-
7/27/2019 Hypertension Lecture for Cci 2013
1/74
Hypertensive Disorders in Pregnancy
Hypertensive Disorders in
Pregnancy
Joseph U. Olivar MD, FPOGS, FPSMFM
Department of OB-GYN
Seamens Hospital
FEU-NRMF Medical Center
-
7/27/2019 Hypertension Lecture for Cci 2013
2/74
Hypertensive Disorders in Pregnancy
Case
28 y/o, G1, 32 weeks came in for first prenatal
check-up. BP of 130/90 mmHg. Repeat BP the
next day 140/80 mmHg.Is the woman hypertensive?
YES OR NO?
-
7/27/2019 Hypertension Lecture for Cci 2013
3/74
Hypertensive Disorders in Pregnancy
Gestational Hypertension
Preeclampsia
Eclampsia
Chronic Hypertension
Superimposed Preeclampsia on Chronic
hypertension
Classification of Hypertensive Disorders complicating
pregnancy
(Working Group of the NHBPEP 2000):
-
7/27/2019 Hypertension Lecture for Cci 2013
4/74
Hypertensive Disorders in Pregnancy
BP 140/90mmHg for the first during
pregnancy after 20 weeks
No proteinuria
BP returns to normal
-
7/27/2019 Hypertension Lecture for Cci 2013
5/74
Hypertensive Disorders in Pregnancy
Seizures that cannot be attributed to other
causes in a woman with preeclampsia
Eclampsia
-
7/27/2019 Hypertension Lecture for Cci 2013
6/74
Hypertensive Disorders in Pregnancy
BP 140/90 mm Hg before pregnancy or
diagnosed before 20 weeks' gestation not
attributable to gestational trophoblasticdisease;
or hypertension first diagnosed after 20 weeks'gestation and
persistent after 12 weeks'
postpartum
CHRONIC HYPERTENSION
-
7/27/2019 Hypertension Lecture for Cci 2013
7/74Hypertensive Disorders in Pregnancy
New-onset proteinuria 300 mg/24 hours in
hypertensive women but no proteinuria before 20
weeks' gestation
A sudden increase in proteinuria or blood pressure or
platelet count < 100,000/mm3 in women with
hypertension and proteinuria before 20 weeks'
gestation
SUPERIMPOSED PREECLAMPSIA
(ON CHRONIC HYPERTENSION)
-
7/27/2019 Hypertension Lecture for Cci 2013
8/74Hypertensive Disorders in Pregnancy
Case
38 y/o, G5, 12 weeks came in for first prenatal
check-up. BP of 180/110mmHg.
Urine protein +4
Diagnosis?
-
7/27/2019 Hypertension Lecture for Cci 2013
9/74Hypertensive Disorders in Pregnancy
-
7/27/2019 Hypertension Lecture for Cci 2013
10/74
Hypertensive Disorders in Pregnancy
-
7/27/2019 Hypertension Lecture for Cci 2013
11/74
Hypertensive Disorders in Pregnancy
Classification of Preeclampsia
-
7/27/2019 Hypertension Lecture for Cci 2013
12/74
Hypertensive Disorders in Pregnancy
Classification of Preeclampsia
Mi ld non-severe lesssevere
Severe= preeclampsia + 1 of aseries of complications
-
7/27/2019 Hypertension Lecture for Cci 2013
13/74
Hypertensive Disorders in Pregnancy
Criteria for the Diagnosis of Severe Preeclampsia
Symptoms of central nervoussystem dysfunction
Blurred vision, scotomata,
altered mental status, severeheadache
Symptoms of liver capsuledistention or rupture
Persistent right upper quadrant
and/ orepigastricpain
Symptoms
Norwitz. Expectant management of severe preeclampsia remote from
term. Am J Obstet Gynecol 2008 .
-
7/27/2019 Hypertension Lecture for Cci 2013
14/74
Hypertensive Disorders in Pregnancy
Criteria for the Diagnosis of Severe Preeclampsia
Blood pressure criteria 160/110
Eclampsia
Pulmonaryedema or cyanosis
Cerebrovascularaccident Cortical blindness
IUGR (EFW < 5thpercentile for age or< 10thpercentile with
evidence of
fetalcompromise
Signs
Norwitz. Expectant management of severe preeclampsia remote from
term. Am J Obstet Gynecol 2008 .
