-
8/9/2019 Hydatiform Mole With Hyperthyroid
1/46
HYDATIFORM MOLEWITH HYPERTHYROIDISM
Presented by Adam Ridha
OBSTETRY AND GYNECOLOGY DEPARTMENT
MEDICAL FACULTY TANJUNGPURA UNIVERSITY
RSU DOKTER SOEDARSO
Supervisor
dr Pi!d" #u$"%u&u' Sp OG (K)
-
8/9/2019 Hydatiform Mole With Hyperthyroid
2/46
INTRODUCTIONChapter I
-
8/9/2019 Hydatiform Mole With Hyperthyroid
3/46
Molar pregnancy the incidence appearsto be quite high in South
Asia.1,3
Gestational hrophoblastic !isease pregnancy related group o"
disorders #o"ten fatal in the ast.$
%ydatidi"orm mole a&ects 1#3 ' 1(((pregnancies.$
1() o" hydatidi"orm moles !alignantfo"!s o"
G!*G+.$H#e"th#"oi$is!in complete molarpregnancy ), cured by
e-acuationo" molar tissue.31. Nousheen Aziz, Sajuda Yousfani,
Irfanullah Soomro, Firdous Mumtaz. Original article estational
tro!ho"lastic disease. # A$u" Med %ollA""otta"ad &'1&(
&) *1+
&. Se"ire N. #., Secl M. #. %linical re-ie / estational
tro!ho"lastic disease0 current management of h$datiform mole. M#
&''2( 334. a153,
doi0 1'11367"mj a153. &''2, -ol 334 *)83/82+0 M#
3. 9a-e Nandini, Fernandes Sarita, Am"i :da$, I$er ;ermalata.
%ase
-
8/9/2019 Hydatiform Mole With Hyperthyroid
4/46
CASE REPORTChapter II
-
8/9/2019 Hydatiform Mole With Hyperthyroid
5/46
PATIENT
IDENTITYPatient as e/amined on May $3th, $(10+ame ' Mrs. I
e/ ' 2emaleAge ' 0 years oldAddress ' ui 4a5ap6thnic ' 7ugis8ob
' %ouseholdReligion ' Islam+o. MR ' 9:#:
-
8/9/2019 Hydatiform Mole With Hyperthyroid
6/46
ANAMNESISChieft Co!laint lump in the abdomen since $ months
Histo"# of P"esent Illnes lump in the abdomen since $ months and
"elt
getting bigger. Patient also complained o" decreasedappetite
accompanied by nausea and -omiting,
especially a"ter meals. since 0 days "elt blooddischarge
increasing "rom the genitals, especially atnight hich o"ten "orm a
blood clot. Patientsde"ecate once a ee5, urinate in the normal
range.ince 0 months "elt a lump in the nec5 that is not"elt pain.
ometimes "elt trembling, seating, andpalpitations.
-
8/9/2019 Hydatiform Mole With Hyperthyroid
7/46
Histo"# of O%stet"i&
G 9 P A (M (
No' Te!
at
%e"sal
in
Tahu
n
(enis
e"salin
an
(enis
)ela!i
n
*e"at +,g- ,ea$a
an
ana)
. Rumah 1;9$ pontan P < %idup
/ Rumah 1;90 pontan = < %idup
0 Rumah 1;9 pontan P < %idup
1 Rumah 1;;( pontan P < %idup
2 Rumah 1;;3 pontan P < %idup
3 Rumah 1;;0 pontan = < %idup
4 7idan $(( pontan P 3.9(( %idup
5 >ang ini
-
8/9/2019 Hydatiform Mole With Hyperthyroid
8/46
Histo"# of Disease6Oe"ationhyroid disease ?@
Histo"# of P"esent P"egnan
Menarche age o" 10 years ith a $9#day cycle, theduration o"
days. Much reduced ithout e/cessi-epain. he Brst day o" last period
1: 2ebruary $(10.Pregnancy 13 ee5s 0 days.
Histo"# of So&ial7E&ono!i&
he patient or5ed as a housei"e and ha-e 7P8health insurance
grade 3.
