Embed Size (px)
Citation preview
1
Daniel H Ward DDS
Heartland Study ClubHeartland Study Club
Topeka, KansasTopeka, Kansas
October 23, 2015October 23, 2015
Uncommon Common Sense: What YOU need to know NOW about Restorative Dentistry and Materials
Daniel H Ward DDSGraduated 1979 OSUGraduated 1979 OSUPrivate PracticePrivate Practice--Columbus, OhioColumbus, OhioAssistant Clinical Professor The Assistant Clinical Professor The
Ohio State UniversityOhio State University--13 years13 yearsFACD, FICD, FAGD, FASDAFACD, FICD, FAGD, FASDA
“I get by with a little help from my friends…” Dr Harry AlbersDr Harry Albers Dr Paul BelvedereDr Paul Belvedere Dr Gordon ChristensenDr Gordon Christensen Dr George FreedmanDr George Freedman Dr Geoff KnightDr Geoff Knight Dr Doug LambertDr Doug Lambert Dr Karl Dr Karl LeinfelderLeinfelder Dr Graeme Dr Graeme MilicichMilicich Dr Buddy Dr Buddy MopperMopper Dr Dr HienHien NgoNgo Dr Brian Dr Brian NovyNovy Dr Jorge Dr Jorge PerdagPerdagãoão Dr Robert Dr Robert SeghiSeghi Dr Irwin Dr Irwin SmigelSmigel Dr Ed SwiftDr Ed Swift
Company Affiliations AdDentAdDent BISCOBISCO Caulk/Caulk/DentsplyDentsply CentrixCentrix CliniciansClinicians’’ ChoiceChoice Coltene/WhaledentColtene/Whaledent GC AmericaGC America HeraeusHeraeus KulzerKulzer IvoclarIvoclar PulpdentPulpdent ShofuShofu SDISDI SSWhiteSSWhite TokuyamaTokuyama TriodentTriodent 33--MM
Some Images May be: Cropped
Rotated
Levels adjusted
No Images Were: Site adjusted
Enhanced to produce a better result
Enough about me,
How long have you been in practice?
Where do you practice?
What challenges do you have that you would like to have answered today?
Tell me about YOU!

2
Common sense is often uncommon
Health and appearance conscious
The Public has concerns about:
Appearance
Metals
Patients are more knowledgeable than ever
We must listen more to our patients

3
We must provide alternatives for our patients
…but the rightalternatives
Composite
The most USED
and ABUSED
Material in Dentistry
Composite
Uncommon, common sense
•What is the most important restoration that determines the long term prognosis of a tooth?
•Are flowable composites always an inferior restoration?
•Does fluoride present within the enamel of an un-prepared tooth margin result in a better bond between resin and tooth?
Uncommon, common sense
•Does the addition of fluoride to a resin result in efficacious fluoride release?
•Should preparations for tooth to be restored with a composite be the same as for a tooth to be restored with amalgam?
•What is the effect of warming composite immediately prior to placement?

4
MMinimally inimally IInvasive nvasive DDentistryentistry
Conservative approach
Remove only diseased portion of tooth
Preserve healthy tooth structure for future restorative needs
Surgical ModelSurgical Model
“Dentistry begets Dentistry”
“The more dentistry you do for a patient, the more dentistry they will
eventually need.”
“Dentistry begets Dentistry”
Re-Treatment CompleteNotice the lower anterior teeth
Lifetime of tooth often determined by first dentist intervention
15 Year Old
Fissurotomy bur
201.3VF
Conservative Tooth Preparation
169L330
5
Low Viscosity Flowable Composite
How do you restore?
Low Viscosity Flowable Composite
G-aenial Universal Flo
Homogeneous spherical particles
Better wear resistance
Higher flexural strength (167 MPa)
Filled 50% by volume
Good polishability
Visibly blends in well Mean particle size 200 nm
Low Viscosity Flowable Composite
Beautifil Flow 00
Unique glass ionomer filler particles
Releases fluoride and other ions
Neutralizes pH-Antibacterial
Reduced plaque accumulation
Good polishability
Visibly blends in well S-PRG (Surface pre-treated Glass Ionomer) Dispenser Gun
Tray
Compule Tray
Warmer
CALSETThermal Assisted Light Polymerization
WARMER
Improved flowability of composites
Improved marginal adaptation
Improved rate of polymer conversion
Improved surface hardness/durability/polishing.
Decreased curing time and increased depth of cure
Increased sculptability and ease in shaping anatomy
ADVANTAGESADVANTAGESThermal Assisted Light PolymerizationThermal Assisted Light Polymerization
Stansbury JW. Use of near-IR to monitor the influence of external heating on dental composite photopolymerization. Dent Mat 2004; 20(8).
Low Viscosity Flowable Composite & Warmed Composite
Completed Tooth Restorations

6
“Dentistry begets Dentistry”
“The more dentistry you do for a patient, the more dentistry they will
eventually need.”
“Dentistry begets Dentistry”
Re-Treatment CompleteNotice the lower anterior teeth
15 Year Old
Buildup dentin replacement with opaque darker hybrid –typically A3-A3.5
Buildup remaining form with shade similar to desired final color with hybrid (typically A1-A2)
Add special effects to simulate imperfections within tooth structure
Add translucent incisal hybrid or microfill
Add dentin shade
•Aura
•Miris
Add A-2
•Venus Pearl
•Kalore
•TPH Spectra
Add A-1
Add Characterization
Important-Junction must be invisible
Add Facial Surface
•Beautifil II
•Miris Enamel
•Kalore GT
•Esthelite Sigma QuickOptrasculpt

7
Finish and polish restoration
Restore adjacent tooth
Shape, finish and polish restorations
Restore opposite teeth
Pre-Operative
Finished Restorations
Marginal Integrity
Composite Direct Placement Challenges
Expose ends of enamel rods
EnamelEnamel
Enamel Bonding
96% inorganic carbonate hydroxyapatite 96% inorganic carbonate hydroxyapatite calcium phosphatecalcium phosphate
4% organic (tyrosine rich amelogenin 4% organic (tyrosine rich amelogenin protein) and waterprotein) and water
Enamel rods 4Enamel rods 4--8 microns in diameter8 microns in diameter Bonding occurs within enamel rodsBonding occurs within enamel rods HydrophobicHydrophobic

8
Sheared enamel Sheared enamel rodsrods
White Lines
Unprepared Margins
Expose fresh ends of the enamel rods with a very fine diamond
Koase K, Inoue S, Noda M, Tanaka T et al. Effect of burKoase K, Inoue S, Noda M, Tanaka T et al. Effect of bur--cut dentin on bond strength cut dentin on bond strength using two allusing two all--inin--one and one twoone and one two--step adhesive systems. step adhesive systems. J Adhes DentJ Adhes Dent. 2004;6:97. 2004;6:97--104.104.
Hosoya Y, Shinkawa H, Suefiji C, Nozaka Ket al. Effects of diamHosoya Y, Shinkawa H, Suefiji C, Nozaka Ket al. Effects of diamond bur particle ond bur particle size on dentin bond strength. size on dentin bond strength. Am J DentAm J Dent. 2004;17:359. 2004;17:359--364.364.
Use a fine 25 micron diamond when using self-etching primers
Exposing ends of enamel rods resulting inGreater angle than direction of enamel rods
Better bonding and less shearing of enamel rods
Class II Interproximal Margin Preparation
Expose the ends of the enamel rods to avoid tooth fracture at margins
Class II Interproximal Margin Preparation
Composite Composite PreparationPreparation
Amalgam Amalgam PreparationPreparation

9
Bevel Interproximal Enamel for better bonding and less shearing of enamel rods
Class II Interproximal Margin Preparation
Importance of flaring Class II Interproximals
Fractured tooth structure
Importance of flaring Class II Interproximals
Parallel preparation
Importance of flaring Class II Interproximals
Result
Post-Operative Sensitivity
Composite Direct Placement Challenges
Hydrodynamic Theory
Hydrodynamic Theory
Fluid flow within dentinal tubules causes PAINBrannstrom M. The Cause of post restorative sensitivity and its prevention. J Endod 1986;12:475-481.

10
Hydrodynamic Theory
Opened, unsealed dentinal tubules causes PAIN
DentinDentin
Dentin Bonding
70% inorganic carbonate hydroxyapatite 70% inorganic carbonate hydroxyapatite calcium phosphatecalcium phosphate
30% organic (collagen) and water30% organic (collagen) and water
Dentinal tubules 0.06Dentinal tubules 0.06--3 microns in diameter3 microns in diameter
Most Bonding occurs between dentinal tubulesMost Bonding occurs between dentinal tubules
HydrophilicHydrophilic
Oh NO, not another bonding lecture!
•What are MMP’s and what agents can affect their effects?
•What is the effect of the width of the hybrid layer and dentin bond strengths?
•What new Self-Etching Primer Dentin Bonding Agent has bond strengths to un-etched enamel greater than 40 MPa ?
Oh NO, not another bonding lecture!
•Is there a relationship between post-operative sensitivity and dentin bond strengths?
•What are the characteristics of alcohol, acetone and water based solvents of dentin bonding agents?
•What are Universal Dentin Bonding Agents?
Etched Dentin

11
Demineralize surfaceExpose collagen fibersRemove smear layer Increase porosity of intertubular dentinOpen up dentinal tubules Increase surface area
Etched Dentin
•Total Etch Technique Fill and Occlude open dentinal tubules
Bonding agent should not leave the dentinal tubules open
Method #1-Reducing Post-Op Sensitivity
Placement of Etchant
Total Etch Technique
“Moist” Dentin”
Rinsing of Etchant
Placement of Resin Primer
Apply multiple coats
Moist Moist
Placement of Resin Primer
“Overwet” Phenomenon
Tay FR, Gwinnett AJ, Wei Sh. The overwet phenomenon: a scanning electron microscopic study of surface moisture in the acid-conditioned, resin-dentin interface. Am J Dent. 1996;9(3):109-114.

