Embed Size (px)
Citation preview
340
graphically to have alterial occlusions, the clinical his
tOIY and exam can be relied upon to detect appropriate patients for rr-PA.
The Furure of Stroke The approval of rr-PA as the first accepted treatment for acute stroke is only the beginning. The limitation of the 3-hour window reduces the feasib il ity of administering the drug to all patients who present with stroke symptoms. The first step towards improving stroke treatment lies within education of the general population and health care providers. Stroke has to be thought of as an emergency that requires immediate medical intervention. Most patients do not recognize the symptoms of stroke. It is crucial that the general population identify the warning signs of stroke and associate the signs with a "brain attack."
The idea of administering a "stroke cocktail" in the treatment of acute stroke is not far from reality. The abil ity to preserve viable brain tissue in the area of the infarction is the concept behind neuroprotection. Neuroprotection can be used to extend the therapeutic window so that a greater numbers of patients can be treated. It might also offer some benefit in the treatment of
hemorrhagic stroke. By attacking the mecharusm of stroke at various sites, the likelihood of reducing the degree of deficits and improving the functiona l outcome is greater.
References 1. Adams HP Jr, Brott TG, Furlan A), et al. Guidelines
for thrombolytic therapy for acute stroke: a supplement to the gUidelines for the management of patients with acute ischemic stroke. Circulation ] 996; 94,1167.
2. Brott TG, Haley EC Jr, Levy DE, Urgent u,erapy for stroke: parr 1: pi lot study of tissue plasminogen activator administe red within 90 mi nutes. Stroke 1992; 23,632.
3. caplan L, Mohr JP, Kistler JP, Korosue K. Should thrombolytic therapy be the first-line treatment for acute ischemic s(Ioke? thrombolysis--not a panacea for ischemic stroke. N Engl ] Med 1997; 33n309.
4. Collen D, Strassen JM, Marafino BJ Biological properties of human tissue-type plasminogen activator obrtained by expression of recombinant DNA in manunalian cells. J Pharmacol Exp Ther ]984; 231:
146.
5. del Zoppo G. Acute stroke: on the threshold of a
therapy' N Engl J Med 1995; 333,1632-1633.
6. del Zoppo G, Copeland BR, Waltz TA, Zyroff J, Plow EF, Harker LA. The beneficial effect of intra carotid
urokinase on acute stroke in a baboon mode l. Stroke 1986; 17,638.
7. del Zoppo G, Poeck K, PeSSin MS, ct al. Recombi-
nant tissue plasminogen activator in acute throm
botic and embolic stroke. Ann Neurol ]992; 32:78.
8. Feldmann E, Gordon N, Brooks )M, et al. Factors associated with early presentation of acu te stroke. Stroke 1993; 24,1805.
9. Hacke W, Kaste M, Fieschi C, et al. Randonllsed double-blind placebo~controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Lancet 1998; 352,1245.
10. Haley EC, Brott TG, Sheppard GL, et al. Pilot randomized trial of tissue plasminogen activator in acute ischemic stroke. Stroke ]993; 24:1000.
11. Haley ECJr, Levy DE, Brott TG, et al. Urgent therapy for stroke: part II: pilot study of ti ssue plasminogen activator administered 91-]80 minutes from onset. Stroke 1992; 23,641.
]2. NINDS rt-PA Stroke Srudy Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995; 333,1581.
13. NINDS TPA Stroke Study Group. Generalized efficacy of rt-PA for acute stroke. Stroke 1997; 28,2119.
14. ]{jngelstein EB, Biniek R, WeUler C, Ammeling B,
Nolte PN . Type and extent of hemispheric brain infarctions and clinical outcome in early and delayed middle cerebral artery recanalization. Neurology
1992; 42,289.
15. Sussman B, Fitch T. Thrombolysis with fibrinolysin in cerebral arterial occlusion. JA1v1A 1958; 167:1705.
]6. The E(ASS Study Group. European cooperative acute stroke study (ECASS) rt-PA-thrombolysis in
acute stroke study design and progress report. EUr J Neu rol 1995; 1.213.
