Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Hypoglycemia Begets Hypoglycemia:The Order Effect in the ASPIRE In-Clinic Study
Satish K. Garg, MD,1 Ronald L. Brazg, MD,2 Timothy S. Bailey, MD,3
Bruce A. Buckingham, MD,4 Robert H. Slover, MD,1 David C. Klonoff, MD,5
John Shin, PhD,6 John B. Welsh, MD, PhD,6 and Francine R. Kaufman, MD6
Abstract
Background: The ASPIRE in-clinic study established that automatic suspension of insulin with the thresholdsuspend (TS) feature reduces the duration of induced hypoglycemia. The study’s crossover design allowed theeffects of antecedent hypoglycemia to be studied.Subjects and Methods: The study enrolled 50 subjects who exercised until plasma glucose (YSI glucose andlactate analyzer; YSI, Inc., Yellow Springs, OH) reached £ 85 mg/dL. Hypoglycemia was evaluated after theYSI value reached < 70 mg/dL. In TS experiments, insulin was stopped for 2 h once a sensor glucose (SG) valueof £ 70 mg/dL was detected; in control experiments, basal insulin delivery continued. Subjects were randomlyassigned to Group A (TS in Period 1; control in Period 2) or Group B (control in Period 1; TS in Period 2).Experiments were separated by 3–10 days.Results: Hypoglycemia was 63.7 min shorter in Period 1 TS experiments (no preceding control experiment)than in Period 2 TS experiments (one or more preceding control experiment(s)) (P < 0.01). The number ofexperiments prior to a successful TS experiment was lower for Period 1 than for Period 2 (0.36 – 0.64 vs.1.57 – 0.84; P < 0.001), as was the cumulative duration of antecedent hypoglycemia (16.6 min vs. 204.6 min;P < 0.001). The between-groups difference in hypoglycemia duration was not attributable to differences in SGrates of change, the duration of exercise, or area under the curve of <70 mg/dL · min in the 2 days before thesuccessful experiment (all P > 0.3).Conclusions: The TS feature’s ability to mitigate hypoglycemia was decreased by an episode or episodes ofprolonged antecedent hypoglycemia, suggesting hypoglycemia begets hypoglycemia. The effect of antecedenthypoglycemia should be taken into consideration in the design of future experiments assessing strategies toreduce hypoglycemia.
Introduction
Severe hypoglycemia has been described as the mostformidable barrier to intensive insulin treatment in type 1
diabetes.1 In many instances, this results from a combinationof iatrogenic hyperinsulinemia and the loss or attenuation ofglycogen stores and counterregulatory hormone release inpart due to antecedent hypoglycemia. The resulting cycle ofautonomic compromise, hypoglycemia unawareness, andincreased risk for severe hypoglycemia constitutes hypo-
glycemia-associated autonomic failure (HAAF).2 Becausehypoglycemia is both a cause and a consequence of HAAF,hypoglycemia prevention may have both acute and sustainedbenefits.
In the ASPIRE in-clinic study,3 we examined the glycemicresponse to overnight fasting and exercise in adults with type1 diabetes and compared the effects of continued basal in-sulin delivery with the effects of automatic insulin pumpsuspension triggered at a preset sensor threshold (thresholdsuspend [TS], formerly known as low glucose suspend). As
1University of Colorado Denver, Aurora, Colorado.2Rainier Clinical Research Center, Renton, Washington.3AMCR Institute, Escondido, California.4Stanford University, Stanford, California.5Mills-Peninsula Health Services, San Mateo, California.6Medtronic, Inc., Northridge, California.
DIABETES TECHNOLOGY & THERAPEUTICSVolume 16, Number 3, 2014ª Mary Ann Liebert, Inc.DOI: 10.1089/dia.2013.0219
125

expected, hypoglycemia was attenuated in the experimentsthat included automatic pump suspension (TS experiments)compared with experiments with continued basal insulindelivery (control experiments).4 Specifically, the TS featurewas found to reduce the duration of hypoglycemia(138.5 – 76.68 min vs. 170.7 – 75.91 min in TS vs. controlexperiments, respectively; P = 0.006) and its severity (meannadir glucose, 59.5 – 5.72 vs. 57.6 – 5.69 mg/dL in TS vs.control experiments; P = 0.015).4 In addition, the risk ofsubsequent rebound hyperglycemia after the 2-h pump sus-pension was found to be low.
