Embed Size (px)
Citation preview

HYDROCODONE RESCHEDULING AND MEDICAL MARIJUANA
Lynn R. Webster, M.D.Vice President of Scientific Affairs
PRA Health SciencesSalt Lake City, UT
[email protected](801) 892-5140
www.LynnWebsterMD.comTwitter: @LynnRWebsterMD

• AstraZeneca• Cara Therapeutics• Charleston Laboratories• Collegium Pharmaceuticals• Depomed• Egalet• Inspirion Pharmaceuticals• Insys Therapeutics• Kaléo Pharmaceuticals
• Mallinckrodt• Marathon Pharmaceuticals• Merck• Orexo• Pfizer• Proove Biosciences• Signature Therapeutics• TEVA• Trevena• Zogenix
12-Month Financial Disclosures
Updated 10/1/15
The Impact of Hydrocodone Rescheduling in People With Pain:
The First 100 DaysJan F. Chambers1, Rae Marie Gleason1, Kenneth L. Kirsh2,
Bob Twillman3, Lynn Webster4, Jon Berner5, Steven D. Passik2
1National Fibromyalgia & Chronic Pain Association (NFMCPA); 2Millennium Research Institute; 3American Academy of Pain Management; 4PRA Health Sciences; 5Woodinville Psychiatric

Background
• On October 6, 2014, the DEA rescheduled hydrocodone products from
Schedule III to Schedule II in an effort to curb abuse
• The NFMCPA partnered with health care professionals (HCPs), PRA
Health Sciences, the AAPM, and MRI to create a survey to track the
rescheduling consequences on patients’ lives during the first 100 days
Abbreviations: AAPM, American Academy of Pain Management; DEA, Drug Enforcement Administration; MRI, Millennium Research Institute.

Materials and Methods• Survey
• Cross-sectional, anonymous, blinded• IRB approved through Aspire IRB, Santee,
California• Administered online via SurveyMonkey® • Explored patients’ experiences after
hydrocodone rescheduling
Abbreviation: IRB, institutional review board.

Materials and Methods (cont’d)• Participants
• Recruited via newsletters, e-mails, Web pages, and social media by the NFMCPA, the U.S. Pain Foundation, and other patient organizations
• Eligibility requirements• >18 years of age• Had been prescribed hydrocodone
• Survey dates• Launched: February 5, 2015• Closed: April 3, 2015

Respondent Demographics6420 Total Participants
90% Caucasian
90% Women
59% Married
82% At Least Some College
61% PrivateInsurance
53%
19%
Primary Pain Site
Global body Lower back NeckLeg Pelvis Other

18-24 25-34 35-44 45-54 55-64 65-74 75+0
5
10
15
20
25
30
35
Age
Age, y
% o
f R
esp
on
den
ts
FT PT
Homem
aker
Disab
led
Unemplo
yed
Retire
d
Studen
t0
10
20
30
40
50
Employment Status
% o
f R
esp
on
den
ts
Respondent Demographics (cont’d)
Abbreviations: FT, full-time; PT, part-time.

Duration of Hydrocodone Use
• 38% of patients who had been on hydrocodone for at least 1 year had required at least 1 dose escalation
82%
18%
>1 year1 year or less

Hydrocodone Use After Rescheduling13% borrowed hydrocodone because they were unable to refill their prescriptions
18% borrowed hydrocodone to supplement their
prescribed supply

Prescribing Changes After ReschedulingChange in Hydrocodone Prescribinga Reponses, No. (%)None 2296 (39.0)Dose lowered 501 (8.5)Dose lowered with intent to discontinue 343 (5.8)Immediate discontinuation with no substitute 525 (8.9)Alternative drug prescribed 873 (14.8)a Most commonly reported changes are shown.

