Hypertension And Blood Pressure Management Guidelines In
12
Version 3 December 2016 - Review December 2019 Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward (Consultant Paediatric Nephrologists) Page 1 of 12 SETTING Bristol Royal Hospital for Children (BRHC) and Neonatal wards, St Michael’s Hospital FOR STAFF Medical and nursing staff caring for children with suspected hypertension PATIENTS Children with suspected hypertension _____________________________________________________________________________ GUIDANCE Definitions of hypertension 1. Systolic or diastolic blood pressure > 95th centile for BP by sex, age and height with an appropriately sized cuff, measured on three occasions. [1] 2. ‘Hypertensive crisis’ is the term used to describe acute elevation in blood pressure that can rapidly cause end-organ damage. Can be further subdivided into hypertensive urgency where patients with an acutely elevated blood pressure may manifest symptoms (headache and nausea etc.) but have no evidence of acute target-organ injury. Or hypertensive emergency which is associated with evidence of acute target-organ injury. Hypertensive crisis requires urgent investigation and management and will commonly require IV anti- hypertensives to safely lower the blood pressure. [2] 3. Prehypertension: Mean systolic or diastolic ≥ 90 th percentile but ≤ 95 th percentile (or ˃120/80mmHg, even if BP below the 90 th percentile for sex, age and height) [1] Measurement of blood pressure in children 1. Children over 3 years of age should have their blood pressure measured at least once during every hospital admission [1, 3] 2. Children under the age of 3 years should have their blood pressure measured as clinically indicated. [1, 3] 3. A range of cuff sizes from newborn to large adult should be available (see table 1) [1] 4. Blood pressure should be measured with the weight of the arm supported after the child has been sitting quietly for at least 3 minutes using an appropriately sized cuff 5. The appearance of Korotkoff sound (K1) should be used to define the systolic blood pressure and the disappearance of Korotkoff sounds (K5) should be used to define the diastolic blood pressure when auscultation is used to measure blood pressure [3] Clinical Guideline HYPERTENSION AND BLOOD PRESSURE MANAGEMENT IN CHILDREN Extended until May 2022
Hypertension And Blood Pressure Management Guidelines In
Hypertension And Blood Pressure Management Guidelines In
ChildrenAuthor(s) Ann Ratcliffe (registrar) Jan Dudley, Carol
Inward (Consultant Paediatric Nephrologists)
Page 1 of 12
SETTING Bristol Royal Hospital for Children (BRHC) and Neonatal
wards, St Michael’s Hospital
FOR STAFF Medical and nursing staff caring for children with
suspected hypertension
PATIENTS Children with suspected hypertension
_____________________________________________________________________________
GUIDANCE Definitions of hypertension
1. Systolic or diastolic blood pressure > 95th centile for BP by
sex, age and height with an appropriately sized cuff, measured on
three occasions. [1]
2. ‘Hypertensive crisis’ is the term used to describe acute
elevation in blood pressure that can
rapidly cause end-organ damage. Can be further subdivided into
hypertensive urgency where patients with an acutely elevated blood
pressure may manifest symptoms (headache and nausea etc.) but have
no evidence of acute target-organ injury. Or hypertensive emergency
which is associated with evidence of acute target-organ injury.
Hypertensive crisis requires urgent investigation and management
and will commonly require IV anti- hypertensives to safely lower
the blood pressure. [2]
3. Prehypertension: Mean systolic or diastolic ≥ 90th percentile
but ≤ 95th percentile (or 120/80mmHg, even if BP below the 90th
percentile for sex, age and height) [1]
Measurement of blood pressure in children
1. Children over 3 years of age should have their blood pressure
measured at least once during every hospital admission [1, 3]
2. Children under the age of 3 years should have their blood
pressure measured as clinically indicated. [1, 3]
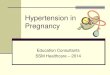
3. A range of cuff sizes from newborn to large adult should be
available (see table 1) [1]
4. Blood pressure should be measured with the weight of the arm
supported after the child has
been sitting quietly for at least 3 minutes using an appropriately
sized cuff
5. The appearance of Korotkoff sound (K1) should be used to define
the systolic blood pressure and the disappearance of Korotkoff
sounds (K5) should be used to define the diastolic blood pressure
when auscultation is used to measure blood pressure [3]
Clinical Guideline
Extended until May 2022
Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward
(Consultant Paediatric Nephrologists)
Page 2 of 12
6. If an automated oscillometric device is used to measure blood
pressure and it is found to be elevated then manual measurements
should be obtained. [4]
7. Centile charts should be available to allow interpretation of
blood pressure measurement (appendix 1) [1, 5]
8. Elevated blood pressure should be confirmed on at least 3
occasions before characterising a child as having hypertension. The
appropriate time interval depends on the clinical circumstances.