Because of the ASPIRE in-clinic study’s crossover design,subjects participated in at least two hypoglycemic inductionexperiments that were separated by 3–10 days. The a prioristudy design included evaluating the order effect on durationand severity of hypoglycemia. It was found that the durationof hypoglycemia in initial TS experiments was significantlyshorter than those in second or subsequent TS experiments.The factors contributing to the order effect on hypoglycemiaduration were evaluated and are reported in this manuscript.Preliminary results have been presented at the 72nd ScientificSessions of the American Diabetes Association.5,6
Study Design and Methods
The design and methods of the ASPIRE in-clinic study aredescribed elsewhere.3 A history of hypoglycemic seizure orhypoglycemic coma within the last 2 years was an exclusioncriterion. The protocol required that subjects were to havebeen diagnosed with type 1 diabetes and that they had at least3 months of experience with a Medtronic (Northridge, CA)insulin pump; subjects were required to use Veo� pumps andwear Sof-sensor� glucose sensors throughout the study. Theexperiments to induce hypoglycemia were to involve re-peated exercise sessions until the YSI glucose value (mea-sured with the YSI 2300 STAT Plus� glucose and lactateanalyzer [YSI, Inc., Yellow Springs, OH]) reached £ 85 mg/dL,a rest period until the YSI glucose value reached < 70 mg/dL,and an observation period. In the postexercise observationperiod, the protocol required the level glucose to be measuredvia the YSI analyzer every 5–15 min to calculate duration andnadir between 50 and 70 mg/dL. The pump was to be set tosuspend insulin delivery for 2 h at a sensor glucose (SG) valueof £ 70 mg/dL in TS experiments or to deliver basal insulinregardless of the SG value in control experiments. Subjectswere to be randomly assigned to Group A (TS experiments inPeriod 1, followed by control experiments in Period 2) orGroup B (control experiments in Period 1, followed by TSexperiments in Period 2).
The protocol required the duration and severity of hypo-glycemia to be quantified in frequently drawn plasma sam-ples with the YSI 2300 STAT Plus analyzer. Hypoglycemiaduration was defined as the length of time that YSI valueswere < 70 and > 50 mg/dL; hypoglycemia severity was de-fined as the lowest observed YSI value. Experiments wereabandoned in the interest of patient safety if the YSI value fellbelow 50 mg/dL or exceeded 300 mg/dL; data from suchexperiments were not analyzed. The primary end point was acomparison of the duration and severity of hypoglycemiameasured with the YSI analyzer during successful TS andcontrol experiments. The effect of the order of TS and controlexperiments was deemed significant for P £ 0.1. If this order
effect criterion was met, pre- and post-crossover sessionswere to be analyzed separately. The two-sample t test wasused to compare attributes of successful experiments betweenperiods. Efficacy of the TS feature was defined as a reductionin either duration or severity of hypoglycemia at the 0.0154level of significance.
Results
The glycated hemoglobin (A1C) level (mean – SD) of all50 subjects was 7.9 – 0.6%. Comparison of the 48 successfulTS Period 1 experiments (which, by design, were not pre-ceded by any control experiments but might have been pre-ceded by an experiment that had been terminated earlybecause of a YSI value of < 50 mg/dL or patient issues) withthe 50 successful TS Period 2 experiments (which werepreceded by one or more control experiments) showed thatthe duration of hypoglycemia was 63.7 min shorter in Period1 than in Period 2 (107.8 – 71.2 min in Period 1 versus171.5 – 67.0 min in Period 2; P < 0.01).
Additional analysis was performed to assess the order ef-fect. Table 1 shows the cumulative duration of antecedenthypoglycemia was also significantly less prior to Period 1 TSexperiments than prior to Period 2 TS experiments (16.6 minvs. 204.6 min; P < 0.001). In addition, there were signifi-cantly fewer induction experiments prior to the Period 1 ex-periments than prior to the Period 2 experiments (0.36 – 0.64vs. 1.57 – 0.84; P < 0.001). However, the order effect did notappear to be attributable to differences in YSI rates of change,the duration of exercise, or area under the curve (AUC) of< 70 mg/dL · min in the 2 days before the successful experi-ment (all P > 0.9). Table 2 shows the disposition of all at-tempted and failed experiments.
