Embed Size (px)
Citation preview

I.Gramnegative anaerobe
Stäbchen
II.Gram positive sporenbildende
Stäbchen
Dr. Bános ZsuzsaDr. Bános Zsuzsa17 November 200917 November 2009

I.Gramnegative anaerobe
Stäbchen
Dr. Bános ZsuzsaDr. Bános Zsuzsa17 November 200917 November 2009

GRAMNEGATIVE STÄBCHEN
AEROBBordetellaBrucellaFrancisella
PseudomonasAcinetobacterLegionella
FAKULTATIV ANAEROBHaemophilusPasteurella
Familie:EnterobacteriaceaeVibrionaceae
CardiobacteriumEikenellaKingellaActinobacillus
ANAEROBBacteroidesPrevotellaPorphyromonasFusobacterium
MIKROAEROPHILCampylobacterHelicobacter

GramnegativeGramnegative anaerobeanaerobe StäbchenStäbchen((BacteroidaceaeBacteroidaceae))
Gattung ArtBacteroides B. fragilis
und weiterePrevotella P. intermedia
P. melaninogenicaund weitere
Porphyromonas P. gingivalisP. asaccharolytica
und weitereFusobacterium F. nucleatum u.w.

P. gingivalis, Fusobakterienwww.genomenewsnetwork.org

Porphyromonas spp.pharmacie.univ-lille2.fr

Prevotella intermediapharmacie.univ-lille2.fr

Prevotella intermediapharmacie.univ-lille2.fr

Prevotella – schwarze Pigmente fluoreszierenpharmacie.univ-lille2.fr

pharmacie.univ-lille2.fr
Prevotella melaninogenica

Vorkommen und Krankheiten-1Normalflora- der Mundhöhle (Porphyromonas, Prevotella, Fusobacterium)- des Darmtraktes (Bacteroides, Fusobacterium)- des Respirationstraktes/Orophyarynx (Prevotella)- des Urogenitaltraktes (Prevotella)
Endogene Infektion – Mischinfektionen
VirulenzfaktorenAdhäsineKapselExoenzyme (Hyaluronidase, Kollagenase, Neuraminidase)Exotoxine, Toxische SubstanzenEndotoxin

Vorkommen und Krankheiten-2
In der Mundhöhle- Fusospirochätose:
Treponema vincentii + Fusobakterien- Angina Plaut-Vincent- Akute nekrotisierende geschwürsbildende Gingivitis
-Gingivostomatitis-Parodontitis Porphyromonas, Prevotella-Zahnabszesse


www.lg1.ch Flora Plaut - Vincent, Angina Plaut-Vincent

Flora Plaut - Vincent, Angina Plaut-VincentDas massenhafte gemeinsame Vorkommenvon Fusobacterium-Arten und Treponema vincentii, (Bestandteile der normalen Haut- u. Schleimhautflora) kann zu Gewebsnekrosenu. damit zur Schaffung anaeroberGewebsverhältnisse führen. Folge sindFusospirochätosen (= Fusoborreliosen) wiedie Angina Plaut-Vincent, Stomatitis ulcerosa, Alveolarpyorrhö, Noma, Nosokomialgangrän, Balanitis circinata, Ulcus tropicum, Lungengangrän etc.www.lg1.ch

www.lg1.ch Mischflora: Fusobakterien und Treponemen

Flora Plaut - Vincent, Fusobacterium fusiforme und Treponema (Borrelia) vincentii Eine Mischung aus Fusobacterien und Treponemen (Borrelien) verursacht einesogenannte Fusospirochätose welch sich alsPharyngitis oder Gingivitis manifestiert. Benannt nach den Bakteriologen Hugo CarlPlaut, 1858–1928, Hamburg und Jean Henry Vincent, 1862-1950, Bakteriologe und Epidemiologe, Paris.
www.lg1.ch

