Embed Size (px)
Citation preview

ICU SKILLS UPDATE
February/March 2007
By Dianne Brown
ICU Skills Update
Theory and Hands On Practice
1. Bispectral Index Monitoring

BISPECTRAL INDEX MONITOTING

BISPECTRAL INDEX MONITORING
The bispectral index (BIS) is a fairly recent technology used to measure the effects of anesthetics and sedatives on the brain and consciousness
Uses a complex mathematical algorithm based upon descriptive EEG parameters from the frontal cortex to suggest various levels of sedation

BISPECTRAL INDEX MONITORING
A sensor, placed on the patient’s forehead, sends raw EEG waveforms to the monitor, where they are analyzed and a BIS index is calculated
This value ranges from 100 (completely awake) to 0 (isoelectric EEG)

BISPECTRAL INDEX MONITORING

BISPECTRAL INDEX MONITORING


Understanding the relationship between BIS and EEG
When BIS monitoring is initiated, a sensor is placed across the patient’s forehead per manufacturer’s recommendations to detect one channel of EEG activity
The EEG signal is filtered and digitalized The EEG state (frequency/amplitude) is
calculated and associated with the level of sedation, arousal or anesthesia
Understanding the relationship between BIS and EEG
The BIS value is a single number based on the previous 15 seconds of EEG data and is updated frequently
The BIS monitor provides a single channel of an EEG tracing from the right or left frontal-temporal montage electrode placement
ICU Sedation: A Bipolar Challenge
Over-sedation Patient unable to
participate in care Delayed weaning ↑Ventilator-associated
pneumonia ↑Unnecessary testing ↑ICU and hospital
length of stay ↑Costs
Under-sedation Anxiety, agitation ↑Cost, nursing time ↑Use of neuromuscular
blocking agents ↑Risk of
recall/awareness of unpleasant events
↑Unintended medical device removal

Potential Indications for BIS Monitoring
Use with neuromuscular blockade: BIS monitoring may help to identify patients at risk of awareness, recall and pain when paralyzed
Use of BIS values to guide sedation and analgesia Titrating sedation/analgesia in patients receiving
controlled ventilation Avoiding extremes of under and over sedation Titration of medications for medication-induced
coma

Factors affecting the BIS value
Sedation: decrease in BIS value Analgesia: decrease in BIS value Neuromuscular blocking agents: decrease in
BIS value related to attenuation of high-frequency muscle activity across the patient’s forehead
Painful (noxious) stimulation: if analgesia inadequate, arousal response may be produced within cerebral cortex
Factors affecting the BIS value
Sleep: BIS range is lower (20-70) during deep sleep, and BIS range is higher (75-92) during REM sleep
Hypothermia: decrease in BIS value Cerebral ischemia: decrease in BIS value Neurological states: decrease in BIS value
depending of location of injury and degree to which overall cerebral metabolism is affected

Factors affecting the BIS value
Encephalopathic states: severe anoxic/ischemia encephalopathy (decrease in BIS value)
High-frequency electrical artifact from patient care equipment, such as pacemaker or muscle activity; rapid head or eye movement (increase in BIS value)
Interpretation of BIS value
BIS is interpreted over time, in response to stimulation and within the context of whether therapeutic endpoints and overall goals of therapy are met
Decisions to increase or decrease titration of sedative or analgesic should be based on clinical assessment/judgement, goals of therapy, and the BIS value

Interpretation of BIS value
Relying on BIS alone for sedation/analgesia management is not recommended
Movement such as in response to painful stimulation may occur with low BIS values

BIS increases suddenly or is higher than expected
Is the sedative sufficient?
Has the sedation been decreased?
Is there an increase in stimulation?
Is there any muscle shivering or pt motion?
Is the NMBA wearing off?

BIS decreases suddenly or is lower than expected
Has been a decrease in stimulation?
Has patient recently received NMBA?
Has there been an increase in sedation?
Is the patient sleeping? Has the pt recently received
analgesic? Has there been a sudden
significant drop in BP?