17. von Kummer R, Hacke W. Safety and efficacy of intravenous tissue plasminogen activator and heparin in acute middle cerebral artery stroke. Stroke 1992; 2H46.
]8. Zivin JA, Fisher M, DeGirolami U, Hemenway CC, Stashak KA. Tissue plasminogen activator reduces neurological damage aner cerebral embolism. Science 1985; 230,1289.
12:55 pm
IA Stroke Therapy: Why and Why Not
Brian Berger, MD
Radiology Consultants
Nashville, Tennessee
1:20 pm
IA Stroke Therapy: The Brain Plumbing How-to
Guide Gary M. Nesbitt, MD
Oregon Health Sciences University
Portland, Oregon

Introduction Intraarterial CIA) thrombolysis has shown promise for the treatment of acute stroke, although the technique is not yet in widespread use. Despite the caveat that this is a procedure in evolution with only preliminary scientific evidence, applying certain principles in the appropriate patient setting can make significant strides in improving outcome in patients with acute stroke. This presentation will discuss some of the evidence supporting intraarterial thrombolysis, the mechanics of the procedure, which patients and sellings are appropriate, and some problem solving advice.
Rationale Stroke represents a major cause of death in the United States and a Significant cause for long-term morbidity and dependence. The success demonstrated in the systemic fibrinolytiC treatment of myocardial infarction nearly two decades ago raised the possibility of applying fibrinolysis in the treatment of acute ischemic stroke with significant deficit. This led to numerous intravenous (IV)
thrombolysis trials for acute stroke, and the recent positive randomized trials of IV tissue plasminogen activator (t- PA) which demonstrated significant improvements in outcome within 3 hours of stroke onset (31). No benefn has been shown with IV treatment between 3 and 6 hours (8). Concurrently, the continued development of microcatheter delivery systems during the past 15 years raises the possibility of applying these fibrinolytics directly to the thrombus in an effort to improve recanalization rates and extend the treatment window in acute
stroke. The different responses of the brain and heart to vascular insults make direct application of the paradigm from one to the other risky.
Treatment of stroke is contemplated because of the poor prognosis associated with the natural history of the disease. Middle cerebral artery (MCA) strokes without treatment carry an 80% risk of not returning to a favorable lifestyle, although the acute mortality is relatively low (12%- 28%) (43,7,17). Those who do recover \vell from a severe deficit do so early, suggesting rapid spontaneous recanalization plays an important role in patient outcome (43). The results in posterior circulation infarcts are even worse. Left untreated, basilar artery thrombosis has a high mortality so the risks of conservative therapy are substantial. In Hacke's series, only 3 of 22 03.6%) survived vertebrobasilar occlusion given conservative, conventional treatment (21).
