Embed Size (px)
Citation preview

5/13/2014
1
Hyponatremia, Hypercalcemiaand HyperparathyroidismDr. Tyler Dunphy
Essentia Health‐Brainerd Clinic
5/16/14
Goals
• Diagnostic workup of hyponatremia‐understanding the role of ADH.
• management of hyponatremia
• Differential diagnosis of hypercalcemia and hyperparathyroidism.
• Management of hypercalcemia and hyperparathyroidism
5/13/2014
2
Hyponatremia:The Water Problem and ADH
• Where does ADH act in the kidney?
Hyponatremia:The Water Problem and ADH
Anti‐diuretic Hormone
Secreted by the hypothalamus
Acts on cortical and medullary collecting ducts of the kidney to increase water permeability
Controlled by osmoreceptors and volume receptors (Bavlis, Am J Physiol. 1987)
The vast majority of hyponatremia is mediated by too much ADH (appropriate or inappropriate).

5/13/2014
3
The Nephron
Nephron at Wikipedia, 5.9.2014
Diagnostic Workup
Break down with serum osmolality (normal 275‐290)
• Low vs. normal/high serum osmolality.
• Sosm= 2x Na + glucose/18 + BUN/2.8

5/13/2014
4
Diagnostic Workup
• Break down with serum osmolality (normal 275‐290)
– Low vs. normal/high serum osmolality.
– Sosm= 2x Na + glucose/18 + BUN/2.8
Can anybody think of a condition where there is a high serum osmolality, but low sodium?
Normal/High Serum Osmolality
• Hyperglycemia (1.6/100 below 400, 4/100 above 400) (Hillier et al. Am J Med. 1999)
• Azotemia
• Alcohol intoxication
• Mannitol infusion
• Irrigant absorption (TURP)
• Pseudohyponatremia (hyperlipidemia, hyperproteinemia)

5/13/2014
5
Low Serum OsmolalityLifeinthefastlane.com 3/2014
Lifeinthefastlane.com 3/2014

5/13/2014
6
Lifeinthefastlane.com 3/2014
Lifeinthefastlane.com 3/2014

5/13/2014
7
Treatment (inpatient vs outpatient)
• Goal of less than 9 meq per 24 hours (Central pontine myelinolysis)
• More rapid correction depending on symptoms, but same 24 hour goal.
• Correct underlying cause
• Sodium deficient
• Vasopressin antagonist
• Fluid restriction
• Volume correction
Hypercalcemia
• Typically >10.5
• Ca = SerumCa + 0.8 * (NormalAlbumin ‐PatientAlbumin) (Payne et al. Br Med J. 1973)

5/13/2014
8
Etiology (bionews‐tx.com, 2013)
Etiology
• C‐calcium intake
• H‐hyperparathyroidism
• I‐ immobility
• M‐milk alkali syndrome
• P‐pagets disease
• A‐addison’s disease
• N‐neoplasm
• Z‐zollinger‐ellison syndrome
• E‐excess vitamin A
• E‐excess vitamin D
• S‐sarcoidosis
5/13/2014
9
Etiology
• 90% of hypercalcemia related to either hyperparathyroidism or malignancy.
• PTH mediated and PTH independent.
PTH mediated
• Primary hyperparathyroidism
• Renal failure and secondary hyperparathyroidism
• Familial hypocalciuric hypercalcemia

5/13/2014
10
PTH mediated
• Primary hyperparathyroidism
• Renal failure and secondary hyperparathyroidism
• Familial hypocalciuric hypercalcemia
PTH mediated
• Primary hyperparathyroidism
• Renal failure and secondary hyperparathyroidism
• Familial hypocalciuric hypercalcemia
What differentiates these two conditions?