webs.wichita.eduHöhle und Gingivitis

Ulcerativ Gingivitiswebs.wichita.edu

Vorkommen und Krankheiten-3
Nekrotische Abszessen, generalisierte, septischeKrankheiten
Bauchraum (Bacteroides, Fusobacterium)Peritonitis, intraabdominelle Abszesse, Leberabszesse
Respirationstrakt (Prevotella, Porphyromonas)Aspirationspneumonie, Lungenabszess, Pleuraempyem
Urogenitaltrakt (Prevotella, Porphyromonas)Bakterielle Vaginose!Douglas-, und tuboovarielle - AbszessZNS – Hirnabszesse (Prevotella, Porphyromonas)
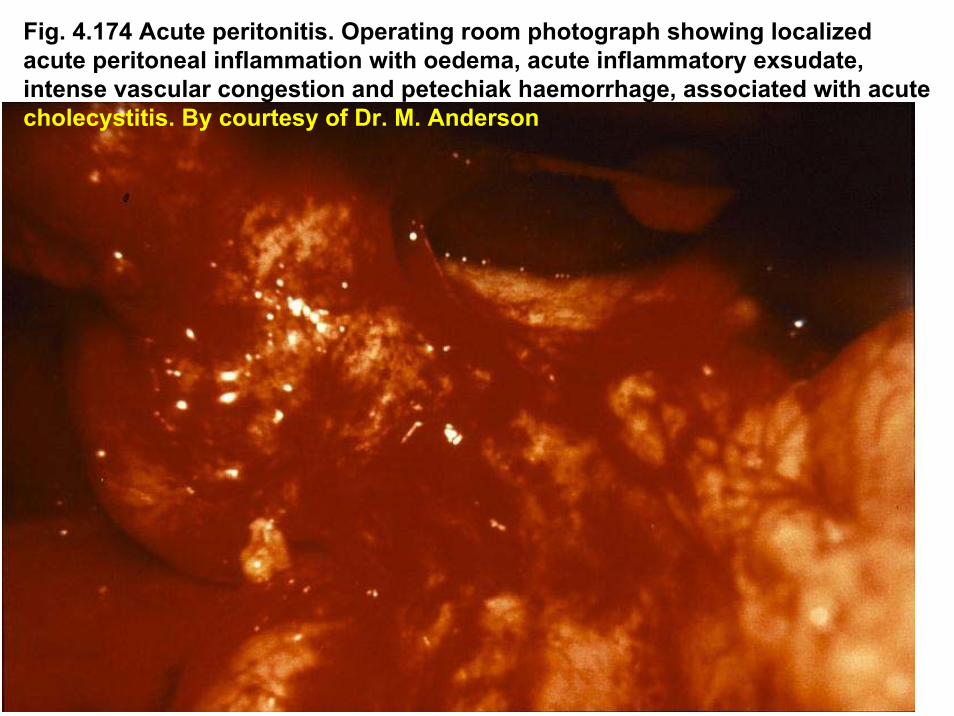
Fig. 4.174 Acute peritonitis. Operating room photograph showing localizedacute peritoneal inflammation with oedema, acute inflammatory exsudate, intense vascular congestion and petechiak haemorrhage, associated with acutecholecystitis. By courtesy of Dr. M. Anderson

Fig. 4.175 Acuteperitonitis. Cloudy, infected peritonealdialysate removed from a patient undergoingperitoneal dialysis.

Fig. 4.173 Appendiceal abscess. Ultrasound studies showing anabscess in the pouch of Douglas secondary to a ruptured appendix.Lateral view (left) and transverse view (right). By courtesy of Dr. A.E. Joseph

Fig. 4.176 Intraabdominal abscess. CT scan at the level of the seminalvesicles showing an elliptical abscess to the left of the midline.

Vorkommen und Krankheiten-3
Nekrotische Abszessen, generalisierte, septischeKrankheiten
Bauchraum (Bacteroides, Fusobacterium)Peritonitis, intrabdominelle Abszesse, Leberabszesse
Respirationstrakt (Prevotella, Porphyromonas)Aspirationspneumonie, Lungenabszess, Pleuraempyem
Urogenitaltrakt (Prevotella, Porphyromonas)Bakterielle Vaginose!Douglas- und tuboovarielle AbszessZNS – Hirnabszesse (Prevotella, Porphyromonas)

Abscess cavity
Fig. 2.91 Lung abscess. Chest radiographs, postanterior and lateral, showing abscesscavity in lower lobe of right lung.
Fig. 2.94 Large encysted empyema of right lungwith additional small effusion.

Fig. 2.92 Lung abscess. Gram stain of pus showing Gram-positive cocci andvaroius Gram negative and Gram positive rods. By courtesy of J.R. Cantey

Vorkommen und Krankheiten-3
Nekrotische Abszessen, generalisierte, septischeKrankheiten
Bauchraum (Bacteroides, Fusobacterium)Peritonitis, intrabdominelle Abszesse, Leberabszesse
Respirationstrakt (Prevotella, Porphyromonas)Aspirationspneumonie, Lungenabszess, Pleuraempyem
Urogenitaltrakt (Prevotella, Porphyromonas)Bakterielle Vaginose!Douglas-, tuboovarielle-AbszessZNS – Hirnabszesse (Prevotella, Porphyromonas)

Fig. 7.21 Bacterial vaginosis. The clue-cell – a vaginal epithelial cellwith attached microorganism. The attached bacteria give the clue cell a stippled appearance. By courtesy of Dr. R.J.Arko and Prof G.P. Schmid

Fig. 7.90 Tuboovarian abscess. Ultrasound study of left sagittal section of thepelvis showing complex thick-walled cystic left adnexal man with internalseptation.

Vorkommen und Krankheiten-4
DiagnostikNachweis des ErregersDirekt mikroskopisch (Angina Plaut-Vincent)
KulturUnter streng anaeroben BedingungenUntersuchungsmaterial: Eiter, Exsudat – Entnahme! AnaerobeTransportmedienInkubationszeit: 1-2 WocheNachweis organischer Säuren im Medium Gaschromatographie
Antibiogramm!
BehandlungPenicilline (Amoxycillin+Clavulansäure) + Metronidasol


II.Gram positive
sporenbildende Stäbchen
Dr. Bános ZsuzsaDr. Bános Zsuzsa17 November 200917 November 2009

