002
and 2006, 344 (0.13%) had Down syndrome, including 199
(57.8%) males and 146 females (42.2%). Twelve (3.5%)
died during the newborn period, and no additional data were
collected on these subjects. Three hundred thirty-two chil-
dren had otoscopic and audiologic data available for analy-
sis. Two hundred thirty-two newborns (69.9%) with DS
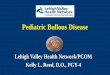
passed their newborn hearing screening (NBS; Figure 1).This
percentage is lower than the 92.8% of all infants
(234,545) who passed during this period. Eighty-seven
(26%) failed their screening, and 13 (3.9%) did not undergo
screening. The percentage of all infants not screened was
less than the DS group at 1.8% (4741 infants).
Distribution of Hearing Loss in the DS Newborns WhoDid Not Pass
Their NBS
Of the 87 (26.2%) newborns with DS who did not pass their
NBS, 16 newborns with DS (18.4%) were subsequently
Newborns with DSAlive
n = 332
DS Failed NBSn = 87
DS Passed NBSn = 232
DS No NBSn = 13
Normal Hearingn = 16
(18.4%)
Conductive HLn = 33
(37.9%)
Sensorineural HLn = 5
(5.7%)
Mixed HLn = 3
(3.4%)
Indeterminantn = 8
(9.2%)
No Follow-upn = 22 (25.3%)
Figure 1. Distribution of normal and hearing loss in the Down
syndrome (DS) population. HL, hearing loss; NBS, newborn
hearingscreening.
136 OtolaryngologyHead and Neck Surgery 146(1)
at IMSS on May 26, 2015oto.sagepub.comDownloaded from
-
found to have normal hearing (Figure 1). Thirty-three(37.9%)
newborns with DS were diagnosed with a conduc-
tive hearing loss. Twenty-five of these infants had normal
hearing following insertion of ventilation ear tubes. Seven
infants had a persistent conductive hearing loss following
ear tube insertion and following resolution of otorrhea or
middle ear effusion. Audiologic testing for 1 infant was
inconclusive following tube insertion.
Five infants (5.7%) with DS were diagnosed with sensori-
neural hearing loss. The distribution of hearing loss ranged
from moderate to profound. Three of the 5 infants had
unilat-
eral loss. The time from screening to diagnosis of a hearing
loss was 485 6 601 days (range, 16-1185 days). Three of the5
infants were diagnosed within 3 months of birth. One child
diagnosed 1185 days after birth had a complicated medical
his-
tory, including DiGeorge syndrome, Robertsonian
translocation,
antiphospholipid syndrome, encephalopathy, stroke, seizure
dis-
order, aspiration, and ventilator dependence. Presumably,
the
childs numerous hospitalizations and surgical procedures
delayed the diagnosis and treatment of his sensorineural
hearing
loss. The other child diagnosed with hearing loss more than
3
months after birth required repair of an esophageal atresia.
During his hospitalization in the neonatal intensive care unit,
he
underwent otoacoustic emission (OAE) and ABR testing at 16
days of life. The audiologist documented a concern for a
right
moderate to severe hearing loss. The child unfortunately was
not seen for subsequent testing for another 3 years.
Three infants (3.4%) with DS were diagnosed with a
mixed hearing loss. Time from screening to a diagnosis of a
mixed hearing loss was 60 6 77 days. One child was diag-nosed
later than 90 days. This child had an unbalanced
atrioventricular (AV) canal requiring a pulmonary artery
banding followed by a Fontan procedure. The complex
congenital heart problems may have delayed a timely diag-
nosis for this infant. Eight children (9.2%) had an
indetermi-
nant diagnosis. Twenty-two children (25.3%) were lost to
follow-up. Community otolaryngologists treated some of
these infants, and their audiograms could not be found in
the IHC electronic medical record system.
Distribution of Hearing Loss in the DS Newborns WhoPassed Their
NBS
Two hundred thirty-two newborns with DS passed their NBS
(Figure 2). One hundred twenty-four children (53.4%) main-tained
normal hearing. However, 101 infants developed con-
ductive hearing loss, and 97 (96%) required insertion of
ventilation ear tubes. One child (0.4%) apparently developed
a
sensorineural hearing loss. This child was born at 35 weeks
gestation and required admission to the neonatal intensive
care
unit shortly after birth for maternal chlamydia, dysphagia,
and
cardiomegaly. The chlamydia was treated with antibiotics.
