Embed Size (px)
Citation preview
HYPERTENSIONHYPERTENSION
SYAIFUL AZMI
Subdivision of Nephrology, Faculty of Medicine
Andalas University
Padang
Buku pegangan.Buku pegangan.
• HARRISON : INTERNAL MEDICINE
• SUPARTONDO : ILMU OENYAKIT DALAM
• NORMAN KAPLAN : CLINICAL
HYPERTENSION
Section 1: Definition and Classification Section 1: Definition and Classification of Hypertensionof Hypertension
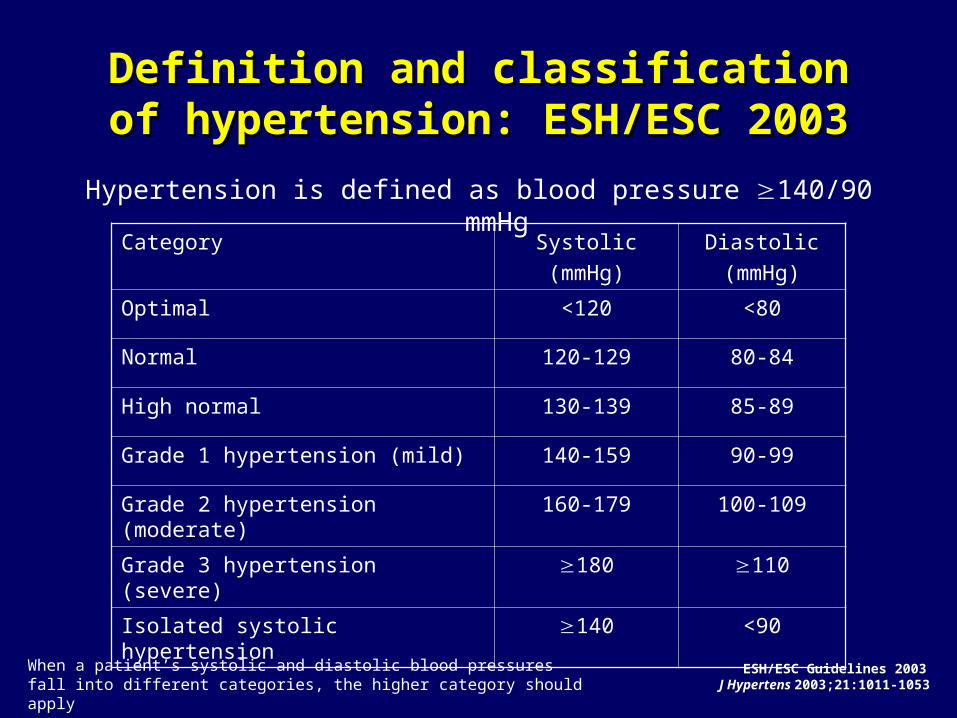
Definition and classification of Definition and classification of hypertension: ESH/ESC 2003hypertension: ESH/ESC 2003
Hypertension is defined as blood pressure 140/90 mmHg
Category Systolic
(mmHg)
Diastolic
(mmHg)
Optimal <120 <80
Normal 120-129 80-84
High normal 130-139 85-89
Grade 1 hypertension (mild) 140-159 90-99
Grade 2 hypertension (moderate) 160-179 100-109
Grade 3 hypertension (severe) 180 110
Isolated systolic hypertension 140 <90
ESH/ESC Guidelines 2003 J Hypertens 2003;21:1011-1053
When a patient’s systolic and diastolic blood pressures fall into different categories, the higher category should apply
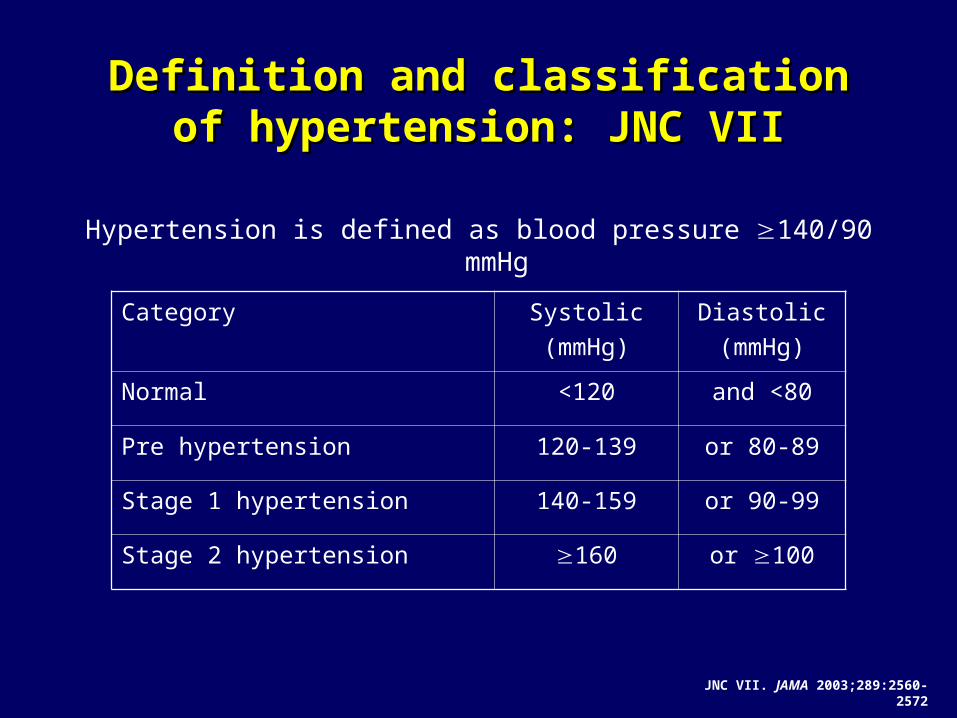
Definition and classification of Definition and classification of hypertension: JNC VIIhypertension: JNC VII
Hypertension is defined as blood pressure 140/90 mmHg
Category Systolic
(mmHg)
Diastolic
(mmHg)
Normal <120 and <80
Pre hypertension 120-139 or 80-89
Stage 1 hypertension 140-159 or 90-99
Stage 2 hypertension 160 or 100
JNC VII. JAMA 2003;289:2560-2572
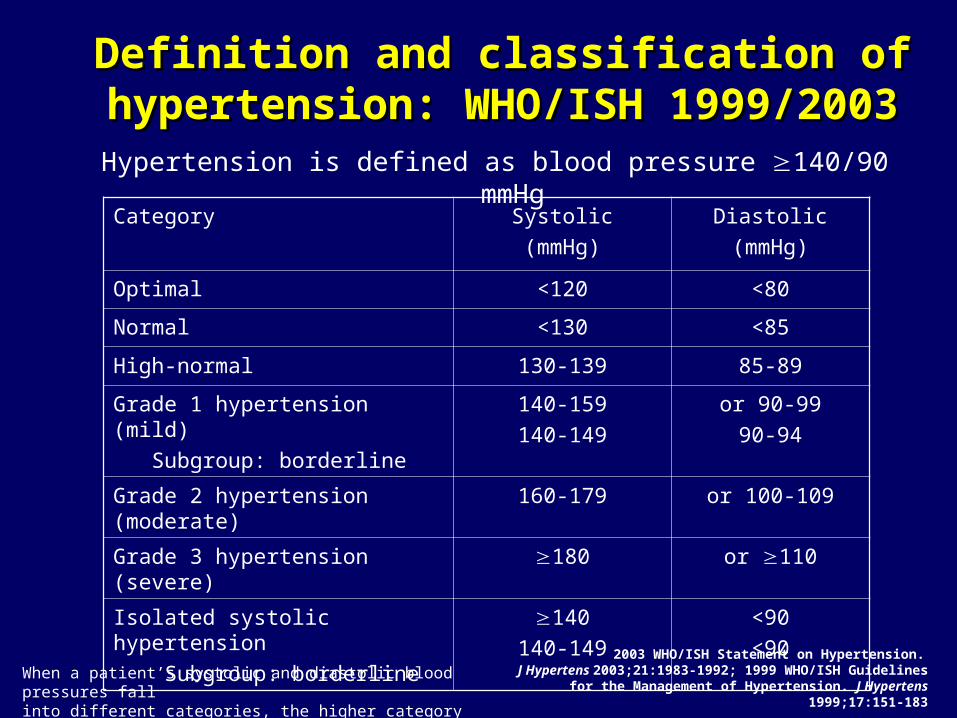
Definition and classification of Definition and classification of hypertension: WHO/ISH 1999/2003hypertension: WHO/ISH 1999/2003
Hypertension is defined as blood pressure 140/90 mmHg
Category Systolic
(mmHg)
Diastolic
(mmHg)
Optimal <120 <80
Normal <130 <85
High-normal 130-139 85-89
Grade 1 hypertension (mild)
Subgroup: borderline
140-159140-149
or 90-99
90-94
Grade 2 hypertension (moderate) 160-179 or 100-109
Grade 3 hypertension (severe) 180 or 110
Isolated systolic hypertension
Subgroup: borderline
140140-149
<90<90
2003 WHO/ISH Statement on Hypertension. J Hypertens 2003;21:1983-1992; 1999 WHO/ISH Guidelines for the
