Embed Size (px)
Citation preview

CONTINUING EDUCATION
ICD-10 Medical Coding: TheRole of Perioperative Services inAddressing ImplementationChallenges 1.6 www.aornjournal.org/content/cme
TONI L. WING, BSN, RN, CNOR
Continuing Education Contact Hoursindicates that continuing education (CE) contact hours are
available for this activity. Earn the CE contact hours byreading this article, reviewing the purpose/goal and objectives,and completing the online Examination and Learner Evalua-tion at http://www.aornjournal.org/content/cme. A score of 70%correct on the examination is required for credit. Participantsreceive feedback on incorrect answers. Each applicant whosuccessfully completes this program can immediately print acertificate of completion.
Event: #16504Session: #0001Fee: For current pricing, please go to: http://www.aornjournal.org/content/cme.
The contact hours for this article expire February 28, 2019.Pricing is subject to change.
Purpose/GoalTo provide the learner with knowledge specific to theInternational Classification of Diseases, 10th Revision (ICD-10)medical coding system and its effects on perioperative services.
Objectives1. Describe ICD-10.2. Identify how ICD-10 affects perioperative services.3. Discuss how ICD-10 differs from ICD-9.4. Explain considerations for using ICD-10 in perioperative
settings.5. Describe strategies for implementing the use of ICD-10.
AccreditationAORN is accredited as a provider of continuing nursingeducation by the American Nurses Credentialing Center’sCommission on Accreditation.
ApprovalsThis program meets criteria for CNOR and CRNFA recerti-fication, as well as other CE requirements.
AORN is provider-approved by the California Board of Regis-tered Nursing, Provider Number CEP 13019. Check with yourstate board of nursing for acceptance of this activity for relicensure.
Conflict-of-Interest DisclosuresAs a consultant for Coratek Perioperative Consulting, LLC,Toni L. Wing, BSN, RN, CNOR, has declared an affiliationthat could be perceived as posing a potential conflict of interestin the publication of this article.
The behavioral objectives for this program were created byHelen Starbuck Pashley, MA, BSN, CNOR, clinical editor,with consultation from Susan Bakewell, MS, RN-BC, director,Perioperative Education.Ms Starbuck Pashley andMs Bakewellhave no declared affiliations that could be perceived as posingpotential conflicts of interest in the publication of this article.
Sponsorship or Commercial SupportNo sponsorship or commercial support was received for this article.
DisclaimerAORN recognizes these activities as CE for RNs. This recognitiondoes not imply that AORN or the American Nurses CredentialingCenter approves or endorses products mentioned in the activity.
http://dx.doi.org/10.1016/j.aorn.2015.12.008ª AORN, Inc, 2016
www.aornjournal.org AORN Journal j 177

ICD-10 Medical Coding: TheRole of Perioperative Services inAddressing ImplementationChallenges 1.6 www.aornjournal.org/content/cme
TONI L. WING, BSN, RN, CNOR
ABSTRACTThe International Classification of Diseases, 10th Revision (ICD-10) was adopted in the United Stateson October 1, 2015. Replacing the outdated ICD, Ninth Revision, Clinical Modification (ICD-9-CM)coding system was long overdue, and the updated classifications were needed to accurately collectdata and improve patient care. However, the complexity of ICD-10 may present substantial challengesfor health information management coders and affect hospital revenue collection. Because theOR generates a large share of a hospital’s overall revenue, perioperative services personnel musttake a critical look at ICD-10 changes and address adoption challenges to minimize the negativeeffects ICD-10 may have on surgical revenue and help personnel identify perioperative services’important role in ICD-10 implementation. AORN J 103 (February 2016) 178-185. ª AORN, Inc, 2016.http://dx.doi.org/10.1016/j.aorn.2015.12.008
Key words: ICD-10, revenue, assessment, coding, charge description master.