12
Overdrying
Gwinnett AJ. Dentin bond strength after air drying and rewetting. Am J Dent. 1994;7(3):144-148.
Collapsed collagen fibrils
Overdrying
SEM Perdigao
Un-collapsed collagen fibrils Collapsed collagen fibrils
Proper Moisture Moisture Variability
Acetone
Alcohol
Water
Bonding Agent SolventsAir only syringe Warm air dryer
Air/water syringe Air/water syringe
Evaporating the solvent with dry air

13
Bond StrengthSensitivity
Variability
Lopez CL, Perdigao J, Lopes M et al. Dentin Bond Strengths of Simplified Adhesives:Effect of Dentin Depth. Compendium. 2006;27(6):340-345.
17.6(+/-5.9)
18.4(+/-4.8)
14.2(+/-7.0)
Deep
Dentin
21.0(+/-7.4)
18.9(+/-4.1)
22.1(+/-2.8)
Superficial
Dentin
Clearfil
Liner
Bond
Optibond
Solo
Single Bond
Adhesive
System
Mean shear bond strength in MPa
Effect of Dentin Depth on Bond Strengths
•Occludes tubules
•Anti-bacterial
GLUMA
•Occlusions
Total Etch Technique
Summary
Most technique sensitiveRequires proper attention to detailUse in ideal sized preparations
Total Etch Technique
Materials-4th
Generation
Acetone solvent Alcohol solvent

14
Total Etch Technique
Materials-5th
Generation
Acetone solvent Alcohol solvent Water solvent
•Self Etch Technique Never leave the dentinal tubules open
Bonding agent should not leave the dentinal tubules open
Method #2-Reducing Post-Op Sensitivity
Acid-groupsHydrophilic end
etches tooth structure (self
limiting)
Spacer-chainlink between
functional groups
Methacrylate-groupHydrophobic end
connects to polymer-network
COOH
COOH
CH 2
CH 2
O
OO
O
Self-Etching Primer“Self Etching” Primer
Acidifying Primer accompanies etch
Acid reaction is self-limiting
Lohbauer U, Nikolaenko SA, Petschelt A, Frankenberger R.. Resin Tags do not contribute to dentin adhesion in self-etching adhesives. J Adhes Dent. 2008;10(2):97-103 .
Resin Tags do not Contribute to Dentin Adhesion in SE Adhesion Self-Etch Technique
Challenges
Decreased bond strength to un-etched enamel
Marginal gap formation with un-etched enamel
Bond incompatibility to self-cure and dual-cure resins
More susceptible to hydrolytic degradation resulting in significantly diminished bond strengths over time

15
Self etching Primer
37% H3PO4 etched Unprepared enamel surface for 15s.
Popular SE primer etched Unprepared enamel surface
•Tests confirm that preparing the enamel margin improves bond strength especially with self-etch dentin bonding agents
Substrate All-Bond UniversalSelf-Etch
All-Bond UniversalTotal-Etch
Uncut Enamel 18.7±6.7 31.4±7.1
Cut Enamel 29.0±5.5 35.6±3.6
Bisco in-house data.. Lee IS, Son SA, Hur B, Kwon YH, Park JK. The effect of additional etching and curing mechanism of composite resin on the dentin bond strength. J Adv Prosthodont. 2013;5:467-484.
55% improvement
Effect of Enamel Etching-Bond Strength
•Tests show that etching uncut enamel with phosphoric acid increases bond strength to enamel with 1- bottle dentin bonding agents
Substrate All-Bond UniversalSelf-Etch
All-Bond UniversalTotal-Etch
Uncut Enamel 18.7±6.7 31.4±7.1
Cut Enamel 29.0±5.5 35.6±3.6
Bisco in-house data.. Lee IS, Son SA, Hur B, Kwon YH, Park JK. The effect of additional etching and curing mechanism of composite resin on the dentin bond strength. J Adv Prosthodont. 2013;5:467-484.
67% improvement
Effect of Enamel Etching-Bond Strength
Substrate All-Bond UniversalSelf-Etch
All-Bond UniversalTotal-Etch
Uncut Enamel 18.7±6.7 31.4±7.1
Cut Enamel 29.0±5.5 35.6±3.6
Bisco in-house data.. Lee IS, Son SA, Hur B, Kwon YH, Park JK. The effect of additional etching and curing mechanism of composite resin on the dentin bond strength. J Adv Prosthodont. 2013;5:467-484.
22% improvement
Effect of Enamel Etching-Bond Strength
•Tests show that etching cut enamel with phosphoric acid increases bond strength to enamel with 1- bottle dentin bonding agents

16
•SEM analysis found no marginal gapformation of enamel etched w phosphoric acid prior to application of a self-etching 6th
generation bonding agent (Clearfill SE) following thermocycling•SEM analysis reported marginal gap formationof enamel not etched w phosphoric acid prior to application of a self-etching 6th generation bonding agent (Clearfill SE) following thermocycling
Souza-Junior EJ, Prieto LT, Araújo CT, Paulillo LA. Selective enamel etching: effect on marginal adaptation of self-etch LED-cured bond systems in aged Class I composite restorations. Oper Dent. 2012;37:195-204.
Effect of Enamel Etching-Marginal Gaps
Solution: “Etching prepared enamel w phosphoric acid promoted better marginal integrity with self-etching bonding agents.”
Souza-Junior EJ, Prieto LT, Araújo CT, Paulillo LA. Selective enamel etching: effect on marginal adaptation of self-etch LED-cured bond systems in aged Class I composite restorations. Oper Dent. 2012;37:195-204.
Effect of Enamel Etching-Marginal Gaps
When the pH of a dentin bonding agent is too low (more acidic), tertiary amines (necessary for the polymerization reaction) are deactivated resulting in bond incompatibility with self and dual cured resins.
Bond Incompatibility with Self and Dual Cured Resins
Suh BI, Feng L, Pashley DH, Tay FR. Factors contributing to the incompatibility between simplified-step adhesives and chemically-cured or dual -cured composites. Part III. Effect of acidic resin monomers. J Adhes Dent 2003;5:267-282.
Solution: Use of a higher pH (>3.0)self-etching dentin bonding agent does not inactivate the tertiary amines and allows for polymerization.
Suh BI, Feng L, Pashley DH, Tay FR. Factors contributing to the incompatibility between simplified-step adhesives and chemically-cured or dual -cured composites. Part III. Effect of acidic resin monomers. J Adhes Dent 2003;5:267-282.
Bond Incompatibility with Self and Dual Cured Resins
pH=3.2
Solution: Use a dual-cure activator
Bond Incompatibility with Self and Dual Cured Resins
“The cured layer of 1-step self-etching adhesives is hydrophilic and a permeable membrane.”
Tay F, Suh B, Pahsley D, Carvalho R. Single Layer Adhesives are Permeable membranes. J Dent 2002;30:371-382.
Hydrolytic Degradation

17
Solution: Use 2 layers-a hydrophilic layer covered with a hydrophobic layer
Yoshida Y, Yoshihara K, Nagaoka N, Hayakawa S, Tori Y, Ogawa T, Osaka A, Van Meerbeek B. Self-assembled nano-kayering at the adhesive interface. J Dent Res 2012;9:376-381.
Hydrolytic Degradation
Solution: Use MDP containing bonding agents which become hydrophobic upon polymerization due to high amount of cross-linkage.“MDP-containing adhesives form nano-layering at the adhesive interface. Stable MDP-Ca salt deposition along with nano-layering may explain the high stability of MDP-based bonding.”
Yoshida Y, Yoshihara K, Nagaoka N, Hayakawa S, Tori Y, Ogawa T, Osaka A, Van Meerbeek B. Self-assembled nano-kayering at the adhesive interface. J Dent Res 2012;9:376-381.
Hydrolytic Degradation
Self Etch Technique
OptiBond XTR
6th generation DBA that effectively etches enamel
Unprepared enamel surface
Etched with 37% Phosphoric Acid OptiBond XTR 6th Generation DBA
Popular 6th Generation DBA Popular 7th Generation DBA
Swift E, et al. J Esthet Restor Dent. 2011;23(6):390-398.
Self Etch Technique
OptiBond XTR
Self Etch Technique
OptiBond XTR
2 component self-etch 15% filled by volumeHydrophilic acidic self-etching primer with
enhanced etching capabilitiesHydrophobic adhesive to maximize
material compatibility, increase strength and promote bond durability

18
Self Etch Technique
OptiBond XTR
Primer contain acetone, alcohol and water solvents
Low film thickness (5 micron)Bonds to gold, non-precious metal,
zirconia, porcelain Direct and indirect restorative procedures
Seventh Generation DBA
BeautibondDual acidic monomersLow film thickness (5 micron)RadiopaqueEasy to use-single application 10 sec
Self Etch Technique
Materials 6th & 7th
Generation
Sixth Generation Seventh Generation
All-Bond SE Clearfil SE Protect
BeautiBond One Coat 7.0OptibondXTR
Long Term Dentin Bond StabilityMMP-Matrix MetalloproteasesMMPs are naturally occurring proteases
involved in dentin formation and trapped during odontogenesis
Not bacteria but proteolytic enzymes found within dentin capable of degrading collagen within newly created adhesive hybrid layers
Low pH causes dentin to release these inherent MMPs which attack exposed collagen fibrils
Osorio R, Yamauti M. Osorio E., et al. Effect of dentin etching on metalloproteinase-mediated collagen degradation. Eur J Oral Sci 2011;119:79-85.
Long Term Dentin Bond StabilityCysteine Proteases (Cathepsins)
Lysosomal enzymes that become activated in lysosomes by a low pH
Secreted by osteoclasts in bone resorption
Regulated by chondroitin
Collagenase activity breaks down collagen and hydrolyzes collagen into small peptides
Terasariol Il, Geraldeli S., ,Minciotti Cl., et al., Cysteine catepsins in human dentin pulp complex. J Dent Res 2011; 90:506-11.
MMP-Matrix Metalloproteases
Carrilho et al., JDR 2007; 86; 529Brackett et al.,Operative Dentistry; 2009;34(4):381-385
In-vivo 12 m w/PBNT (Acetone)
Immediate (MPa)Control 29.3 (9.2)CHX 32.7 (7.6)
w/CHX in 12 m
14 mo (MPa)Control 19.0 (5.2)CHX 32.2 (7.2)