Management of Hypertension. J Hypertens 1999;17:151-183When a patient’s systolic and diastolic blood pressures fall into different categories, the higher category should apply
Section 2: Prevalence of HypertensionSection 2: Prevalence of Hypertension
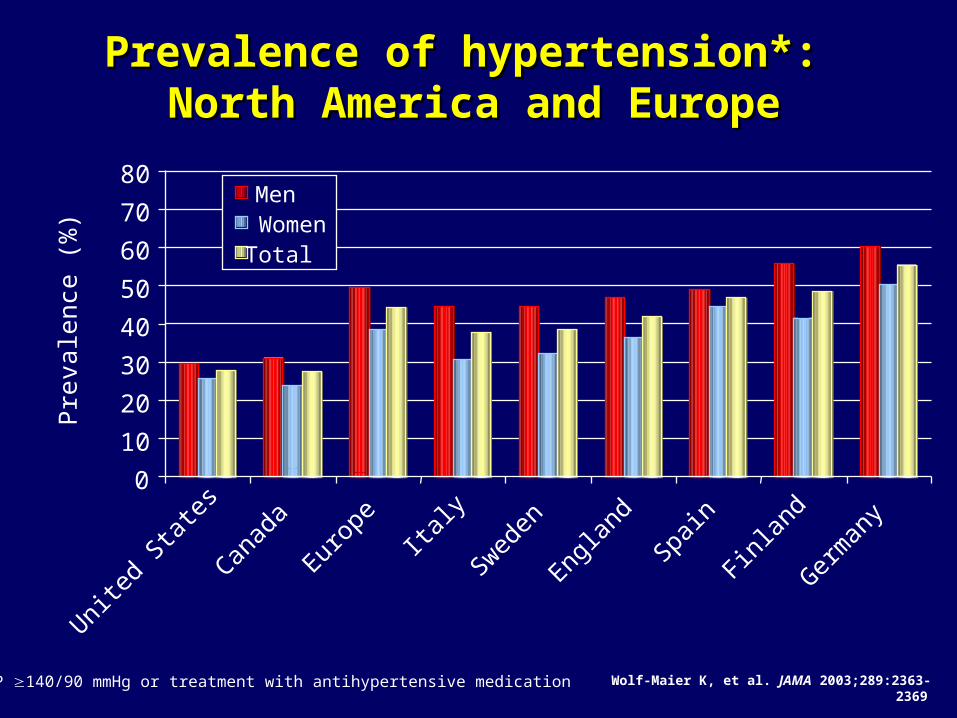
Prevalence of hypertension*: Prevalence of hypertension*: North America and EuropeNorth America and Europe
0
10
20
30
40
50
60
70
80
United
Sta
tes
Canad
a
Europ
eIta
ly
Sweden
Englan
d
Spain
Finlan
d
Germ
any
Pre
vale
nce
(%)
MenWomenTotal
Wolf-Maier K, et al. JAMA 2003;289:2363-2369 * BP 140/90 mmHg or treatment with antihypertensive medication
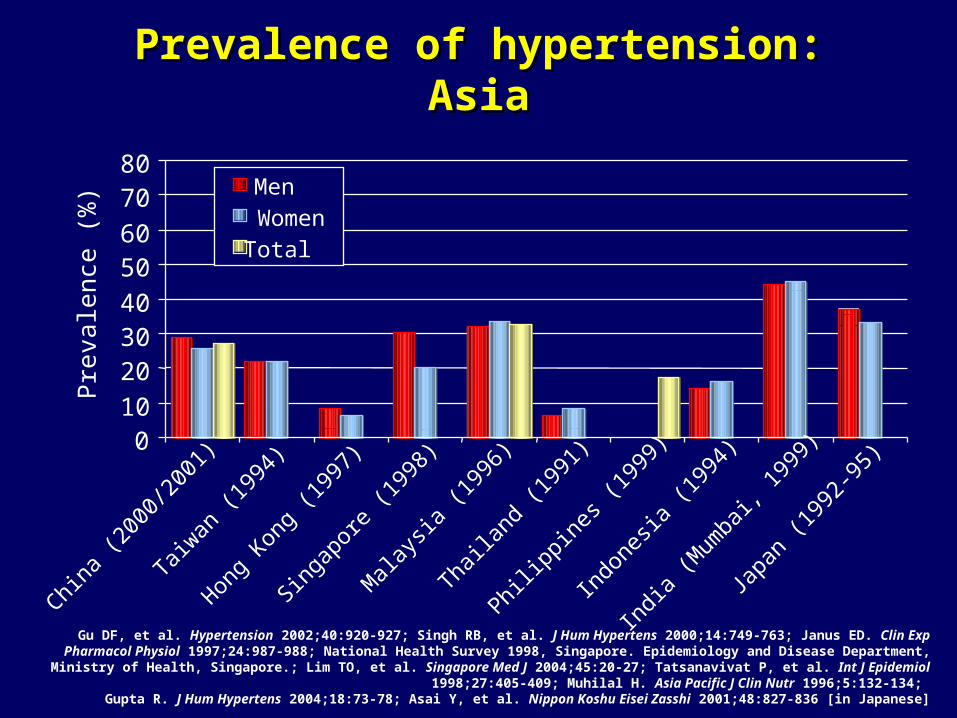
Prevalence of hypertension: AsiaPrevalence of hypertension: Asia
010
203040
5060
7080
China
(200
0/20
01)
Taiwan
(199
4)
Hong
Kong
(199
7)
Singap
ore
(199
8)
Mala
ysia
(199
6)
Thaila
nd (1
991)
Philipp
ines (
1999
)
Indo
nesia
(199
4)
India
(Mum
bai, 1
999)
Japa
n (1
992-
95)
Pre
vale
nce
(%)
MenWomenTotal
Gu DF, et al. Hypertension 2002;40:920-927; Singh RB, et al. J Hum Hypertens 2000;14:749-763; Janus ED. Clin Exp Pharmacol Physiol 1997;24:987-988; National Health Survey 1998, Singapore. Epidemiology and Disease Department, Ministry of Health, Singapore.; Lim TO, et al.
Singapore Med J 2004;45:20-27; Tatsanavivat P, et al. Int J Epidemiol 1998;27:405-409; Muhilal H. Asia Pacific J Clin Nutr 1996;5:132-134; Gupta R. J Hum Hypertens 2004;18:73-78; Asai Y, et al. Nippon Koshu Eisei Zasshi 2001;48:827-836 [in Japanese]
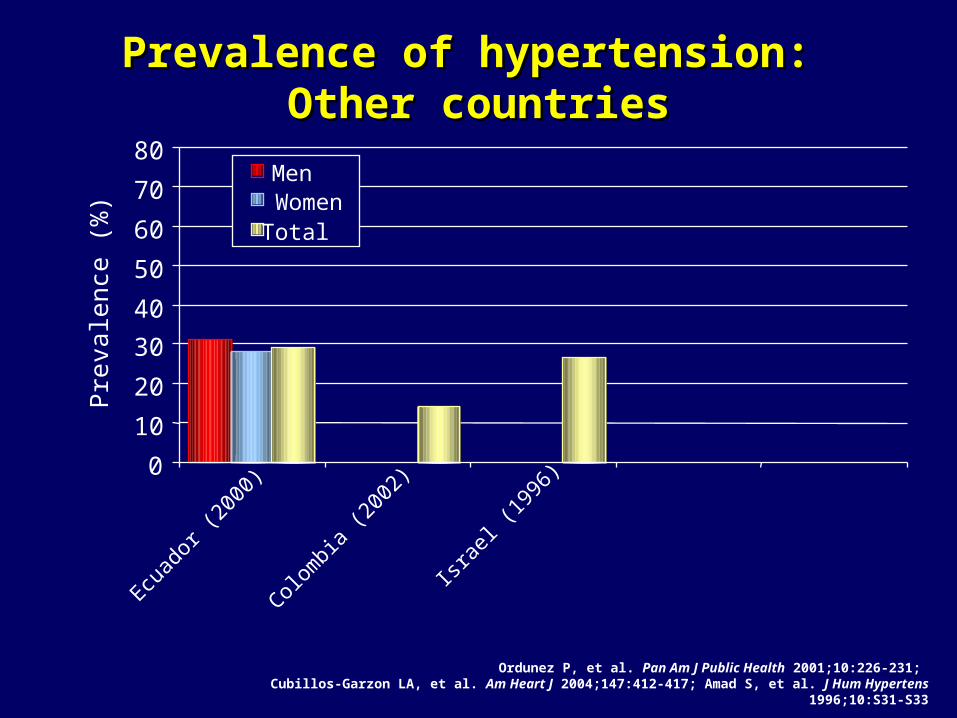
Prevalence of hypertension: Prevalence of hypertension: Other countriesOther countries
0
10
20
30
40
50
60
70
80
Ecuad
or (2
000)
Colom
bia (2
002)
Israe
l (19
96)
Pre
vale
nce
(%)
MenWomenTotal
Ordunez P, et al. Pan Am J Public Health 2001;10:226-231; Cubillos-Garzon LA, et al. Am Heart J 2004;147:412-417; Amad S, et al. J Hum Hypertens 1996;10:S31-S33
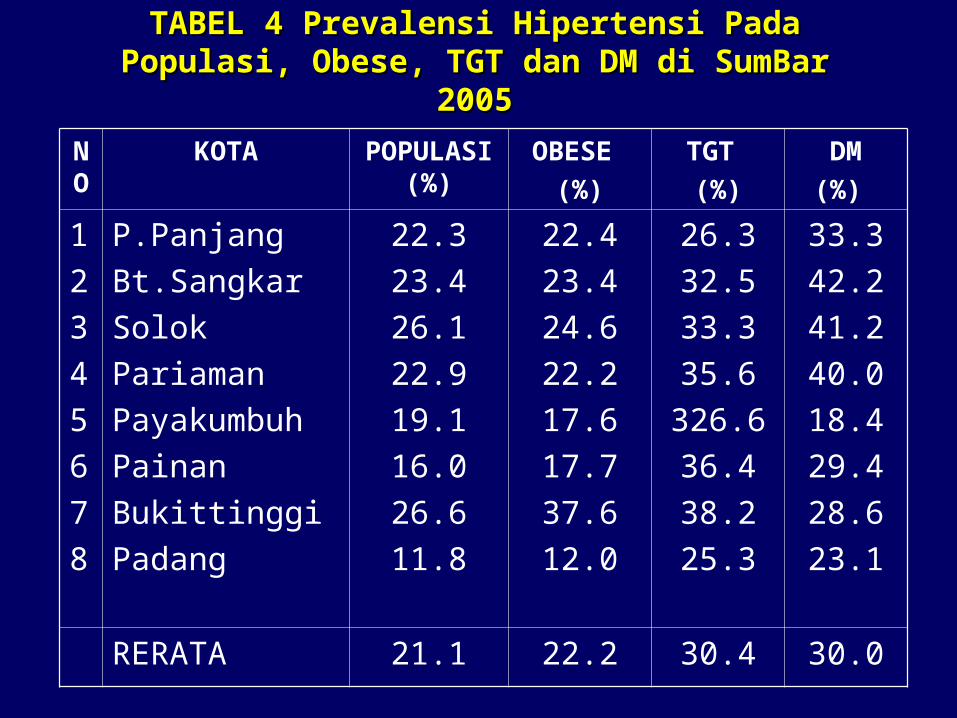
TABEL 4 Prevalensi Hipertensi Pada TABEL 4 Prevalensi Hipertensi Pada Populasi, Obese, TGT dan DM di SumBar Populasi, Obese, TGT dan DM di SumBar
20052005
NO