For most chief financial officers, the InternationalClassification of Diseases, 10th Revision (ICD-10)will remain at the top of the list of concerns in 2016.1
The term ICD-10 relates to diagnosis and procedure codingused to bill for medical and surgical services. Although mostindustrialized countries switched to ICD-10 coding years ago,the Unites States adopted the new coding system on October1, 2015.2 In anticipation of potential negative effects ofICD-10 on hospital revenue due to delayed billing and deniedclaims as hospital information management (HIM) codersadapt to the significantly expanded coding system, the Centersfor Medicare & Medicaid Services (CMS) establishedmany resources to assist in the coding process, including anICD-10 ombudsman for provider questions and concerns.3
Because the OR generates as much as 60% of a hospital’soverall revenue, now is the time for perioperative servicespersonnel to take a critical look at how ICD-10 affects the OR.
Some perioperative managers may dismiss concerns about thenew procedural and diagnosis coding and its effect on periop-erative services. Personnel involved in hospital-wide clinicaldocumentation improvement initiatives also may be over-looking the documentation needs for effective procedure codingand the challenges this presents to HIM coders. Dismissing theeffects of ICD-10 on surgical revenue and ignoring the roleperioperative services plays in successful ICD-10 implementa-tion could be very costly.4 To understand and implement thesechanges, nurses can help team members identify the necessarysteps to develop effective strategies for working with ICD-10.5
ICD-10 PROCEDURE CODINGASSESSMENTWithin the ICD-10 coding structure are two distinct codingsystems, the ICD-10 Clinical Modification (ICD-10-CM) used
http://dx.doi.org/10.1016/j.aorn.2015.12.008ª AORN, Inc, 2016
178 j AORN Journal www.aornjournal.org

for coding all diagnoses, and the ICD-10 Procedure CodingSystem (ICD-10-PCS) used for coding procedures in the inpa-tient hospital setting.5 The ICD-9-CM has been in use in theUnited States since 1979, and replacing this outdated codingsystem to allow for standardized, codified data collection waslong overdue. The unique coding structure of ICD-10-PCS willprovide detailed data collection opportunities for measuringservices provided to patients, comparing performance amongsurgical service lines, and researching and developing evidence-based best practices. Most importantly, it will identifyopportunities to improve patient care and outcomes.5 Unlikethe generic structure and limited coding within ICD-9-CM,ICD-10-PCS contains more granular codes for each procedureand allows easy additions and modifications as technology andadditional procedures are developed.
Although ICD-10-CM is required for all diagnosis coding, ICD-10-PCS coding is only required for inpatient hospital billing,which complicates perioperative coding. Surgeons will continueto bill all inpatient and outpatient surgical procedures using theCurrent Procedural Terminology (CPT) coding system devel-oped and licensed through the American Medical Association.6
However, hospitals will continue to use the CPT procedurecoding system for all outpatient procedures and only use thenew ICD-10-PCS system for inpatient procedure billing.
Assigning ICD codes to surgical procedures for hospitalbilling has routinely occurred outside of the OR in the HIMcoding department with little to no effect on surgical services.However, with this new procedure classification system,finding the correct code will require much more than thesurgical procedure name. For coders to arrive at the correctICD-10-PCS code, they will need detailed clinical documen-tation regarding the procedure, its anatomical location, thesurgical approach, and any devices implanted.
Classification SystemThe 2016 version of the ICD-10 PCS Reference Manual,developed by 3M Health Information Systems under thedirection of the CMS, reveals some of the significant changesfrom ICD-9-CM.7 Understanding these changes will allowperioperative services personnel to assist the HIM team inbridging the gap between surgical procedures performed andaccurate procedure code determination for effective revenuecycle management.