-
7/27/2019 Hypertension Lecture for Cci 2013
15/74
Hypertensive Disorders in Pregnancy
Criteria for the Diagnosis of Severe Preeclampsia
> 5 G per 24 hours or >/= 3+ on 2 random urinesamples that
are collected at least 4 hours apartProteinuria
Urine output < 500 mL per 24 hours and/ or serumcreatinine
> 1.2 mg/ dL
Oliguria and/or renal failure
Evidence ofhemolysis (abnormal peripheral smear,total bilirubin
>1.2 mg/ dL, LDH >600 U/L)
Elevated liver enzymes (ALT >70 U/L)
Low platelets (
-
7/27/2019 Hypertension Lecture for Cci 2013
16/74
Hypertensive Disorders in Pregnancy
Criteria for the Diagnosis of Severe Preeclampsia
Liver enzymes 2x normalHepatocellular
injury
< 100,000 platelet / mm3Thrombocytopenia
Prolonged PT Low platelet count
Low fibrinogen
Coagulopathy
Laboratory findings
Norwitz. Expectant management of severe preeclampsia remote from
term. Am J Obstet Gynecol 2008 .
-
7/27/2019 Hypertension Lecture for Cci 2013
17/74
Hypertensive Disorders in Pregnancy
Pathophysiology of hypertension in pregnancy
absent trophoblastic invasion of the uterine artery
vasospasm hepatic
ischemia
hepatic
infarction
hematoma
liver
rupture
endothelial damage
edema platelet
consumption
hemolysis
-
7/27/2019 Hypertension Lecture for Cci 2013
18/74
Hypertensive Disorders in Pregnancy
Pathophysiology
brain
liver
kidneys
Hematology CBC
- platelet count
Abruptio placenta
Pulmonary edema
-
7/27/2019 Hypertension Lecture for Cci 2013
19/74
Hypertensive Disorders in Pregnancy
WHAT IS THE DEFINITIVETREATMENT?
-
7/27/2019 Hypertension Lecture for Cci 2013
20/74
Hypertensive Disorders in Pregnancy
Delivery is the only
cure for preeclampsia
Cunningham, Leveno. Pregnancy Hypertension.
In: Williams Obstetrics, 23rd ed. 2010.
-
7/27/2019 Hypertension Lecture for Cci 2013
21/74
Hypertensive Disorders in Pregnancy
Main Objectives in the Management of Severe
Preeclampsia
Safety of the mother
Deliver a healthy infant
Forestall convulsion
Prevent intracranial hemorrhage
Avoid serious damage to vital organs
-
7/27/2019 Hypertension Lecture for Cci 2013
22/74
Hypertensive Disorders in Pregnancy
When is the woman with severe preeclampsia
delivered?
Pregnancies 34 weeks of gestation
complicated by severe preeclampsia isbest managed by delivery
after
maternal stabilization
Grade A
RCOG. The Management of Severe Preeclampsia. 2006
At 34 weeks
age of
gestation
short and long term neonatal
outcomes are excellent
fetal survival is already similar
to that of term gestation
pulmonary lung maturity is
achieved
Level I
-
7/27/2019 Hypertension Lecture for Cci 2013
23/74
Hypertensive Disorders in Pregnancy
SURVIVAL BY GESTATIONAL AGE
-
7/27/2019 Hypertension Lecture for Cci 2013
24/74
Hypertensive Disorders in Pregnancy
Acute Morbidity by Gestational Age
-
7/27/2019 Hypertension Lecture for Cci 2013
25/74
Hypertensive Disorders in Pregnancy
Chronic Morbidity by Gestational Age
-
7/27/2019 Hypertension Lecture for Cci 2013
26/74
Hypertensive Disorders in Pregnancy
Severe Preeclampsia Remote from Term
Although delivery is always appropriate
for the mother, it may not be optimal forthe premature fetus (
34 weeks )
Sarsam DS. Expectant versus Aggressive Management in Severe
Preeclampsia Remote from Term. Singapore Med J. 2008.
