Embed Size (px)
DESCRIPTION
hypertension
Citation preview

SYSTEMIC HYPERTENSIONRATIONAL MANAGEMENT IN GENERAL PRACTICEDr Anidu PathiranaMBBS(Col.) MD(Col.) MRCP(UK)

SOME DIFFICULTIES GP’S HAVE WITH HYPERTENSION
MANAGEMENT When to inform a patient as hypertensive
When to refer to a Specialist
How to control high BP to the target
How to convince & persuade a patient to take medication (often several) lifelong, for an asymptomatic condition and where drugs may have significant side effects.

TAKE HOME MESSAGES Measure BP accurately and record Take adequate time to diagnose
hypertension Decide BP target, try to hit it, tell
target to patient Use low cost, tolerated drugs in
effective combination Address CV risk reduction, decide on
LDL, HbA1c targets and try to hit Convince the patient for follow up

SYSTEMIC HYPERTENSION DEFINITION
Blood pressure elevation Systolic above 139 mmHg
and/or Diastolic above 89 mmHg
on repeated measurements in adults >18y
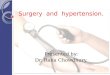
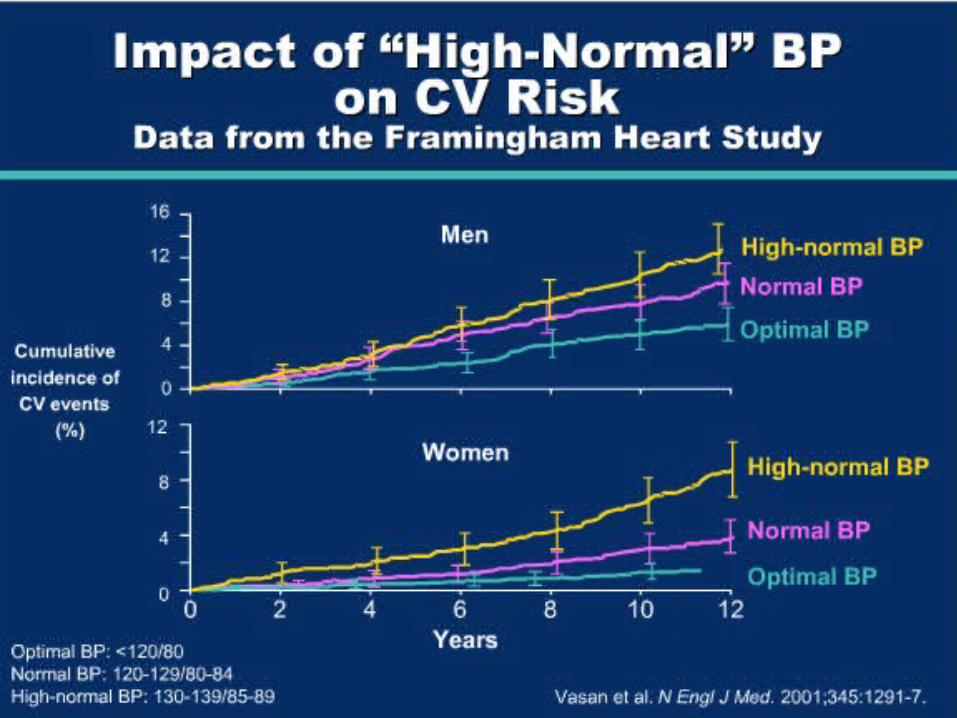
‘NORMAL’ DISTRIBUTION OF DIASTOLIC BP WITHIN A POPULATION
0
5
10
15
20
50 60 70 80 90 100 110 120 130
Diastolic BP, mmHg
% o
f sc
reen
ed p
opul
atio
n

HYPERTENSION: A PRACTICAL DEFINITION
That level of blood pressure at which investigation and
treatment do less harm than good

HYPERTENSION IS COMMON
Prevalence 25% adult populations
Normotensive at 55 year has a 90% lifetime risk of developing hypertension

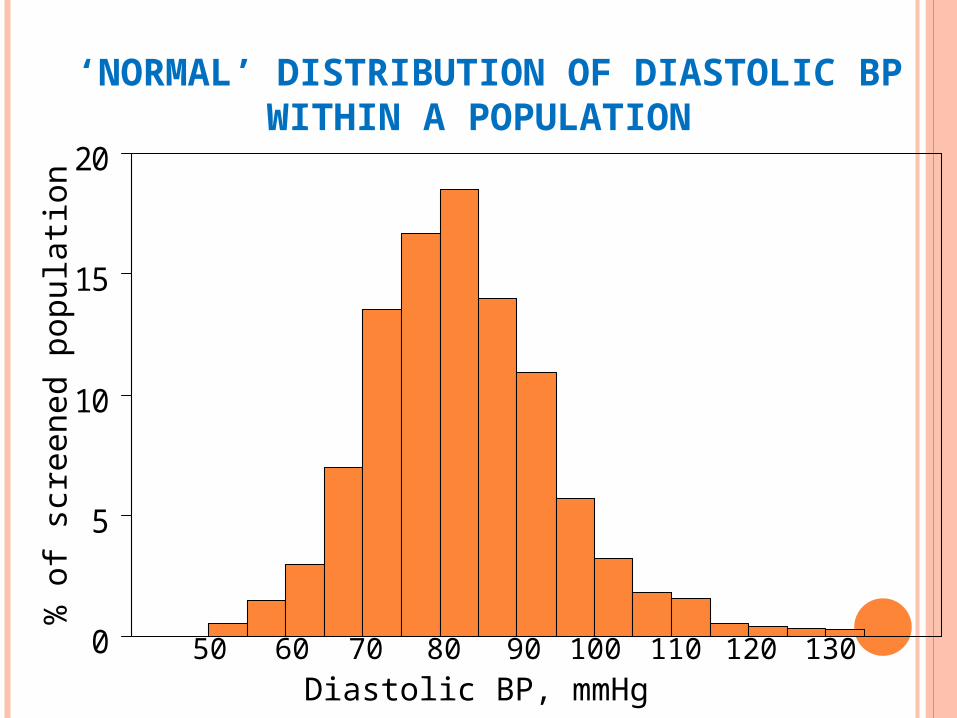
HYPERTENSION IS SERIOUS
Global mortality 2000Health risk factors

