Embed Size (px)
Citation preview
HYPERTENSIVEEMERGENCIES
Louis Muller
11 March 2009
Content
• Introduction• Definitions• Prevalence/morbidity/mortality• Etiology & pathophysiology• Diagnosis• Causes• Differential diagnoses• Workup• Management• Treatment• Pharmacology IV Anti-hypertensives• References
Introduction
• Hypertension(HPT) very common Western soc.• 50 mil. US – affected (world - approx. 1 billion people)• Despite awareness + treatment still 30% adults unaware• 40% known with HTN - not on treatment• 60% on treatment BP not controlled to <140/90 mm Hg
• New data – shown incr. lifetime risk of HPT - incr. risk of CVS complications with “normal” BP levels
Classification
• Joint National Committee (JNC – 7) introduced a new classification system for HTN – 2004
• Normal – SBP<120 and DBP<80• Prehypertension – SBP 120-139 or DBP 80-89• Stage I hypertension – SBP 140-159 or DBP 90-
99• Stage II hypertension – SBP >160 or DBP >100• Stage II HPT further divided into:
– Hypertensive urgency– Hypertensive emergency
Other Terminology
• Severely elevated BP (JNC VII)• Defined as BP > 180/120
• “accelerated HPT”– term used to describe individuals with chronic
hypertension with associated group 3 Keith-Wagener-Baker retinopathy
• “malignant HPT”– describe those individuals with group 4 KWB
retinopathy changes + papilledema

Definitions
• HPT emergency(crisis): Is characterized by a severe elevation in BP, complicated by evidence of impending or progressive target/end organ dysfunction
VS
• HPT urgency: is a severe elevation in BP without progressive target organ dysfunction
NB – these definitions do not specify absolute BP levels
Conditions constituting evidence of EOD
• Hypertensive encephalopathy• Intracerebral heamorrhage• Stroke• Head trauma• Ischemic heart disease (most common)
– AMI– Acute LVF with P/oedema– Unstable angina
• Aortic dissection• Eclampsia• Life threatening arterial bleed

Prevalence/ morbidity/ mortality
Prevalence:- With progress in anti-hypertensive Rx – decrease in the lifetime
incidence of HPT emergencies from 7% to 1%- Hypertensive crisis more common among elderly and black patients- Studies – HPT related problems amount for 25% of all pt visits to
medical section of ED. 33% of these - HTN emergencies.
Morbidity/mortality - Dependent on the extent of EOD on presentation and the degree to
which BP is controlled subsequently.- 1year survival rate has increased from 20% to more than 90% with
appropriate treatment.- 10-year survival rate approaches 70% with approp treatment- 1-year and 5-year mortality rate - following untreated HPT
emergency are 70 to 90% and 100% respectively
Etiology• Most common - rapid unexplained rise in BP in pt with chronic essential HPT- most have history of poor treatment/compliance or an abrupt discont
of their meds
• Other causes- Renal parenchymal disease (80% of sec.causes)- Systemic disorders with renal involvement (SLE)- Renovascular disease (Atheroscleroses/fibromuscular dysplasia)- Endocrine ( phaeochromocytoma/cushing syndrome)- Drugs (cocaine/amphetam/clonidine withdrawal/diet pills)- CNS (trauma or spinal cord disorders – Guillain-Barre- Coarctation of the aorta- Preeclampsia/Eclampsia- Postop. HPT

Pathophysiology
• Not well understood• Failure of normal autoregulation + abrupt rise in SVR• Increase in SVR due to release of humoral vasoconstrictors
from the stressed vessel wall.• Endothelium plays a central role in BP homeostasis via
substances as Nitric oxide and prostacyclin • Increased pressure starts a cycle of - endothelial damage - local activation of clotting cascade - fibrinoid necrosis of small vessels - release of more vasoconstrictors• Process leads to progressive increase in resistance and
further endothelial dysfunction
PathophysiologyPathophysiology
• Single organ inv. in approximately 83%• Two organ inv found in 14%• Multiorgan involvement found in 3% of pts
• Most common clinical presentations - cerebral infarction(24%) - pulmonary oedema (22%) - HPT encephalopathy(16%) - Cong. HF (12%)
• Less common presentations – IC hemorrhage, aortic dissection and eclampsia
Case example - HPT Case example - HPT EncephalopathyEncephalopathy
• 52yr male presents to ED• worsening headache and confusion, numbness and weakness
involving right side of body, blurry vision over past 12 hrs• PMx: HPT, bilateral artery stenosis, cocaine abuse,
hyperlipidemia.• Exam:
– BP 213/134– confused, papilledema on fundoscopy– Mild motor weakness (4/5) right arm– Lab studies rased creatinine– ECG – LVH– CT Brain – diffuse bilateral white matter changes – HPT
encephalopathy
Case example – HPT Case example – HPT EncephalopathyEncephalopathy
• Mx– admitted ICU– started on IV Nitroprusside– BP decreased to 190/100 mmHg over first 3hrs
• Outcome:– Neurology symptoms resolved within 5hrs– he was switched to his usual oral regimen on
3rd day in hospital– discharged day 5 – controlled BP