Procedure description changesTable 1 shows some examples of the procedure descriptiondifferences.8-10 A comparison of the new ICD-10 procedure
descriptions with an OR surgery schedule or CPT and ICD-9 code descriptions quickly reveals the absence of commonOR language. The new system has no
� diagnosis or disease process descriptions (eg, aneurysm, cleftlip, hernia, fracture);
� procedure descriptions named after people (eg, Nissen fun-doplication, Bankart repair, Roux-en-Y anastomosis);
� use of acronyms (eg, coronary artery bypass graft [CABG],extracorporeal shock wave lithotripsy [ESWL], posteriorlumbar interbody fusion [PLIF], open reduction internalfixation [ORIF]);
� common procedure names (eg, appendectomy, tracheos-tomy, arthroscopy, laparoscopy, laminectomy) and replacesthese procedure names by surgical root operations:o resection (eg, appendectomy),o bypass (eg, tracheostomy),o inspection (eg, diagnostic arthroscopy, diagnostic lapa-roscopy), and
o excision (eg, laminectomy); and� combination procedures (eg, tonsillectomy with adenoidec-tomy), and it requires separate codes for each procedure(with rare exceptions).7
Constructed rather than fixed codesUnlike ICD-9-CM fixed codes, this new coding system usesseven distinct characteristics of the procedure performed,including anatomical location, surgical approach, and devicesimplanted to construct an alpha-numeric procedure code.Using reference tables and indexes from the ICD-10 manualalong with clinical data from the surgeon’s operative note andthe operative record, the coder will select an alpha or numericcharacter from each of the seven categories to arrive at the finalbillable code.
A look at the seven categories described in the ICD-10-PCSReference Manual reveals the detailed clinical data informa-tion that nonclinical HIM coders will need to accurately selectthe procedure code. Coders will need to know the
� procedure category (eg, medical, surgical, obstetrics);� body system or general anatomical location (eg, centralnervous system, heart and great vessels, eye, muscles, lowerjoints);
� root operation (eg, bypass, excision, replacement)dtranslatingthe surgeon’s operative notes, which may contain commonprocedure names and OR language, into the correct rootoperation may prove to be a challenge (eg, identifyingthe “intent” of the surgery, understanding that these rootoperations have distinct meanings);
February 2016, Vol. 103, No. 2 ICD-10 Medical Coding
www.aornjournal.org AORN Journal j 179

� body part or the specific anatomical site where the procedurewas performeddunlike the generic body system, thisdescription provides detail (eg, pulmonary artery, left; lacrimalduct, right; lumbosacral disk), and operative notes withdetailed descriptions of the procedures performed are required;
� approach or technique used to perform the procedure (eg,open, percutaneous, percutaneous endoscopic);
� device left in place at the end of the procedure, if applicable(eg, grafts, prostheses, implants, mechanical or electronicappliances, drainage device, radioactive element, monitoringdevice, synthetic substitute, autologous tissue substitute,infusion device)dthis area by far will present the greatestchallenge for coders to convert commercial device andimplant names into the correct device category (eg, anextraluminal device or an intraluminal device; total hipimplants as metal, metal on polyethylene, ceramic, orceramic on polyethylene); and
� qualifier or additional information or attribute of the pro-cedure (eg, diagnostic)dto identify this character, detaileddescriptions in the operative note will be essential.7
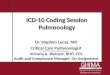
Figure 1 shows an example of how a coder would buildthe ICD-10-PCS code for a right total knee arthroplasty.10
As a result of this coding method, there are more than60,000 different and distinct ICD-10-PCS codes for surgicalprocedures.