-
7/27/2019 Hypertension Lecture for Cci 2013
27/74
Hypertensive Disorders in Pregnancy
RDS
IVHNEC
SepsisDeath
Complications of Prematurity
-
7/27/2019 Hypertension Lecture for Cci 2013
28/74
Hypertensive Disorders in Pregnancy
20 y/o G1 at 30 weeks with a BP of 150/90 mmHg
was brought to the OPD because of bilateral pedal
edema. Urinalysis done outside revealed a +4
protein and platelet count of 95,000. What is the bestmanagement
for this case?
A. Admit, give MgS04, steroids, monitor BP
B. Admit, give MgS04,steroids then deliver
C. Admit, stabilize and deliver by CS
D. Admit for induction of labor then give
MgS04 postpartum
CASE
-
7/27/2019 Hypertension Lecture for Cci 2013
29/74
Hypertensive Disorders in Pregnancy
Sibai BM. Expectant Management of PreeclampsiaAJOG June 2007
An Algorithm in The Managementof Severe Preeclampsia
( < 34 weeks )
-
7/27/2019 Hypertension Lecture for Cci 2013
30/74
Hypertensive Disorders in Pregnancy
Admit to labor and delivery suite
Maternal-fetal evaluation for 24 hours
Magnesium sul fatefor 24 hours
Ant ihypertensivesif systolic blood pressure >160mmHg,
diastolic blood pressure > 110 mmHg, or mean
arterial pressure >125 mmHg
-
7/27/2019 Hypertension Lecture for Cci 2013
31/74
Hypertensive Disorders in Pregnancy
Magnesium sulfate in severe preeclampsia
Loading Dose: 4 grams IV5 grams IM / buttocks
Maitenance Dose: 1-2 grams / hour
-
7/27/2019 Hypertension Lecture for Cci 2013
32/74
Hypertensive Disorders in Pregnancy
Case
20 y/o primi 36 weeks came in with a BP of
160/110 mmHg. 5mg hydralazine was given and
repeat BP after 15 minutes revealed 170/100
mmHg. What meds at the ER will you give?
-
7/27/2019 Hypertension Lecture for Cci 2013
33/74
Hypertensive Disorders in Pregnancy
Case
30 y/o primi 32 weeks came in with a BP of
140/90 mmHg. She came from the lab with UA
result CHON (+1);
Ultrasound: SLIUP compatible with 28 weeks,
900 grams. Doppler of the UMA revealed
absent end flow.
Diagnosis?
What meds will you give?
-
7/27/2019 Hypertension Lecture for Cci 2013
34/74
Hypertensive Disorders in Pregnancy
Case
25 y/o primi 37 weeks came in with a BP of
140/90 mmHg. She went to the laboratory to
have her CBC done. After 6 hours she came
back with a BP of 150/90 mmHg.
Platelet count = 90,000.
Diagnosis?
What meds will you give?
-
7/27/2019 Hypertension Lecture for Cci 2013
35/74
Hypertensive Disorders in Pregnancy
Magnesium sulfate in severe preeclampsia
Loading Dose: 4 grams IV5 grams IM / buttocks
-
7/27/2019 Hypertension Lecture for Cci 2013
36/74
Hypertensive Disorders in Pregnancy
Magnesium sulfate in severe preeclampsia
Maintenance
Dose:
1-2 grams / hour
-
7/27/2019 Hypertension Lecture for Cci 2013
37/74
Hypertensive Disorders in Pregnancy
Questions:
Is magnesium sulphate an antihypertensive?
What are the 3 parameters to monitor when
giving the maintenance dose of MgS04?
What is the antidote for magnesium sulphate
toxicity?
Level of Magnesium resulting to toxicity
therapeutic dose 4-7 meq/L
loss of patellar
reflex
8-10 meq/L
respiratory
depression
12 meq/L
respiratory and
Cardiac Arrest
> 12 meq/L
Ad it t l b d d li it
-
7/27/2019 Hypertension Lecture for Cci 2013
38/74
Hypertensive Disorders in Pregnancy
Admit to labor and delivery suite
Maternal-fetal evaluation for 24 hours
Magnesium sul fatefor 24 hours
Ant ihypertensivesif systolic blood pressure >160mmHg,
diastolic blood pressure > 110 mmHg, or mean
arterial pressure >125 mmHg
-
7/27/2019 Hypertension Lecture for Cci 2013
39/74
Hypertensive Disorders in Pregnancy
When is antihypertensive therapy indicated?