KOTA POPULASI (%)
OBESE
(%)
TGT
(%)
DM
(%)
1
2
3
4
5
6
7
8
P.Panjang
Bt.Sangkar
Solok
Pariaman
Payakumbuh
Painan
Bukittinggi
Padang
22.3
23.4
26.1
22.9
19.1
16.0
26.6
11.8
22.4
23.4
24.6
22.2
17.6
17.7
37.6
12.0
26.3
32.5
33.3
35.6
326.6
36.4
38.2
25.3
33.3
42.2
41.2
40.0
18.4
29.4
28.6
23.1
RERATA 21.1 22.2 30.4 30.0
Section 3 : Classification of Section 3 : Classification of hypertensionhypertension
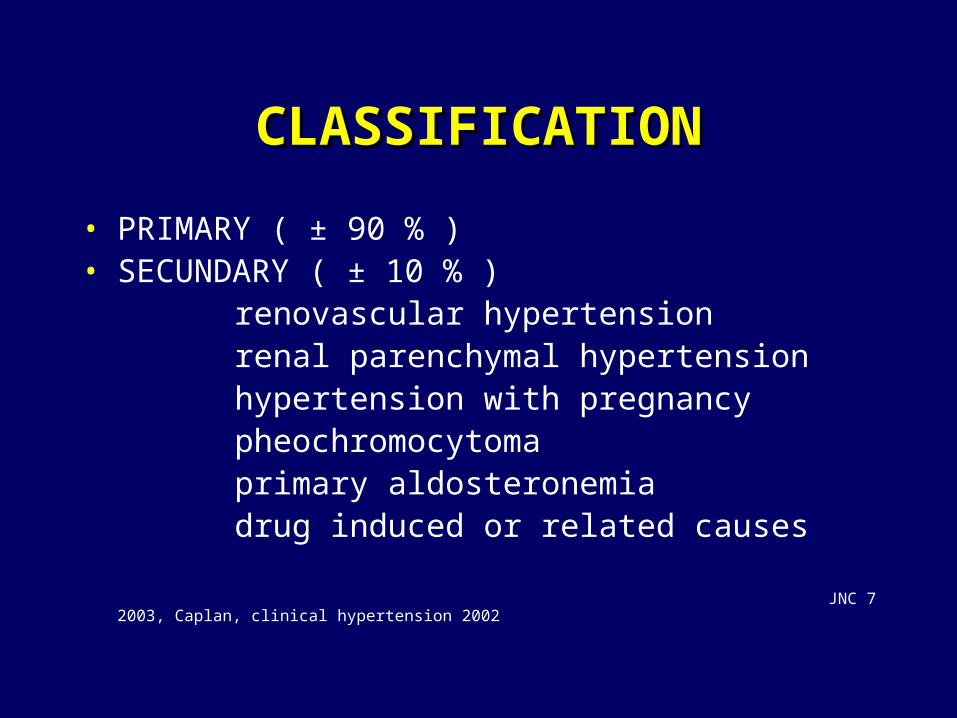
CLASSIFICATIONCLASSIFICATION
• PRIMARY ( ± 90 % )• SECUNDARY ( ± 10 % ) renovascular hypertension renal parenchymal hypertension hypertension with pregnancy pheochromocytoma primary aldosteronemia drug induced or related causes
JNC 7 2003, Caplan, clinical hypertension 2002
Section 4 : Risk factors of Section 4 : Risk factors of HypertensionHypertension
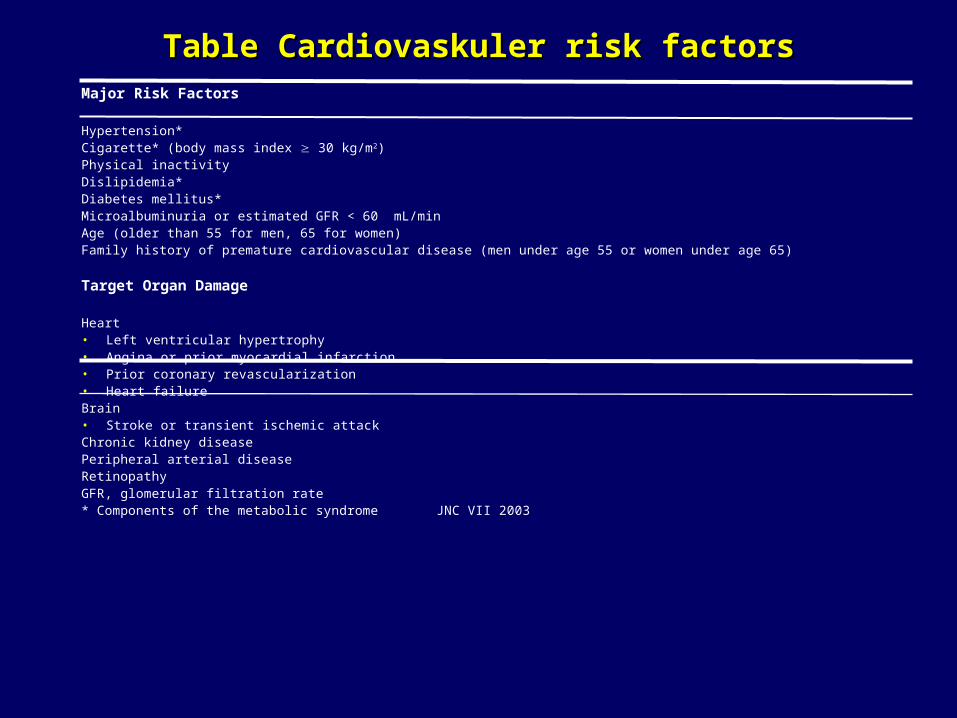
Table Cardiovaskuler risk factorsTable Cardiovaskuler risk factorsMajor Risk Factors Hypertension*Cigarette* (body mass index 30 kg/m2)Physical inactivityDislipidemia*Diabetes mellitus*Microalbuminuria or estimated GFR < 60 mL/minAge (older than 55 for men, 65 for women)Family history of premature cardiovascular disease (men under age 55 or women under age 65)
Target Organ Damage
Heart• Left ventricular hypertrophy• Angina or prior myocardial infarction• Prior coronary revascularization• Heart failureBrain• Stroke or transient ischemic attackChronic kidney diseasePeripheral arterial diseaseRetinopathyGFR, glomerular filtration rate* Components of the metabolic syndrome JNC VII 2003
Risk factorsRisk factors
• Gender• Race• Age• Family history• Cigarette smoking• Obesity ( BMI ≥ 30 Kg/m2 )*• Physical activity• Dyslipidemia*• Diabetes Mellitus*• Microalbuminuria
* componen of metabolic syndrome JNC 7 2003
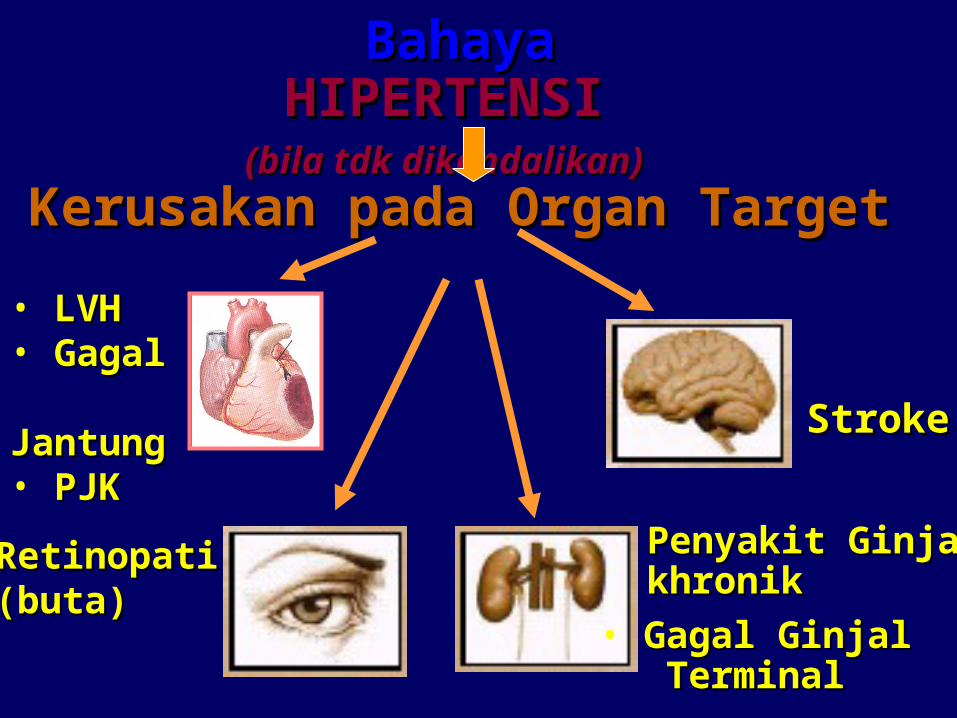
Bahaya Bahaya HIPERTENSI HIPERTENSI (bila tdk dikendalikan)(bila tdk dikendalikan)
Kerusakan pada Organ Target Kerusakan pada Organ Target
StrokeStroke
RetinopatiRetinopati(buta)(buta)
• LVH LVH • Gagal Gagal JantungJantung• PJKPJK
Penyakit GinjalPenyakit Ginjalkhronikkhronik
• Gagal GinjalGagal Ginjal TerminalTerminal