His
cardiomegaly resolved following a patent ductus arteriosus
(PDA) ligation; his feedings were transitioned from enteral
feeding to oral by the time he was discharged approximately
14 days later. The mother was concerned about her sons hear-
ing as early as 6 months of age. It is unclear why she did
not
obtain audiologic testing for him until he was 4 years old.
She
did not know the results of his NBS. Audiologic testing
revealed a right profound and left severe sensorineural
hearing
loss. He has been treated with hearing aids.
One child (0.4%) was diagnosed with an indeterminant
hearing loss. ABR testing revealed a mild to moderate bilat-
eral hearing loss. Otoscopic examination showed no evi-
dence of middle ear fluid. No bone conduction testing was
performed to help differentiate the type of hearing loss. He
Newborns with DSAlive
n = 332
DS Failed NBSn = 87
DS Passed NBSn = 232
DS No NBSn = 13
Normal Hearingn = 124(53.4%)
Conductive HLn = 101(43.5%)
Sensorineural HLn = 1
(0.4%)
No Follow-upn = 5
(2.2%)
Indeterminantn = 1
(0.4%)
Figure 2. Distribution of hearing loss in patients with Down
syndrome (DS) who passed their newborn hearing screening (NBS). HL,
hear-ing loss.
Park et al 137
at IMSS on May 26, 2015oto.sagepub.comDownloaded from
-
has been treated with hearing aids. Five newborns (2.2%)
with DS were lost to follow-up.
Distribution of Hearing Loss in the DS Newborns WhoDid Not Have
NBS
Thirteen newborns (3.9%) with DS did not undergo new-
born hearing screening (Figure 3). Subsequent audiologictesting
indicated 1 child (7.7%) with normal hearing and 1
(7.7%) with a conductive hearing loss. That child underwent
ventilation tube insertion, and a later audiogram demon-
strated normal hearing thresholds. Eleven children (84.6%)
had no follow-up audiologic data reported or available.
Overall Breakdown of Hearing Loss Incidence
The overall incidence of hearing loss and hearing loss type
is shown in Figure 4. Of the 332 children with DS evalu-ated,
141 (42.5%) had normal hearing, 153 (46.1%) had a
hearing loss, and 38 (11.4%) had no audiologic data. Of the
153 with hearing loss, 135 (88.2%) had a conductive hear-
ing loss. Six children with DS (3.9%) had a sensorineural
hearing loss; 3 with DS (2.0%) had a mixed loss. Nine chil-
dren (5.9%) had an indeterminant hearing loss.
Discussion
Of the 332 children with DS evaluated, 42.5% had normal
hearing, 46.1% had a hearing loss, and 11.4% were lost to
follow-up. SNHL was detected in 3.9% of hearing loss
patients; a mixed hearing loss was less common at 2.0%.
Our reported rate of conductive hearing loss is similar to a
number of prior studies.6,11-14 Our reported rate of SNHL is
slightly lower than Davies 4% rate.14
More than 96% of all infants with DS born in Utah
between 2002 and 2006 underwent NBS. It is not clear why
13 DS infants did not undergo hearing screening. For other
infants born in Utah, we know that parental refusal and
labor and delivery staff failing to perform audiologic
testing
are common reasons for missed NBS. Also, nearly 800
births per year are home births involving a midwife and
are less likely to be screened. The opportunity to obtain
NBS is crucial for these patients because our results
indicate
that more than 84% of the infants who did not undergo
NBS did not obtain subsequent audiologic testing.
For the children who underwent NBS, we identified 87
(26.2%) who did not pass their hearing screen. Most were
found to have middle ear effusions requiring ear tube inser-
tions. Not all these patients, however, had normal hearing
following tube insertion. Seven children with DS (21.2%)
had a persistent conductive hearing loss after surgery. This
result is slightly lower than the 40% rate of conductive
hear-
ing loss not attributable to middle ear effusion or tympanic
membrane perforation reported by Balkany et al15 but sup-
ports the need for accurate audiologic testing of all
patients
with DS following tube insertion.
