Embed Size (px)
Citation preview

10/21/2017
1
IBBM PBMS (Specialist)IBBM PBMS (Specialist)IBBM PBMS (Specialist)IBBM PBMS (Specialist)Basic Blood & Physiology ReviewBasic Blood & Physiology ReviewBasic Blood & Physiology ReviewBasic Blood & Physiology Review
Keith Samolyk CCP Emeritus
October 21st 2017
Q & O Meeting Portland OR
ETHICS OF BLOOD MANAGEMENTETHICS OF BLOOD MANAGEMENTETHICS OF BLOOD MANAGEMENTETHICS OF BLOOD MANAGEMENT
-First Do No Harm “Primum Non Nocere”
-Transfuse only when Absolutely Necessary
-Transfuse Only what’s Required and Sparingly
- Use the Freshest Blood Components Possible
- Minimal Sampling “Blood Draws” (Peds Tubes if poss)
-Avoid Waste/ Recover as much Autologous as possible
-Use POC Labs to Justify Transfusions
-Use Evidence Based Medicine to Guide Decisions
-It’s not Blood Management… It’s Fluid Management!
- NEJM Oct 2017 “Crisis in the Sustainability of the U.S. Blood System”
H Klein NIH

10/21/2017
2
***Multidisciplinary Approach***“PEOPLE IN THE CHAIN”
Door to Door HemovigilanceOr it Doesn’t Work at All !
Primary Doctor
Cardiologist
Admission Care Team
Anesthesia
Surgeon
Perfusion
ICU Care Team, Nurses Hospital Wide
Administrators
It only takes 1 weak Link in the Chain And a Patient is then Exposed to “Donor”
Allogeneic Blood Products!
Hawk-like Multidisciplinary Teamwork is the ONLY Way it Works
Treat every Patient like a JW with a Small BSA for Best Practice Outcomes!

10/21/2017
3
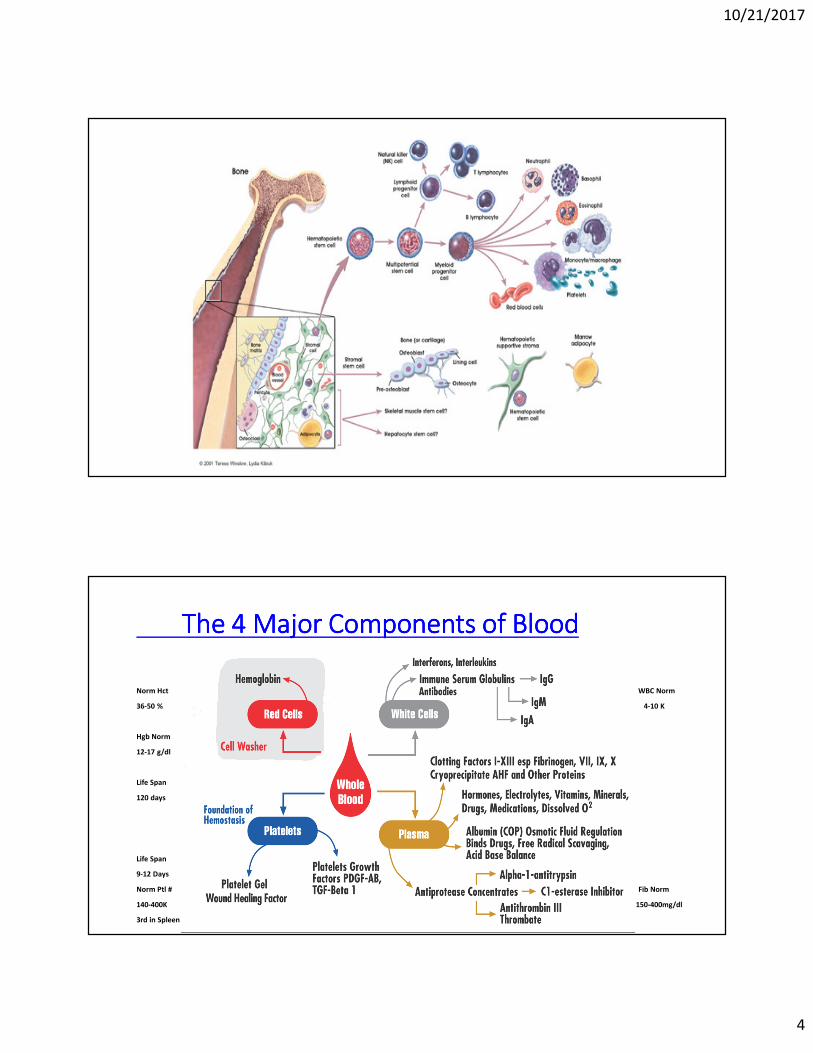
To Start What is Blood?
Whole Blood
Red Cells
White Cells
Platelets
Plasma
Hemoglobin
Hematocrit
Interleukins
Salts, Sugars,
Hormones, Vitamins, Enzymes, Minerals,
etc.
Interferons
Foundation
of
Hemostasis
Clotting Factors
Proteins
-COP- Albumin,
Globulins,
etc.
Fibrinogen Factors:
VII, VIII, IX, X, etc.
TThhee BBiigg PPiiccttuurree ooff WWhhoollee BBlloooodd
Protection
Wound Healing
10/21/2017
4
The 4 Major Components of BloodThe 4 Major Components of BloodThe 4 Major Components of BloodThe 4 Major Components of Blood
Norm Hct WBC Norm
36-50 % 4-10 K
Hgb Norm
12-17 g/dl
Life Span
120 days
Life Span
9-12 Days
Norm Ptl # Fib Norm
140-400K 150-400mg/dl
3rd in Spleen