Reactive causes of hypertension for example emotion, activity or
pain should be excluded.
9. Consider ambulatory BP monitoring [6, 7, 8]. This may be helpful
in cases of uncertainty, where three BP measurements are borderline
or anxiety cannot be excluded.
Neonatal Blood Pressure
Normal blood pressure in newborn babies depends on a variety of
factors (gestational age, postnatal age, and birth weight).
The incidence of hypertension in healthy newborn babies is very low
(estimated 0.2%) and routine screening is not recommended.
[9]
Hypertension is more common in ‘at-risk’ newborns (those admitted
to NICU) and incidence ranges from 0.7-2.5%. [9]
The Care Quality Commission have recommended that NHS England ask
NICE to develop national guidance on which babies require blood
pressure monitoring and the frequency of observations.[19]
There is no current definitive national or international reference
ranges of ‘normal’ neonatal blood pressure. Tables of estimated BP
values after 2 weeks of age have been synthesised from current
available date.(see appendix 2) [9]
Aetiology of Hypertension
Secondary hypertension is more common than primary hypertension in
children under 10 and the younger the child the more likely that a
definable cause will be identified. Primary hypertension is more
likely in children over 10 years especially if they are overweight,
obese of there is a family history of hypertension. [4]
Table 1 [1]: Available cuff
sizes
Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward
(Consultant Paediatric Nephrologists)
Page 3 of 12
Underlying causes of secondary hypertension (Appendix 3) [10]: 1.
Renal disease (80%). [4] 2. Reno-vascular disease (10%). [4] 3.
Cardiovascular (Coarctation of the aorta should be excluded) 4.
Endocrine causes 5. Central Nervous System 6. Genetic 7. Autoimmune
8. Miscellaneous
Investigations First line:
pulse and blood pressure • Fundoscopy • Consider stigmata of
underlying cause
• Urinalysis and early morning urine for protein:creatinine ratio
and albumin:creatinine ratio.
• Urine for MC+S if suggestive history of Urinary Tract Infection
(UTI) or abnormal urinalysis
• Urea &Electrolytes /Bicarbonate/Bone profile / Magnesium /
Full Blood Count /Thyroid Function/Random Glucose/Random Lipids
(with fasting if results indicate)
• Ultrasound of abdomen and renal tract with doppler imaging of
renal vessels • Consider ambulatory BP monitoring (ABPM).
Interpretation needs comparison with
an appropriate reference range; reference values provided by the
German Working Group on Paediatric Hypertension are currently
considered the best available data for paediatric ABPM [11,
12]
• Further assessment of end organ damage ECG/ECHO/CXR •
Ophthalmology
Second Line: For indication, discuss with Paediatric
Nephrologist
• DMSA (radionuclide scan using dimercaptosuccinic acid) • Renin
and aldosterone (consider whether any current medications could
influence
result). Ideally collect after patient has been awake for 2 hours
and seated for 5-15 minutes.
• Suspected Cushings disease (reduced linear growth with increased
weight): 24 hour urine free cortisol (at least 2 tests) or
dexamethasone suppression test on liason with endocrinology.
• Suspected phaeochromocytoma: Urinary catecholamines (ideally 24
hour collection but random sample if not). High clinical suspicion
– plasma metanephrines
• Suspected neuroblastoma: Urine VMA (Vanillylmandelic acid) and
HVA (Homovanillic acid). • Urine steroid profile – very rarely
indicated and requires discussion with consultant
nephrologists and biochemistry. (indications are suspected apparent
mineralocorticoid excess or congenital adrenal hyperplasia)
Extended until May 2022
Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward
(Consultant Paediatric Nephrologists)
Page 4 of 12
• MRA/Renal angiography/MRI Non-pharmacological management
Lifestyle changes are recommended for children with established
hypertension and pre- hypertension. Consider addressing the
following:
• Sodium restriction • Weight loss • Exercise • Attention to other
cardiovascular risk factors: Control of blood lipids, glycaemic
control
in diabetes
Oral maintenance treatment
Aim to maintain BP <95th centile in children with uncomplicated
primary hypertension with no
evidence of end organ damage and <90th centile in children with
renal impairment (Chronic Kidney Disease [CKD] ≥ stage 2), diabetes
or evidence of end organ damage. [1, 13]
Choice of oral agents (see Specific considerations for treatment of
hypertension):