Every child with DS identified with a mixed hearing
loss, and all but 1 child identified with SNHL failed their
initial NBS. Unfortunately, the time from screening to diag-
nosis of an SNHL was not within the 90-day period recom-
mended by the JCIH.10 Multiple factors appear to influence
the time to diagnosis of hearing loss in this population. As
described earlier, at least 2 children had multiple medical
problems that probably delayed the hearing loss diagnosis.
The known high incidence of conductive hearing loss from
middle ear fluid may have clouded the view of some practi-
tioners. The medical records indicated that some physicians
accepted normal sound field responses as sufficient audiolo-
gic workup for a possible hearing loss. This view is
contrary
to our finding that 3 of 5 patients with SNHL had a unilat-
eral hearing loss. Several studies have also reported on the
adverse effects of unilateral hearing loss on speech
develop-
ment and quality of life of otherwise developmentally
normal children.16,17 Unilateral hearing loss in developmen-
tally delayed children would also be expected to adversely
affect their speech development and quality of life.
Twenty-two infants with DS (25.3%) who did not pass
their NBS were lost to follow-up or lost to documentation.
Newborns with DSAlive
n = 332
DS Failed NBSn = 87
DS Passed NBSn = 232
DS No NBSn = 13
Normal Hearingn = 1
(7.7%)
No Follow-upn = 8
(61.5%)
Conductive HLn = 4
(30.8%)
Figure 3. Distribution of hearing loss in Down syndrome
(DS)patients who did not undergo newborn hearing screening
(NBS).HL, hearing loss.
Newborns with DS Alive
n = 332(100%)
DS Normal Hearingn = 141(42.5%)
DS Hearing Lossn = 153(46.1%)
DS no follow-upn = 38
(11.4%)
Conductive HLn = 135(88.2%)
Sensorineural HLn = 6
(3.9%)
Mixed HLn = 3
(2.0%)
Indeterminantn = 9
(5.9%)
Figure 4. Distribution of hearing loss in a population with
Downsyndrome (DS). HL, hearing loss.
138 OtolaryngologyHead and Neck Surgery 146(1)
at IMSS on May 26, 2015oto.sagepub.comDownloaded from
-
This rate is unfortunately consistent with many universal
newborn hearing screening and intervention programs.18,19
Shulman et al20 reported that 38% of all infants from 46
states and territories surveyed in need of a diagnostic eva-
luation did not receive one. They also noted that less than
half of all infants who failed an initial hearing screening
obtained an evaluation by 3 months of age. Improving sur-
veillance data, ensuring a medical home, increasing subspe-
cialty participation, providing family support programs, and
promoting the importance of early detection have been rec-
ommended to address this challenge.20
One hundred one infants (43.5%) with DS who initially
passed their NBS developed a conductive hearing loss from
middle ear fluid. Almost all these patients required ear
tube
insertions. One can conclude from these numbers that regu-
lar otoscopic examination of these patients is critical to
avoid delays in hearing loss diagnosis. The discovery of 1
patient with SNHL following a normal NBS also supports
the need for regular audiologic testing of these children.
Davies14 reported on 1 patient with DS with progressive
SNHL over an 8-year period.
We would advocate a more aggressive and directed
approach toward the evaluation and treatment of children
with DS. Perhaps an approach advocated by Shott et al21
should be implemented. Their group recruited 48 children
with DS for serial otoscopic and audiologic examinations
over a 5-year period. Every child was seen every 6 months;
those with stenotic ear canals (approximately 40% of the
group) were seen every 3 months. Pediatricians were encour-
aged to send children for otolaryngologic microscopic ear
exams if they were unable to visualize the tympanic mem-
branes. An auditory brainstem response study was performed
at least once for every child. Biweekly phone calls were
done
to track patient care. The authors noted that 83% of the
patients required ear tube insertion and that they were able
to
achieve a 98% normal hearing rate in these patients. They
also reported that only 1 patient was lost to follow-up.