19
Potential MMP Inhibitors
Long Term Dentin Bond Stability
Chlorhexidine (CHX)
Benzalkonium Chloride
MDPB ((12-methacryloxydodecalpyridinium bromide)
Galardin (mimics MMP-binds Zn atom) (inhibits tumor growth and metastasis)
Epigallocatechin-3-gallate (green tea polyphenol)
Perdigao J, Resi A, Loguercio AD. Dentin Adhesion and MMPs: A Comprehensive Review. J Esthet Restor Dent 2012: 25:219-241.
Disinfect to prevent MMPs
Use Etchant containing 1% Benzalkonium Chloride
TE-Apply 2% Chlorhexidine after acid etching for 30 sec
SE-Apply 2 coats 2% Chlorhexidine prior to application of primer
OR
Long Term Dentin Bond Stability
Disinfect to prevent MMPs
MDPB (12-methacryloxydodecalpyridinium bromide)
Long Term Dentin Bond Stability
Pashley DH, Tay FR, Imazato S. Hot to Increase the durability of Resin-Dentin Bonds. Compend. 2010;32(7):60-64.
• SE 1-step adhesives are too hydrophilic and permeable even after polymerization
• The best way to minimize these weaknesses is to apply a neutral-pH, hydrophobic adhesive resin layer in a separate step
• Acidic components cause incompatibility with self-cured composites.
• 3-step, etch-and-rinse adhesives remain the “gold standard” in terms of adhesive durability.
Dentin Bonding Solutions
De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Broem M, Van Meerbeek B. A Critical Review of the Durability of Adhesion to Tooth Tissue: Methods and Results. J Dent Res. 2005;84(2):118-132.
Selective Etch TechniqueApply etch to enamel only for 15 secondsWash thoroughlyPlace self-etching primer
Frankerger R, Lohbauer U, Roggendorf MJ, Naumann M, Taschner M. Selective enamel etching reconsidered:better than etch-and-rinse and self etch? J. Adhes Dent. 2008;10:339-344.
Selective Etch TechniqueHigh Viscosity allows precise placementContains BAC

20
Selective Etch TechniqueAllows total etch or self etch of enamel
and/or dentin
G-aenial Bond
Selective Etch TechniquePrecursor to “Universal” Bonding agentsBond strength same to total vs self etch
Dentin Bond Strength
Self-Etch Total Etch Moist
Total Etch Wet
Total, Self or Selective Etch Universal Bonding
Materials
Total-etch, self-etch or selective-etch technique
Can be used for direct and indirect restorations
Bond to all indirect substrates-metal, ceramics, zirconia, porcelain and lithium disilicate.
Compatible with light-cured, self-cured and dual-cured composite and luting cements.
Universal Bonding Materials
Total, Self or Selective Etch
All-Bond UniversalTotal-etch, self-etch or selective-etch
Single bottle for direct and indirectrestorations
High bond strengths to metal, ceramics, zirconia, porcelain & lithium disilicate.
Compatible with light-cured, self-cured and dual-cured composite and luting cements since pH is 3.2
Becomes hydrophobic upon setting
Total, Self or Selective Etch Total Etch vs. Self EtchShear bond strength of Universal Adhesives on Tooth Structures MPa*
*Manufacturer supplied data

21
Universal Bonding Materials
Total, Self or Selective Etch Universal Bonding
Materials
Total, Self or Selective Etch
•Total Etch Technique Never open the dentinal tubules
Bonding agent should not leave the dentinal tubules open
Method #3-Reducing Post-Op Sensitivity
Resin-Modified Glass Ionomer
RMGI Liner
No dentin conditionerneeded due to self-etch
primer component
RMGI BaseReprepare
Dentin conditionerpreferred to achieve optional dentin bond

22
10. It’s not necessary
9. It takes more time
8. It costs more money
7. I don’t understand which product to use
6. Not necessary with today’s Hundredth generation bonding agents
TOP TEN REASONS:GI isn’t used under every restoration
5. I don’t know how to use
4. Not as strong: I “bond” everything-holding tooth together and making it stronger
3. It doesn’t bond as well to dentin as resin
2. Fluoride release is transient
1. Old fashioned: used before better bonding agents were available
TOP TEN REASONS:GI isn’t used under every restoration
••Make initial access opening w small burMake initial access opening w small bur
••Use slow speed to remove decayUse slow speed to remove decay
••Use high speed to refine preparationUse high speed to refine preparation
••Smooth margins with a football diamond.Smooth margins with a football diamond.
Clinical Class I Restoration
••Completed PreparationsCompleted Preparations
Ivoclar P-1
••Place glass ionomer base/linerPlace glass ionomer base/liner
••Etch enamel then dentin, wash and dryEtch enamel then dentin, wash and dry
••Place & scrub multiple coats bonding Place & scrub multiple coats bonding agent, wait, evaporate solvent and cureagent, wait, evaporate solvent and cure
••Place composite and adapt to sidesPlace composite and adapt to sides
•If large use incremental layers
•Cure thoroughly
Ivoclar
Astropol
SS White
Jazz
Caulk Enhance/POGO
••Blend margins with finishing carbidesBlend margins with finishing carbides
••Adjust occlusionAdjust occlusion
••Finish and polishFinish and polish
Etch, wash/dry and apply surface sealantEtch, wash/dry and apply surface sealant

23
Summary
Best reduction of post-operative sensitivity
Insurance of fluoride releaseBest bond to enamelLong term stable bond to dentinUse in majority of posterior preparations
Total Etch with RMGI Liner/Base So, Now do you Understand?Cna yuo raed tihs? The phaonmneal pweor of the hmuan mnid, aoccdrnig to a rscheearch at Cmabrigde Uinervtisy, it dseno't mtaetr in waht oerdr the ltteres in a wrod are, the olny iproamtnt tihng is taht the frsit and lsat ltteer be in the rghit pclae. The rset can be a taotl mses and you can sitll raed it whotuit a pboerlm. Tihs is bcuseae the huamn mnid deos not raed ervey lteter by istlef, but the wrod as a wlohe. Azanmig hu h? yaeh and I awlyas tghuhot slpeling was ipmorantt!
•What’s all this talk about bulk fill composites?
•Polymerization shrinkage and polymerization shrinkage stress are the same
•To achieve good Class II interproximal contacts with composite, you just use the same armementarium as amalgam
WhatWhat’’s new under the sun with s new under the sun with Composites?Composites?
New Filler TechnologyNew Filler TechnologyGiomer FillersGiomer Fillers
Unique Filler particles made of set glass ionomer with special surface coating
Set Glass Ionomer Material Surface Modified Pre-Reactive Glass Ionomer Filler
Surface modified layer
Glass Ionomer phase
Glass Core
New Filler TechnologyNew Filler TechnologyGiomer FillersGiomer Fillers
BeautiSealant BeautiBond
Beautifil IIBeautifil Flow Plus
Agl MicrofillAgl MicrofillHeliomolarHeliomolar
MicroMicro--HybridHybridMiris, Point4, Miris, Point4, EsthetX, Venus EsthetX, Venus
NanoclusterNanoclusterFiltek SupremeFiltek Supreme
NanoNano--HybridHybridSynergy Nano, Synergy Nano, Tetric EvoTetric Evo--Ceram, Ceram, KaloreKalore
New Filler TechnologyNew Filler Technology

24
Low Shrinkage CompositesLow Shrinkage Composites
Nano/Hybrids in green
Open Margin Cracked Enamel
(white line)
Effects of polymerization shrinkage STRESS
Fractured Cusp
Prepolymerized Filler
Average Size 17 µm400 nm Strontium Glass
100 nm Lanthanoid fluoride
Glass Fillers
700 nm Strontium Glass700 nm Fluoroaluminum Silicate Glass
Non-aggregated nano silica filler
16 nm Silica filler
KaloreKalore
New Filler TechnologyNew Filler TechnologyNanofill/HybridNanofill/Hybrid
New Filler TechnologyNew Filler TechnologySpheroidal FillersSpheroidal Fillers
Easy polishing and retention
Blends well into tooth structure
Esthelite Sigma Quick-1 layer
Omega-2-3 layers
Estelite Sigma Quick
1μm
New Filler TechnologyNew Filler TechnologySpheroidal FillersSpheroidal Fillers
1μm
Estelite Sigma Quick
4 Seasons
Venus
Filtek Supreme Premise
Nano Clusters
(5,000 Magnification)
Tetric Evo-Ceram
1μm
DX-511
MW 895
BIS-GMA
MW 512
UDMA
MW 470
TEGMA
MW 286MW=Molecular Weight
New Resin TechnologyNew Resin TechnologyNanofill/HybridNanofill/Hybrid

25
Concern about bis-GMA
Shrinkage of bis-GMA,TEGMA
Higher molecular weight-less shrinkage
New advances possible through resin technology
DX-511
New Resin TechnologyNew Resin TechnologyNanofill/HybridNanofill/Hybrid
Increasing the size and molecular weight of monomers reduces overall shrinkage
Low Molecular weight
Shrinkage
High Molecular weight
Polymerization
Less Shrinkage
New Resin TechnologyNew Resin TechnologyNanofill/HybridNanofill/Hybrid
Pre-Operative
Completed Preparation
KaloreKalore--Clinical CaseClinical Case
Fuji II LC Resin Modified Glass Ionomer Base
Kalore
Venus Diamond
New Resin Nanofill/Hybrid New Resin Nanofill/Hybrid Composites used in my officeComposites used in my office
Bulk Fill CompositesBulk Fill Composites
Allow many posterior restorations to be built up in 1 segment
Descriptions– “Stick the stuff in the hole and cure”– Evolutionary– Monolithic
Physical Advantages– Deeper depth of cure– Less Polymerization Shrinkage– Less Polymerization Shrinkage Stress– Reduced likelihood of air voids between layers

26
Bulk Fill CompositesBulk Fill Composites
Modes of Action– Improved initiators– Greater translucency allows better light transmission– Delayed gel state formation– Increased elasticity
Materials– Flowable– Conventional
Advantages– Quicker, easier– Less chance of enamel and cusp fractures– Increased likelihood of adequate resin polymerization
Bulk Fill Flowable CompositesBulk Fill Flowable CompositesLow Shrinkage StressStress
•Surefill SDR
• Voco Xtra
•Beautifil Bulk Flowable
•Venus Bulk Fill
Surefill SDRSurefill SDR
•Reduced polymerization shrinkage stress
• Bulk fill to 4mm
•Increased sensitivity to light
Great placement with metal tips
•Self-leveling
•A1, A2, A3 Universal shades
Roggendorf MJ1, Krämer N, Appelt A, Naumann M, Frankenberger R. Marginal quality of flowable 4-mm base vs. conventionally layered resin composite. J Dent. 2011;39:643-647.
To measure Shrinkage… Composite is cured unconstrained
To measure Shrinkage… Composite is cured unconstrained
To measure Stress… Composite is Always bonded