HYPERTENSION IS SERIOUS
Untreated hypertension reduces life expectancy by 5 years
Hypertension is responsible for - 25% of all premature deaths - 25% of all CAD deaths - 50% of all stroke deaths - 50% of all Congestive Heart
Failure - Commonest cause of CKD overall
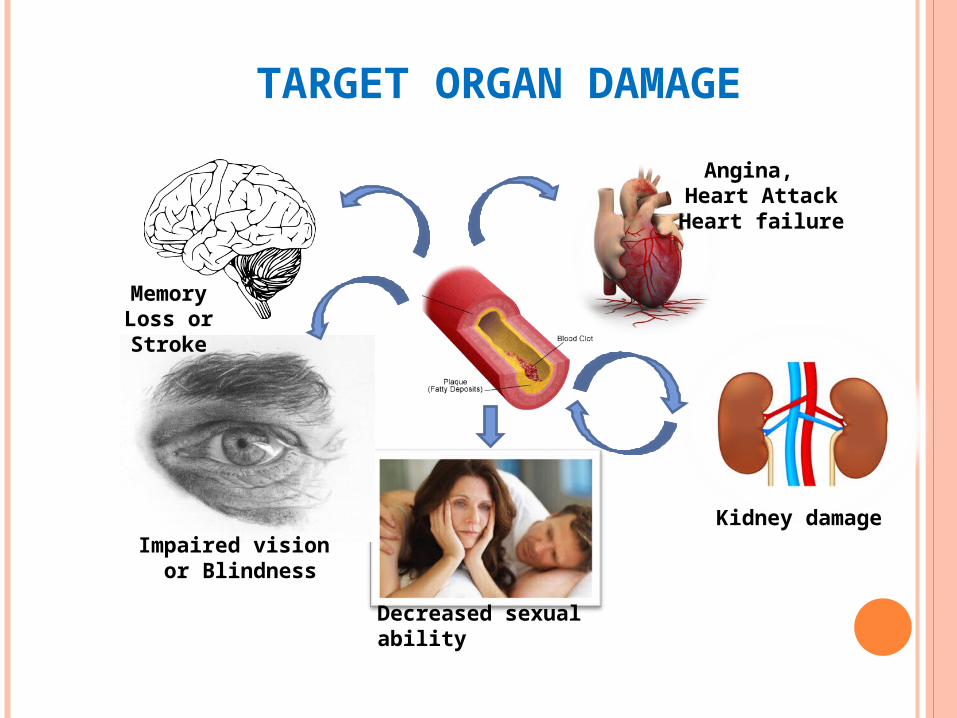
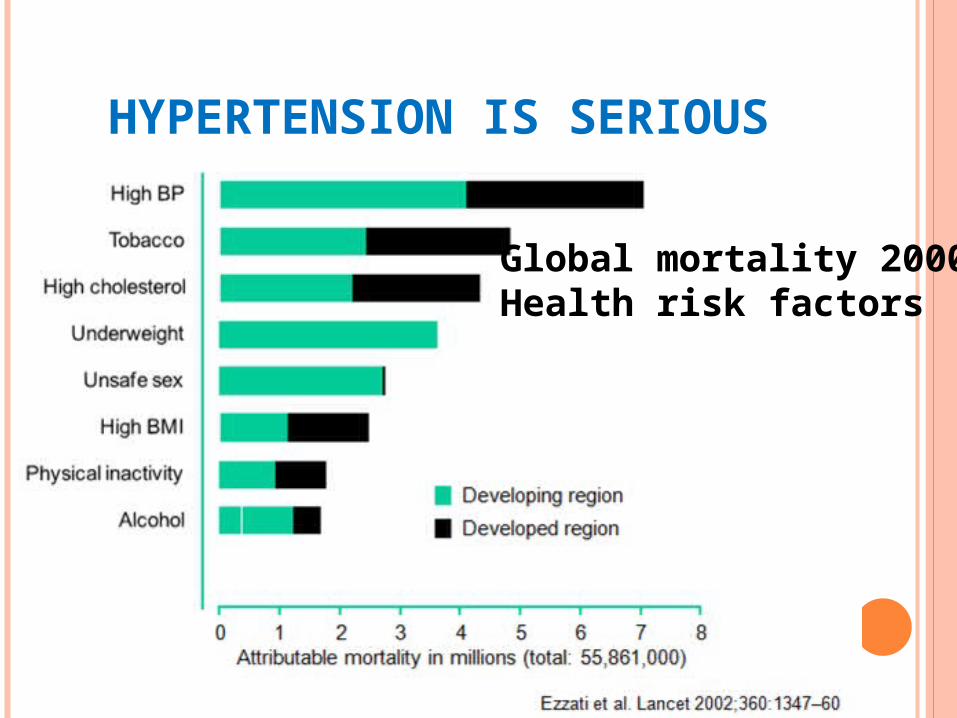
TARGET ORGAN DAMAGE
Memory Loss or Stroke
Angina, Heart AttackHeart failure
Kidney damageImpaired vision
or Blindness
Decreased sexual ability