Primary care physicians need to be aware of the rela-
tively high incidence of hearing loss in their patients with
Down syndrome and our relatively poor success in achiev-
ing timely diagnosis and treatment. Perhaps these results
are
not surprising because any earlier study by our group
reported a high degree of parental frustration and
difficulty
achieving prompt evaluation and intervention in normal
children with hearing loss.18 Perhaps earlier otolaryngology
evaluation is warranted because these children commonly
have very stenotic ear canals, rendering otoscopic examina-
tion challenging, and many of these children will eventually
require insertion of tympanostomy tubes to remove chronic
middle ear effusions. The otolaryngologist can address both
conditions.
A strength of this study was the ability to identify a large
number of patients with DS from a statewide Utah registry
and the ability to use the Utah Department of Healths infor-
mation tracking and management system and IHCs elec-
tronic medical record system. An outstanding collaborative
environment with the Utah Early Hearing Detection and
Intervention (EHDI) staff, Primary Childrens Medical Center
audiology and otolaryngology personnel, made this study
possible. The existence of just 1 childrens hospital in the
state also improved our ability to minimize any lost
patients
to follow-up. A limitation of this study is its
retrospective
design. Not all the patient data with respect to audiology
test-
ing or examinations were available. Physicians whose medi-
cal records are not kept in the IHC electronic medical
record
system saw some patients. When an otolaryngologist outside
the IHC system treated a patient, we attempted to contact
the
practice for audiologic and otoscopic data.
In summary, patients with Down syndrome present with
a relatively high incidence of conductive, mixed, and sen-
sorineural hearing loss. Providers caring for this
particular
population need to be aware of this high rate of hearing
loss. Unfortunately, there continues to be a shortage of
spe-
cialists in rural areas who are trained to work with infants
and pediatric patients, and there is a general lack of
under-
standing among most parents regarding hearing screening,
follow-up, and hearing loss. Although there has been
signifi-
cant improvement recently and physician knowledge and
attitudes regarding hearing loss are improving, the wait-
and-see approach is still pervasive. Therefore, it is not
sur-
prising that many state systems, including Utah, have failed
in their ability to consistently meet the national EHDI
goals
of screening before 1 month, diagnosis before 3 months,
and referral to appropriate intervention programs before 6
months with these or any other children with special health
care needs.
Author Contributions
Albert H. Park, involved in project conception, analyzed the
data,
and rewrote the manuscript; Matt A. Wilson, obtained the
data
and wrote the initial manuscript draft; Paul T. Stevens,
involved
in the original concept of the project, obtained IRB
approval,
obtained the initial data, and involved in reviewing the
manuscript;
Richard Harward, involved in the conception of the project
and
data acquisition and was instrumental in the analysis and
editing of
the article; Nancy Hohler, involved in project conception,
data
acquisition, and preparation of the manuscript.
Disclosures
Competing interests: None.
Sponsorships: None.
Funding source: None.
References
1. Blaser S, Propst EJ, Martin D, et al. Inner ear dysplasia
is
common in children with Down syndrome (trisomy 21).
Laryngoscope. 2006;116:2113-2119.
2. Shott SR. Down syndrome: common otolaryngologic
manifesta-
tions. Am J Med Genet C Semin Med Genet. 2006;142:131-140.
3. Strome M. Downs syndrome: a modern otorhinolaryngologi-
cal perspective. Laryngoscope. 1981;91:1581-1594.
4. Shibahara Y, Sando I. Congenital anomalies of the
eustachian
tube in Down syndrome: histopathologic case report. Ann Otol
Rhinol Laryngol. 1989;98:543-547.
Park et al 139
at IMSS on May 26, 2015oto.sagepub.comDownloaded from
-
5. Fulton RT, Lloyd LL. Hearing impairment in a population
of
children with Downs syndrome. Am J Ment Defic. 1968;73:
298-302.
6. Brooks DN, Wooley H, Kanjilal GC. Hearing loss and middle
ear disorders patients with Downs syndrome (mongolism). J
Ment Defic Res. 1972;16:21-29.