BRIDGING THE GAPThe team that best understands the OR is the surgical team;however, traditional methods of identifying proceduresand conditions for coding purposes have changed. Withoutsurgical team members understanding and adapting tothis change, hospital coders will have difficulty interpretingvague operative notes, poor clinical documentation, implantlists, and the many brand-name surgical devices used in theOR. Translating common surgical procedure names into rootoperations and surgical approaches, sifting through clinicaldocumentation for anatomical locations, and decipheringimplant descriptions for the correct device type is delayingbill submission and reimbursement while hospital coders
Table 1. Examples of Procedure Description Differences
Source Procedure Description
OR surgery schedule Open reduction internal fixation right femur fracture
CPT Open treatment of femoral shaft fracture with plate/screws, with or without cerclage
ICD-9-CM Open reduction fracture internal fixation femur
ICD-10-PCS Reposition right femoral shaft with internal fixation device, open approach
OR surgery schedule Appendectomy
CPT Appendectomy
ICD-9-CM Other appendectomy
ICD-10-PCS Resection of appendix, open approach
OR surgery schedule Tracheostomy
CPT Tracheostomy planned, separate procedure
ICD-9-CM Other permanent tracheostomy
ICD-10-PCS Bypass trachea to cutaneous with tracheostomy device, open approach
OR surgery schedule Arthroscopy right knee
CPT Arthroscopy, knee, diagnostic, with or without synovial biopsy
ICD-9-CM Arthroscopy, knee
ICD-10-PCS Inspection of right knee joint, percutaneous endoscopic approach
OR surgery schedule Laparoscopic Nissen fundoplication
CPT Laparoscopy, surgical, esophagogastric fundoplasty
ICD-9-CM Laparoscopic procedures for creation of esophagogastric sphincter competence
ICD-10-PCS Restriction of esophagogastric junction, percutaneous endoscopic approach
CPT ¼ Current Procedural Terminology; ICD-9-CM ¼ International Classification of Diseases, 9th Revision, Clinical Modification;ICD-10-PCS ¼ International Classification of Diseases, 10th Revision, Procedure Coding System.
Editor’s note: Current Procedural Terminology is a registered trademark of the American Medical Association, Chicago, IL.
Wing February 2016, Vol. 103, No. 2
180 j AORN Journal www.aornjournal.org

become familiar with using the new code set. The first stepto conquering these challenges is for perioperative servicesteam members to join forces with HIM team membersto develop strategies for success. Surgeons and OR staffmembers are not expected to become professional hospitalcoders; however, they can collect the clinical data in sucha way as to compile information that allows the coder tobe effective in decision making when selecting the correctprocedure code.
Some managers may consider replacing their current surgicalprocedure file used for scheduling OR procedures withICD-10-PCS procedure names; however, with more than60,000 current procedure codes, the maintenance, updates,and effects on physician preference cards would be significant.Software also may be affected because many of the ICD-10-PCS procedure descriptions exceed the software vendors’character limits. Converting the current surgical proceduredescriptions to ICD-10-PCS nomenclature would also presentchallenges to OR schedulers and staff members.
The following scenarios depict potential challenges with usingICD-10-PCS procedure nomenclature. Office personnel for avascular surgeon call to schedule a right femoral arterythrombectomy. The OR scheduler searches the surgical pro-cedure file for the word thrombectomy and finds a proceduredescription similar to this CPT procedure: embolectomy/thrombectomy; femoropopliteal/aortoiliac artery, leg incision.However, using ICD-10-PCS procedure descriptions, the ORscheduler must understand that surgical procedures such asthrombectomy are not part of the new coding language; he orshe will need to search for the word extirpation to find thecorrect ICD-10 procedure: extirpation of matter from rightfemoral artery, percutaneous approach. Realizing that this pro-cedure has multiple approaches, the scheduler will need to
clarify with the office scheduler whether the procedure will beperformed open or percutaneous.
The effect on the OR team is similar. Preparing for the repairof a ventral hernia with mesh, the OR team must use theprocedure terms supplement abdominal wall with syntheticsubstitute, open approach rather than the familiar procedureterms ventral hernia repair with mesh. In another example, anOR team prepares for a below-knee amputation of the left leg.Because ICD-10-PCS descriptions do not contain commonnames for surgical procedures, the team will need to use theprocedure terms detachment at left lower leg, low, openapproach. These scenarios demonstrate the significant differ-ences between common OR language and the new ICD-10-PCS procedure nomenclature.
Before restructuring the entire surgical process or investing inexpensive new software, it is important for information tech-nology (IT) staff members to inquire about what strategiesvendors have developed to support the facility’s electronicperioperative system and how they may be able to assist HIMcoders with surgical procedure code assignment. It is alsoimportant for perioperative IT specialists to assess theirfacility’s current system and workflows and to identify op-portunities to use existing software to capture the neededICD-10 information.