Antihypertensive treatment should be started
in women with BP 160/110 mmHg. In a
woman with other markers of potentiallysevere disease, treatment
can be considered
at lower degrees of BP
Grade C
Report of the National High Blood Pressure Education Program
Working Group
on High Blood Pressure in Pregnancy. Am J Obstet Gynecol
2000
-
7/27/2019 Hypertension Lecture for Cci 2013
40/74
Hypertensive Disorders in Pregnancy
Anti-hypertensive meds during pregnancy
Blood Pressure 160/110 mmHg
Purpose: To prevent intracerebralhemorrhage
-
7/27/2019 Hypertension Lecture for Cci 2013
41/74
Hypertensive Disorders in Pregnancy
Anti-hypertensive meds during pregnancy
DRUG DOSE/ROUTE COMMENTS
LABETALOL 10-20 mg IV, then
20 -80 mg every 30
min; max of 300 mg
Not available locally
HYDRALAZINE 5 mg IV or IM then
5 mg every 15 min;
max of 20 mg
Long experience of
safety and efficacy;
drug of choice
NIFEDIPINE 10-30 mg PO then
10mg every 45 min;
max 50mg
Can be safely used
with MgS04
Update on the Use of Antihypertensive Drugs in Pregnancy. AHA,
2008
-
7/27/2019 Hypertension Lecture for Cci 2013
42/74
Hypertensive Disorders in Pregnancy
Anti-hypertensive meds during pregnancy
DRUG DOSE/ROUTE COMMENTS
IV NICARDIPINE D5W 90 mL + Nicardipine
10 mg in soluset
Concentration =
0.1 mg/ mL
Start drip at 10 ugtts/min
(equivalent to 1 mg/hr)
Titrate every hour
(increments of 1 mg/hr).Maximum dose 10 mg/hr
Note: The IV infusion site
must be changed every 12
hours
Can be safely
used with
MgS04
Update on the Use of Antihypertensive Drugs in Pregnancy. AHA,
2008
-
7/27/2019 Hypertension Lecture for Cci 2013
43/74
Hypertensive Disorders in Pregnancy
Anti-hypertensive meds during pregnancy
DRUG DOSE/ROUTE COMMENTS
METHYDOPA (B) Max of 3 grams per
day
Drug of choice
NIFEDIPINE 10 mg PO every 6hours; max of 120
mg / day
Slow or long actingpreparations may be
used; SL preparation
no longer
recommendedHYPRALAZINE 50 mg every 8
hours; max 300mg
per day
Long experience
with few adverse
effects
Update on the Use of Antihypertensive Drugs in Pregnancy. AHA,
2008
-
7/27/2019 Hypertension Lecture for Cci 2013
44/74
Hypertensive Disorders in Pregnancy
What blood pressure is the aim of anti-
hypertensive therapy?
The aim of anti-hypertensive therapy is to
keep the systolic BP between 140-155 anddiastolic BP between
90-100 mmHg.
Grade C
Report of the National High Blood Pressure Education Program
Working Group
on High Blood Pressure in Pregnancy. Am J Obstet Gynecol
2000
-
7/27/2019 Hypertension Lecture for Cci 2013
45/74
Hypertensive Disorders in Pregnancy
Reminders:
Diuretics are relatively contraindicated and
reserved only for pulmonary edema
Hyperosmotic agents (albumin) have the
potential to promote edema formation in
the lungs and brain
Admit to labor and delivery suite
-
7/27/2019 Hypertension Lecture for Cci 2013
46/74
Hypertensive Disorders in Pregnancy
y
Maternal-fetal evaluation for 24 hours
Magnesium sulfate for 24 hours
Antihypertensives if systolic blood pressure >160 mmHg,
diastolic blood pressure > 110 mmHg, or mean arterial
pressure >125 mmHg
Any of the following present?