Changes After Hydrocodone Rescheduling
Hydrocodone Discontinued
(n=1628)
47% consumed alcohol
8% used illicit drugs
62% used marijuana
66% borrowed medications
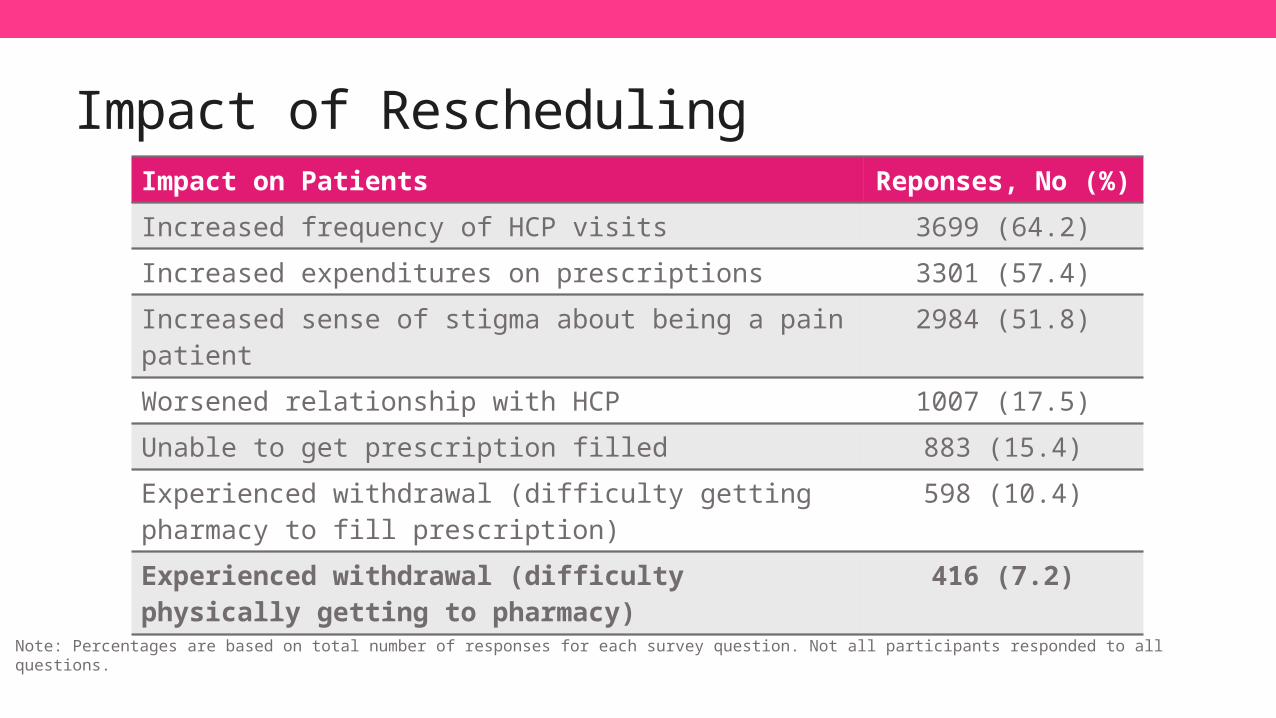
Impact of ReschedulingImpact on Patients Reponses, No (%)
Increased frequency of HCP visits 3699 (64.2)
Increased expenditures on prescriptions 3301 (57.4)
Increased sense of stigma about being a pain patient 2984 (51.8)
Worsened relationship with HCP 1007 (17.5)
Unable to get prescription filled 883 (15.4)
Experienced withdrawal (difficulty getting pharmacy to fill prescription)
598 (10.4)
Experienced withdrawal (difficulty physically getting to pharmacy)
416 (7.2)
Note: Percentages are based on total number of responses for each survey question. Not all participants responded to all questions.