Hypertensive encephalopathy
• Clinical manifestation of cerebral edema and microhemorrhages seen with dysfunction of cerebral autoregulation
• Defined as an acute organic brain syndrome or delirium in the setting of severe hypertension

HTN Encephalopathy
• Symptoms– Severe headache– Nausea and vomiting– Visual disturbances– Confusion– focal or generalized
weakness
• Signs– Disorientation– Focal neurologic
defects– Focal or generalized
seizures– nystagmus

HPT Encephalopathy
• Not adequately treated – cerebral heamorrhage, coma and death.
• BUT with proper treatment – completely reversible
• Clinical diagnoses (exclusion)
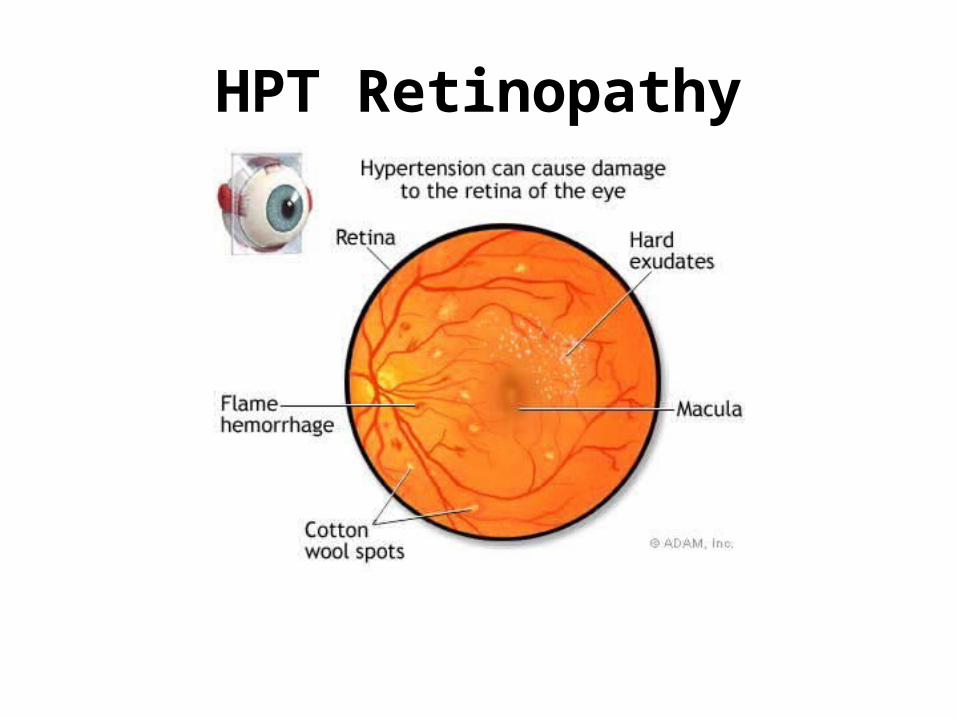
Hypertensive Retinopathy
• Fundoscopy used to be considered a definitive tool in diagnosing HTN encephalopathy