TREATMENT IS EFFECTIVE

HYPERTENSION IS TREATABLE
Antihypertensive drug therapy (almost) always
Lifestyle changes Assist in hypertension control and
reduce number of drugs

2 mm Hg decrease in mean SBP
7% reduction in risk of ischemic heart disease mortality
10% reduction in risk of stroke mortality
SBP REDUCTIONS AS LITTLE 2 MMHG REDUCES CV RISK BY 10%

140/90 mmHg


GOAL IS TO HIT THE TARGET High risk < 130 and 80
mmHg (CVD,CKD,DM) Others < 140 and 90
mmHg
>80y < 150 and 90 mmHg
Patients should know their starting BP & Goal BP

Hypertension is mostly asymptomatic
Need for opportunistic screening
CASE HISTORY
A 38y old man BP 154/96 mmHg
WHAT TO DO
Diagnostic pathway
Treatment pathway

IMPORTANT QUESTIONS
When should I tell him as having Hypertension?
Can I manage him or should I refer him to a Specialist?
When should I start him on drugs?
What are the best drugs?
When should I see him next?

ACCURATE BLOOD PRESSURE MEASUREMENT
Equipment should be regularly inspected and validated.
Operator should be trained and regularly retrained.
Patient must be properly prepared

TECHNIQUES OF BP MEASUREMENT
Clinic measurements (doctor or nurse)
Home BP measurement (patient)
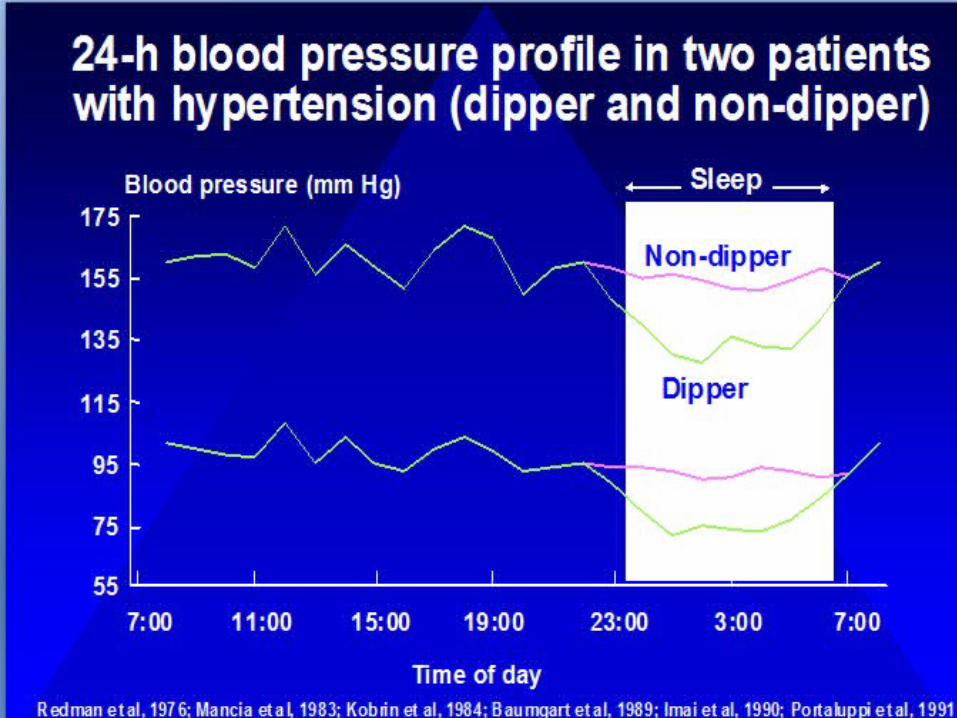
24h ambulatory BP measurement (automatically)

TYPES OF B P MONITORS
Mercury sphygmomanometers
Android ( Mercury-free)
Automated upper arm devices

What size cuff?
Size does matter
Using too small a cuff/bladdercan overestimate the blood pressureBladder should encircle arm by 80-100%
5

Too tight clothing
If the sleeves are too tight or bulky they act as a tourniquet giving inaccurate readings
6
MYTH:The position of the arm is immaterialDuring BP measurement?
FACT:
The arm should be well supported at HEART level (both sitting & standing)
An unsupported arm is performing isometric exercise thus raising BP
4
MYTH:Mercury sphygmomanometer shouldbe positioned level with the patients heart?
It should be level with eye
9

At what rate should the cuff be deflated
on a Mercury sphygmomanometer?
FACT:
2mm/Hg per second
FACT: BP should be recorded to
the nearest 2mm/Hg on
mercury sphygmomanometer
RULES FOR MEASUREMENT
Seated for 5 min in a quite place No exercise, smoking, caffeine within 30 min. Measure in both arms on first visit. If
difference >20 mmHg repeat measurements in both arms. If remains so measure subsequent BP in arm with higher reading.
If BP >140/90: Take a second reading during same consultation. At least 1-2 min. apart. If it differs > 20 take a third measurement. Record lower of the last two measurement as the clinic BP

Care Pathway

FOLLOW-UP BASED ON INITIAL BPMEASUREMENTS FOR ADULTS
Initial B P value Follow-up recommendation
Normal <130/85 Re check in2 years
Pre hypertension or high normal130-139/85-89
Re check in 1 years
140-159/90-99 Confirm within 2 months
160-179/100-109 Confirm within 1 month
>180/110 Evaluate & treat immediately or within 1 week