Section 5 : Pathophysiology and Section 5 : Pathophysiology and Pathogenesis of HypertensionPathogenesis of Hypertension
PATHOPHYSIOLOGY OF HYPERTENSIONPATHOPHYSIOLOGY OF HYPERTENSION
Several hypothesis exists of the original pathogenesis of hypertension- Excess Na intake- Renal Na retention- RAS- Stress & sympathetic activity- Peripheral resistance- Endothelial dysfunction- Obesity- Insulin resistance
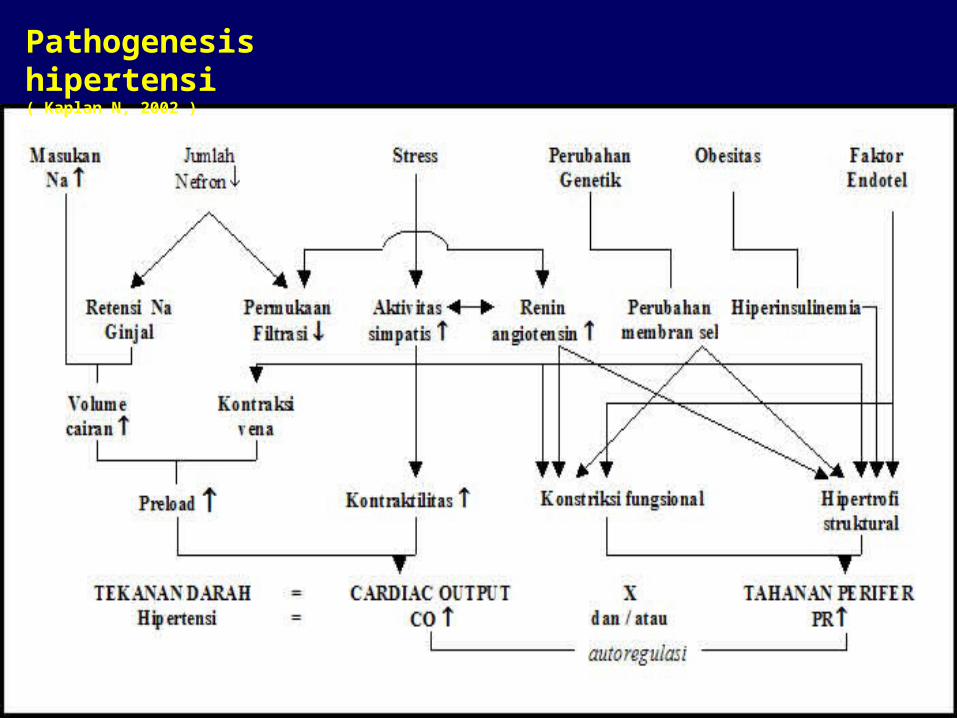
Pathogenesis hipertensi( Kaplan N, 2002 )
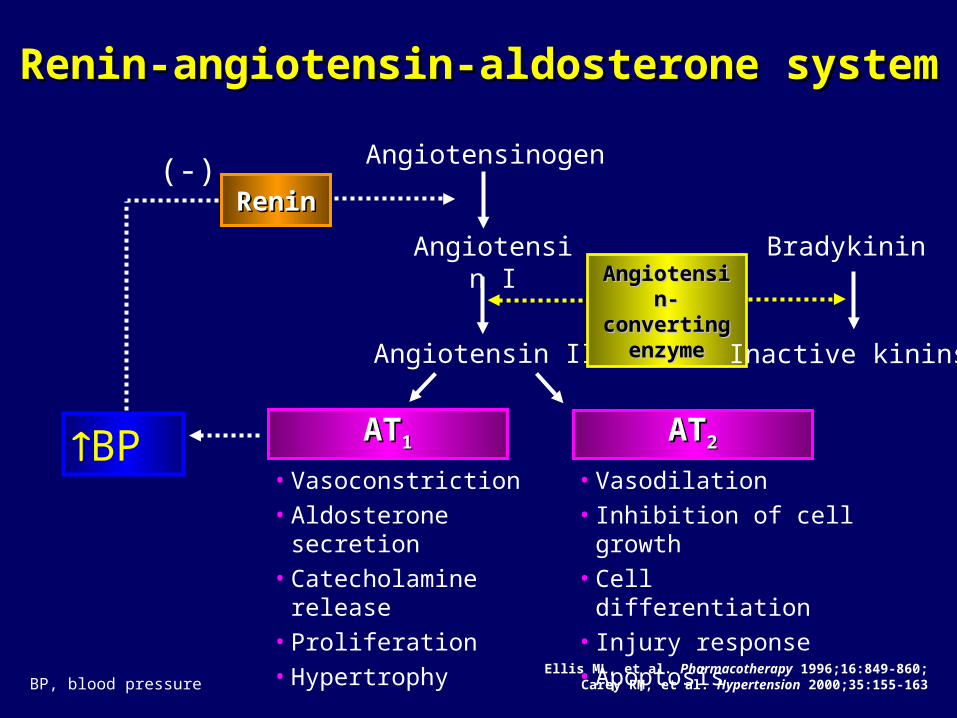
Angiotensinogen
Angiotensin I
Angiotensin II
Ellis ML, et al. Pharmacotherapy 1996;16:849-860;Carey RM, et al. Hypertension 2000;35:155-163
ATAT11 ATAT22
• Vasoconstriction
• Aldosterone secretion
• Catecholamine release
• Proliferation
• Hypertrophy
• Vasodilation
• Inhibition of cell growth
• Cell differentiation
• Injury response
• Apoptosis
BP
(-)
Renin-angiotensin-aldosterone systemRenin-angiotensin-aldosterone system
ReninRenin
Angiotensin-Angiotensin-converting converting
enzymeenzyme
Bradykinin
Inactive kinins
BP, blood pressure
Section 6 : Diagnosis of HypertensionSection 6 : Diagnosis of Hypertension
SYMPTOMSSYMPTOMS
Headache Nocturia Palpitation Dizziness Tinitus Epistaxis
Kaplan N , 2002
PHYSICAL EXAMINATIONPHYSICAL EXAMINATION
25
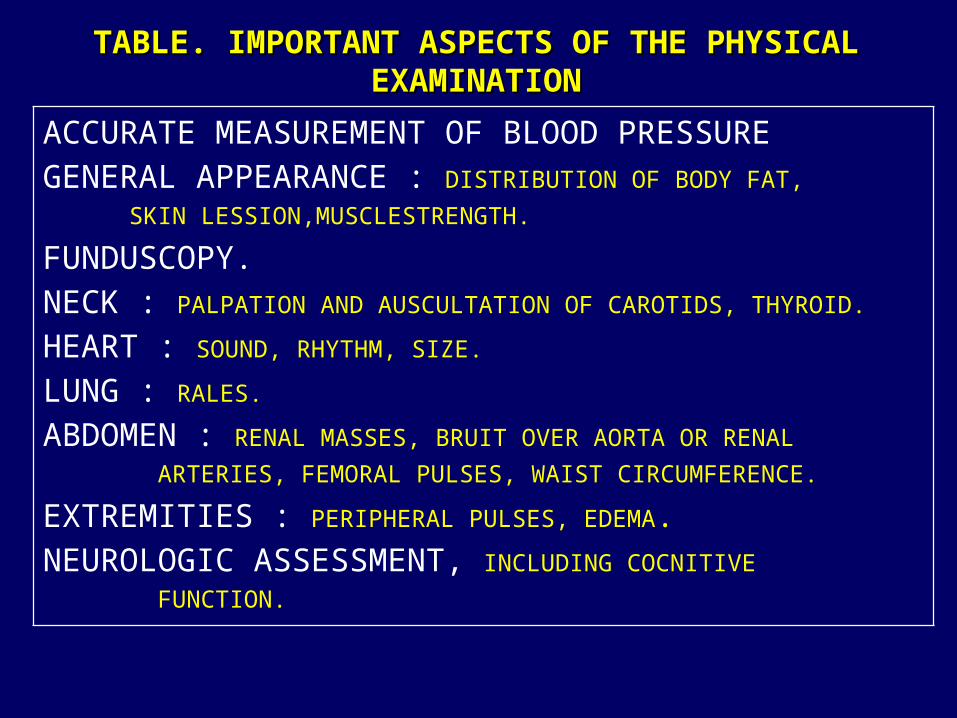
TABLE. IMPORTANT ASPECTS OF THE PHYSICAL TABLE. IMPORTANT ASPECTS OF THE PHYSICAL EXAMINATIONEXAMINATION
ACCURATE MEASUREMENT OF BLOOD PRESSUREGENERAL APPEARANCE : DISTRIBUTION OF BODY FAT,
SKIN LESSION,MUSCLESTRENGTH.
FUNDUSCOPY.NECK : PALPATION AND AUSCULTATION OF CAROTIDS, THYROID.
HEART : SOUND, RHYTHM, SIZE.
LUNG : RALES.
ABDOMEN : RENAL MASSES, BRUIT OVER AORTA OR RENAL
ARTERIES, FEMORAL PULSES, WAIST CIRCUMFERENCE.
EXTREMITIES : PERIPHERAL PULSES, EDEMA.NEUROLOGIC ASSESSMENT, INCLUDING COCNITIVE
FUNCTION.
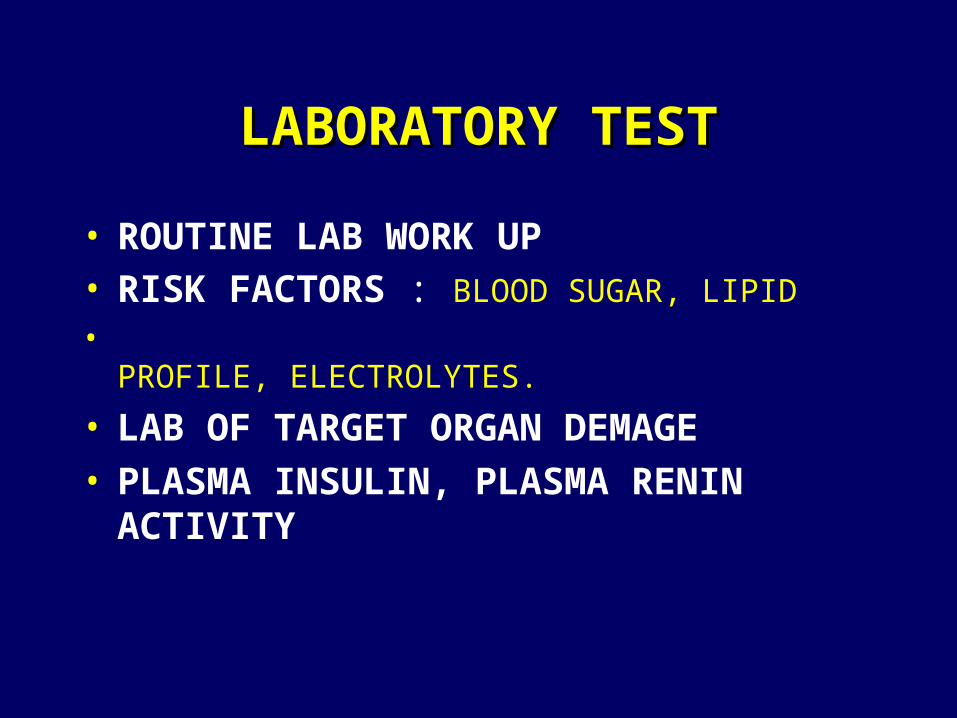
LABORATORY TESTLABORATORY TEST
• ROUTINE LAB WORK UP• RISK FACTORS : BLOOD SUGAR, LIPID
• PROFILE, ELECTROLYTES.
• LAB OF TARGET ORGAN DEMAGE • PLASMA INSULIN, PLASMA RENIN
ACTIVITY
FUNDUSCOPY EXAMINATION : FUNDUSCOPY EXAMINATION : RETINOPATHYRETINOPATHY
