Embed Size (px)
Citation preview
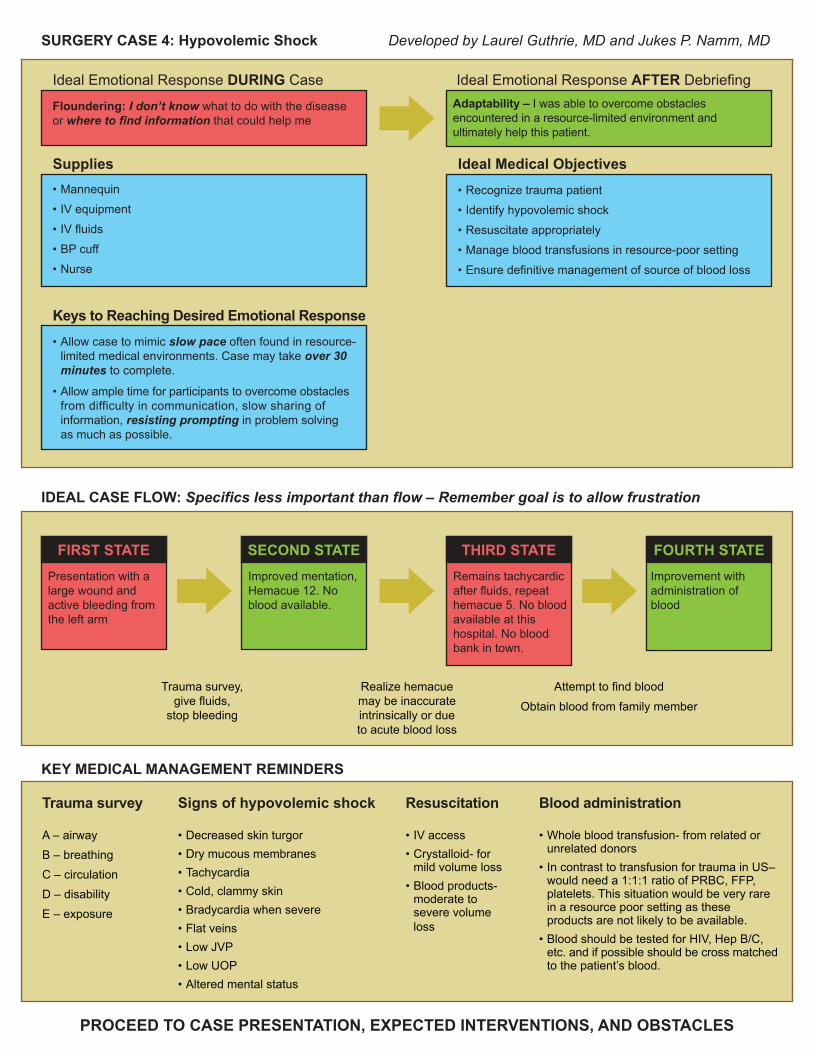
Floundering: I don’t know what to do with the disease or where to find information that could help me
• Mannequin
• IV equipment
• IV fluids
• BP cuff
• Nurse
Adaptability – I was able to overcome obstacles encountered in a resource-limited environment and ultimately help this patient.
Ideal Emotional Response DURING Case Ideal Emotional Response AFTER Debriefing
Developed by Laurel Guthrie, MD and Jukes P. Namm, MD
IDEAL CASE FLOW: Specifics less important than flow – Remember goal is to allow frustration
KEY MEDICAL MANAGEMENT REMINDERS
Trauma survey Signs of hypovolemic shock
Supplies• Recognize trauma patient
• Identify hypovolemic shock
• Resuscitate appropriately
• Manage blood transfusions in resource-poor setting
• Ensure definitive management of source of blood loss
Ideal Medical Objectives
Presentation with a large wound and active bleeding from the left arm
FIRST STATEImproved mentation, Hemacue 12. No blood available.
SECOND STATE
Trauma survey,give fluids,
stop bleeding
Remains tachycardic after fluids, repeat hemacue 5. No blood available at this hospital. No blood bank in town.