At present, thrombolYSiS for stroke in the United States is only approved as rt-PA administered intravenously within 3 hours fmm symptom onset, based on one randomized trial (31). Other trials have failed to show benefit and still others have shown worsening of outcomes \vith intravenous thrombolytic treatment (20,29,14). The recanalization rate for IV thrombolYSis is low, ranging from 210/1)-
43%, although neither vascular occlusion nor recanalization was documented in any of the recent major IV thromoolysis trials (35), Anecdotal and case series evidence have
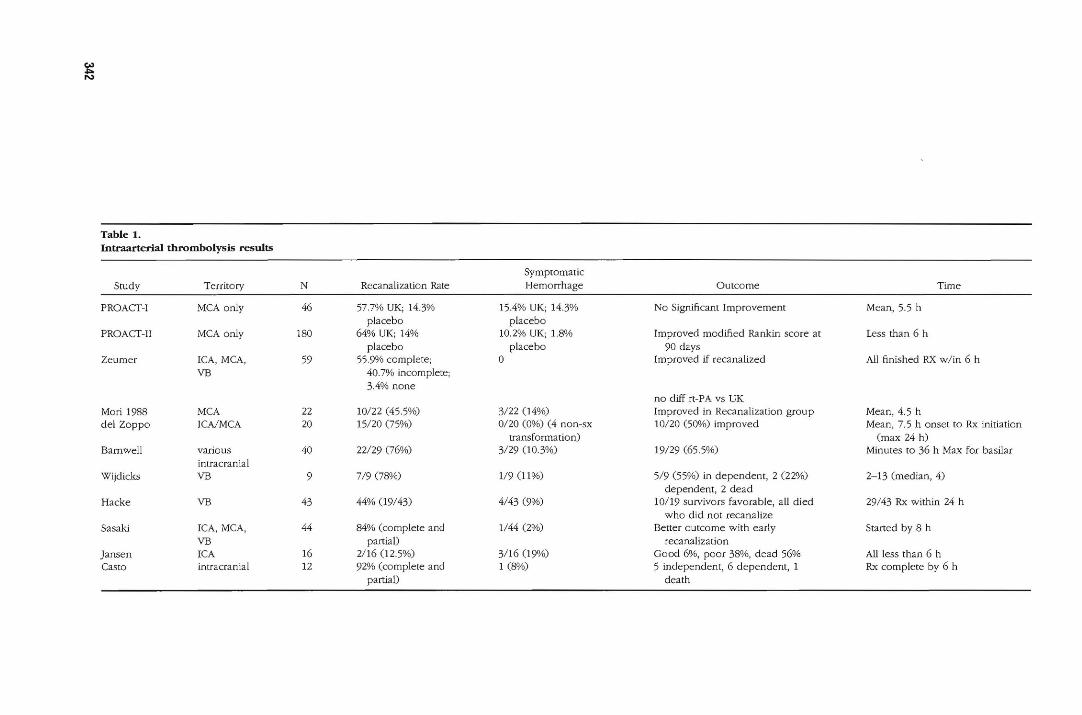
shown the efficacy of intraarterial thromoolysis in recanalization v.rith results from 440/1)-87% (see Table 1) (11,17,44,28,12,3,40,25,35,21,6). Most of these studies suf
fer from lack of intemal controls and nonrandom patient selection but do show a trend.
The best suppOtting evidence comes from the ~'o randomized control studies of intraarterial thrombolysis using prourokinase. These studies demonstrated a rela
tively high recanalization rate (57.7% and 67% vs. 14%
and 17% for placebo), which was statistically significant in the larger PROACT II trial. The primary endpOint, the modified Rankin score at 90 days, demonstrated a 40%
rate of favorable outcome (Rankin 0, 1, or 2) in the treatment group compared 25% for the controls. This difference was statistically Significant. The rate of symptomatic hemorrhage was 10.2% for the treated group compared to 1.8% for heparin-treated control group
(11,m. Theoretically, treatment with intraarterial thromboly
sis allows recanalization with a potentially lower throm
bolytiC dose with direct application. With angiographic monitoring, treatment can be discontinued with successful recanalization, or redirected as warranted, and a
decrease in the systemic fibrinolytic effect is possible with this lower overall dose (34). Intraarterial thrombol
ysis is best suited to larger vessel occlusions, such as the MCA or basilar, where TV treatment may be less effective
(37,38).
On the minus Side, intraarterial therapy is much more invasive and takes additional time to initiate compared to intravenous thrombolysis. Direct comparison of intravenous with intraarterial thrombolysis has not been done,
although one study compared their results of IV versus intracarotid thrombolysis versus local high-dose thrombolysis. Local intraarterial thrombolysis was superior (84% response) to intracarotid 01%) and intravenous (11 %) administration in recanalization, although the IV and intracarotid patients had been treated with relatively low-dose, non-current regimens, so the comparison is weak (5). It may be that intraarterial and intravenous therapy could be complementary, with some authors suggesting early intravenous therapy to capitalize on the rapidity with which it can be administered, followed by further intraarterial therapy without delay (6).