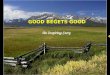
Figure 1 shows the order effect by plotting mean YSIvalues at various times after hypoglycemia was achieved. InTS Period 1 experiments, YSI values returned to the normalrange faster than in TS Period 2 experiments. YSI values inTS Period 1 experiments were consistently higher than YSIvalues from TS Period 2 experiments. The mean glucosevalues in control experiments remained in the hypoglycemicrange for the entire 4-h observation period and were similar inPeriods 1 and 2.
Figure 2 shows the percentage of subjects with YSI valuesin the hypoglycemic range (50–70 mg/dL) at various timesafter the start of hypoglycemia in Period 1 and Period 2 ex-periments. There was an early (within 60 min) decrease in thepercentage of subjects who remained hypoglycemic in TSPeriod 1 experiments; this low percentage of hypoglycemicsubjects was maintained throughout the observation period(Fig. 2A). This is in contrast to TS Period 2 experiments,where most patients experienced > 120 min of hypoglycemiaand approximately 50% of patients were hypoglycemic at theend of the observation period (Fig. 2B). In control experi-ments in both Period 1 and Period 2, most subjects’ YSIvalues were in the hypoglycemic range for the entire obser-vation period. No serious adverse events occurred, as re-ported previously.4
Discussion
Several studies of the TS feature have now been reported.These have shown a reduction in the duration of hypogly-cemia in children7 and in the overnight hours among those at
126 GARG ET AL.

greatest risk.8 Analysis of pump suspensions lasting for 2 h(the maximum allowed by the Veo pump) showed that theydo not result in severe hypoglycemia,9,10 and regular use ofthe TS feature was associated with reductions in the numberand severity of severe hyperglycemic episodes.10 In a ran-domized controlled trial, use of the TS feature over a 3-monthperiod in the home setting was shown to significantly reducethe mean AUC of nocturnal hypoglycemic events, as well asthe weekly rate of those events, without significantlychanging A1C levels.11
The ASPIRE in-clinic study’s crossover design allowedcomparison of subjects’ recovery from hypoglycemia under
various conditions and showed that recent hypoglycemia isdetrimental to recovery from subsequent hypoglycemia. Theeffect was only apparent in experiments that stopped insulindelivery (i.e., the TS experiments), where spontaneous re-covery from exercise-induced hypoglycemia was possible. InTS Period 1 experiments, with no recent exposure to severeand prolonged hypoglycemia, this recovery was significantlyfaster than the recovery in TS Period 2 experiments, wheresubjects had been exposed to recent episode(s) of severe andprolonged hypoglycemia. This suggests that one or moremechanisms for glucose homeostasis remained impairedwhen Period 2 TS experiments were initiated.
Table 1. Attributes of Successful Experiments
Experiment type, period
TS Control
1 2 P value 1 2 P value
Preceding cumulative inducedhypoglycemia (min)a
16.6 – 57.3 204.6 – 123.7 < 0.001 29.3 – 82.6 115.9 – 111.3 0.003
Number of prior experiments(n)b
0.36 – 0.64 1.57 – 0.84 < 0.001 0.32 – 0.63 1.64 – 0.81 < 0.001
Maximal YSI rate of change(mg/dL/min)c
- 1.34 – 0.46 - 1.35 – 0.60 0.935 - 1.02 – 0.48 - 1.09 – 0.36 0.545
Duration of exercise (min)d 101.0 – 58.03 99.7 – 59.66 0.941 80.2 – 53.09 80.4 – 46.10 0.987AUC < 70 (mg/dL · min)
for the prior 2 dayson CGM
1,687.8 – 1,883.3 1,716.5 – 2,919.5 0.968 1,224.2 – 1,827.3 1,500.0 – 2,581.0 0.665
Data are mean – SD values. P values refer to Period 1 versus Period 2 comparisons.aTotal time spent with YSI values between 50 and 70 mg/dL in previous successful and unsuccessful experiments.bNumber of previous successful and unsuccessful experiments.cLargest negative rate of change of YSI glucose readings on the day of the experiment.dTime from the initiation of exercise to the first YSI value £ 85 mg/dL.AUC, area under the curve; CGM, continuous glucose monitoring; TS, threshold suspend.
