Embed Size (px)
Citation preview

HYPERKALEMIA WORSHOP
♣Que ,Francesca Lin, Yun Hsing ♣
Reyes, Elaine♣

POTASSIUM IN THE BODY• Potassium: major ion of the body. • Nearly 98% intracellular ( Na+/K+–ATPase pump) • The ratio of intracellular to extracellular potassium is
important in determining the cellular membrane potential.
• A balance of GI intake and renal potassium excretion achieves long-term potassium balance.
• Normal potassium level: 3.5-5.0 mEq/L, • Total body potassium stores are approximately 50
mEq/kg (3500 mEq in a 70-kg person).

HYPERKALEMIAdefined as a potassium level greater than 5.5 mEq/L Ranges are as follows: 5.5-6.0 mEq/L - Mild condition 6.1-7.0 mEq/L - Moderate condition 7.0 mEq/L and greater - Severe condition

CAUSES OF HYPERKALEMIA

A. Decreased or impaired potassium excretion •Decreased GFR (eg, acute /chronic renal failure) - most common•Decreased mineral corticoid activity (Addison’s dse)Defect in tubular secretion (eg, renal tubular acidosis II and IV) Drugs (eg, NSAIDs, cyclosporine, potassium-sparing diuretics)
B. Excessive endogenous potassium load•Internal hemorrhage/ Hemolysis •Rhabdomyolysis
C.Exogenous potassium load•Parenteral administration•Excess in diet •Potassium supplements/Salt substitutes
D.Transmembrane shifts / Redistribution•Metabolic Acidosis (uncontrolled DM) •Insulin deficiency•Drugs (e.g.beta-blockers,digoxin,succinylcholine)
E.Factitious or pseudohyperkalemia •Hemolysis (in lab tubes) / Venipuncture - most common•Thrombocytosis , Leukocytosi

HISTORY TAKING• Hyperkalemia can be difficult to diagnose clinically because
complaints may be vague. • Frequently is discovered as an incidental laboratory finding.• Patients may be asymptomatic or report the following:
– Generalized fatigue– Weakness– Paresthesias– Paralysis– Palpitations
• Hyperkalemia is suggested in any patient with a predisposition toward elevated potassium level.

PHYSICAL EXAMINATION• Evaluation of vital signs (to determine hemodynamic stability & presence of arrhythmias)• Cardiac examination may reveal extrasystoles, pauses, or
bradycardia.• Neurologic examination may reveal diminished deep tendon
reflexes or decreased motor strength.• In rare cases, muscular paralysis and hypoventilation may be
observed.• Search for the stigmata of renal failure, such as edema, skin
changes, and dialysis sites.• Look for signs of trauma that could put the patient at risk for
rhabdomyolysis

CASE SCENARIO
A 62 year old male diabetic with chronic kidney disease and a creatinine level of 3.5 mg.dl with an estimated GFR of of 15ml/min. He has been eating fruits with each meal for the past two weeks . he consulted because of inability to lift himself from a chair.
On PE, he was conscious with BP 110/ 70. PR 90/min, RR 28/min. He had pale, palpebral conjunctivae, poor skin turgor, and marked proximal weakness. The rest of the findings were normal.
12L ECG showed peak T-waves and some widening of the P wave and QRS complex. Lab exams showed Na 130 meq/L, K 8.5 meq/L, Cl 98 meq/L, HCO 7meq/L , SCr 3.5 mg/dl . Arterial pH 7.30, CBG 400 mmol/L , serum acetone (+).
SALIENT FEATURES
62 year old diabetic chronic kidney disease poor skin turgor marked proximal weakness 12L ECG : peak T-waves widening of the P wave and QRS complex
CHIEF COMPLAINT : inability to lift himself from a chair
.

Lab ResultsNa (136-145 meq/L) 130 meq/L HYPONATREMIA
K (3.5-5.0 meq/L) 8.5 meq/L HYPERKALEMIA
Cl (98-106 meq/L) 98 MEQ/L NORMAL
HCO3 (21-30 meq/L) 7meq/L METABOLIC ACIDOSIS
pH (7.35-7.45) 7.30
Crea (<1.5 mg/dL) 3.5 mg/dL

1. What are the most likely factors responsible for the elevation of the plasma K+ concentration?
Diabetes Insulin deficiency and hypertonicity (e.g. hyperglycemia) promote K+ shift from ICF to ECF
Chronic kidney disease ↓ renal K+ excretion: impaired secretion or diminished distal solute
delivery ↓ K+ secretion by principal cells: impaired Na+ reabsorption or ↑ Cl-
reabsorption in acute oliguric renal failure: ↑ K+ release from cells (acidosis, catabolism)
and ↓ excretion in chronic renal insufficiency: ↑ distal flow rate and K+ secretion per
nephron compensate for decreased renal mass --- adaptive mechanisms eventually fail to maintain K+ balance when GFR falls below 10-15 ml/min or oliguria ensues
1. Eating fruits with each meal for the past 2 weeks ↑ K+ intake rarely the sole cause of hyperkalemia since the phenomenon of potassium
adaptation ensures rapid K+ excretion in response to increases in dietary consumption