5/13/2014
11
Primary Hyperparathyroidism
• Normal to high PTH in the setting of hypercalcemia.
• General symptoms of hypercalcemia, plus nephrolithiasis, ? cardiovascular mortality(Nilsson et al. J
Bone Miner Res. 2002; Wermers et al. Am J Med. 1998), osteoporosis
• Parathyroid hyperplasia vs adenoma.
– Rare tumor secretion.
Primary Hyperparathyroidism‐workup
• Urinary calcium excretion
– Should be normal to high (40%) Vitamin D testing
• Renal imaging to look for nephrolithiasis
• DEXA
• Once diagnosis is established imaging studies such as NM, CT, MRI can be used for localization.
5/13/2014
12
Familial Hypocalciuric Hypercalcemia
• Autosomal dominant inheritance
• Mutation of the calcium‐sensing receptor in the parathyroid glands and kidneys. – Leads to mild (generally asymptomatic) hypercalcemia with a normal or elevated PTH
• Distinguished from hyperparathyroidism by urinary calcium excretion. – Hypocalciuric
– Important to make the distinction.
PTH Independent
• Malignancy—Activation of osteoclasts, PTHrP
• Immobilization
• Pagets disease
• Vitamin A
• Hyperthyroidism
• Milk alkali syndrome
• Elevated Vitamin D
• Lithium
• Thiazides
• Pheochromocytoma
• Adrenal insufficiency
• Rhabdomyolysis
• Theophylline toxicity
• Congenital lactase deficiency
5/13/2014
13
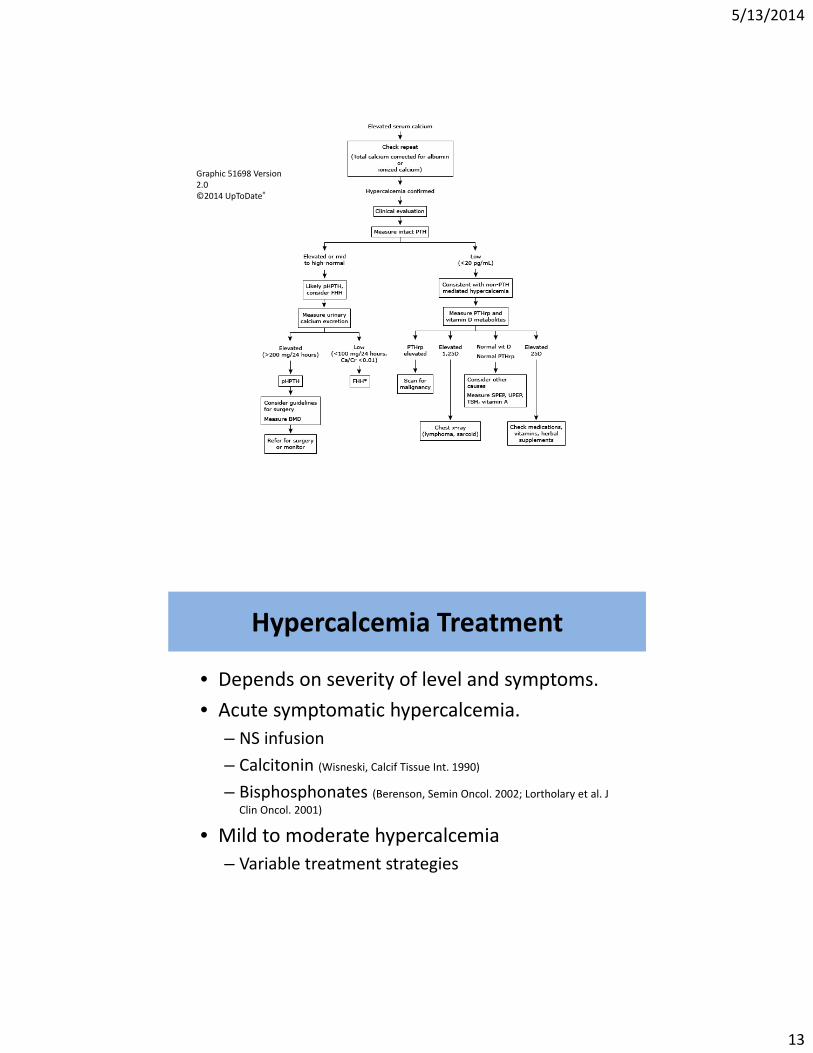
Graphic 51698 Version 2.0©2014 UpToDate®
Hypercalcemia Treatment
• Depends on severity of level and symptoms.
• Acute symptomatic hypercalcemia.
– NS infusion
– Calcitonin (Wisneski, Calcif Tissue Int. 1990)
– Bisphosphonates (Berenson, Semin Oncol. 2002; Lortholary et al. J
Clin Oncol. 2001)
• Mild to moderate hypercalcemia
– Variable treatment strategies

5/13/2014
14
Hyperparathyroidism Treatment
• Surgery for symptomatic disease
– Fracture risk, improvement in nephrolithiasis
• Non‐surgical treatments include
– Monitoring
– bisphosphonates, avoiding triggers of hypercalcemia
– Treat Vitamin D deficiency
– Cinacalcet (mostly used in secondary hyperparathyroidism due to renal failure).
– Estrogen/progestin therapy
Take Home Points
• When you see hyponatremia, think elevated ADH and what is driving elevated ADH.
• Remember revised glucose correction of hyponatremia in the setting of hyperglycemia‐1.6/100 below 400, 4/100 above 400 .
• 90% of hypercalcemia is related to hyperparathyroidism or malignancy.
• Bisphosphonates are the treatment of choice for hypercalcemia secondary to bone breakdown.
• Hypocalciuria differentiates Familial hypocalciurichyercalcemia from primary hyperparathyroidism.

5/13/2014
15
References
• Fuleihan Gel‐H. Familial benign hypocalciuric hypercalcemia. J Bone Miner Res. 2002;17 Suppl2:N51.
• Nilsson IL, Yin L, Lundgren E, Rastad J, Ekbom A. Clinical presentation of primary hyperparathyroidism in Europe‐‐nationwide cohort analysis on mortality from nonmalignant causes. J Bone Miner Res. 2002;17 Suppl 2:N68
• Wermers RA, Khosla S, Atkinson EJ, Grant CS, Hodgson SF, O'Fallon WM, Melton LJ 3rd. Survival after the diagnosis of hyperparathyroidism: a population‐based study. Am J Med. 1998;104(2):115
• Silverberg SJ, Shane E, Jacobs TP, Siris ES, Gartenberg F, Seldin D, Clemens TL, Bilezikian JP. Nephrolithiasis and bone involvement in primary hyperparathyroidism. Am J Med. 1990;89(3):327
• Baylis PH. Osmoregulation and control of vasopressin secretion in healthy humans. Am J Physiol. 1987;253(5 Pt 2):R671
• Hillier TA, Abbott RD, Barrett EJ. Hyponatremia: evaluating the correction factor for hyperglycemia. Am J Med. 1999;106(4):399
• Major P, Lortholary A, Hon J, Abdi E, Mills G, Menssen HD, Yunus F, Bell R, Body J, Quebe‐Fehling E, Seaman J. Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, controlled clinical trials. J Clin Oncol. 2001;19(2):558.
• Berenson JR. Treatment of hypercalcemia of malignancy with bisphosphonates. Semin Oncol. 2002;29(6 Suppl 21):12.
• Wisneski LA. Salmon calcitonin in the acute management of hypercalcemia. Calcif Tissue Int. 1990;46 Suppl:S26