27
To measure Stress… Composite is Always bonded If no adhesive is used…
And the tooth is restored with resin…
…and the resin is light-cured
…and the resin is light-cured
There is shrinkage & gap formation

28
If adhesive is used.. If adhesive is used..
If adhesive is used.. If adhesive is used..
The composite tries to Shrink..
The adhesive tries to hold..
Stress buildsStress builds--upup
Marginal gap formation may result
29
Or white line/sheared enamel rods
Or fractured cusps
Layering techniques may reduce polymerization shrinkage stress
But air voids are common between
layers
“Modulator” slows down polymerization allowing relaxation
resulting in reduced stress
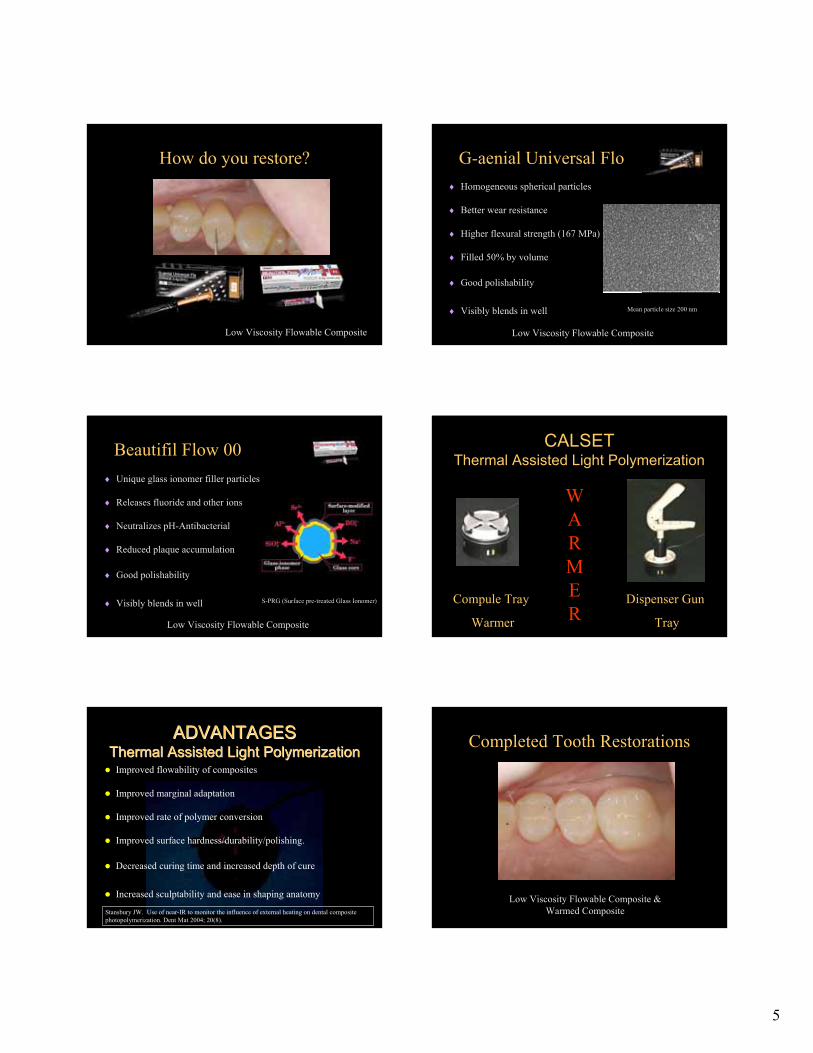
Polymerization Shrinkage Polymerization Shrinkage StressStress(MPa)(MPa)
Voco Xtra BaseVoco Xtra Base
•Reduced polymerization shrinkage stress
• Able to bulk fill up to 4mm
•Very sensitive to light
•Good adaptation and self-leveling
•A2, Universal shades
•Come in compules and syringes
BeautifilBeautifil Bulk FlowBulk Flow
•Very heavily filled by volume
• Able to bulk fill up to 4mm
•Giomer filler particles
•Two shades (Dentin and Universal)`
•Come in compules and syringes

30
Venus Bulk FillVenus Bulk Fill
•Reduced polymerization shrinkage stress
• Able to bulk fill up to 6mm
•Good adaptation and self-leveling
•Universal shade
•Come in compules and syringes
Bulk Fill Posterior CompositesBulk Fill Posterior CompositesLow Shrinkage StressStress
• Voco Xtra Fill
•Beautifil Bulk Flow
•Tetric Evo-Ceram Bulk Fill
•Fill It Bulk Fill
•Sonic Fill
Voco Xtra FillVoco Xtra Fill
•1.7% volumetric shrinkage
• Able to bulk fill up to 4mm
•Very light sensitive
•One universal shade
•Very translucent
•Come in compules and syringes
BeautifilBeautifil Bulk FillBulk Fill
•Very heavily filled by volume
• Able to bulk fill up to 4mm
•Giomer filler particles
•Two shades (A and Universal)
•Better color blending-not too translucent
•Come in compules and syringes
Tetric EvoTetric Evo--Ceram Bulk FillCeram Bulk Fill
•Low shrinkage stress-
• Able to bulk fill up to 4mm
•Comes in 3 shades
•Smooth surface and low wear
•Come in compules and syringes
Tetric EvoTetric Evo--Ceram Bulk FillCeram Bulk Fill
Lucirin Camphor‐quinone
nm
Ivocerin
Unique Reactive Initiator allows greater depth of cure
Ge
OO
O O

31
Tetric EvoTetric Evo--Ceram Bulk FillCeram Bulk Fill
Pre-polymerized filler particles help to absorb polymerization shrinkage stress
Tetric EvoTetric Evo--Ceram Bulk FillCeram Bulk Fill
“A” Shade
“B” Shade
“W” Shade
Sonic Energy Assisted Light Sonic Energy Assisted Light PolymerizationPolymerization
Sonic FillSonic Fill
Improved flowability of composites
Improved marginal adaptation
5mm depth of cure
Increased sculptability and ease in shaping anatomy
Composite designed specifically for use
ADVANTAGESADVANTAGESSonic Energy Assisted Light Sonic Energy Assisted Light
PolymerizationPolymerization
Sonic Energy Assisted Light Sonic Energy Assisted Light PolymerizationPolymerization
Sonic FillSonic Fill
Sonic Energy Assisted Light Sonic Energy Assisted Light PolymerizationPolymerization
Sonic FillSonic Fill

32
Interproximal Contacts
Composite Direct Placement Composite Direct Placement ChallengesChallenges
Christensen JJ. Duplicating the form and function of posterior teeth with Class II resin-based composite. Gen Dent. 2012;60:104-108.
Microband Focu-tip Trimax
Interproximal ContactsInterproximal ContactsOriginal Attempted SolutionsOriginal Attempted Solutions
Not enough pressure to separate teeth
Fly off
Wedge in the way
Interproximal ContactsInterproximal ContactsSectional Matrix ChallengesSectional Matrix Challenges
Interproximal ContactInterproximal Contact
SolutionSolution
Contact Perfect
Interproximal ContactInterproximal Contact
SolutionSolution
Contact Perfect
TofflemireTofflemire vs. Sectional vs. Sectional MatricesMatrices
Tofflemire System
Thin contact at the marginal ridge
Non‐anatomical Foodtrapbelowcontact
Increasedlikelihoodof:fracture,recurrentcariesandperiodontaldisease.
SectionalMatrices
Broad contacts at the proper height of contour
Anatomicallyshapedcontacts
TightContactsPropercontactsthatflossproperlyandpromotegingivalhealth

33
Interproximal ContactInterproximal Contact
RetainersRetainers
TrioDent/Palodent
Universal V3 Ring Narrow V3 Ring
Interproximal ContactInterproximal Contact
Also Available as:Also Available as:
Palodent Plus
Universal Ring Narrow Ring
Interproximal ContactInterproximal Contact
BandsBands
TrioDent/Palodent Plus
Bendable tab
Side holes for easy removal
Holes allow grip with Pin-Tweezers
Marginal Ridge Contour
Pin Tweezers
Interproximal ContactInterproximal Contact
BandsBands
TrioDent/Palodent Plus
Bicuspid
Molar
Sub-gingival Molar
Interproximal ContactInterproximal Contact
Anatomical WedgesAnatomical Wedges
Wave Wedges
Pin Tweezers
TrioDent/Palodent Plus

34
Challenge:
Adjacent Class II Composite Restorations
Prepare enamel margins
Place contoured
band, wedge & V-Ring
Selective etching
Wash thoroughly
Apply bonding agent
Fill box 2/3’s full
Compress w 1P
Cure
Finish buildup
Cure
Sonicfill
Remove wedge peel band back
Cure IP
Remove band & cure ContacEZ
Re-contour diamond/finishing
carbides
Finishing strips
Place V-Ring on adjacent tooth
Burnish desired contact area
Selective etching
Place Universal bonding agent
Light Cure
Peel back band
Cure from both sides at
gingiva
Place Composite as before
Light Cure

35
Finish and polish
Adjust occlusion
V4 Clear‐Metal Matrix System
•Transparent ring tines, wedge and matrix band to allow cure –through – great with bulk fill and deep cavities
•Very versatile – can be used on missing cusps, large boxes and where little tooth structure remains
•Superior grip, even on severely compromised teeth
V4 Ring
Clear tinesLight passes through the tines
New tine shapeIncreased grip and stability
VersatileCan be used:
•where little tooth structure remains•on large boxes •misaligned/malpositionedteeth •missing cusps•more compatible with circumferential bands
Easier to clean and more durable tines
ClearMetal Matrix
Resin filled Micro‐Windows for optimum curing
•Hundreds of cure‐through micro‐windows•Similar curing to plastic matricesHighly anatomical
•SuperCurveMatrix•Malleable• Burnishale
Non‐stick•Transparent, non‐stick coating•Leaves no marks on restoration
ClearMetal Matrix
Resin filled Micro‐Windows for optimum curing
•Hundreds of cure‐through micro‐windows•Similar curing to plastic matricesHighly anatomical
•SuperCurveMatrix•Malleable• Burnishale
Non‐stick•Transparent, non‐stick coating•Leaves no marks on restoration
ClearMetal Matrix
Small tip light output Small tip light output through band