HypertensiveUrgency /
Emergency
HypertensiveUrgency /
Emergency
Diagnosisof HTN
Diagnosisof HTN
Elevated Out of the Clinic BP
measurement
Elevated Out of the Clinic BP
measurement
Elevated Random Clinic BP
Measurement
Elevated Random Clinic BP
Measurement
Hypertension Visit 1BP Measurement,
History and Physical examination
Hypertension Visit 1BP Measurement,
History and Physical examination
Diagnostic tests orderingat visit 1 or 2
Diagnostic tests orderingat visit 1 or 2
Visit 1

Urgent referral for urgent treatment
• Impending complications (e.g. TIA, LVF, angina)
• Particularly severe hypertension (>220/120mmHg)
• Accelerated hypertension (severe hypertension and grade III-IV retinopathy)

HISTORY&
EXAMINATION
Hypertension risk factorsWeight
Family historySalt, Alcohol, Stress, Sleep
Target organ damageHeart: angina,MI,HF
Brain: TIAEyes
Kidneys
Clues to 2o HTSymptoms
Drugs:OCP,NSAIDSSigns
Other CV risk factorsLipids
SmokingDiabetesExercise
Concurrent conditionsAsthma
GoutPregnancy

INVESTIGATIONS Urinalysisprotein,blood,microalbuminuri
a
ECGFBSFasting lipidsSerum creatinine & e-GFRSerum electrolyteHb%, PCVTSH, Ionized calciumSerum uric acid

ASYMPTOMATIC TARGET ORGAN DAMAGE
ECG & Echo evidence of LVH CKD with eGFR <60 ml/min/1.76 m2
BSA Microalbuminuria- 30 mg/ g
creatinine or 30-300 mg/24h Pulse pressure >60 mmHg in elderly Increased pulse wave velocity carotid-
femoral Carotid IMT or plaque Ankle brachial index < 0.9
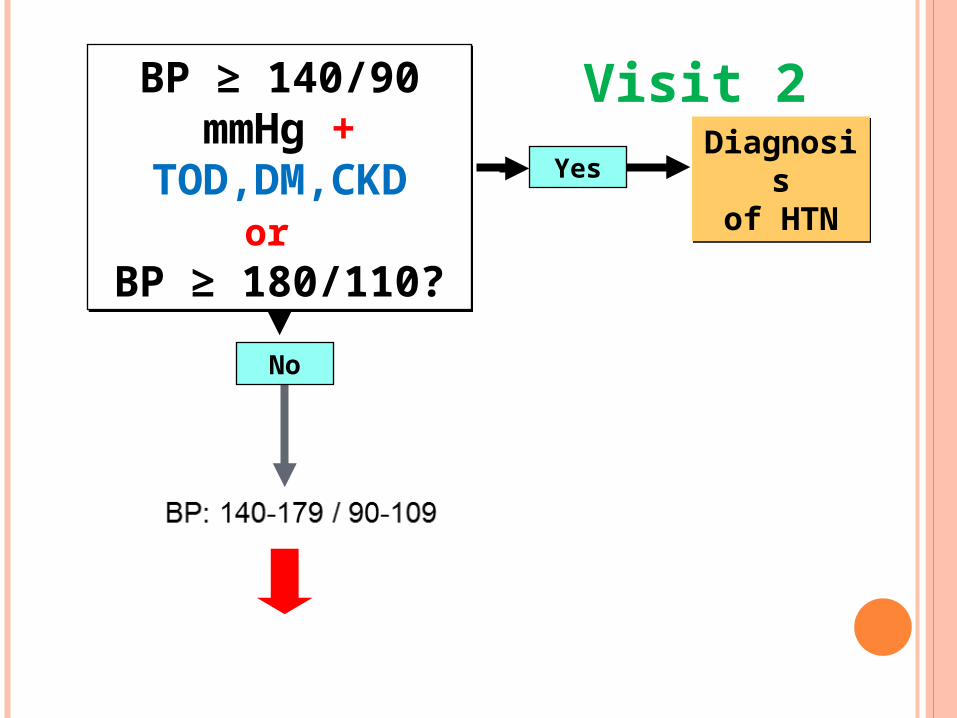
Yes
BP ≥ 140/90 mmHg +
TOD,DM,CKDor
BP ≥ 180/110?
BP ≥ 140/90 mmHg +
TOD,DM,CKDor
BP ≥ 180/110?
Diagnosisof HTN
Diagnosisof HTN
No
Visit 2

DIAGNOSTIC ALGORITHM CONT.
BP: 140-179 / 90-109BP: 140-179 / 90-109
ABPM (If available)ABPM (If available)Clinic BPClinic BP HBPM HBPM
Diagnosisof HTN
Awake BP≥ 135 SBP or
≥ 85 DBPOr 24-hour
≥ 130 SBP or≥ 80 DBP
Awake BP≥ 135 SBP or
≥ 85 DBPOr 24-hour
≥ 130 SBP or≥ 80 DBP
Awake BP< 135/85 and
24-hour< 130/80
Awake BP< 135/85 and
24-hour< 130/80
Continue to follow-up
Diagnosisof HTN
Hypertension visit 3
≥ 160 SBP or ≥ 100 DBP
≥ 140 SBP or≥ 90 DBP
< 140 / 90
Diagnosisof HTN
Continue to follow-up
< 160 / 100
Hypertension visit 4-5
ABPM or HBPMor
≥ 135 SBP or ≥ DBP 85
≥ 135 SBP or ≥ DBP 85
< 135/85 < 135/85
Diagnosisof HTN
Continue to follow-up
or