Other disadvantages of intraarterial delivery of thrombolytiC include inherent risks for angiography and selective catheterization, the paucity of facilities and personnel trained to perform the procedure, and time reqUired to initiate treatment. The risks of angiography alone are minimal, with a complication rate of approximately 1.4%, and probably lower with current techniques (27,15). No direct microcatheter-related complications were reported in the PROACf trial (11). Depending on the time of day and location, the intraarterial thrombolysis probably add" another 30 - 60 minutes before beginning definitive treatment, compared to intravenous therapy. Our experience demonstrates that, by rapid ER assessment of severity and immediate transport from CT
341


344
given and a Foley catheter placed. Suction should be checked before initiation of the procedure because vomiting is a frequent sequela. Standard inrerventional neu· roradiology setup, including constant-pressure drip sa· line should be initiated. Some medications may need to
be ordered from a pharmacy in advance if not normally maintained in the angiography area. These details can be simultaneously addressed so as not to delay the proce·
dure. A predefined plan with specific roles for the interventionist, neurologist, technologist, and nurse is recommended.
Routine use of a femoral sheath has several advantages: it allows easy exchange of gUidecatheters, takes onJy a minute to insert, and can greatly facilitate navigation of the guide catheter with better torque control. J[
also provides the benefit of continuous, accurate pressure monitoring. The femoral sheath is sutured in place and left in overnight, allowing for initial thrombolytiC anticoagulation to resolve.
Angiographic Evaluation Becduse time is of the essence, the angiographic evaluation should be limited to evaluation of the level of occlusion and the presence and adequacy of circle of Willis, pial, and external carotid collaterals. Underlying this assessment is a weighing of the relative risks of the occlusion and the risks of thrombolysis. We perform
angiography of the clinically obstnlcted vessel first to determine obstruction, and chen assess the collateral circulation. By first assessing the involved vessel, the amount of additional assessment may be limited. If the occlusion involves or is proximal to the circle of Willis, then the remaining components of the circle need as~ sessment. If the occlusion is cUstal to the circle (Ml, P2, A2, or beyond) then only the pial collaterals require evaluation.
Poor or absent pial collaterals implies that the area of brain affected by the large vessel occlusion has been without circulation and is more likely unsalvageable. The resulting dense ischemia also raises the risk of hemorrhage with subsequent reperfusion, with or without arterial thrombolysis. Conversely, abundant pial or leptomeningeal collaterals signal brain receiving at least some supply, which may benefit from reperfusion (36). Parenchymal blush is also evaluated as a marker for
tissue perfuSion. In the case of a suspected MeA occlUSion, the finding
of normal angiography with patent ICA, MCA, and ACA warrants funher evaluation into the cause of the symptoms. Spontaneous lysis of thrombus, small vessel infarct, venous thrombosiS, and hypoperfusion will present with infarction and clinical stroke. Small branch occlusions will often be seen with spontaneous lysis of a more proximal occlUSion, whereas small vessel infarct or hypoperfusion is angiographically occult. Venous thrombosis often can be differentiated on the screening CT if peripheral hemorrhages are evident or a dense dural sinus is presenL The venous phase of angiography
can demonstrate venous occlusion if not recognized or evident prospectively. The last alternative to conSider in {he face of a negative angiogram is the case of imaging the wrong vessel territolY. This may be as simple as right~left confUSion, but more commonly is caused by
anterio r versus posterior Circulation, as the symptoms can, at times, be misleading, and angiographic evalua
tion of the other circulation is warranted.
Navigation to the Thrombus
The use of a guide catheter with a larger ID (O.050-inch
or larger) facilitates performance of road mapping via injection through the gUide catheter over the microcathetee. This makes for easier pOSitioning of the microcatheter, repeats assessment angiography, and minimizes the degree of contrast staining of the basal ganglia. A variety
of microcatheters and micro-guide wires are available. We favor the use of a standard end-hole catheter as it allows precise placement of the lytic agent. The wire
should have a gentle curve at the tip for some degree of torque control. This curve also helps prevent inadveltent entry and puncture of the small perforating arteries. An
understanding of the co rrela tive vascular and skull anatomy is crucial for recogn izing and reaching the occlusion. Proper projection selection initilally involves standard AP and lateral projections, as those are most
familiar. Some obliquity may be necessary to separate
branches and optimize visualization of the microcatheter and wire.
