Embed Size (px)
Citation preview

A
C
HE
E
a
b
c
R
hO
2
cta Otorrinolaringol Esp. 2012;63(1):68---71
www.elsevier.es/otorrino
ASE STUDY
yperfunctional Parathyroid Carcinoma With Mediastinalxtension�
manuele Ferri,a,∗ Enrico Armato,a Francisco José García Purrinos,b Riccardo Manconic
Servicio de Otorrinolaringología, Hospitales de Dolo y Mirano, Venecia, ItalyServicio de Otorrinolaringología, Hospital del Mar Menor, Murcia, SpainServicio de Anatomía Patológica, Hospitales de Dolo y Mirano, Venecia, Italy
eceived 20 July 2010; accepted 2 November 2010
KEYWORDSCarcinoma;Parathyroid;Hyperparathyroidism;Parathyroid hormone
Abstract Parathyroid carcinoma (PC) is an extremely rare malignancy, of which 0.005% are ofall tumours and between 0.5% and 5% of all parathyroid neoplasms. Preoperative diagnosis isoften difficult and is almost always obtained only after post-surgical histopathology. The prog-nosis is related to the local extent of disease and to complete surgical resection of the tumour.
We report an uncommon case of hyperfunctional PC with mediastinal extension, emphasisingthe diagnostic difficulties, histopathological features and treatment strategies. The most recentdata in the literature are analysed as well.© 2010 Elsevier España, S.L. All rights reserved.
PALABRAS CLAVECarcinoma;Paratiroides;Hiperparatiroidismo;Parathormona
Carcinoma hiperfuncionante paratiroideo con extensión mediastínica
Resumen El carcinoma de paratiroides (CP) es una neoplasia maligna extremadamente rara,que constituye el 0,005% de todos los tumores y entre el 0,5 y el 5% de todas las neoplasias delas paratiroides. El diagnóstico clínico de CP es difícil y en la mayoría de los casos se realiza trasel examen histopatológico. El pronóstico está vinculado a la extensión local de la enfermedad
y a la radicalidad de la extirpación quirúrgica.Presentamos un raro caso de CP hiperfuncionante con extensión mediastínica, enfatizandolas dificultades diagnósticas, las características histopatológicas, las estrategias terapéuticas,a la luz de los más recientes datos de la literatura médica.
. Tod
© 2010 Elsevier España, S.L� Please cite this article as: Ferri E, et al. Carcinomaiperfuncionante paratiroideo con extensión mediastínica. Actatorrinolaringol Esp. 2012;63:68---71.∗ Corresponding author.
E-mail address: [email protected] (E. Ferri).
I
PnbnFf
173-5735/$ – see front matter © 2010 Elsevier España, S.L. All rights re
os los derechos reservados.
ntroduction
arathyroid carcinoma (PC) is an extremely rare malig-ant neoplasm, which represents 0.005% of all tumours and
etween 0.5% and 5% of all parathyroid neoplasms. It origi-ates in the parenchymatous cells of the parathyroid glands.rom a functional endocrine standpoint, PC is often hyper-unctional, although it represents less than 5% of primaryserved.

Hyperfunctional Parathyroid Carcinoma With Mediastinal Extension 69
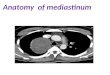
Figure 1 Chest-thorax CT scan, before the intervention.There is an expansive growth, over 5 cm in size and with mediumdensity, at the base of the neck, at the left paramedian level.
Figure 2 EE 5×: tubuloalveolar architecture with subtle,vascular-fibrous septa of relatively monomorphic neoplasm,iw
pauacCr
r(fswyp
ro
D
TaedoTmoioooab
This reaches the upper mediastinum, diverting the trachea con-tralaterally.
hyperparathyroidism causes. Given the rarity of this tumour,no prospective studies on its management exist; its knowl-edge is based both on the description of sporadic cases andon data obtained from retrospective studies. Since the firstdescription by De Quervain in 1904 until the present day,there have been less than 400 cases of PC worldwide. Arecent epidemiological study conducted in the United Statesbetween the years 2000 and 2003 estimated that the inci-dence of PC in the US population was 5.73 per 10 millioninhabitants. Another study showed that this cancer was moreprevalent in Japan compared to Western countries, consid-ering that about 5% of patients with hyperparathyroidismpresented PC. Affecting males and females equally, PC hasa higher incidence between the ages of 45 and 55 years.1---7
We present a rare case of hyperfunctional PC withintrathoracic extension, stressing its preoperative diagnos-tic difficulties, histopathological features and treatmentstrategies, in light of the latest data from the medical liter-ature.