7. Balkany TJ, Downs MP, Jafek BW, Krajicek MJ. Hearing loss
in Downs syndrome: a treatable handicap more common than
generally recognized. Clin Pediatr (Phila). 1979;18:116-118.
8. Keiser H, Montague J, Wold D, Maune S, Pattison D.
Hearing
loss of Down syndrome adults. Am J Ment Defic. 1981;85:
467-472.
9. Dahle AJ, McCollister FP. Hearing and otologic disorders in
chil-
dren with Down syndrome. Am J Ment Defic. 1986;90:636-642.
10. Year 2007 position statement: principles and guidelines
for
early hearing detection and intervention programs.
Pediatrics.
2007;120:898-921.
11. McIntire MS, Menolascino FJ, Wiley JH. Mongolism: some
clinical aspects. Am J Ment Defic. 1965;69:794-800.
12. Glovsky L. Audiological assessment of a mongoloid
popula-
tion. Train Sch Bull (Vinel). 1966;63:27-36.
13. Fulton RT, Giffin CS. Audiological-otological
considerations
with the mentally retarded. Ment Retard. 1967;5:26-31.
14. Davies B. Auditory disorders in Downs syndrome. Scand
Audiol Suppl. 1988;30:65-68.
15. Balkany TJ, Mischke RE, Downs MP, Jafek BW. Ossicular
abnormalities in Downs syndrome. Otolaryngol Head Neck
Surg. 1979;87:372-384.
16. Lieu JE. Speech-language and educational consequences of
unilateral hearing loss in children. Arch Otolaryngol Head
Neck Surg. 2004;130:524-530.
17. Lieu JE, Tye-Murray N, Karzon RK, Piccirillo JF.
Unilateral
hearing loss is associated with worse speech-language scores
in children. Pediatrics. 2010;125(6):e1348-1355.
18. Park AH, Warner J, Sturgill N, Alder SC. A survey of
parental
views regarding their childs hearing loss: a pilot study.
Otolaryngol Head Neck Surg. 2006;134:794-800.
19. Liu CL, Farrell J, MacNeil JR, Stone S, Barfield W.
Evaluating loss to follow-up in newborn hearing screening in
Massachusetts. Pediatrics. 2008;121:e335-e343.
20. Shulman S, Besculides M, Saltzman A, Ireys H, White KR,
Forsman I. Evaluation of the universal newborn hearing
screening
and intervention program. Pediatrics. 2010;126(suppl
1):S19-S27.
21. Shott SR, Joseph A, Heithaus D. Hearing loss in children
with
Down syndrome. Int J Pediatr Otorhinolaryngol. 2001;61:199-
205.
140 OtolaryngologyHead and Neck Surgery 146(1)
at IMSS on May 26, 2015oto.sagepub.comDownloaded from
/ColorImageDict > /JPEG2000ColorACSImageDict >
/JPEG2000ColorImageDict > /AntiAliasGrayImages false
/CropGrayImages true /GrayImageMinResolution 150
/GrayImageMinResolutionPolicy /OK /DownsampleGrayImages true
/GrayImageDownsampleType /Bicubic /GrayImageResolution 300
/GrayImageDepth -1 /GrayImageMinDownsampleDepth 2
/GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true
/GrayImageFilter /DCTEncode /AutoFilterGrayImages true
/GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict >
/GrayImageDict > /JPEG2000GrayACSImageDict >
/JPEG2000GrayImageDict > /AntiAliasMonoImages false
/CropMonoImages true /MonoImageMinResolution 1200
/MonoImageMinResolutionPolicy /OK /DownsampleMonoImages true
/MonoImageDownsampleType /Bicubic /MonoImageResolution 1200
/MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000
/EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode
/MonoImageDict > /AllowPSXObjects false /CheckCompliance [ /None
] /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false
/PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000
0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox false
/PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ]
/PDFXOutputIntentProfile (U.S. Web Coated \050SWOP\051 v2)
/PDFXOutputConditionIdentifier () /PDFXOutputCondition ()
/PDFXRegistryName (http://www.color.org) /PDFXTrapped /Unknown
/CreateJDFFile false /SyntheticBoldness 1.000000 /Description
>>> setdistillerparams> setpagedevice