Gram Gram popossititiivvee StäbchenStäbchenNicht SporenbildendeAEROBCorynebacteria
C. diphtheriaediphtheroideC. jeikeium
Listeria monocytogenesErysipelothrix rhusiopathiaeANAEROBLactobacillus spp.
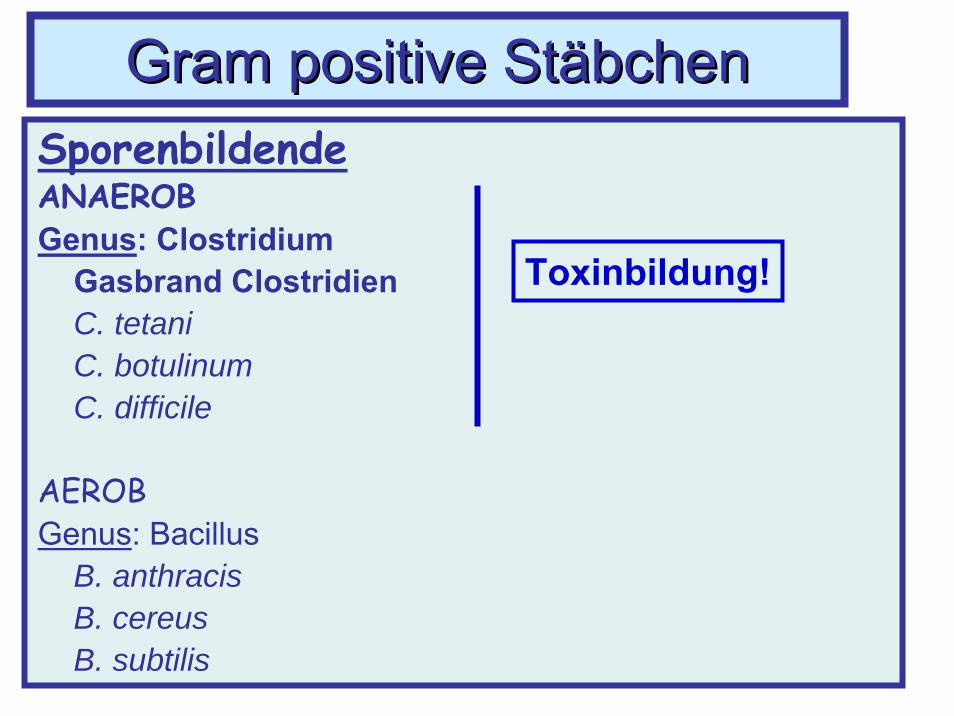
SporenbildendeAEROBGenus: Bacillus
B. anthracisB. cereusB. subtilis
ANAEROBGenus: Clostridium
C. tetaniC. botulinumC. difficileGasbrand Clostridien

SporenbildendeAEROBGenus: Bacillus
B. anthracisB. cereusB. subtilis
ANAEROBGenus: Clostridium
C. tetaniC. botulinumC. difficileGasbrand Clostridien
Gram Gram popossititiivvee StäbchenStäbchen
Gram Gram popossititiivvee StäbchenStäbchenSporenbildendeANAEROBGenus: Clostridium
Gasbrand ClostridienC. tetaniC. botulinumC. difficile
AEROBGenus: Bacillus
B. anthracisB. cereusB. subtilis
Toxinbildung!

ClostridienClostridienSIND- Begeisselte Bakterien (Ausnahme: C. perfringens – KAPSEL)- Anaerobe- Resistent - Sporen gegen Hitze hochresistent!
Sie ertragen 100°C 3-5 Stunden lang, 140°C trockeneWärme 1 Std lang
BILDEN- Endosporen- Speziesspezifische Exotoxine - Intoxikation

MorphologieGrampositive Stäbchen
VorkommenErdbodenDarmtrakt der Menschenund Tiere
GasbrandGasbrand ClostridienClostridienC. C. perfringensperfringens, C. , C. novyinovyi, C. , C. septicumsepticum u.au.a..

Clostridium perfringensKulturBlutagar: doppel-Haemolyse (α + β); relativ aerotolerant

Clostridium perfringens
Pathogenese1. Verletzungen, Trauma2. Kontamination (mit Sporen)3. Vermehrung der Keime unter anaeroben Bedingungenim traumatisch veränderten Muskelgewebe
4. ToxinbildungAnaerobe Zellulitis
Nekrotisierende Myositis + + Allgemeinintoxikation
GasbrandSchockTod

Clostridium perfringensTyp: A, B, C, D und E
Toxineα – δ: letale, nekrotisierende, haemolytische, zell-lysierendeWirkung(α-Toxin = Lecithinase)Enterotoxin
EnzymeKollagenasenHyaluronidaseDNasenProteinasenPerfringolysin
Clostridium perfringens
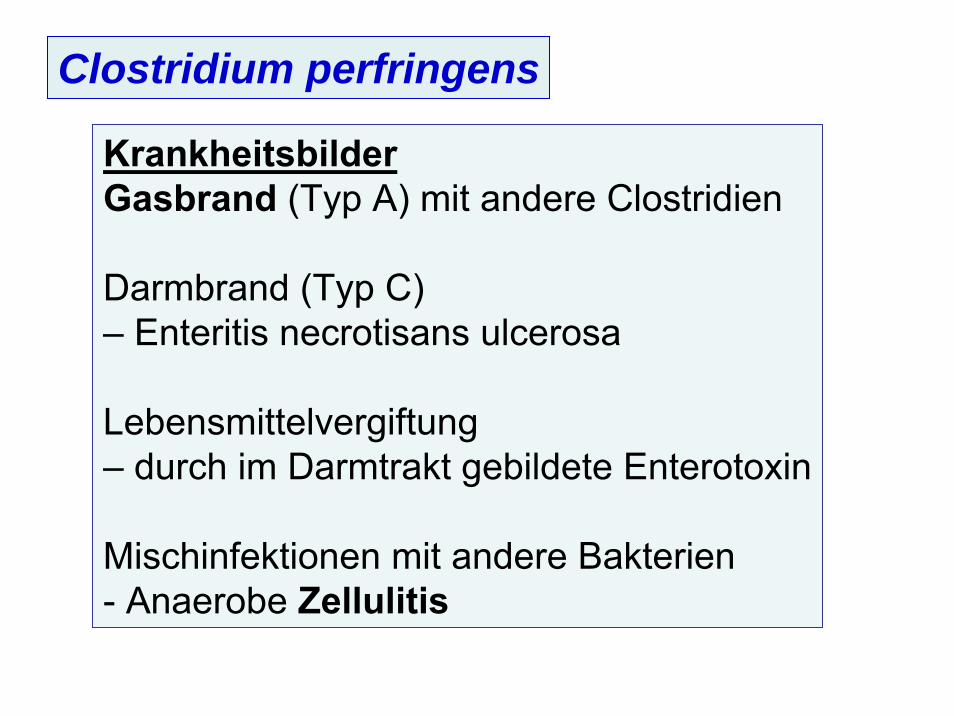
KrankheitsbilderGasbrand (Typ A) mit andere Clostridien
Darmbrand (Typ C)– Enteritis necrotisans ulcerosa
Lebensmittelvergiftung– durch im Darmtrakt gebildete Enterotoxin
Mischinfektionen mit andere Bakterien- Anaerobe Zellulitis