36
V4 Wedge
•Notches split the wedge into 3 sections
•Sections compress and expand independently allowing for more interproximal anatomical variations
•Transparent, to allow cure‐through
•Great sealing on the gingival margin whatever the interproximal anatomy
We must communicate better with our patients
– Patients are more informed
– Patients are more demanding
– Patients want choices
•I’m too old to change to Digital Radiography
•I don’t take intra-oral photographs because I don’t know how
•Where should I buy a camera for my office?
Trust me, ITrust me, I’’m the doctor and I know m the doctor and I know what is best for you!what is best for you!
•How do patients often judge their dentists?
•Show and Tell
•Is the golden proportion really golden?
Trust me, ITrust me, I’’m the doctor and I know m the doctor and I know what is best for you!what is best for you!
We must communicate better with our patients
Digital RadiographyDigital Radiography
Digital Radiography
37
Advantages– Instant Viewing
– Able to manipulate contrast-magnification
– WOW factor to patients
– More environmentally friendly
– Email to insurance companies-films not lost
– Able to access remotely
– Adds value and higher perception if selling practice
Disadvantages– Sensor can be bulky for some patients
– Sensor is expensive and may need to be shared
Digital Radiography Digital Dental Photography
Clinipix
Procedures, Conditions, PathologyProcedures, Conditions, Pathology
Uses of Dental Photography Patient Communication
Allows them to see what you seeAllows them to see what you see
Uses of Dental Photography Patient Communication
Uses of Dental Photography Patient Communication
Imaged Full Face SmilesImaged Full Face Smiles
Uses of Dental Photography Uses of Dental Photography DiagnosticDiagnostic
Measurement of tooth dimensionsMeasurement of tooth dimensions
GoldenGolden ProportionProportion
78% width/height ratio78% width/height ratio1:16 House Rule1:16 House Rule
REDRED ProportionProportion

38
Uses of Dental Photography Uses of Dental Photography Laboratory CommunicationLaboratory Communication
““Singular SuccessSingular Success””
Uses of Dental Photography Uses of Dental Photography Laboratory CommunicationLaboratory Communication
Root fractureRoot fracture
Uses of Dental Photography Uses of Dental Photography Laboratory CommunicationLaboratory Communication
Paint tints onto shade tabPaint tints onto shade tab
Uses of Dental Photography Uses of Dental Photography Laboratory CommunicationLaboratory Communication
Take photos and send to labTake photos and send to lab
Print JPEG
Uses of Dental Photography Uses of Dental Photography Laboratory CommunicationLaboratory Communication
““Singular SuccessSingular Success”” Periodontists, Orthodontists, Endodontists, Periodontists, Orthodontists, Endodontists, Oral Surgeons, PathologistsOral Surgeons, Pathologists
Uses of Dental Photography Uses of Dental Photography Communication w/ SpecialistsCommunication w/ Specialists

39
Uses of Dental Photography Uses of Dental Photography Communication w/ SpecialistsCommunication w/ Specialists
E Mail w/ SpecialistsE Mail w/ Specialists
Uses of Dental Photography Uses of Dental Photography Communication w/ SpecialistsCommunication w/ Specialists
E Mail w/ SpecialistsE Mail w/ Specialists
Uses of Dental Photography Uses of Dental Photography Communication w/Insurance CoCommunication w/Insurance Co
DocumentationDocumentation DocumentationDocumentation
Uses of Dental Photography Uses of Dental Photography Medical/LegalMedical/Legal
Denture TryinDenture Tryin
Uses of Dental Photography Uses of Dental Photography SelfSelf--EvaluationEvaluation
Learning from every caseLearning from every case
Uses of Dental Photography Uses of Dental Photography SelfSelf--EvaluationEvaluation

40
••Canon Rebel T5i camera bodyCanon Rebel T5i camera body
••Canon 100mm macro EF lensCanon 100mm macro EF lens
••Canon MRCanon MR--14EX ring flash14EX ring flash
Digital Dental PhotographyDigital Dental Photography
•100-105mm macro w 1:1 capabilities
•Ring flash-TTL capabilities
•Rhodium mirrors
•Cheek retractors
Single Lens Reflex (SLR)Single Lens Reflex (SLR)
Equipment needed
•ISO 200
•Flash Sync speed 1/200 second
•Aperture Priority (Av setting)
•Over exposure override +0.5-1.5 f stops
•Full face (1:10 but 1:15 digital) at f 8 or 11
•Full smile (1:2 but 1:3 digital) at f 22 or 32
•Closeup (1:1 but 1:1.5 digital) at f 32
•Manual focus
Single Lens Reflex (SLR)Single Lens Reflex (SLR)
Camera Settings
Digital Dental Photography
Shofu Eye Special C-II
Digital Dental Photography
Shofu Eye Special C-II
Digital Dental Photography
Shofu Eye Special C-II
41
Digital Dental Photography
Shofu Eye Special C-II
Shofu Eye Special C-II
Lightweight
All-in-on
Auto exposure system
Programmed Dental Modes- intra-oral, mirror, face, whitening
Camera indicates if you are at proper distance-Auto Zoom
Touch panel interface
Patients’ information can be input by QR code or entering patient number
Unique color tuning system
Eye Fi WirelessEye Fi Wireless
WOW Factor!WOW Factor!
Downloading & Printing ImagesDownloading & Printing ImagesDownloading & Printing Images
Eye Fi WirelessEye Fi Wireless
SD Card in cameraSD Card in camera InIn--Office WirelessOffice Wireless
Memory CardsMemory Cards
Downloading & Printing ImagesDownloading & Printing ImagesDownloading & Printing Images
Eye Fi WirelessEye Fi Wireless
Desktop ShortcutDesktop Shortcut Target FolderTarget Folder
Memory CardsMemory Cards
Downloading & Printing ImagesDownloading & Printing ImagesDownloading & Printing Images
Eye Fi WirelessEye Fi Wireless
Double click for PreviewDouble click for Preview
Memory CardsMemory Cards
Downloading & Printing ImagesDownloading & Printing ImagesDownloading & Printing Images

42
Photoshop ElementsPhotoshop Elements
Before
After
Quick Fix Mode/Smart FixQuick Fix Mode/Smart Fix
Viper SoftViper Soft SciCan Image FXSciCan Image FX Digident Digital DentistDigident Digital Dentist
Dental Imaging ProgramsDental Imaging Programs
Imaging ProgramsImaging Programs
Downloading & Printing ImagesDownloading & Printing ImagesDownloading & Printing Images
Dental Imaging LibrariesDental Imaging Libraries
Imaging ProgramsImaging Programs
Is this possible?Is this possible?
Downloading & Printing ImagesDownloading & Printing ImagesDownloading & Printing Images
ProportionProportion--based Imagingbased Imaging
Imaging ProgramsImaging Programs
Downloading & Printing ImagesDownloading & Printing ImagesDownloading & Printing ImagesImaging ProgramsImaging Programs
This is possible!This is possible!
ProportionProportion--based Imagingbased Imaging
Downloading & Printing ImagesDownloading & Printing ImagesDownloading & Printing Images

43
RED Proportion
Ward DH. Proportional smile design using the RED
proportion. Dent Clin North Am 2001;45:143-154.
“The proportion between the successive widths of the teeth as viewed from the frontal should remain
constant as you move distally”
RED Proportion
Ward DH. Proportional smile design using the RED
proportion. Dent Clin North Am 2001;45:143-154.
Without pre-existing constraints
Sample RED Proportions
Ward DH. Proportional smile design using the RED
proportion. Dent Clin North Am 2001;45:143-154.
x 0.8x 0.64x
x 0.7x 0.49x
x 0.62x 0.38x
Same size Central Incisors
Sample RED Proportions
Ward DH. Proportional smile design using the RED
proportion. Dent Clin North Am 2001;45:143-154.
Same Inter-Canine Width
Same Tooth Heights
DifferentCentral
Incisor W/H Ratios
“The majority (of dentists surveyed) chose central incisors that were as close to 0.75-0.78 width/height ratio as possible.”
Rosenstiel SF, Ward DH, Rashid RG. Dentists’ Preferences of Anterior
Tooth Proportion-A Web-based Study. J Prosthodont 2000;9:123-136.
Preferred RED Proportions
86% W/L Ratio 78% W/L Ratio
Width/Length Ratio of Central Incisors
Naturally Observed Dentist Preferred

44
Sterrett JD, Oliver T, Robinson F, et al. Width/length ratios of normal clinical crowns of the maxillary anterior dentition in man. J ClinPeriodontol 1999;26:153-157.
Width/Length Ratio of Central Incisors
Naylor CK. Esthetic Treatment Planning: The Grid Analysis System. J Esthet Restor Dent 2002;14:76-84. Wolfart S. Thormann H, Freitag S, Kern M. Assessment of dental appearance following changes in incisor proportions. J Oral Rehabil 2006;33:489-495.
Width/Length Ratio of Central Incisors
Rosenstiel SF, Ward DH, Rashid RG. Dentists’ Preferences of Anterior
Tooth Proportion-A Web-based Study. J Prosthodont 2000;9:123-136.
Width/Length Ratio of Central Incisors Summary Natural
Preston Proportion 86% W/L CI
Summary Preferred
70% RED Proportion 78% W/L CI
Preferred RED Proportions
78% w/hratio
78% w/hratio
78% w/hratio
Very Short
Normal
Very Tall
Same Inter-canine tooth width
Relative Tooth heights

45
Individual Tooth % of ICW
Ward DH. Using the RED Proportion to Engineer
the Perfect Smile. Dent Today 2008;27(8):112-117.
Rosenstiel SF, Ward DH, Rashid RG. Dentists’ Preferences of Anterior
Tooth Proportion-A Web-based Study. J Prosthodont 2000;9:123-136.
Summary
•The taller the tooth the smaller the preferred RED Proportion
•The shorter the tooth the larger the preferred RED Proportion
•The 78% w/h ratio of the central incisor should be maintained
Average Length Face
70% RED
Short Length Face
80% RED
Tall Length Face
62% RED
Short Average Tall
80% RED 70% RED 62% RED