EclampsiaPulmonary edema
Acu te renal failure
Dissem inated intravascu lar coagu lat ion
Suspected abruptio placenta
Non-reassuring fetal status
Labor or rupture of membranes >34 weeks gestation
Admit to labor and delivery suite
-
7/27/2019 Hypertension Lecture for Cci 2013
47/74
Hypertensive Disorders in Pregnancy
y
Maternal-fetal evaluation for 24 hours
Magnesium sulfate for 24 hours
Antihypertensives if systolic blood pressure >160 mmHg,
diastolic blood pressure > 110 mmHg, or mean arterial
pressure >125 mmHg
Magnesium sulfateand delivery
Any of the following present?
EclampsiaPulmonary edema
Acute renal failure
Disseminated intravascular coagulation
Suspected abruptio placenta
Non-reassuring fetal status
Labor or rupture of membranes >34 weeks
YES
Admit to labor and delivery suite
-
7/27/2019 Hypertension Lecture for Cci 2013
48/74
Hypertensive Disorders in Pregnancy
y
Maternal-fetal evaluation for 24 hours
Magnesium sulfate for 24 hours
Antihypertensives if systolic blood pressure >160 mmHg,
diastolic blood pressure > 110 mmHg, or mean arterial
pressure >125 mmHg
HELLP syndromePersistent symptoms
Magnesium sulfate
and delivery
Any of the following present?
Eclampsia
Pulmonary edema
Acute renal failure
Disseminated intravascular coagulationSuspected abruptio
placenta
Non-reassuring fetal status
Labor or rupture of membranes >34 weeks gestation
YES
NO
-
7/27/2019 Hypertension Lecture for Cci 2013
49/74
Hypertensive Disorders in Pregnancy
HELLP Syndrome
H hemolysis LDH > 600 U/Ltotal Bili > 1.2
mg/dL
abnormal PBS
EL elevated liverenzymes
SGPT > 70 U/L
LP low platelets
-
7/27/2019 Hypertension Lecture for Cci 2013
50/74
Hypertensive Disorders in Pregnancy
Maternal-fetal evaluation for 24 hours
Magnesium sulfate for 24 hours
Antihypertensives if systolic blood pressure >160 mmHg,
diastolic blood pressure > 110 mmHg, or mean arterial
pressure >125 mmHg
HELLP syndrome
Persistent symptomsSteroids
Magnesium sulfateand delivery
Any of the following present?
Eclampsia
Pulmonary edema
Acute renal failureDisseminated intravascular coagulation
Suspected abruptio placenta
Non-reassuring fetal status
Labor or rupture of membranes >34 weeks gestation
YES
NO
YES
ANTENATAL CORTICOSTEROIDS
-
7/27/2019 Hypertension Lecture for Cci 2013
51/74
Hypertensive Disorders in Pregnancy
ANTENATAL CORTICOSTEROIDS
12 mg IM q 24 hours x 2 dosesBetamethasone
6 mg IM q 12 hours x 4 dosesDexamethasone
REDUCES
RDS
IVH
NEC
Perinatal death
Long term neurological problem
Admit to labor and delivery suite
Maternal fetal evaluation for 24 hours
-
7/27/2019 Hypertension Lecture for Cci 2013
52/74
Hypertensive Disorders in Pregnancy
Maternal-fetal evaluation for 24 hours
Magnesium sulfate for 24 hours
Antihypertensives if systolic blood pressure >160 mmHg,
diastolic blood pressure > 110 mmHg, or mean
arterial pressure >125 mmHg
HELLP syndrome (Hemolysis, Elevated Liver enzymes, and Low
Platelets)
Persistent symptoms Steroids
Magnesium sulfate and delivery
Any of the following present?