Fig. 10.46 Postoperativegangrenous cellulitis. A hugearea of ulceration filled withgangrenous skin and sloughtlies adjancent to the wound. There is surrounding cellulitisand a further area of necroticskin in the flank.
Fig. 10.47 Postoperativegangrenous cellulitis. Samepatient as Fig. 10.46 later.The cellulitis has resolved andthe ulcerated area is filled withblack necrotic tissue.

Fig. 10.49 Clostridial cellulitis, following compound fracture of the tibia. Crepituswas noted on examination and the presence of gas was confirmed radiologically.
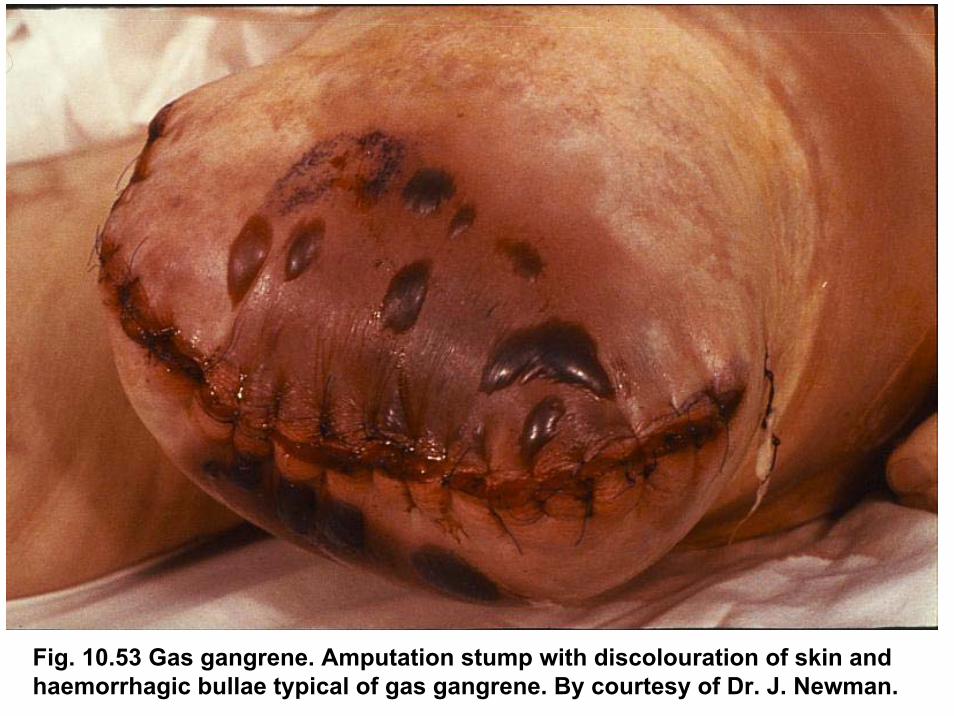
Fig. 10.53 Gas gangrene. Amputation stump with discolouration of skin andhaemorrhagic bullae typical of gas gangrene. By courtesy of Dr. J. Newman.

Gas gangrene evident in a patient's leg stump followingamputation (Pelczar, Chan & Grieg, 1993, pp. 747) www.podiatry.curtin.edu.au

Fig. 10.54 Gas gangrene. There is a serosanguinous discharge from the lowerend of the surgical wound and the affected muscles show pallor and failure tobleed. By courtesy of Mr. E. Taylor.


www.ooze.com

www.worldortho.com

Fig. 10.51 Fournier’s gangrene. Extensive necrosis of the skin and subcutaneoustissues of the scrotum and abdominal wall in a diabetic man. The presence of necrosis extending beyond the upper margin of the wound shows thatinsufficient debriment has been preformed and further surgery is necessary.