Reasons for Refusal to Fill Prescriptions
Other
Pharmacist believed medication was inappropriate
Pharmacist believed dose was inappropriate
No reason given
Pharmacy no longer stocking hydrocodone
National shortage of medication
No hydrocodone in stock
Not enough medication in stock
0 5 10 15 20 25 30 35 40 45
% of Respondents

Pharmacy Issues
3% of pharmacists refused to submit
hydrocodone claims to an insurance company
9% of pharmacists asked respondents to
pay cash for prescriptions

Alternative Opioids Prescribed
None (30.4%)
Tramadol (22.7%)
Oxycodone (16.7%)
Other (30.2%)

Patient Perspectives on FairnessPatient Perspective on Regulatory Changes Reponses, No. (%)a
Deny chronic pain patients their right to adequate treatment 4288 (88.0)
Will not hinder addicts in their quest to acquire illegal prescription drugs 3673 (75.3)
Will not hinder criminals in acquiring and distributing illegal prescription drugs 3618 (74.2)
Harmful to people with chronic pain 3568 (73.2)
Result in prescription of less effective medications for patients with chronic pain (so doctors can avoid legal hassles) 3427 (70.3)
Have increased my cost of care 2280 (46.8)
a Participants could select >1 response.

Missed Work
Missed Work Because of
Hydrocodone Rescheduling
(n=801)
Increased pain (76%)
Increased number of HCP visits (71%)
More time spent getting prescriptions filled (29%)

Additional Consequences of Rescheduling
19% 27%

Qualitative Data
The hydrocodone rescheduling “makes legitimate chronic pain
sufferers feel as though they are criminals,” and “All we want is to live
life pain-free and be our normal selves again without being treated
like pill addicts.”

Survey Limitations• Sampling bias
– Recruitment via patient advocacy Web sites
– May impact generalizability of findings
• Men not well represented

Conclusions• Negative consequences of hydrocodone rescheduling• Increased pain• Withdrawal symptoms• Inconvenience • Increased cost • Stigma• Alienation from physicians and pharmacists

MEDICAL MARIJUANA

Prevalence of Marijuana Use
Ages 12 to 17 Ages 18 to 25 Ages 26 or Older0%
20%
40%
60%
80%
100%
16%
52%46%
Lifetime Marijuana/Hashish Use
National Institute on Drug Abuse. http://www.drugabuse.gov/drugs-abuse/marijuana. Accessed September 18, 2015.

Marijuana Substance Abuse
Substance Abuse and Mental Health Services Administration. The CBHSQ Report: A Day in the Life of American Adolescents: Substance Use Facts Update. Rockville, MD: Center for Behavioral Health Statistics and Quality; 2013.
Number of Adolescents Admitted to Publically Funded Substance Abuse Treatment Facilities on a Typical Day
Marijuana Alcohol Heroin or Other
Opiates
Stimulants Cocaine Other Drugs
0
50
100
150
200
250
300266
58
12 10 3 8

Legal Status of Marijuana• Illegal at the federal level (classified as Schedule I by the DEA)
Bryn B; American Association for the Advancement of Science. http://www.aaas.org/news/cannabis-new-frontier-therapeutics. Published February 15, 2015. Accessed September 18, 2015.

Cannabinoids in Marijuana• >100 cannabinoids in marijuana• Major cannabinoids: cannabidiol (CBD) and tetrahydrocannabinol (THC)
CBD-type cannabinoids(noneuphoriant)
Δ8-trans-THC-type cannabinoids(euphoriant)
Elsohly MA, Slade D. Life Sci. 2005;78(5):539-548.

Trend Toward Increased THC and Decreased CBD in Illicit Marijuana
Burgdorf JR, Kilmer B, Pacula RL. Drug Alcohol Depend. 2011;117(1):59-61.

Targets of Cannabinoids
Abbreviations: CB1, cannabinoid receptor type 1; CB2, cannabinoid receptor type 2.Peak Pharmaceuticals. http://peakpharma.com/science/overview/. Accessed September 18, 2015.

Signaling via Central CB1 Receptor
Hill MN, Patel S. Biol Mood Anxiety Disord. 2013;3(1):19.