Because the occluding thrombus will prevent adequate opacification of the artery, navigation of the wire
and microcatheter are often "blind." Thorough knowledge of the arterial anatomy, particularly of the small
lenticulostriate and thalamostriate (the aptly named "perforators") and the anterior choroidal artery is essential to avoid or recognize inadvertent puncture. Knowledge of the arterial anatomy with respect LO the osseous anatomy is important, especia lly if the patient is unable to remain motionless. Abnormal wire or catheter position should raise the possibility of small vessel entry or may be the first sign of perforation. Other signs are contrast extravasation or Cushing response (bradycardia and hypertension) from the patient A small , slow test injection through the microcatheter minimizes overdistension of a
small vessel that may rupture. If a perforation is detected, the wire or microcatheter should not be Withdrawn, as the device may be occluding the opening. Vital s igns and the patient are assessed, urokinase is stopped and heparin reversed with protamine sulfate. Guide wire or microcatheter perforations may be benign, but with throm
bolysis and systemic anticoagulation, this is unlikely. Any resultant hypertension should be treated. In this
case, a neurosurgeon is consulled while the patient is stabilized. If bleeding or deterioration continues, coils can be placed into the perforation. This may occlude the artery; however, an occluded artery is preferred to a
bleeding one.

Thrombolysis The lhrombus characteristics may alter the efficacy of thrombolysis. Fresh clot, so-caJled red thrombus, responds much more rapidly to thrombolysis. Older clot,
white thrombus, is more typical of emboli , has more
fibrin cross links, is relatively plate let rich and plasminogen poor, and generally does not respond as well. The
volume of (he thrombus also probably contributes to the effectiveness of thrombolysis with a larger clot requiring
more time and thrombolytic agent. A larger thrombus is
also more likely to involve branches with poor collateral circulation.
Three main thrombolytics are available in various forms: streptokinase (STK), urokinase (UK), and tissue plasminogen activator (t-PA). None has proven clearly superior for intld.arteriai use. All currently used agents work through the same mechanism of activating the body's own fibrin-degrading enzyme, plasmin. Plasmin itse lf is too short-lived to use clinically. To lyse the clot, the activator must have ava ilable substrate (plasminogen), which is found w ithin the dot and in Circulating plasma. When the plasminogen within the clot has been used, more must be supplied by flowing blood, as even high concentrations of activator without substrate will
not lyse clot. Streptokinase (STK) has been largely abandoned for
acute stroke after several intravenous trials were halted after shOWing unacceptable rates of imracranial hemorrhage and early death (29,39), Urokinase (UK) has been readily available and less expensive lhan rt-PA as it is currently supplied. Doses for standard imraarterial UK range from 180,000 to 1.5 million units, with 1- 1.5 million units a common maximum dose (3,6,28,40,44). Prourokinase, which is a proenzyme similar to UK, is the most extenSively studied in int raarterial thrombolysis trials 07,11). Urokinase is not currently available as its
potential for infectious agent transmission is being reassessed.
Tissue plasminogen activator is derived from recombinant DNA, and directs most of the anticoagulant activity at the clot itself rather than having a systemic effect and accounts for its favored use in rv th rombolysis tria ls. The systemic half-life of rt-PA is 5 minutes, but the thrombus-dissolving acLion by the bound rt-PA lasts longer. In case se ries comparing UK LO rt-PA for IA thrombolysis, Zeumer found no difference in reca nalization between UK and rt-PA for intracranial occlUSion, but the type of occlusions included in the rt-PA group were probably more difficult to treat (44). One rrtillion units of UK is considered approximately equ ivalent to 10 mg rt-PA, but direct human dose equivalents are not established, and an equiva lent dose might be Significantly lower, even for different preparations of rt-PA (9). Dose ranges are typically from 10 to 20 mg, although doses over 100 mg have been used intraarterially 06,44).