www-instruct.nmu.edu
Clostridium perfringens
KrankheitsbilderGasbrand (Typ A) mit andere Clostridien
Darmbrand (Typ C)– Enteritis necrotisans ulcerosa
Lebensmittelvergiftung– durch im Darmtrakt gebildete Enterotoxin
Mischinfektionen mit andere Bakterien- Anaerobe Zellulitis
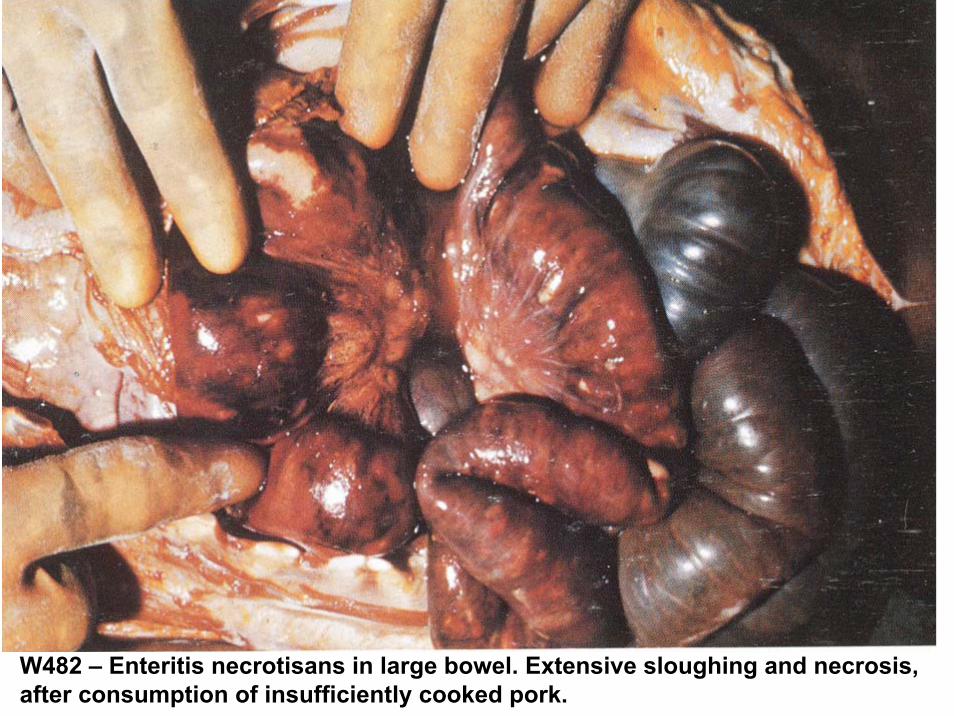
W482 – Enteritis necrotisans in large bowel. Extensive sloughing and necrosis, after consumption of insufficiently cooked pork.

www.3tres3.com
Enteritis necrotisans

Fig. 4.55 Necrotizing enteritis. (pi-bel) Gross specimen of small bowel from a case seen in Uganda. The lower piece of opened jejunum shows greyish-blackareas of necrosis, particularly involving the superficial part of the tranversemucosal folds. By courtesy of Professor M.S.R. Hutt.

GASBRAND
DiagnoseKlinisch!!!
ErregernachweisMikroskopischKultur – Blutagar

Gram FärbungExsudat
GASBRAND

Histologie
MyonekroseGas
GASBRAND
GASBRAND
Speziesdiagnose der Clostridien:Biochemische LeistungenGaschromatographie
Differenzierung von Typen: Spezifisches Antiserumhemmt die letale Wirkung ihrer Toxine
Toxinneutralisation in MeerschweinchenNagler-test

Fig. 4.54 Nagler’sreaction detects thelecithinase produced byC. perfringens whichgives a precititate inegg-yolk media. Thereare two parallel streamsof growth. Zones of opacity are seen on theright half but not on theleft, on which antitoxin was placed beforeinoculation.

GASBRAND
TherapieChirurgisch!!!Penicillin G i.v.MetronidazoleKombination: Breitspektrum Antibiotika (Mischinfektionen!)Alternativen: Penicillin + Clindamycin; Chloramphenicol
Behandlung mit hyperbaren O2 in einer Überdruckkammer
ProphylaxeChirurgische – WundtoilettePenicillin, Cephalosporine
Hospitalinfektionen! – Gips!

Clostridium tetani
Morphologie„Trommelschläger”
www.textbookofbacteriology.net

Clostridium tetani
KulturUnter anaeroben BedingungenBlutagar – keine Haemolyse

Clostridium tetani
Pathogenese, InfektionVorkommen- Darm der Pflanzenfresser (Pferd! – Menschen selten)- Sporen gelangen in den gedüngten Erdboden, in denStrassenstaub, in den Wohnungstaub
Infektionsquelle- Sporenhaltiger Staub,- Kontaminierte Instrumente
Eintrittspforte- Verletzte Haut – Unfälle, Postoperativ- Auskeimung – Vermehrung – Toxinbildung

Clostridium tetani TetanustoxinA-B ToxinLeichte Kette (A): Zink-MetalloproteaseSchwere Kette (B): Bindung an motorischenNeuronenDLM: 1 ng/kg (Maus)
A Kette gelangt retroaxonal in das Rückenmark, wirdvon Hemm-Neuronen aufgenommen, zerstört durchProteolyse Synaptobrevine keine inhibitorischeImpulse auf die motorische Neurone Spasmen derSkelettmuskeln

Clostridium tetani
KrankheitTetanus = Starrkrampf
Tonische Spannung de Kiefer- und Gesichtsmuskelnmit Kieferklemme = TrismusDie gespannte Nacken- und Rückenmuskulatur führtzur Zwangshaltung mit hohlem Rücken: OpisthotonusLetalität: >50%

Fig. 3.122 Tetanus. Risussardonicus, due to spasmof the facial muscles. Bycourtesy of Dr. T.F. Sellers, Jr.