• NOW – still usefull in recognizing acute EOD as in HTN encephalopathy, but the absence of retinal exudates, hemorrhages, or papilledema does not exclude the diagnoses.
• Fundoscopy findings
HPT Retinopathy - Fundoscopy
• Keith-Wagener classification– Stage I arteriolar sclerosis with thickening, irregularity
and tortuosity– Stage II AV dipping or compression– Stage III Flame shaped haemorrhages and cotton
wool spots– Stage IV Papilledema
• “presence of stage III and IV lesions – implies failure of the CNS vascular autoregulation and makes the Dx of Malignant HPT definitive”
HPT Retinopathy
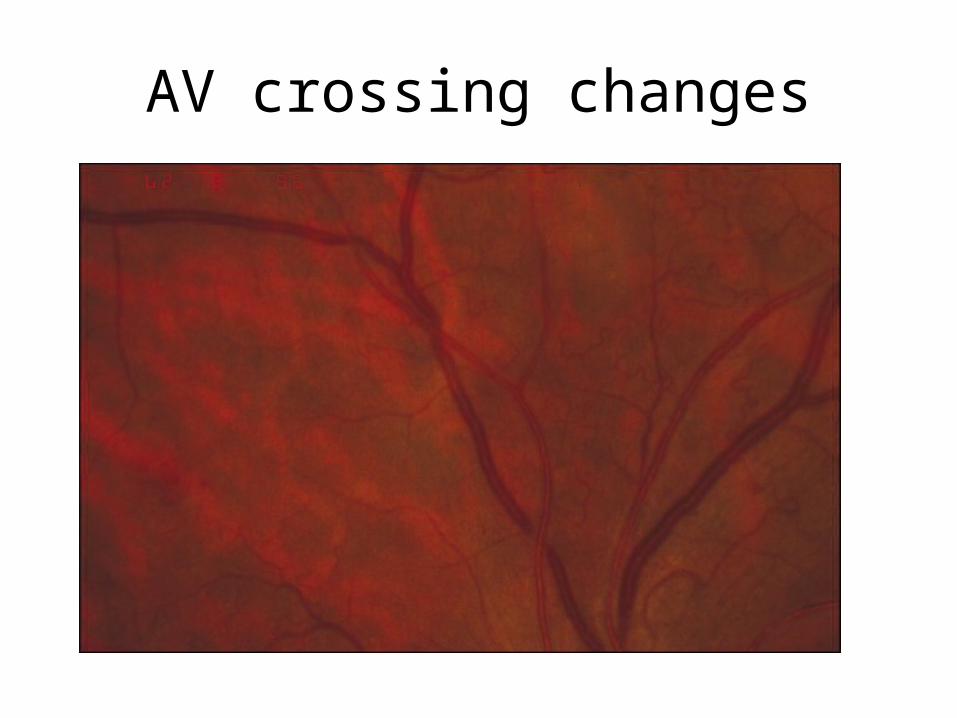
AV crossing changes
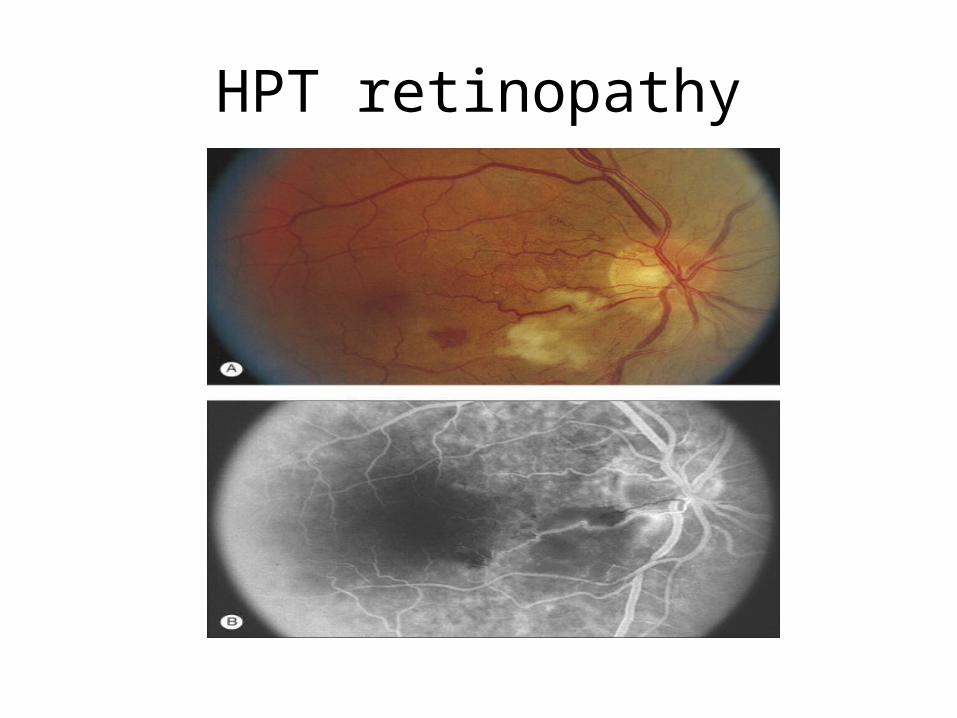
HPT retinopathy