IMPLEMENTATION STRATEGIESAn integrated team approach is best when strategizing forsuccess. Nurses and other members of the team can join theirorganization’s clinical documentation improvement processes.Perioperative nurses and surgical technologists possessthe expertise required to review operative notes and periop-erative records for accuracy. These perioperative team
print&web4C=F
PO
Figure 1. This illustration shows an example of how a coder would build the ICD-10-PCS code for a right total kneearthroplasty.
February 2016, Vol. 103, No. 2 ICD-10 Medical Coding
www.aornjournal.org AORN Journal j 181

members also have an established rapport with surgeons andprovide the perfect opportunity to assist with documentationimprovement initiatives. The following are implementationstrategies that can help ensure success with using ICD-10 codes.
� Develop a task team with HIM personnel to explore op-portunities to streamline the procedure coding process.
� Establish coder training sessions with the OR team to allowthe surgical experts to help coders quickly find informationin the operative documentation (eg, devices, laterality)and read the surgeon’s operative notes to decipher surgicalapproach, anatomical locations, and additional detailsneeded to accurately code the procedure.
� Create a perioperative resource team that includes nurses andsurgical technologists who can be available to answer coders’questions. This can provide quicker responses and decrease
the need for physician queries to help minimize surgeonfrustration.
� Work with the HIM team to create coder reference charts andprocedure crosswalks. Start by examining the surgery proce-dure list for procedure names that are difficult to interpret(determine if modifying the procedure description would helpthe coder identify the root operation). Review the implantabledevices in the surgery catalogdcheck if the device names arelisted by manufacturer name and assess if a coder could easilydetermine whether the device type is intraluminal versusextraluminal, synthetic versus nonautologous, or an infusiondevice versus a monitoring device. Look for opportunities toidentify these device types in the electronic item catalog and/or create reference charts for quick identification.6
Using the 80/20 rule whereby 80% of the cases performednormally encompass the top 20% of the procedure file,
print&web4C=F
PO
Figure 2. By tracking coding tests in a spreadsheet, coders and other team members can merge and sort the datato facilitate team reviews.
Wing February 2016, Vol. 103, No. 2
182 j AORN Journal www.aornjournal.org

print&web4C=F
PO
Figure 3. An evaluation tool for surgical procedure coding can help managers collect feedback from coders,identify challenges, assess the usefulness of available resources, and address areas of concern.
February 2016, Vol. 103, No. 2 ICD-10 Medical Coding
www.aornjournal.org AORN Journal j 183

it would be logical that by focusing on the facility’s topfive service lines (eg, the top 10 to 20 procedures), facilitymanagers can affect the largest amount of work inthe shortest period of time. Specifically, the perioperativeteam should evaluate current documentation practicesand look for opportunities to provide clarity for HIMcoders. Managers or IT personnel should investigatesurgical software capabilities to incorporate documentationprompts for capturing root operation, anatomical site, anddevice types. Perioperative technology specialists can beenlisted to assist HIM coders and perioperative team memberswith using existing procedural terminology to create datacrosswalks, which with report extracts can assist in the interimor as an ongoing strategy to streamline procedural codecollection.
In addition to procedure coding challenges, there also may bedisconnects between the ICD-10-PCS code and the actualcharges assigned to that procedure for claims submission. Withthe increased specificity of ICD-10 coding, the potential for amismatch between automated charge coding from the chargedescription master (CDM) and manually determined proce-dure codes could exponentially increase claim denials becauseof inaccurate charge code submission. When evaluating thecoding for the top procedures performed with HIM coders,the CDM team should be involved to help identify risk areasthat could result in potential charge entry inaccuracies andomissions.11 Confronting these ICD-10 procedure challengeson the front end will expedite the coding process on theback end, thereby minimizing any projected disruptions tocash flow.