Eclampsia
Pulmonary edema
Acute renal failureDisseminated intravascular coagulation
Suspected abruptio placentaNon-reassuring fetal status
Labor or rupture of membranes >34 weeks gestation
YES
YES
NO
< 24 weeks 2432 weeks 33 34 weeks
Steroids
Delivery 24 hours
after completion of
steroids
MgSO4 for 24 hou rs
Antihypertensivesif needed
SteroidsDaily evaluationof maternal-
fetal condition
Delivery if with indications
Delivery at 33-34 weeks
NO
-
7/27/2019 Hypertension Lecture for Cci 2013
53/74
Hypertensive Disorders in Pregnancy
Magnesium sulfate during expectant
management
Loading Dose: 4 grams IV5 grams IM / buttocks
Maintenance
Dose:
1-2 grams / hour
given for 24 hours
once a delivery decision is made and
continued for 24 hours postpartum
Admit to labor and delivery suite
Maternal-fetal evaluation for 24 hours
-
7/27/2019 Hypertension Lecture for Cci 2013
54/74
Hypertensive Disorders in Pregnancy
Maternal-fetal evaluation for 24 hours
Magnesium sulfate for 24 hours
Antihypertensives if systolic blood pressure >160 mmHg,
diastolic blood pressure > 110 mmHg, or mean
arterial pressure >125 mmHg
HELLP syndrome (Hemolysis, Elevated Liver enzymes, and Low
Platelets)
Persistent symptoms Steroids
Magnesium sulfate and delivery
Any of the following present?
Eclampsia
Pulmonary edema
Acute renal failureDisseminated intravascular coagulation
Suspected abruptio placentaNon-reassuring fetal status
Labor or rupture of membranes >34 weeks gestation
YES
YES
NO
< 24 weeks 2432 weeks 33 34 weeks
Steroids
Delivery after 48 hours
MgSO4 for 24 hou rs
Ant ihyper tensivesi f needed
SteroidsDaily evaluationof m aternal-fetal cond it ion
Del ivery i f wi th indicat ions
Delivery at 33-34 weeks
Admit to labor and delivery suite
Maternal-fetal evaluation for 24 hours
-
7/27/2019 Hypertension Lecture for Cci 2013
55/74
Hypertensive Disorders in Pregnancy
Maternal fetal evaluation for 24 hours
Magnesium sulfate for 24 hours
Antihypertensives if systolic blood pressure >160 mmHg,
diastolic blood pressure > 110 mmHg, or mean
arterial pressure >125 mmHg
HELLP syndrome (Hemolysis, Elevated Liver enzymes, and Low
Platelets)
Persistent symptoms Steroids
Magnesium sulfate and delivery
Any of the following present?
Eclampsia
Pulmonary edema
Acute renal failureDisseminated intravascular coagulation
Suspected abruptio placentaNon-reassuring fetal status
Labor or rupture of membranes >34 weeks gestation
YES
YES
NO
< 24 weeks 2432 weeks 33 34 weeks
Steroids
Delivery after 48 hours
MgSO4 for 24 hours
Ant ihyper tensivesi f needed
SteroidsDaily evaluationof maternal-fetal
condi t ion
Delivery i f with ind icat ions
Delivery at 33-34 weeks
-
7/27/2019 Hypertension Lecture for Cci 2013
56/74
Hypertensive Disorders in Pregnancy
Maternal Evaluation
weigh patient daily
BP monitoring q 4 hours except between 12mn
and 6am
Labs:
CBC with platelet count Urinalysis
Creatinine 24 hour urine albumin
SGPT, SGOT LDH, PBS, Total bilirubin
-
7/27/2019 Hypertension Lecture for Cci 2013
57/74
Hypertensive Disorders in Pregnancy
Fetal Evaluation
Baseline CTG
Women in labor should havecontinuous EFM
Biometry q 2 weeks, BPS 2x / week,doppler weekly and daily
NST
Grade B
Grade B
Grade A
Admit to labor and delivery suite
Maternal-fetal evaluation for 24 hours
-
7/27/2019 Hypertension Lecture for Cci 2013
58/74
Hypertensive Disorders in Pregnancy
Magnesium sulfate for 24 hours
Antihypertensives if systolic blood pressure >160 mmHg,
diastolic blood pressure > 110 mmHg, or mean
arterial pressure >125 mmHg
HELLP syndrome (Hemolysis, Elevated Liver enzymes, and Low
Platelets)
Persistent symptoms Steroids
Magnesium sulfate and delivery
Any of the following present?