Table 2. Attempted and Failed Hypoglycemia Induction Experiments
TS Control
Experiments (n) Subjects (n) Experiments (n) Subjects (n)
Attempted induction experiments 69 (35, 34) 50 (25, 25) 65 (33, 32) 50 (25, 25)Failed induction experiments 21 (10, 11) 14 (8, 6) 15 (8, 7) 12 (6, 6)
YSI ‡ 70 mg/dL 9 (5, 4) 8 (5, 3) 5 (3, 2) 5 (3, 2)YSI < 50 mg/dL 9 (3, 6) 5 (2, 3) 8 (3, 5) 7 (3, 4)Others 3 (2, 1) 3 (2, 1) 2 (2, 0) 2 (2, 0)
Sensor dislodged 1 (1, 0) 1 (1, 0) 0 (0, 0) 0 (0, 0)
Site stopped experiment earlybecause there was early activationof the TS feature in two instancesbefore YSI reached £ 70 mg/dL
1 (1, 0) 1 (1, 0) 0 (0, 0) 0 (0, 0)
Early cessation of observationperiod due to site error
0 (0, 0) 0 (0, 0) 1 (1, 0) 1 (1, 0)
Subject gave himself 1 unit of insulin2 h prior to induction experiment(without investigator being aware)
0 (0, 0) 0 (0, 0) 1 (1, 0) 1 (1, 0)
TS feature was errantly left off by site 1 (1, 0) 1 (1, 0) 0 (0, 0) 0 (0, 0)
Successful induction experiments 48 (25, 23) 48 (25, 23) 50 (25, 25) 50 (25, 25)
Values represent the total for Period 1 and Period 2 experiments, followed in parentheses by the number of experiments or subjects ineach individual period.
TS, threshold suspend.
ANTECEDENT HYPOGLYCEMIA IN THE ASPIRE STUDY 127

In TS Period 1 experiments, subjects’ recovery from hy-poglycemia at 60 and 180 min might represent the decay ofinsulin from the subcutaneous depot (at rates that are depen-dent on individual factors), combined with rapid increases inglycogenolysis and later increases in gluconeogenesis. In TSPeriod 2 experiments, the relatively protracted hypoglycemiamay be due to more glycogen depletion from the prior hy-poglycemic episode(s), which we would expect to have beenfurther depleted in the recovery phase. Impaired autonomicresponses to prolonged hypoglycemia may also have played arole in TS Period 2 experiments (not evaluated in this study).
When basal insulin delivery continued throughout the hy-poglycemic episode (i.e., the control experiments), no detri-mental effect of antecedent hypoglycemia was seen. Thisability of continued basal insulin delivery to impair recoveryfrom hypoglycemia may be due to its ability, at physiologicalconcentrations, to suppress gluconeogenesis by approximately20% and to completely block glycogenolysis,12 combined withits activation of glycolysis and glycogenesis.
When basal insulin delivery is suspended during hypo-glycemia, the liver and sympathoadrenal system play criticalroles in the timing and magnitude of recovery, and a detailedmathematical model of hepatic glucose metabolism13 sug-gests a multifaceted etiology for the order effect. Early inhypoglycemia, glycogenolysis predominates; with time,glycogen stores are depleted, and the relative contribution ofgluconeogenesis to overall hepatic glucose production in-creases. In Period 2 TS experiments, the modest decrease inthe percentage of subjects in hypoglycemia at 60 min may beattributable to a relative lack of glycogen, and the recovery ofsubjects after 60 min may be attributable to increased rates of
gluconeogenesis (Fig. 2). The order effect may also be due toother effects of exercise that can significantly modify themetabolic and endocrine responses to subsequent exercise.14
Antecedent hypoglycemia is known to attenuate the sym-pathoadrenal and symptomatic responses to hypoglycemia,15
which may further contribute to the observed order effect.This analysis of the ASPIRE in-clinic study has several
limitations, including that it did not measure or attempt tocontrol for the fitness of the participants, caloric expendi-tures, or counterregulatory hormones. In addition, a widerange of between-experiment intervals (3–10 days) was al-lowed, and the time between experiments was not adjustedfor the duration or extent of prior hypoglycemic exposure.The 50 mg/dL glucose threshold at which experiments werehalted helped to ensure patient safety but limited the study’sability to resolve potential differences in hypoglycemia se-verity; the observed difference in nadir glucose values ofapproximately 2 mg/dL is likely not clinically significant.The rate of failed experiments (36 out of 134 attempts) atteststo the difficulty of achieving and maintaining hypoglycemiain subjects in the absence of carbohydrate administration oralterations in preprogrammed insulin delivery. The mean andmedian sensor bias values in the 40–70 mg/dL range were6.3 – 13.3 mg/dL and 7.7 mg/dL, respectively. Although thispositive bias may have triggered the pump to suspend atreference glucose values higher than 70 mg/dL and sensorheterogeneity may have contributed to differences in theseverity and/or duration of induced hypoglycemia episodes,no attempt was made to relate the performance characteris-tics of individual sensors to the outcomes of individualexperiments.