Fig. 3.123 Tetanus. Risussardonicus in a newborninfant.

Fig. 3.124 Tetanus. Risussardonicus in an adult.

Fig. 3.121 Tetanus. Opisthotonus in an infant due to intensecontraction of the paravertebral muscles. By courtesy of Dr. T.F. Sellers, Jr.

Sir Charles Bell’s portrait of a soldier dying of tetanuswww.textbookofbakteriology.net

Clostridium tetani
Immunität – keine(Toxin ist hochwirksam als Antigen aber zu gering)
Diagnose- Erregernachweisin WundsekretGewebestücke- Kultur- Toxinnachweisim Wundmaterial(Tierversuch)
Fig. 3.120 This organism is a slender bacillus formingterminal spores giving a „drumstick” appearence. Gram stain. Sporeformation in tissues.

Clostridium tetani TherapieChirurgischSymptomatisch (Curare)Antibiotika: PenicillinPassive Immunisierung - Tetanus Immunglobulin von Menschen
ProphylaxeAktive Immunisierung (Toxoid)Grundimmunisierung: ab 3. Lebensmonat – 11-15 JahreAuffrischungsimpfung: in Abständen von 10 Jahren
Bei VerletzungenA) vollständig immunisierter Personen: Auffrischimpfung (Toxoid)B) nicht immunisierter Personen: Simultanimmunisierung
(Aktive+Passive)

Clostridium botulinum
Morphologie„Tennisschlägerform”
Vorkommen: Erdboden
Botulinustoxin = NeurotoxinDLM ca. 1 ng/kg (Mensch)Typ: A, B, C1, C2, D, E, F
WirkungBlockade der Acethylcholinproduktion an denneuromuskulären Endplatten Paralyse

PathogeneseAufnahme von Lebensmittelnn in denen C. botulinum TOXIN gebildet hat
KrankheitsbildProgressive Bulbärparalyse
DiagnoseTOXINNACHWEIS – im Tierversuch(Mageninhalt, Blutserum, Nahrungsmittel)Typ wird im Neutralisationstest bestimmt
BehandlungAntitoxin (gegen Typ A, B, E) – schnell!
Clostridium botulinum

Fig. 3.125 Botulism. Clinical photograph showing dilated, unreactive, fixed pupils. By courtesy of Dr. Z. McGee.
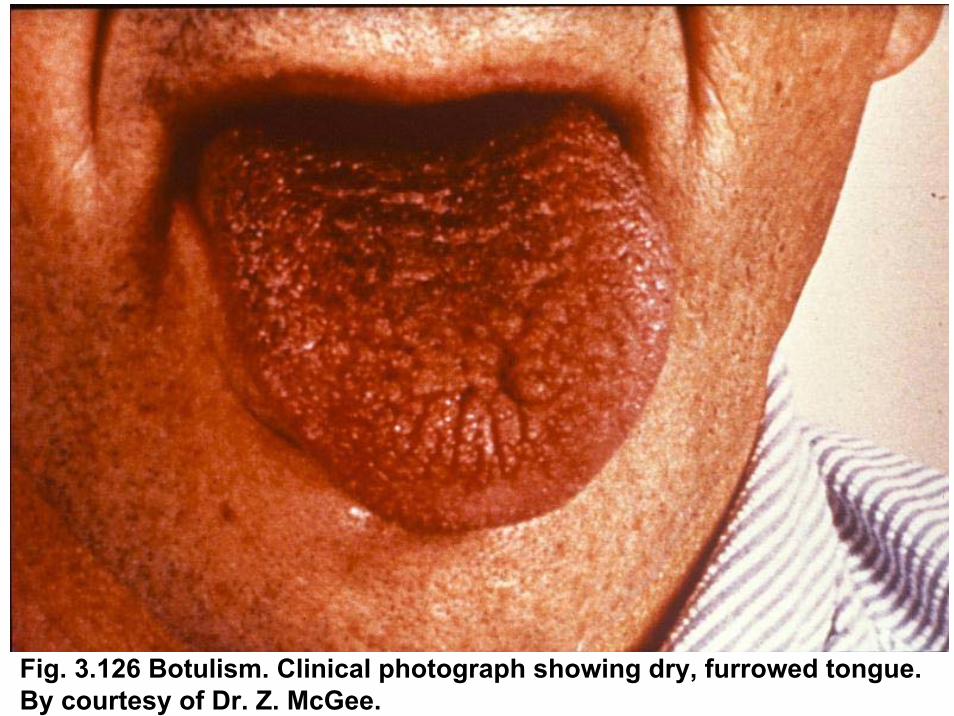
Fig. 3.126 Botulism. Clinical photograph showing dry, furrowed tongue. By courtesy of Dr. Z. McGee.