THIRD STATEImprovement with administration of blood
FOURTH STATE
Attempt to find blood
Obtain blood from family member
Realize hemacuemay be inaccurateintrinsically or dueto acute blood loss
A – airway B – breathing C – circulation D – disabilityE – exposure
Resuscitation
• IV access• Crystalloid- for mild volume loss• Blood products- moderate to severe volume loss
Blood administration
• Whole blood transfusion- from related or unrelated donors • In contrast to transfusion for trauma in US– would need a 1:1:1 ratio of PRBC, FFP, platelets. This situation would be very rare in a resource poor setting as these products are not likely to be available. • Blood should be tested for HIV, Hep B/C, etc. and if possible should be cross matched to the patient’s blood.
• Decreased skin turgor• Dry mucous membranes• Tachycardia• Cold, clammy skin• Bradycardia when severe• Flat veins• Low JVP• Low UOP• Altered mental status
PROCEED TO CASE PRESENTATION, EXPECTED INTERVENTIONS, AND OBSTACLES
SURGERY CASE 4: Hypovolemic Shock
• Allow case to mimic slow pace often found in resource-limited medical environments. Case may take over 30 minutes to complete.
• Allow ample time for participants to overcome obstacles from difficulty in communication, slow sharing of information, resisting prompting in problem solvingas much as possible.
Keys to Reaching Desired Emotional Response
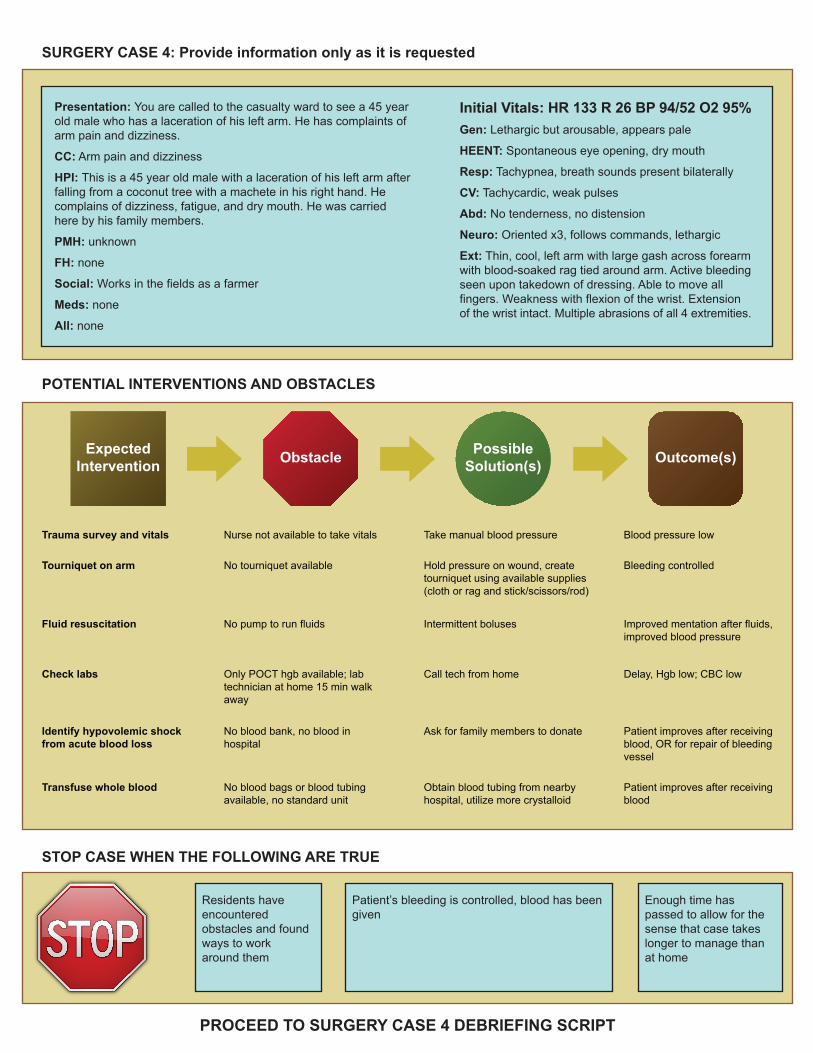
SURGERY CASE 4: Provide information only as it is requested
PROCEED TO SURGERY CASE 4 DEBRIEFING SCRIPT
POTENTIAL INTERVENTIONS AND OBSTACLES
STOP CASE WHEN THE FOLLOWING ARE TRUE
Presentation: You are called to the casualty ward to see a 45 year old male who has a laceration of his left arm. He has complaints of arm pain and dizziness.