HPT retinopathy

PanOptic ophtalmoscope

Diagnosis• History
1) focus on presence of Sx of end-organ dysfunction(eod) 2) any identifiable etiology
• Hypertension Hx– last known normal BP– prior diagnoses + Rx– dietary and social factors
• Medication– Steroid use– Estrogens– Sympathomimetics– MAO inhibitors
• Social history– smoking, alcohol– illicit drugs (cocaine, stimulants)
• Family history– early HPT in family members– cardiovascular and cerebrovascular disease– Diabetes– Pheochromocytoma
• Pregnant?
Diagnoses• History (cont)• Symptom spesific Hx – suggesting EOD• CVS Hx
– previous MI/angina/arrhythmias – chest pain/SOB/Sx of CF/claudication/flank or back pain
• Neurologic Hx– prior strokes, neuro dysfunction– visual changes, blurriness, loss of visual fields, severe headaches,
nausea and vomiting, change in mental status• Renal Hx
– Underlying renal disease (RF)– Acute onset changes in renal frequency (anuria/oliguria)
• Endocrine Hx– diabetes, thyroid dysfunction, Cushing’s syndrome
DiagnosesExamination1) Confirm elevated BP
» Proper position, appropriate cuff size» Supine and standing and both arms
2) Asses – EOD present• Fundoscopy
• Chronic HPT will have findings• Acute changes
new retinal bleedsSuperficial/flame shapedDeep/punctuate
exudates hard/cotton wool spots papilledema
• NeckEnlarged thryoid, carotid bruit, jugular venous distention
• CVSEnlarged heart, S3, asymmetric pulses, arrhythmias
• PulmonarySigns of LV dysfunction ( crackles, rhonchi)
• RenalRenal bruit, abdominal masses
• NeurologicLevel of consciousness, evidence of stroke, any focal signs

WorkupWorkup• Lab studies- Electrolytes, urea and creatinine- FBC and smear- Urinalysis – dipstix + microscopy- Optional - tox screen - BHCG - Endocrine testing
• Imaging studies- CXR (chest pain or SOB)- Head CT/MRI brain (abn neurology)- Chest CT/TEE/Aortic angio (Aortic dissection)
• Other Tests- ECG
ManagementManagement• ED considerations
- Many HPT pts – only small number will require emergent treatment
- Primary goal of EP?
The pts – syptoms of EOD and require immediate iv parenteral therapy.
VS
The pt with acutely elev BP(SBP>200 or DBP>120) without EOD symptoms, who require initiation of medical therapy and close follow up as outpatient /inpatient
ManagementManagement
• The EP must be capable of:
- Appropriately evaluating pts with an elevated BP- Correctly classify the HPT- Determine the aggressiveness and timing of
therapeutic interventions- Making disposition decisions
Remember - “treat the patient and not the number”

TreatmentTreatment
• Prehospital care
- Address the manifestations of a HPT emergency eg.chest pain or HF
- Reduction of BP not indicated in prehospital setting
- Rapid lowering of BP can critically decrease end-organ perfusion

TreatmentTreatment• ED Care - general principles
1. Consider context of elevated BP (pain, anxiety)2. Screen for EOD (Hx/workup) - Pts without evidence of EOD – d/c + f/up
Misconception - never d/c patient from ED with elevated BP ? - oral nifedipine – NOT indicated and may be dangerous!
- Pts with EOD – require ICU admission and rapid but gradual lowering of BP - using IV meds.
3. BP should not be lowered to normal levels- Rapid reduction in BP – below the autoregulatory range results in reduction in organ
blood flow – risk of ischemia and infarction- General rule – the MAP should be lowered by no more than 20% - 1st hour
remains stable - BP lowered to 160/110 in next 2-6hrs NB Exceptions
- BP goals best achieved by a continuous infusion of a short-acting, titratable, parenteral anti-HPT agent, along with constant intensive patient monitoring
TreatmentTreatment
• Medication options
1. Oral antihypertensives• Chronic hypertensive• Hypertensive urgency
2. IV antihypertensives• Hypertensive emergency
Pharmacology – IV anti-HPTPharmacology – IV anti-HPT
1. Vasodilators• Sodium nitroprusside• Nitroglycerin• Nicardipine• Fenoldapam• Hydralazine• Enalapril
2. Adrenergic inhibitors• Labetalol• Esmolol• Phentolamine