FIG. 1. Mean ( – SEM) YSI glucose values during hypoglycemia induction experiments: solid lines, Period 1; dashedlines, Period 2; triangles, threshold suspend (TS); and circles, control. Time 0 represents the time when the YSI glucosevalue fell below 70 mg/dL.
128 GARG ET AL.

Scrupulous avoidance of hypoglycemia is critical tobreaking the cycle of HAAF.2 The value of the automaticpump stoppage feature therefore includes not just acutemitigation of hypoglycemia, but also preservation of thenormal autonomic response to existing or impending hypo-glycemia. Complete reversal of HAAF is difficult to predictor establish, but sustained euglycemia is now a reasonablegoal for many people with type 1 diabetes. We anticipate thatimprovements in closed-loop insulin delivery systems willhelp more people reach this goal.
Conclusions
Prolonged hypoglycemia was induced by overnight fast-ing, exercise, and continued basal insulin delivery in theASPIRE in-clinic study, regardless of prior exposure to hy-poglycemia. Automatic insulin pump suspension triggered
by low sensor glucose concentrations significantly reducedthe duration and severity of hypoglycemia. Because thiseffect was attenuated in subjects with recent hypoglycemia,we conclude that recent hypoglycemia is a risk factor forprolonged hypoglycemic episodes—that ‘‘hypoglycemiabegets hypoglycemia.’’16 This effect was not due to theduration of exercise, the rate of change of glucose concen-tration, or spontaneous exposure to hypoglycemia during thepreceding 2 days. By mitigating the duration of hypoglyce-mic episodes, automatic pump suspension may help to pre-serve the normal autonomic response to hypoglycemia inpatients with type 1 diabetes.
In future experiments or clinical trials of hypoglycemia,our observations suggest that the crossover design should beused with caution, if at all, and that avoidance of hypogly-cemia for more than 10 days may be necessary to allow fornear-normal responses to hypoglycemia.
A
B
FIG. 2. Percentage of subjects in hypoglycemia (YSI glucose value of 50–70 mg/dL) at various times after the start of ahypoglycemia episode in (A) Period 1 and (B) Period 2 experiments: solid columns, threshold suspend (TS); and opencolumns, control.
ANTECEDENT HYPOGLYCEMIA IN THE ASPIRE STUDY 129

Acknowledgments
The authors thank Scott W. Lee, MD, an employee ofMedtronic, Inc., for comments on an earlier draft of thismanuscript, and the subjects who participated in the study.This research was funded by Medtronic, Inc.
Author Disclosure Statement
J.S., J.B.W., and F.R.K. are employees of Medtronic, Inc.S.K.G., R.L.B., T.S.B., B.A.B., R.H.S., and D.C.K. havereceived research support from Medtronic, Inc. D.C.K. is aconsultant to Google, Insuline, Voluntis, and Sanofi. No otherpotential conflicts of interest relative to this article werereported.
References
1. Cryer PE: Death during intensive glycemic therapy of di-abetes: mechanisms and implications. Am J Med 2011;124:993–996.
2. Cryer PE: Mechanisms of hypoglycemia-associated auto-nomic failure and its component syndromes in diabetes.Diabetes 2005;54:3592–3601.
3. Brazg RL, Bailey TS, Garg S, Buckingham BA, Slover RH,Klonoff DC, Nguyen X, Shin J, Welsh JB, Lee SW: TheASPIRE study: design and methods of an in-clinic cross-over trial on the efficacy of automatic insulin pump sus-pension in exercise-induced hypoglycemia. J Diabetes SciTechnol 2011;5:1466–1471.