Monitor for SuccessAfter the team develops an action plan and the tools andprocesses are in place, continued evaluation and modifica-tions are necessary to ensure success. The team shouldconduct ICD-10-PCS procedure code education and reviewsessions. To ensure accurate coding scenarios, the teamshould work with actual surgical procedure documentationfrom the surgery schedule to practice ICD-10 coding,which will help identify documentation gaps. Codersshould keep track of their practice sessions in a spreadsheetsimilar to the example in Figure 2, which will allow teammembers to merge and sort the data and use the findingsto facilitate team reviews with OR personnel and HIMcoders. The review session should evaluate for codeaccuracy, identify documentation components, practicewith using the resource tools, and establish positiveworking relationships.
It will also be beneficial to evaluate the effectiveness of theeducation and review session itself. Managers should developan evaluation tool (Figure 3) for surgical procedure coding tocollect feedback from the coders, pinpoint trouble spots, assessthe usefulness of the resource tools, and address areas ofconcern. Providing and reinforcing education and modifyingtools and processes and assessing their effectiveness helps toensure a smooth transition.
CONCLUSIONReplacing the ICD-9-CM coding system with the uniquecoding structure of ICD-10 will provide detailed data collec-tion opportunities for measuring patient care services andidentifying opportunities to improve patient care and out-comes. Nurses can help with the transition to this new systemby being informed participants and helping to educatepeers and minimize any negative effects that ICD-10 couldhave on surgical revenue. Nurses should be proactive, helpperform an ICD-10 assessment in their perioperativeservices department, and help educate peers by familiarizingthemselves with the system and identifying strategiesfor success. �Acknowledgment: The author wishes to acknowledge MarionSparks-McCall, BBA, RN, CNOR, CPHIMS, for her insight andexpert advice in the preparation of this manuscript.
Editor’s note: CPT is a registered trademark of the AmericanMedical Association, Chicago, IL.
References1. Whittle K. ICD-10 aftershocks: 4 challenges every CFO can expect
in the wake of go-live. http://www.beckershospitalreview.com/finance/icd-10-aftershocks-4-challenges-every-cfo-can-expect-in-the-wake-of-go-live.html. Published August 19, 2015. AccessedNovember 18, 2015.
2. Centers for Disease Control and Prevention. International class-ification of diseases, (ICD-10-CM/PCS) transition - background.http://www.cdc.gov/nchs/icd/icd10cm_pcs_background.htm. Publish-ed October 1, 2015. Accessed December 22, 2015.
3. Centers for Medicare & Medicaid Services. ICD-10 ombudsmanand ICD-10 Coordination Center (ICC). https://www.cms.gov/Medicare/Coding/ICD10/ICD10OmbudsmanandICD10CoordinationCenterICC.html.Published November 25, 2015. Accessed December 22, 2015.
4. Britt J, McReavy D. Preparing for ICD-10’s impact on your revenuecycle. Beckers Hospital Review. http://www.beckershospitalreview.com/white-papers/preparing-for-icd-10-s-impact-on-your-revenue-cycle.html. Accessed October 19, 2015.
5. ICD-10. Centers for Medicare & Medicaid Services. http://www.cms.gov/Medicare/Coding/ICD10/index.html?redirect¼/icd10.Accessed January 30, 2015.
Wing February 2016, Vol. 103, No. 2
184 j AORN Journal www.aornjournal.org

6. CPT-Current Procedural Terminology. American Medical Association.http://www.ama-assn.org/ama/pub/physician-resources/solutions-managing-your-practice/coding-billing-insurance/cpt.page. AccessedJanuary 10, 2015.
7. Butler R, Mullin R, Grant T, Averill R, Steinbeck B. ICD-10-PCSReference Manual, 3M Health Information Systems. Updatedfor Fiscal Year (FY) 2016. http://www.cms.gov/Medicare/Coding/ICD10/2016-ICD-10-PCS-and-GEMs.html. Accessed June 11, 2015.
8. ICD-9-CM diagnosis and procedure codes: abbreviated and fullcode titles. Version 32. Centers for Medicare & Medicaid Services.http://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/codes.html. Accessed December 23, 2014.