DEFINITION BY OFFICE & OUT-OF-OFFICE B P LEVELS

HOME/SELF BP MONITORING
Advise patients on accurate, independently validated, well maintained monitors
Advise use of appropriate cuff sizeSuggested measurement routine for patients Two consecutive measurements 1 min apart, seated Measure BP for 7 days prior to appointment Record BP twice a day. Morning and evening Discard first 24 hours of readings Take an average of at least 12 of these readings

Indications for ABPM
24 hour BP monitoring (ABPM)
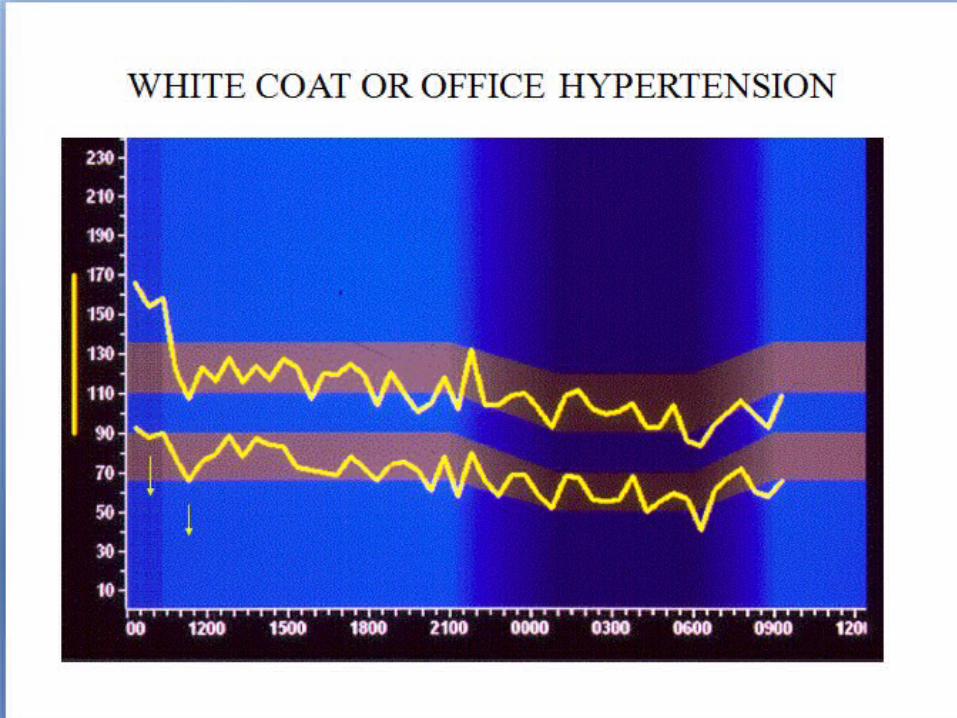
• Possible ‘white coat’ hypertension
• Informing equivocal decisions
• Determining efficacy of drug treatment over 24 hours
• Evaluation of symptomatic hypotension
• Unusual BP variability
• Evaluation of drug resistant hypertension



THE CONCEPT OF MASKED / WHITE COAT HYPERTENSION
From Pickering, Hypertension 1992
Clinic SBP mmHg
Hom
e o
r dayti
me A
BPM
SB
P
mm
Hg
Truehypertensive
TrueNormotensive White Coat HTN
Masked HTN
135
140
135
140
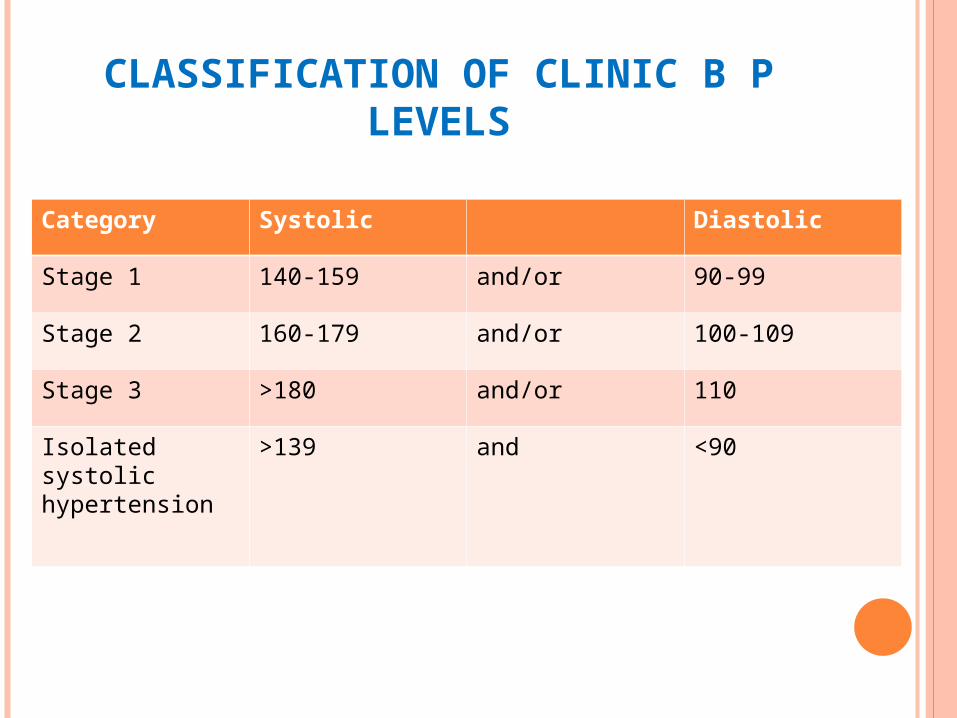
CLASSIFICATION OF CLINIC B P LEVELS
Category Systolic Diastolic
Stage 1 140-159 and/or 90-99
Stage 2 160-179 and/or 100-109
Stage 3 >180 and/or 110
Isolated systolic hypertension
>139 and <90