CC: Arm pain and dizziness
HPI: This is a 45 year old male with a laceration of his left arm after falling from a coconut tree with a machete in his right hand. He complains of dizziness, fatigue, and dry mouth. He was carried here by his family members.
PMH: unknown
FH: none
Social: Works in the fields as a farmer
Meds: none
All: none
Initial Vitals: HR 133 R 26 BP 94/52 O2 95%Gen: Lethargic but arousable, appears pale
HEENT: Spontaneous eye opening, dry mouth
Resp: Tachypnea, breath sounds present bilaterally
CV: Tachycardic, weak pulses
Abd: No tenderness, no distension
Neuro: Oriented x3, follows commands, lethargic
Ext: Thin, cool, left arm with large gash across forearm with blood-soaked rag tied around arm. Active bleeding seen upon takedown of dressing. Able to move all fingers. Weakness with flexion of the wrist. Extension of the wrist intact. Multiple abrasions of all 4 extremities.
Residents have encountered obstacles and found ways to work around them
Patient’s bleeding is controlled, blood has been given
Enough time has passed to allow for the sense that case takes longer to manage than at home
ExpectedIntervention Obstacle Possible
Solution(s) Outcome(s)
Blood pressure lowTake manual blood pressureNurse not available to take vitalsTrauma survey and vitals
Patient improves after receiving blood, OR for repair of bleeding vessel
Ask for family members to donateNo blood bank, no blood inhospital
Identify hypovolemic shock from acute blood loss
Patient improves after receiving blood
Obtain blood tubing from nearby hospital, utilize more crystalloid
No blood bags or blood tubing available, no standard unit
Transfuse whole blood
Bleeding controlledHold pressure on wound, create tourniquet using available supplies (cloth or rag and stick/scissors/rod)
No tourniquet availableTourniquet on arm
Improved mentation after fluids, improved blood pressure
Intermittent bolusesNo pump to run fluidsFluid resuscitation
Delay, Hgb low; CBC lowCall tech from homeOnly POCT hgb available; lab technician at home 15 min walk away
Check labs

SURGERY CASE 4 DEBRIEFING SCRIPT1
Remember: Goal of debriefing is not to lecture, but to facilitate discussion
1Adapted with permission from Eppich, W., & Cheng, A. (in press). Promoting Excellence And Reflective Learning in Simulation (PEARLS):Development and Rationale for a Blended Approach to Healthcare Simulation Debriefing. Simul Healthc.
Setting the Scene: “We are going to spend the next 20-30 minutes debriefing the case. We are going to focus our attention on the emotions encountered but will also address the management of the case. We also want to focus on how you overcame obstacles often encountered when managing a case like this in a resource-limited environment.”
Reaction: “How did that feel?” Pay attention to cues pointing to overcoming lack of knowledge with ability to use available resources.
Description/Clarification: “Can someone summarize what the case was about from a medical standpoint by taking us through what just happened? I want to make sure we are all on the same page.”
You may need to clarify and keep this moving by asking follow up questions. “What happened next?”
Application/Summary: “Is there anything you learned during the course of this case, that has changed your perspective about your experience abroad?”
End with each learner providing a take-home point from the case
Analysis: “What aspects of the case do you think you managed well?” “Were there aspects you’d wish to manage differently the next time?” “What was different about this case management or flow than what you are used to?” “How might you see yourself reacting to those changes abroad? How might your reactions be perceived by the local medical providers?” “What obstacles did you encounter to providing the care that you felt the patient needed?” “How did you overcome those obstacles?”
Review the individual obstacles on Page 2 of the case and the possible solutions. Review appropriate considerations and indications for blood transfusion.
Framework for Formulating Effective Debriefing Questions – Choose one prompt from each column
Observation Point of View Question
I noticed that... I liked that... How do you all see it?
I saw that... I was thinking... What were the team’s priorities at the time?