Clostridium difficile
Vorkommen:Darmtrakt 1-4 % Erwachsene; 30-50% Kleinkinder
VirulenzfaktorenToxin A: EnterotoxinToxin B: Zytotoxin
Behandlung mit Breitspektrumantibiotika
Pseudomemranöse Colitis
Therapie:Aufhören mit Antibiotikum BehandlungPer os Metronidazole, Vancomycin
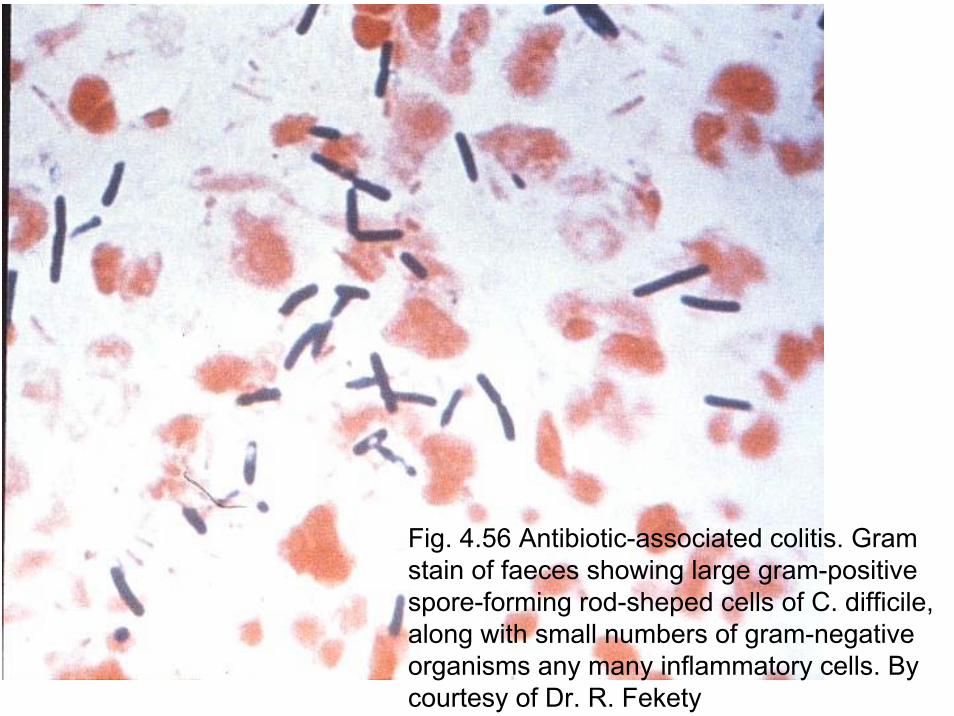
Fig. 4.56 Antibiotic-associated colitis. Gram stain of faeces showing large gram-positivespore-forming rod-sheped cells of C. difficile, along with small numbers of gram-negativeorganisms any many inflammatory cells. Bycourtesy of Dr. R. Fekety

Fig. 4.57 Gross specimen of colons from fatal cases of antibiotic-associated colitis. Right: Extensive inflammatory pseudomembrane. Middle: numerous small plaques, some almost confluent. Left: Confluent pseudomembrane covering most of the epithelial surface.

Fig. 4.58 Macroscopic appearance of typical pseudomembranous colitisshowing the discrete yellow plaques.

Fig. 4.59 Sigmoidoscopic view of pseudomembranous colitisdue to antibiotic treatment. The yellow-white „membrane” contrast with the reddened colonic mucosa. By courtesy of Prof. R. Hunt

Fig. 4.60 Sigmoidoscopiv view demonstrating multiple pseudomembranouslesions in a patient with antibiotic-associated colitis due to C. difficile.

Fig. 4.64 Antibiotic-associated colitis. Assay of C. difficile toxin showing normal baby-hamster kidney cells (left) and cells after exposure to toxin (right). Note rounding up of cells following exposure to toxin. By courtesy of Dr. R. Fekety

Gram Gram popossititiivvee StäbchenStäbchenSporenbildendeAEROBGenus: Bacillus
B. anthracisB. cereusB. subtilis
ANAEROBGenus: Clostridium
C. tetaniC. botulinumC. difficileGasbrand Clostridien

Bacillus anthracisBacillus anthracis
Morphologie:Gram + sporenbildende, 5-10 μm, dicke, Stäbchen
www.textbookofbacteriology.net

Gram Färbung
B. anthracis B. subtilis

Sporenfärbung - Ziehl Neelsen

Bacillus anthracisBacillus anthracis
Blutagarwww.textbookofbacteriology.net
Kultur:einfach