WAYS TO LOWER “PRESSURE”

• Get 30 to 60 minutes of exercise per day
• Eat a healthy diet: fresh fruits & vegetables, low-fat dairy, whole grains, low-fat meat, fish, poultry
• Stop smoking forever
LIFE STYLE MEASURES TO ALL
Physically Active
Eat Healthy
Smoke-Free
• If you are overweight, losing 10 lbs (5 Kg) will reduce high blood pressure

LIFE STYLE MEASURES TO ALL
• Reduce stress• You can control your blood pressure:
• If you are on medications: take them as directed by your doctor
• Limit alcohol to less than 2 drinks a day for men and approximately 1 drink a day for women
Less Salt
Less Stress
Medications
Less Alcohol
• Processed and restaurant foods contain high amounts of salt
• Hidden Salt
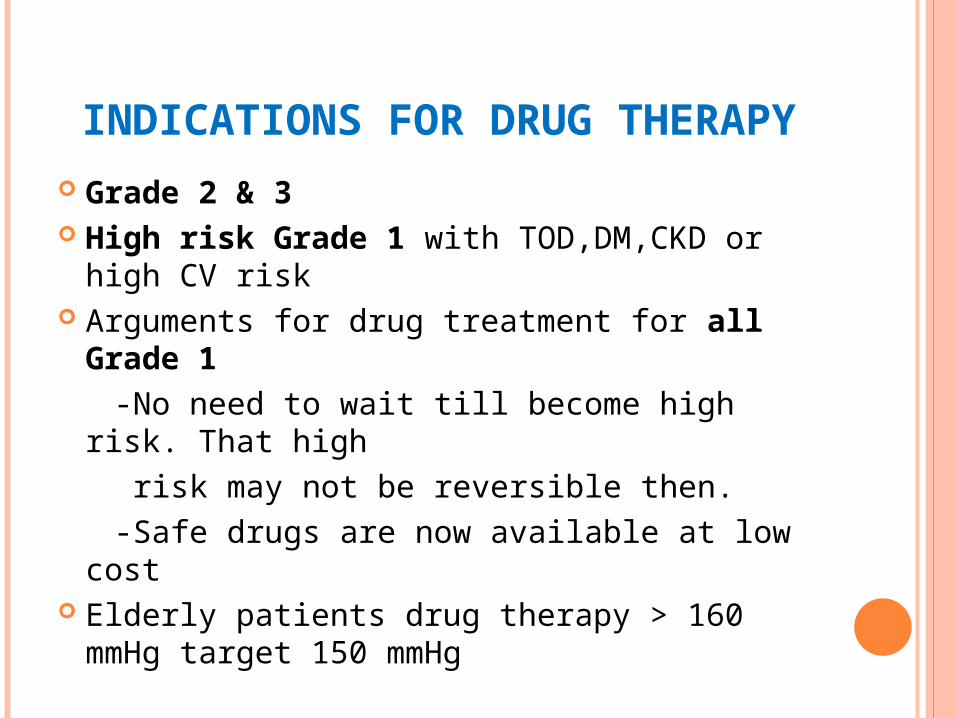
INDICATIONS FOR DRUG THERAPY
Grade 2 & 3 High risk Grade 1 with TOD,DM,CKD or
high CV risk Arguments for drug treatment for all Grade
1 -No need to wait till become high risk. That
high risk may not be reversible then. -Safe drugs are now available at low cost Elderly patients drug therapy > 160 mmHg
target 150 mmHg
RISK FACTORS
Male sex Age >55 y in male, >65 y in female Smoking Dyslipidemia ( total >190 mg/dl, LDL >115,
HDL <40 in male & <46 in female, TG >150) FBS 102-125 mg/dl or abnormal IGT BMI > 30, Abdominal obesity > 90 cm in
male & > 80 cm in female Family history of premature CV disease <55
y in male, <65 y in female

INITIATION OF LIFE STYLE CHANGES & DRUGS

DRUG THERAPYEffective: Proven in trials
Tolerance: Minimal side effects
Cost: LowFour main classes: ACEI/ARA, BB, CCB, Diuretics