46
Smile VisionSmile Vision Laboratory performedLaboratory performed
••PrePre--op Photoop Photo
••Template*Template*
••Imaged Photo*Imaged Photo*
Outsourced ImagingOutsourced Imaging
Imaging ProgramsImaging Programs
*Valley Dental Arts*Valley Dental Arts
Downloading & Printing ImagesDownloading & Printing ImagesDownloading & Printing Images Digital Dental CamerasDigital Dental Cameras
IF you want to call yourself a IF you want to call yourself a ““cosmeticcosmetic”” dentistdentist
IF you want to effectively IF you want to effectively communicate with your patients communicate with your patients and laboratoryand laboratory
IF you want to treat Maxillary IF you want to treat Maxillary Anterior Teeth with Indirect Anterior Teeth with Indirect RestorationsRestorations
IF you want to be able to IF you want to be able to defend yourself in a Court of defend yourself in a Court of LawLaw
Digital Dental CamerasDigital Dental Cameras
Then BUY, BUY, BUY a Then BUY, BUY, BUY a professional digital dental professional digital dental camera tomorrow!camera tomorrow!
Population 60+ by Age: 1900-2050Source: U.S. Bureau of the Census
0
20,000,000
40,000,000
60,000,000
80,000,000
100,000,000
120,000,000
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010 2020 2030 2040 2050
Num
ber o
f Per
sons
60+
Age60-64
Age65-74
Age75-84
Age85+
Number of people aged 60+
28 M42 M
57 M
92 M
US Population is Aging
Percentage 60+ by Age: 1900-2050Source: U.S. Bureau of the Census
0
0
0
0
0
0
0
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010 2020 2030 2040 2050
Perc
enta
ge 6
0+
Age60-64
Age65-74
Age75-84
Age85+
Percentage of people aged 60+
14%17%
18%
25%
10
5
15
20
25
30
US Population is Aging
• Xerostomia
• Difficulty maintaining oral hygiene
• Root exposures
• Some unable to tolerate long appointments
• Difficulty coming to office
• Fixed Income
US Population is Aging

47
US Population is Aging
DonDon’’t miss appointmentst miss appointments
AppreciativeAppreciative
Pay billPay bill
Often need more treatmentOften need more treatment
Refer new patientsRefer new patients
Say Thank You!Say Thank You!
60+ Patients are Wonderful Multiple Medications
Oral Environment Challenges-Xerostomia
Oral Environment Challenges-Xerostomia
“40% of all prescription drugs have dry mouth listed in the PDR as a possible side effect”
Chalmers J. Personal Communication. 2006.Chalmers J. Personal Communication. 2006.
Oral Environment Challenges-Xerostomia
In a published study of 131 different prescribed medications the most common side effect cited was xerostomia.
Smith RG, Smith RG, BurtnerBurtner AP. Oral sideAP. Oral side--effects of the most frequently prescribed drugs. effects of the most frequently prescribed drugs. Spec Spec Care Dent.Care Dent. 1994;14:961994;14:96--102. 102.
Oral Environment Challenges-Antacids
Ingredients:Calcium carbonate, adipic acid, corn starch, crospovidone, dextrose, flavors, malodextrin, sucrose, talc, colors.
OneOne--Visit TechniqueVisit Technique
Direct/Indirect Composite Direct/Indirect Composite OnlayOnlay

48

49
Before
After
OneOne--Visit TechniqueVisit Technique
Indirect/InIndirect/In--Office Composite Office Composite OnlayOnlay
•Open contact
•Decayed & Stained Margins
•Cracked cusp
•Take impression
•Pour with slurry water
•Trim interproximal
•Mark margins
•Pour solid model
•Coat w glycerin
•Buildup with composite
•Light Cure
•Translux
•Heat optional
•Triad
•Adjust contacts on solid model

50
•Tryin mouth
•Adjust & polish interproximals
•Sandblast intaglio
•BondBefore
After
OneOne--Visit TechniqueVisit Technique
Direct Bonded Provisional Direct Bonded Provisional CrownCrown
•Take alginate impression
•Pour up model
•Cut off crown
•Remove decay
•Place GI base
•Reprepare
•Fabricate vacuum formed matrix
•Seat with bis-acryl composite
•Trim and shape
•Adjust occlusion
•Bond

51
OneOne--Visit TechniqueVisit Technique
Immediate placement natural tooth Immediate placement natural tooth fiberfiber--reinforced bonded reinforced bonded ponticpontic
•Perio abcess
•Sub-gingival distal decay
•Carefully extract tooth
•Suture
•Tryin and prepare slots
•Shape root area to support tissue
•Cut lingual slot when trying in
•Place groove inline with 2 adjacent teeth
•Prepare fibers
•Place tooth
•Etch and bond
•3 months later

52
Oral Environment Challenges-Carbohydrates
Nutrition Facts: Serving Size: 8.3 fl. oz Calories: 140 Total Fat: 0g Sodium: 200mg Protein: 0g Total Carbohydrates: 28g Sugars: 28g
Nutrition Facts:16 fl oz; calories 140; total fat 0g; sodium 220mg; potassium 60mg; total carbs 28g; sugars 28g
Oral Environment Challenges-Bottled Water
Fluoride-less water Fluoridated water
Oral Environment Challenges-Illegal Drugs
“Meth mouth” or chronic marijuana use
Xerostomia patients
High carbohydrate users
Non-fluoridated water users
Drug abusers
Need TherapeuticRestorations
Composite Challenges
•Post-operative sensitivity
•Recurrent decay
•Achieving proper moisture
•Polymerization shrinkage
•Increased time-layering
•Technique sensitivity
Low post-op sensitivity
Fluoride Release
Moisture variability
No shrinkage
Bulk placement
Simple-more forgiving
Glass Ionomer
Look, we all know that Glass Ionomers are weak!
•Which wears more resin modified glass ionomers or pure glass ionomers?
•How many Mega pascals of polymerization shrinkage stress are exerted onto tooth structure when glass ionomer sets?
•What is the percentage of volumetric shrinkage of resin modified glass ionomers?

53
Look, we all know that Glass Ionomers are weak!
•According to research what is the average 10 year survival rate of posterior single surface glass ionomers?
•Which form(s) of glass ionomer can be used as an RUC under bonded crowns? Under conventionally cemented crowns?
•Will placement of large glass ionomers always result in less total tooth and restored surface than placement of composites?
Fuji IX Self Cure Glass Ionomer
Glass IonomerBase/Restorative
SDI Self Cure Glass Ionomer
•More highly filled-reduced wear
•Self-curing in 2.5-5 minutes
•No polymerization (setting) shrinkage stress
•Expansion/contraction similar to tooth
•High fluoride release
•Bioactive
Glass IonomerCharacteristics •Multiple cervical carious lesions
•Pediatric Patients
•Sealants
•Class V restorations
•Sandwich Technique
•Crown buildups
•Long term interim restorations
•Cements
Glass Ionomer Uses
High caries rate individuals
Glass Ionomer RestorationsGlass Ionomer Restorations
Remove decay and place matrices
Glass Ionomer RestorationsGlass Ionomer Restorations

54
Treat dentin with PAA
Glass Ionomer RestorationsGlass Ionomer Restorations
Place, shape and wait 2:30
Glass Ionomer RestorationsGlass Ionomer Restorations
Shape with diamonds w/ water
Glass Ionomer RestorationsGlass Ionomer Restorations
Dry and place Surface Sealant
No phosphoric acid
Glass Ionomer RestorationsGlass Ionomer Restorations
High caries rate individuals
Glass Ionomer RestorationsGlass Ionomer Restorations
Spoon out decay and refine prep
Glass Ionomer RestorationsGlass Ionomer Restorations

55
Place and rinse Poly-acrylic acid
Glass Ionomer RestorationsGlass Ionomer Restorations
Mix Gi and quickly place and push out
Glass Ionomer RestorationsGlass Ionomer Restorations
Allow to set 2:30
Glass Ionomer RestorationsGlass Ionomer Restorations
Hold down ginviva and shape
Glass Ionomer RestorationsGlass Ionomer Restorations
Dry and place surface sealant
Glass Ionomer RestorationsGlass Ionomer Restorations
High caries rate individuals
Glass Ionomer RestorationsGlass Ionomer Restorations

56
Pediatric Patients
Glass Ionomer RestorationsGlass Ionomer Restorations
Pediatric Patients
Glass Ionomer RestorationsGlass Ionomer Restorations
Class V root caries
Glass Ionomer RestorationsGlass Ionomer Restorations
Class V root caries
Glass Ionomer RestorationsGlass Ionomer Restorations
Repair around crown margins
Glass Ionomer RestorationsGlass Ionomer Restorations
Repair around crown margins
Glass Ionomer RestorationsGlass Ionomer Restorations