10/21/2017
5
Systemic and Pulmonary Circulation Around
the body to the Organ Systems
Where the Volume Goes and Under what
Pressure, “Everything is Hydrokinetic”

10/21/2017
6
Arteries to Veins
VASCULAR ANATOMY

10/21/2017
7
But This is!
Where the Rubber Meets the Road
What is Microcirculation?
Microcirculation deals with the flow of blood from arterioles to capillaries or sinusoidsto venules. Blood flows freely between an arteriole and a venule through a vessel channel called a thoroughfare channel. Capillaries extend from this channel and structures called precapillary sphincters control the flow of blood between the arteriole and capillaries.
The precapillary sphincters contain muscle fibers that allow them to contract. When the sphincters are open, blood flows freely to the capillary beds where gases, nutrients and waste can be exchanged with body tissue. When the sphincters are closed, blood is not allowed to flow through the capillary beds and flows directly from the arteriole to the venule through the thoroughfare channel.
It is important to note that blood is supplied to all parts of the body at all times but all capillary beds do not contain blood at all times. Blood is diverted to the parts of the body that need it most at a particular time. For ex. when you eat a meal blood is diverted from other parts of your body to the digestive tract, or the Fight or Flight response ie: Tiger! CO = 5 lpm to 20 lpm
Vessel Sizes
Vessel Diameter in Microns
Arterioles 20-50
Capillaries 5-10
Sinusoids 30-40
Venules 30-40

10/21/2017
8
What Sizes
Arterioles
Small precapillary resistance vessels (10-50 µ) composed of an
endothelium surrounded by one or more layers of smooth muscle.
Richly innervated by sympathetic adrenergic fibers and highly
responsive to sympathetic vasoconstriction via both a 1 and a 2
post junctional receptors. Represent the major site for regulating
SVR systemic vascular resistance (***Vascular Tone***).
Primary function within an organ is flow regulation, thereby
determining oxygen delivery and the washout of metabolic by-
products. Regulated, in part, capillary hydrostatic pressure and
therefore influences capillary fluid exchange.

10/21/2017
9
Vaso-Action of the Arterioles in Regulating SVR
***Norm= 800-1200d/cm2***
Hypotension is NOT always Hypovolemia! (No Heavy Handed Fluids)
Push the SVR not the Starling Curve! normal 800-1200.
Hemodilution is the Enemy! It leads to Organ Edema and Organ
Dysfunction that leads to Morbidity and Mortality!
HD creates to a Dilutional Anemia and a Dilutional Coagulopathy that leads
to Blood Products and that leads to M&M!
Give as little Volume as necessary and keep the SVR High Normal if possible
Anesthesia Can Really
Help out a lot Here!

10/21/2017
10
What are capillaries?
Capillaries walls are thin and are composed of endothelium (a single layer of overlapping flat cells). Oxygen, carbon dioxide, nutrients and wastes are exchanged through the thin walls of the capillaries.
The flow of blood is controlled by structures called precapillary sphincters. These structures are located between arterioles and capillaries and contain muscle fibers that allow them to contract. When the sphincters are open, blood flows freely to the capillary beds of body tissue. When the sphincters are closed, blood is not allowed to flow through the capillary beds
Image courtesy of Carolina Biological Supply/Access
Excellence
Capillary Size
Capillaries are so small that red blood cells can only travel through them in single file.
•5-10 microns in diameter.