1. Angiotensin converting enzyme inhibitors (ACEI; e.g.
enalapril/lisinopril) or angiotensin II receptor antagonists (ARB;
losartan, irbesartan)
a. May cause hyperkalaemia. Monitor serum potassium; check levels
within 7 days of starting or increasing dose
b. Avoid if renal artery stenosis suspected c. Avoid in the early
period after renal transplantation
2. Beta blockers: Metoprolol has selective blockade and non-renal
excretion. a. Use if concerns about the possibility of renal artery
stenosis or ACEI/ARB
contraindicated 3. Calcium channel blockers: Amlodipine/ nifedipine
4. Consider diuretics if fluid overload is contributing
Once daily dosing schedules improve compliance
Emergency management of Hypertensive Crisis: Discuss with
paediatric nephrologist
• Patients may require management on PICU/renal ward or appropriate
HDU setting • Slow reduction over 72 hours to avoid sudden drop in
perfusion pressure which may cause
catastrophic cerebral ischaemia. Aim to drop by no more than 25% of
the overall planned BP reduction over the first eight hours of
treatment [14]. Avoid mydriatics for fundoscopy so pupillary
responses can be monitored
Extended until May 2022
Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward
(Consultant Paediatric Nephrologists)
Page 5 of 12
• Site 2 IV cannulae. One is used to deliver IV antihypertensive
agent and the second to
deliver a 10ml/kg 0.9% sodium chloride bolus if the blood pressure
falls significantly.
• The choice of IV agent should be the one with which the clinician
is most familiar with and can include the following: Labetalol /
Nicardipine / Sodium Nitroprusside. These agents should be
administered using a sliding scale to titrate dose administered
with BP, measured every 15 minutes (usually monitored via arterial
line in patients on PICU) – liaise with nephrologist for
details
Once control has been established with parenteral agents, convert
to oral agents as above.
Specific considerations for treatment of hypertension
1. Following renal transplantation there is no evidence that any
antihypertensive agent is better than any other but the use of
angiotensin converting enzyme inhibitors or angiotensin II receptor
antagonists are not generally used in the first 3 months post
transplant. [15] Calcium channel blockers are a sensible choice and
there is evidence that use of these agents in the peri-operative
period reduce the incidence of post-transplant acute tubular
necrosis [16].
2. Phaeochromocytoma. This is characterised by episodic
hypertension/palpitations and
sweating. Control of hypertension is required before surgery
generally using alpha and then beta blockade.[17] This should be
discussed with a consultant anaesthetist pre-operatively.
3. Renovascular disease. This is characterised by very high renin
levels and may be secondary to renal artery stenosis or obstruction
to vessels by cysts in polycystic kidney disease. In this
situation, intra-glomerular pressure depends on efferent arteriolar
constriction and therefore ACE inhibitors or angiotensin II
receptor antagonists must be used with caution as these agents
cause efferent arteriolar dilatation. Investigations may include:
MRA/Angiography. Treatment: metoprolol / amlodipine / other.
4. Rare single gene disorders GRA (glucocorticoid remedial
hyperaldosteronism), Gordons,
Liddle syndrome [18] and AME (apparent mineralocorticoid excess)
are characterised by hypertension due to interruption of the
renin-aldosterone axis. They are often associated with hypo- or
hyperkalaemia and diagnosis is with a urine steroid profile.
Treatment includes the use of potassium sparing diuretics.
Extended until May 2022
Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward
(Consultant Paediatric Nephrologists)
Page 6 of 12
References
1. The fourth report on the diagnosis, evaluation, and treatment of
high blood pressure in children and adolescents. Pediatrics
(2004)114: 555-576
2. Patel NH, Romero SK , Kaelber DC. Evaluation and management of
pediatric hypertensive crises: hypertensive urgency and
hypertensive emergencies. Open Access Emergency Medicine (2012);
4:85–92.
