Embed Size (px)
Citation preview

I Reunión “Avances en SCA”(día 2)
Ángel Cequier
Vicepresidente Sociedad Española de Cardiología
Director Area de Enfermedades del Corazón
Hospital Universitario de Bellvitge. IDIBELL
Universidad de Barcelona. Hospitalet de Ll. Barcelona

Non ST Non ST -- Elevation Acute Elevation Acute
Coronary SyndromeCoronary Syndrome
Embolization and Embolization and microvascularmicrovascular
occlusion in nonocclusion in non--ST ACSST ACS
Plaque rupture and Plaque rupture and
thrombus in STEMIthrombus in STEMI
ST ST -- Elevation Acute Elevation Acute
Myocardial InfarctionMyocardial Infarction

Hamm CW et al. EHJ 2011 doi:10.1093/ehr236
DecisionDecision--Making Algorithm in ACSMaking Algorithm in ACS

2011 ACC/AHA Focused Update Guidelines for UA/NSTEMI2011 ACC/AHA Focused Update Guidelines for UA/NSTEMI
Anderson et al. Circulation/JACC 2011
Early Invasive Early Invasive vsvs Conservative TherapyConservative Therapy
Relative Risk of Outcomes. Mean F/U 2 yearsRelative Risk of Outcomes. Mean F/U 2 years
AllAll--cause mortalitycause mortality Recurrent nonRecurrent non--fatal MIfatal MI

Influencia del tipo de Hospital en el Tratamiento y Influencia del tipo de Hospital en el Tratamiento y
Pronóstico de los ptes con SCAseSTPronóstico de los ptes con SCAseST
Ruiz-Nodar JM, Cequier A, Lozano T, et al. REC 2010; 63: 390
Estudio GYSCAEstudio GYSCA
Curvas KaplanCurvas Kaplan--Meier de supervivencia libre Meier de supervivencia libre
de MACE (muerte, SCAseST o de MACE (muerte, SCAseST o
revascularización)revascularización)
Pacientes con SCAseST ingresados en Hospitales sin Hemodinámica son tratados Pacientes con SCAseST ingresados en Hospitales sin Hemodinámica son tratados
con menor adherencia a las Guías. Adicionalmente el tipo de Hospital puede tener con menor adherencia a las Guías. Adicionalmente el tipo de Hospital puede tener
una influencia en el pronósticouna influencia en el pronóstico
p<0.01 todas las comparacionesp<0.01 todas las comparaciones
Hospital Terciario Comarcal
AngiographyAngiography: 61 : 61 -- 63 %63 %
PCI: 31PCI: 31-- 34 %34 %
MASCARA MASCARA RegistryRegistry. REC 2008; 61: 803. REC 2008; 61: 803
GYSCA GYSCA RegistryRegistry. REC 2010; 63: 390. REC 2010; 63: 390
SYNERGY. JAMA 2005: 294: 2594SYNERGY. JAMA 2005: 294: 2594
Cequier A. REC 2008; 61: 793Cequier A. REC 2008; 61: 793

Ticagrelor Ticagrelor vs Clopidogrel in Patients with ACSvs Clopidogrel in Patients with ACS
WallentinWallentin et al. NEJM 2009; August 30; on lineet al. NEJM 2009; August 30; on line
PLATO StudyPLATO Study
TicagrelorTicagrelor: : 180 mg loading dose, 90 mg twice daily180 mg loading dose, 90 mg twice daily
Clopidogrel: Clopidogrel: 300300--600 mg loading dose, 75 mg daily600 mg loading dose, 75 mg daily
Composite endComposite end--point: point:
CV death, MI or strokeCV death, MI or stroke Time to the First Major Bleeding endTime to the First Major Bleeding end--pointpoint
11.7%
9.8 %
n= 18624 n= 18624 ptspts, ACS, with or without ST, ACS, with or without ST--segment elevation segment elevation
(28% planned for non(28% planned for non--invasive management)invasive management)