TAILORED THERAPY
Compelling indications
Compelling contra indications


MOST PATIENTS NEED COMBINATION OF DRUGS TO
ACHIEVE TARGET
On average each medication will reduce blood pressure 10/5 (“Rule of 10/5”)
Stage1: start ONE drugStage2: start COMBINATION of two
Even in stage 1 hypertension two classes of drugs needed to BP goals
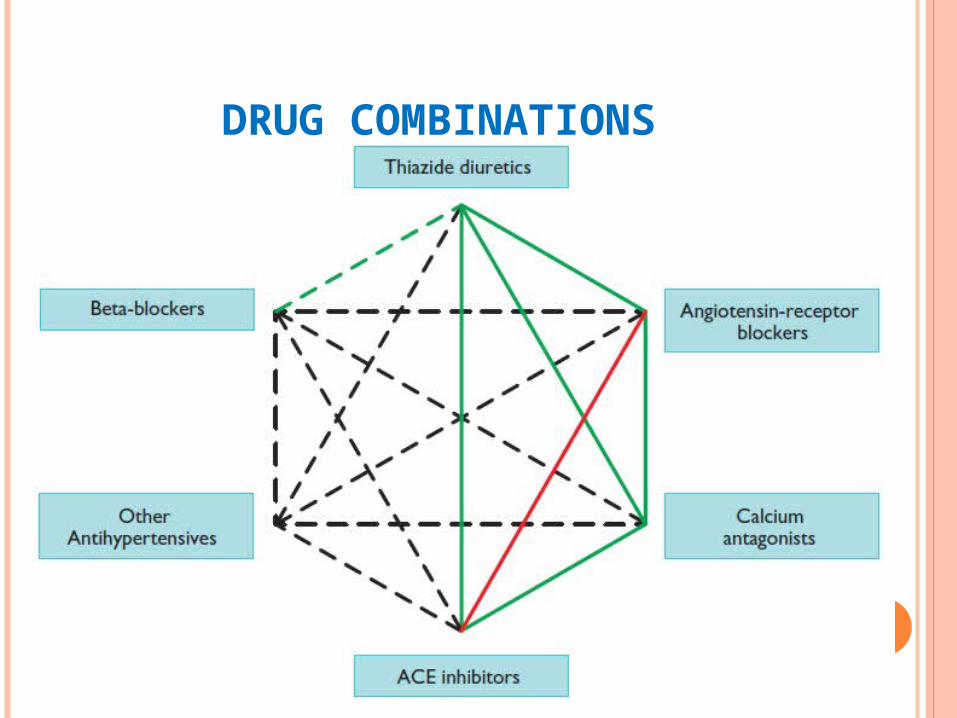
DRUG COMBINATIONS

GENERAL PRINCIPLE DRUG THERAPY
Low dose and titrate up Long acting drugs 24h efficacy with
once a day dosing at least 50% drug effect remaining at the end of 24h
Each medication may require 2-3 dose adjustments
Recommended interval between adjustments (new or dose increase) is 2 weeks
Usually one adjustment per visit

STEP-UP
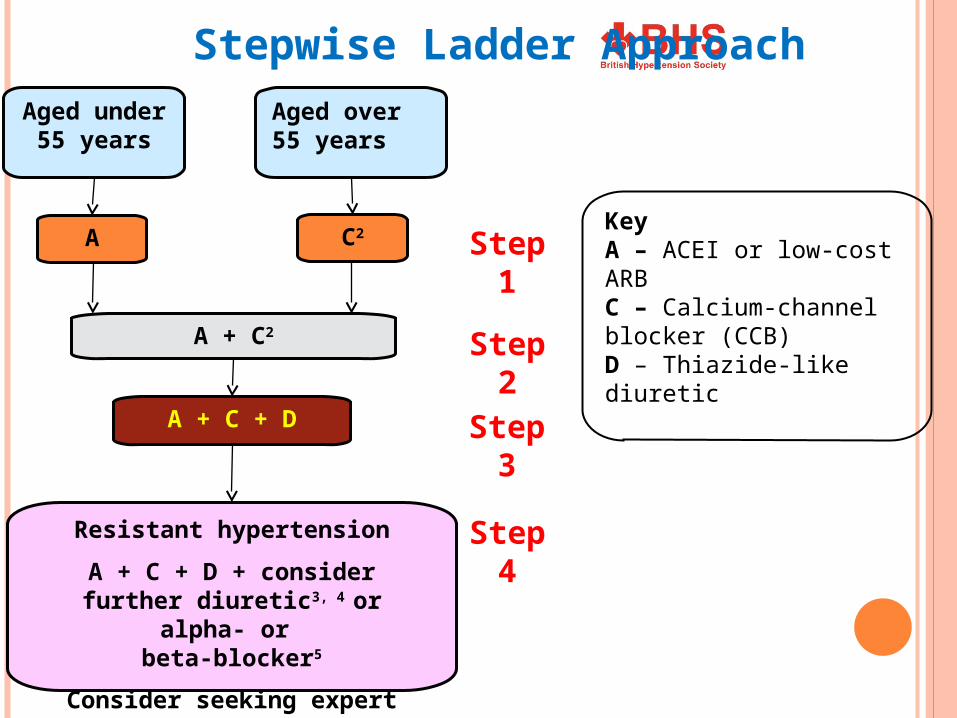
Step 4
Aged over 55 years
Aged under
55 years
C2A
A + C2
A + C + D
Resistant hypertension
A + C + D + consider further diuretic3, 4 or alpha- or
beta-blocker5
Consider seeking expert advice
Step 1
Step 2
Step 3
KeyA – ACEI or low-cost ARB C – Calcium-channel blocker (CCB) D – Thiazide-like diuretic
Stepwise Ladder Approach

Possible underlying cause
• Any clue in history or examination of a secondary cause, eg. low potassium, proteinuria, hematuria
• Raised serum creatinine
• Sudden onset or worsening of hypertension
• Resistant to multi-drug regimen (> 3 drugs)
• Young age (<40 years)
Indications for Specialist referral

Therapeutic problems• Multiple drug intolerance
• Multiple drug contraindications
• Persistent non-compliance
Special situations• Unusual blood pressure variability
• Possible ‘white coat’ hypertension
• Hypertension in pregnancy
Indications for Specialist referral

GLOBAL RISK REDUCTION
ADD-ON TREATMENT
Aspirin 75 mg/d if high renal and CV risk,TOD,DM with BP controlled <150/90
Statin: Without previous CVD moderately high CV risk to target LDL 115 mg/dl Overt CHD target LDL 70 mg/dl
FOLLOW UP Once a month initially.More often if high
risk
If BP at goal and stable review at 3-6 m
Serum creatinine & electrolyte in 6-12 m
Consider reducing doses and number of agents after one year at or below goal BP