10/21/2017
11
Hct 40%
Hct23%
Normal Hct = 40+/-%
For Every 1000 mLsof Crystalloid Fluid
Given to Patients
Only 200-300 mLs will remain Intravascular in 30-45 mins
Dilution leads to organ dysfunction and a coagulopathy
Chappell Fluid Article: Trauma patient study by Lowell et. al.
Hemodiluted Hct = +/- 23%
Tonicity of Fluids
• Osmolarity
• Ions (osmotic force)
• Proteins (oncotic force)
• Hypotonic
• Cells placed in a hypotonic solution swell
• Isotonic
• Hypertonic
• Cells placed in a hypertonic solution shrink

10/21/2017
12
Oncotic States
ALBUMIN IS IMPORTANT
Albumin is derived from adult human plasma. It is an oncotic protein in normal blood
serum concentrations of 3.6- 5.2 g/ dl that contributes to a normal colloidial osmotic
pressure COP of > 20 Torr. Levels below 3.2 gdl are generally considered dangerous
Serum albumin is increased in dehydration, and decreased in malnutrition, chronic liver
disease, malabsorption, nephrotic syndrome, SLE, burns. Is a Function of Nutrition.
During extracorporeal circulation a cardiovascular perfusion related phenomenon of
"third spacing" a condition where extracellular water migrates into the interstitial
spaces presents itself.
When third spacing is identified, e.g. fluid balances, low protein levels, additional
Albumin may be administered to regain fluid lost to the interstitum.
When injected intravenously, 50 mL of 25% albumin draws approximately 175 mL of
additional fluid into the circulation within 15 minutes, except in the presence of
marked dehydration.

10/21/2017
13
Albumin Albumin Albumin Albumin –––– Physiological rolePhysiological rolePhysiological rolePhysiological role
• Major functions
• Most abundant protein in plasma (69 kDa)
• +/- 80% of plasma colloid osmotic pressure
Normal COP is 18-22 mmHg (and Hemodilution really drops it)
• Transport and sequestration of bilirubin
• Transport of fatty acids, hormones, vitamins, enzymes, drugs (Warfarin, Diazepam, Digoxin, NSAIDS, Midazolam, Thiopental and others)
• Antioxidant and Free Radical Scavenger
• Inhibit Endothelial Cell Apoptosis and influences the Microcirculation by modifying the capillary permeability “by Protecting the Glycocalyx”
• Buffer in Acid Base Balance (as it fixes to H+ ions)
• No Maximal Dose and has No Effect on Hemostasis
gm/dl mmHg % of COP
Albumin 4.50 21.80 78%
Globulins 2.50 6.00 21%
Fibrinogen 0.30 0.20 1%
Total 7.30 28.00 100%
Plasma Protein Effects on Total
Colloid Osmotic Pressure
Plasma Proteins: The Key Elements of COP