-
8/9/2019 Hydatiform Mole With Hyperthyroid
9/46
General condition' Compos Mentis, ea5
%eart rate ' 10(/*m
Respiration rate ' $/*m
7lood pressure ' 10(*9( mm%g
6ye ' anemic conungti-a ?#*#, icteric sclera?#*#
+ec5 ' mass ?@,palpable thyroid glands, supple,no pain, mobile,
bruit ?#
PHYSICAL E8AMINATION 6
9ENERAL STATUS
-
8/9/2019 Hydatiform Mole With Hyperthyroid
10/46
%eart ' ictus cordis not -isible and palpablein IC ID
midcla-icule sinistra, auscultation1*$ single, regular, mur mur ?#,
gallop ?#
=ungs ' auscultation basic breath sounds-esicular, ronchi ?#*#,
heeEing ?#*#,percusssion sonor in both lungs, "remitustactile in
both lung is same
Abdomen ' abdominal distention ?#, boelsounds ?@, epigastric
pain ?#, palpablesuprapubic mass 11 / 10 cm
65strimities ' pitting edema ?#*#, muscle tone
-
8/9/2019 Hydatiform Mole With Hyperthyroid
11/46
O*STETRIC STATUS
E)ste"nal e:a!ination 2undal height ' one Bnger under
umbilicus
2etal heart rate ' negati-e
Presentation ' # %is ' negati-e
6stimated "etal eight ' #
Inte"nale:a!ination Portio ' thic5 er-ical dilatation ' ( cm
!ecend ' #
Amniotic ' #
-
8/9/2019 Hydatiform Mole With Hyperthyroid
12/46
%aemoglobin ' 11,9 g*d=
Red blood cells ' 0,0$ M*u=
hite blood cells ' .$((*mm3
Plateles ' $$ 4*u=
%aematocrit ' 30,( )
2asting blood glucose ' 1,:mg*d=
SUPPOTI;E E8AMINATION%aematologic e/amination in 1 o" may
$(10
Post#prandial ' 99 mg*d=
Hreum ' 39,1 mg*d=
Creatinine ' (,0 mg*d= A= ' ,( ? 31,( # high
A ' :3, ? 3$,( # high
Albumin ' 0,$ g*d=
-
8/9/2019 Hydatiform Mole With Hyperthyroid
13/46
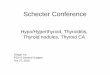
Ra$iolog# e:a!inationin 1 o" May $(10
O%g US9huge uterus ith snow stormappearance i!"ession of !ole
h#$atifo"!
Tho"a: PAthere is no abdormalities in cor and pulmo
-
8/9/2019 Hydatiform Mole With Hyperthyroid
14/46
Diagnosis
%ydati"orm mole in G9 P A( M( 13ee5s 0 days gestation
ithhypertiroidism
-
8/9/2019 Hydatiform Mole With Hyperthyroid
15/46
THERAPHYGeneral condition, -ital signs, -aginal bleeding
obser-asionIntra -enous Fuid dehydration Ringer lactate $(
dpmCurretageConsultation to internist
-
8/9/2019 Hydatiform Mole With Hyperthyroid
16/46
P"ognosis
Ad -itam ' dubia ad bonam Ad "unctionam ' dubia ad malam
Ad sanactionam' dubia ad bonam
-
8/9/2019 Hydatiform Mole With Hyperthyroid
17/46
FOLLOW UP
-
8/9/2019 Hydatiform Mole With Hyperthyroid
18/46
21 of May 2014
' abdominal pain, abdominal lump since $ months andbigger,
appetite ?, nausea J -ommiting ?#, ala%lene&) !ass +
-
8/9/2019 Hydatiform Mole With Hyperthyroid
19/46
-
8/9/2019 Hydatiform Mole With Hyperthyroid
20/46
23 of May 2014 ' nausea ?@
K ' %R ;$ /*m, RR $( /*m, 7P 10(*9( mm%g, Bnetremmor ?@, lab.
Result' 7C .((*mm3, R7C 3,:;M*u=, H* ?= g6$L, HCT /5?0 , P= $9
4*u=
A ' %ydati"orm mole in G9 P A( M( 10 ee5sgestation ith
hypertiroidism @ Ane!ia e'&' @aginal%lee$ing
P '
ID2! R= $( dpm, curretage,
Bhole %loo$ t"ansfusion 02= &&?