Adverse Impact of Adverse Impact of
Bleeding on Bleeding on
Prognosis in PatientsPrognosis in Patients
with ACSwith ACS
Mortality during the first 30 days
p<.0001p<.0001
12.8 %12.8 %
2.5 %2.5 %
OASIS Registry, OASISOASIS Registry, OASIS--2, 2,
CURE CURE (n= 34146 ptes)(n= 34146 ptes)
Circulation 2006; 114: 774Circulation 2006; 114: 774
ACUITY ACUITY
TrialTrial
JACC 2007; JACC 2007;
49:136249:1362
3 %3 %
8 %8 %
p< .001p< .001
Blood Blood
Transfusion Transfusion
and and
Clinical Clinical
Outcome in Outcome in
ACSACS
Rao et al. JAMA Rao et al. JAMA
2004; 292: 15572004; 292: 1557
Major Bleeding
Non access-site related
60 - 70 %
(ACUITY, TRITON-TIMI 38)
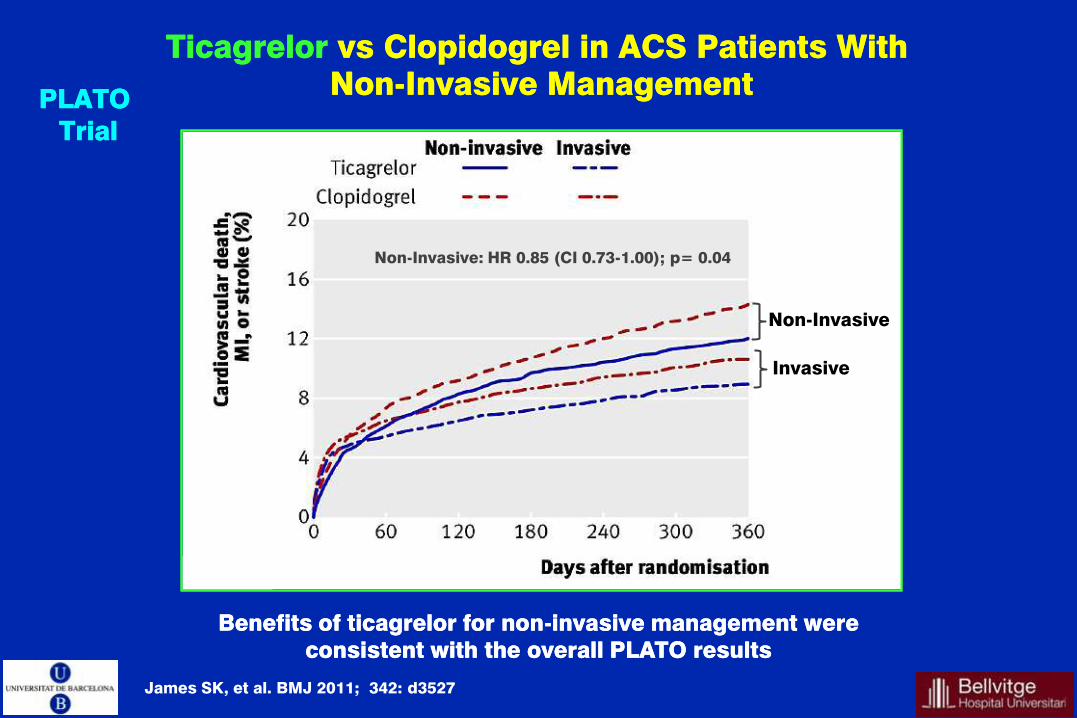
TicagrelorTicagrelor vs Clopidogrel in ACS vs Clopidogrel in ACS PatientsPatients WithWith
NonNon--IInvasivenvasive ManagementManagement PLATO PLATO
TrialTrial
James SK, et al. BMJ 2011; 342: d3527
Benefits of ticagrelor for nonBenefits of ticagrelor for non--invasive management were invasive management were
consistent with the overall PLATO resultsconsistent with the overall PLATO results
Non-Invasive
Invasive
Non-Invasive: HR 0.85 (CI 0.73-1.00); p= 0.04

*Major bleeding: non-CABG-related TIMI major bleeding
1. Antiplatelet Trialists' Collaboration, 1994; 2. Antithrombotic Trialists' Collaboration, 2002;
3. Wiviott et al, 2007; 4. Wallentin et al, 2009
20.0 2.8* 2.2* 0.8 1.3
1.8* 2.4* 0
5
10
15
20
25
None
–25%
15.0
ASA1,2
–20%
12.1
ASA + clopidogrel3
ASA +
–19%
9.9
prasugrel3
11.7
ASA + clopidogrel4
Even
t ra
te (
%)
–16%
ASA +
9.8
ticagrelor4
CV death, MI or stroke
Major bleeding
Prevención Secundaria en el SCA
La incidencia de nuevos eventos CV (muerte, IM o ictus) a 1 año
tras un evento inicial, continúa siendo elevada, ~10%
TRITON TIMI 38 PLATO

Reperfusion Therapy for
Patients with STEMI
2012


Tarantini G, et al. EHJ 2010; 31: 676 / Tarantini G, et al. AHJ 2011; 161: 247.
PPCI for AMI PPCI for AMI
The RiskThe Risk--Time relationshipTime relationship
The need to quantify the impact of delayThe need to quantify the impact of delay
Baseline mortality risk of STEMI is a major determinant of the
acceptable time delay to choose the most acceptable therapy.

IntraaorticIntraaortic BalloonBalloon SupportSupport forfor AMI AMI
withwith CardiogenicCardiogenic ShockShock IABPIABP--SHOCK II SHOCK II
TrialTrial
Thiele H, et al. NEJM 2012; 367: 1287
The use of The use of IAoBIAoB counterpulsationcounterpulsation did not reduce 30did not reduce 30--day mortality in day mortality in
ptesptes with cardiogenic shock complicating AMI treated with PPCIwith cardiogenic shock complicating AMI treated with PPCI
600 patients with cardiogenic shock 600 patients with cardiogenic shock
complicating AMI, randomized to complicating AMI, randomized to IAoBPIAoBP
vsvs NO NO IAoBPIAoBP. .
Primary endPrimary end--point: point:
3030--day allday all--cause mortalitycause mortality
Time-to-Event
Curves for the
Primary End Point
Subgroup Analysis
I Reunión “Avances en SCA”





