10/21/2017
14
Edema: Most common clinical manifestation of an
Imbalance of forces at the capillary wall
Excess accumulation of fluid in the interstitial space that has not been
readsorbed into capillaries or taken up by the lymphatics
The 4 Causes of Edema include
• Obstruction
• Permeability or change in reflection coefficient
Increased protein permeability results in an imbalance
• Occurs in trauma, thermal injury, inflammation
• Life threatening manifestations - endotoxic shock, ARDS
• Plasma Proteins
• Reduction in circulating plasma proteins, esp Albumin• Liver dysfunction, malnutrition, or acute alteration of fluid status
• Albumin attenuates extravasation of fluid out of intravascular space
into the interstitial space
• Capillary pressure27
STARLINGS LAW
10/21/2017
15
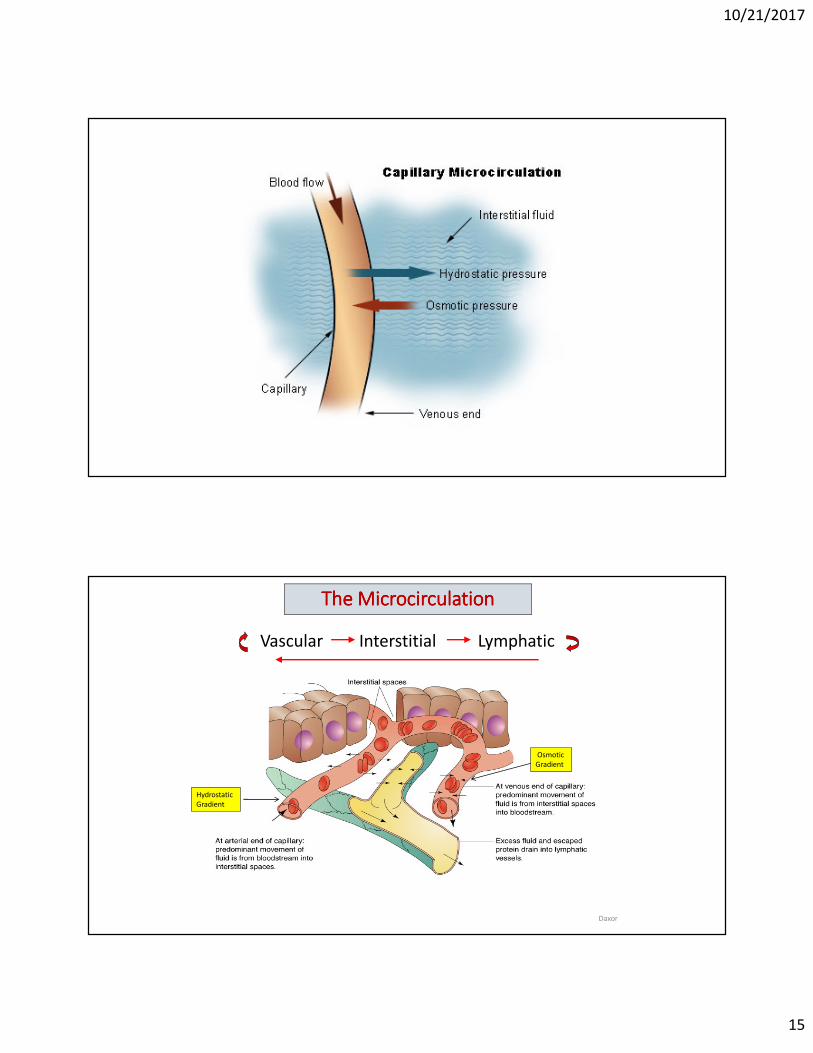
The Microcirculation The Microcirculation The Microcirculation The Microcirculation
Daxor
Vascular Interstitial Lymphatic
Hydrostatic
Gradient
Osmotic
Gradient

10/21/2017
16
The Lymphatic
System
The Loss of Protein and Lymphatic Flow
Proteins
Lymph Flow

10/21/2017
17
The Lymphatic System Is a network of conduits that carry a clear fluid called lymph. It also includes the lymphoid
tissue that the lymph travels through. Lymphoid tissue is found in many organs,
particularly the lymph nodes, and in the lymphoid follicles associated with the digestive
system such as the tonsils. The system also includes all the structures dedicated to the
circulation and production of lymphocytes, which includes the spleen, thymus, bone
marrow and the lymphoid tissue associated with the digestive system.
The dissolved constituents of the blood do not directly come in contact with the cells and
tissues in the body, but first enter the interstitial fluid, and then the cells of the body.
Lymph is the fluid that is formed when interstitial fluid enters the conduits of the
lymphatic system. The lymph is not pumped through the
body like blood, it is moved predominately by the
contractions and movements of skeletal musclesThe lymphatic system has three interrelated functions. It is responsible for the removal of
interstitial fluid from tissues. It absorbs and transports fatty acids and fats as chyle to the
circulatory system. The last function of the lymphatic system is the production of
immune cells, such as lymphocytes, including antibody & producing monocytes. Diseases
and dysfunction/obstruction of the lymphatic system can cause swelling , edema and
other symptoms. Problems with the system can impair the body's ability to fight.
Fluid Overload is an Independent Predictor of Mortality
Chappell: A Rational Approach to Perioperative Fluid Management. Anesthesiology 2008: 109:723–40

10/21/2017
18
Clinicians can Reverse the Fluid Shifts that cause 3rd Spacing from Hemodilution and optimize the Patient’s Red Cell MassPatient’s Red Cell MassPatient’s Red Cell MassPatient’s Red Cell Mass, so that allogeneic blood products to treat a Dilutional Anemia and a Dilutional Coagulopathy can be minimized. *Extubate ASAP!Extubate ASAP!Extubate ASAP!Extubate ASAP!
ALBUMIN
Osmitrol
LASIX
Mannitol
HEMOCONCENTRATORS
Tools to Minimize Hemodilution
Chappell Fluid Article