Eclampsia
Pulmonary edema
Acute renal failureDisseminated intravascular coagulation
Suspected abruptio placentaNon-reassuring fetal status
Labor or rupture of membranes >34 weeks gestation
YES
YES
NO
< 24 weeks 2432 weeks 33 34 weeks
Steroids
Delivery after 48 hoursMgSO4 for 24 hours
Ant ihyper tensivesi f needed
Steroids
Daily evaluationof maternal-fetal co ndit io n
Delivery i f with indicat ion s
Delivery at 33-34 weeks
Indications for Delivery (24 32 weeks)
-
7/27/2019 Hypertension Lecture for Cci 2013
59/74
Hypertensive Disorders in Pregnancy
Indications for Delivery (24-32 weeks)
Variable Indication
Maternal Persistent severe headache or visual changes;
eclampsia
Pulmonary edema
Epigastric/RUQ pain with AST or ALT > 2 times the upper
limits of normal
Uncontrolled severe hypertension, despite maximum doses of
antihypertensive agents
Oliguria (
-
7/27/2019 Hypertension Lecture for Cci 2013
60/74
Hypertensive Disorders in Pregnancy
Indications for Delivery
Variable Indication
Fetal Severe FGR (EFW < 5th percentile for gestational
age)
Persistent severe oligohydramnios (AFI
-
7/27/2019 Hypertension Lecture for Cci 2013
61/74
Hypertensive Disorders in Pregnancy
What is the mode of delivery?
The mode of delivery should be determined
after considering the presentation of the fetus
and the fetal condition, together with thelikelihood of success
of induction of labor
after assessment of the cervix
Grade C
RCOG. The Management of severe preeclampsia. Evidence Based
Clinical
Guideline No. 10, 2006
How is postpartum hypertension
-
7/27/2019 Hypertension Lecture for Cci 2013
62/74
Hypertensive Disorders in Pregnancy
How is postpartum hypertension
managed?
Anti-hypertensives for BP 150/100 mmHg
Anti-hypertensive agents
Diuretics
Avoid NSAIDs
Grade C
Grade C
Grade C
Grade A
Admit to labor and delivery suite
Maternal-fetal evaluation for 24 hours
M i lf t f 24 h
-
7/27/2019 Hypertension Lecture for Cci 2013
63/74
Hypertensive Disorders in Pregnancy
Magnesium sulfate for 24 hours
Antihypertensives if systolic blood pressure >160 mmHg,
diastolic blood pressure > 110 mmHg, or mean
arterial pressure >125 mmHg
HELLP syndrome (Hemolysis, Elevated Liver enzymes, and Low
Platelets)
Persistent symptoms Steroids
Magnesium sulfate and delivery
Any of the following present?
Eclampsia
Pulmonary edema
Acute renal failure
Disseminated intravascular coagulation
Suspected abruptio placentaNon-reassuring fetal status
Labor or rupture of membranes >34 weeks gestation
YES
YES
NO
< 24 weeks 2432 weeks 33 34 weeks
Steroids
Delivery after 48 hours
MgSO4 for 24 hours
Antihypertensivesif needed
SteroidsDaily evaluationof
maternal-fetal condition
Delivery if with indications
Delivery at 33-34 weeks
Terminate
pregnancy
Severe Preeclampsia < 24 weeks
-
7/27/2019 Hypertension Lecture for Cci 2013
64/74
Hypertensive Disorders in Pregnancy
Severe Preeclampsia < 24 weeks
High maternal morbidity
High perinatal morbidity and
mortality
Pregnancy termination is
recommended
Bombrys AE. Expectant Management of Severe Preeclampsia at less
than
27 week gestation. Am J Obstet Gynecol, 2008.
Admit to labor and delivery suite
Maternal-fetal evaluation for 24 hours
Magnesium sulfate for 24 hours
-
7/27/2019 Hypertension Lecture for Cci 2013
65/74
Hypertensive Disorders in Pregnancy
Magnesium sulfate for 24 hours
Antihypertensives if systolic blood pressure >160 mmHg,
diastolic blood pressure > 110 mmHg, or mean
arterial pressure >125 mmHg
HELLP syndrome (Hemolysis, Elevated Liver enzymes, and Low
Platelets)
Persistent symptoms Steroids
Magnesium sulfate and delivery
Any of the following present?