CARDIAC ASSESSMENT : LVH, ARYTHMIA
CEREBRAL ASSESSMENT :
ENCEPHALOPATHY
RENAL ASSESSMENT
Section 7 : Treatment GuidelinesSection 7 : Treatment Guidelines
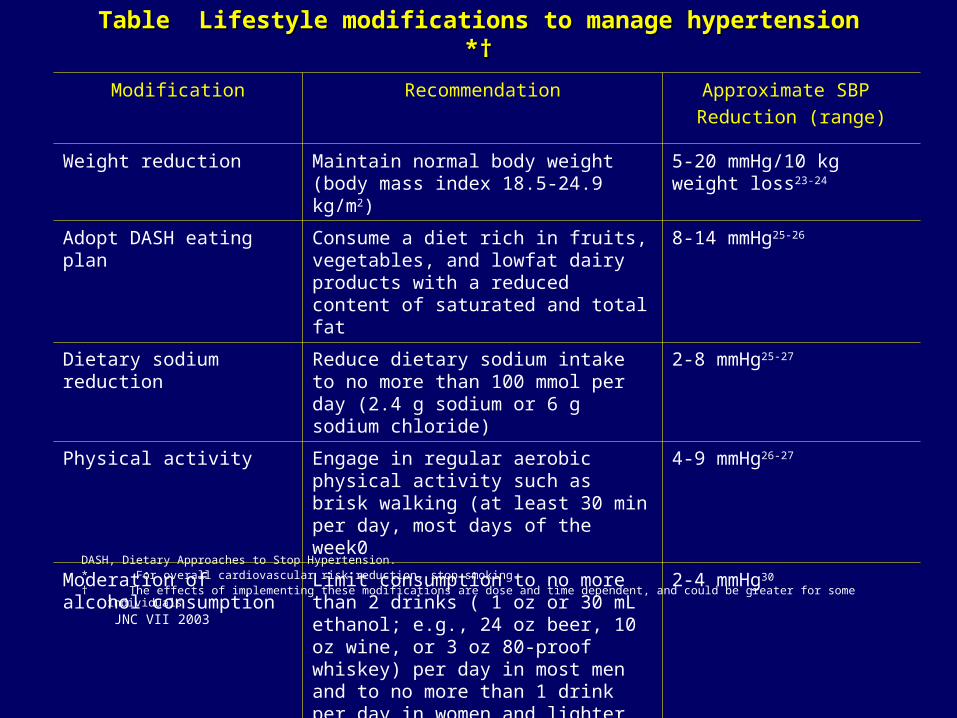
Table Lifestyle modifications to manage hypertension *†Table Lifestyle modifications to manage hypertension *†
DASH, Dietary Approaches to Stop Hypertension.* For overall cardiovascular risk reduction, stop smoking.† The effects of implementing these modifications are dose and time dependent, and could be greater for some individuals
JNC VII 2003
Modification Recommendation Approximate SBP
Reduction (range)
Weight reduction Maintain normal body weight (body mass index 18.5-24.9 kg/m2)
5-20 mmHg/10 kg weight loss23-24
Adopt DASH eating plan Consume a diet rich in fruits, vegetables, and lowfat dairy products with a reduced content of saturated and total fat
8-14 mmHg25-26
Dietary sodium reduction Reduce dietary sodium intake to no more than 100 mmol per day (2.4 g sodium or 6 g sodium chloride)
2-8 mmHg25-27
Physical activity Engage in regular aerobic physical activity such as brisk walking (at least 30 min per day, most days of the week0
4-9 mmHg26-27
Moderation of alcohol consumption
Limit consumption to no more than 2 drinks ( 1 oz or 30 mL ethanol; e.g., 24 oz beer, 10 oz wine, or 3 oz 80-proof whiskey) per day in most men and to no more than 1 drink per day in women and lighter weight persons
2-4 mmHg30
THE IDEAL ANTIHYPERTENSIVE AGENTTHE IDEAL ANTIHYPERTENSIVE AGENT
- Effectively reduces BP- Maintains BP control over 24 hours with
once-a-day dosing- Effective in all hypertensive patients- No adverse effects- No negative metabolic side effects
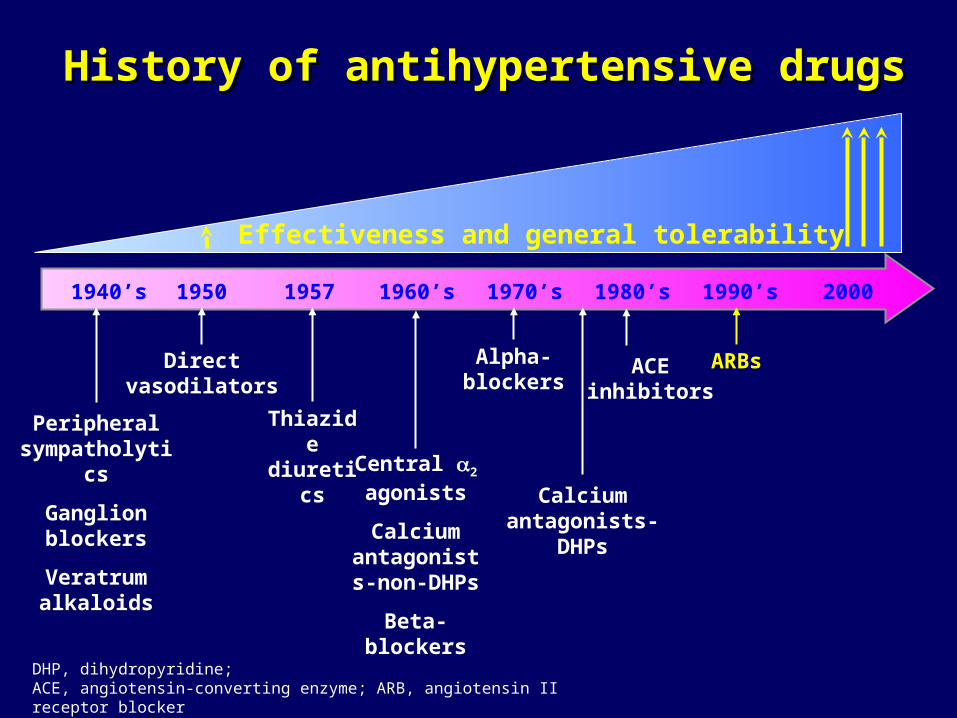
History of antihypertensive drugsHistory of antihypertensive drugs
Directvasodilators
Alpha-blockers
Peripheralsympatholytics
Ganglion blockers
Veratrumalkaloids
Central 2 agonists
Calciumantagonists-non-DHPs
Beta-blockers
Thiazidediuretics
Calciumantagonists-
DHPs
ARBs
1940’s 1950 1957 1960’s 1970’s 1980’s 1990’s 2000
ACEinhibitors
DHP, dihydropyridine; ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker
Effectiveness and general tolerability
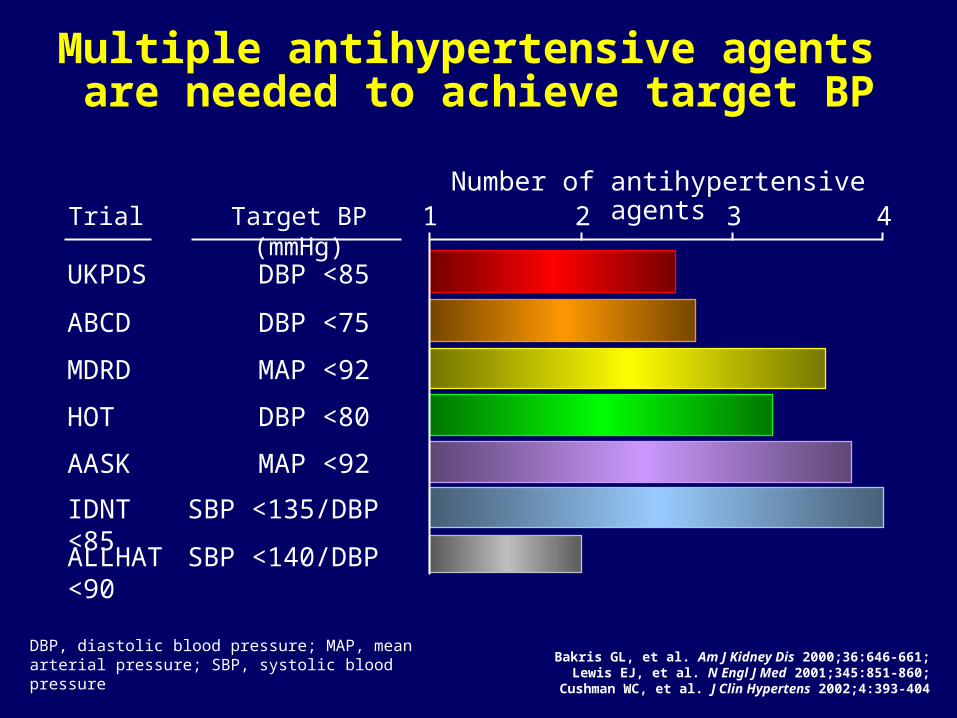
AASK MAP <92
Target BP (mmHg)
Multiple antihypertensive agents are needed to achieve target BP
Number of antihypertensive agents1
UKPDS DBP <85
ABCD DBP <75
MDRD MAP <92
HOT DBP <80
Trial 2 3 4
DBP, diastolic blood pressure; MAP, mean arterial pressure; SBP, systolic blood pressure
IDNT SBP <135/DBP <85
ALLHAT SBP <140/DBP <90
Bakris GL, et al. Am J Kidney Dis 2000;36:646-661;Lewis EJ, et al. N Engl J Med 2001;345:851-860;
Cushman WC, et al. J Clin Hypertens 2002;4:393-404
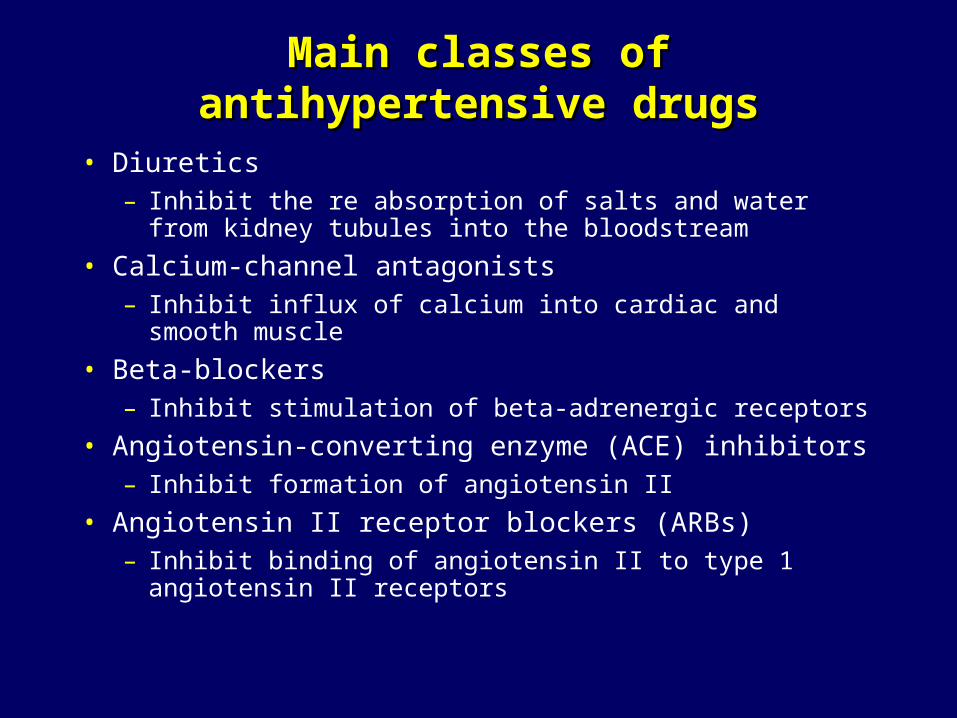
Main classes of antihypertensive drugsMain classes of antihypertensive drugs
• Diuretics– Inhibit the re absorption of salts and water from kidney
tubules into the bloodstream
• Calcium-channel antagonists– Inhibit influx of calcium into cardiac and smooth muscle
• Beta-blockers– Inhibit stimulation of beta-adrenergic receptors
• Angiotensin-converting enzyme (ACE) inhibitors– Inhibit formation of angiotensin II
• Angiotensin II receptor blockers (ARBs)– Inhibit binding of angiotensin II to type 1 angiotensin II
receptors
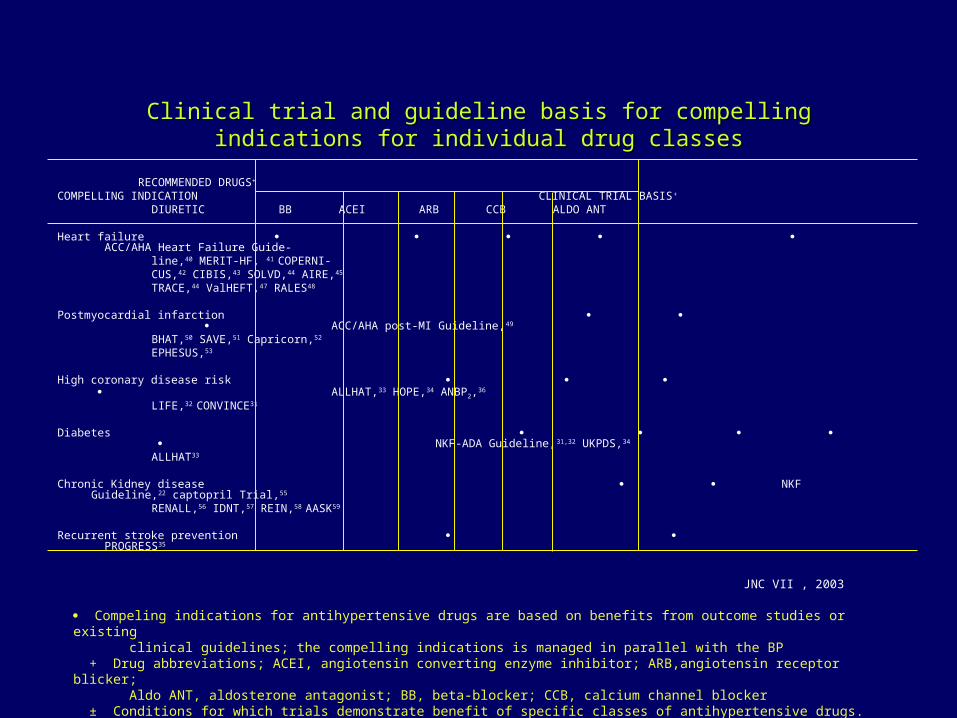
Clinical trial and guideline basis for compelling indications for individual drug Clinical trial and guideline basis for compelling indications for individual drug classesclasses
RECOMMENDED DRUGS+
COMPELLING INDICATION CLINICAL TRIAL BASIS+
DIURETIC BB ACEI ARB CCB ALDO ANT
Heart failure ACC/AHA Heart Failure Guide- line,40 MERIT-HF, 41 COPERNI- CUS,42 CIBIS,43 SOLVD,44 AIRE,45 TRACE,44 ValHEFT,47 RALES48
Postmyocardial infarction ACC/AHA post-MI Guideline,49
BHAT,50 SAVE,51 Capricorn,52
EPHESUS,53
High coronary disease risk ALLHAT,33 HOPE,34 ANBP2,36
LIFE,32 CONVINCE31
Diabetes NKF-ADA Guideline,31,32 UKPDS,34
ALLHAT33
Chronic Kidney disease NKF Guideline,22 captopril Trial,55
RENALL,56 IDNT,57 REIN,58 AASK59
Recurrent stroke prevention PROGRESS35
JNC VII , 2003