Propanolol $ / 1( mg
-
8/9/2019 Hydatiform Mole With Hyperthyroid
21/46
24 of May 2014 ' nausea J -omitting ?@, appetite ?, -aginal
bleeding ?@ decreasing
K ' %R ;$ /*m, RR $( /*m, 7P 1:(*11( mm%g, Bnetremmor ?@, 2undal
heigh 1 Bnger under umbilicus
A ' %ydati"orm mole in G9 P A( M( 10 ee5s 1 daygestation ith
hypertiroidism @ Anemia e.c. -aginalbleeding
P ' ID2! R= $( dpm,
curretage,
Propanolol $ / 1( mg
-
8/9/2019 Hydatiform Mole With Hyperthyroid
22/46
25 of May 2014
=aboratory result' 7C .3((*mm3, R7C 39( M*u=,H* ?1 g6$L, %C $;,
), P= $1; M*u=
-
8/9/2019 Hydatiform Mole With Hyperthyroid
23/46
26 of May 2014
' "eels heat K ' %R 9 /*m, RR $( /*m, 7P 13(*9( mm%g, 2undal
heigh
the same as umbilicus. Re&onsultation to inte"nist +
-
8/9/2019 Hydatiform Mole With Hyperthyroid
24/46
27 of May 2014
' "eels heat ?#, -aginal bleeding ?# K ' %R 11$ /*m, RR $ /*m,
7P 11(*( mm%g, 2undal heigh
the same as umbilicus.
A ' %ydati"orm mole in G9 P A( M( 10 ee5s 0 daysgestation ith
hypertiroidism @ Anemia e.c. -aginal
bleeding @ inus tachycardy
P ' ID2! R= $( dpm,
Propanolol $ / 1( mg
yrosol 1 / 1( mg Bhole %loo$ t"ansfusion 02= &&,
%R e-aluation ?(#1(( /*m
P"o7Histe"e&to!# until sign s#!to!s ofth#"oto:i&osis is
negati@e
-
8/9/2019 Hydatiform Mole With Hyperthyroid
25/46
28 of May 2014 ' -aginal bleeding ?@ minimal, palpitation ?@ K '
%R ;$ /*m, RR $( /*m, 7P 13(*9( mm%g, 2undal
heigh 3 Bnger under umbilicus. Curettage asper"omed, PA
e/amination on mola Fuid and blood. =ab.Result' 7C 9.0((*mm3, R7C
0,$9 M*u=, H* ..?1 g6$L,%C 31,; ), P= $1$ 4*u=
A ' Post &u"ettagein indication o" hydati"orm moleith
hypertiroidism
P ' Propanolol $ / 1( mgyrosol 1 / 1( mg
C#tote: PO / ta%s
%R e-aluation ?(#1(( /*m
-
8/9/2019 Hydatiform Mole With Hyperthyroid
26/46
29 of May 2014 =ab. Result ' W*C '3==6!!0, R7C 0,9; M*u=, H*
./?4g6$L, %C 3,$ ), P= $1 4*u=
-
8/9/2019 Hydatiform Mole With Hyperthyroid
27/46
30 of May 2014 ' complain ?#
K ' %R ;$ /*m, RR $( /*m, 7P 1$(*( mm%g, 2undal heigh3 Bnger
under umbilicus.
A ' Post curettage in indication o" hydati"orm
ithhypertiroidism
P ' Propanolol $ / 1( mg
yrosol 1 / 1( mg
A!o:i&illin 0 : 2== !g
Mefena!i& a&i$ 0 : 2== !g
Ci"oo:a&in / : 2== !g
Waiting PA "esult
Rontgent tho"a: PA
Out atient? )lini& &onsultation.
-
8/9/2019 Hydatiform Mole With Hyperthyroid
28/46
LITERATURERI;IEW
Chapter III
-
8/9/2019 Hydatiform Mole With Hyperthyroid
29/46
INTRODUCTION Gestational trophoblastic neoplasia ?G+ is
comprised o" a spectrum o" conditions, each o"hich is
characterised by lo incidence and highcure rates.$,0
&. Se"ire N. #., Secl M. #. %linical re-ie / estational
tro!ho"lastic disease0 current management of h$datiform mole. M#
&''2( 334. a153,
doi0 1'11367"mj a153. &''2, -ol 334 *)83/82+0 M#
). Phillip a-age. Clinical "atures o" molar pregnancies and
gestatioal trophoblastic neoplasia
-
8/9/2019 Hydatiform Mole With Hyperthyroid
30/46
HYDATIFORM
MOLE Molar pregnancies and G+ origin "rom the
placental trophoblast.
+ormal trophoblast yncytiotrophoblast in-ades the endometrial
stroma
ith implantation o" the blastocyst and is the cell typethat
produces human chorionic gonadotropin ?hCG.