Clinical Case
We present the clinical case of a 76-year-old woman seenin consultation in 2007 following the onset of persistentasthenia, dysphonia and slight dysphagia associated withleft laterocervical swelling. Both a clinical examination anda videolaryngoscopy confirmed the presence of a markedhypomobility of the left hemilarynx with severe functionaladductor deficit.
Following the completion of haematological studies(PTH: 1.184; Ca: 3.3) and instrumental tests (CT, FNAB,ultrasound, PET) (Fig. 1), we suspected the existence ofa ‘‘hyperfunctional parathyroid adenoma’’ as the cause of
hyperparathyroidism. We then proceeded to remove theleft cervical lesion extended to the retrosternal region bycervicosternotomy, including the recurrent and mediastinallymph nodes at the sixth level. During the surgery it wasrh1
ncluding occasional nuclear polymorphisms as well as elementsith a clear and ample cytoplasm.
ossible to preserve the left recurrent nerve, whichppeared compressed by the mass but not infiltrated. Val-es for PTH and calcium dropped significantly in the first 24 hfter the intervention (PTH: 53; Ca: 2.41), with data beingonfirmed 1 week (PTH: 45; Ca: 2.39) and 1 month (PTH: 32;a: 2.35) after the intervention. The definitive histologicalesult was compatible with PC (Fig. 2).
Two years after surgery, the patient suffered a localecurrence (with an increase in PTH and calcium values)PTH: 322; Ca: 3.18), which was treated with further surgery,ollowed by complementary radiation therapy. During thaturgery it became necessary to sacrifice the recurrent nerveith consequent irreversible paralysis of the left hemilar-nx. There were no changes in respiratory rate during theostoperative period.
About 15 months after the second surgery, the patientemains with normal calcium levels and without symptomsf disease.
iscussion
he clinical diagnosis of PC is often difficult and is almostlways obtained, as in the present case, only after a postop-rative histopathological examination. The intraoperativeiagnosis of PC is unreliable because the pathologist maynly raise the suspicion of malignant parathyroid neoplasm.he examination may, in fact, show atypical cytological ele-ents (nuclear pleomorphism, increased mitoses) but not
ther data such as capsular and/or vascular or lymph nodalnvasion that are essential for the diagnosis of PC.8 Intra-perative macroscopic aspects of the tumour such as sizever 3 cm, multilobular surface, solid consistency, presencef a thick fibrous capsule and infiltration of neighbouringnatomical structures may help in the differential diagnosisetween benign and malignant neoplasm.9---11
The clinical criteria for suspicion of malignant parathy-oid neoplasm are: (1) age below 55 years; (2) markedypercalcaemia and hyperparathormonaemia (more than0 times over the limit); (3) severe bone symptoms

7
(scs
daofic
feaisaans
nsaptPaIsslpHKpficd
mDtto2l
thp(gtifTPn
e
fitttas
fcitmc
iraiifghttmIiccdtrudtia
C
T
R
0
fibrocystic osteitis in 40%---70% of cases) and kidneyymptoms (nephrocalcinosis, nephrolithiasis in 30%---60% ofases); (4) recurrent laryngeal paralysis due to tumour inva-ion; (5) palpable cervical swelling in 30%---50% of cases.2
Imaging studies (ultrasound, CT scan, MRI, PET) are notefinitive in the differential diagnosis between adenomand parathyroid carcinoma.10 Fine needle aspiration cytol-gy is not recommended due to both the high probability ofalse negatives (which may influence the surgical approachncorrectly) and to the obvious disruption of the neoplasticapsule with subsequent neoplastic spread.12,13
Even from a histopathological point of view, the dif-erential diagnosis may not be simple. Upon microscopicxamination, some PCs are almost indistinguishable fromdenomas while others are totally anaplastic. The coex-stence of PC with major cell hyperplasia and adenoma,ometimes present in familial forms, is not excluded. Gener-lly, PC is grey and has a larger size compared with adenoma,
hard consistency (due to the consistent fibrous compo-ent), occasional foci of necrosis and signs of infiltration ofurrounding tissues.