EVIDENCE IN THE LITERATURE OF THE EFFICACY AND SAFETY OF MEDICAL MARIJUANA

CBD Decreased Vomiting Induced by Lithium Chloride
Mean Number of Vomiting Episodes
*p<0.05 vs other groups in study (not all shown).Rock EM, et al. Br J Pharmacol. 2012;165(8):2620-2634.
Vehicle(n=14)
CBD(n=16)

Abbreviations: AEA, anandamide; IL, interleukin.****p<0.0001 vs incubation control; †††p<0.001 vs IL-17A; ††††p<0.0001 vs IL-17A.Harvey BS, Sia TC, Wattchow DA, Smid SD. Cytokine. 2014;65(2):236-244.
Control IncubationControl
IL-17A IL-17A + AEA
IL-17A + hydro-cortisone
IL-17A + CBD
CBD Attenuated Mucosal Damage in a Human Colonic Explant Model
Luminal Epithelial Damage (%)

Summary of Randomized Controlled Studies on Cannabinoids and Pain
Jensen B, Chen J, Furnish T, Wallace M. Curr Pain Headache Rep. 2015;19(10):524.

Summary of Randomized Controlled Studies on Cannabinoids and Pain (cont’d)
Jensen B, Chen J, Furnish T, Wallace M. Curr Pain Headache Rep. 2015;19(10):524.

Cannabinoids in Pain, Meta-analysis
Note: Nabiximols contain THC and CBD.Whiting PF, et al. JAMA. 2015;313(24):2456-2473.

Cannabinoid Safety, Meta-analysis
*Incidence rate = events/person-years. The number of person-years was 445 for cannabinoid exposure and 239 for control.Wang T, Collet JP, Shapiro S, Ware MA. CMAJ. 2008;178(13):1669-1678.

Cannabinoid Safety, Meta-analysis (cont’d)
*Incidence rate = events/person-years. The number of person-years was 445 for cannabinoid exposure and 239 for control; †For both cannabinoid exposure and control, all events in this category were classified as “altered mood”; ‡Due to myocardial ischemia.Wang T, et al. CMAJ. 2008;178(13):1669-1678.

Cannabinoid Safety, Meta-analysis (cont’d)
*Classified according to Medical Dictionary for Regulatory Activities.Wang T, et al. CMAJ. 2008;178(13):1669-1678.

THE IMPACT OF MEDICAL MARIJUANA ON OPIOID ABUSE

Bachhuber MA, Saloner B, Cunningham CO, Barry CL. JAMA Intern Med. 2014;174(10):1668-1673.
Reductions in Death From Opioid Overdose After Medical Marijuana Was Legalized

Impact of Medical Marijuana Dispensaries Treatment Admission for Opioid Pain
Reliever Addiction Opioid Overdose Deaths
Powell D, Pacula RL, Jacobson M. Do Medical Marijuana Laws Reduce Addictions and Deaths Related to Pain Killers? Cambridge, MA: National Bureau of Economic Research; 2015.

THE FUTURE OF MEDICAL MARIJUANA

Evolving Public Opinion
Pew Research Center. http://www.people-press.org/2013/04/04/majority-now-supports-legalizing-marijuana/. Published April 4, 2013. Accessed September 21, 2015.
Options for Improved Regulation• Hold medical marijuana to the same standards as other drugs
• Standardize• Ensure quality control
• More consistently control THC and CBD content

Summary/Next Steps for Medical Marijuana• Cannabinoids are a promising therapeutic option for pain and other
therapeutic areas
• Additional rigorous research is needed
• Legalization facilitates investigations of efficacy and safety

The Painful Truth
• Available now for purchase from online and local retailers
• Find out more at thepainfultruthbook.com
• Watch for “The Painful Truth” Documentary to be released late Fall 2015!

Thank You!
Twitter: @LynnRWebsterMD
www.LynnWebsterMD.com




