57
Long term interim restoration
Glass Ionomer RestorationsGlass Ionomer Restorations
Long term interim restoration
Glass Ionomer RestorationsGlass Ionomer Restorations
Long term interim restoration
Glass Ionomer RestorationsGlass Ionomer Restorations
Long term interim restoration
Glass Ionomer RestorationsGlass Ionomer Restorations
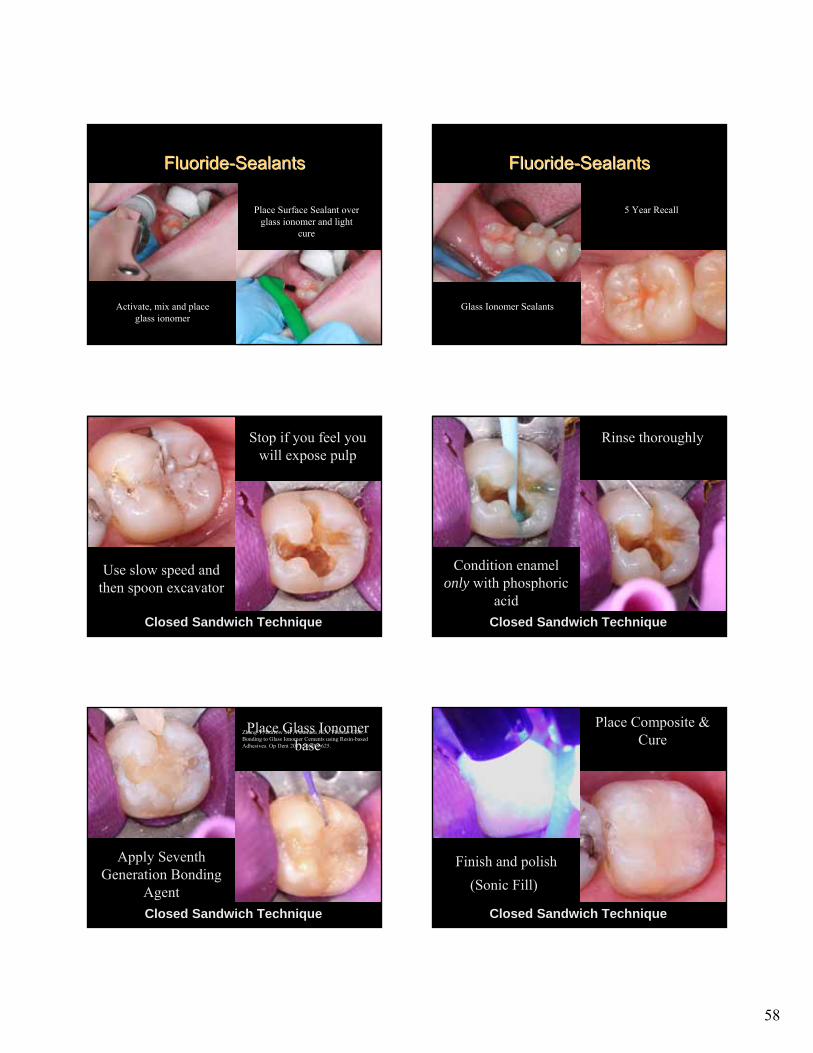
FluorideFluoride--SealantsSealants
Fuji Triage
FluorideFluoride--SealantsSealants
Decalcified areas in partially erupted tooth
Treat with phosphoric acid
58
FluorideFluoride--SealantsSealants
Activate, mix and place glass ionomer
Place Surface Sealant over glass ionomer and light
cure
FluorideFluoride--SealantsSealants
Glass Ionomer Sealants
5 Year Recall
Gain access to decay using a high speed
Closed Sandwich Technique
Use slow speed and then spoon excavator
Stop if you feel you will expose pulp
SEM of dentin treated with PCA
Condition dentin with poly-acrylic acid for 10 seconds and wash
Closed Sandwich Technique
CARD
OS
O et al. J D
ent 2010
Condition enamel only with phosphoric
acid
Rinse thoroughly
Re-prep if necessary after set
Place Glass Ionomer base
Closed Sandwich Technique
Wait 2:30
Apply Seventh Generation Bonding
Agent
Zhang Y, Burrow MF, Palamara JEA, Thomas CDL. Bonding to Glass Ionomer Cements using Resin-based Adhesives. Op Dent 2011;36:618-625.
Closed Sandwich Technique
Finish and polish
Place Composite & Cure
(Sonic Fill)
59
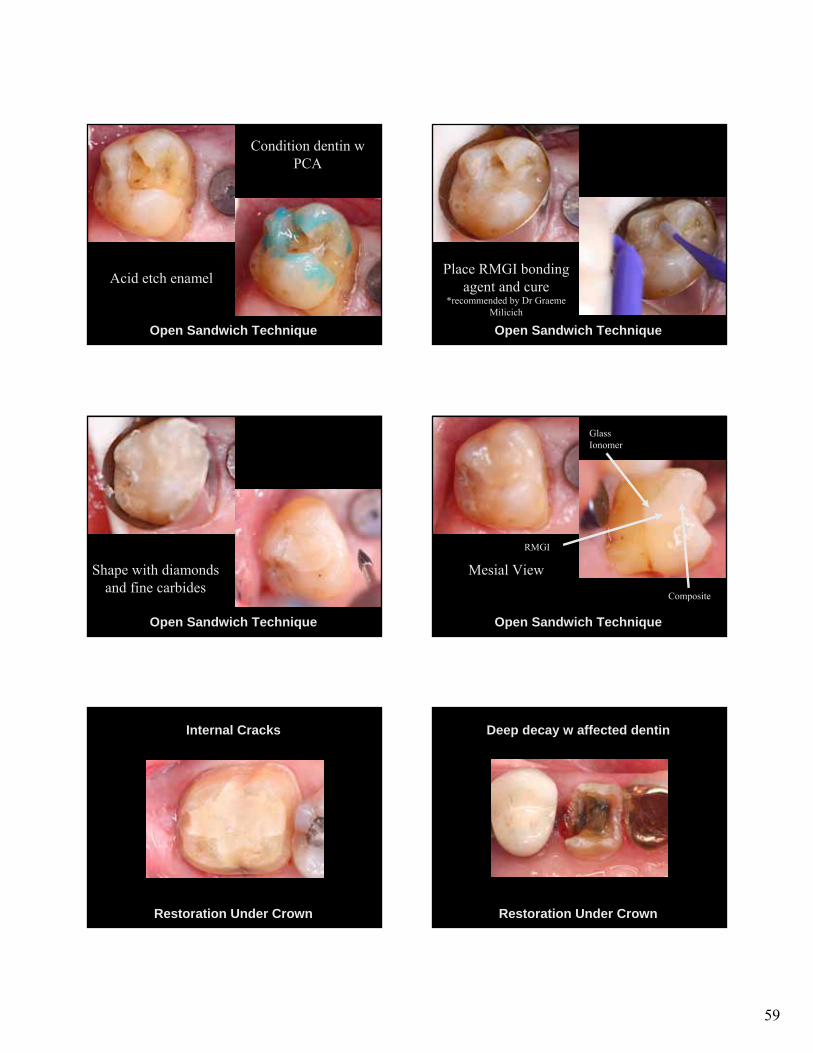
Preparation w cervical margin in
dentin
Open Sandwich Technique
Acid etch enamel
Condition dentin w PCA
Place glass ionomer base
Open Sandwich Technique
Place RMGI bonding agent and cure
*recommended by Dr Graeme Milicich
Build up tooth with composite
Open Sandwich Technique
Shape with diamonds and fine carbides
Finished occlusal view
Open Sandwich Technique
Mesial View
Glass Ionomer
Composite
RMGI
Restoration Under Crown
Internal Cracks
Restoration Under Crown
Deep decay w affected dentin

60
Restoration Under Crown
Deep decay w affected dentin
Restoration Under Crown
Deep decay w affected dentin
Restoration Under Crown
Deep decay w affected dentin
Restoration Under Crown
Do Not Use in Anterior Teeth to replace Large Defects
RUC with crack Long term interim restoration

61
But… How long do they last?
Zanata RL, Fagundes TC, Freitas MC, Lauris JR, Navarro MF. Ten-year survival of ART restorations in permanent posterior teeth. Clin Oral Investig. 2011;15(2):265-71
Placement 2 years 10 years
92.7% success
65.2% success
Survival Rate
Single Surface Restorations*(*based on placement of older GI formulations)
But… How long do they last?
Zanata RL, Fagundes TC, Freitas MC, Lauris JR, Navarro MF. Ten-year survival of ART restorations in permanent posterior teeth. Clin Oral Investig. 2011;15(2):265-71
Placement 2 years 10 years
86.8% success
30.6% success
Survival Rate
Multiple Surface Restorations*
(n=62)
(*based on placement of older GI formulations)
But… How long do they last?
Five Year Restorations
Long term interim restoration
How long do they last?• 8-12 years- single surface
• 5-8 years- multiple surface
• The larger the restoration, the shorter its lifetime
Long term interim restoration
Then what?• Re-prepare surface and place posterior
composite restoration
• Prepare tooth for a crown
Equia
Glass Ionomer/Filled Resin Sealant
62
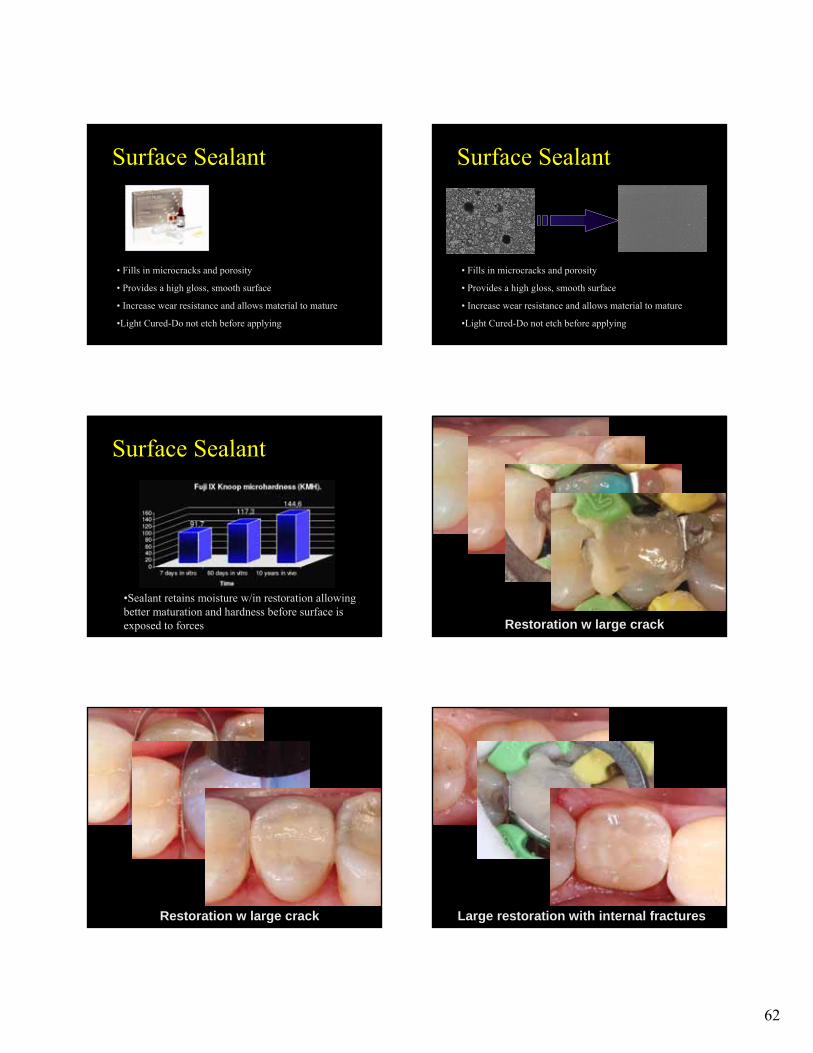
Surface Sealant
• Fills in microcracks and porosity
• Provides a high gloss, smooth surface
• Increase wear resistance and allows material to mature
•Light Cured-Do not etch before applying
Surface Sealant
• Fills in microcracks and porosity
• Provides a high gloss, smooth surface
• Increase wear resistance and allows material to mature
•Light Cured-Do not etch before applying
•Sealant retains moisture w/in restoration allowing better maturation and hardness before surface is exposed to forces
Surface Sealant
Restoration w large crack
Restoration w large crack Large restoration with internal fractures
63
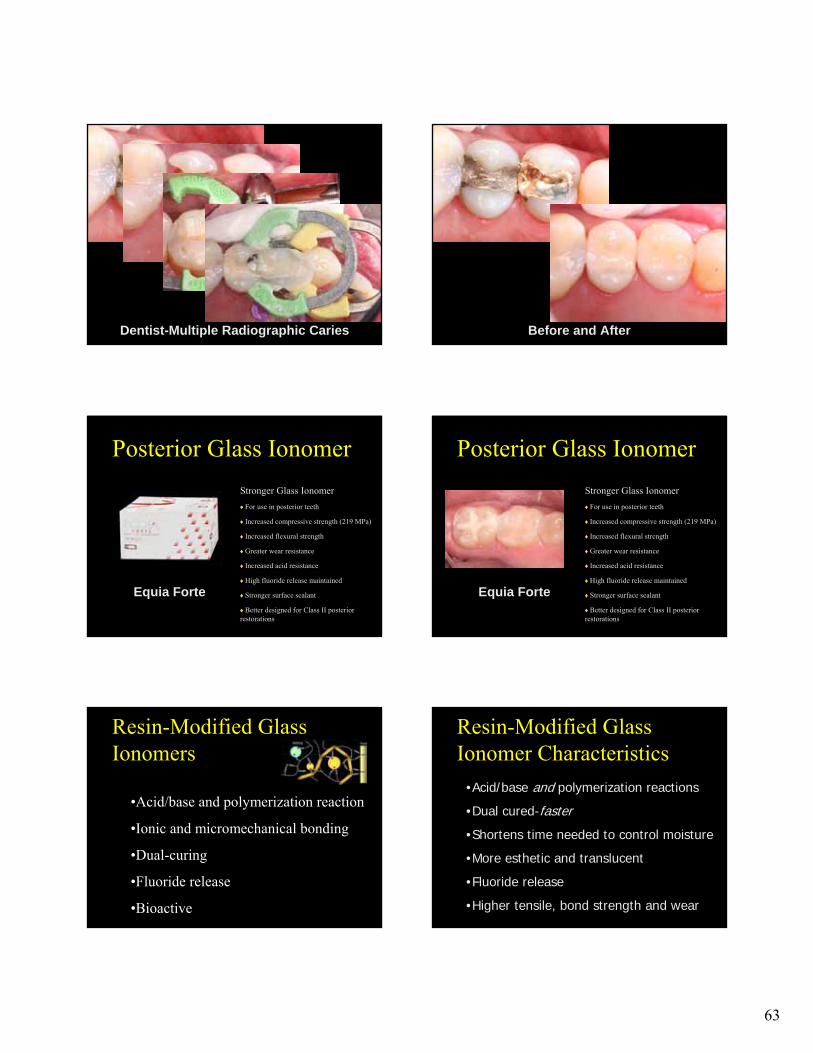
Dentist-Multiple Radiographic Caries Before and After
Equia Forte
Posterior Glass Ionomer
Stronger Glass Ionomer
For use in posterior teeth
Increased compressive strength (219 MPa)
Increased flexural strength
Greater wear resistance
Increased acid resistance
High fluoride release maintained
Stronger surface sealant
Better designed for Class II posterior restorations
Equia Forte
Posterior Glass Ionomer
Stronger Glass Ionomer
For use in posterior teeth
Increased compressive strength (219 MPa)
Increased flexural strength
Greater wear resistance
Increased acid resistance
High fluoride release maintained
Stronger surface sealant
Better designed for Class II posterior restorations
•Acid/base and polymerization reaction
•Ionic and micromechanical bonding
•Dual-curing
•Fluoride release
•Bioactive
Resin-Modified Glass Ionomers
•Acid/base and polymerization reactions
•Dual cured-faster
•Shortens time needed to control moisture
•More esthetic and translucent
•Fluoride release
•Higher tensile, bond strength and wear
Resin-Modified Glass Ionomer Characteristics