Cytotrophoblast "unctions to supply the syncytium ithcells in
addition to "orming outpouchings that become
the chorionic -illi co-ering the chorionic sac. Intermediate
trophoblast is located in the -illi, the
implantation site, and the chorionic sac.
3 types trophoblast G! hen they proli"erate.
6. #ohn
-
8/9/2019 Hydatiform Mole With Hyperthyroid
31/46
%ydatidi"orm moles are abnormal conceptions ith
e/cessi-eplacental, and little or no "etal, de-elopment.
rophoblastic proli"eration ?cytotrophoblast J
syncytiotrophoblast and -esicular selling o" placental
-illiassociated ith an absent or an abnormal "etus*embryo.
he to maor typesLcomplete and partial ?C%M and P%M.
A&ect omen 1 yo J :( yo, tin or multiple gestation.
-
8/9/2019 Hydatiform Mole With Hyperthyroid
32/46
C%M undergo early and uni"orm hydatidenlargement o" -illi in the
a%sen&eo" anascertainable fetus o" e!%"#o, the trophoblast
isconsistently hyperplastic ith -arying degrees o"atypia, and
-illous capillaries are absent.:,
P%M demonstratei$entia%le fetal o"e!%"#oni& tissue,
chorionic -illi ith "ocaledema that -ary in siEe and shape,
scalloping and
prominent stromal trophoblastic inclusions, and a"unctioning
-illous circulation, as ell as "ocaltrophoblastic hyperplasia ith
mild atypia only.:,
-
8/9/2019 Hydatiform Mole With Hyperthyroid
33/46
CLINICAL
PRESENTATION Most common abnormal -aginal bleeding at #1 ee5s o"
gestation.:,3
Palpable uterus larger than the gestational ageaccording to the
last normal menstruationperiod.:,3
%yperemesis gra-idarum, anemia,hyperthyroidism, -ery high le-els
o" N#%CG and
pre#eclampsia be"ore $( ee5s o" gestation. %istory o" passing
hydropic -esicles or grape#li5e pieces o" tissue.:,3
-
8/9/2019 Hydatiform Mole With Hyperthyroid
34/46
DIA9NOSIS Hltrasounddiagnostic tool in diagnosing molar
pregnancy O C%M
hos mi/ed echogenic pattern, comprising
hydropic -illi, an absent "etus and no amniotic Fuid,e/hibiting
sno storm patternQ ith or ithouttheca lutein cysts
Hltrasound appearance is non#speciBc, andthere"ore molar
pregnancies are "requentlymisdiagnosed as incomplete
miscarriages
Hltrasound Bnding in cases o" P%M, includes a "etus?sometimes
groth restricted, amniotic Fuid and"ocal areas o" anechogenic
spaces in the placenta.
-
8/9/2019 Hydatiform Mole With Hyperthyroid
35/46
-
8/9/2019 Hydatiform Mole With Hyperthyroid
36/46
MANA9EMENT !ilatation and suction e-acuation is the standard
treatment o" all patients presenting ith a possiblediagnosis o"
molar pregnancy.:
2ull blood count, coagulation proBle, renal "unctionassessment,
li-er "unction test, thyroid "unctions,quantitati-e N#%CG le-el,
and blood groupcompatibility, chest #ray and C scan in
selectedcases.
-
8/9/2019 Hydatiform Mole With Hyperthyroid
37/46
HYDATIFORM MOLE WITHHYPERTHYROIDISM
2all in % suggests that it is %CG that causesincreased secretion
o" 3 and 0.
%yperthyroidism ?deBned as a suppressed % ith
raised 23 or 20 is more common in trophoblasticdisease than
normal pregnancy.
%CG in G! enhanced tyrotrophic acti-ity.
-
8/9/2019 Hydatiform Mole With Hyperthyroid
38/46
DISCUSSIONChapter ID
-
8/9/2019 Hydatiform Mole With Hyperthyroid
39/46
Mrs. I>, )6 $o
2 ?4
A"dominal lum!since & months
1: 2ebruary$(10A!!etite @@
N7B
Baginal "leeding CC
=um! in the nec
since ) months D
trem"ling, seating,
and !al!itations
tach$cardia
1)'72' mm;g
uterus / &'/ees gestation
;$datiform mole in 2?4 13 ees gestation
E% sinus tach$cardia
sno storm a!!earance
th$roid/function CC
;$!erth$roidism
anemia
M"!"*e+e!$
-
8/9/2019 Hydatiform Mole With Hyperthyroid
40/46
rophoblastic hyperthyroidism thyroidstimulation by hCG
he clinical "eatures
fatigue, eight loss,muscle ea5ness, e:&essi@e
sBeating,ner-ousness, heat intole"an&e, ta&h#&a"$iaand
minimal enla"ge!ent of the th#"oi$glan$.