Compeling indications for antihypertensive drugs are based on benefits from outcome studies or existing clinical guidelines; the compelling indications is managed in parallel with the BP + Drug abbreviations; ACEI, angiotensin converting enzyme inhibitor; ARB,angiotensin receptor blicker; Aldo ANT, aldosterone antagonist; BB, beta-blocker; CCB, calcium channel blocker ± Conditions for which trials demonstrate benefit of specific classes of antihypertensive drugs.
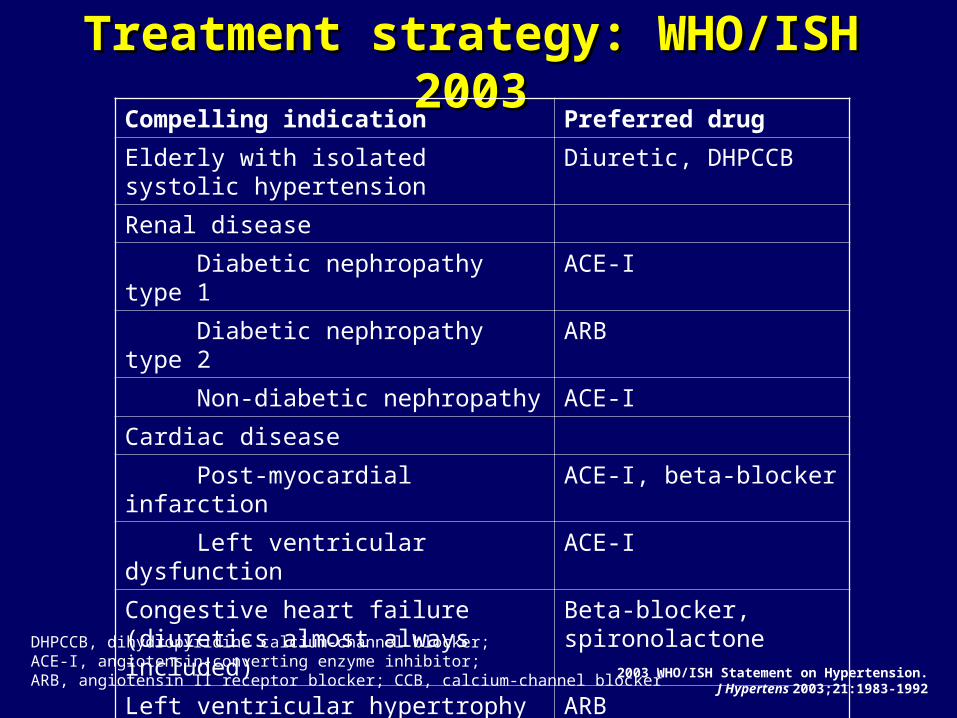
Treatment strategy: WHO/ISH 2003Treatment strategy: WHO/ISH 2003
2003 WHO/ISH Statement on Hypertension.J Hypertens 2003;21:1983-1992
Compelling indication Preferred drug
Elderly with isolated systolic hypertension
Diuretic, DHPCCB
Renal disease
Diabetic nephropathy type 1 ACE-I
Diabetic nephropathy type 2 ARB
Non-diabetic nephropathy ACE-I
Cardiac disease
Post-myocardial infarction ACE-I, beta-blocker
Left ventricular dysfunction ACE-I
Congestive heart failure (diuretics almost always included)
Beta-blocker, spironolactone
Left ventricular hypertrophy ARB
Cerebrovascular disease ACE-I + diuretic, diuretic
DHPCCB, dihydropyridine calcium-channel blocker; ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; CCB, calcium-channel blocker
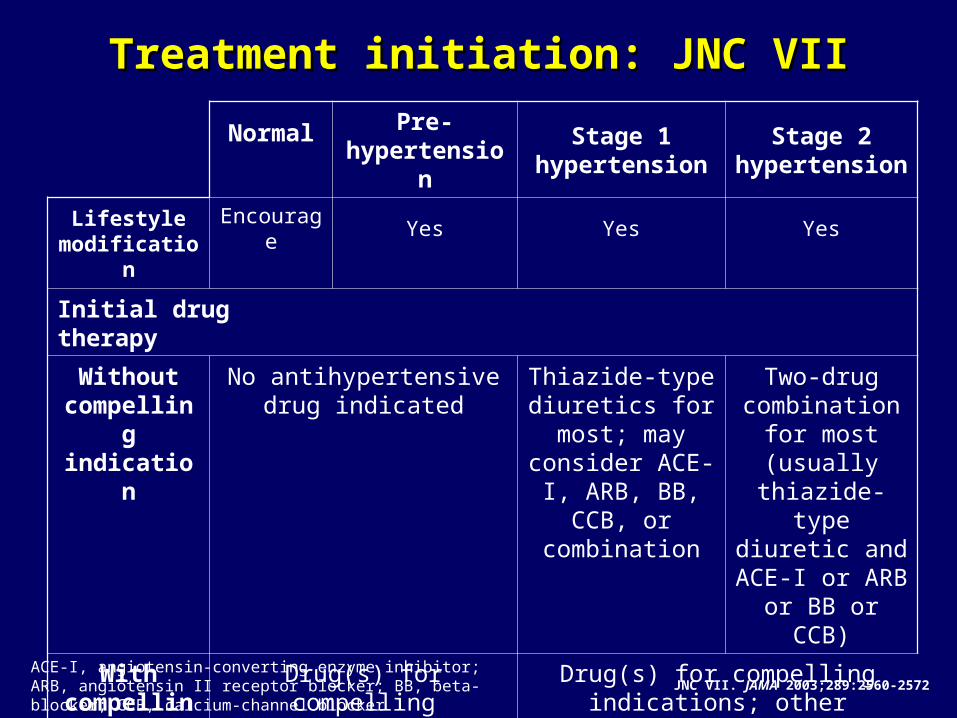
Treatment initiation: JNC VIITreatment initiation: JNC VII
Normal Pre-hypertension
Stage 1 hypertension
Stage 2 hypertension
Lifestyle modification
Encourage Yes Yes Yes
Initial drug therapy
Without compelling indication
No antihypertensive drug indicated
Thiazide-type diuretics for most;
may consider ACE-I, ARB, BB,
CCB, or combination
Two-drug combination for most (usually thiazide-type diuretic and
ACE-I or ARB or BB or CCB)
With compelling indications
Drug(s) for compelling indications
Drug(s) for compelling indications; other antihypertensive drugs
(diuretics, ACE-I, ARB, BB, CCB) as needed
ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BB, beta-blocker; CCB, calcium-channel blocker JNC VII. JAMA 2003;289:2560-2572
Goals of treatment: JNC VIIGoals of treatment: JNC VII
• The SBP and DBP targets are <140/90 mmHg
• The primary focus should be on achieving the SBP goal
• In patients with hypertension and diabetes or renal disease, the BP goal is <130/80 mmHg