TAKE HOME MESSAGES Measure BP accurately and record Take adequate time to diagnose
hypertension Decide BP target, try to hit it, tell
target to patient Use low cost, tolerated drugs in a
effective combination Address CV risk reduction, decide on
LDL, HbA1c targets and try to hit Convince the patient for follow up

Compelling and possible indications, contraindications, and cautions for the major classes of antihypertensive drugs Class of drug
Compelling indications
Possible indications
Caution
Compelling contraindications
Beta-blockers MI, Angina
Heart failure Heart failure, PVD,
Diabetes (except with CHD)
Asthma/COPD, Heart block
CCBs (dihydropyridine)
Elderly, ISH Angina - -
CCBs (rate limiting)
Angina Elderly Combination with beta-blockade
Heart block Heart failure
Thiazide/thiazide-like diuretics
Elderly ISH Heart failure 2 o stroke prevention
Gout

BP NOT CONTROLLED Improper BP measurement (large cuff) Poor compliance Volume overload- Inadequate diuretic,
Excessive salt intake, progressive renal failure Failure to modify lifestyle- Weight gain,
Stressful life, Excessive alcohol Drugs- NSAIDs, OCP, herbal medicine Obstructive sleep apnoea Unsuspected secondary cause
INFORMATION TO A NEWLY DIAGNOSED PATIENT
“You are at significant risk of heart attack, stroke and kidney damage.
“This risk can be significantly reduced by reducing your BP to target level”
“Your target blood pressure is 140/90 (or less)”

INFORMATION TO A NEWLY DIAGNOSED PATIENT
Most people need 2 or more drugs to control their blood pressure and need to stay on them for life
Most medications take several weeks to show their full effect so be patient
You need to visit every two weeks to adjust drug doses
INFORMATION TO A NEWLY DIAGNOSED PATIENT
Medications only work if you take them!
Stopping a treatment when blood pressure returns to normal can cause your blood pressure to rise again to dangerous levels

INFORMATION TO A NEWLY DIAGNOSED PATIENT
Because the medications have controlled the blood pressure does not mean that the blood pressure has been completely cured
Your treatment is life longLife style changes, healthy diet,
physical activity and reduce mental stress are helpful

CARE PATHWAY
CBPM ≥160/100 mmHg & ABPM/HBPM
≥ 150/95 mmHg
Stage 2 hypertension
Consider specialist referral
Offer antihypertensive drug treatment
Offer lifestyle interventions
If younger than 40 years
If TOD, established CVD,CKD,DM or 10-year CV risk > 20%
Offer review of care to monitor blood pressure, provide support and discuss lifestyle, symptoms and medication
Offer patient education to support adherence to treatment
CBPM ≥140/90 mmHg & ABPM/HBPM ≥ 135/85 mmHg
Stage 1 hypertension

HEALTHY DIET A high sodium diet can increase blood
pressure
Choose more often• Fresh fruits and vegetables• Low-fat milk products• Whole grains• Low-fat meat, fish, chicken
and turkey• Use herbs and spices to
replace salt• Foods with 5% or less of the
daily value of sodium
Choose less often• Fast food, restaurant and
packaged foods• Foods with more than the
15% daily value of sodium• Ketchup, mustard, soy
sauce, gravy• Pickled foods, olives, salsa,
chips• Cured/smoked meat or fish
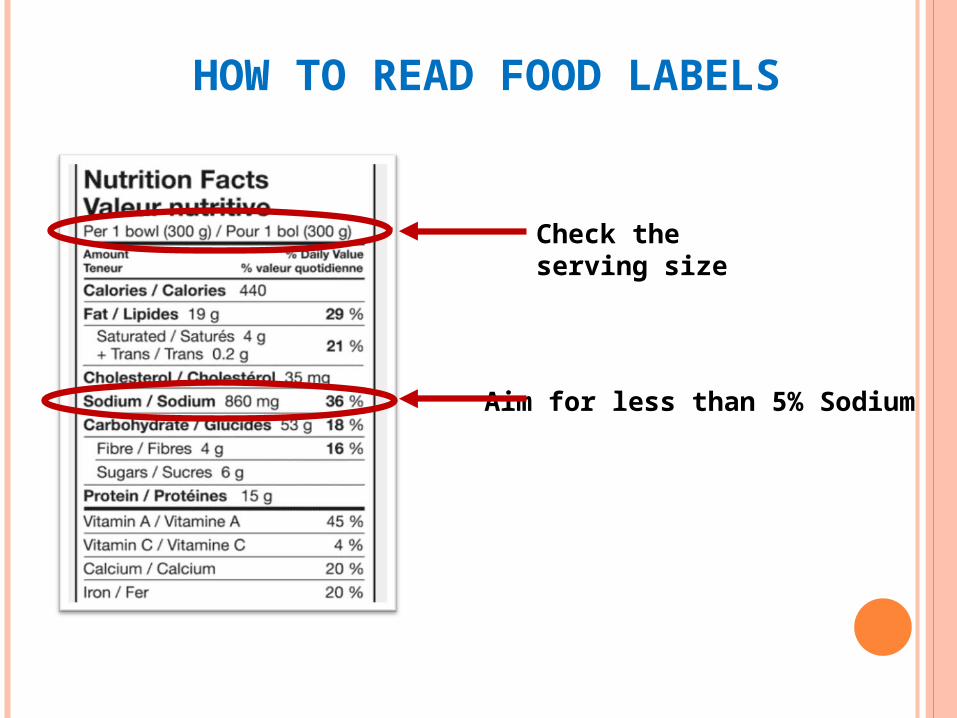
HOW TO READ FOOD LABELS
Check the serving size
Aim for less than 5% Sodium