Embed Size (px)
Citation preview

Hypersensitivity Pneumonitis
(HP)
By : ziba Loukzadeh, M.DOccupational Medicine
departmentYazd University of Medical
Sciences

Definition
Immune (hypersensitive) response Extrinsic allergic alveolitis:
granulomatous, interstitial, bronchiolar and alveolar-filling lung diseases caused by repeated exposure and subsequent sensitization to a variety of organic and chemical antigens

Etiology
Microbial agents
Animal proteins
Low molecular weight chemicals

Microbial agentsBacteria
-Farmer’s lung -Bagassosis -Mushroom worker’s lung
Fungi -Wood pulp worker’s lung -Cheese washer lung Ameba -Humidifier lung

Bacteria
cause occupation
Agent source
Major antigen
Farmer's lung
Agriculture worker
Moldy hay
thermoactinomycet
Mushroom worker's
Mushroom worker
Compost thermoactinomycet
Bagassosis Bagass worker
Moldysugarcane
thermoactinomycet

Animal proteins
Avian proteins : Bird breeder’s lung
Urine ,Serum ,Pelts : Animal handler’s lung
Wheat weevil : Wheat weevil lung

Chemicals
Isocyanate HP TDI , MDI , HDI
TMA HP Trimellitic anhydride

Pathogenesis
Immunology Repeated inhalation of antigens
sensitization immunology response(type III,IV) influx of neutrophiles shift T lymphocytes (~70%)(predominantly of CD8)
Antibodies in HP are IgG class Response delay by 3-8 hours

Pathogenesis (cont’)
Host factors -Non smokers > smokers
-Polymorphism in TNF-α gene
-No association with HLA

Pathogenesis (cont’) Exposure factors: -Ag concentration -Duration of exp. -Frequency & intermittency of exp. -Particle size -Use of respiratory protection Farmer's lung disease: winter Bird breeder's lung: summer Indirect exposure

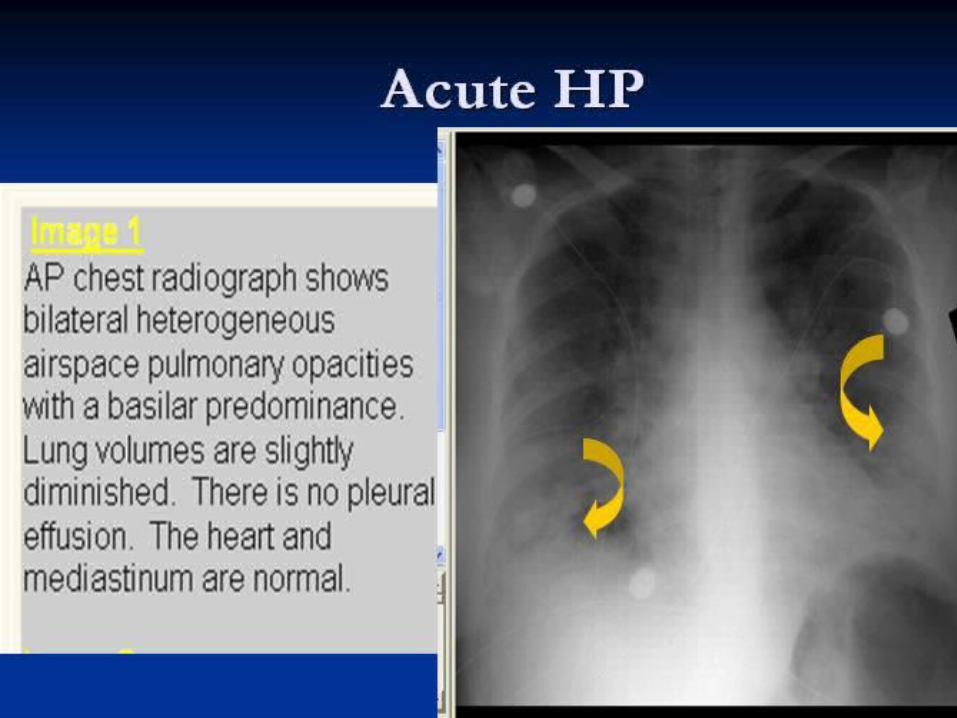
Clinical features Acute HP :
fever ,chill ,myalgia ,cough & dyspnea + basilar rales in Ph/E (4-12 h after heavy exp. )Recurrent febrile episodes (most frequent presentation)
Subacute & chronic HP : insidious onset of respiratory symptoms ,malaise , fatigue , weight loss + basilar rales ,wheezing cyanosis ,right sided HF in Ph/E

DDx
Inhalation fevers others granulomatous
disorder(Sarcoidosis) immunologic disease (Asthma) infection fibrotic lung disease (IPF)

Comparison HP& Inhalation fever
Feature HP Inhalation fever
Example Farmer`s lung disease
Metal fume fever
Etiology Thermoactinomyces
Zinc fume fever
pathophysiology
Hypersensitive reaction
Cytokine- mediated (??)
Exposure dose
Low dose High dose
Sensitization required
Yes No

Comparison HP& Inhalation fever
(cont´)Feature HP Inhalation
feverFever Yes Yes
Flu-like syndrome
Yes Yes
Cough Expected Not necessary
Dyspnea Yes Not typically
Chest exam Rales normal

Comparison HP& Inhalation fever
(cont´)Feature HP Inhalation
feverCXR Alveolar
infiltrationNo
PFT Decreased DLCO&volums
Minimal change
BAL Lymocytosis Inincreased Neutrophiles
Chronic sequle
~yes None
Natural Hx Reccurent or progressive
Complete recovery within 3 day

Lab. studies
Precipitin Ab: Helpful but not specific, not sensitive, not
hallmark
Leukocytosis ,mild elevation of ESR ,CRP , IgG , IgA ,IgM ,ACE ,ANA

PFT
Normal (early dis.) Restrictive Obstructive Mixed decreased DLCO (most sensitive
physiologic test in early HP )
CXR Acute : diffuse ground glass ,fine
nodular or reticulonodular pattern (lower lung )
Subacute : reticulonodular pattern
Chronic : fibrosis ,reticular opacity, honey combing
mediastinal lymphadenopathy (up to 50%)

HRCTGround glass Centrilobular nodules Airspace consolidation Mosaic pattenFibrosis Emphysema


Normal CXR





Histopathology
Classic triad :
cellular bronchiolitis lymphoplasmocytic interstitial
infiltration non-necrotizing granuloma

diagnosis
Temporal relationship between symptoms and certain activities is often the first clue to the diagnosis of HP

diagnosis
environmental history: pets and other domestic animals hobbies such as gardening and lawn
care recreational activities, for example, use
of hot tubs and indoor swimming pools use of humidifiers, cool mist vaporizers,
and humidified air conditioners moisture indicators such as leaking,
flooding, or previous water damage to carpets and furnishings

Diagnostic criteria
Required appropriate exposure
dyspnea on exertion inspiratory crackles lymphocytic alveolitis
Supportive recurrent febrile episodes
infiltrative on CXR decreased DLCO precipitating antibodies granulomatous on lung biopsy improvement with contact avoidance

Treatment
Best treatment : Removal from exp. Preferred approach : Elimination of
Ag. Oral corticosteroid : in severe or
progressive disease O2 ,inhaled steroid & B-agonist in
airflow limitation






