3. Lurbe, Empar, Cifkova, et al. Management of high blood pressure
in children and adolescents: recommendations of the European
Society of Hypertension. Journal of Hypertension Sep 2009 vol 27:
issue 9: p 1719-1742
4. Ingelfinder J. The Child or Adolescent with Elevated Blood
Pressure. N Engl J Med 2014; 370: 2316-25
5. Jackson LV, Thalange NK, Cole TJ. Blood pressure centiles for
Great Britain. Arch Dis Child (2007) 92: 298-303
6. Soergel M, Kirschstein M, Busch C, et al. Oscillometric
twenty-four-hour ambulatory blood pressure values in healthy
children and adolescents: a multicenter trial including 1141
subjects. J Pediatr (1997) 130: 178-184
7. Flynn JT. Urbina EM. Pediatric ambulatory blood pressure
monitoring: indications and interpretations. J Clin Hypertension
(2012); 14: 372-82
8. Butani L, Morgenstern BZ. Are pitfalls of oscillometric blood
pressure monitoring preventable in children? Pediatr Nephrol (2003)
18: 313-8
9. Dionne J, Abitbol C, Flynn JT. Hypertension in Infancy:
Diagnosis, management and outcome. Pediatr Nephrol (2012) 27:
17-32
10. Singh D, Akingbola O et al. Emergency Management of
Hypertension in Children (2012). International Journal of
Nephrology: Article ID 420247, 15 pages
11. Flynn JT, Daniels SR Update: Ambulatory Blood Pressure
Monitoring in Children and Adolescents. A Scientific Statement From
the American Heart Association. Hypertension. 2014; 63:
1116-1135.
12. Wühl E, Witte K, et al. German Working Group on Pediatric
Hypertension. Distribution of 24-h ambulatory blood pressure in
children: normalized reference values and role of body dimensions.
J Hypertens (2003); 21:2205-2206
13. National Kidney Foundation Kidney Disease Outcomes Quality
Initiative (NFK KDOQI) - Clinical Practice Guidelines on
Hypertension and Antihypertensive Agents in Chronic Kidney
Disease
14. Flynn JT, Tallus K. Severe hypertension in children and
adolescents: pathophysiology and treatment. Pediatr Nephrol.
2009;24(6):1101
15. Post operative care of the renal transplant recipient (2011).
The Renal Association. 16. Shilliday I, Sherif M (2007) Calcium
channel blockers for preventing acute tubular
necrosis in kidney transplant recipients. Cohrane Database Syst Rev
4: CD003421 17. S. G. Waguespack, T. Rich et al. A Current Review
of the Etiology, Diagnosis, and
Treatment of Pediatric Pheochromocytoma and Paraganglioma (2011).
JCEM; 95: 5 18. Warnock DG. Liddle syndrome: an autosomal dominant
form of human hypertension.
Kidney Int (1998) 53: 18-24 19. Care Quality Commission Report July
2016: Identifying and managing clinical risks in
Extended until May 2022
Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward
(Consultant Paediatric Nephrologists)
Page 7 of 12
_____________________________________________________________________________
None
SAFETY Children with hypertensive crises should be managed in a
suitable environment e.g. renal unit/HDU/PICU by experienced staff
Blood Pressure should not be allowed to fall abruptly in
hypertensive crisis and therefore short acting nifedipine should be
avoided as its absorption and efficacy is unpredictable. These
guidelines were produced in good faith by the authors reviewing
available evidence. They were designed for use by medical and
nursing staff at the Bristol Royal Hospital for Children for
children under their care. Responsibility for use of these
guidelines lies with the individuals caring for the patients.
QUERIES Contact the on-call Paediatric Nephrology registrar on
bleep 2938 if any queries or to make a referral
Extended until May 2022
Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward
(Consultant Paediatric Nephrologists)
Page 8 of 12
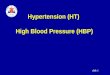
Appendix 1: BP percentiles in children and adolescents [1] (based
on mercury sphygomanometry)
Extended until May 2022
Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward
(Consultant Paediatric Nephrologists)
Page 9 of 12
Extended until May 2022
Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward
(Consultant Paediatric Nephrologists)
Page 10 of 12
Appendix 2: Estimated BP values after 2 weeks of age in infants
from 26 to 44 weeks post conceptual age. [9]
Extended until May 2022
Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward
(Consultant Paediatric Nephrologists)
Page 11 of 12
Renal
Author(s) Ann Ratcliffe (registrar) Jan Dudley, Carol Inward
(Consultant Paediatric Nephrologists)
Page 12 of 12
Genetic