“IDEAL IV ANTI-HYPERTENSIVE”
• Lower the BP without compromising blood flow to critical organs
• Vasodilators generally considered 1st , because they preserve organ blood flow in the face of reduced perfusion and also tend to increase CO.
Profile of an ideal IV Profile of an ideal IV antihypertensiveantihypertensive
• Preserves GFR and renal blood flow• Few or no drug reactions• Little or no potential for exacerbation of co-morbid conditions• Rapid onset and offset of action• Minimal hypotension “overshoot”• Minimal need for continuous BP monitoring and frequent
dose titration• No acute tolerance• Ease of use and convenience• Safe and no toxic metabolites• Multiple formulations for short and long term use• Minimal symphathetic activation

Sodium NitroprussideSodium Nitroprusside(Hypoten L)
• MoA:
– Direct smooth muscle dilator (art + ven)– Nitric oxide compound– Potent preload and afterload reducer– Causes cerebral vasodilation
• Ultra short acting• Immediate onset - DoA : 10min• Dose: 0.1-0.5mcg/kg/min IV infusion titrate to desired effect rates>10mcg/kg/min – cyanide toxicity
• Adverse affects/Precautions:
– Cyanide and thiocyanate toxicity (pts with liver/renal dysfunction) Max dose, max 10min– Can cause precipitous drop in BP (hypotensive effects unpredictable) Ideally Art.line with continuous BP monitoring– Causes significant reflex tachycardia ( incr Oxygen demand) (angina/aortic dissection/cerebral oedema)– Nausea and vomiting– Increased ICP
• Drug of choice:
– Perioperative HPT– Cocaine toxicity– Aortic dissection(combination)– Neurologic syndromes
NitroglycerinNitroglycerin(Nitrocine / Isoket / Tridal)
• MoA:– Potent vasodilator (nitric oxide compound)– Primary affects the venous system, decrease preload (CO + BP)– Decreases coronary vasospasm
• Dose: cont infusion start 5mcg/min, incr by 5mcg/min every 3-5min to 20mcg/min If NO Response increase by 10mcg/min every 3-5min,up 200mcg/min• Onset : 2-5min/DoA : 5-10min
• Adverse effects/precautions:– Constant monitoring is essential– Tolerance from uninterrupted use (12hr withdrawal)– Headache, tachycardia, flushing
• Contra ind: – Concurrent use with PDE-5 inhibitors - causes significant hypotension– Head trauma/cerebral haemorrhage– Severe anaemia
• Drug of choice:– Acute HF– ACS
NicardipineNicardipine(Nimodipine – Nimotop)
• Ca channel blocker – selective arterial vasodilator• Onset: 1-5min• DoA: 15-30min• Dose: start 5mg/hr IV infusion, titrate every 15min to max 15mg/hr.• Advantages:
– Cause cerebral and coronary vasodilatation• Precautions: can worsen/cause HF and liver failure can exacerbate renal insuff.• Ideal for CNS emergencies• Not available SA
FenoldapamFenoldapam(Carlopam)(Carlopam)
• New (not available SA)• MoA:
– Peripheral dopamine agonist (high vs low doses)– causes selective neuro vasodilatation– mesenteric vasodilatation– increases renal blood flow and sodium excretion
• Onset – <5min, but more gentle, lasts for 30min (titratable, predictable and stable)• Standard BP monitoring is sufficient, no toxic metabolites• Dosing:
• Start at 0.1-0.3mcg/kg/min IV infusion• May be increased in increments of 0.05-0.1mcg/kg/min every 15min, until target BP reached• Max infusion rate – 1.6mcg/kg/min
• Precautions:– Pts with glaucoma or intraocular hypertension– Dose related tachycardia can occur – angina– Close BP monitoring – Close K monitoring– Caution with raised ICP
• Drug of choice– Renal insuffiency – Strokes ( combination with nicardipine)
HydralazineHydralazine(Apresoline)