Heparin usage and dose have not been clarified and, so far, conflicting results persist. The PROACf trial demonstrated increases in the recanalization and hemor-
rhage rate with higher heparin doses (100 IU/ kg bolus followed by 1000 IU/ hour X 4 hours) compared to lower doses (2000 IU bolus fOllowed by 500 IU/hr X 4 hours)
and, to minimize risk, the dose in the follow~up study was reduced (1). A trade~off exists between increased hemorrhage risk and prevention of rethrombosis with heparin. The rationa le for the use of heparin during thrombolysis is to prevent clot formation on the catheter, and more importantly, prevention of f·urther thrombus formation during thrombolysis. Thrombus is a potent initiator of further thrombosis and by exposing this surface, may potentiate rethrombosis.
Heparin is usua lly given when beginning microcatheter navigation. We give a 2000-U bolus, followed by 500 U/h for 4 hours, then no funher heparin afler the PROACT low-dose and PROACT-II gUidelines 07,11). Before infUSion, the UK is injected into a ste rile 10-mL syringe through a 5-pm-pore filter needle to remove undissolved particulates. This syringe is connected to the catheter and a 1-mL syringe via a 3-way stopcock. The solution is aspirated from the 10-rnL syringe into the I-mL syringe, then injected into the catheter from the I -mL syringe. Most favor embedding the rrticrocatheter within [he clot rather than just at the proximal face. The PROACT studies forbade clot penetration, which may account fo r a lower recanalization rate. A variation we favor involves traversing the clot, injecting a small O -rnL) bolus of
urokinase distally, then lacing the thrombus with a second l -rnL aliquot as the microcatheter is slowly with
drawn into the th rombus, stopping in the proximal third. The thrombolytic is given slowly in one of two prin
Ciple fashions, continuous infusion or pulse-spray, neither with proven superiority for intracranial use. We prefer a gentle pulse-spray delivery as favored in peripheral thrombolysis with approximately O.05-mL boluses given at 5-1O-second intervals from the 1-rnL syringe intermittently over the course of several minutes. This is continued until approximately 250,000 U of urokinase have been injected and repeat angiography performed through the guide catheter. The postulated advantage is that the small puff forces some agent deeper into the clot ra the r than s imply bathing the surface. The disadvantage is that if the injected volume exceeds the capacity of the unthrombosed segment, much of it will reflux and have only systemic effect. We also advocate clot disruption by gentle passage of the wire and catheter through the thrombus intermitte ntly after 10- 15 minutes, with the purpose of mixing the UK into the thrombus and givi~g the clot more surface area for fibrinolysis to occur. The constant infusion technique can be used with an infus ion pump set to deliver a specified volume in a set time (eg, 250,000-750,000 U/h UK; 5 mglh rHA). This has the advantage of supplying a constant supply of thrombolytic to the cJot. One mill ion units is generally regarded as the upper limit for urokinase; however, many authors have exte nded this limit to 1.5 million units at times.
The angiographic endpOint is restoration of antegrade flow. Complete dissolution of the clot is not a
345

346
necessary outcome if good flow is established. Branch occlusions beyond M2 or P2, or perforating branches originating from the vertebral or basilar arteries are generally not pursued. Branch occlusions that involve eloquent territory, such as Broca's area, midbrain, or the motor strip, may warrant a more aggressive approach.
An occlusion that does not resolve despite near maximal thrombolytic infusion prompts a reevaluation of the situation. An underlying stenosis may be present, particularly in the posterior circulation, with angioplasty helpful to relieve stenosis before maximum thrombolysis. Other considerations include presence of old thrombus, which is more resistant to thrombolytics. Emboli, which are calcified, mycotic, or composed of myoma or plaque, will, of course, not respond well to any degree of thrombolysis and, because of potential wall damage, may have increased hemorrhage risk. Tnnovative approaches in these cases have included snaring the clot. However, the additional risks of such maneuvers must be weighed. Unlike in the coronary system, primary angioplasty is
usually not regarded as a first line of treatment because of the larger amount of thrombus and the presumed further embolization of thrombus distally. Tn areas with branches, angioplasty may tightly pack clot into tl1e side
branches and only worsen the ischemia. Adjunctive agents such as abcL'{imab (19) may be useful here, but the added risk of hemorrhage must be considered.