B. anthracis - Blutagar
Bacillus anthracisBacillus anthracis
www.textbookofbacteriology.net
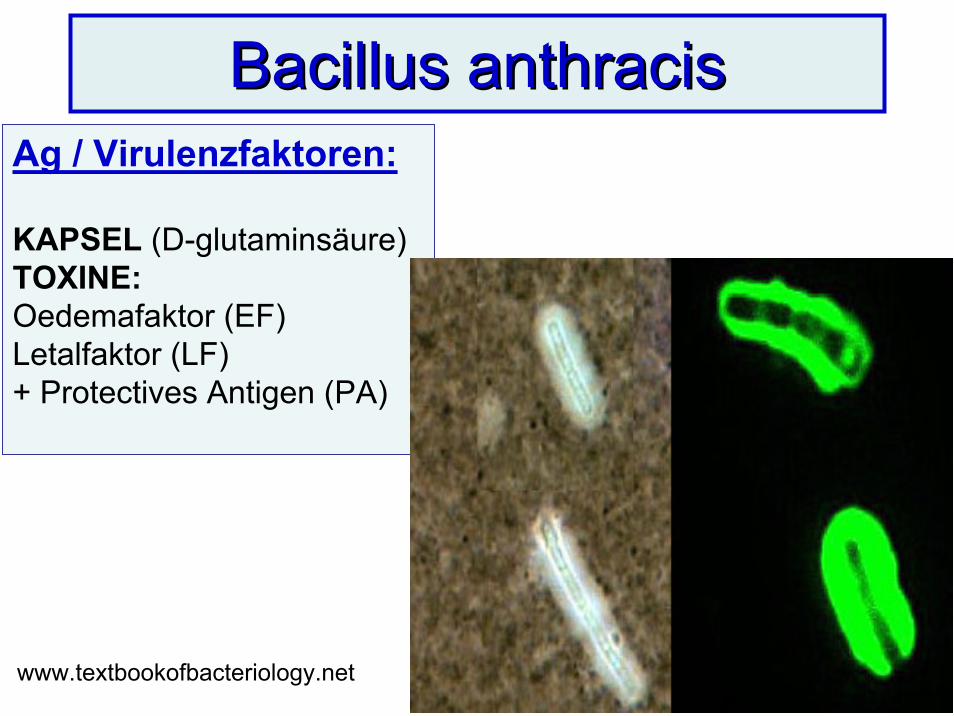
Ag / Virulenzfaktoren:
KAPSEL (D-glutaminsäure)TOXINE:Oedemafaktor (EF)Letalfaktor (LF)+ Protectives Antigen (PA)

Zellmembran
Toxinbildung
Source: Medmicro
PathogeneseZoonose!Infektionsquelle: • Tiere (Kranke, Cadaver), tierische Produkte• Erdboden (Sporen)Eintrittspforte:• Mucosa• Haut (Verletzungen)Übertragung: nicht Kontagiös
Bacillus anthracisBacillus anthracis

Bacillus anthracisBacillus anthracisKrankheitsbilder: Anthrax = Milzbrand•Hautanthrax (direkt, Wunden) – Pustula maligna•Lungenanthrax (Inhalation von Sporen)•Darmanthrax (direkt, kontaminiertes Lebensmittel)•Sepsis (Letalität 5-20%)
Diagnose:Erregernachweis: mikroskopisch, Kultur
Therapie:PenicillineLungen - Darmanthrax: Ciprofloxacin + Penicillin(lange: 60 Tage!)

Hautanthrax I. - Pustulamaligna

Hautanthrax II.
Source: CDC Anthrax Images

Source: CDC Anthrax Images Local laesion + oedema
Hautanthrax III.

Fig. 10.97 Anthrax. The eschar can be seen on the lower eyelid and thereis extensive oedemaof the face. By courtesy of Dr. T.F. Sellers, Jr.
Pustula maligna+ Oedema

Pustula maligna und Oedema

Krankheitsbilder:• Hautanthrax (direkt, Wunden) – Pustula maligna• Lungenanthrax (Inhalation von Sporen)• Darmanthrax (direkt, kontaminierte Lebensmittel)
Bacillus anthracisBacillus anthracis

Inhalation/Lungenanthrax (X-ray)
Mediastinal widening … and pleural effusion
Source: CDC Anthrax Images

Prophylaxe• Vernichtung infektiöser Tiere• Dekontamination von Erdboden, Desinfektionkontaminierter Produkte• Aktive Immunisierung: Zellfreie Vakzine
- Risikogruppen: Armee (USA), Tierärzte• Chemoprophylaxe der Lungenanthrax:Kontaktpersonen, Ciprofloxacin
WHO MeldepflichtBioterrorismus!
Bacillus anthracisBacillus anthracis

Biologische Waffen - Zusammenfassung
Biologische Waffen: Organismen, Toxine, VirenZiel:• Individuen, ganze Populationen erkranken zulassen oder gar auszurotten• Ökonomische schaden
Biokriegsführung (militärische Konflikts)Bioterrorismus (ideologische Motive)Bioverbrechen (persönliche Ziele)

Biologische Waffen - Zusammenfassung
Kap. X. 129. Tab. 129.1. (Hahn)
Kategorie: A, B, CGefährlichste: AB. anthracis, C. botulinum, F. tularensis, Y. pestis
Einfache KultivierungAusbreitung durch AtemwegeHohe LetalitätTherapie?Plötzliche AuftretenZahlreiche Fälle

Forrás: anthrax BBC tények
Verbreitung von Anthrax
JetBriefe
Theoretisch
WindUndRegen
Billig, aber fliegende Sporen??USA 200110 Lungenmilzbrand7 Hautmilzbrand5 Todesfälle
Realität

Forrás: anthrax BBC tények
Biologische Waffen und Anthrax
Aufzählung
Unfall
Japanische Terroristen

B. cereus
Vorkommen-Ubiquitär
BILDET- Enzyme (Kollagenase, Proteasen, Amylase, Phospholipase, Lecithinase, Haemolysin)- Enterotoxin
Lebensmittelvergiftung(Emetisches und Diarrhoe – Toxin)Wund – Generalisierte Infektionen

B. subtilis
Wundinfektion – Stichverletzungen des Auges durchStroh, erdbehaftete Fremdkörperverletzungen
Differenzierung von B. anthracis!Sie sind nicht bekapselte, bewegliche Keime, rufen β-Haemolyse hervor, sind apathogen inTierversuch

ENDEMauritius, 2006





