Current Status of the Literature
BIS scores do not provide a differential diagnosis. BIS scores can be affected by many cerebral events including sedation, sleep and cerebral ischemia
BIS/EEG activity can also be affected by age, temperature, PaCO2, hyper/hypo-glycemia, electroyte imbalances, hepatic or renal function, endocrine disorders

Current Status of the Literature BIS scores can be affected by many forms of
artifact:
- Artifact occurs with excessive muscle activity – movement, swallowing, blinking, shivering etc.
- Artifact can also occur with concomitant use of other electrical devices and monitoring equipment - EEG
Current Status of the Literature
Neuromuscular activity typically elevates BIS scores. Hence the effects of NMBAs or their metabolites may cause lower BIS scores as a result of decreased muscle activity and not decreased LOC
The synergistic action of agents affecting muscle relaxation must be considered when interpreting scores
Current Status of the Literature
Overall conflicting research results May predict recovery of consciousness related to
sedation and possibly traumatic brain injury Several studies have found variable correlations
between BIS scores and sedation scores BIS monitoring may serve as an adjunct measure to
subjective scales of sedation monitoring in ICU patients, particularly in patients who are heavily sedated or chemically paralyzed
Clinical Applications
BIS is only one part of a multi-modal assessment strategy
It remains unclear as to what BIS actually measures: Awareness? Hypnosis with recall? Delirium? Extent of brain injury, brain function or generalized cerebral electrical activity?

Clinical Applications
Only use trended scoresWhen interpreting results, consider
multiple factors including measurements error as well as the special/individual circumstances of each patient
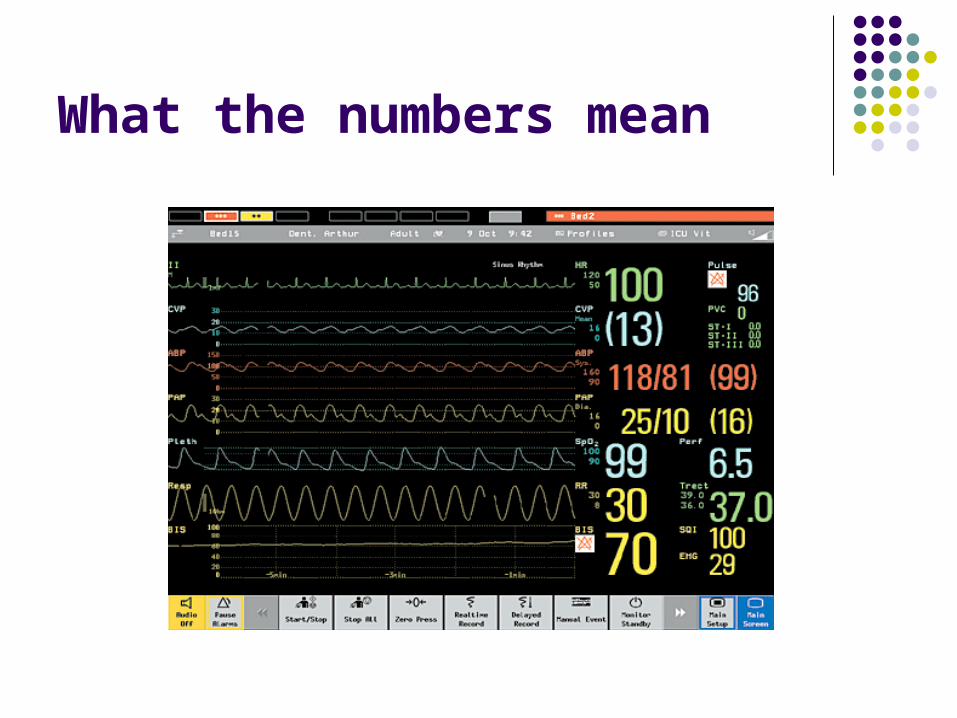
What the numbers mean

BIS Number
What the numbers mean:
0 = no electrical brain activity
100 = fully awake For moderate sedation, aim for range from 60-
70, below 60 is associated with a low probability of explicit recall
For deeper sedation, aim for range from 40-60. A patient with a BIS value of less than 45 is approaching a deep hypnotic state

BIS Number
For a patient receiving neuromuscular blockage, sedation, analgesia therapy, the medication should be titrated for a BIS value between 45 and 60

SQI: Signal Quality Index
What the numbers mean: 0 = poor quality
100 = excellent quality Aim for range from 80-100%

EMG: Electromyographic Activity
Reflects the electrical power of muscle activity or artifact
What the numbers mean: the higher the number, the greater the muscle activity
- if the EMG is high, can make the number artificially high (it incorrectly reads the increased muscle activity as increased EEG activity
Acceptable EMG is less than 55 dB Optimal EMG is less than 30 dB

Electrode Placement
Prep skin with alcohol prior to electrode placement
Electrode should be changed every 24 hours, alternating temples daily
Look at electrode packaging for placement instructions

Electrode Placement
To ensure adequate placement and impedance, check on the screen

Resources
Guidelines and Procedure available in AACN Procedural Manual for Critical Care, Procedure 86, page 699





