After Care Postthrombolysis gUidelines adapted from the IV NIH rt-PA trial can be used, although no strict ru les are published (31). Close monitoring of the blood pressure is maintained with the goal systolic BP less than 185. If good flow has been achieved and there is no hemodynamic stenosis, the blood pressure may be lowered even further. Heparin is usually discontinued and allowed to reverse spontaneously, or at most, continued for 4 hours . A postthrombolysis Cf is obtained to evaluate for hemorrhage. Repeated microcatheter injections can stain the infarcted basal ganglia with contrast, Simulating hemorrhage; however, this is typically more dense than blood . The sheath is left in until the thrombolytic and anticoagulant effect has time to wear off, generally overnight. Good intensive care nursing with close monitoring, in
cluding the groin, is necessary because serious injuries and death have occurred with inadvertent sheath with
drawal.
The Future Certainly intraarterial thrombolysis has not yet been perfected or rigorously proven. The preliminary PROACT II results are promising and we await the final analysis. Further studies will follow to further refine the technique. Factors that we find helpful, such as mechanical
disruption, need to be proven, hopefully augmenting the early success. Further refinements may be made in imaging and current techniques will be evaluated to triage patients to IV or LA treatment, and divert those with a
poor response and high risk to some other treatment. Other reperfusion techniques may augment or supplant current techniques. Nonetheless, treatment for acute stroke has come.
References 3. Barnwell SL, Nesbit GM, Clark \VM. Local thrombo
lytic therapy for cerebrovascular disease: current Oregon Health Sciences University experience Quly 1991 tllrough April 1995). ]VIR 1995; 6(suppl}78S-82S.
4. Brott TG, Haley EC, Levy DE, et aJ. Urgent therapy for stroke. Part T: pilot study of tissue plasminogen activator administered within 90 minutes. Stroke
19n 23,6.32- 640.
5. Bron T, Lu M, Kothari R, et aL Hypertension and its treatment in the NINDS rt-PA stroke trial. Stroke 1998; 29,1504-1509
6. Casto L, Caverni L, Camerlingo M, et a1. Intra-arterial thrombolYSiS in acute ischaemic stroke: experience with a superselective catheter embedded in the clot. ] Neurol Neurosurg Psyehiatly 1996; 60£67-670.
7. Chambers SR, NorrisJW, Shurvell BL, et a1. Progno
sis of acute stroke neurology 1987; 37:221-225.
8. Clark WM, Albers GW, for the ATLANTIS Stroke Study Tnvestigators. The Atlantis rt-PA (Alteplase) acute stroke trial: Anal results presented at the 24th American Heart Association International Conference on Stroke and Cerebral Circulation; February 4, 1999; Nashville, TN.
9. Connors ]J, Wojak ]c. Current directions in emergency su'oke therapy. In, Connors ]], Wojak ]C, eds . lnterventional 1\leuroradiotogy. Philadelphia, PA: WE Saunders; 1999; Chaps 56, 58.
11. del Zoppa G], Higashida RT, Furlan A], et aJ. PRO
ACf: a phase II randomized trial of recombinant pro-urokinase by direct arterial delivery in acute middle cerebral artery. Stroke 1998; 29:4-1l.
12. del Zoppo G], Ferbert A, Otis S, et al. Local intraarterial fibrinolytic therapy in acute carotid territory stroke. a pilot study. Stroke 1988; 19>307-313.
14. Donnan GA, Davis SM, Chambers BR, et al. Trials of streptokinase in severe acute ischaemic stroke. Lan
cet 1995; 345578-579.
15. Earnest F IV, Forbes G, Sandok BA, et aJ. Complications of cerebral angiography: prospective assessment of risk. A]R 1984; 142,247- 253.
16. Emergency Management of Stroke (EMS) Investigators. Combined intra-arterial and intravenous rt-PA for stroke. Presented at the 22nd International Joint Conference on Stroke and Cerebral Circulation; Feb
fUary 8, 1997; Anaheim, CA.
17. Furlan A], Higashida R, Wechsler L, et al. PROACT II. recombinant prourokinase (r-ProUK) in acute cere-