Just as there is no tumour staging system (TNM) for PC,o universally accepted grading system has been encodedo far. The dimensions and metastasising of PC do notctually represent parameters that may have a role in itsrognosis.14 The presence of long fibrous stretches and arabecular growth pattern is statistically more common inC. A useful morphological criterion in diagnosis is capsularnd vascular invasion, which is present in over 60% of cases.nfiltration may be limited to the capsule or may spread tourrounding soft tissues (skeletal muscle, thyroid, nervoustructures) with finger-like extension through the capsu-ar collagen fibres. Immunohistochemical tests are usuallyositive for cytokeratin, neuroendocrine markers and PTH.owever, studies of cell cycle proteins p27, bcl-2, mdm2 andi-67 have found that only 30% of cases present 3 molecularhenotypes in PC different from adenoma. Therefore, thesendings have established that the aforementioned proteinsannot be considered as useful markers in the differentialiagnosis.15
From a genetic standpoint, the most frequent abnor-ality in PC is overexpression of oncogene PRAD1/cyclin1, located on chromosome 11. It has been hypothesisedhat cyclin D1 inactivates the product of the retinoblas-oma tumour suppressor gene (RB), thus facilitating thentogenetic process. Such overexpression is also present in0%---40% of adenomas and 60% of hyperplasias, which wouldimit its value as a marker in the differential diagnosis.16,17
A somatic and germinal mutation of the HRPT2umour suppressor gene has been demonstrated in aigh percentage of PC cases associated with inheritedrimitive hyperparathyroidism with mandibular tumourhyperparathyroidism-jaw tumour syndrome, HPT-JT). Thisene is located on chromosome 1q25, which encodes a pro-ein called ‘‘parafibromin’’. This protein can be identifiedn RNA polymerase II and the PAF1 complex, and plays aundamental role in chromatin transcription and modelling.he discovery of similar, apparently sporadic mutations in
C may be indicative of a latent HPT-JT syndrome or a phe-otypic variant.18,19The prognosis of PC is closely linked to local diseasextension at the time of diagnosis, surgical radicality of the
E. Ferri et al.
rst intervention and the possibility of local relapse withinhe first 2 years of treatment. The last scenario may condi-ion a decidedly ominous evolution. When the Ki-67 is morehan 10%, PC has a higher risk of short term recurrence, evenfter radical surgical treatment.20 Percentages of 10-yearurvival range from 49% to 77%.14,21
Regarding secondary locations, PC metastases occur mostrequently in the lungs (40%), the laterocervical lymphatichain (30%) and the liver (10%). Other, less frequentlynvolved areas are the bone, pleura and pericardium. Inhe absence of obvious signs of recurrence, the presence ofetastases can be suspected in cases of persistent hypercal-
aemia or in cases of progressive increase in PTH values.22,23
Surgery is the treatment of choice; block resectionncludes the affected parathyroid gland, the ipsilateral thy-oid lobe, the lymphatic lobes of the recurrent chain and thenatomical structures infiltrated by the neoplasm, includ-ng, if necessary, the recurrent nerve. The purpose of surgerys not only oncological but also endocrine functional. Inact, the morbidity and mortality associated with PC areenerally more related to various functional aspects (PTHypersecretion and severe persistent hypercalcaemia) thano oncological aspects.5 In selected cases of distant metas-ases, it is possible to perform surgical treatment on theetastasis with the use of rapid intraoperative PTH doses.
n patients with disease progression, palliative pharmacolog-cal therapy with bisphosphonates and calcimimetic drugsan be useful to control the symptoms of severe hypercal-aemia, despite having no influence on the prognosis of theisease. Calcimimetic drugs become fixed on calcium recep-ors located on the membrane of parathyroid cells, thuseducing PTH secretion. This mechanism of action has beensed successfully in the case of a patient with metastaticisease.24---26 Despite being considered a radiation-resistantumour, treatment with adjuvant radiotherapy significantlymproves survival. However, the effectiveness of chemother-py has not yet been demonstrated.27
onflict of Interests
he authors have no conflicts of interest to declare.
eferences
1. De Quervain F. Parastruma maligna aberrata. Deutsche ZeitschrChir. 1904;100:334---52.
2. Obara T, Fujimoto Y. Diagnosis and treatment of patients withparathyroid carcinoma: an update and review. World J Surg.1991;15:738---44.
3. Pelizzo MR, Piotto A, Bergamasco A, Rubello D, Casara D.Parathyroid carcinoma: therapeutic strategies derived from 20years of experience. Minerva Endocrinol. 2001;26:23---9.
4. Rao SR, Shaha AR, Singh B, Rinaldo A, Ferlito A. Management ofcancer of the parathyroid. Acta Otolaryngol. 2002;122:448---52.
5. Busaidy NL, Jimenez C, Habra MA, Schultz PN, El-Naggar AK,Clayman GL, et al. Parathyroid carcinoma: a 22-year experi-ence. Head Neck. 2004;26:716---26.