4. Garg S, Brazg RL, Bailey TS, Buckingham BA, Slover RH,Klonoff DC, Shin J, Welsh JB, Kaufman FR: Reduction induration of hypoglycemia by automatic suspension of in-sulin delivery: the in-clinic ASPIRE study. DiabetesTechnol Ther 2012;14:205–209.
5. Garg S, Brazg RL, Bailey TS, Buckingham BA, KlonoffDC, Shin J, Welsh JB, Kaufman FR: The order effect of thein-clinic ASPIRE study: hypoglycemia begets hypoglyce-mia [abstract]. Diabetes 2012;61:A58–A59.
6. Garg S, Brazg RL, Bailey TS, Buckingham BA, KlonoffDC, Shin J, Welsh JB, Kaufman FR: Automatic insulinpump suspension for induced hypoglycemia: the ASPIREstudy [abstract]. Diabetes 2012;61:A59.
7. Danne T, Kordonouri O, Holder M, Haberland H, Golem-bowski S, Remus K, Blasig S, Wadien T, Zierow S, Hart-mann R, Thomas A: Prevention of hypoglycemia by usinglow glucose suspend function in sensor-augmented pumptherapy. Diabetes Technol Ther 2011;13:1129–1134.
8. Choudhary P, Shin J, Wang Y, Evans ML, Hammond PJ,Kerr D, Shaw JA, Pickup JC, Amiel SA: Insulin pumptherapy with automated insulin suspension in response tohypoglycemia: reduction in nocturnal hypoglycemia inthose at greatest risk. Diabetes Care 2011;34:2023–2025.
9. Ly TT, Nicholas JA, Retterath A, Davis EA, Jones TW:Analysis of glucose responses to automated insulin sus-pension with sensor-augmented pump therapy. DiabetesCare 2012;35:1462–1465.
10. Agrawal P, Welsh JB, Kannard B, Askari S, Yang Q,Kaufman FR: Usage and effectiveness of the low glucosesuspend feature of the Medtronic Paradigm Veo insulinpump. J Diabetes Sci Technol 2011;5:1137–1141.
11. Bergenstal RM, Klonoff DC, Garg SK, Bode BW, MeredithM, Slover RH, Ahmann AJ, Welsh JB, Lee SW, KaufmanFR; the ASPIRE In-Home Study Group: Threshold-basedinsulin-pump interruption for reduction of hypoglycemia. NEngl J Med 2013;369:224–232.
12. Gastaldelli A, Toschi E, Pettiti M, Frascerra S, Quinones-Galvan A, Sironi AM, Natali A, Ferrannini E: Effect ofphysiological hyperinsulinemia on gluconeogenesis innondiabetic subjects and in type 2 diabetic patients. Dia-betes 2001;50:1807–1812.
13. Konig M, Bulik S, Holzhutter HG: Quantifying the con-tribution of the liver to glucose homeostasis: a detailedkinetic model of human hepatic glucose metabolism. PLoSComput Biol 2012;8:e1002577.
14. Galassetti P, Mann S, Tate D, Neill RA, Wasserman DH,Davis SN: Effect of morning exercise on counterregulatoryresponses to subsequent, afternoon exercise. J Appl Physiol2001;91:91–99.
15. Arbelaez AM, Powers WJ, Videen TO, Price JL, Cryer PE:Attenuation of counterregulatory responses to recurrenthypoglycemia by active thalamic inhibition: a mechanismfor hypoglycemia-associated autonomic failure. Diabetes2008;57:470–475.
16. Cryer PE: Hypoglycemia begets hypoglycemia in IDDM.Diabetes 1993;42:1691–1693.
Address correspondence to:Satish K. Garg, MD
University of Colorado DenverBarbara Davis Center for Childhood Diabetes
1775 Aurora CourtAurora, CO 80045
E-mail: [email protected]
130 GARG ET AL.








![Hypoglycemia and Diabetes · hypoglycemia, including severe hypoglycemia, occur in people with type 2 diabetes.[25] There is no doubt that hypoglycemia can be fatal.[26] In addition](https://img.dokumen.tips/doc/110x75/5f0518c07e708231d4113f09/hypoglycemia-and-hypoglycemia-including-severe-hypoglycemia-occur-in-people-with.jpg)