64
•Liner or Base
•Class V Restorations
•Restoration Under Crown
•Temporary prior to crown
•Sandwich technique
•Cements
Resin-Modified Glass Ionomer Uses
Resin-Modified Glass Ionomers-Advantages
Brackett WW, Dib A, Brackett MG, Reyes AA, Estrada BE. Two-year clinical performance of Class V resin-modified glass-lonomer and resin composite restorations. Oper Dent. 2003;28:477-81
37 pairs of caries-free unprepared abfraction lesions were treated with resin modified and resin composite restorations (single bottle total etch dba). Retention of the composite restorations at six months was below the minimum specified in the ADA Acceptance Program for Dentin and Enamel Adhesives. At two years retention was 96% for the resin-modified glass ionomer and 81% for the resin composite. The resin composite restorations generally had a better appearance, with a 100% alpha rating in color match, versus 85% for the resin-modified glass ionomer.
•Better retention
Resin-Modified Glass Ionomer Base/Restorative
Capsule
Fuji II LC RIVA LCFuji Filling LC
Resin-Modified Glass Ionomer Base/Restorative
Ketac Nano
Paste-Paste
383
Gingival recession & root caries
• 1st molar and bicuspids
Resin-Modified Glass Ionomer
384
Gingival recession & root caries
• 1st molar and bicuspids
Condition with PAA
• Decay removed
• Pre‐treated with dentin conditioner
(Poly‐acrylic acid)
Resin-Modified Glass Ionomer

65
385
Material Placed and Light Cured
• Place excess material
• Light Cure
Resin-Modified Glass Ionomer
386
Final Restorations
• Shape restorations
• Hold back gingiva and shape with fine
diamond
• Etch with phosphoric acid, wash and dry
• Place surface sealant and light cure
Material Placed and Light Cured
• Place excess material
• Light Cure
Resin-Modified Glass Ionomer
Restoration Under Crown Quick Temporary prior to Crown
Temporary placed 5 years ago Sandwich Technique

66
Telio – Temporary Concept, Team IV Spain, Madrid, November 2009
Resin-modified Bonding Agent–Triturated
–Reduces polymerization shrinkage
stress
–Novel concept
Riva Bond LC
•Exposed to occlusion
•Able to control moisture
•Not acid etching
•No shrinkage stress
•Highest fluoride release
•Out of occlusion
•Need quickness
•Need to acid etch
•Need to bond
•↑translucence/esthetic
Resin-Modified Glass Ionomer
Glass Ionomer
•Core-Cemented posterior crowns
•Entire Class I or II (Long Term Interim)
•Class V-high caries
•All deciduous posteriors
•Sandwich technique-Co Cure
Glass Ionomer Preferred Uses
•Core-all crowns
•Base Class I or II-re-prepared sandwich
•Class V-more esthetic
•Quickly placed short-term interim restorations
Resin-Modified Glass Ionomer
Preferred Uses
Calcium Aluminate/RMGI cement–Hybrid cement
Ceramir
GI Initial setting and early strength Fluoride release
Calcium Aluminate Long term-increased strength and retentionApatite formation Sealing at marginal interface Sustained long term properties w/o degradingHigher pH (not acidic)-virtually no sensitivity
Ceramir

67
Calcium Aluminate/RMGI cement–Hybrid cement
–Forms Apatite crystals
Ceramir
Telio – Temporary Concept, Team IV Spain, Madrid, November 2009
Ceramir
Forms apatite crystals(a group of phosphate minerals, usually referring to hydroxyapatite, fluorapatite and chlorapatite, named for high concentrations of OH−, F−, Cl− or ions, respectively, in the crystal. The formula of the admixture of the four most common end members is written as Ca10(PO4)6(OH,F,Cl)2, and the crystal unit cell formulae of the individual minerals are written as Ca10(PO4)6(OH)2, Ca10(PO4)6(F)2 and Ca10(PO4)6(Cl)2.)
Telio – Temporary Concept, Team IV Spain, Madrid, November 2009
Ceramir
Forms apatite crystals Powder and water are mixed Dissolution results in nano-crystal formation Gibbsite and Katoite forms
Gibbsite
Tooth apatite
Mixed zoneChemically formed apatiteGibbsite(Calcite)
Katoite
Telio – Temporary Concept, Team IV Spain, Madrid, November 2009
Ceramir
Forms apatite crystals Powder and water are mixed Dissolution results in nano-crystal formation Gibbsite and Katoite forms Crystals form on tooth and restoration Long-term stable bond Ceramir Dentin
Telio – Temporary Concept, Team IV Spain, Madrid, November 2009
Calcium Aluminate/RMGI cement–Hybrid cement
–Forms Apatite crystals
–Excellent physical properties
Ceramir Physical Properties
– Creates Apatite when in contact with phosphates– No shrinkage– Hydrophilic system with Alkaline pH– Thermal properties similar to tooth structure– Low film thickness -15 microns– 160 Mpa compressive strength– Anti-bacterial-inhibits caries– Gets stronger over time– Acid resistant– Bonds well to metal, porcelain, ceramics, zirconium
Ceramir

68
Telio – Temporary Concept, Team IV Spain, Madrid, November 2009
Calcium Aluminate/RMGI cement–Hybrid cement
–Forms Apatite crystals
–Excellent physical properties
–Low film thickness-easy to use
Ceramir
Telio – Temporary Concept, Team IV Spain, Madrid, November 2009
Ceramir
Jeffries SR, Fuller AE, Boston DE. Preliminary Evidence that Bioactive Cements Occlude Artificial Marginal Gaps. J Esthet Restor Dent. 2015.
Self Adhesive Resin Cement
Resin-Modified Glass Ionomer
Glass Ionomer
Calcium AluminateRMGI
Calcium Silicate
0:00
Ceramir
2:00
Ceramir
4:00
Ceramir
Calcium Aluminate/RMGI cement– Hybrid cement
– Forms apatite crystals
– Excellent physical properties
– Low film thickness-easy to use
– Virtually no sensitivity
Ceramir

69
Glass IonomersThe “missing link” of esthetic
restorative materials
IN TODAY’S ECONOMY
•Golden Rule•Stay current on the latest technologies•Communicate effectively with patients•Offer choices•Be passionate about what you do!
Thank You!





