• MoA:– Decreases systemic resistance by direct vasodilation of arterioles
• Dose:– 5-20mg IV bolus or 10-40mg IM repeat every 4-6hrs
• “old school”– used too much– boluses takes 20min to work– not titratable
• Adverse effects/Precautions– tachycardia, flushing, headache– sodium and water retention– increased ICP– adjust dose in severe renal dysfunction– response may be delayed and unpredictable
• Still drug of choice in pregnancy(Eclampsia), but B-blocker/Labetalol and Fenoldapam are also safe options
• Only available PO, Dihydralazine discontinued
EnalaprilatEnalaprilat• The active component of Enalapril (hydrolyzed in liver and kidney)
• MoA:– ACE inhibitor
• Dose:– 0.625-2.5mg every 6hr IV– Not titratable
• Onset – within 30 min + long half life
• Adverse effects/Precautions– Contra-indicated – volume depletion, renal vascular disease– Prolonged ½ life
• Expensive, not available SA
LabetalolLabetalol(Trandate)
• MoA:– selective alpha blocker – will reduce vascular smooth m. resistance – non-selective Beta blocker – decrease cardiac inotropy and miocard O2 consumption, will prevent reflex
tachycardia
• Dose:– Bolus: effect in 5-10min,max effect at 20min. (DoA: 2-6hrs) 1st dose 20mg then every 10-20min 2nd dose 40mg, 3rd dose 80mg.– Cont. infusion: 0.5 – 2mg/min – titrate to response,max 300mg total dose– Difficult to titrate due to very wide dose range
• Advantages:– smooth onset– Transition to oral Rx easy (dose equivalent)– Improve cerebral bloodflow – stroke pt– No need for ICU/Arterial line
• Adverse effects/precautions– Relative CI – Heart failure, heart block, Asthma (bronchoconstriction)– Vomiting, scalp tingling– Impaired hepatic function– Elderly patients
• Contraindicated in HPT secondary to Cocaine use/Phaeochromocytoma (B-blocker effect outway the alpha effect, thus unapposed alpha constriction)
• Drug of choice:– Aortic dissection– Hypertensive emergencies
EsmololEsmolol(Brevibloc)
• MoA:– highly selective beta blocker
• Dose: (titratable)– bolus: 250-500mcg/kg IV over 1-3min– infusion: 50-100mcg/kg/min– may repeat bolus after 5min or increase infusion rate to 300mcg/kg/min
• Onset 1-2min / short acting• Adverse effect/Precautions
– Hypotension common– nausea– Asthma– 1st degree AV block– heart failure
• Contraindications– Sinus bradycardia– Heart block– Cardiogenic shock– Bronchial asthma– Uncompensated CF– pregnancy
• Drug of choice:– Aortic dissection ( with nitrate)
• Not availalble anymore
PhentolaminePhentolamine((Regitine)
• MoA:– alpha adrenergic receptor blocker
• Dose:– load 5-20mg IV every 5min or– infusion 0.2-0.5mg/min
• Onset 1-2min• Adverse effect/precautions
– tachycardia– flushing/headache– MI– cerebrovascular spasm
• Contra-indications– renal impairment– Concurrent use with PDE-5 inhibitors– coronary or cerebral arteriosclerosis
• Drug of choice– Cocaine associated HPT crisis– Pheochromocytoma HPT crisis
• Not available in SA anymore
Neurological emergenciesNeurological emergencies
• Hypertensive encephalopathy– reduce MAP by 25% or diastole to 100mmHg
over 8 hrs– If neurology worsens, suspend Rx– Drug of choice:
• Sodium nitroprusside• Labetalol

Neurological emergenciesNeurological emergencies
• Acute Ischemic stroke– often loss of cerebral autoregulation
– ischemic region more prone to hypoperfusion
– thus BP reduction not recommended
– unless SBP>220 or DBP>120
– UNLESS planning fibrinolysis – SBP<185
and DBP< 110
– Drug of choice:• Labetalol• Nicardipine• Sodium Nitroprusside