9. Abraham M, Ahlman J, Anderson C, et al. Current ProceduralTerminology CPT�2012 Professional Edition. Chicago, IL:American Medical Association; 2011.
10. 2016 Code Tables and Index. Centers for Medicare & MedicaidServices. http://www.cms.gov/Medicare/Coding/ICD10/2016-ICD-10-PCS-and-GEMs.html. Updated May 26, 2015. AccessedJune 11, 2015.
11. Pilato J. Charging vs. coding: untangling the relationship for ICD-10. J AHIMA. 2013;84:58-60.
Toni L. Wing, BSN, RN, CNOR, is an RN consultant,Coratek Perioperative Consulting, LLC, Johnson City, TN.As a consultant for Coratek Perioperative Consulting,LLC, Ms Wing has declared an affiliation that could beperceived as posing a potential conflict of interest in thepublication of this article.
February 2016, Vol. 103, No. 2 ICD-10 Medical Coding
www.aornjournal.org AORN Journal j 185

EXAMINATION
Continuing Education:ICD-10 Medical Coding: TheRole of Perioperative Services inAddressing ImplementationChallenges 1.6 www.aornjournal.org/content/cme
PURPOSE/GOALTo provide the learner with knowledge specific to the International Classification of Diseases, 10thRevision (ICD-10) medical coding system and its effects on perioperative services.
OBJECTIVES1. Describe ICD-10.2. Identify how ICD-10 affects perioperative services.3. Discuss how ICD-10 differs from ICD-9.4. Explain considerations for using ICD-10 in perioperative settings.5. Describe strategies for implementing the use of ICD-10.
The Examination and Learner Evaluation are printed here for your convenience. To receivecontinuing education credit, you must complete the online Examination and Learner Evaluationat http://www.aornjournal.org/content/cme.
QUESTIONS1. The term ICD-10 relates to diagnosis and procedure
coding used to bill for medical and surgical services.a. true b. false
2. The effect of ICD-10 on hospital revenue includes1. delayed billing.2. frustration for surgeons.3. denied claims.4. a lack of jobs for coding personnel.
a. 1 and 3 b. 2 and 4c. 1, 2, and 4 d. 1, 2, 3, and 4
3. Because the OR generates as much as _____ of ahospital’s overall revenue, it is vital to understand howICD-10 affects the OR.
a. 50% b. 60%c. 70% d. 80%
4. The unique coding structure of ICD-10-PCS (ProcedureCoding System) will provide1. detailed data collection.2. the ability to measure services provided to patients.3. performance comparison among surgical service lines.4. opportunities to improve patient care.5. in-depth research data.
a. 4 and 5 b. 1, 2, and 3c. 1, 2, 3, and 4 d. 1, 2, 3, 4, and 5
5. The ICD-10-CM (Clinical Modification) coding isrequired for all diagnosis and procedure coding.a. true b. false
186 j AORN Journal www.aornjournal.org

6. The differences in procedure descriptions in ICD-10as compared with a typical OR surgery schedule, theCurrent Procedural Terminology, and ICD-9 codinginclude that the new system has no1. differences between outpatient and inpatient
procedures.2. procedure descriptions containing terms named after
people.3. use of acronyms.4. diagnosis or disease process descriptions.5. combination procedure names.
a. 1, 3, and 5 b. 2, 4, and 5c. 2, 3, 4, and 5 d. 1, 2, 3, 4, and 5
7. The categories that nonclinical hospital informationmanagement coders will need to know to accurately selecta procedure code under the new system include1. the procedure category.2. the body system.3. the root operation.4. the approach or technique used.5. any device left in place at the end of the procedure.6. any qualifier or additional information.
a. 1, 3, and 5 b. 2, 4, and 6c. 2, 3, 4, 5, and 6 d. 1, 2, 3, 4, 5, and 6
8. Issues that hospital coders may encounter with regard tocoding surgical procedures that could delay reimburse-ment include1. the use of vague operative notes or poor clinical
documentation.2. the inability to determine the length of a procedure.3. translating common surgical procedure names into
root operations and surgical approaches.4. attempting to find anatomical locations.5. attempting to determine who the operating surgeon
was.