2. How do you know that this is not pseudohyperkalemia?
Pseudohyperkalemia• artificially elevated plasma K+ concentration due to K+
movement out of cells immediately prior to or following venipuncture
• Contributing factors– prolonged use of a tourniquet with or without repeated fist
clenching– hemolysis and marked leukocytosis or thrombocytosis: elevated
serum K+ concentration due to release of intracellular K+ following clot formation
• should be suspected in an otherwise asymptomatic patient with no obvious underlying cause.
If proper venipuncture technique is used and a plasma (not serum) K+ concentration is measured, it should be normal.

SIGNS & SYMPTOMS

3. What are the signs and symptoms of hyperkalemia in this patient?Explain the pathophysiology.
A. Marked proximal weakness
Increase in membrane excitability
RMP closer to threshold potential
depolarization
Na channel become inactivated
Decrease in excitability

B . Metabolic Acidosis
Hyperkalemia
Inhibits ammoniagenesis
Reabsorption of NH4
Impaired net acid secretion
K moves out of the cell

C. ECG changes
• Peaked T waves – ventricular repolarization• Widening of the P wave – atrial depolarization• & QRS complex – ventricular depolarization
• decrease membrane potential
•Decreases upstroke velocity
•Slows intraventricular conduction
•Depression of conduction in myocardium

Peaked t-waves in hyperkalemia
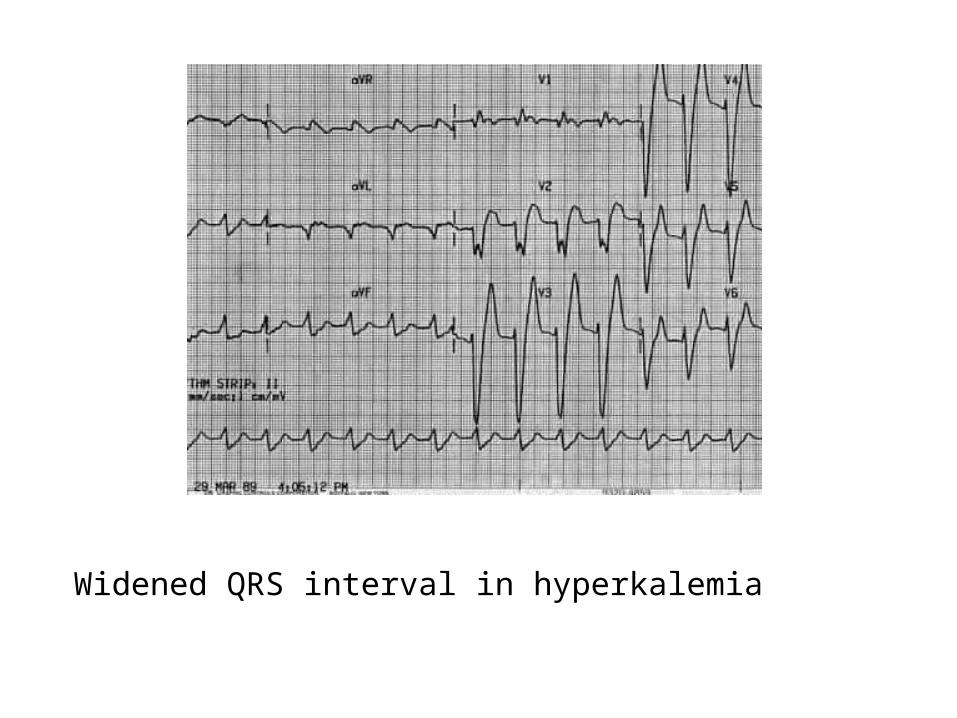
Widened QRS interval in hyperkalemia

Treatment

1. Immediate discontinuation of all sources of potassium intake and agents that affect potassium homeostasis
2. Emergency treatment – reversal of membrane abnormalities by giving:
• Calcium gluconate (Decrease membrane excitability) – 10mL of 10% solution infused in 2-3min– repeat if no change in electrocardiogram after 5-10min
• Hypertonic sodium chloride (for hyponatremic patients)

3. Redistribution of potassium from extracellular space to intracellular space using:
• Intravenous sodium bicarbonate• Insulin and glucose• Stimulation of β2 adrenergic
receptors – Salbutamol + nebulization

4. External removal of potassium through:• Stools
– Sodium polystrene sulfonate is a cation exchange resin that promotes the exchange of sodium for potassium in the GIT
• Urine– Loop + thiazide diuretics enhances renal excretion if renal function is
adequate.
• Dialysis– Hemodialysis
» Most rapid & effective– Peritoneal dialysis
» 15 – 20% as effective ashemodialysis

5. Treatment of underlying cause:• Dietary modification• Correction of metabolic acidosis• Volume expansion• Administration of exogenous mineralocorticoid





