Neurological emergenciesNeurological emergencies
• Acutes ICH/SAH– Treatment based on clinical/radiographic
evidence of raised ICP– Raised ICP – MAP<130 (1st 24hrs)– No raised ICP – MAP<110– Drug of choice:
• Sodium Nitroprusside• Labetalol• Nicardipine

Cardiovascular emergenciesCardiovascular emergencies
• ACS– treat if SBP>160 and/or DBP>100– Reduce MAP by 20 -30% of baseline– nitrates should be given till symptoms
subside or until DBP<100– Drug of choice:
• Nitroglycerine• Labetalol• Nicardipine
CVS emergenciesCVS emergencies
• Acute HF (pulmonary edema)– treat with vasodilator (additional to diuretics)– Sodium Nitroprusside in conjunction with
morphine, oxygen and loop diuretic– Enalaprilat also an option

CVS emergenciesCVS emergencies
• Aortic dissection– anti-hypertensive Rx is aimed at reducing the
shear stress on aortic wall (BP and Pulse)– immediate lowering of BP – lifesaving– maintain SBP<110, unless signs of end
organ hypoperfusion– preferred Rx is combination of Morphine,
B-blocker and vasodilator– Nitroprusside + Labetalol
Other disordersOther disorders
• Cocaine toxicity/pheochromocytoma– Hpt and tachycardia rarely require spesific Rx– Alpha adrenergic blockers – preferred– B – blockers can be added, but only after
alpha blockade.– Drug of choice
• Phentolamine• Labetalol• Diazepam
Other disordersOther disorders
• Pre-eclampsia/Eclampsia– Goal SBP<160 and DBP<110 in pre-and-
intrapartum periods.– Platelets < 100 000, BP should be
maintained < 150/100– IV Magnesium to prevent seizures– Drug of choice:
• Methyldopa• Hydralazine

Other disordersOther disorders
• Perioperative hypertension– target BP to within 20% of baseline, except if
potential for life threatening arterial bleeding– typically related to catecholamine surge post-
op.– Drug of choice:
• B-blocker• Labetalol

LocalLocal
• Tygerberg– F1(medical outpatients)
• Nitroglycerine
– Cardiology ICU• Nitroglycerine
– Renal unit • Labetalol
– Obstetrics• Labetalol• Hydralazine

LocalLocal
• Grootte Schuur (C15)– Nitroglycerine (Tridal)
• Victoria– Nitroglycerine (Tridal/Nitrocine)– Labetalol– Can get Sodium nitroprusside

SummarySummary
• HPT crisis - serious condition - associated with EOD, if left untreated
• High mortality - untreated• Main causes – non-compliance and poorly
controlled chronic hypertension.• Urgency vs emergency• Treatment should be tailored to the individual’s
condition • HPT urgency – initial goal max 25% drop in MAP
in first 3 hours• Precipitous drop just as bad – good continuous
monitoring essential
References1. Joint National Committee on prevention, detection, evaluation and treatment of high
blood pressure.Seventh Report. Hypertension 42:2003; 1206-12522. Kitiyakara C, Guzman NJ. Malignant hypertension and hypertensive emergencies.J
Am Soc Nephrol 1998;9:1353. Vaidya CK, Ouellette JR. Hypertensive Urgency and Emergency. Hospital Physician
March 2007; 43-504. Vidt D. Hypertensive Crises: emergencies and urgencies. The Cleveland clinic
disease management project. 12 Jan 2006. Available at www.clevelandclinicmeded.com/diseasemanagement/nephrology/crises/crises.htm
5. McCowan C. Hypertensive Emergencies. Available at www.emedicine.medscape.com/emergencymedicine/cardiovascular. Updated Jan 26, 2009
6. Hollander JE. Cocaine intoxication and hypertension. Ann Emerg Med. Mar 2008;51:S18-20
7. Characteristics and management op patients presenting to the emergency department with hypertensive urgency. J.Clin Hypertens. 8:2006;12-18
8. Peck TE, Hill SA, Williams M.Pharmacology for anaesthesia and intensive care. 3rd Edition.Chapters 15 & 16,p246-269.
9. AggarwalMD, Khan IA. Hypertensive Crisis: Hypertensive emergencies and Urgencies.Cardiology Clinics 24:2006;135-146
10. Flanigan JS.Vitberg D.Hypertensive Emergency and Severe Hypertension: What to Treat, Who to Treat, and How to Treat. Med Clin N Am 90:2006;439-451





