I heard you say... It seemed to me... How did the team decide that...
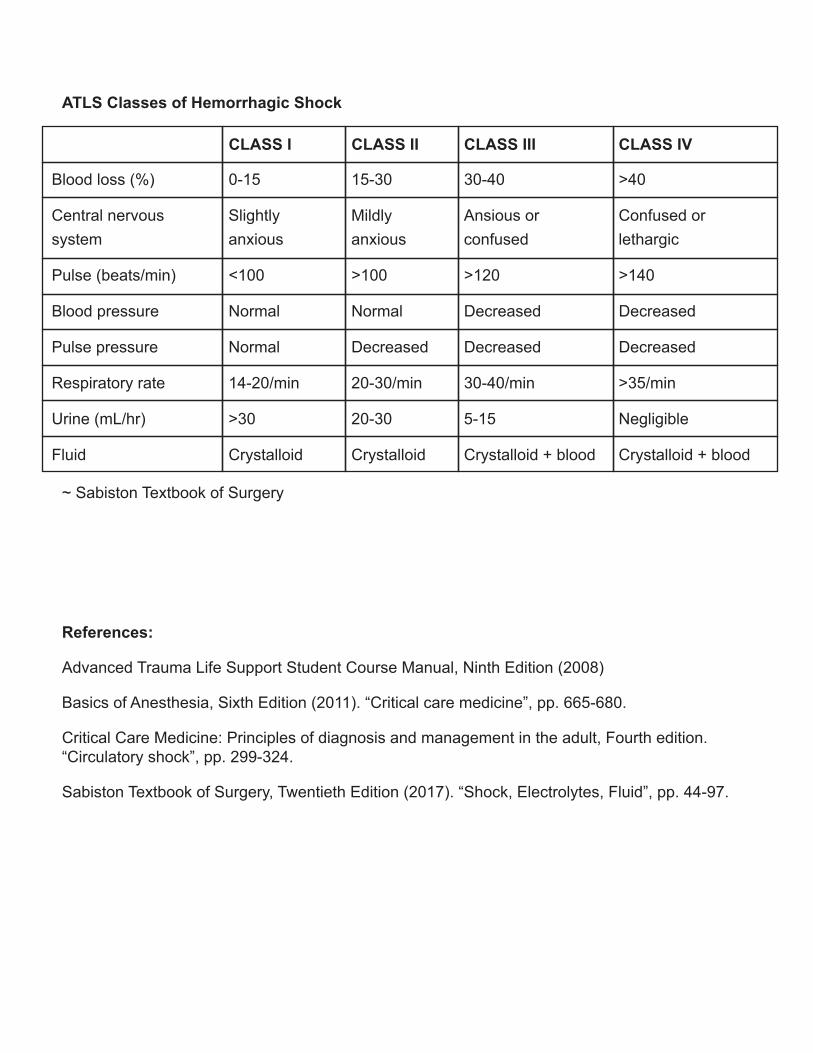
References:
Advanced Trauma Life Support Student Course Manual, Ninth Edition (2008)
Basics of Anesthesia, Sixth Edition (2011). “Critical care medicine”, pp. 665-680.
Critical Care Medicine: Principles of diagnosis and management in the adult, Fourth edition.“Circulatory shock”, pp. 299-324.
Sabiston Textbook of Surgery, Twentieth Edition (2017). “Shock, Electrolytes, Fluid”, pp. 44-97.
~ Sabiston Textbook of Surgery
ATLS Classes of Hemorrhagic Shock
Blood loss (%) 0-15
CLASS I
15-30
CLASS II
30-40
CLASS III
>40
Pulse (beats/min) <100 >100 >120 >140
Blood pressure Normal Normal Decreased Decreased
Pulse pressure Normal Decreased Decreased Decreased
Respiratory rate 14-20/min 20-30/min 30-40/min >35/min
Urine (mL/hr) >30 20-30 5-15 Negligible
Fluid Crystalloid Crystalloid Crystalloid + blood Crystalloid + blood
Central nervoussystem
Slightlyanxious
Mildlyanxious
Ansious orconfused
Confused orlethargic
CLASS IV





