6. deciphering implant descriptions.a. 1, 3, and 5 b. 2, 4, and 6c. 1, 3, 4, and 6 d. 2, 3, 4, 5, and 6
9. An integrative team approach to adjusting to the newICD-10 coding system could include1. examining the surgery procedure list to identify
difficult-to-interpret procedure names.2. hiring extra staff members.3. establishing coder training sessions with the OR
team.4. creating a perioperative resource team that includes
nurses and surgical technologists who can be availableto answer coders’ questions.
5. developing a task team with hospital informationmanagement personnel to explore opportunities tostreamline the procedure coding process.
6. assuming responsibility for physician coding.a. 1, 3, and 5 b. 2, 4, and 6c. 1, 3, 4, and 5 d. 1, 2, 3, 4, 5, and 6
10. In focusing on the facility’s top five service lines to helpexpedite the coding process and minimize any projecteddisruptions to cash flow,1. perioperative team members should evaluate current
documentation practices.2. perioperative team members should look for oppor-
tunities to provide clarity to coding staff.3. managers or information technology personnel
should investigate surgical software capabilities.4. perioperative technology specialists can help create
data crosswalks.5. the charge master team should help identify risk areas
that could result in potential charge entry inaccuraciesand omissions.a. 1 and 2 b. 3, 4, and 5c. 1, 2, 4, and 5 d. 1, 2, 3, 4, and 5
February 2016, Vol. 103, No. 2 ICD-10 Medical Coding
www.aornjournal.org AORN Journal j 187

LEARNER EVALUATION
Continuing Education:ICD-10 Medical Coding: TheRole of Perioperative Services inAddressing ImplementationChallenges 1.6 www.aornjournal.org/content/cme
This evaluation is used to determine the extentto which this continuing education programmet your learning needs. The evaluation is
printed here for your convenience. To receive continuingeducation credit, you must complete the online Examinationand Learner Evaluation at http://www.aornjournal.org/content/cme. Rate the items as described below.
OBJECTIVESTo what extent were the following objectives of thiscontinuing education program achieved?1. Describe ICD-10.
Low 1. 2. 3. 4. 5. High
2. Identify how ICD-10 affects perioperative services.Low 1. 2. 3. 4. 5. High
3. Discuss how ICD-10 differs from ICD-9.Low 1. 2. 3. 4. 5. High
4. Explain considerations for using ICD-10 in perioperativesettings.Low 1. 2. 3. 4. 5. High
5. Describe strategies for implementing the use of ICD-10.Low 1. 2. 3. 4. 5. High
CONTENT6. To what extent did this article increase your knowledge
of the subject matter?Low 1. 2. 3. 4. 5. High
7. To what extent were your individual objectives met?Low 1. 2. 3. 4. 5. High
8. Will you be able to use the information from this articlein your work setting?1. Yes 2. No
9. Will you change your practice as a result of reading thisarticle? (If yes, answer question #9A. If no, answerquestion #9B.)
9A. How will you change your practice? (Select all that apply)1. I will provide education to my team regarding why
change is needed.2. I will work with management to change/implement
a policy and procedure.3. I will plan an informational meeting with physicians
to seek their input and acceptance of the need forchange.
4. I will implement change and evaluate the effect ofthe change at regular intervals until the change isincorporated as best practice.
5. Other: __________________________________
9B. If you will not change your practice as a result ofreading this article, why? (Select all that apply)1. The content of the article is not relevant to my
practice.2. I do not have enough time to teach others about the
purpose of the needed change.3. I do not have management support to make a change.4. Other: __________________________________
10. Our accrediting body requires that we verify the timeyou needed to complete the 1.6 continuing educationcontact hour (96-minute) program: _______________
188 j AORN Journal www.aornjournal.org