JNC VII. JAMA 2003;289:2560-2572SBP, systolic blood pressure; DBP, diastolic blood pressure; BP, blood pressure
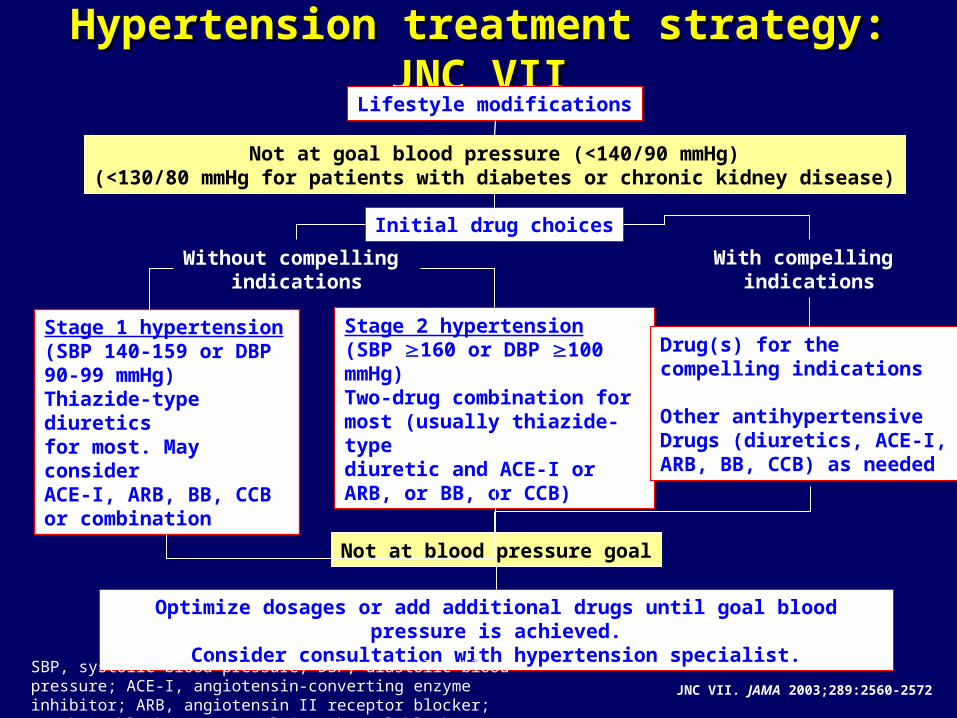
Hypertension treatment strategy: JNC VIIHypertension treatment strategy: JNC VIILifestyle modifications
Not at goal blood pressure (<140/90 mmHg)(<130/80 mmHg for patients with diabetes or chronic kidney disease)
Initial drug choices
Without compelling indications
With compelling indications
Stage 1 hypertension(SBP 140-159 or DBP90-99 mmHg)Thiazide-type diuretics for most. May consider ACE-I, ARB, BB, CCBor combination
Stage 2 hypertension(SBP 160 or DBP 100 mmHg)Two-drug combination formost (usually thiazide-typediuretic and ACE-I or ARB, or BB, or CCB)
Drug(s) for the compelling indications
Other antihypertensiveDrugs (diuretics, ACE-I, ARB, BB, CCB) as needed
Not at blood pressure goal
Optimize dosages or add additional drugs until goal blood pressure is achieved.Consider consultation with hypertension specialist.
JNC VII. JAMA 2003;289:2560-2572
SBP, systolic blood pressure; DBP, diastolic blood pressure; ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BB, beta-blocker; CCB, calcium-channel blocker
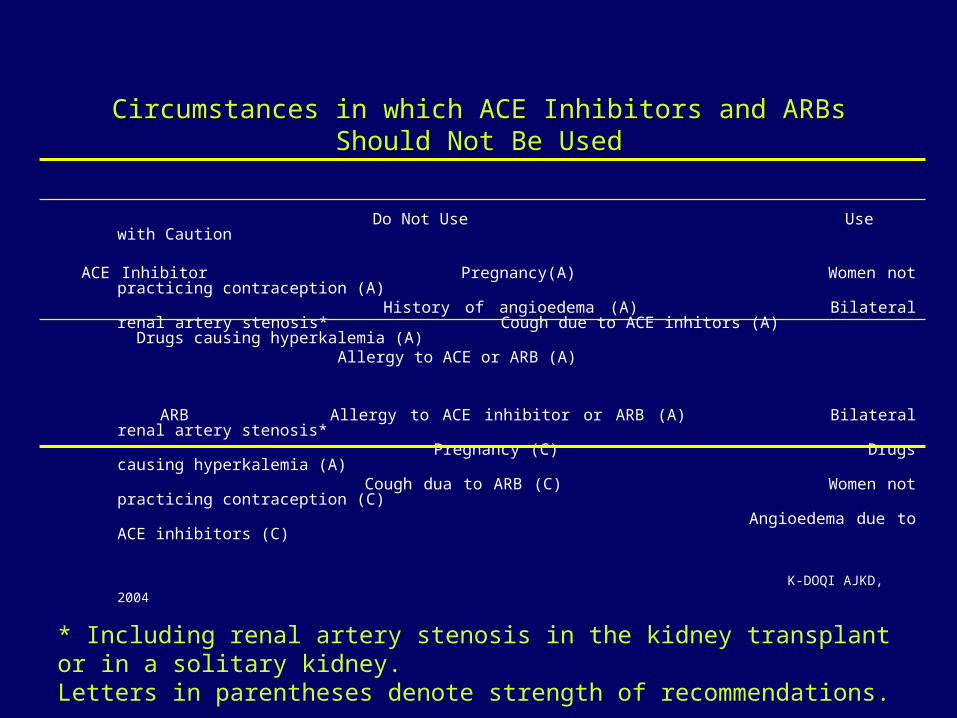
Circumstances in which ACE Inhibitors and ARBs Should Not Be Circumstances in which ACE Inhibitors and ARBs Should Not Be UsedUsed
Do Not Use Use with Caution
ACE Inhibitor Pregnancy(A) Women not practicing contraception (A) History of angioedema (A) Bilateral renal artery stenosis*Cough due to ACE inhitors (A) Drugs causing hyperkalemia (A) Allergy to ACE or ARB (A)
ARB Allergy to ACE inhibitor or ARB (A) Bilateral renal artery stenosis* Pregnancy (C) Drugs causing hyperkalemia (A) Cough dua to ARB (C) Women not practicing contraception
(C) Angioedema due to ACE inhibitors
(C)
K-DOQI AJKD, 2004
* Including renal artery stenosis in the kidney transplant or in a solitary kidney.Letters in parentheses denote strength of recommendations.
Diuretik : Hati hati pada :
- gangguan elektrolit
- dislipidemia
Beta bloker hati hati pada :
- Asma bronkhial / spasme bronkhus
- Diabetes melitus