-
8/9/2019 Hydatiform Mole With Hyperthyroid
41/46
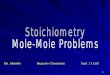
Ta%le /' Th#"oi$ Fun&tion Test
$$ o" May
$(10
TSH +=?/4 7 1?4
IU6!L-=?=.1
T0 +=?/ /?00
n!ol6L-1?35
T1 +3= ./=
n!ol6L-/4?43
-
8/9/2019 Hydatiform Mole With Hyperthyroid
42/46
-
8/9/2019 Hydatiform Mole With Hyperthyroid
43/46
Propanolol $ / 1( mg
yrosol 1 / 1( mg !ilatation and curretage
-
8/9/2019 Hydatiform Mole With Hyperthyroid
44/46
CONCLUTION Mrs. I, 0 years old ith diagnose o" hydati"orm mole
in G9 P %. 13
ee5s ith hyperthyroidism and anemia. he management hich is
gi-enis'
ID2! R= $( dpm
Curretage
Propanolol $ / 1( mg
yrosol 1 / 1( mg
Amo/icillin 3 / :(( mg
Me"enamic acid 3 / :(( mg
CiproFo/acin $ / :(( mg
aiting PA result
Rontgent thora/ PA
Kut patient, 5linic consultation.
-
8/9/2019 Hydatiform Mole With Hyperthyroid
45/46
REFERENCES1. +ousheen AEiE, auda >ous"ani, Ir"anullah oomro,
2irdous MumtaE. Kriginal article O Gestational
trophoblastic disease. 8 Ayub Med Coll Abbottabad $(1$S $0 ?1.
!onloaded "romhttp'**.ayubmed.edu.p5*8AMC*$0#1*+ousheen.pd"
$. ebire +. 8., ec5l M. 8. Clinical re-ie # Gestational
trophoblastic disease' current management o"hydati"orm mole. 7M8
$((9S 33. a1;3, doi' 1(113*bm a1;3. $((9, -ol 33 ?0:3#:9' 7M8.
!onloaded"rom
http'**.eottd.com*p#content*uploads*$(1$*(1*=ybol.pd"
3. !a-e +andini, 2ernandes arita, Ambi Hday, Iyer %ermalata.
Case Report O hydati"orm mole ithhypertiroidism O perioperati-e
challanges. 8 obstet gynecol india -ol. :;, no. 0 S uly*agust $((;
pg 3:#3:.!onloaded "rom
http'**medind.nic.in*aq*t(;*i0*aqt(;i0p3:.pd"
0. Phillip a-age. Clinical "atures o" molar pregnancies and
gestatioal trophoblastic neoplasia. !onloaded"rom
http'**.isstd.org*isstd*chapter(9TBles*G!3R!C%(9.pd"
:. !eep 8.P., =.7. edhai, 8. +apit, 8. Pariyar. Re-ie article O
Gestational trophoblastic disease. 8ournal o"Chitan Medical Collage
$(13S 3?0' 0#11. !onloaded "rom
http'**.cmc.edu.np*images*gallery*Re-ie)$(Articles*an5DRe-ie)$(Articles)$($.pd"
. 8ohn R. =urain. Gestational trophoblastic disease I'
epidemiology, pathology, clinical presentation anddiagnosis o"
gestational trophoblastic disease, and management o" hydati"orm
mole. $(1(, american ournalo" obstetric and gynecologis' mosby,
Inc. doi'1(.1(1*.aog.$(1(.(.(3. donloaded
"romhttp'**ournalsconsultapp.else-ier#eprints.com*uploads*articles*aog1.pd"
. al5ington =., 8 ebster, 7..%ancoc5, 8. 6-erard, R.6. Coleman.
%yperthyroidism and human chorionicgonadotrophin production in
gestational trophoblastic disease. 7ritish 8ournal o" Cancer ?$(11
1(0, 1:#1;' cancer research H4. !onloaded
"romhttp'**.nature.com*bc*ournal*-1(0*n11*pd"*bc$(1113;a.pd"
-
8/9/2019 Hydatiform Mole With Hyperthyroid
46/46
TERIMA,A
SIH
UTU