10/21/2017
19
The Fluid Gate Keeper
The “Glycocalyx” the New Frontier
The Endothelial Glycocalyx, is a gel-like layer that coats the inner surface of the endothelium throughout the entire vascular tree less than 100nm thick
and is made up of negatively charged carbohydrate polymeric glycoproteins and
plasma soluble molecules produced by bacteria, epithelia and other protein cells.
Think of it as a non-stick Teflon coating on the luminal endothelial surfaces. The slime on the outside of a fish is actually considered to be a Glycocalyx.
The Glycocalyx layer contains very fine hair-like structures that contribute to cell-
cell recognition and transmit intracellular adhesion changes and shear forces to
the endothelium, ultimately regulating nitric oxide release, it consists of a wide
range of enzymes and proteins that regulate Leukocyte and Platelet adherence.
Its principal role in the vasculature is to maintain plasma and vessel wall homeostasis and equilibrium.
The Glycocalyx

10/21/2017
20
Glycocalyx has multiple functions: it mediates nitric oxide synthesis and superoxide
dysmutation, it acts as a protective "sieving" barrier, inhibits platelet adherence,
and coagulation, and it regulates inflammation by preventing leukocyte adhesion to the vessel walls.
One of its most important functions is to keep the endothelial wall responsive to
changes in vascular fluid dynamics within the vascular endothelium as it shields the vascular walls from direct exposure to blood flow shear stress, while serving as a vascular permeability barrier.
The Glycocalyx
A Non-Stick Coating Unless Disrupted
The Glycocalyx can get damaged from sheer stress decreasing NO availability,
increased oxidative stress, leakage of macromolecules, increased platelet
adherence, thrombin generation, and increased leukocyte adhesion, all of which set the stage for inflammation and thrombotic events. These damaged
Glycocalyx areas increase perivascular edema leading to a leakage of fluids and
proteins which causing tissue damage and loss of capillaries.
*Paper “Endothelial Glycocalyx and CPB” JECT Oct 2017 Myers & Wegner

10/21/2017
21
Its hypothesized that hypoxic perfusion of the Glycocalyx is sufficient enough to initiate a degradation mechanism of the endothelial barrier. Studies found that flow of oxygen throughout the blood vessels did not have to be completely absent (ischemic hypoxia), but that minimal levels of oxygen were sufficient enough to cause the degradation. Anesth Volume Loading Patient Reduces the Glycocalyx
Shedding of the Glycocalyx can be triggered by Fluid Shear Stress (FSS) ie the start up motion of an RBC in a tight capillary bed or the crushing passage of a WBC or Microbubble, and inflammatory stimuli such as Tumor necrosis factor (TNFa).
Whatever the stimulus, shedding of the Glycocalyx leads to a drastic increase in vascular permeability. This permeability enabling the passage of macromolecules and other harmful antigens leading to 3rd spacing, edema, organ edema and dysfunction. So it’s Really Important to Protect it!
Glycocalyx Shedding = Vascular Permeability.
Normal Abnormal

10/21/2017
22
APATHYAPATHYAPATHYAPATHYApathy is a state of indifference, or the
suppression of emotions such as concern,
excitement, motivation and passion. An
apathetic individual has an absence of
interest or concern to emotional, social,
or physical life. Don’t be Apathetic…
Change the Paradigm at your Institution.
Be The Leader in Blood Management!
Remember Hemodilution leads to Edema & Blood Products! Remember Hemodilution leads to Edema & Blood Products! Remember Hemodilution leads to Edema & Blood Products! Remember Hemodilution leads to Edema & Blood Products! And If its not yours its an “Organ Transplant” And If its not yours its an “Organ Transplant” And If its not yours its an “Organ Transplant” And If its not yours its an “Organ Transplant” with with with with Consequences! Consequences! Consequences! Consequences!
Do your best to avoid heavy handed Do your best to avoid heavy handed Do your best to avoid heavy handed Do your best to avoid heavy handed HemodilutionHemodilutionHemodilutionHemodilution!!!!Your decisions effect the patient for the rest of their life! Your decisions effect the patient for the rest of their life! Your decisions effect the patient for the rest of their life! Your decisions effect the patient for the rest of their life!

10/21/2017
23
Thank you for your time!Thank you for your time!Thank you for your time!Thank you for your time!





