Eclampsia
Pulmonary edema
Acute renal failure
Disseminated intravascular coagulation
Suspected abruptio placentaNon-reassuring fetal status
Labor or rupture of membranes >34 weeks gestation
YES
YES
NO
< 24 weeks 2432 weeks 33 34 weeks
Steroids
Delivery after 48 hours
MgSO4 for 24 hours
Antihypertensivesif needed
SteroidsDaily evaluationof
maternal-fetal condition
Delivery if with indications
Delivery at 33-34 weeks
Terminate
pregnancy
CASE
-
7/27/2019 Hypertension Lecture for Cci 2013
66/74
Hypertensive Disorders in Pregnancy
20 y/o G1 at 30 weeks with a BP of 150/90 mmHg
was brought to the OPD because of bilateral pedaledema.
Urinalysis done outside revealed a +4
protein and platelet count of 95,000. What is the bestmanagement
for this case?
A. Admit, give MgS04, steroids, monitor BP
B. Admit, give MgS04,steroids then deliver
C. Admit, stabilize and deliver by CS
D. Admit for induction of labor then give
MgS04 postpartum
CASE
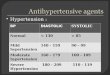
Regarding management how does
-
7/27/2019 Hypertension Lecture for Cci 2013
67/74
Hypertensive Disorders in Pregnancy
Regarding management, how does
severe preeclampsia differ from mild
preeclampsia and gestationalhypertension?
A. Giving of MgS04
B. AOG of delivery
C. Giving of antihypertensive
GH and Mild
Preeclampsia
Severe
Preeclampsia
MgS04
AOG at
delivery
37 weeks 34 weeks
Anti-HPN 160/110 mmHg 160/110 mmHg
CASE
-
7/27/2019 Hypertension Lecture for Cci 2013
68/74
Hypertensive Disorders in Pregnancy
G1, 37 weeks, BP = 160/110 mmHg. Urine dipstick (-) protein.
How will you manage the patient?
A. Give MgS04, antihypertensive and do
antenatal fetal surveillance
B. Give antihpn and proceed with induction of
labor
C. Give antihpn and send home once stableD. Give MgS04,
antihypertensive and proceed
with induction of labor
CASE
CASE
-
7/27/2019 Hypertension Lecture for Cci 2013
69/74
Hypertensive Disorders in Pregnancy
35 y/o G5P4 (4004), 28 weeks AOG, was brought
to the ER due to tonic clonic convulsion.
BP = 180/110 mmHg. Stat urine protein is +3. What is thebest
management?
A. Give MgS04, steroids and antihpnB. Give MgS04, steroids and
deliver by
induction of labor
C. Give MgS04, stabilize and deliver by CSD. Give MgS04,
steroid, antihpn and do
conservative management
CASE
21 y/o G1 38 weeks diagnosed with severe
-
7/27/2019 Hypertension Lecture for Cci 2013
70/74
Hypertensive Disorders in Pregnancy
21 y/o G1, 38 weeks, diagnosed with severe
preeclampsia underwent induction of labor under
continuous EFM. CTG suddenly revealed this
IE: cephalic, fully dilated, station +5 trace. IEdone: fully
dilated, cephalic, station +3. Management?
A. Proceed with CS
B. Await deliveryC. Do forceps
D. Resuscitate
-
7/27/2019 Hypertension Lecture for Cci 2013
71/74
Hypertensive Disorders in Pregnancy
16 y/o G1, no PNCU, 1st consult at the OPD.
AOG by LMP: 34 weeks. BP = 140/90 mmHg.
FH: 24 cm, FHT: 140s. What is the best courseof management?
A. Request for biometry and doppler studiesB. Monitor bp, give
methyldopa as home meds
C. Give MgS04 and antihpn
D. Admit for induction of labor
-
7/27/2019 Hypertension Lecture for Cci 2013
72/74
Hypertensive Disorders in Pregnancy
25 y/o G2, with severe preeclampsia is undergoing
induction of labor. IE: 4cm. Baseline CTG revealed
What statement/s is/are WRONG?
A. Intermittent auscultation every 15
minutes is acceptable
B. Continuous CTG is done
C. Hook to O2 and put to left lateral
decubitus position
D. All of the above
-
7/27/2019 Hypertension Lecture for Cci 2013
73/74
Hypertensive Disorders in Pregnancy
-
7/27/2019 Hypertension Lecture for Cci 2013
74/74
The End