6. Lee PK, Jarosek SL, Virnig BA, Evasovich M, Tuttle TM. Trendsin the incidence and treatment of parathyroid cancer in the
United States. Cancer. 2007;109:1736---41.7. Schoretsanitis G, Daskalakis M, Melissas J, Tsiftsis DD. Parathy-roid carcinoma: clinical presentation and management. Am JOtolaryngol. 2009;30:277---80.

tensi
1
1
2
2
2
2
2
2
2
Hyperfunctional Parathyroid Carcinoma With Mediastinal Ex
8. Cheah WK, Rauff A, Lee KO, Tan W. Parathyroid carcinoma: acase series. Ann Acad Med Singapore. 2005;34:443---6.
9. Shane E. Clinical review 122: parathyroid carcinoma. J ClinEndocrinol Metab. 2001;86:485---93.
10. Lee YS, Hong SW, Jeong JJ, Nam KH, Chung WY, Chang HS,et al. Parathyroid carcinoma: a 16-year experience in a singleinstitution. Endocrine J. 2010;57:493---7.
11. Dudney WC, Bodenner D, Stack Jr BC. Parathyroid carcinoma.Otolaryngol Clin North Am. 2010;43:441---53.
12. Spinelli C, Bonadio AG, Berti P, Materazzi G, Miccoli P. Cutaneousspreading of parathyroid carcinoma after fine neddle aspirationcytology. J Endocrinol Invest. 2000;23:255---7.
13. Thompson SD, Prichard AJ. The management of parathyroidcarcinoma. Curr Opin Otolaryngol Head Neck Surg. 2004;12:93---7.
14. Hundahl SA, Fleming ID, Fremgen AM, Menck HR. Two hun-dred eight-six cases of parathyroid carcinoma treated in theUS between 1985---1995: a National Cancer Data Base Report.Cancer. 1999;86:538---44.
15. Bondeson L, Grimelius L, De Lellis RA. Parathyroid carcinoma.In: De Lellis RA, Lloyd RV, Heitz PU, Eng C, editors. World HealthOrganization classification of tumours. Pathology and Genet-ics of tumours of endocrine organs. Lyon: IARC Press; 2004. p.124---7.
16. Kitola S, Farnebo F, Obara T, Isola J, Grimelius L, Farnebo LO,
et al. Patterns of chromosomal imbalances in parathyroid car-cinomas. Am J Pathol. 2000;157:579---86.17. Mittendorf EA, McHenry C. Parathyroid carcinoma. J Surg Oncol.2005;89:136---42.
2
on 71
8. Shattuck TM, Valimaki S, Obara T, Gaz RD, Clark OH,Shoback D, et al. Somatic and germ-line mutations of theHRPT2 gene in sporadic parathyroid carcinoma. N Engl J Med.2003;349:1722---9.
9. Bradley KJ, Cavaco BM, Bowl MR, Harding B, CranstonT, Fratter C, et al. Parafibromin mutations in hereditaryhyperparathyroidism syndromes and parathyroid tumors. ClinEndocrinol. 2006;64:299---306.
0. Lihara M, Okamoto T, Suzuki R. Functional parathyroid carci-noma: long-term treatment outcome and risk factor analysis.Surgery. 2007;142:936---43.
1. Clayman GL, Gonzalez HE, El-Naggar A. Parathyroid carci-noma: evaluation and interdisciplinary management. Cancer.2004;100:900---5.
2. Hundley JC, Albertson DA, Bradley RF, Levine EA. Resection ofpulmonary metastasis from parathyroid carcinoma. Am Surg.2003;69:779---83.
3. Chiofalo MG, Scognamiglio F, Losito S, Lastoria S, Marone U,Pezzullo L. Huge parathyroid carcinoma: clinical considerationsand literature review. World J Surg Onc. 2005;3:39---46.
4. De Francisco AM. Cinacalcet HCl: a novel therapeutic for hyper-parathyroidism. Expert Opin Pharmacother. 2005;6:441---52.
5. Rodgers SE, Perrier ND. Parathyroid carcinoma. Curr Opin Oncol.2006;18:16---22.
6. Poissonnet G, Castillo L, Bozec A, Peyrottes I, Ettore F, Santini J,
et al. Parathyroid carcinoma. Bull Cancer. 2006;93:283---7.7. Messerer CL, Bugis SP, Baliski C, Wiseman SM. Normocalcemicparathyroid carcinoma: an unusual clinical presentation. WorldJ Surg Onc. 2006;4:10---5.